BLOOD- VESSEL TUMOURS OF THE BRAIN* By C. WORSTER-DROUGHT, M.A., M.D., F.R.C.P. Physician, West End Hospitalfor Nervous Diseases; Physician and Neurologist, Metropolitan Hospital, London, etc. Blood-vessel tumours or angiomata which occur in the brain may be classified under two headings: (i) Malformations of blood-vessels and (2) Haemangioblastomata, or true neoplasms of the elements forming blood-vessels. The former result from a fault in development, and differ from the haemangioblastomata in that they consist of an accumulation of definite, although enlarged, blood-vessels with nervous tissue, intact or com- pressed, between the vascular loops constituting the angioma. It is generally agreed that all types of intra- cranial angiomata are of congenital origin, although often of only slow growth and development. Angiomatous malformations include the following conditions: (a) Telangiectatic angiomata. These are small, mainly capillary, lesions similar to those frequently seen in the skin, and are of no clinical importance as they do not cause symptoms. Such telangiec- tases are discovered only incidentally during post- mortem examinations, and occur most frequently in the floor of the fourth ventricle and in the upper part of the pons. (b) Capillary angiomata involve the meninges and surface of the brain, and frequently co-exist with similar capillary naevi of the face; and some- times of the trunk on the same side of the body. This association is known as the Sturge-Kalischer- Weber syndrome. Sturge, in 1879, reported the case of a girl, aged six years, with an extensive capillary naevus, especially of the right side of the face and head, and focal epileptiform attacks starting in the left hand. He concluded that the right side of the brain was involved in the naevoid condition. Kalischer, in I897, reported a case of diffuse con- genital naevus involving the scalp and face which, on post-mortem examination, showed a lesion described as a blood-vessel tumour composed of capillaries and veins. Parkes Weber, in 1922, reported the radiographic appearances of the skull of a typical case which showed a large capillary naevus involving especially the left side of the face, and a right-sided upper neurone hemiplegia. * Based on a postgraduate lecture given at the West End Hospital for Nervous Diseases, London. FIG. I.-Sturge-Kalischer-Weber Syndrome. A girl, aged 4* years, showing extensive cutaneous naevi on left side of face, upper part of chest and arm. The upper part of the back on the left side, the left leg, both buttocks, and to a lesser extent the right side of the face, also showed scattered naevus formations. The child was mentally deficient and suffered from right-sided hemiplegia and Jack- sonian epilepsy. X-ray examinationr of the skull showed bilateral intracranial calcification, but more pronounced on the left side. X-ray examination of the skull revealed a more or less calcified lesion on the surface of the left cerebral hemisphere. The symptoms and signs of Sturge-Kalischer- Weber syndrome consist in the presence of a facial naevus, with or without similar lesions in other parts of the body (Fig. i), and epilepsy-usually Jacksonian in type and involving the side of the body contralateral to the facial naevus. Not in- frequently, a definite hemiparesis is present (Fig. i) with consequent increase in tendon reflexes and an extensor plantar reflex. These conditions may also be associated with buphthalmos (ox-eye or i6o
Transcript
BLOOD-VESSEL TUMOURS OF THE BRAIN*By C. WORSTER-DROUGHT, M.A., M.D., F.R.C.P.
Physician, West End Hospitalfor Nervous Diseases;Physician and Neurologist, Metropolitan Hospital, London, etc.
Blood-vessel tumours or angiomata which occurin the brain may be classified under two headings:(i) Malformations of blood-vessels and (2)Haemangioblastomata, or true neoplasms of theelements forming blood-vessels. The formerresult from a fault in development, and differfrom the haemangioblastomata in that they consistof an accumulation of definite, although enlarged,blood-vessels with nervous tissue, intact or com-pressed, between the vascular loops constitutingthe angioma.
It is generally agreed that all types of intra-cranial angiomata are of congenital origin, althoughoften of only slow growth and development.
