British Juurrtal of Urology (1974), 46, 209-214 Bilateral Breast Metastases from Carcinoma of the Prostate JAMES SCOTT, A. H. T. ROBB-SMITH and IAN BURNS United Oxford Hospitals In patients with carcinoma of the prostate who develop breast tumours the differentiation between primary breast pathology and prostatic metastases is difficult to determine by conventional histological techniques. However, histochemical analysis of tuniour tissue for its acid phosphatase content may provide the diagnosis, as illustrated in the following case. Case Report A 75-year-old male presented in October 1970 with a 3-month history of anorexia and urinary frequency. There were no associated symptoms and no relevant past history. On examination the only significant findings were that he was clinically anaemic, had a firm non-tender fixed mass in the left supraclavicular fossa, and an enlarged irregular prostate with obliteration of the median sulcus. Fig. 1. Shows bilateral breast enlargement. There is some bruising of the right breast at the biopsy site. Laboratory investigations: Haenioglobin, 6.5 g per 100 ml; E.S.R. 160 mm in the first hour; a blood film showed an early leucoerythroblastic picture; urea, 33 mg per 100 ml; serum acid phosphatase 260 units. I.V.P. showed a mild bilateral hydronephrosis and a moderate residual volume of urine after micturition. Radiography showed several sclerotic deposits in the lumbar spine and pelvis. Biopsy of the supraclavicular mass revealed 209
Transcript
British Juurrtal of Urology (1974), 46, 209-214
Bilateral Breast Metastases from Carcinoma of the Prostate
JAMES SCOTT, A. H. T. ROBB-SMITH and IAN BURNS
United Oxford Hospitals
In patients with carcinoma of the prostate who develop breast tumours the differentiation between primary breast pathology and prostatic metastases is difficult to determine by conventional histological techniques. However, histochemical analysis of tuniour tissue for its acid phosphatase content may provide the diagnosis, as illustrated in the following case.
Case Report
A 75-year-old male presented in October 1970 with a 3-month history of anorexia and urinary frequency. There were no associated symptoms and no relevant past history. On examination the only significant findings were that he was clinically anaemic, had a firm non-tender fixed mass in the left supraclavicular fossa, and an enlarged irregular prostate with obliteration of the median sulcus.
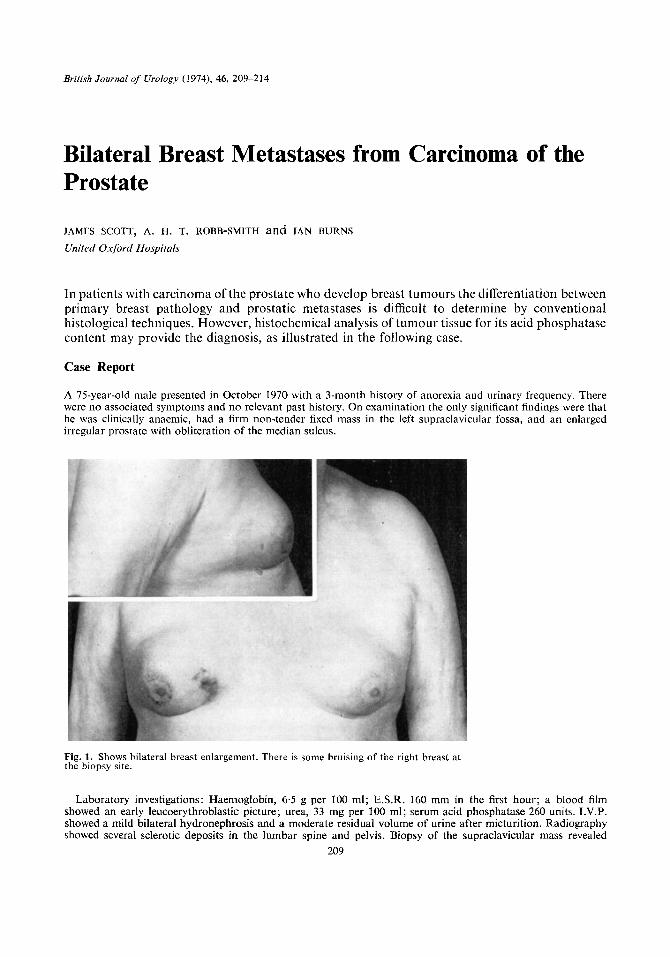
Fig. 1. Shows bilateral breast enlargement. There is some bruising of the right breast at the biopsy site.
