Antonia M. Calafat, Ph.D. Division of Laboratory Sciences National Center for Environmental Health Centers for Disease Control and Prevention Atlanta, GA Biomonitoring for Exposure Assessment: Role, Challenges, and Needs
Transcript
Antonia M. Calafat, Ph.D.
Division of Laboratory SciencesNational Center for Environmental Health
Centers for Disease Control and PreventionAtlanta, GA
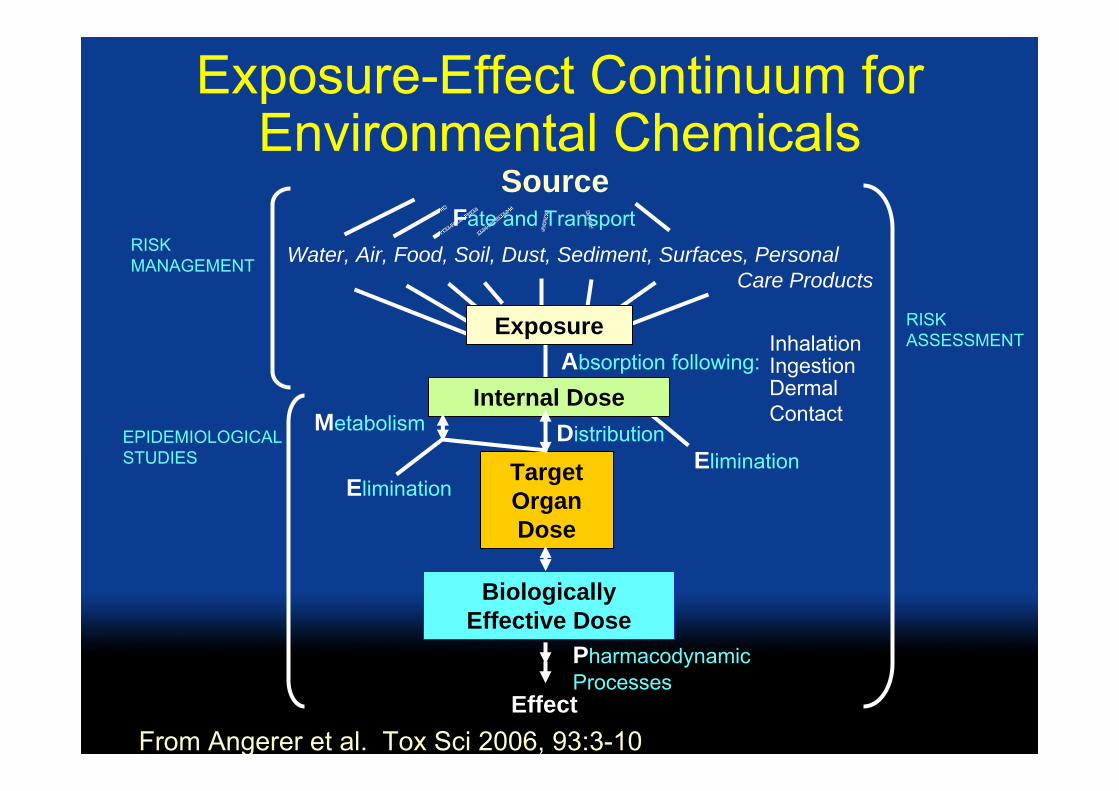
Exposure-Effect Continuum for Environmental Chemicals
From Angerer et al. Tox Sci 2006, 93:3-10
Exposure
Fate and Transport
Biomonitoring
Assessment of internal dose by measuring the parent chemical (or its metabolite or reaction product) in human blood, urine, milk, saliva, adipose, or other tissue
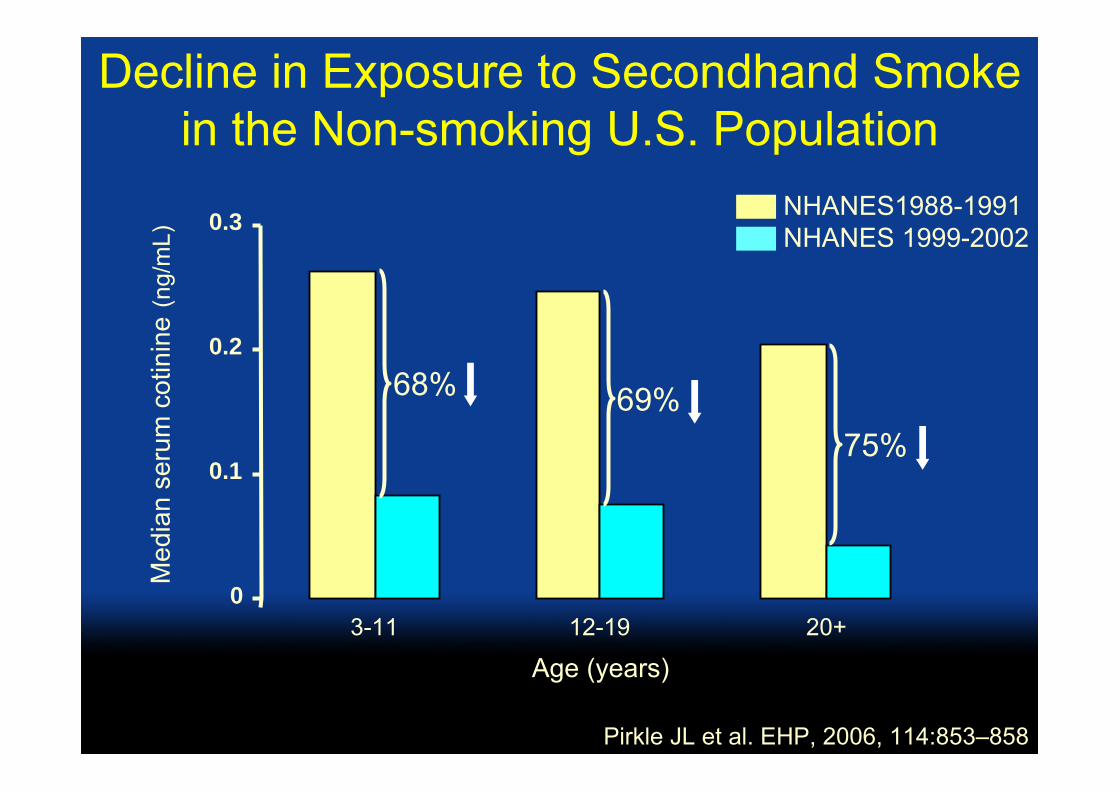
CDC’s Biomonitoring Programs for Exposure Assessment
• National Health and Nutrition Examination Survey (NHANES)
• Epidemiological studies of specific populations
What is NHANES?