Angiomatous malformations include the followingconditions:
(a) Telangiectatic angiomata. These are small,mainly capillary, lesions similar to those frequentlyseen in the skin, and are of no clinical importanceas they do not cause symptoms. Such telangiec-tases are discovered only incidentally during post-mortem examinations, and occur most frequentlyin the floor of the fourth ventricle and in theupper part of the pons.
(b) Capillary angiomata involve the meningesand surface of the brain, and frequently co-existwith similar capillary naevi of the face; and some-times of the trunk on the same side of the body.This association is known as the Sturge-Kalischer-Weber syndrome.
Sturge, in 1879, reported the case of a girl,aged six years, with an extensive capillary naevus,especially of the right side of the face and head,and focal epileptiform attacks starting in the lefthand. He concluded that the right side of thebrain was involved in the naevoid condition.Kalischer, in I897, reported a case of diffuse con-genital naevus involving the scalp and face which,on post-mortem examination, showed a lesiondescribed as a blood-vessel tumour composed ofcapillaries and veins. Parkes Weber, in 1922,reported the radiographic appearances of the skullof a typical case which showed a large capillarynaevus involving especially the left side of theface, and a right-sided upper neurone hemiplegia.
* Based on a postgraduate lecture given at the WestEnd Hospital for Nervous Diseases, London.
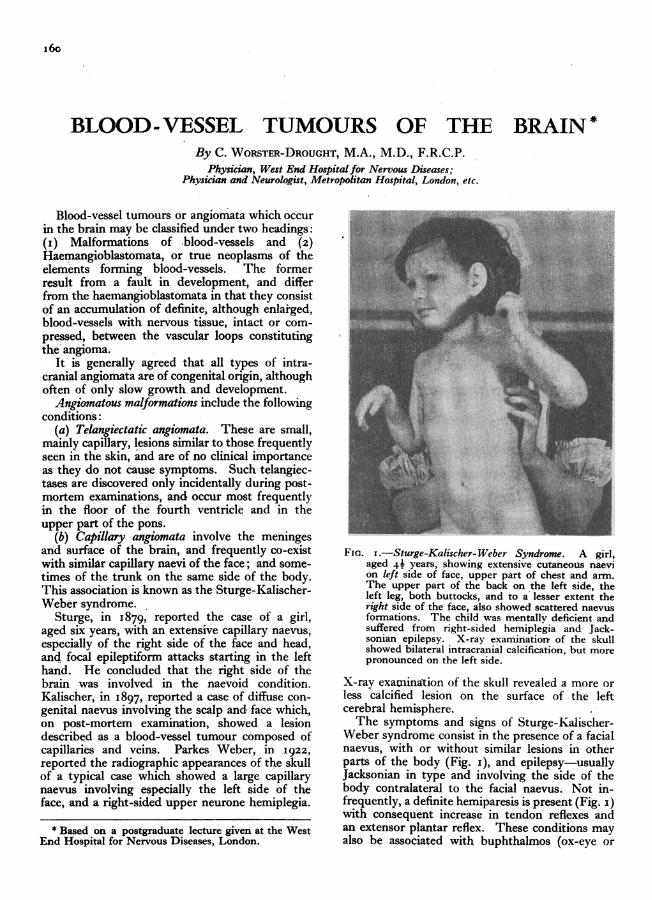
FIG. I.-Sturge-Kalischer-Weber Syndrome. A girl,aged 4* years, showing extensive cutaneous naevion left side of face, upper part of chest and arm.The upper part of the back on the left side, theleft leg, both buttocks, and to a lesser extent theright side of the face, also showed scattered naevusformations. The child was mentally deficient andsuffered from right-sided hemiplegia and Jack-sonian epilepsy. X-ray examinationr of the skullshowed bilateral intracranial calcification, but morepronounced on the left side.
