43
Bloodborn e Pathogens ENVH 451/541 November 12, 2008
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 214 times |
| Download: | 0 times |

Bloodborne
Pathogens
ENVH 451/541
November 12, 2008
Bloodborne Pathogens (BBPs)
Other Potentially Infectious Materials
Present in
Blood or
Bloodborne Pathogens• semen
• vaginal secretions
• body fluids such as pleural, cerebrospinal, pericardial, peritoneal, synovial, and amniotic
• saliva in dental procedures (if blood is present)
• any body fluids visibly contaminated with blood
• body fluid where it is difficult to differentiate
• any unfixed tissue or organ (other than intact skin) from a human (living or dead)
• HIV- or HBV-containing cultures (cell, tissue, or organ), culture medium, or other solutions
• blood, organs, & tissues from animals infected with HIV, HBV, or BBPs
OPIM

2 Methods of Entry:
• Mucocutaneous– Enters through mucus membranes
• Percutaneous– Enters through some opening of the skin
Mucocutaneous (through a mucous membrane))
• Having infected blood or other body fluids splashed into eyes, nose or mouth
Modes of Transmission
Percutaneous (through the skin)
• Being stuck with needles or other sharps
• Having infected blood or other body fluids splashed onto skin that is cut, scratched, has sores or rashes or other skin conditions
Modes of Transmission

Bloodborne Pathogen Diseases
Some examples of bloodborne pathogens:
• Malaria • Syphilis • Brucellosis• Leptospirosis
• Arboviral infections • Relapsing fever • Creutzfeld-Jakob Disease • Viral Hemorrhagic Fever
• Ebola, Marburg
Primary Pathogens of Concern:
• Hepatitis B Virus (HBV)• Hepatitis C Virus (HCV)• Human Immunodeficiency Virus (HIV)

HIV

A global view of HIV infection33 million people [30–36 million] living with
HIV, 2007
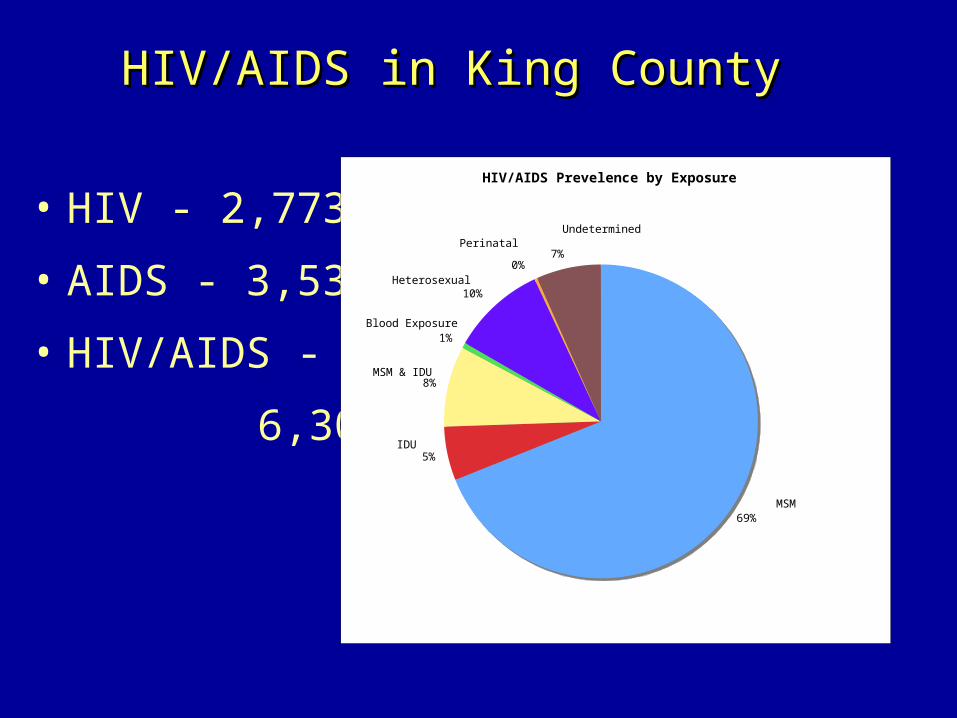
HIV/AIDS in King CountyHIV/AIDS in King County
• HIV - 2,773
• AIDS - 3,532
• HIV/AIDS -
6,305
HIV/AIDS Prevelence by Exposure
69%
5%
8%
1%
10%
0%7%
MSM
Heterosexual
Blood Exposure
Perinatal
MSM & IDU
Undetermined
IDU

