28
A A place for Beta Blocker Agents in Perioperative : When and How Ike Sri Redjeki Department of Anesthesiology and ICU Medical Faculty/ Padjadjaran University Bandung
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | kuncupcupu1368 |
| View: | 45 times |
| Download: | 0 times |

A A place for Beta Blocker Agents in Perioperative : When and How
Ike Sri Redjeki Department of Anesthesiology and ICU Medical Faculty/ Padjadjaran University
Bandung

Introduction to β-blockers Are a class of drugs used for – Management of cardiac arrhythmia – Cardioprotection after myocardial infarction – Once first-line treatment for hypertension (their role was
downgraded in June 2006 in the United Kingdom to fourth-line) – Propanolol was the first clinically useful beta adrenergic receptor
antagonist – Direct sympatho adrenal inhibition à reduction of heart rate à
play a major role in the therapeutic efficacy of beta-blockade in congestive heart failure
– In chronic heart failure à the myocardium undergoes a phenotype change à alterations of the activity of enzymes regulating calcium homoeostasis

Site of action of beta blocker

Indications
• Reduction of risk of cardiovascular mortality in the early phase following an acute MI in hemodynamically stable patients
• Treatment of mild to moderate hypertension (in which a cardioselective beta-blocker is preferred)
• Angina pectoris when oral therapy is not feasible • Management of hypertensive urgencies • Peri -operative, cardioselective beta blockade,
when indicated • Possible therapy in acute aortic dissection

Indication of Beta Blocker Therapy
• Hypertension • Arrhythmias • Angina/Coronary artery disease • Acute coronary syndromes • Congestive Heart Failure • Postmyocardial infarction • Perioperative
Role of Peri-operative Beta-Blockers • Beta -blockers are used to correct the imbalance between
myocardial oxygen demand and supply in times of stress • Reduce HR: increase diastolic time and increase coronary artery
perfusion • Reduce myocardial oxygen consumption by suppressing
lipolysis, causing myocardium to metabolize more glucose compared to free fatty acid
• May increase stability of coronary atherosclerotic plaques • May increase the threshold for ventricular fibrillation in presence
of ischemia

Important question; the use of beta blocker in perioperative period
• Which patients should be targeted ? • What is the optimal time to begin these agents, and when
should they be stopped ? • Which type of beta blocker should be used ? • How can a practical and effective strategy be
implemented at hospitals on the basis of this evidence ?

Which patients should be targeted ?
Minor criteria • Age > 65 years • Current smoking • Hypercholesterolemia • Hypertension
Major criteria • History of MI, angina, or any
revascularization, Q waves on ECG, current or past use of nitroglycerine
• History of transient ischemic attack or cerebrovascular accident
• Diabetes • Vascular surgery planned for
arteries of chest, abdomen, or pelvis
• Creatinin > 2mg/dl


Patients at risk who should not received Beta Blockers
2 type of patients : • Focus primarily on the patients ability to handle fluids
load and cardiac output : congestive heart failure caused by depressed ejection fraction and systolic dysfunction à beta blocker therapy improves long term survival in these group à but it should not be started in the perioperative period as part of routine practice
• Focus on improving myocardial perfusion à patients with physiologically significant aortic valvular disease beta blocker should not be given

What is the optimal time to begin these agents, and when should they be stopped ?
• Pre – induction period à still an unanswered question • It seems sensible to try to developed an approach in which beta
blocker started as far in advance as possible à giving the opportunity to titrate the drug to an effective heart rate before surgery
• But last minute identification and administration on the day of surgery are likely to be effective
• Longer treatment with beta blocker appears to extend the protective benefit of adrenergic blockade
• For patients who do not require lifelong beta blocker therapy à th/ up to 30 days à provides maximal protective benefit

Which type of beta blocker should be used ?
• Metoprolol is probably the most common agent available à the parenteral form can lead directly to oral administration à for NPO ( R/ Farpressor )
• Short acting beta blocker à esmolol à for unstable patients
• Atenolol