Laboratory investigations: Haenioglobin, 6.5 g per 100 ml; E.S.R. 160 mm in the first hour; a blood film showed an early leucoerythroblastic picture; urea, 33 mg per 100 ml; serum acid phosphatase 260 units. I.V.P. showed a mild bilateral hydronephrosis and a moderate residual volume of urine after micturition. Radiography showed several sclerotic deposits in the lumbar spine and pelvis. Biopsy of the supraclavicular mass revealed
209
210 BRITISH JOURNAL OF UROLOGY
fatty connective tissue widely infiltrated with anaplastic spheroidal cells compatible with a diagnosis of prostatic metastasis. After a blood transfusion of 6 units he was started on fosfestrol (Honvan) 1,000 mg intravenously, daily for 7 days followed by 250 mg orally, b.d. One month later he was well, with less urinary frequency. His serum acid phosphatase had fallen to 42.5 units. Three months later, however, he had developed diarrhoea and had stopped taking the Honvan. He was therefore started on stilboestrol 5 mg t.d.s. and apart from minor joint pains felt well. 18 months later, in May 1972, he was noted to have bilateral painless breast enlargement. The right breast contained a firm, round mass which was fixed to the skin with some inversion of the nipple. The left breast contained a smaller mass with no discrete borders (Fig. 1).
Biopsy of the right breast lesion showed this to be a poorly differentiated spheroidal cell carcinoma. In June 1972 he had a right simple mastectomy and an excision biopsy of the lesion in the left breast. Histological examination showed a tumour similar to that of the biopsy from the right breast and histochemical analysis gave a positive acid- phosphatase reaction, suggesting very strongly that these tumours were prostatic metastases. His oestrogen therapy was therefore continued and in August 1972 he had a bilateral subcapsular orchidectomy. During this admission to hospital he was given a 3-unit blood transfusion as haematological investigations revealed a haemoglobin of 9.8 g % with a blood film showing a leucoerythroblastic picture similar to previous examinations. He made an uneventful postoperative recovery and is well and active with no specific symptoms 4 months later (December 1972).
Comment
General Discussion. The development of a breast lesion in a patient with carcinoma of the prostate receiving oestrogen therapy is rare. There are only 18 such cases reported in the English literature: 16 reviewed by Lome and Austen (1970), and 1 each reported by O’Grady and McDivitt (1969) and Hartley and Little (1 97 1). Of these, the reported histological interpretation was metastatic in 9 cases, primary in 6 cases and in the remaining 3 cases no histological interpretation was offered. But, as already stated, the only reliable differentiating guide is obtained by selective staining for acid phosphatase and in only4of the previously recorded cases was this test performed. In each case where the acid phosphatase reaction was recorded it was reported as positive and the breast lesion therefore deemed metastatic. Campbell and Cummins (1951) were the first to report the acid phosphatase reaction of 1 such tumour and to indicate that an element of doubt must remain over the correct diagnosis in the reported cases, which now number 14, where histochemical analysis was not performed. The interpretation of the pathology in the first few recorded cases was strongly affected by the belief that oestrogen therapy could be an aetiological factor in the development of carcinoma in the male breast. Lacassagne had in 1932 induced breast tumours in male mice by the administration of oestrogens. However, there is now con- siderable evidence that this is not a significant factor in the aetiology of human male tumours. In a series of 198 cases of primary carcinoma of the male breast reviewed by Holleb, Freeman and Farrow (1968) no cases were associated with concomitant oestrogen therapy. They also quoted a review made in 1946 of more than 17,000 cases of prostatic carcinoma treated with oestrogens which yielded only 2 cases of breast cancer. Amongst their conclusions were “at present there does not appear to be any causal relationship between male breast cancer and oestrogen administration”. More recently this observation has been confirmed by Crichlow (1972) in a review of the world literature on carcinoma of the male breast. It is of interest that in those cases previously recorded which were deemed metastatic by histological methods, where survival after the development of breast metastases was recorded, the average survival was only 4 months.