X-ray examination of the skull revealed a more orless calcified lesion on the surface of the leftcerebral hemisphere.The symptoms and signs of Sturge-Kalischer-
Weber syndrome consist in the presence of a facialnaevus, with or without similar lesions in otherparts of the body (Fig. i), and epilepsy-usuallyJacksonian in type and involving the side of thebody contralateral to the facial naevus. Not in-frequently, a definite hemiparesis is present (Fig. i)with consequent increase in tendon reflexes andan extensor plantar reflex. These conditions mayalso be associated with buphthalmos (ox-eye or
i6o
W()RSTER-DR(UGIIT: Blood-Vessel Tlumouirs of the Brain
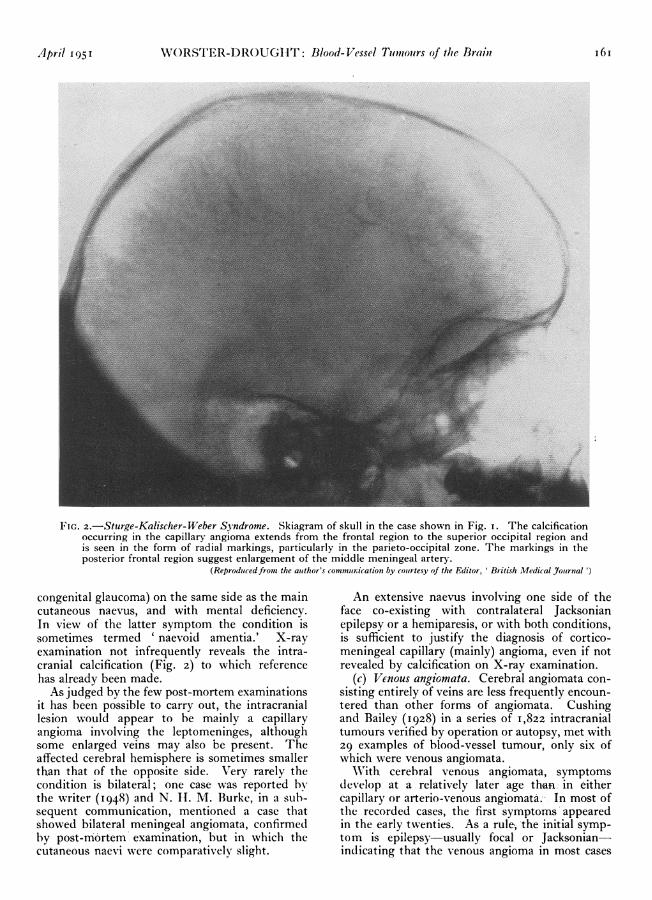
FIG. 2.-Sturge-Kalischer-Weber Syndrome. Skiagram of skull in the case shown in Fig. i. The calcificationoccurring in the capillary angioma extends from the frontal region to the superior occipital region andis seen in the form of radial markings, particularly in the parieto-occipital zone. The markings in theposterior frontal region suggest enlargement of the middle meningeal artery.
(Reproducedfrom the author's conmmurnication by courtesy of the Editor, British Medical Journal ')
congenital glaucoma) on the same side as the maincutaneous naevus, and with mental deficiency.In view of the latter symptom the condition issometimes termed ' naevoid amentia.' X-rayexamination not infrequently reveals the intra-cranial calcification (Fig. 2) to which referencehas already been made.As judged by the few post-mortem examinations
it has been possible to carry out, the intracraniallesion would appear to be mainly a capillaryangioma involving the leptomeninges, althoughsome enlarged veins may also be present. Theaffected cerebral hemisphere is sometimes smallerthan that of the opposite side. Very rarely thecondition is bilateral; one case was reported bythe writer (I948) and N. 1I. M. Burke, in a sub-sequent communication, mentioned a case thatshowed bilateral meningeal angiomata, confirmedby post-mortem examination, but in which thecutaneous naevi were comparatively slight.
An extensive naevus involving one side of theface co-existing with contralateral Jacksonianepilepsy or a hemiparesis, or with both conditions,is sufficient to justify the diagnosis of cortico-meningeal capillary (mainly) angioma, even if notrevealed by calcification on X-ray examination.
(c) Venous angiomata. Cerebral angiomata con-sisting entirely of veins are less frequently encoun-tered than other forms of angiomata. Cushingand Bailey (1928) in a series of 1,822 intracranialtumours verified by operation or autopsy, met with29 examples of blood-vessel tumour, only six ofwhich were venous angiomata.