Prehospitalization / immediately following admission • Giving metoprolol 25 – 100 mg/ PO bid • Begin as outpatient surgery up to 30 days prior
to surgery • Titrate new or pre-existing beta blocker to heart
rate of < 65/minute
Preoperative Period ( in pre-anesthesia holding area )
• All Patients : Give metoprolol 5 mg iv every 10 minute to reach target heart rate before induction anesthesia if needed
In hospital period and transition to oral medication à Patients not taking oral medication who are hemodynamically stable • Metoprolol 5 mg iv every 15 minute up to 15 mg titrate
to heart rate of 65/mnt repeat every 6 hour à monitoring continuous ECG
• Alternatives à clonidin ICU patients à HD unstable caused by blood loss or prolonged surgery • Esmolol 500micr/kg iv over 1 minute then infuse 50 –
200 micr/kg/min to target heart rate • May also use metoprolol per floor protocol
One of the most crucial practices in the use of
perioperative beta blocker Is
They be titrated in such a way that a target heart rate
is achieved

Important data àβ-blockers for ICU and perioperative
• Metoprolol iv àwhen it was infused over 10 minute à in normal volunteers à maximum beta blockade was achieved at approximately 20 minute
• Doses 5 – 15 mg à reduced HR ( after stimulation ) 10% - 15%
• Half – life of drug à 2.8 hour • Drug disappeared approximately after 5 – 8 hour ( à 5 –
15 mg administration)

Potential Hazard of iv B-Blocker
• Cardiac failure • Severe sinus bradycardia: antidote à atropine • Partial heart block à antidote à atropine; if
unresponsive à isoproterenol or temporary pacing • Bronchospasm antidote à salbutamol • Profound beta-blockade à antidote when other
measures have failed à glucagon

Side Effect Management
• Beta – blocker / Metoprolol à only used in stable HD patients ( not shock state à MAP and peripheral perfusion)
• AV – Block à if occur after drug administration à Give SA 0.25 – 0.5 mg iv
• Hypotension : if systolic BP < 90 mmHg à give fluids and positive inotropic, if associated with bradycardia à SA
• Pheochromocytoma: B-Blocker should be used in combination with alpha – blocker à to avoid paradoxical increase in BP due to the attenuation of B-mediated vasodilatation in skeletal muscle
• In à DM à may mask tachycardia in hypoglycemia

Perioperative Beta Blocker
• The stress induced by surgery can cause an asymptomatic coronary plaque unstable and rupture à resulting complete occlusion of a portion of the coronary artery
• The perioperative risk associated with unstable plaque can be reduced pharmacologically with : aspirin, statin and chronic beta – blocker therapy
• POISE trial à ( 2008 ) – 9298 patients , RCT, > 45 years old patients, non cardiac surgery,
at high risk of atherosclerotic disease – Intervention : metoprolol 2 – 4 hour start preoperatively and
continued for 30 days

Risk Stratification
Revised Cardiac Index ( RCI )
Risk Factors High risk surgery (intraperitoneal, intrathoracic, aortic) Ischemic heart disease (prior MI, angina, nitrate use) History of CHF History of cerebrovascular disease Insulin therapy for diabetes Preoperative serum Cr >2.0 mg/dl
Points 1 1 1 1 1 1
(Lee et al, Circula.on 1999; 100: 1043)

Risk Stratification
Revised Cardiac Index *Cardiac Complication: MI, CHF, VF, complete heart block (Lee et al, Circulation 1999; 100: 1043)
Class # Factors Cardiac Complication Rate*
I 0 0.5%
II 1 1.3%
III 2 3.6%
IV 3-6 9.1%

