50
Biliary Emergencies Biliary Emergencies Murad Aljiffry Murad Aljiffry MD FRCSC MD FRCSC
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | eustacia-james |
| View: | 214 times |
| Download: | 0 times |
Biliary EmergenciesBiliary EmergenciesMurad Aljiffry Murad Aljiffry MD FRCSCMD FRCSC

Case 1Case 1
61 year old male61 year old male Abdominal pain for 5 days Associated with: Fever, malaise, chest pain with
shortness of breath and anorexia Past Hx.: diverticulitis treated Physical examination
HR 120, B/P 100/60 Localized RUQ peritoneal findings

Case 1Case 1
Lab: WBC: 18, Hb: 10, Creat 130, T.bili 60, ALP 350, Alb 25
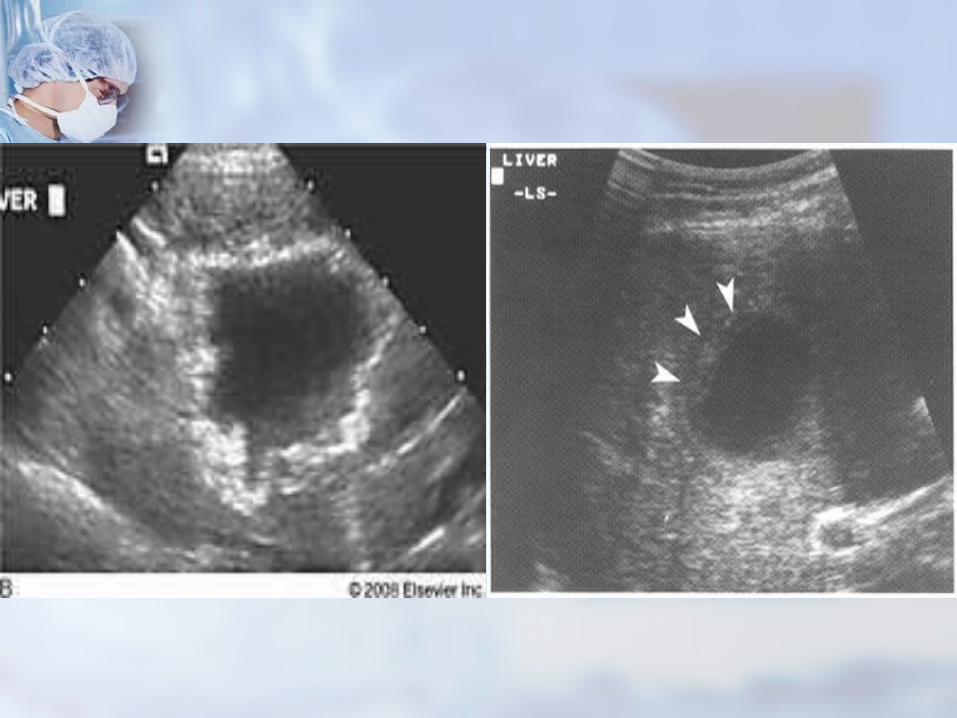
US: Hypoechoic liver lesion with
thickened irregular wall Gall stones
What next?

Case 1Case 1
Abdominal CT (contrast-enhanced) Hypodense lesion of left
lobe(5.5cm) occupies segment II and III
well demarcated, round

Liver AbscessLiver Abscess
Pyogenic(80%): E. coli, K.PPyogenic(80%): E. coli, K.P Paracytic(10%): Entamaeba Paracytic(10%): Entamaeba
histolyticahistolytica Others(10%): candidaOthers(10%): candida
EpidemiologyEpidemiology
Incidence in the US is 8-15 per Incidence in the US is 8-15 per 100,000100,000
Male to female ratio is 2:1 in Male to female ratio is 2:1 in recent studiesrecent studies
55thth-7-7thth decades of life decades of life Risk factors : DM, underlying Risk factors : DM, underlying
hepatobiliary or pancreatic hepatobiliary or pancreatic malignancy, and liver transplantmalignancy, and liver transplant

EtiologyEtiology
Biliary disease accounts for 20-Biliary disease accounts for 20-40% 40%
Extrahepatic obstruction leading Extrahepatic obstruction leading to ascending cholangitis and to ascending cholangitis and abscessabscess CBD stonesCBD stones Benign and malignant tumorsBenign and malignant tumors Biliary enteric anastamoses or Biliary enteric anastamoses or
manipulationmanipulation

EtiologyEtiology
Infection via portal systemInfection via portal system Infectious process originates in Infectious process originates in
abdomen, reaches liver by abdomen, reaches liver by embolization through portal embolization through portal systemsystem
Appendicitis, diverticulitis, IBD, Appendicitis, diverticulitis, IBD, proctitisproctitis

