26
Bile duct system / Papilla of vater Standards and innovations Brigitte Schumacher EVK Düsseldorf Germany
Bile duct system / Papilla of vater
Standards and innovations
Brigitte SchumacherEVK Düsseldorf
Germany
Bile duct system / Papilla of vater Standards and innovations
diagnostic – why ?
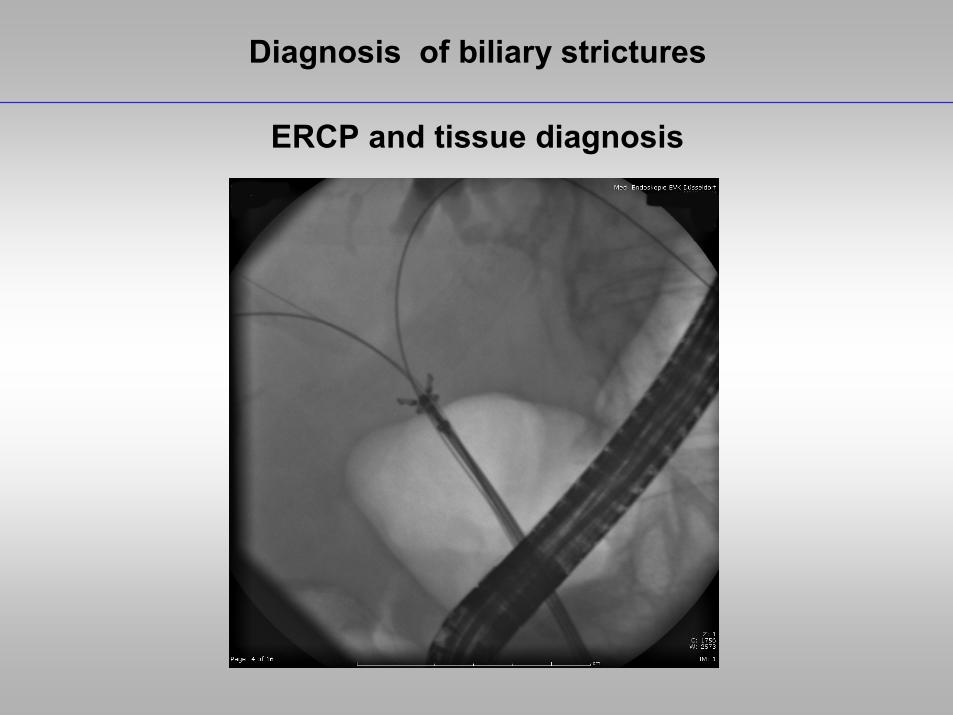
Diagnosis of biliary strictures
ERCP and tissue diagnosis
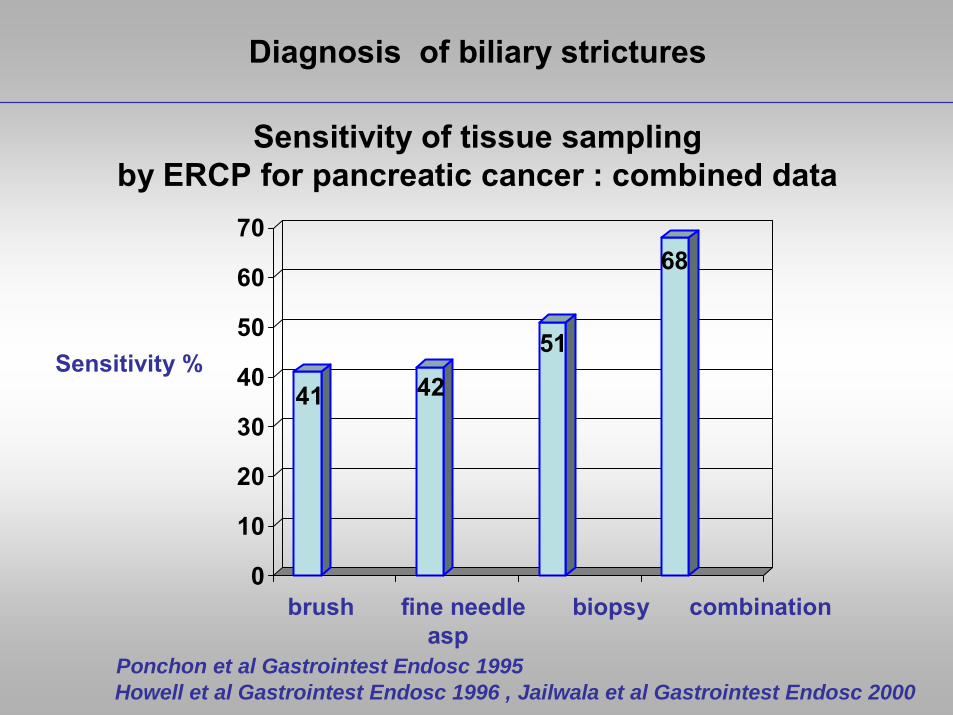
Diagnosis of biliary strictures
Sensitivity of tissue samplingby ERCP for pancreatic cancer : combined data
41 42
51
68
0
10
20
30
40
50
60
70
Sensitivity %
brush fine needle biopsy combinationasp
