Blue Distinction ® Centers for Bariatric Surgery 2020 Provider Survey Bl ueD isti nction® Specialty Care & ' BlueCross T. .. BlueShield Association Printed version of this document is for reference purposes only. A completed Provider Survey will need to be submitted via the online web application BD Portal SM . Paper copies of the Provider Survey will not be accepted. Review instructions below to complete the Provider Surveyvia the online web application BD Portal. BD Portal SM Instructions: • In the Survey Actions screen, under Survey, click on “Check Out ” and then “Take Survey” to open the Provider Survey. • To save your responses, click “Save.” • If you need to edit the Provider Survey at a later time, click on “Save and Exit.” This will save your responses and exit the Provider Survey. • You must also “Release” the Provider Survey on the Survey Actions screen, as applicable, if other contacts need to access the Provider Survey. • Once the Provider Survey is complete and ready to be submitted, click on “ Submit.” Close the survey window to bring you back to the Survey Actions screen. • Each applicant facility must submit a complete electronic version of the Provider Survey in BD Portal for a complete submission. • Please be sure that the status of your electronic application displays “ Submitted,” which will confirm that the applicant facility has successfully submitted a complete Provider Survey. (You may need to refresh your browser for the status to update.) Program Materials The following 2020 Bariatric Surgery materials are available to help applicant facilities gather the necessary information ahead of time, prior to completing the online application in BD Portal. • Provider Survey (PDF version) o NOTE: Each applicant facility must submit an electronic version of the Provider Survey in BD Portal; paper responses will not be accepted. • Supplemental Instructions to Complete the 2020 Provider Survey – available in BD Portal Library • Evaluation Components Additional program materials for the Blue Distinction Centers ® for Bariatric Surgery are available on www.bcbs.com. Blue Cross Blue Shield Association is an association of independent Blue Cross and Blue Shield companies. BDCBS_020520 1
Transcript
Blue Distinction® Centers for Bariatric Surgery 2020 Provider Survey
Bl ueD isti nction® Specialty Care
& ' BlueCross T. ~ .. BlueShield Association
Printed version of this document is for reference purposes only.
A completed Provider Survey will need to be submitted via the online web application BD PortalSM.
Paper copies of the Provider Survey will not be accepted.
Review instructions below to complete the Provider Survey via the online web application BD Portal.
BD PortalSM Instructions:
• In the Survey Actions screen, under Survey, click on “Check Out” and then “Take Survey” to open the Provider Survey.
• To save your responses, click “Save.” • If you need to edit the Provider Survey at a later time, click on “Save and Exit.” This will save
your responses and exit the Provider Survey. • You must also “Release” the Provider Survey on the Survey Actions screen, as applicable, if
other contacts need to access the Provider Survey. • Once the Provider Survey is complete and ready to be submitted, click on “Submit.” Close
the survey window to bring you back to the Survey Actions screen. • Each applicant facility must submit a complete electronic version of the Provider Survey in BD
Portal for a complete submission. • Please be sure that the status of your electronic application displays “Submitted,” which will
confirm that the applicant facility has successfully submitted a complete Provider Survey. (You may need to refresh your browser for the status to update.)
Program Materials
The following 2020 Bariatric Surgery materials are available to help applicant facilities gather the necessary information ahead of time, prior to completing the online application in BD Portal.
• Provider Survey (PDF version) o NOTE: Each applicant facility must submit an electronic version of the Provider Survey
in BD Portal; paper responses will not be accepted. • Supplemental Instructions to Complete the 2020 Provider Survey – available in BD Portal
Library
• Evaluation Components
Additional program materials for the Blue Distinction Centers® for Bariatric Surgery are available on www.bcbs.com.
Blue Cross Blue Shield Association is an association of independent Blue Cross and Blue Shield companies.
Please complete all Provider Survey information pertaining to the applicant facility’s current and active bariatric surgery program for adults (18 years and older). Please be sure that all Provider Survey responses are complete before submitting.
Provider Survey Question Numbers
Facility Information 1 - 5
Comprehensive Center Information 6 - 37
Ambulatory Surgery Center Information 38 - 70
Transfer Facility and Team Tables 71 - 73
Network Status and Hospital Based Physicians 74 - 76
Terms & Conditions n/a
FACILITY INFORMATION
Please note that the Blue Distinction Specialty Care designation is for individual facilitiesonly, and does not designate hospital systems or groups. The data and information submitted in this Provider Survey should ONLY be for the individual applicant facility located at the address listed below. Each facility that provides bariatric surgery services will need tocomplete its own Bariatric Surgery 2020 Provider Survey.
APPLICANT FACILITY’S ADDRESS AND IDENTIFIERS WILL BE PRE-POPULATED IN THE ONLINE VERSION OF THIS PROVIDER SURVEY IN BD PORTAL.
If any of the applicant facility’s information shown above is incorrect, submit a Case in BD Portal or contact your local Blue Cross and/or Blue Shield Plan directly to have the information corrected.
To submit a Case in BD Portal go to the Case Management tab New Provider Case - then enter the correct information in the Description Box.
To access your Provider Record, click on your facility’s name on the ‘Survey Actions’ tab in BD Portal. Please review your National Provider Identifier (NPI), Federal Tax Identification Number (FEIN), and CMS Certification Number (CMS ID) on your Provider Record in BD Portal, to confirm accuracy. These Key Identifiers referenced are essential to data collection, and when incorrect, can jeopardize the completeness and accuracy of eligibility results.
BDCBS_020520 2
□ □
1§1
1. Populate the following information for the person responsible for completing and submitting this Provider Survey:
Primary ContactName: Title: Phone: Email:
2. Populate the following information for the applicant facility’s legal contact. This individual may be contacted in the event there are questions related to potential brand conflicts that need to be addressed.
3. The Blue Distinction Centers for Bariatric Surgery designation is awarded to individual facilities(i.e., unique bricks-and-mortar facilities with unique addresses) only. Any applicant facility with multiple locations (different addresses) must complete a separate Provider Survey for each location. Health systems and other groups of multiple facilities will not be designated collectively.
Is the Quality information submitted in this Provider Survey (e.g., accreditations, volume, outcomes) only for the single applicant facility whose name and address are listed in the Facility Information Section, above, and for no other facilities or locations?
YES NO
If NO, please explain. (Only opens if ‘No’ is checked; unlimited text)
4. On claims submitted by the applicant facility to the local Blue Plan, please tell us which fields will allow this applicant’s location to be distinguished from other facilities’ locations (as well as other facilities within your health system).
Rationale: Evaluation of Blue Plans’ healthcare claims data for Blue Distinction eligibility requires use of the same distinct provider identifiers that are present on submitted claims, in order for the corresponding claims data to match back to the applicant facility’s application. These identifiers must identify not just the overall provider system, but the individual distinct location that is completing this application.
Mark all that apply and, if desirable, provide additional guidance on the best method of distinguishing the applicant facility’s claims from others.
Federal Employer Identification Number (FEIN / Tax ID) National Provider Identifier (NPI) CMS Certification Number (CCN)
BDCBS_020520 3
LJ LJ
□ LJ □ LJ
□
□
□
Distinct Provider Location Name on Claims Distinct Provider Location Address/ZIP Code on Claims Specific sequence of Claim Control Numbers Plan Provider Number (Provider ID with Blue Plan) Locations within our health system cannot be distinguished on claims DO NOT KNOW: We do not have insight into this information and cannot answer at this time.
