Session : Monday September 21, 2015 at 11:45-12:30 Biomarkers to Diagnostics The Essential Tool Box for Drug Development The Essential Tool Box for Drug Development Johan Luthman Johan Luthman, VP Neuroscience Clinical Development Eisai Neuroscience & General Medicine Product Creation Unit, Wood Cliff Lake NJ USA Evolution Summit; Wood Cliff Lake, NJ, USA September 20-22, 2015, Red Rock Resort & Spa, Las Vegas, NV
Transcript
Session:Monday September 21, 2015 at 11:45-12:30
Biomarkers to DiagnosticsThe Essential Tool Box for Drug DevelopmentThe Essential Tool Box for Drug Development
Johan LuthmanJohan Luthman, VP Neuroscience Clinical Development
Eisai Neuroscience & General Medicine Product Creation Unit, Wood Cliff Lake NJ USA
Evolution Summit;
Wood Cliff Lake, NJ, USA
;September 20-22, 2015, Red Rock Resort & Spa, Las Vegas, NV
Critical Tools - Animal Models & Biomarkers
Overall Program RiskBeyond target validationy g
EL
strong
MEDIUM LOW
MO
DE MEDIUM LOW
Validated modelNo biomarker
Validated modelValidated biomarker
NIM
AL
MEDIUMHIGHN d l
AN
none
e g
No modelNo biomarker
No modelValidated biomarker
BIOMARKERnone
stro
n
Steps from Biomarker to Diagnostic/Outcome Measure
Regulatory Process
Clinical QualificationDiagnostic
g yApproved DiagnosticAccepted Outcome measure
Diagnostic Outcome measure (surrogate)
Assay ValidationPrototype assay to Assay “lock down” A f t i ( kit)
Exploratory BiomarkerExploration of candidate biomarker
Fit for Purpose AssayCustom developed assay
Biomarker IdentificationHypothesis driven or Un-biasedModality? / Invasive or Non-invasive?
p
Biomarkers in Early Development
Drug Presence & Target Engagement (TE)Drug reaches target organ & interacts with target
1g g g g
• Proof of Distribution / Presence - Reaching target organ• Proof of Target Occupancy - Binding to molecular target (TE)
Proof of Mechanism (PoM)Proof of Mechanism (PoM)Target mechanism = Pharmacodynamic (PD) readout• Proof of Biological Activity (PoBA)• Mechanism of Action (MoA)
2
• Mechanism of Action (MoA)
Proof of Principle (PoP)Mechanism influences pathophysiology
I ti t b t l h lth l t if h i l i t th h i l
3• In patients, but also healthy volunteers if physiology approximates pathophysiology • Also called “PoC Lite”
Proof of Concept (PoC)4 p ( )Mechanism can be used to treat disease• Traditionally Phase IIB study, however strive is to obtain PoC as early as possible in
• Valid PoC requires adequate receptor occupancyC ffi i t b hi t ll t l t d d ?– Can sufficient occupancy be achieve at well tolerated doses ?
– Is it worthwhile testing efficacy?
No occupancy - no efficacy – not surprising New molecule needed
Full occupancy – no efficacy- concept flawed Do something else
• PET helps dose selection for efficacy trialsOpen therapeutic window and limit manufacturing costs– Open therapeutic window and limit manufacturing costs
Borsook, Becerra and Hargreaves (2006) Nature Reviews Drug Discovery 5: 411-425h
Target Engagement – PET OccupancyTranslational biomarker (animal-Ph0-Ph1)
PET set doses for H3 Inverse Agonist PoC Study•PET imaging of H3 receptorB s lin
7.5 mg 50 mg PET imaging of H3 receptor occupancy in humans
•H3 PET tracer allowed dose selection of MK-0249 in PoC study
Baseline 6h post-dose 6h post-dose
•Acceleration of Phase I to IIB94%80%AN04
POC f E i D ti Sl iPOC for Excessive Daytime Sleepiness:
Program termination:Program termination: MK-0249 in POC study had excellent dose –occupancy range, but p y g ,kept humans awake in sleep period
Car driving – On the road or SimulatorEfficacy read-out in e.g. Excessive Daytime Sleepiness patientsEfficacy read out in e.g. Excessive Daytime Sleepiness patients
Safety data on CNS active drugs
Differentiation from Standard of Care (sedative/hypnotics)
Standard Deviation of Lane Position (SDLP) Assesses “weaving”
Differentiation from Standard of Care (sedative/hypnotics)
Verster, 2006
National Advanced Driving Simulator (NADS, U of Iowa) MiniSim
Notch Signature in Hair Follicles Reveals Side Effect Liability with γ-Secretase Inhibitors
• Prognostic (Predictive) – Treatment effect– Outcome measure in trialsOutcome measure in trials– Ultimate goal surrogate outcome measure
Surrogacy qualification time-consuming & costly
• Predictive – Drug safety assessmentPredictive Drug safety assessment
• Stratification– Segmentation into predetermined categoriesg p g
• Enrichment– Inclusion criteria in trials– Companion Diagnostics 14
Role of Diagnostic Biomarkers
• Clinical phenotype – Different diagnostic criteria• Histopathology gold-standard in biomarker qualificationHistopathology gold standard in biomarker qualification