Pathological Discussion. In 1935 Kutscher and Wolbergs identified a phosphatase in urine with optimum activity at pH 4-5 and showed that it was derived from prostatic tissue. Gomori (1941) devised a histochemical test for acid phosphatase using lead sulphide as an indicator, after fixation in ice-cold acetone and paraffin embedding. Maximum activity was present in normal and malignant prostatic tissue, but acid phosphatase could be detected in normal and neoplastic conditions of the gastrointestinal tract, though breast was negative as was pancreas and ovary. Gomori’s original method was somewhat capricious, but was made more reliable by the modification of Wolf, Kabat and Newman (1943). Abdul-Fad1 and King (1947, 1948), anxious to differentiate the prostatic acid phos- phatase in serum from that in erythrocytes, showed that the former was inhibited by tartrate, whereas the acid phosphatases of erythrocytes and most other tissues was inhibited by formalin, which had no effect on prostatic phosphatase. It was at this time that Dean and Woodward (1947) showed that it was possible to distinguish pros-
BILATERAL BREAST METASTASES FROM CARCINOMA OF THE PROSTATE 21 1
tatic carcinomatous tissues from neoplastic tissues in adjoining areas of rectum and bladder by estimating the acid phosphatase content of tumour extracts.
As has been mentioned, Campbell and Cummins (1951) were the first to use the histochemical acid phosphatase technique to determine whether or not mammary tumours developing during oestrogenic therapy for prostatic carcinoma were metastases from the prostate or hormonally induced primary mammary tumours. The neoplastic tissue of the breast and prostate from the postmorten examination of their case both gave a strong positive reaction for acid phosphatase. Gliick (1952) was unconvinced by Campbell and Cunimins’ histochemical findings and ob- tained positive acid phosphatase reactions in over 70% of a large number of biopsies of normal, hyperplastic and neoplastic breast tissue using their technique.
Histochemists were dissatisfied with the Gomori method and its modifications for acid phosphatase. Reiner, Rutenburg and Seligman (1957), in a review of acid phosphatase activity in human tumours, used an azocoupling method which they had developed in which biopsies were fixed in cold neutral 10% formalin for 24 hours and then frozen sections were cut on which the reaction was applied; they obtained a strong positive reaction in prostatic carcinoma and gastro-intestinal neoplasms and moderate reactions in neoplasms of the breast, thyroid and skin. They noted that fixation in acid formalin reduced the enzyme reaction but reported a case in which a lymph node, infiltrated with a poorly differentiated carcinoma, gave a strong positive reaction for acid phosphatase although the material had been fixed in non-buffered formalin for 2 days and surgical investigations confirmed that the primary growth was in the prostate.
Fanger and Barker (1959), in a detailed histochemical study of breast tissues, obtained positive acid phosphatase reactions in a range of pathological conditions using both the azo and lead methods on frozen sections after fixation in neutral formalin for 2 hours.