EtiologyEtiology
Hematogenous via hepatic arteryHematogenous via hepatic artery From systemic septicemia such From systemic septicemia such
as endocarditis and as endocarditis and pyelonephritis pyelonephritis
Direct extension or traumaDirect extension or trauma No cause (cryptogenic) in 20-No cause (cryptogenic) in 20-
40% of cases40% of cases

EtiologyEtiology
Underlying etiology of 1086 cases of liver abscess compiled Underlying etiology of 1086 cases of liver abscess compiled from the literature from the literature

MicrobiologyMicrobiology
Most contain more than one organismMost contain more than one organism Blood cultures positive in 33-65%Blood cultures positive in 33-65% E.Coli E.Coli Klebsiella (Klebsiella (is an important emerging is an important emerging
infection infection associated with associated with endophthalmitis )endophthalmitis )
BacteroidesBacteroides Streptococcal (including S. aureus and Streptococcal (including S. aureus and
S. pyogenes)S. pyogenes) Candida species : usually occurs in Candida species : usually occurs in
immunosuppressedimmunosuppressed patients patients
MicrobiologyMicrobiology
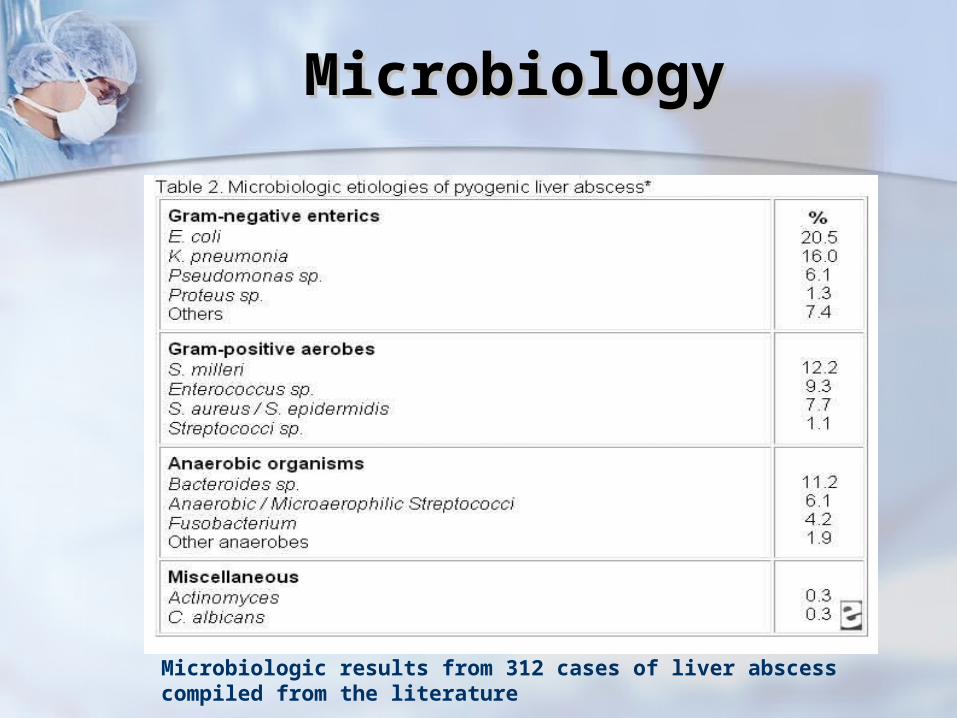
Microbiologic results from 312 cases of liver abscess compiled from the literature

ClinicalClinical
Fever (85-100%), abdominal pain Fever (85-100%), abdominal pain (50-75%)(50-75%)
About one-half of patients with About one-half of patients with liver abscess have liver abscess have hepatomegaly, RUQ tenderness, hepatomegaly, RUQ tenderness, or jaundice or jaundice
Right shoulder pain, pleuritic Right shoulder pain, pleuritic chest painchest pain
Anorexia, weight loss, mental Anorexia, weight loss, mental confusionconfusion

Diagnosis-LabDiagnosis-Lab
CBC: anemia in 50-80%, CBC: anemia in 50-80%, leukocytosis in 75-96%leukocytosis in 75-96%
LFTs: elevated alkaline LFTs: elevated alkaline phosphatase 95-100%, elevated phosphatase 95-100%, elevated AST, ALT 40-60%AST, ALT 40-60%
Elevated bilirubin in 20-50%Elevated bilirubin in 20-50% Decreased albumin in 71-87%Decreased albumin in 71-87%