Ponchon et al Gastrointest Endosc 1995 Howell et al Gastrointest Endosc 1996 , Jailwala et al Gastrointest Endosc 2000
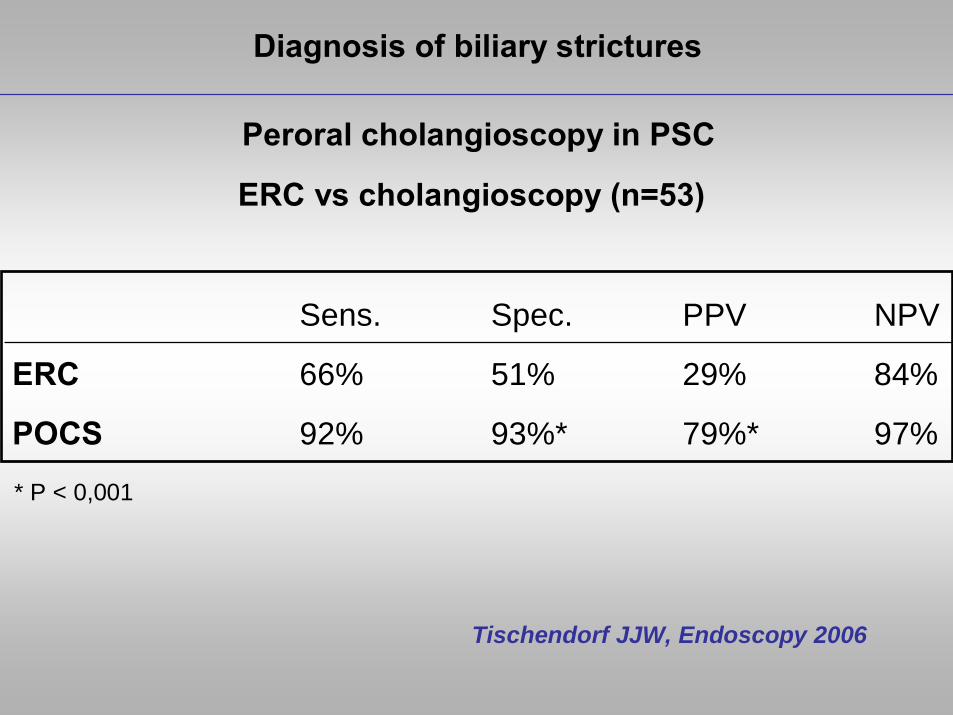
Peroral cholangioscopy in PSC
Sens. Spec. PPV NPV
ERC 66% 51% 29% 84%
POCS 92% 93%* 79%* 97%
Tischendorf JJW, Endoscopy 2006
ERC vs cholangioscopy (n=53)
* P < 0,001
Diagnosis of biliary strictures

SpyGlass Direct Visualisation System
SpyScope™ Access & Delivery Catheter
• 4 Lumens
• 10 FR
• 1.2 mm Accessory Channel
• Four Direction Steering Capability
• Independent Irrigation Channel
• Single Use
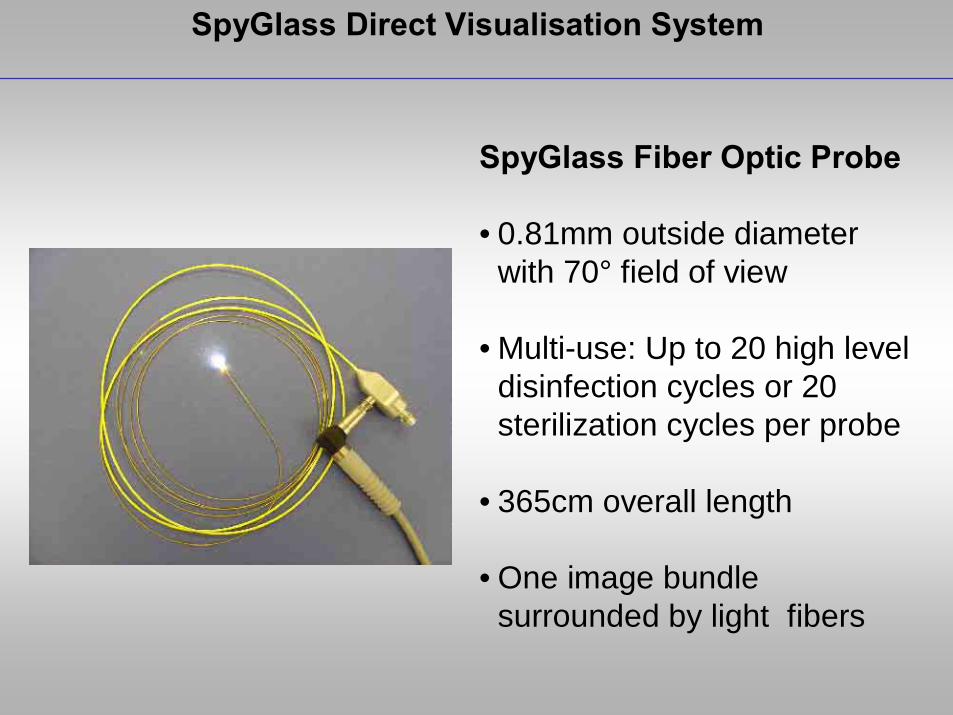
SpyGlass Direct Visualisation System
SpyGlass Fiber Optic Probe
• 0.81mm outside diameter with 70° field of view