• Annual survey (since 1999) conducted by the National Center for Health Statistics, CDC
• Stratified, multistage probability sample of the civilian, noninstitutionalized U.S. population• ~5,000 persons/year• 15 counties/year (mobile examination centers)
• Includes detailed medical history, dental & physical examinations, laboratory tests
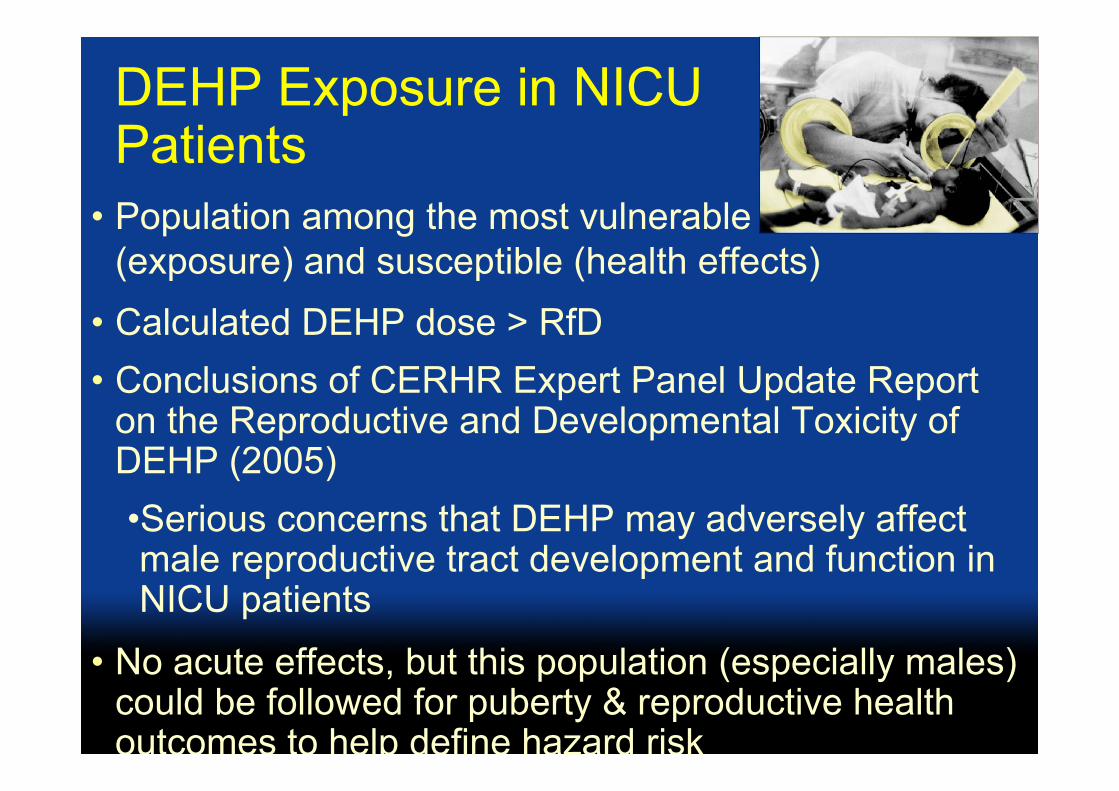
on the Reproductive and Developmental Toxicity of DEHP (2005)•Serious concerns that DEHP may adversely affect male reproductive tract development and function in NICU patients
• No acute effects, but this population (especially males) could be followed for puberty & reproductive health outcomes to help define hazard risk
Other Potential Roles of Biomonitoring in Risk Assessment• Hazard identification
• Vulnerable/susceptible populations• Specific situations• Internal dose in animal studies
• Going from concentration to exposure• Improve understanding of toxicokinetics• Improve epi data
• Collection of additional data (e.g., urinary output)• Ranges vs point estimates
• Communication of results – public perception
THANK YOU!
“The findings and conclusions in this presentation have not been formally disseminated by the Centers for Disease Control and Prevention and should not be construed to represent any agency determination or policy”
This paper was produced for a meeting organized by Health & Consumer Protection DG and represents the views of its author on thesubject. These views have not been adopted or in any way approved by the Commission and should not be relied upon as a statement of the Commission's or Health & Consumer Protection DG's views. The European Commission does not guarantee the accuracy of the dataincluded in this paper, nor does it accept responsibility for any use made thereof.