Risk Stratification
Clinical Markers (ACC/AHA Guidelines JACC, 2002)
Major Intermediate Minor " ACS " Decompensated CHF " Significant arrhythmia " Severe valvular disease
" Mild angina " Prior MI " Compensated CHF " Diabetes Mellitus
" Advanced age " Abnormal ECG " Rhythm other than sinus " Low functional capacity " Prior CVA " Uncontrolled HTN
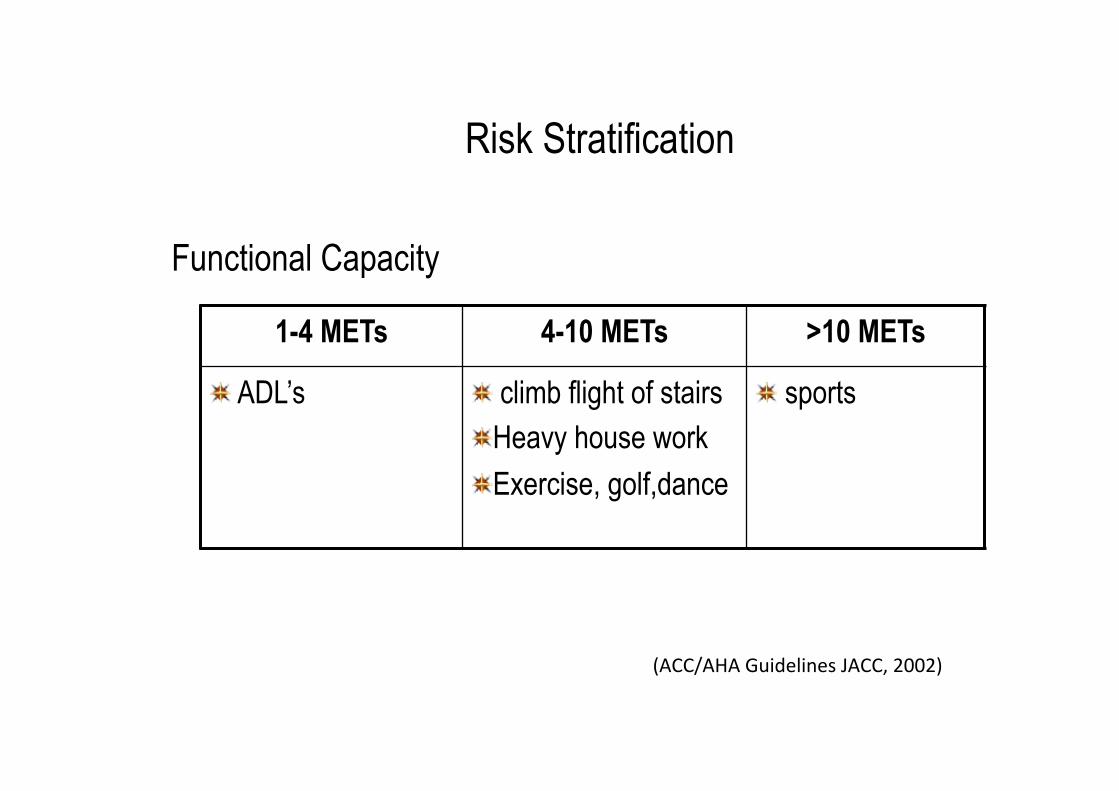
Risk Stratification
Functional Capacity
(ACC/AHA Guidelines JACC, 2002)
1-4 METs 4-10 METs >10 METs
" ADL’s " climb flight of stairs " Heavy house work " Exercise, golf,dance
" sports