• Multi-use: Up to 20 high level disinfection cycles or 20 sterilization cycles per probe
• 365cm overall length
• One image bundle surrounded by light fibers
Diagnosis of biliary strictures
unclear stenosis in PSC

Diagnosis of biliary strictures
Spy Glass dataBiopsy of indeterminate biliary strictures multicenter registry
N = 60Indication for Spy Glass
Indeterminate strictures in non PSC 62 %
Dominant PSC – strictures 14 %
Non – diagnostic prior tissue sampling 10 %
Indeterminate filling defects 7 %
Other 7 %
Adequate tissue amount in 87 % Sensitivity 78 % Specificity 100 %PPV 100 % NPV 60 %
Pleskow et al DDW 2008
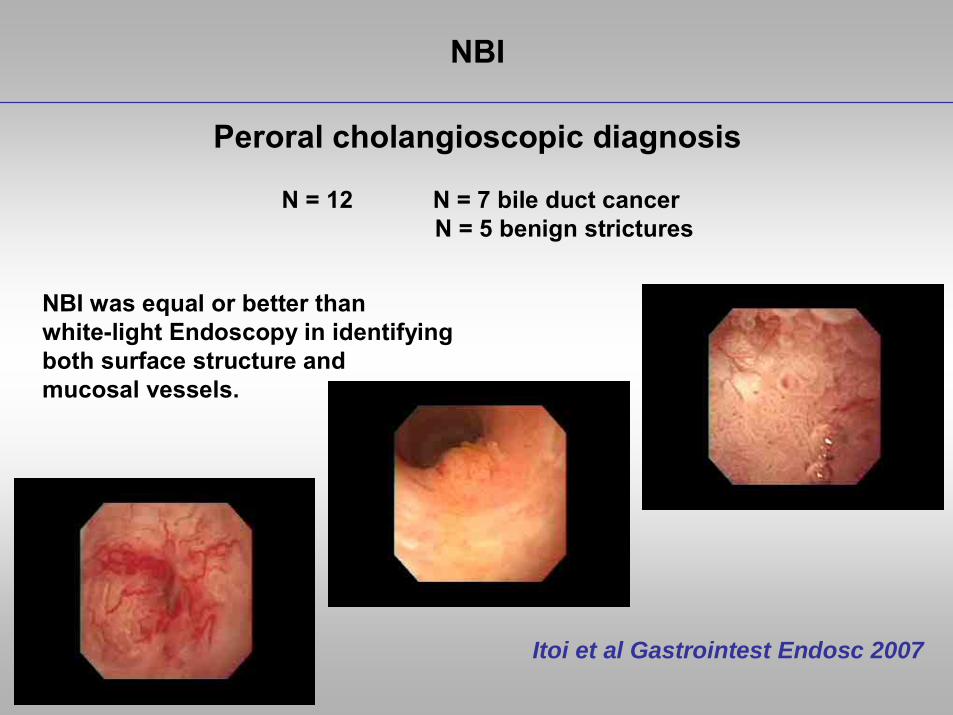
NBI
Peroral cholangioscopic diagnosis