Diagnosis-ImagingDiagnosis-Imaging
CT and ultrasound are the CT and ultrasound are the modalities of choice (80-100% modalities of choice (80-100% sensitive)sensitive)
An abscess appears An abscess appears radiologically as a fluid collection radiologically as a fluid collection with surrounding edema and with surrounding edema and inflammation (rim enhancement) inflammation (rim enhancement) that may contain loculated that may contain loculated subcollections and gassubcollections and gas


TreatmentTreatment
Initiation of antibiotic therapyInitiation of antibiotic therapy Diagnostic aspiration and Diagnostic aspiration and
drainage of abscessdrainage of abscess Surgical drainage in selected Surgical drainage in selected
patientspatients
Antibiotic TherapyAntibiotic Therapy
Empiric broad-spectrum antibiotics Empiric broad-spectrum antibiotics (draw blood culture before)(draw blood culture before)
A third generation cephalosporin A third generation cephalosporin such as ceftriaxone + metronidazolesuch as ceftriaxone + metronidazole
Fluoroquinolone (eg, ciprofloxacin) + Fluoroquinolone (eg, ciprofloxacin) + metronidazolemetronidazole
Monotherapy with a carbapenem or Monotherapy with a carbapenem or an extended spectrum penicillinan extended spectrum penicillin
Antibiotic TherapyAntibiotic Therapy
Immunocompromised patients Immunocompromised patients with multiple abscesses are best with multiple abscesses are best treated with high dose antibiotics treated with high dose antibiotics rather than open or rather than open or percutaneous drainagepercutaneous drainage

DrainageDrainage
For single abscesses with diameter ≤5 For single abscesses with diameter ≤5 cm : cm : percutaneous catheter drainage or needle percutaneous catheter drainage or needle
aspiration is acceptable (usually multiple)aspiration is acceptable (usually multiple) For single abscesses with diameter >5 For single abscesses with diameter >5
cm :cm : Percutaneous management (catheter Percutaneous management (catheter
drainage no needle aspiration)drainage no needle aspiration) Some favor surgical intervention over Some favor surgical intervention over
percutaneous drainage, treatment failure percutaneous drainage, treatment failure lower with surgical drainagelower with surgical drainage
Success 70-90%Success 70-90%


Complications of Complications of Percutaneous Percutaneous
DrainageDrainage Perforation of a viscousPerforation of a viscous PneumothoraxPneumothorax BleedingBleeding Leakage of pus into the abdomenLeakage of pus into the abdomen
Surgical TherapySurgical Therapy
Indications of surgical drainage:Indications of surgical drainage: Co-existing intra-abdominal disease Co-existing intra-abdominal disease
that requires operative managementthat requires operative management Failure of percutaneous drainageFailure of percutaneous drainage Multiple abscesses Multiple abscesses Loculated abscesses Loculated abscesses Abscesses with viscous contents Abscesses with viscous contents
obstructing the drainage catheterobstructing the drainage catheter Ascites or coagulopathyAscites or coagulopathy
Surgical TherapySurgical Therapy
Transthoracic, extraperitoneal, Transthoracic, extraperitoneal, transperitonealtransperitoneal
Transperitoneal is preferred as Transperitoneal is preferred as intra-abdominal pathology can intra-abdominal pathology can be dealt withbe dealt with
Laparoscopic or openLaparoscopic or open

Duration of therapy Duration of therapy
Follow imaging, WBC count and Follow imaging, WBC count and serum CRPserum CRP
Drainage catheters should Drainage catheters should remain in place until drainage is remain in place until drainage is minimal minimal
Patients should be treated for 2-4 Patients should be treated for 2-4 weeksweeks

ComplicationsComplications
Result from rupture of abscess Result from rupture of abscess into adjacent organs or cavitiesinto adjacent organs or cavities
Pleuropulmonary include Pleuropulmonary include effusions, empyema, bronch-effusions, empyema, bronch-hepatic fistulahepatic fistula
Intraabdominal include Intraabdominal include subphrenic abscess, rupture into subphrenic abscess, rupture into peritoneal cavity, or any peritoneal cavity, or any intraabdominal organintraabdominal organ

PrognosisPrognosis
Mortality rate : 10- 20%Mortality rate : 10- 20% If untreated fatal (100% mortality If untreated fatal (100% mortality
rate)rate) Mortality appears to be related to Mortality appears to be related to
underlying comorbidities rather than underlying comorbidities rather than to the abscess itselfto the abscess itself
Poor prognosis: age >70, multiple Poor prognosis: age >70, multiple abscesses, polymicrobial infection, abscesses, polymicrobial infection, immunosupression, malignancy, and immunosupression, malignancy, and delay diagnosisdelay diagnosis

Questions?Questions?