Risk Stratification
Surgery Specific Risk
(ACC/AHA Guidelines JACC, 2002)
High > 5% Risk of MI/Death
Intermediate < 5% Risk of MI/Death
Low < 1% Risk of MI/
Death " Emergent surgery " Aortic or other major vascular surgery " Peripheral vascular " Prolonged surgery
" Carotid endarterectomy " Head and Neck " Intraperitoneal " Intrathoracic " Orthopedic " Prostate
" Endoscopic " Superficial " Cataract " Breast
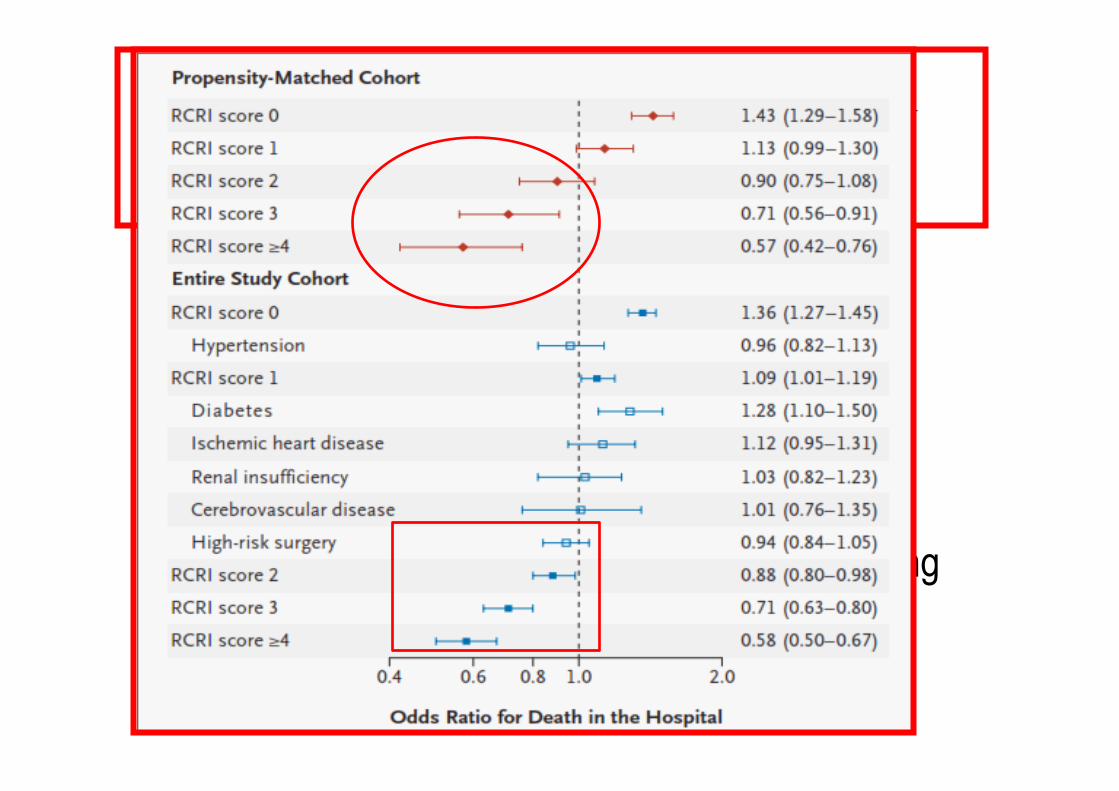
• Conclusion : – Perioperative B blocker therapy is associated
with a reduced risk of in hospital mortality à among the High Risk patients – But not in low risk patients – Patient safety may be enhanced by increasing
the use of B blockers in high risk patients
NEJM 2005 ; 349-61

Normalization of cellular
metabolsm
Decrease cardiac
dysfunction Cytokine
effect
Improved glucose metabolism

Preeclampsia with immediate post operative hypertension
• Post operative post SC patients à HR increase to 170x/ mnt and BP increase to 190/99 mmHg
• ECG à ST depression in Lead I, II, III • SpO2 99% with nasal catheter 2l/mnt • Conscious cm, with no other symptoms • NRS à 1, no pain only not comfortable

Preeclampsia with immediate post operative hypertension
• Metoprolol iv ( R/ Farpressor) strart with 2,5 mg à 15 minute, in 10 minute BP decrease to 170/87 mmHg à HR 160 x/ mnt
• Another 2,5 mg iv was given in 5 minute à HR decrease to 100/ mnt and BP 160/80 mmHg
• Patients was observed for 2 hours HR 105/mnt with BP 163/78 mmHg
• Another 2,5 mg metoprolol iv was given and patients HR 76 – 84 / mnt with PB around 130 – 140 systolic / 75 – 80 mmhg diastolic
Conclusions
If you want to use beta blocker à use them sensibly, carefully, and act directly à for
complication

