Zugibe (1970) was the first histochemist to recognise the problem of determining whether an undifferentiated carcinomatous metastasis was of prostatic origin or not, and applied the inhibition technique devised by Abdul- Fad1 and King ( I 948). Zugibe recommends that unfixed frozen sections should be stained by the azocoupling method, which would be controlled by adding formalin or tartrate to the substrate and control sections of prostate and non-prostatic tissue should be stained at the same time. The addition of tartrate will inhibit the reaction with prostatic acid phosphatase whereas the addition of formalin inhibits the acid phosphatase of tissue other than prostate.
Of the 4 cases already reported of breast metastases from prostatic carcinoma in which a histochemical test was applied, Campbell et al. (1951, 1962) merely state that the Wolf, Kabat and Newrnan method was used, so pre- sumably the material was fixed in acetone, though in their second case they estimated the acidoglycophosphate content of the breast. Boutouras, Woodhams and Brown (1965) explain that the prostatic origin of the breast neoplasm “was confirmed by physico-chemical acid phosphatase test” while Lome and Austen (1970) found that “the Gomori acid phosphatase stains gave positive results”.
Histochemical Investigations in this Case
In the case reported here, the material consisted of a formalin fixed paraffin block, and the remains of the surgical specimen which had been preserved in formal saline (pH 4.8) at room temperature for 4 weeks and so had not received the special care which the histochemist requires.
I-Iowever, haematoxylin eosin stained sections of the breast showed a diffuse infiltration with a spheroidal cell carcinoma and normal mammary ducts could be seen lying in the carcinomatous tissue (Fig. 2); i t would be difficult on morphological grounds to state categorically that the tumour was not a poorly differentiated primary carcinoma of the breast and stains for mucins gave no help.
Cryostat sections of the formalin-fixed material were stained for acid phosphatase using the azocoupling method of Rosales et al. (1966). The tumour tissue stained very strongly, as did control sections of prostatic liyperplasia which had been fixed i n formalin at pH 7.0 for 7 days. The addition of 10% 0-2M tartrate solution to the incubation medium markedly reduced the staining of the tumour tissue from the breast and the prostatic control.
However, 111 view of the reports by Gliick (1952) and Fanger and Barker (1959) that primary breast carcinomata gave strong acid phosphatase reaction using their technique, it seemed desirable to test this, using material which had received similar treatment to the breast specimen of the case reported here. Accordingly 4 specimens of primary breast carcinomata which had been fixed in formalin at pH 7.0, 1 for 24 hours, the others for 7 days, were treated in a similar manner and all failed to stain, although the prostatic controls stained strongly.
Six further breast specimens (4 carcinomata and 1 fibro-adenosis of the female breast and 1
212 BRITISH JOURNAL OF UROLOGY
primary carcinoma of the male breast) were obtained in the unfixed state. Cryostat sections were prepared and all gave a strong positive reaction for acid phosphatase; post-fixation in formalin (pH 7.0 for hour) reduced the staining slightly, the reduction was more marked after 1 hour and there was no staining after 3 hours, although post-formalin fixation had no effect on the control prostatic tissue. Addition of tartrate to the incubation medium inhibited the staining of the breast carcinomata and reduced the staining of the prostatic control.
Numerous other experiments were carried out, which will be reported elsewhere, but it is possible to conclude that if carcinomatous tissue which has been fixed in formal saline for more than 24 hours gives a positive acid phosphatase reaction with an azocoupling technique, it is
Fig. 2. Section of breast tumour of patient (Haematoxylin-eosin x65). There is a diffuse infiltration with a poorly differentiated spheroid cell carcinoma which is surrounding the normal breast ducts.
highly probable that it is of prostatic origin and this probability is increased if addition of tartrate to the incubation medium inhibits the reaction; naturally it is necessary to have control tissues treated in a similar way. On the other hand, if fresh unfixed tissue or tissue fixed in acetone should give a positive acid phosphate reaction it cannot be presumed to be of prostatic origin, unless the reaction is not inhibited when formalin is added to the substrate and is inhibited by the addition of tartrate (Fig. 3).
By adopting these procedures it should usually be possible to determine whether or not a breast tumour is of prostatic origin so that treatment may be adjusted accordingly.