Additional guidance for distinguishing this location’s claims: (Note: unlimited text with large box to view typing)
5. Indicate the applicant facility’s intent to apply as either an inpatient acute care facility (with/without outpatient capabilities) or ambulatory surgery center (ASC) for the Blue Distinction Centers for Bariatric Surgery designation.
The applicant facility listed above intends to apply as an inpatient acute care facility(with/without outpatient capabilities). (CONTINUE TO QUESTION 6)
The applicant facility listed above intends to apply as a free standing ambulatory surgery center (ASC). (SKIP TO QUESTION 38)
The applicant facility listed above does NOT intend to submit a Provider Survey for the Blue Distinction Centers for Bariatric Surgery program. If you have selected this option, please “Save and Exit” this Provider Survey. Do not complete the remaining Questions.
COMPREHENSIVE CENTER INFORMATION
The ‘Comprehensive Center Information’ section should be completed by inpatient acute care facilities (with/without outpatient capabilities) that have a bariatric surgery program.
Questions in this section that refer to “my,” “your,” “my program/facility” or “your program/facility” all refer to the applicant facility’s own adult bariatric surgery program (not the Blue Distinction Centersfor Bariatric Surgery program).
Please refer to the Supplemental Instructions for guidance in completing the Provider Survey.
BDCBS_020520 4
□
□
□
□
□
□
□
□
□
□
□
□
□
6. Indicate which of the following statements describes the applicant facility’s current bariatric surgery program’s Metabolic and Bariatric Surgery Accreditation and Quality ImprovementProgram (MBSAQIP) accreditation status. (Check only one)
The applicant facility’s bariatric surgery program has full approval as an MBSAQIPComprehensive Center.
The applicant facility’s bariatric surgery program has full approval as an MBSAQIP Comprehensive Center with Adolescent Qualifications.
The applicant facility’s bariatric surgery program has full approval as an MBSAQIP Comprehensive Center with Obesity Medicine Qualifications.
The applicant facility’s bariatric surgery program has full approval as an MBSAQIP Comprehensive Center with Adolescent and Obesity Medicine Qualifications.
The applicant facility’s bariatric surgery program has full approval as an MBSAQIP Low Acuity Center.
The applicant facility’s bariatric surgery program is currently in the process of applying for MBSAQIP accreditation.
The applicant facility’s bariatric surgery program is not in the process of applying for MBSAQIP accreditation, but will be applying within the next 12 months.
The applicant facility is not currently accredited nor in the process of obtaining MBSAQIP accreditation. (If checked, cannot check any boxes above)
7. Indicate which of the following statements describes the applicant facility's current accreditation status. Check ALL that apply.
The applicant facility is fully accredited (without provision or condition) by The Joint Commission (TJC) in the Hospital Accredited Program. www.jointcommission.org
The applicant facility is fully accredited by Healthcare Facilities Accreditation Program (HFAP) of the Accreditation Association for Hospital and Health Systems (AAHHS) as an acute care hospital. www.hfap.org
The applicant facility is fully accredited by DNV GL Healthcare in the National Integrated Accreditation for Healthcare Organizations (NIAHO®) Hospital Accreditation Program. www.dnvaccreditation.com
The applicant facility is fully accredited by the Center for Improvement in Healthcare Quality (CIHQ) in the Hospital Accreditation Program. www.cihq.org
The applicant facility is not fully accredited by any of the above organizations. (If checked, cannot check any boxes above)
8. Opioid use is now recognized as one of the most serious healthcare problems in the United States. Opioid-overdose deaths have increased every year for the past two decades, driving a drug-overdose epidemic that killed more than 70,000 Americans in 2017.i Until recently, many providers considered this a societal and political problem beyond the means of most healthcare providers to address. However, it has become increasingly clear that many patients suffering from opioid dependence and addiction are first exposed to opioids through postoperative prescriptions.ii i National Center for Health Statistics. Vital statistics rapid release: provisional drug overdose death counts. Vital statistics rapid release. November 2018 (https://w ww.cdc.gov) ii Corey S. Davis, J.D., M.S.P.H., The SUPPORT for Patients and Communit ies Act— What Will It Mean for the Opioid-Overdose Crisis? New England Journal of Medicine, 2018
Does the applicant facility participate in the metabolic and bariatric quality improvement collaborative, Bariatric Surgery Targeting Opioid Prescriptions (BSTOP)? (This Question is informational only.)
YES NO
9. Does the applicant facility collect patient satisfaction data for its bariatric service line (e.g., Hospital Consumer Assessment of Healthcare Providers and Systems [HCAHPS] measures)?
YES NO
Bariatric Surgery Site Case Volume
For Questions 10 through 20, please use the applicant facility’s MBSAQIP Data Registry online non-risk-adjusted “Site Case Volume Report” to enter its bariatric surgery total case volumes from 1/1/2019 through 12/31/2019. Responses should reflect the applicant facility’s true volume (including procedures that may not have been entered into the data registry).
Note: Do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant facility does not have the requested data, check ‘Data Not Available.’
Question # Procedure Type
Number of Bariatric Surgery Cases Performed at Your ‘Site’ for the time
period of 1/1/2019 – 12/31/2019
Data Not Available
10. Laparoscopic Sleeve Gastrectomy (LSG)
# (whole number only up to 5 characters, zero is a valid
response)
(If Checked, can’t enter in numeric
value)
11. Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’tenter in numeric
value)
12. Laparoscopic Adjustable Gastric Band (LAGB)
# (whole number only up to 5 characters, zero is a valid
Number of Bariatric Surgery Cases Performed at Your ‘Site’ for the time
period of 1/1/2019 – 12/31/2019
Data Not Available
13. Open Roux-en-Y Gastric Bypass (ORYGB) (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’tenter in numeric
value)
14. Biliopancreatic Diversion with Duodenal Switch BPD/DS
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’tenter in numeric
value)
15. Other (Primary) #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
16. LAGB Removal/Revision #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
17. Reoperation/RevisionEmergency and Non-emergency Cases
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’t enter in numeric
value)
18. Stapling Procedures* #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
19. Non-Stapling Procedures #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
20. Total Number of Bariatric Surgery Procedures
(Automatic Calculation sum of Questions 18 and 19)
*Stapling Procedures:MBSAQIP defines “Stapling Procedure” as any procedure involving the use of a surgical stapler for the anastomosis or resection of any part of the gastrointestinal (GI) tract. Procedures involving hand-sutured anastomosis are also included as Stapling Procedures in this procedure category.
Bariatric Surgery Patient Follow-up and Co-Morbidity Improvement
For Questions 21 through 23, please use the applicant facility’s MBSAQIP Data Registry online non-risk-adjusted “Site Case Volume Report” to enter its bariatric surgery total case volumes from 1/1/2018 through 12/31/2018. The volumes will be used to answer Questions 24 through 28.
Note: Do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant facility does not have the requested data, check ‘Data Not Available.’