Itoi et al Gastrointest Endosc 2007
N = 12 N = 7 bile duct cancerN = 5 benign strictures
NBI was equal or better than white-light Endoscopy in identifyingboth surface structure and mucosal vessels.
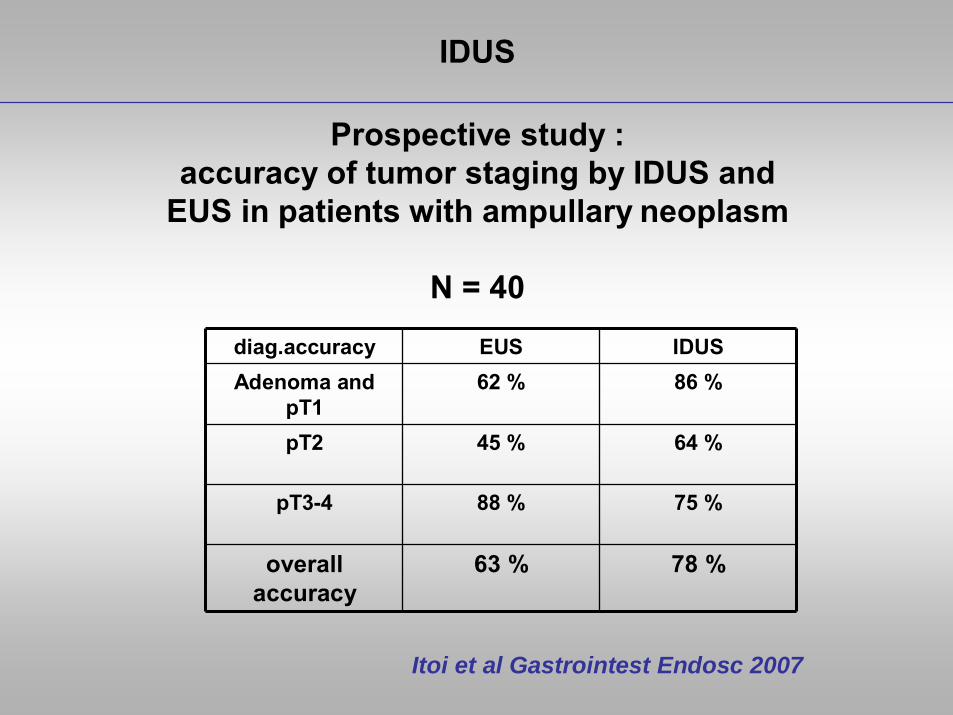
IDUS
Prospective study : accuracy of tumor staging by IDUS and
EUS in patients with ampullary neoplasm
N = 40
Itoi et al Gastrointest Endosc 2007
diag.accuracy EUS IDUSAdenoma and
pT162 % 86 %
pT2 45 % 64 %
pT3-4 88 % 75 %
overall accuracy
63 % 78 %

PSC
Complications after ERCP in patients with PSC
30 pat. with PSC comparing 45 pat. with no PSC
Complicationrate PSC non PSCin urgent 29.2 % 6.6 %
elective 7 % 0 %
overall 12.9 % 8,6 %
P<0.001
n.s.