Summary
A case of bilateral breast metastases developing in a patient with carcinoma of the prostate while on oestrogen therapy is described.
Differentiation between prostatic metastases and primary breast tumours under these circum- stances is important as the treatment for each is different.
BILATERAL BREAST METASTASES FROM CARCINOMA OF THE PROSTATE 213
1 ’2 3 4
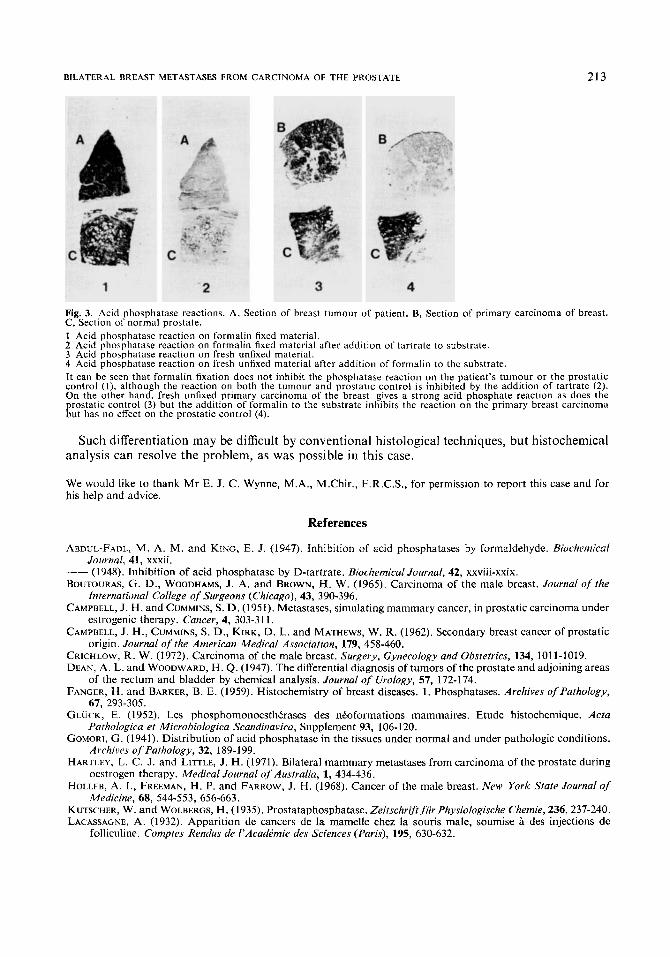
Fig. 3. Acid phosphatase reactions. A, Section of breast tumour of patient. B, Section of primary carcinoma of breast. C, Section of normal prostate. 1 Acid phosphatase reaction on formalin fixed material. 2 Acid phosphatase reaction on formalin fixed material after addition of tartrate to substrate. 3 Acid phosphatase reaction on fresh unfixed material. 4 Acid phosphatase reaction on fresh unfixed material after addition of formalin to the substrate. It can be seen that formalin fixation does not inhibit the phosphatase reaction on the patient’s tumour or the prostatic control (1). although the reaction on both the tumour and prostatic control is inhibited by the addition, of tartrate (2). On the other hand. fresh unfixed primary carcinoma of the breast gives a strong acid phosphate reaction as does the prostatic control (3) but the addition of formalin to the substrate inhibits the reaction on the primary breast carcinoma but has no effect on the prostatic control (4).
Such differentiation may be difficult by conventional histological techniques, but histochemical analysis can resolve the problem, as was possible in this case.
We would like to thank Mr E. J. C. Wynne, M.A., M.Chir., F.R.C.S., for permission to report this case and for his help and advice.