Bridging clinical & histopathology phenotypes (Alzheimer’s disease as example)
“Context of Use” AcceptancePurpose of the measurement (“Clinical Qualification”)Purpose of the measurement ( Clinical Qualification )
– Stand Alone or Companion Diagnostic– Outcome Measure - Surrogate Outcome Measure
“Assay” ApprovalTest performing the measurement (“Assay Validation”)
– Medical Device• In Vivo Ex Vivo or In Vitro application• In Vivo, Ex Vivo or In Vitro application• Do not work via chemical action in the body
– IND / IMP• In Vivo application• Work via chemical action in the body, e.g. PET ligand
Context of Use Qualification of Drug Development Tools (DDT)
FDA - Drug Development Tools Qualification Programs– Allows use in the qualified Context of Use during drug developmentAllows use in the qualified Context of Use during drug development
• Office of Translational Sciences evaluation• No need CDER reconfirming DDT suitability for the qualified context of use
EMA - Qualification of Novel Methodologies for Drug Development
– Voluntary pathway to CHMP opinion (public) or a Scientific Advice– Voluntary pathway to CHMP opinion (public) or a Scientific Advice (confidential) on novel methodologies or methods & drug development tools
• Qualification of biomarkers for a specific intended useQualification of biomarkers for a specific intended use
Biomarkers qualification requires a reliable measurement method of the biomarker, but is conceptually independent of the specificof the biomarker, but is conceptually independent of the specific test performing the measurement• Qualification does not mean approval of a specific test device
Biomarker Context of Use Qualification
Critical Path Institute (Tucson, Arizona) Bridging the Gap between Science & Regulatory acceptance
RegulatoryE l t
Bridging the Gap between Science & Regulatory acceptance
Regulatory Application of
Biomarkers
Exploratory Biomarkers Bmx Qual
• Independent, non-profit organization “Executive” spin-out based on the Critical Path Initiative (FDA)
• Bringing FDA, industry & academia together to improve path forBringing FDA, industry & academia together to improve path for innovative new drugs & diagnostics
• Several projects for DDT qualification with FDA & EMA
Assay Approval “Fluid” Biomarker Assay Maturity FDA (EMA) Terminology
Research Use Only (RUO)– Not for diagnostic use
E l t d i & f– Evaluate design & performance– Developing knowledge related to human disease
Investigational Use Only (IUO)Investigational Use Only (IUO)– Undergoing performance evaluation– Used for diagnosis or treatment decisions or used as part of a drug trial to
determine which arm of the trial subjects will be placed inj p– Meet criteria for Investigational Device Exemption (IDE)
• Pre-IDE consultations and IDE submission is a useful pathway when evaluating the clinical utility of a diagnostic product
In Vitro Diagnostic (IVD) Medical Device (kit)– For diagnosis - to cure, mitigate, treat, or prevent disease – FDA - CDRH (Center for Devices & Radiologic Health)– FDA - CDRH (Center for Devices & Radiologic Health)
• Pre-market and post-market controls• Commercialized to CLIA certified labs
– EMA: IVD Devices have to meet the requirements for Self-Declaration
FDA IVD Classification
Likely Class II• Information not used for diagnosis
Likely Class III•Screens for a serious disease or
diti• Predicate device is available
• Likelihood of misuse is small or i ld t t i
condition
•Test information is diagnostic -patient has a disease or not
misuse would not create a serious situation
• 510(k)s - a predicate device
•Likelihood or harm of misuse is significant / serious
clearance
• de novo 510(k)s - no predicate device clearance
•Information tells physician which drug to use, not use, or how much to use
•Pre-Market Approval (PMA)
•Performance of device against a gold standard or other establishedgold standard or other established end point
USA – Oversight Diagnostics
• Laboratory Developed Test (LDT, “homebrews”)D l d & d ithi l b– Developed & used within one lab
• Not available to other labs• Clinical Laboratory Improvement Amendments (CLIA) standard• FDA has a “risk-based” oversight of LDTs
• “Complementary” Diagnostics– FDA developing frame work for new regulatory category
• Provide additional information on drug use• Provide additional information on drug use– Distinct from “companion diagnostics,” (essential for drug use)– Example - gene “signature” pattern linked to a certain disease.