WNith cerebral venous angiomata, symptomsdevelop at a relatively later age than in eithercapillary or arterio-venous angiomata.- In most ofthe recorded cases, the first symptoms appearedin the early twenties. As a rule; the initial symp-tom is epilepsy-usually focal or Jacksonian-indicating that the venous angioma in most cases
April 1951 I6I
POSTGRADUATE MEDICAL J(URNAL
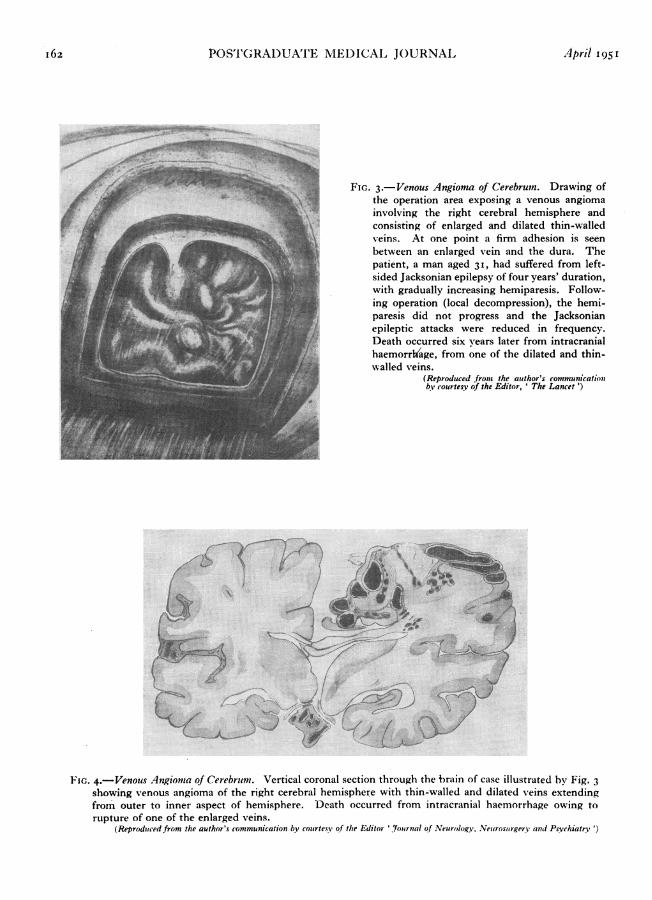
FIG. 3.-Venous Angioma of Cerebrum. Drawing ofthe operation area exposing a venous angiomainvolving the right cerebral hemisphere andconsisting of enlarged and dilated thin-walledveins. At one point a firm adhesion is seenbetween an enlarged vein and the dura. Thepatient, a man aged 31, had suffered from left-sided Jacksonian epilepsy of four years' duration,with gradually increasing hemiparesis. Follow-ing operation (local decompression), the hemi-paresis did not progress and the Jacksonianepileptic attacks were reduced in frequency.Death occurred six years later from intracranialhaemorrhage, from one of the dilated and thin-walled veins.