BDCBS_020520 7
□
□
□
□
□
□
□ □
Question # Procedure Type
Number of Bariatric Procedures Performed at Your ‘Site’ for the time
period of1/1/2018 – 12/31/2018
Data Not Available
21. Stapling Procedures* #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’tenter in numeric
value)
22. Non-Stapling Procedures #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’tenter in numeric
value)
23. Total Number of Bariatric Surgery Procedures
(Automatic Calculation sum ofQuestions 21 and 22)
*Stapling Procedures:MBSAQIP defines “Stapling Procedure” as any procedure involving the use of a surgical stapler for the anastomosis or resection of any part of the gastrointestinal (GI) tract. Procedures involving hand-sutured anastomosis are also included as Stapling Procedures in this procedure category.
24. Please check the timeframe that the applicant facility provides patient follow-up for bariatric surgery patients.
If the applicant facility provides patient follow-up at 30 days, 1 month and/or 1 year, of those patients reported in Question 23 (total number of bariatric procedures), provide the number of bariatric surgery patients who were contacted and received a scheduled clinical assessment.
If the applicant facility does not provide patient follow-up, choose ‘None of the Above’. (Table should be optional to complete)
Patient Follow-up Timeframe Check All That Apply
Of the number of patients reported in Question 23, report the number of patients who were contacted and
received a scheduled clinical assessment for the Patient Follow-up Timeframe Selected
(This column is INFORMATIONAL; If the applicant facility does not have the data or chooses not to respond, leave the cells blank.)
30 Days #
6 Months #
1 Year #
None of the Above Leave blank if ‘None of the Above’ is checked
25. Does the applicant facility utilize the MBSAQIP Bariatric Surgical Risk/Benefit Calculator to guide surgical decision making and informed consent? For more information regarding the Bariatric Surgical Risk/Benefit Calculator, refer to the Bariatric Surgical Risk/Benefit Calculator
26. Does the applicant facility track the percent of Total Weight Loss (%TWL) at 1 year follow-up?
YES (Complete Question 27) NO (Skip to Question 28)
27. Of the patients reported in Question 23, what is the applicant facility’s percent of Total Weight Loss at 1 year follow-up?
Enter %TWL as a number (ex: 15.01) % (2 decimal places, numbers only, no percent % symbol in answer)
Note: This Question is INFORMATIONAL. If you choose not to respond, please leave blank. Only enter zero (0) if the reported value is zero (0).
28. Please check the medical condition(s) the applicant facility tracks for medical improvement post-op bariatric surgery.
Of those bariatric surgery patients reported in Question 21 (stapling volume only), report the number of patients who had an improvement in their medical condition(s) at 1-year post-op.
If the applicant facility does not track improvement of the medical conditions listed, choose ‘None of the Above’.
Medical Conditions Tracked for Improvement
Check All That Apply
Of the number of procedures reported in Question 21 (stapling volume only), report the number of patients who
had an improvement in their medical condition(s) at 1-year post-op
(This column is INFORMATIIONAL; If the applicant facility does not have the data or chooses not to respond, leave the cells blank.)
Insulin Dependent Diabetes #
Hypercholesterolemia #
Hypertension #
None of the Above Leave Blank if ‘None of the Above’ is checked
Bariatric Surgery Patient Outcomes
Questions 29 through 32 are referring to the applicant facility’s risk adjusted MBSAQIP Semiannual Report (SAR) from the January 2020 release, which includes procedures performed from 7/1/2018 through 6/30/2019.
29. Does the applicant facility have risk adjusted Laparoscopic Sleeve Gastrectomy (LSG) Patient Outcomes from the MBSAQIP SAR January 2020 release?
YES (Complete Question 30) NO (Continue on to Question 31)
BDCBS_020520 9
□ □
30. Complete the Laparoscopic Sleeve Gastrectomy (LSG) Patient Outcomes table using the applicant facility’s MBSAQIP SAR January 2020 Report.
Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant facility’s MBSAQIP SAR.
Total Observed Predicted Expected Odds 95% Confidence Interval
Cases Events Rate Observed Rate Rate Ratio Low er Upper
LSG Morbidity
LSG All Occurrence Morbidity
LSG Serious Event
LSG Leak
LSG Bleeding
LSG SSI
LSG All Cause Reoperation
LSG Related Reoperation
LSG All Cause Intervention
LSG Related Intervention
LSG All Cause Readmission LSG Related Readmission
Cases/Events columns = Whole Numbers, 5 characters, zero is an acceptable answ er; Rates, Ratio, Confidence Intervals columns = 2 Decimal places, no value over 100, zero is an acceptable answ er.
31. Does the applicant facility have risk adjusted Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) Patient Outcomes from the MBSAQIP SAR January 2020 release?
YES (Complete Question 32) NO (Continue on to Question 33)
32. Complete the Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) Patient Outcomes table using the applicant facility’s MBSAQIP SAR January 2020 Report.
Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant facility’s MBSAQIP SAR.
BDCBS_020520 10
□
□
□
I I I I Total Observed Predicted Expected Odds 95% Confidence Interval
Cases Events Rate Observed Rate Rate Ratio Lower Upper
LRYGB Morbidity
LRYGB All Occurrence Morbidity
LRYGB Serious Event
LRYGB Leak
LRYGB Bleeding
LRYGB SSI
LRYGB All Cause Reoperation LRYGB Related Reoperation LRYGB All Cause Intervention LRYGB Related Intervention LRYGB All Cause Readmission LRYGB Related Readmission
Cases/Events Columns = Whole Numbers, 5 characters, zero is an acceptable answ er; Rates, Ratio, Confidence Intervals Columns = 2 Decimal places, no value over 100, zero is an acceptable answ er.
33. Please select the statement below that best represents the applicant facility’s Laparoscopic Adjustable Gastric Band (LAGB) procedures. Questions 34 and 35 pertain to the applicant facility’s LAGB volume and outcomes for the time period 7/1/2018 through 6/30/2019. (Check only ONE)
The applicant facility offers LAGB procedures and has LAGB patient outcome data for 7/1/2018 through 6/30/2019. (Complete Questions 34 and 35)
The applicant facility offers LAGB procedures but does NOT have LAGB patient outcome data for 7/1/2018 through 6/30/2019. (Skip to Question 36)
The applicant facility does NOT offer LAGB procedures and does NOT have LAGB patient outcome data for 7/1/2018 through 6/30/2019. (Skip to Question 36)
Questions 34 and 35 are to be completed using the applicant facility’s ability to pull the MBSAQIP Data Registry online non-risk adjusted “30-Day Morbidity and Mortality Report” and “30-Day Readmissions, Reoperations, and Interventions Report” for Laparoscopic Adjustable Gastric Band procedures performed from 7/1/2018 through 6/30/2019.
BDCBS_020520 11
-
34. Laparoscopic Adjustable Gastric Band (LAGB) Patient Outcomes reported from the MBSAQIP Data Registry non-risk adjusted “30-Day Morbidity and Mortality Report” for the time period of 7/1/2018 through 6/30/2019.
Report the data for the applicant facility’s ‘Site.’ The report has the number of cases (numerator) followed by the rate for each measure under the ‘Site’ column. (Table is Optional, cells may be left blank for no data available)
Note: Only enter zero (0) if the response is zero (0) for the corresponding measure. Leave the table cells blank for any measures involving data that is not reported or is reported as N/A in the applicant facility’s non-risk adjusted reports.