n.s.
Etzel et al Gastrointest Endosc 2008
PSC
Standard treatment
Ponsioen et al Am J Gastroenterol 1999Stiehl et al J Hepatol 2002Bjornsson et al Am J Gastroenterol 2004
therapeutic ERC in pat. with dominant stricture,balloon dilation over a guidewire,
10 Fr stent across the stricture for 2-3 weeks
procedures should cover with prophylactic antibiotics
UDCA 20 – 25 mg/kg per day
Biliary sphincterotomy
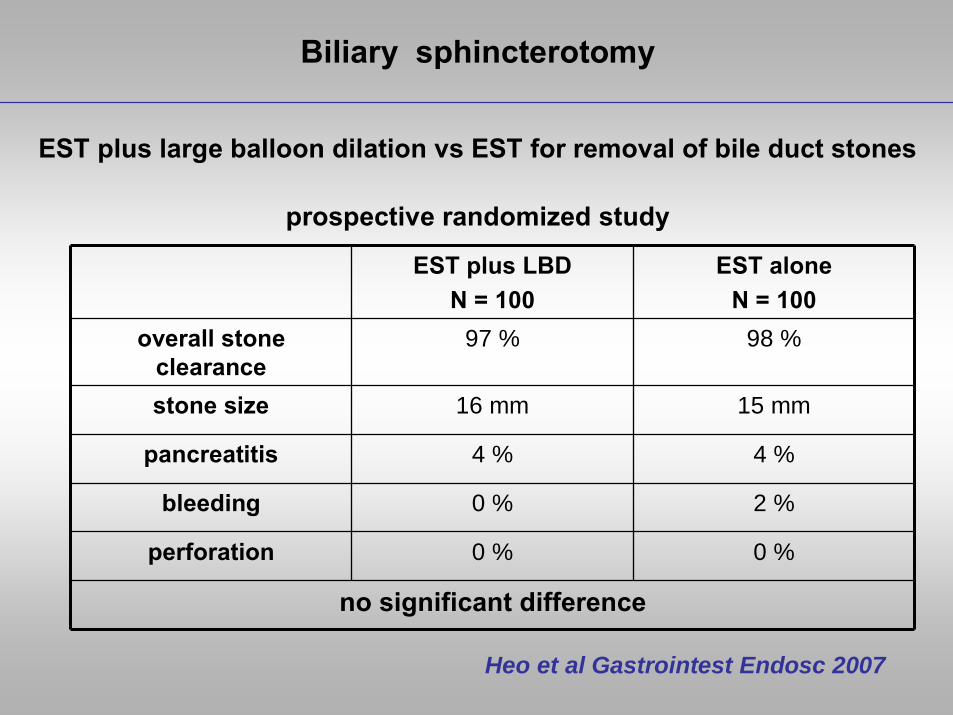
Biliary sphincterotomy
EST plus large balloon dilation vs EST for removal of bile duct stones
Heo et al Gastrointest Endosc 2007
prospective randomized study
EST plus LBDN = 100
EST aloneN = 100
overall stone clearance
97 % 98 %
stone size 16 mm 15 mm
pancreatitis 4 % 4 %
bleeding 0 % 2 %
perforation 0 % 0 %
no significant difference
Stents
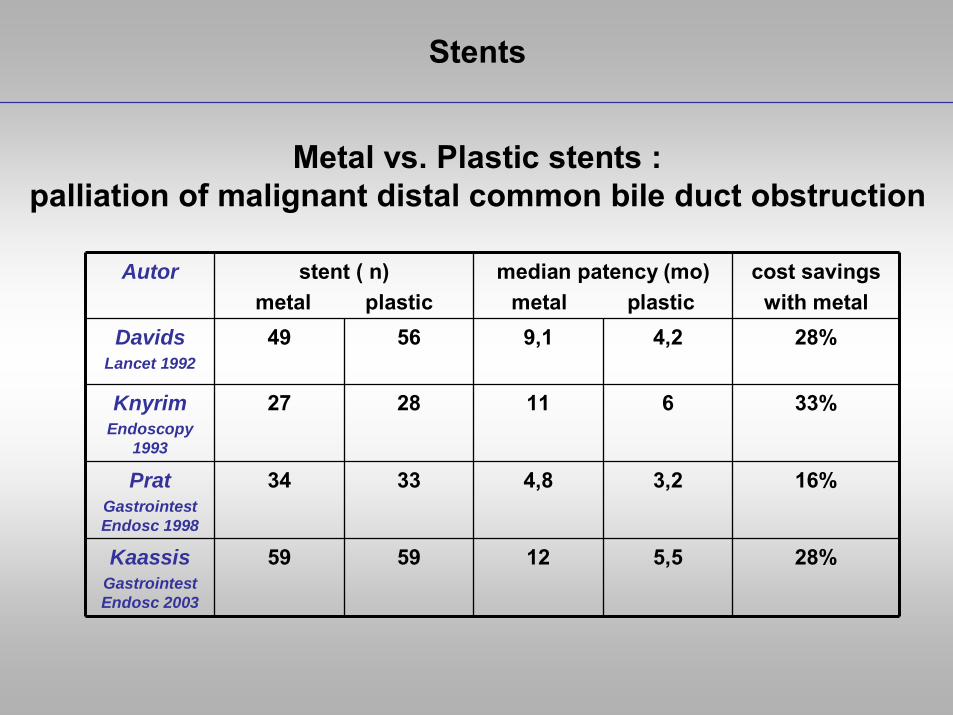