(Reproduced from the author's communicationby courtesy of the Editor, ' The Lancet ')
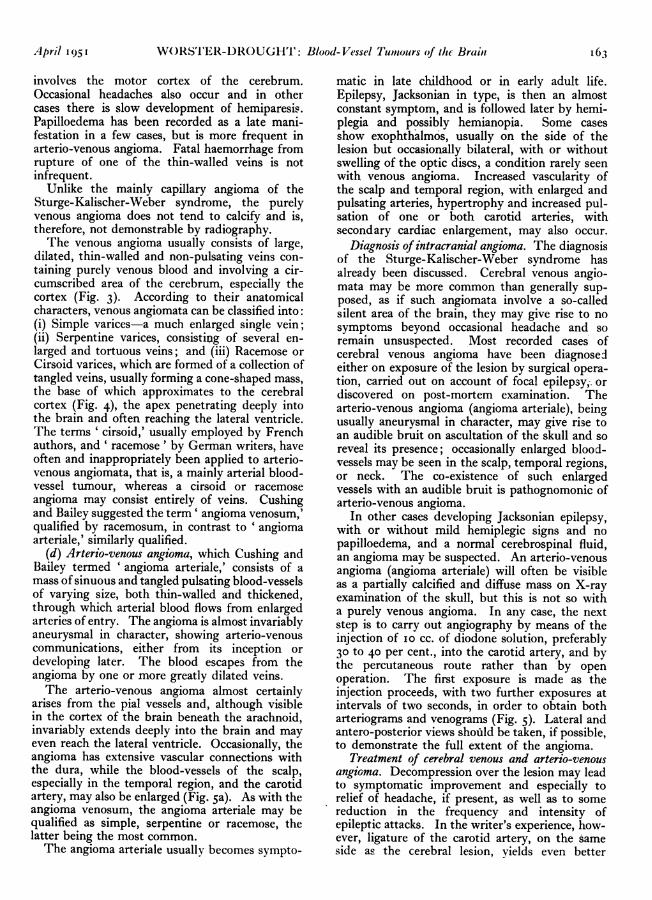
FIG. 4.-Venous Angionta of Cerebrlum. Vertical coronal section through the brain of case illustrated by Fig. 3showing venous angioma of the right cerebral hemisphere with thin-walled and dilated veins extendingfrom outer to inner aspect of hemisphere. Death occurred from intracranial haemorrhage owing torupture of one of the enlarged veins.
(Reproduced from the author's communication by courtesy of the Editor 'Jou4rnal of Neurology, Neurosurgery% and Psychiatry ')
162 April 195 t
... ·..r *·.IJE""
_.*16·'··
.*.VI"
W()RSTER-DROUGHT: Blood-Vessel Tumlours of the Brain
involves the motor cortex of the cerebrum.Occasional headaches also occur and in othercases there is slow development of hemiparesis.Papilloedema has been recorded as a late mani-festation in a few cases, but is more frequent inarterio-venous angioma. Fatal haemorrhage fromrupture of one of the thin-walled veins is notinfrequent.
Unlike the mainly capillary angioma of theSturge-Kalischer-Weber syndrome, the purelyvenous angioma does not tend to calcify and is,therefore, not demonstrable by radiography.The venous angioma usually consists of large,
dilated, thin-walled and non-pulsating veins con-taining purely venous blood and involving a cir-cumscribed area of the cerebrum, especially thecortex (Fig. 3). According to their anatomicalcharacters, venous angiomata can be classified into:(i) Simple varices-a much enlarged single vein;(ii) Serpentine varices, consisting of several en-larged and tortuous veins; and (iii) Racemose orCirsoid varices, which are formed of a collection oftangled veins, usually forming a cone-shaped mass,the base of which approximates to the cerebralcortex (Fig. 4), the apex penetrating deeply intothe brain and often reaching the lateral ventricle.The terms ' cirsoid,' usually employed by Frenchauthors, and ' racemose' by German writers, haveoften and inappropriately been applied to arterio-venous angiomata, that is, a mainly arterial blood-vessel tumour, whereas a cirsoid or racemoseangioma may consist entirely of veins. Cushingand Bailey suggested the term' angioma venosum,'qualified by racemosum, in contrast to ' angiomaarteriale,' similarly qualified.