30 Day Morbidity and Mortality Report Site # of Cases Site Rate %
Total Number of Cases (Denominator) DO NOT ENTER DATA INTO THIS CELL
Mortalities
Morbidity: Cases w ith one or more occurrences
Cases w ith Wound Occurrences
Superficial Incisional SSI
Deep Incisional SSI
Organ/Space SSI
Wound Disruption
Cases With Metabolic/Bariatric Occurrences
Unplanned Admission to ICU w ithin 30 days
Cases With MBSAQIP Specific Events
Band Slippage/Prolapse
Band Erosion
LAGB – Port, Tubing, or Band Problem
Site # Cases Column = Whole Numbers, 5 characters, zero is an acceptable answ er; Site Rate % Column = 2 Decimal places, no value over 100, zero is an acceptable answ er.
35. Laparoscopic Adjustable Gastric Band (LAGB) Patient Outcomes reported from the MBSAQIP Data Registry online non-risk adjusted “30-Day Readmission, Reoperations, and Interventions Report,” for the time period of 7/1/2018 through 6/30/2019.
Report the data for the applicant facility’s ‘Site.’ The report has the number of cases (numerator) followed by the rate for each measure under the ‘Site’ column.
BDCBS_020520 12
-
Note: Only enter zero (0) if the response is zero (0) for the corresponding measure. Leave the table cells blank for any measures involving data that is not reported or is reported as N/A in the applicant facility’s non-risk adjusted reports.
30 Day Readmission, Reoperations, and Interventions Report
Site # of Cases Site Rate %
Total Number of Cases (Denominator) DO NOT ENTER DATA INTO THIS CELL
Total Readm issions (Avg)
Total Reoperations (Avg)
Total Interventions (Avg)
Total Number of Readmissions Related to Principal Procedure (AVG)
Band Slippage/Prolapse
Readm ission
Reoperation
Intervention
Band Erosion
Readm ission
Reoperation
Intervention
LAGB – Port, Tubing, or Band Problem
Readm ission
Reoperation
Intervention
Cases w ith Reoperations
Band Rem oval
Band, Tubing, or Port Revisions
Band Placem ent
Cases w ith Interventions Therapeutic Endoscopy: w ith Band Rem oval
Site # Cases Column = Whole Numbers, 5 characters, zero is an acceptable answ er; Site Rate % Column = 2 Decimal places, no value over 100, zero is an acceptable answ er.
BDCBS_020520 13
□
36. Enter ‘Your Facility’ unadjusted 30-day mortality rate for all cases (primary, revision, etc.), as shown in the 30-Day Mortality snapshot. Your facility should use the MBSAQIP SAR from the January 2020 release for procedures performed from 7/1/2018 through 6/30/2019.
Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant facility’s MBSAQIP SAR. If the applicant facility does not have the data requested, check the box ‘Unable to Report Data’.
Site Number of Sites
Total Cases
Death Cases
30-Day Mortality Rate (%)
Mean Site 30-Day
Mortality Rate (%)
Standard Deviations from Mean Site Rate
Unable to
ReportData
‘Your Facility’
Site # and Cases Columns = Whole Numbers, 5 characters, zero is an acceptable answ er; Rate % Columns = 2 Decimal places, no value over 100, zero is an acceptable answ er.
37. Enter the applicant facility’s 30-Day post-operative bariatric procedure emergency room department (ED) patient visits for procedures performed from 01/1/2019 – 12/31/2019. (This is the number of patients that went to the ER within 30 days from the time of their procedure.)
Note: Enter a numerator and denominator, do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant facility does not have the requested data, enter ’Not Applicable’ in the text box provided.
Numerator: Number of ED Patient Visits: w hole number < total number below , 5 characters, zero is an acceptable answ er
Denominator: Total Number of Bariatric Surgery Patients: whole number, 5 characters, and zero is an acceptable answ er
ED Patient Visit Rate: % (Automatic Calculation) 2 decimal places, no value over 100, zero is an acceptable answ er
Enter ‘Not Applicable’ if applicant facility is unable to report requested data. (Typed text must be exact ‘Not Applicable”) (If N/A, cannot fill out boxes above)
END OF COMPREHENSIVE CENTER INFORMATION SECTION
CONTINUE TO QUESTION 71
BDCBS_020520 14
□
□
□
□
□
□
□
□
□
□
AMBULATORY SURGERY CENTER INFORMATION The ‘Ambulatory Surgery Center Information’ section should be completed by AmbulatorySurgery Centers (ASCs) that have a bariatric surgery program. The applicant ASC’s bariatric surgery program should be accredited, or in the process of becoming accredited, as a Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP)Ambulatory Surgery Center. For this Section, Questions that refer to the “applicant ASC” mean the same as the “applicant facility” whose bariatric surgery program provides services at an ASC.
Questions in this section that refer to “my,” “your,” “my program/facility/ASC” or “your program/facility/ASC” all refer to the applicant ASC’s own adult bariatric surgery program (not the Blue Distinction Centers for Bariatric Surgery program).
Please refer to the Supplemental Instructions for guidance in completing the Provider Survey.
38. Indicate which of the following statements describes the applicant ASC’s current bariatric surgery program’s Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program(MBSAQIP) accreditation status. (Check only one)
The applicant ASC’s bariatric surgery program has full approval as an MBSAQIP Ambulatory Surgery Center.
The applicant ASC’s bariatric surgery program is currently in the process of applying forMBSAQIP Ambulatory Surgery Center accreditation.
The applicant ASC’s bariatric surgery program is not currently in the process of applying, but will be applying within the next 12 months for MBSAQIP Ambulatory Surgery Center accreditation.
The applicant ASC’s is not currently accredited nor in the process of obtaining MBSAQIP accreditation. (If checked, cannot check any boxes above)
39. Indicate which of the following statements describes the applicant ASC’s current accreditation status. Check ALL that apply.
The applicant ASC is fully accredited (without provision or condition) by The Joint Commission (TJC) in the Ambulatory Care Accredited Program. www.jointcommission.org
The applicant ASC is fully accredited by Healthcare Facilities Accreditation Program (HFAP) of the Accreditation Association for Hospital and Health Systems (AAHHS) as an Ambulatory Surgical Center. www.hfap.org
The applicant ASC is fully accredited by the American Association for Accreditation of Ambulatory Surgery Facilities—Surgical (AAAASF). www.aaaasf.org
The applicant ASC is fully accredited by the Accreditation Association for Ambulatory Health Care (AAAHC) as an Ambulatory Surgery Center. www.aaahc.org
The applicant ASC is fully accredited by the Center for Improvement in Healthcare Quality (CIHQ) in the Ambulatory Accreditation Program. www.cihq.org
The applicant ASC is not fully accredited by any of the above organizations. (If checked, cannot check any boxes above)
40. Opioid use is now recognized as one of the most serious healthcare problems in the United States. Opioid-overdose deaths have increased every year for the past two decades, driving a drug-overdose epidemic that killed more than 72,000 Americans in 2017.i Until recently, many providers considered this a societal and political problem beyond the means of most healthcare providers to address. However, it has become increasingly clear that many patients suffering from opioid dependence and addiction are first exposed to opioids through postoperative prescriptions.ii
I National Center for Health Statistics. Vital statistics rapid release: provisional drug overdose death counts. Vital statistics rapid release. November 2018 (https://w ww.cdc.gov) ii Corey S. Davis, J.D., M.S.P.H., The SUPPORT for Patients and Communit ies Act— What Will It Mean for the Opioid-Overdose Crisis? New England Journal of Medicine, 2018.