References
ABDUL-FADL, M. A. M. and KING, E. J. (1947). Inhibition of acid phosphatases by formaldehyde. Biochemical
__ (1948). Inhibition of acid phosphatase by D-tartrate. Biochemical Journal, 42, xxviii-xxix. BOUTOURAS, G. D., WOODHAMS, J. A. and BROWN, H. W. (1965). Carcinoma of the male breast. Journal of rhe
CAMPBELL, J. H. and CUMMINS, S. D. (1951). Metastases, simulating mammary cancer, in prostatic carcinoma under
CAMPBELL, J. H., CUMMINS, S. D., KIRK, D. L. and MATHEWS, W. R. (1962). Secondary breast cancer of prostatic
CRICHLOW, R . W. (1972). Carcinoma of the male breast. Surgery, Gynecology and Obstetrics, 134, 1011-1019. DEAN, A. L. and WOODWARD, H. Q. (1947). The differential diagnosis of tumors of the prostate and adjoining areas
FANGER, H. and BARKER, B. E. (1959). Histochemistry of breast diseases, 1. Phosphatases. Archives ofPathology,
CLUCK, E. (1952). Les phosphomonoesthtrases des ntoformations mammaires. Etude histochemique. Acta
GOMORI, G. (1941). Distribution of acid phosphatase in the tissues under normal and under pathologic conditions.
HARTLEY, L. C. J. and LITTLE, J . H. (1971). Bilateral mammary metastases from carcinoma of the prostate during
HOLLEB, A. I., FREEMAN, H. P. and FARROW, J. H. (1968). Cancer of the male breast. Mew York Sfate Journal of
KUTSCHER, W. and WOLBERGS, H . (1935). Prostataphosphatase. Zeitschrift fur Physiologische Chemie, 236,237-240. LACASSAGNE, A. (1932). Apparition de cancers de la mamelle chez la souris male, soumise a des injections de
Journal, 41, xxxii.
International College of Surgeons (Chicago), 43, 390-396.
estrogenic therapy. Cancer, 4, 303-31 1 .
origin. Journal of the American Medical Association, 179, 458-460.
of the rectum and bladder by chemical analysis. Journal of Urology, 57, 172-174.
67, 293-305.
Pathologica et Microbiologica Scandinavica, Supplement 93, 106-120.
Archives of Pathology, 32, 189-199.
oestrogen therapy. Medical Journal of Australia, 1, 434-436.
Medicine, 68, 544-553, 656-663.
folliculine. Comptes Rendus de I’AcadPmie des Sciences (Paris), 195, 630-632.
214 BRITISH JOURNAL OF UROLOGY
LOME, L. G. and AUSTEN, G. (1970). Metastatic breast carcinoma of prostatic origin. American Journal of Surgery, 120. 113-115.
O’GRADY, W. P. and MCDIVITT, R. W. (1969). Breast cancer in a man treated with diethylstilboestrol. Archives of Pathology, 88, 162-165.
REINER, L., RUTENBURG, A. M. and SELIGMAN, A. M. (1957). Acid-phosphatase activity in human neoplasms. Cancer, 10, 563-576.
ROSALES, C. L., BENNETT, J. M. and RUTENBURG, A. M. (1966). Histochemical demonstration of leucocyte acid phosphatase in health and in disease. British Journal of Haematology, 12, 172-176.
WOLF, A., KABAT, E. A. and NEWMAN, W. (1943). HistochemicaI studies in tissue enzymes 111. A study of the distribution of acid phosphatases with special reference to the nervous system. American Journal of Pathology, 19, 423-439.
ZUGIBE, F. T. (1970). Diagnostic Histochemistry, pp. 171-173. St. Louis, U.S.A.: C . V. Mosby Co.
The Authors
James Scott, FRCS, Registrar in General Surgery, Princess Margaret Hospital, Swindon (now Orthopaedic
A. H. T. Robb-Smith, MD, FRCP, Nuffield Reader in Pathology, University of Oxford. Ian Burns, BSc, Research Officer, Gibson Laboratories, Radcliffe Infirmary, Oxford.