Case 2Case 2
40 y.o. female presents to ER 40 y.o. female presents to ER with 12 hr history of upper with 12 hr history of upper abdominal pain and feverabdominal pain and fever
Associated nausea and vomitingAssociated nausea and vomiting Lab: wbc 12, AST100, ALT220, Lab: wbc 12, AST100, ALT220,
GGT1400, ALP 1340, Tbili 75GGT1400, ALP 1340, Tbili 75

Case 2Case 2
Amylase and Lipase slight Amylase and Lipase slight elevationelevation
U/S – multiple small stones in U/S – multiple small stones in gallbladder, CBD9mm, no gallbladder, CBD9mm, no intrahepatic dilatationintrahepatic dilatation
What next?What next?

Case 2Case 2
H/O gastric bypassH/O gastric bypass 2:00 am2:00 am
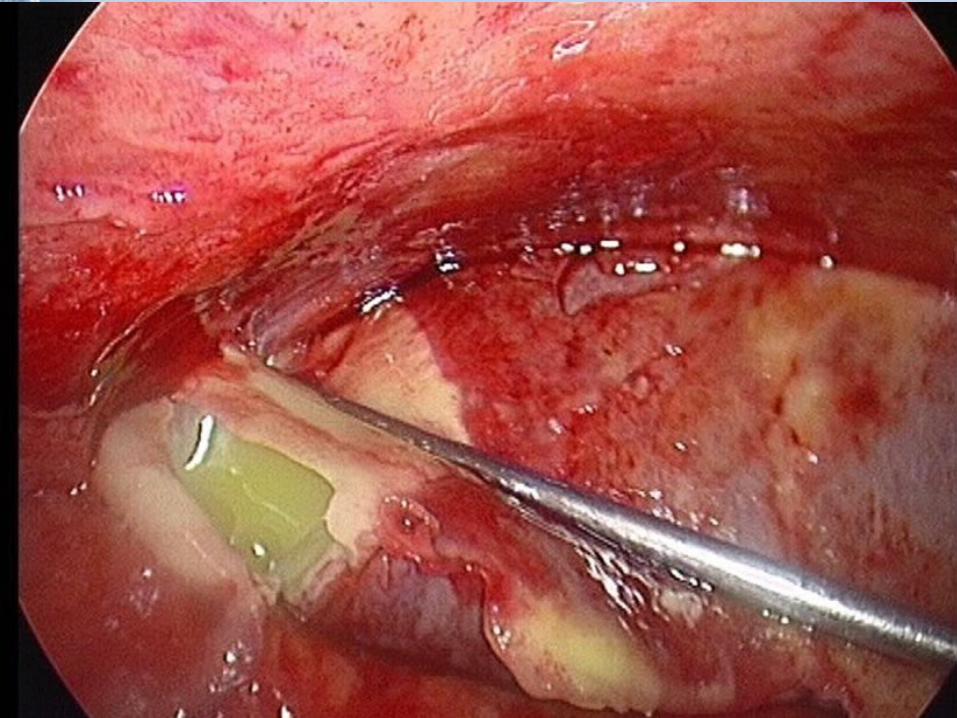
Acute CholangitisAcute Cholangitis
Pus under pressurePus under pressure May be difficult to distinguish May be difficult to distinguish
from acute cholecystitisfrom acute cholecystitis Managed medically with support, Managed medically with support,
antibioticsantibiotics Drainage is keyDrainage is key
EtiologyEtiology
Stone diseaseStone disease Anomalous PBJAnomalous PBJ Malignant biliary obstructionMalignant biliary obstruction Primary sclerosing cholangitisPrimary sclerosing cholangitis Post instrumentationPost instrumentation
CholangiographyCholangiography SurgerySurgery SphincterotomySphincterotomy StentsStents
MicrobiologyMicrobiology
80% patients +ve biliary cultures 80% patients +ve biliary cultures (multiple organisms frequent )(multiple organisms frequent ) E.Coli (commonest)E.Coli (commonest) Enterococci Enterococci Klebsiella spKlebsiella sp Proteus spProteus sp Pseudomonas spPseudomonas sp Bacteroides spBacteroides sp

Clinical PresentationClinical Presentation
Charcot’s triadCharcot’s triad Pyrexia, Pain, JaundicePyrexia, Pain, Jaundice
Elevated liver enzymesElevated liver enzymes LeukocystosisLeukocystosis