• No test yet labeled as complementary diagnostics
Europe: CE Mark
• Requirements of the In Vitro Diagnostic Directive 98/79/EC– Manufacturer's declaration that the product conforms
with “Essential Requirements”with Essential RequirementsSelf-declarationVerified by “Notified Body” (accredited to validate compliance)Permits products’ access to the market
CE Marking is not approval by a Health AuthorityCE M ki i t lid ti f li i l tilit• CE Marking is not validation of clinical utility
• CE Marking is not intended for consumer assurance
Stand- Alone Diagnostic
“Independent” diagnostic –Not associated with specific drug treatmentot assoc ated t spec c d ug t eat e t–“Gold standard" against which to judge performanceperformance
Other established diagnosticPost mortem histopathologyPost mortem histopathology
Companion Diagnostic Pathway
Drug
Pharmaceutical DrugClinical phases RegulatoryDrug
Discovery
Biochemical Biomarker
PreclinicalPhase I Phase II Phase III
Regulatory filing Launch
PMA/CE
BiomarkerDiscovery
Feasibility Verification
RUO assay Prototype
Regulatory review Commer-
cializationIVC
IUO assay
ClinicalQualification
Identifies condition for use of a therapeutic productEnsures the safe & effective use of a therapeutic productEnsures the safe & effective use of a therapeutic product
Context of Use established by drug treatment effectNo "gold standard" requirement to judge performance
• Collaboration between Center for Drug Evaluation and Research (CDER) and CDRH (Center for Devices & Radiologic Health)
•Commonly a Class III device (Requiring Pre-Market Approval)
Companion Diagnostic - EMA
• CoDx viewed as low risk - CE markingCoDx viewed as low risk CE marking• Drug approvals not held up for kit to be CE marked
• Not yet requiring intended uses of diagnostic products toNot yet requiring intended uses of diagnostic products to change when companion diagnostic associated
• Emerging new EMA regulation: • CoDx will be viewed as class C (high risk)( g )
• Increased Notified Body & Competent authority involvement
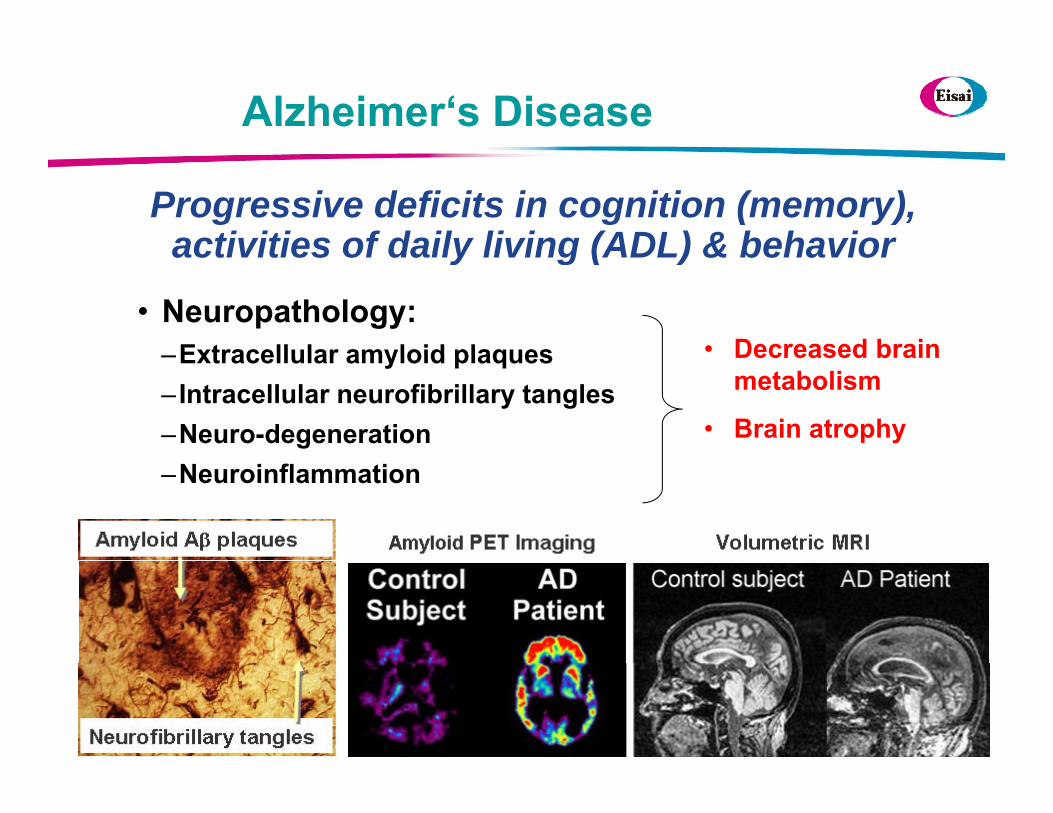
Alzheimer‘s Disease
Progressive deficits in cognition (memory), activities of daily living (ADL) & behavior
Biomarkers Used to Select Prodromal Subjects or to Demonstrate Disease Modification
• Prodromal AD patient “diagnosis” in MCI1 B i l id PET i i1. Brain amyloid PET imaging2. Cerebrospinal fluid (CSF) tau protein / Aβ peptide3 volumetric MRI – hippocampal volume3. volumetric MRI – hippocampal volume
• Outcome measuresBiomarkers as secondary & exploratory endpoints to support Disease Modification claimsDisease Modification claims
1. Hippocampal atrophy - volumetric MRI2. Cerebrospinal fluid total-tau or P-tau 3. Brain amyloid PET imaging (treatment effect)
Amyloid PET For Prodromal AD Diagnosis & Trial Enrichment