(d) Arterio-venous angioma, which Cushing andBailey termed ' angioma arteriale,' consists of amass of sinuous and tangled pulsating blood-vesselsof varying size, both thin-walled and thickened,through which arterial blood flows from enlargedarteries of entry. The angioma is almost invariablyaneurysmal in character, showing arterio-venouscommunications, either from its inception ordeveloping later. The blood escapes from theangioma by one or more greatly dilated veins.The arterio-venous angioma almost certainly
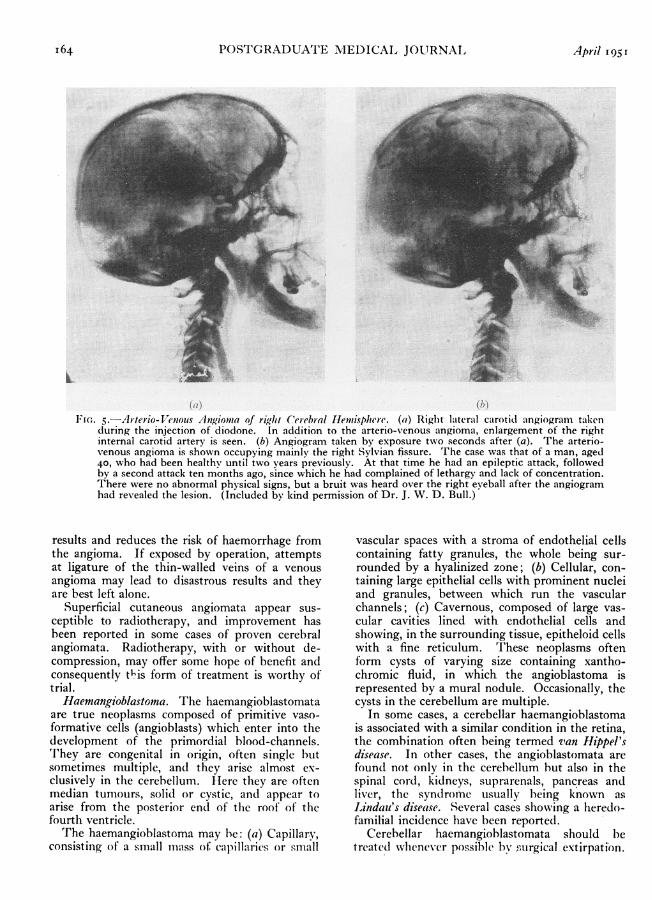
arises from the pial vessels and, although visiblein the cortex of the brain beneath the arachnoid,invariably extends deeply into the brain and mayeven reach the lateral ventricle. Occasionally, theangioma has extensive vascular connections withthe dura, while the blood-vessels of the scalp,especially in the temporal region, and the carotidartery, may also be enlarged (Fig. 5a). As with theangioma venosum, the angioma arteriale may bequalified as simple, serpentine or racemose, thelatter being the most common.The angioma arteriale usually becomes sympto-
matic in late childhood or in early adult life.Epilepsy, Jacksonian in type, is then an almostconstant symptom, and is followed later by hemi-plegia and possibly hemianopia. Some casesshow exophthalmos, usually on the side of thelesion but occasionally bilateral, with or withoutswelling of the optic discs, a condition rarely seenwith venous angioma. Increased vascularity ofthe scalp and temporal region, with enlarged andpulsating arteries, hypertrophy and increased pul-sation of one or both carotid arteries, withsecondary cardiac enlargement, may also occur.
Diagnosis of intracranial angioma. The diagnosisof the Sturge-Kalischer-Weber syndrome hasalready been discussed. Cerebral venous angio-mata may be more common than generally sup-posed, as if such angiomata involve a so-calledsilent area of the brain, they may give rise to nosymptoms beyond occasional headache and soremain unsuspected. Most recorded cases ofcerebral venous angioma have been diagnosedeither on exposure of the lesion by surgical opera-tion, carried out on account of focal epilepsy,. ordiscovered on post-mortem examination. Thearterio-venous angioma (angioma arteriale), beingusually aneurysmal in character, may give rise toan audible bruit on ascultation of the skull and soreveal its presence; occasionally enlarged blood-vessels may be seen in the scalp, temporal regions,or neck. The co-existence of such enlargedvessels with an audible bruit is pathognomonic ofarterio-venous angioma.