Metal vs. Plastic stents :palliation of malignant distal common bile duct obstruction
Autor stent ( n)metal plastic
median patency (mo)metal plastic
cost savingswith metal
DavidsLancet 1992
49 56 9,1 4,2 28%
KnyrimEndoscopy
1993
27 28 11 6 33%
PratGastrointest Endosc 1998
34 33 4,8 3,2 16%
KaassisGastrointest Endosc 2003
59 59 12 5,5 28%
Stents
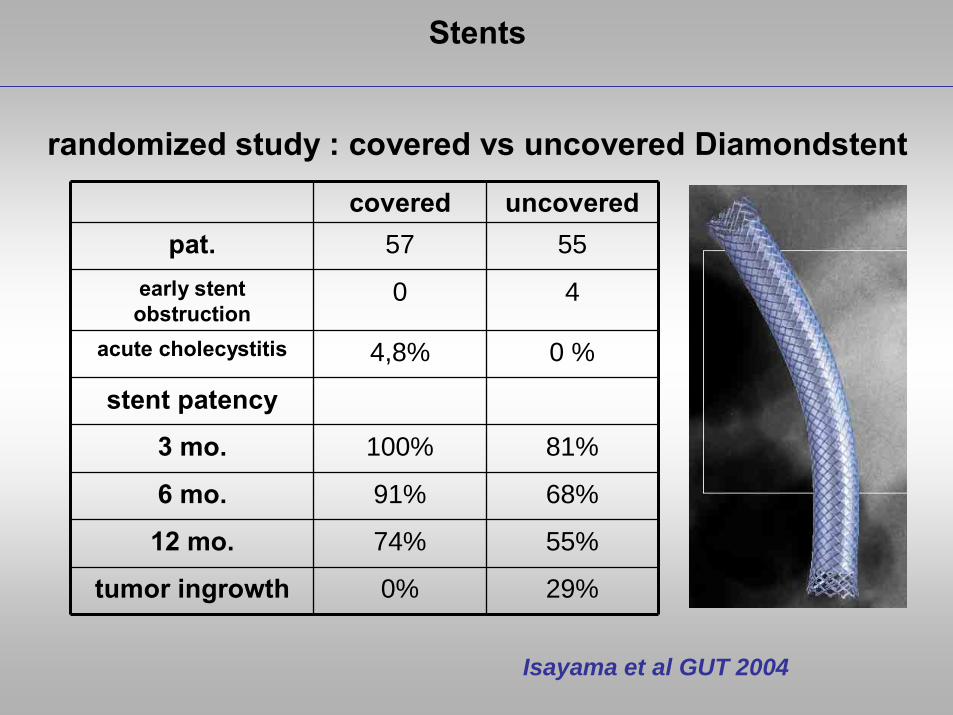
randomized study : covered vs uncovered Diamondstent
covered uncoveredpat. 57 55
early stent obstruction
0 4
acute cholecystitis 4,8% 0 %
stent patency
3 mo. 100% 81%
6 mo. 91% 68%
12 mo. 74% 55%
tumor ingrowth 0% 29%
Isayama et al GUT 2004
Stents
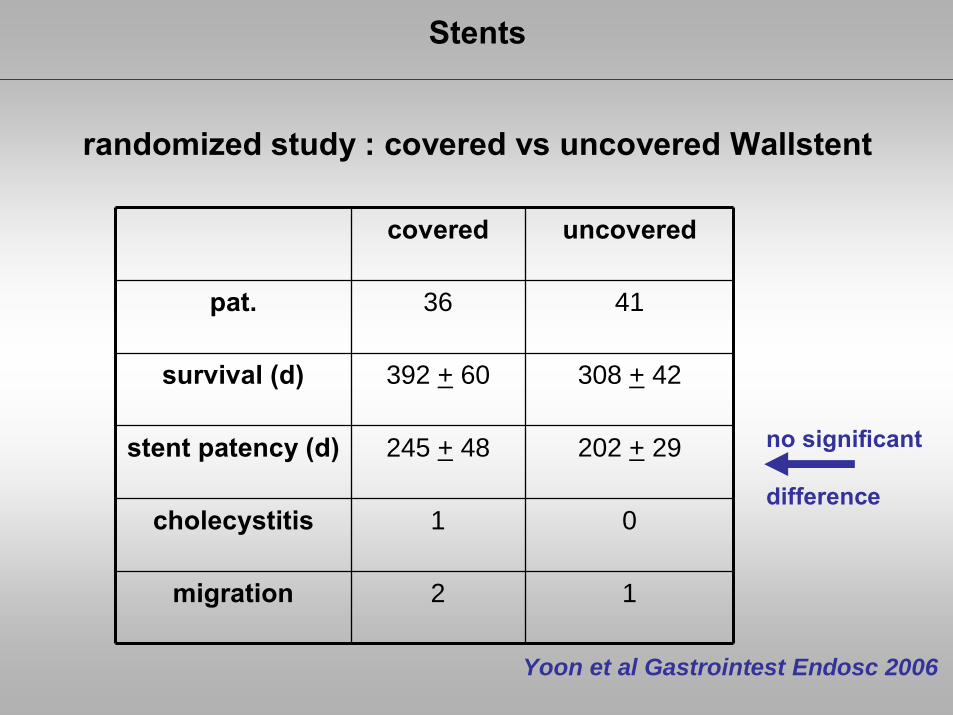
randomized study : covered vs uncovered Wallstent
Yoon et al Gastrointest Endosc 2006
covered uncovered
pat. 36 41