Does the applicant ASC participate in the metabolic and bariatric quality improvement collaborative, Bariatric Surgery Targeting Opioid Prescriptions (BSTOP)? (This Question is informational only.)
YES NO
Bariatric Surgery Patient Satisfaction
41. Does the applicant ASC collect patient satisfaction data for its bariatric service line (e.g., Hospital Consumer Assessment of Healthcare Providers and Systems Outpatient and Ambulatory Surgery Survey [OAS-CAHPS] measures)?
YES NO
Bariatric Surgery Site Case Volume
For Questions 42 through 52, please use the applicant ASC’s MBSAQIP Data Registry online non-risk-adjusted “Site Case Volume Report” to enter its bariatric surgery total case volumes from 1/1/2019 through 12/31/2019. Responses should reflect the applicant facility’s true volume (including procedures that were not entered into the data registry).
Note: Do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant ASC does not have the requested data, check ‘Data Not Available.’
Question # Procedure Type
Number of Bariatric Procedures Performed at Your ‘Site’ for the time
period of 1/1/2019 – 12/31/2019
Data Not Available
42. Laparoscopic Sleeve Gastrectomy (LSG)
# (whole number only up to 5 characters, zero is a valid
response)
(If Checked, can’t enter in numeric
value)
43. Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
# (whole number only up to 5 characters, zero is a valid
Number of Bariatric Procedures Performed at Your ‘Site’ for the time
period of 1/1/2019 – 12/31/2019
Data Not Available
44. Laparoscopic Adjustable Gastric Band (LAGB)
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’tenter in numeric
value)
45. Open Roux-en-Y Gastric Bypass (ORYGB)
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’tenter in numeric
value)
46. Biliopancreatic Diversion with Duodenal Switch BPD/DS
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’t enter in numeric
value)
47. Other (Primary) #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
48. LAGB Removal/Revision #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
49. Reoperation/RevisionEmergency and Non-emergency Cases
# (whole number only up to 5 characters, zero is a valid
response) (If Checked, can’t enter in numeric
value)
50. Stapling Procedures* #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
51. Non-Stapling Procedures #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’t enter in numeric
value)
52. Total Number of Bariatric Surgery Procedures
(Automatic Calculation sum of Questions 50 and 51)
*Stapling Procedures:MBSAQIP defines a “Stapling Procedure” as any procedure involving the use of a surgical stapler for the anastomosis or resection of any part of the gastrointestinal (GI) tract. Procedures involving hand-sutured anastomosis are also included as Stapling Procedures in this procedure category.
Bariatric Surgery Patient Follow-up and Co-Morbidity Improvement
For Questions 53 and 55, please use the applicant ASC’s MBSAQIP Data Registry online non-risk-adjusted “Site Case Volume Report” to enter its bariatric surgery total case volumes from 1/1/2018 through 12/31/2018. The volumes will be used to answer Questions 56 through 60.
Note: Do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant ASC does not have the requested data, check ‘Data Not Available.’
BDCBS_020520 17
□
□
□
□
□
□
□ □
Question # Procedure Type
Number of Bariatric Procedures Performed at Your ‘Site’ for the time
period of1/1/2018 – 12/31/2018
Data Not Available
53. Stapling Procedures* #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’tenter in numeric
value)
54. Non-Stapling Procedures #
(whole number only up to 5 characters, zero is a valid response)
(If Checked, can’tenter in numeric
value)
55. Total Number of Bariatric Surgery Procedures
(Automatic Calculation sum ofQuestions 53 and 54)
*Stapling Procedures:MBSAQIP defines a “Stapling Procedure” as any procedure involving the use of a surgical stapler for the anastomosis or resection of any part of the gastrointestinal (GI) tract. Procedures involving hand-sutured anastomosis are also included as Stapling Procedures in this procedure category.
56. Please check the timeframe that the applicant ASC provides patient follow-up for bariatric surgery patients.
If the applicant ASC provides patient follow-up at 30 days, 1 month and/or 1 year, of those patients reported in Question 55 (total number of bariatric surgery procedures), provide the number of bariatric surgery patients who were contacted and received a scheduled clinical assessment.
If the applicant facility does not provide patient follow-up, choose ‘None of the Above’.
Patient Follow-up Timeframe Check All That Apply
Of the number of patients reported in Question 55, report the number of patients who were contacted and
received a scheduled clinical assessment for the Patient Follow-up Timeframe Selected
(This column is INFORMATIIONAL; If the applicant ASC does not have the data or chooses not to respond, leave the cells blank.)
30 Days #
6 Months #
1 Year #
None of the Above Leave Blank if ‘None of the Above’ checked
57. Does the applicant ASC utilize the MBSAQIP Bariatric Surgical Risk/Benefit Calculator to guide surgical decision making and informed consent? For more information regarding the Bariatric Surgical Risk/Benefit Calculator, refer to the Bariatric Surgical Risk/Benefit Calculator
58. Does the applicant ASC track the percent of Total Weight Loss (%TWL) at 1 year follow-up?
YES (Complete Question 59) NO (Skip to Question 60)
59. Of the patients reported in Question 55, what is the applicant ASC’s percent of Total Weight Loss at 1 year follow-up?
Enter %TWL as a number (ex: 15.01) % (2 decimal places, numbers only, no percent % symbol in answer)
Note: This Question is INFORMATIONAL. If you choose not to respond, please leave it blank. Only enter zero (0) if the reported volume is zero (0).
60. Please check the medical condition(s) the applicant ASC tracks for medical improvement post-op bariatric surgery.
Of those bariatric surgery patients reported in Question 53 (stapling volume only), report the number of patients who had an improvement in their medical condition(s) at 1-year post-op.
If the applicant ASC does not track improvement of the medical conditions listed, choose ‘None of the Above’.
Medical Conditions Tracked for Improvement
Check All That Apply
Of the number of procedures reported in Question 53 (stapling volume only), report the number of patients who had
an improvement in their medical condition(s) at1-year post-op
(This column is INFORMATIIONAL; If the applicant ASC does not have the data or chooses not to respond, leave the cells blank.)
Insulin Dependent Diabetes #
Hypercholesterolemia #
Hypertension #
None of the Above Leave Blank if ‘None of the Above’ checked
Bariatric Surgery Patient Outcomes
Questions 61 through 64 are referring to the applicant ASC’s risk adjusted MBSAQIP Semiannual Report (SAR) from the January 2020 release, which includes procedures performed from 7/1/2018 through 6/30/2019.
61. Does the applicant ASC have risk adjusted Laparoscopic Sleeve Gastrectomy (LSG) Patient Outcomes from the MBSAQIP SAR January 2020 release?
YES (Complete Question 62) NO (Continue on to Question 63)
BDCBS_020520 19
□ □
62. Complete the Laparoscopic Sleeve Gastrectomy (LSG) Patient Outcomes table using the applicant ASC’s MBSAQIP SAR January 2020 Report.
Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant ASC’s MBSAQIP SAR.