In other cases developing Jacksonian epilepsy,with or without mild hemiplegic signs and nopapilloedema, and a normal cerebrospinal fluid,an angioma may be suspected. An arterio-venousangioma (angioma arteriale) will often be visibleas a partially calcified and diffuse mass on X-rayexamination of the skull, but this is not so witha purely venous angioma. In any case, the nextstep is to carry out angiography by means of theinjection of io cc. of diodone solution, preferably30 to 40 per cent., into the carotid artery, and bythe percutaneous route rather than by openoperation. The first exposure is made as theinjection proceeds, with two further exposures atintervals of two seconds, in order to obtain botharteriograms and venograms (Fig. 5). Lateral andantero-posterior views shofld be taken, if possible,to demonstrate the full extent of the angioma.
Treatment of cerebral venous and arterio-venousangioma. Decompression over the lesion may leadto symptomatic improvement and especially torelief of headache, if present, as well as to somereduction in the frequency and intensity ofepileptic attacks. In the writer's experience, how-ever, ligature of the carotid artery, on the sameside as the cerebral lesion, yields even better
April 1951 I63
POSTGRADUATE MEDICAL JOURNAL
L
(a) (1,)FI,. 5.-Arterio- Venous Atngioma of righit Cerebral Hemisphere. (a) Right lateral carotid angiogram taken
during the injection of diodone. In addition to the arterio-venous angioma, enlargement of the rightinternal carotid artery is seen. (b) Angiogram taken by exposure two seconds after (a). The arterio-venous angioma is shown occupying mainly the right Sylvian fissure. The case was that of a man, aged40, who had been healthy until two years previously. At that time he had an epileptic attack, followedby a second attack ten months ago, since which he had complained of lethargy and lack of concentration.There were no abnormal physical signs, but a bruit was heard over the right eyeball after the angiogramhad revealed the lesion. (Included by kind permission of Dr. J. W. D. Bull.)
results and reduces the risk of haemorrhage fromthe angioma. If exposed by operation, attemptsat ligature of the thin-walled veins of a venousangioma may lead to disastrous results and theyare best left alone.
Superficial cutaneous angiomata appear sus-ceptible to radiotherapy, and improvement hasbeen reported in some cases of proven cerebralangiomata. Radiotherapy, with or without de-compression, may offer some hope of benefit andconsequently this form of treatment is worthy oftrial.
Haemangioblastoma. The haemangioblastomataare true neoplasms composed of primitive vaso-formative cells (angioblasts) which enter into thedevelopment of the primordial blood-channels.They are congenital in origin, often single butsometimes multiple, and they arise almost ex-clusively in the cerebellum. Ilere they are oftenmedian tumours, solid or cystic, and appear toarise from the posterior end of the roof of thefourth ventricle.The haemangioblastoma may be: (a) Capillary,
consisting of a small mass of capillaries or small
vascular spaces with a stroma of endothelial cellscontaining fatty granules, the whole being sur-rounded by a hyalinized zone; (b) Cellular, con-taining large epithelial cells with prominent nucleiand granules, between which run the vascularchannels; (c) Cavernous, composed of large vas-cular cavities lined with endothelial cells andshowing, in the surrounding tissue, epitheloid cellswith a fine reticulum. These neoplasms oftenform cysts of varying size containing xantho-chromic fluid, in which the angioblastoma isrepresented by a mural nodule. Occasionally, thecysts in the cerebellum are multiple.
In some cases, a cerebellar haemangioblastomais associated with a similar condition in the retina,the combination often being termed van Hippel'sdisease. In other cases, the angioblastomata arefound not only in the cerebellum but also in thespinal cord, kidneys, suprarenals, pancreas andliver, the syndrome usually being known asLindau's disease. Several cases showing a heredo-familial incidence have been reported.
Cerebellar haemangioblastomata should betreated whenever possible by surgical extirpation.
I64 April 195 r
April 1951 ;KAPLAN: Oesophageal Hiatis Iernia I65
\When the tumour is cystic, following evacuationof the contents of the cyst, care must be taken toremove the nodule in the cyst wall, as otherwise
the symptoms will recur, either from refilling ofthe cystic cavity or from progressive growth of theangioblastomi.