survival (d) 392 + 60 308 + 42
stent patency (d) 245 + 48 202 + 29
cholecystitis 1 0
migration 2 1
no significant
difference

Stents
covered metal vs plastic stents for malignant common bileduct stenosis : a prospective, randomized, controlled trail
metall plastic
patency rate 3,6 mo 1,8 mo
stent – failure 8 22
survival more than 10 mo. without stent failure 8 3
C. Soderlund et al Gastrointest Endosc 2006 ;63:986-95

Klatskin tumor
Determining resectability
potential resectability should be determined before considering ERCP
► MRCP ; CT
► suitability of patient ( age , comorbidity )
► consultion of a hepatobiliary surgeon

Klatskin tumor
Principles of drainage
to relieve jaundice , only a minority of liver (25 %) needs to bedrained problems arise from infection of undrained segments
plastic stents :
► poor outcomes► unilateral drainage causes infection
► bilateral stents are difficult to place and often migrate► high complication rates ( 27 % - 63 % )
uncovered metal stents are superior to plastic for hilar tumors

Diagnosis and management of biliary strictures
*
Rotatable papillotome „Haber ramp“ and second guidewire
Klatskin tumor
bilateral metal stenting

Klatskin tumor
*

Klatskin tumor
*
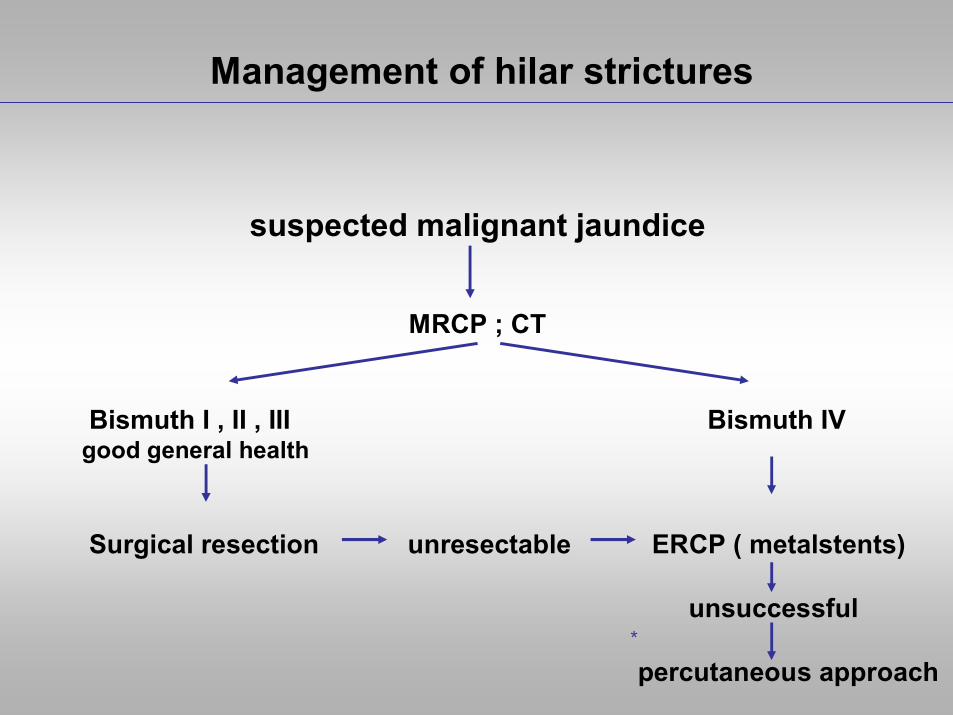
Management of hilar strictures
*
suspected malignant jaundice
MRCP ; CT
Bismuth I , II , III Bismuth IVgood general health
Surgical resection unresectable ERCP ( metalstents)
unsuccessful
percutaneous approach
![Vater v. County of Glenn [DISSENT]](https://static.documents.pub/doc/80x56/61bd190f61276e740b0f53d4/vater-v-county-of-glenn-dissent.jpg)
