Total Observed Predicted Expected Odds 95% Confidence Interval
Cases Events Rate Observed Rate Rate Ratio Low er Upper
LSG Morbidity
LSG All Occurrence Morbidity
LSG Serious Event
LSG Leak
LSG Bleeding
LSG SSI
LSG All Cause Reoperation LSG Related Reoperation LSG All Cause Intervention LSG Related Intervention LSG All Cause Readmission LSG Related Readmission
Cases/Events Columns = Whole Numbers, 5 characters, zero is an acceptable answ er; Rates, Ratio, Confidence Intervals Columns = 2 Decimal places, no value over 100, zero is an acceptable answ er.
63. Does the applicant ASC have risk adjusted Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) Patient Outcomes from the MBSAQIP SAR January 2020 release?
YES (Complete Question 64) NO (Skip to Question 65)
64. Complete the Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) Patient Outcomes table using the applicant ASC’s MBSAQIP SAR January 2020 Report.
Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant ASCs MBSAQIP SAR.
BDCBS_020520 20
□
□
□
Total Observed Predicted Expected Odds 95% Confidence Interval
Cases Events Rate Observed Rate Rate Ratio Lower Upper
LRYGB Morbidity
LRYGB All Occurrence Morbidity
LRYGB Serious Event
LRYGB Leak
LRYGB Bleeding
LRYGB SSI
LRYGB All Cause Reoperation LRYGB Related Reoperation LRYGB All Cause Intervention LRYGB Related Intervention LRYGB All Cause Readmission LRYGB Related Readmission
Cases/Events Columns = Whole Numbers, 5 characters, zero is an acceptable answ er; Rates, Ratio, Confidence Intervals Columns = 2 Decimal places, no value over 100, zero is an acceptable answ er.
65. Please select the statement below that best represents the applicant ASC’s Laparoscopic Adjustable Gastric Band (LAGB) procedures. Questions 66 and 67 pertain to the applicant ASC’s LAGB volume and outcomes for the time period 7/1/2018 through 6/30/2019. (Check only ONE).
The applicant ASC offers LAGB procedures and has LAGB patient outcome data for 7/1/2018 through 6/30/2019 (Complete Questions 66 and 67)
The applicant ASC offers LAGB procedures but does NOT have LAGB patient outcome data for 7/1/2018 through 6/30/2019 (Skip to Question 68)
The applicant ASC does NOT offer LAGB procedures and does NOT have LAGB patient outcome data for 7/1/2018 through 6/30/2019 (Skip to Question 68)
Questions 66 and 67 are to be completed using the applicant ASC’s ability to pull the MBSAQIP Data Registry online non-risk adjusted “30-Day Morbidity and Mortality Report” and 30-Day Readmissions, Reoperations, and Interventions Report” for the applicant ASC’s Laparoscopic Adjustable Gastric Band procedures performed from 7/1/2018 through 6/30/2019.
Note: Only enter zero (0) if the response is zero (0) for the corresponding measure. Leave the table cells blank for any measures involving data that is not reported or reported as N/A in the applicant ASC’s non-risk adjusted reports.
BDCBS_020520 21
-
66. Laparoscopic Adjustable Gastric Band (LAGB) Patient Outcomes reported from the MBSAQIP Data Registry online non-risk adjusted “30-Day Morbidity and Mortality Report” for the time period of 7/1/2018 through 6/30/2019.
Report the data for the applicant ASC’s ‘Site’. The report has the number of cases (numerator) followed by the rate for each measure under the ‘Site’ column.
Note: Only enter zero (0) if the response is zero (0) for the corresponding measure. Leave the table cells blank for any measures involving data that is not reported or is reported as N/A in the applicant facility’s non-risk adjusted reports.
30 Day Morbidity and Mortality Report Site # of Cases Site Rate %
Total Number of Cases (Denominator) DO NOT ENTER DATA INTO TOP CELL
Mortalities
Morbidity: Cases w ith one or m ore occurrences
Cases w ith Wound Occurrences
Superficial Incisional SSI
Deep Incisional SSI
Organ/Space SSI
Wound Disruption
Cases With Metabolic/Bariatric Occurrences
Unplanned Adm ission to ICU w ithin 30 days
Cases With MBSAQIP Specific Events
Band Slippage/Prolapse
Band Erosion
LAGB – Port, Tubing, or Band Problem
Site # Cases Column = Whole Numbers, 5 characters, zero is an acceptable answ er; Site Rate % Column = 2 Decimal places, no value over 100, zero is an acceptable answ er.
67. Laparoscopic Adjustable Gastric Band (LAGB) Patient Outcomes reported from the MBSAQIP Data Registry online non-risk adjusted “30-Day Readmission, Reoperations, and Interventions Report”, for the time period of 7/1/2018 through 6/30/2019.
Report the data for the applicant ASC’s ‘Site’. The report has the number of cases (numerator) followed by the rate for each measure under the ‘Site’ column.
Note: Only enter zero (0) if the response is zero (0) for the corresponding measure. Leave the table cells blank for any measures involving data that is not reported or is reported as N/A in the applicant facility’s non-risk adjusted reports.
BDCBS_020520 22
-30 Day Readmission, Reoperations, and Interventions Report
Site # of Cases Site Rate %
Total Number of Cases (Denominator) DO NOT ENTER DATA INTO TOP CELL
Total Readmissions (Avg)
Total Reoperations (Avg)
Total Interventions (Avg)
Total Number of Readmissions Related to Principal Procedure (AVG)
Band Slippage/Prolapse
Readmission
Reoperation
Intervention
Band Erosion
Readmission
Reoperation
Intervention
LAGB – Port, Tubing, or Band Problem
Readmission
Reoperation
Intervention
Cases w ith Reoperations
Band Removal
Band, Tubing, or Port Revisions
Band Placement
Cases w ith Interventions
Therapeutic Endoscopy: w ith Band Removal
Site # Cases Column = Whole Numbers, 5 characters, zero is an acceptable answ er; Site Rate % Column = 2 Decimal places, no value over 100, zero is an acceptable answ er.