BIBLIOGRAPHY
BULL, J. WV. D. (1949), Proc. Roy. Mcd(., 42, 88o.BURKE, N. H. M. (1948), Brit. Med. J., ii, 531.CUSHING, H., and BAILEY, P. (1928), ' Tumours Arising fromn
the Blood-vessels of the Brain,' Balliere, London, p. 250.KALISCHER, S. (1897), Berl. klin. Wochenschr., 30, I059.STURGE, W. A. (1879), Trans. Clin. Soc. Lond., 12, 162.
WNEBEFR, F'. PARKES (1922), 7. .Xurol. amd P'sychopathol., 3, 134.WORS'lER-DROUGHTC, C., and BALLANCE, C. A. (1922),
Lancet, ii, 125.WORSTER-DROUGHT, C., and DICKSON, W. E. CARNEGIE
(1927), J. Neurol. and Psychopathol., 8, 19.WORSTER-DROUGHT, C. (I948), Brit. Med. J., ii, 214.
OESOPHAGEAL HIATUS HERNIAA Clinical Study of Forty-Five Cases
By SAMUII, KAIPLAN, M.).Dc'/,rtmc'nt of illedicine, Univcersity of Witi (latcrsralnd, JIIoanI( 'sburt
Oesophageal hiatus hernia may be defined as atransdiaphragmatic evisceration of some part ofthe abdominal contents into the thoracic cavity.'The herniation occurs through the oesophagealhiatus and the organ that is most commonly in-vollved is the stomach. It is now well establishedthat herniation through the oesophageal hiatus ofthe diaphragm is not infrequent. 'The complexsymptomatology presented by this anatomicalvariant may, however, render difficulty in itsdiagnosis.
'I'he symptoms for which the patients may seekadvice may be divided into the following groups:
i. A syndrome of' dyspepsia.'2. Pain in the chest stimulating myocardial in-
farction.3. Acute gastrointestinal haemorrhage with
haematemesis, melaena or both.4. Symptoms of anaemia probably due to
chronic gastrointestinal haemorrhage.5. A combination of any or all of the above
groups.In addition to the above groups there is a fre-
quent association of other pathological conditionswith hiatus hernia. These include cholecystitiswith or without cholelithiasis, diverticulosis of thelarge or small intestine, and chest signs possiblydue to aspiration of oesophageal contents.
This report concerns the clinical study of 45cases of oesophageal hiatus hernia that presentedas in and out patients at the Johannesburg GeneralHospital over a period of 12 months endingMarch 1949.Of the 45 cases, 33 were females and I2 males,
giving a ratio of females to males of 3 to I. Theage incidence varied from 35 to 89 years (T'able I).
Hiatus herniae of infancy and childhood and trau-matic herniae are not included in this study.
In this series the cases are divided into categoriesaccording to the following classification intro-duced by Akerlund (1926):
I. Congenital short oesophagus with partialtlioracic stomach.
2. Paraoesophageal hiatus hernia. A portion ofthe cardiac end of the stomach herniates throughthe oesophageal hiatus of the diaphragm. Theoesophagus is of normal length and in its normalposition.
3. Oesophagogastric hernia. Both the cardiacend of the stomach and the lower oesophagusherniate through the oesophageal hiatus.The term ' sliding hernia' is used to designate
those cases in which the stomach returns to itsnormal sub-diaphragmatic position when thepatient is erect. Sliding herniae are only demon-strable with the patient supine or in the Trendel-enburg position. The term 'congenital shortoesophagus' may be a misnomer, although in-stances of true congenital shortening of the oeso-phagus are well known (Gross, I946). In thisseries, however, instances of short oesophagus werefound in elderly patients, the oldest being 89 yearsof age. Although it is possible that the shortenedoesophagus was present from birth, there are othercausal factors to be considered. A paraoesophagealor oesophagogastric hernia may, for instance, be as-sociated with post-ulcerative fibrosis, which mayshorten the oesophagus in a manner indistinguish-able radiologically from a congenital short oeso-phagus. Allison (1948) has produced evidence toshow that short oesophagus is usually an acquiredcondition, due to defects in the diaphragm which