DiagnosisDiagnosis
Clinical Clinical UltrasoundUltrasound
Duct dilationDuct dilation Presence of gallbladder or CBD stonesPresence of gallbladder or CBD stones
CTCT Duct dilationDuct dilation R/O other causesR/O other causes
MRCP (especially for hilar obstruction, MRCP (especially for hilar obstruction, if stable pt.)if stable pt.)
ERCP (generally for therapy)ERCP (generally for therapy)

ManagementManagement
Fluid resuscitation Triage (floor or ICU) Correction of coagulopathy and
electrolytes Blood cultures Antibiotics (broad spectrum)

ManagementManagement
Most pt will respond and will require urgent biliary decompression
10-15% of patients fail to respond or deteriorate within 12-24 hours, thus require emergent biliary decompression

Biliary DrainageBiliary Drainage
EndoscopicEndoscopic SurgicalSurgical PercutaneousPercutaneous
Endoscopic Biliary Endoscopic Biliary DrainageDrainage
Can be done at bedside in ICU with Can be done at bedside in ICU with portable flouroscopyportable flouroscopy
Superior to surgical drainageSuperior to surgical drainage Mortality of endoscopic vs surgical Mortality of endoscopic vs surgical
drainage 10% vs 32% RCT (Lai NEJM drainage 10% vs 32% RCT (Lai NEJM 1992)1992)
Preferable to percutaneous drainagePreferable to percutaneous drainage Morbidity less (Sugiyama Arch Surg 1997, Morbidity less (Sugiyama Arch Surg 1997,
AmJGastro 1998)AmJGastro 1998) Especially in presence of ascites, Especially in presence of ascites,
coagulopathycoagulopathy

Endoscopic Biliary Endoscopic Biliary DrainageDrainage
SphincterotomySphincterotomy Caution due to bleeding riskCaution due to bleeding risk
Stone removalStone removal StentStent


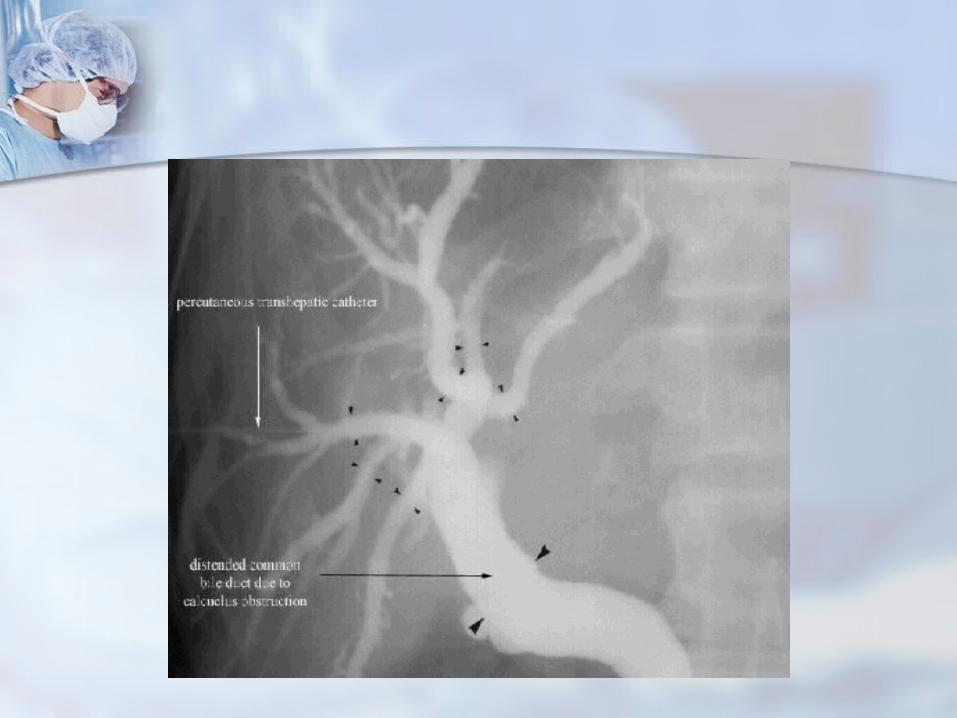
Percutaneous Biliary Percutaneous Biliary draindrain
When endoscopic drainage failsWhen endoscopic drainage fails Inaccessible papillaInaccessible papilla Roux-en-YRoux-en-Y HepatolithiasisHepatolithiasis Segmental cholangitis (complex Segmental cholangitis (complex
hilar tumor)hilar tumor)
Surgical Biliary drainSurgical Biliary drain
Last resort Last resort Decompression of biliary tree Decompression of biliary tree
and placement of T tubeand placement of T tube

Questions?Questions?

