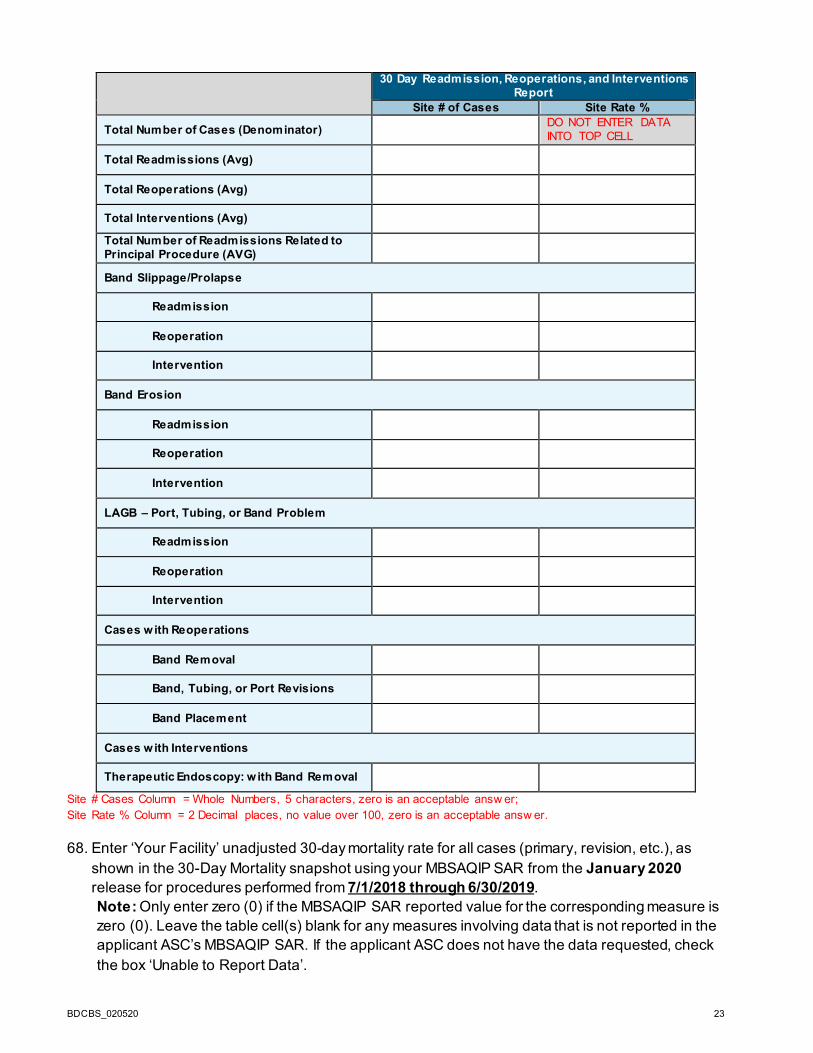
68. Enter ‘Your Facility’ unadjusted 30-day mortality rate for all cases (primary, revision, etc.), as shown in the 30-Day Mortality snapshot using your MBSAQIP SAR from the January 2020 release for procedures performed from 7/1/2018 through 6/30/2019. Note: Only enter zero (0) if the MBSAQIP SAR reported value for the corresponding measure is zero (0). Leave the table cell(s) blank for any measures involving data that is not reported in the applicant ASC’s MBSAQIP SAR. If the applicant ASC does not have the data requested, check the box ‘Unable to Report Data’.
BDCBS_020520 23
□
Site Number of Sites
Total Cases
Death Cases
30-Day Mortality Rate (%)
Mean Site 30-Day
Mortality Rate (%)
Standard Deviations from Mean Site Rate
Unable to
ReportData
‘Your Facility’
Site # Cases Column = Whole Numbers, 5 characters, zero is an acceptable answ er; Site Rate % Column = 2 Decimal places, no value over 100, zero is an acceptable answ er.
69. Enter the applicant ASC’s 30-Day post-operative bariatric procedure emergency room department (ED) patient visits for procedures performed from 01/1/2019 – 12/31/2019. (This is the number of patients that went to the ER within 30 days from the time of their procedure.)
Note: Enter a numerator and denominator, do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant ASC does not have the requested data, enter ’Not Applicable’ in the text box provided.
Numerator: Number of ED Patient Visits: w hole number < total number below , 5 characters, zero is an acceptable answ er
Denominator: Total Number of Bariatric Surgery Patients: whole number, 5 characters, and zero is an acceptable answ er
ED Patient Visit Rate: % (Automatic Calculation) 2 decimal places, no value over 100, zero is an acceptable answ er Enter ‘Not Applicable’ if applicant ASC is unable to report requested data. (Typed text must be exact ‘Not Applicable”)
70. Enter the applicant ASC’s bariatric surgery patient transfers from the applicant ASC to an inpatient acute care facility (includes on-site ICU) for a higher level of care, for procedures performed from 01/1/2019 – 12/31/2019.
Note: Enter a numerator and denominator, do not leave blank. Only enter zero (0) if the reported volume is zero (0). If the applicant ASC does not have the requested data, enter ’Not Applicable’ in the text box provided.
Numerator: Number of Patients Transferred: whole number < total number below , 5 characters, zero is an acceptable answ er
Denominator: Total Number of Bariatric Surgery Patients: whole number, 5 characters, and zero is an acceptable answ er
Patient Transfer Rate: % (Automatic Calculation) 2 decimal places, no value over 100, zero is an acceptable answ er
Enter ‘Not Applicable’ if applicant ASC is unable to report requested data. (Typed text must be exact ‘Not Applicable”)
END OF AMBULATORY SURGERY CENTER INFORMATION SECTIONS
CONTINUE TO QUESTION 71
BDCBS_020520 24
LJ
□ □ □
J LJ LJ LJ
TRANSFER FACILITY AND TEAM TABLES 71. Please Select Provider Type: (Drop Down Box)
Ambulatory Surgery Center (ASC) (Complete Question 72, Transfer Facility Table) Hospital with an onsite Intensive Care Unit (ICU) (Skip to Question 73) Hospital without an onsite Intensive Care Unit (ICU) (Complete Question 72, Transfer
Facility Table)
72. Transfer Facility Table
Transfer Facility Table should only be completed by ASCs and by Hospitals without an ICU.
Please complete the following table for each inpatient facility with which the applicant facility (or applicant ASC) transfers bariatric surgery patients, when in need for a higher level of care, with the appropriate resources (including onsite ICU). Refer to the NPPES NPI Registry to find the transfer facility’s National Provider Identifier (NPI) number.
Transfer FacilityName Address City State Zip Code
Transfer Facility’sNational Provider
Identifier (NPI) xxx xxx xxx xx xxx xxx numeric only
73. Bariatric Surgery Surgeon Team Table
Please complete the Team Table for ALL Surgeons who have privileges AND are actively performing bariatric surgery services for the bariatric surgery program at the applicant facility (or applicant ASC).
Exclusions: • Exclude all Surgeons who are not currently practicing at the applicant facility (or applicant
ASC) at the time of this application’s submission (i.e., retired, left employment). • Exclude all Surgeons who do not perform bariatric surgery. • Exclude all locum tenens Surgeons. • Exclude all Physician Assistants, Nurse Practitioners, and Medical/Surgical Residents in
training.
Instructions for Team Table Completion:
Step 1 – Manually enter Surgeon information (i.e., First Name, Last Name, National Provider Identifier) into the table below. Note, the Surgeon’s National Provider Identifier (NPI) number can be obtained online at: http://npidb.org/npi/.
Step 2 – Click the Save button to update the Surgeon Table. Repeat as necessary until all Surgeons are added to the Table below.
SURGEON’S FIRST NAME LAST NAME TYPE 1 NATIONAL PROVIDER
IDENTIFIER (NPI)
xxx alpha only
NETWORK STATUS AND HOSPITAL BASED PHYSICIANS
The Blue Cross and Blue Shield Association strongly supports efforts to empower patients with greater access to meaningful information that allows them to make the best choices for their healthcare. The following questions ask information about the applicant facility’s (or applicant ASC) efforts to prevent unexpected out of network costs for the consumer, and the participation of physician groups in your local Blue Cross and/or Blue Shield BlueCard Preferred Provider Organization (PPO) network.
74. What action is the applicant facility (or applicant ASC) taking to prevent unexpected out of network costs (sometimes referred to as “surprise billing”)? Check all that apply.
Notify all patients of their rights regarding balance billing, as part of the intake process
Require patients to consent to out-of-network care
Provide information on a patient’s providers’ network status when the services are being scheduled, so changes can be made (if feasible and desired)
Currently engaged in improving the accuracy of the applicant facility’s network status in directories, to ensure reliable information for patients Governed under a state law that addresses surprise bills
Additional Actions and Comments: (Text Box, Unlimited)
None of the above (if this is checked, others may not be)
75. Do ALL of the following hospital-based physicians who bill patients separately on any products or services in connection with applicant facility’s (or applicant ASC’s) bariatric surgery program (with examples including, but not limited to, professional providers, radiology and/or lab services, etc., as described generally in the most recent Provider Survey) (“Hospital-Based Physicians”) participate in the local Blue Cross and/or Blue Shield BlueCard PPO Network?
Hospital-based physicians who bill separately are those whose charges are not bundled and included as part of this applicant facility (or applicant ASC) billed charges.
Note: Do not leave table blank. If you are unable to answer the question or do not know, check ‘Unknown’, if you do not provide the specialty service, check ‘Not Applicable’. You may also provide additional comments.
BDCBS_020520 26
□ □ □ □
□ □ □ □
□ □ □ □
□ □ □ □
□ □ □ □
□ □ □ □
□ □ □ □
n 7
Radiologists Yes No Unknown Not Applicable Additional Comments:
Anesthesiologists Yes No Unknown Not Applicable Additional Comments:
Pathologists Yes No Unknown Not Applicable Additional Comments:
Intensivists Yes No Unknown Not Applicable Additional Comments:
Hospitalists Yes No Unknown Not Applicable Additional Comments:
Emergency Room
Yes No Unknown Not Applicable Additional Comments:
Other (Please Describe in ‘Additional Comments’
Yes No Unknown Not Applicable Additional Comments:
76. Please complete the following table for all of the hospital-based physician groups providing services to bariatric surgery patients where the applicant facility (or applicant ASC) response to Question # 75 was either ‘Yes or No’.
Note: If the applicant facility’s (or applicant ASC’s) response was ‘Unknown’ and/or ‘Not Applicable’, you do not need to provide the information in the table below for those hospital-based physician group(s).
Instructions for Hospital-Based Physician Group Table Completion:
Step 1 – Manually enter Physician Group Name and National Provider Identifier (NPI) into the table below. Note, the hospital-based physician group’s NPI number can be obtained online at: http://npidb.org/npi/. Step 2 – Choose the Physician Group Specialty Type from the drop down list provided. Step 3 – Chose ‘Yes or No’ from the drop down list, indicating if the hospital-based physician group is contracted with the Local Blue Cross and/or Blue Shield BlueCard Plan’s (PPO) Network. Step 4 – Click the Save button to update the Physician Table. Repeat as necessary until all Physicians are added to the Table below.
PHYSICIAN GROUP NAME
NATIONAL PROVIDER
IDENTIFIER (NPI)
PHYSICIAN GROUP SPECIALTY TYPE
(drop dow n list to include: Radiologists, Anesthesiologists,
By submitting its response to this Provider Survey for consideration as a participant in this Blue Distinction Specialty Care® Program (the “Program”), and, if accepted by BCBSA, as a condition to any designation and participation in the Program, this applicant facility (“Facility”) represents and agrees as follows:
1. All information that Facility provides in its response to BCBSA’s Provider Survey for consideration as a participant in this Program (including information provided in Facility’s initial response, as well as any additional materials submitted throughout the evaluation and appeal process for this Provider Survey cycle) is and will be true and complete, as of the date Facility provides such information to BCBSA. Facility will advise BCBSA immediately of any material change in such information during this Provider Survey process, and if Facility is designated as a Blue Distinction Center under this Program, for the duration of such designation.
2. BCBSA may share Facility’s individual Provider Survey responses (“Raw Data”) and results (“Scores”) with BCBSA’s member Plans and, pursuant to a confidentiality agreement, member Plans’ current and prospective accounts, for purposes of evaluation, care management, quality improvement, and member Plans’ design of customized products and networks. BCBSA may combine Facility’s Raw Data and Scores together with other facilities’ data to create aggregate information for public dissemination, provided that such aggregate information will not identify Facility by name, and will not contain any Protected Health Information (“PHI”), as defined under the Health Insurance Portability and Accountability Act of 1996 and its implementing regulations (45 C. F. R. Parts 160-164). Facility’s Raw Data and Scores will not be publicly disseminated beyond the extent permitted above without Facility’s prior written consent, unless required by law (e.g., subpoena).
� PROVIDER attests that it has read, understands, and agrees with the terms set forth in the Attestation (Section A in the scroll down box, above) and represents and agrees that the statements therein are accurate.
B. OPTIONAL – PUBLIC STATEMENT ON HOSPITAL BASED PHYSICIANS’ PPO STATUS Available Only for Providers that are Hospitals, Ambulatory Surgery Centers, and Outpatient Clinics (Not Applicable to Individual Physicians or Physician Groups)
These terms apply only if Provider has elected to opt-in to this optional public disclosure feature for this Program.
BDCBS_020520 28
Optional Public Statement: BlueCard® PPO Network Participation Status of Hospital Based Physicians
Provider, at its option, may elect to disclose that all Hospital Based Physicians who provide Related Services at that Provider participate in the Local Plan’s BlueCard PPO network (with terms as defined and described below). This feature is not a Program requirement. Provider’s decision on whether or not to participate in this feature will not impact its Designation status. If Provider consents to participate in this optional feature for the Program, then Provider represents and warrants voluntarily that, as of the Effective Date of this Agreement, all Hospital Based Physicians who provide Related Services at this Provider participate in the Local Plan’s BlueCard PPO network (with terms as defined and described below). With Provider’s consent, BCBSA and the Local Plan will convey and recognize this participating physician information through transparent public messaging in the National Doctor & Hospital Finder and other related materials. Provider will provide BCBSA and the Local Plan with at least thirty (30) days’ prior written notice: (a) if any Hospital Based Physician who may provide Related Services will not participate in the Local Plan’s BlueCard PPO network, or (b) if any Hospital Based Physician who does participate in the Local Plan’s BlueCard PPO network does not renew its then current participation agreement at least thirty (30) days in advance of its expiration date; and promptly thereafter, BCBSA will remove this public statement from the National Doctor & Hospital Finder and other related materials. BCBSA will provide Provider with notice of opportunities that may arise thereafter to reinstate this public statement, in the event that all Hospital Based Physicians who provide Related Services at this Provider subsequently participate again in the Local Plan’s BlueCard PPO network.
"Hospital Based Physicians" means all of the following physicians rendering services at this Provider:
"Related Services" means all services provided by Hospital Based Physicians for adult patients (age 18 years and older) for all episodes of care covered by this Program (as defined at www.bcbs.com).
� OPTIONAL – CHECK IF PROVIDER CONSENTS TO PARTICIPATE IN OPTIONAL PUBLIC STATEMENT FOR THIS BD PROGRAM. Provider has read and understands the Optional Public Statement terms (Section B in the scroll down box, above) and hereby consents to participate in this optional feature for this Blue Distinction Program, pursuant to the terms set forth therein.
Note: Contact BCBSA if this Provider desires to opt in later, or if this Provider opts in now but later needs to opt out of this feature.
Provider verifies that it responded to the Attestation and Optional Public Statement items above, by and through its duly authorized officer identified below:
Enter Officer’s Name: _______________________________________ Enter Officer’s Title: _______________________________________ Date: ____________