HIV and AIDS
The CDC defines AIDS as a positive HIV test and one of the following:
•The development of an opportunistic infection – an infection that occurs when your immune system is impaired
•A CD4 lymphocyte count of 200 or less –a normal count ranges from 800 to 1,200– directly attack and kill invading cells

Natural History of Infection
Symptoms
• Immediately following infection– Nonspecific “viral illness”
• Low grade fever, rash, muscle aches, headache, fatigue
• Resolve in 5-10 days
• Asymptomatic– Immune system is cycling with CD4 cells
• AIDS– Extreme fatigue, rapid weight loss, swollen lymph
nodes, dry cough and shortness of breath, night sweats

Management
• No “cure”
• HAART– “cocktail” of 3 -4 AR drugs– Difficult: complex regimes,
severe side effects, compliance very important
• Diarrhea, vomiting, nausea, headache, blurred vision, dizziness, congestion, dry mouth, fatique, body ache, fever, rash, sores, feeling loss, difficulty sleeping, changing body shape, hair loss, dry skin, etc.
HIV IN BLOOD
• SURVIVAL OUTSIDE THE BODY– In dry blood the virus can survive for up to 6 days in
laboratory conditions
• QUANTITY OF VIRUS IN BLOOD– 1 mL of blood contains 200-10,000 particles of virus.
• RISK OF INFECTION FOLLOWING NEEDLE STICK INJURY – Low - 0.3% - 3 people in 1,000.
• RISK OF INFECTION FOLLOWING EYE SPLASH– Low - 0.09%
* Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recommendations and Reports, June 29, 2001 / 50(RRll);1-42. Centers for Disease Control and Prevention

Hepatitis C

Global Burden of HCV

Hepatitis C Symptoms
• flu-like symptoms
• jaundice
• fatigue
• dark urine
• abdominal pain
• loss of appetite
• nausea
US HCV Infection• Incubation period Average 6-7
weeksRange 2-26
weeks
• Acute illness (jaundice) Mild (<20%)
• Case fatality rate Low 8-10 K
• Chronic infection 60%-85% 2.7M people
• Chronic hepatitis 10%-70%
• Cirrhosis <5%-20%
• Mortality from CLD 1%-5%

Source: Sentinel Counties, CDC
Sources of Infection forPersons With Hepatitis C
Sexual 15%
Other 1%*
Unknown 10%
Injecting drug use 60%
Transfusion 10%(before screening)
* Nosocomial; iatrogenic; perinatal
Occupational 4%
Occupational Transmission
• Inefficient by occupational exposures
• Incidence 1.8% following needle stick from HCV-positive source – Associated with hollow-bore needles
• Prevalence 1-2% among health care workers – Lower than adults in the general population– Most appear related to HCW substance abuse– No restrictions routinely recommended for HCV-
infected HCWs

Perinatal Transmission of HCV
• Transmission only from women HCV-RNA positive at delivery– Average rate of infection 6%– Higher (17%) if woman co-infected with
HIV– Role of viral titer unclear
• No association with– Delivery method– Breastfeeding
• Infected infants do well– Severe hepatitis is rare
HEPATITIS C IN BLOOD
• SURVIVAL OUTSIDE THE BODY– Little is known but likely to be the same as hepatitis B, up to 10 days
• QUANTITY OF VIRUS IN BLOOD– 1 mL of blood contains 1,000 - 10,000 particles of virus
• RISK OF INFECTION FOLLOWING NEEDLE STICK INJURY – Medium - 3% - 3 people in 100
• RISK OF INFECTION FOLLOWING EYE SPLASH– Low
* Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recommendations and Reports, June 29, 2001 / 50(RRll);1-42. Centers for Disease Control and Prevention

Hepatitis B

Hepatitis BSymptoms• flu-like symptoms
• fatigue
• abdominal pain
• loss of appetite
• nausea, vomiting
• joint pain
• jaundice
Incubation• 60-120 days following
infection
Duration• Several weeks to
months
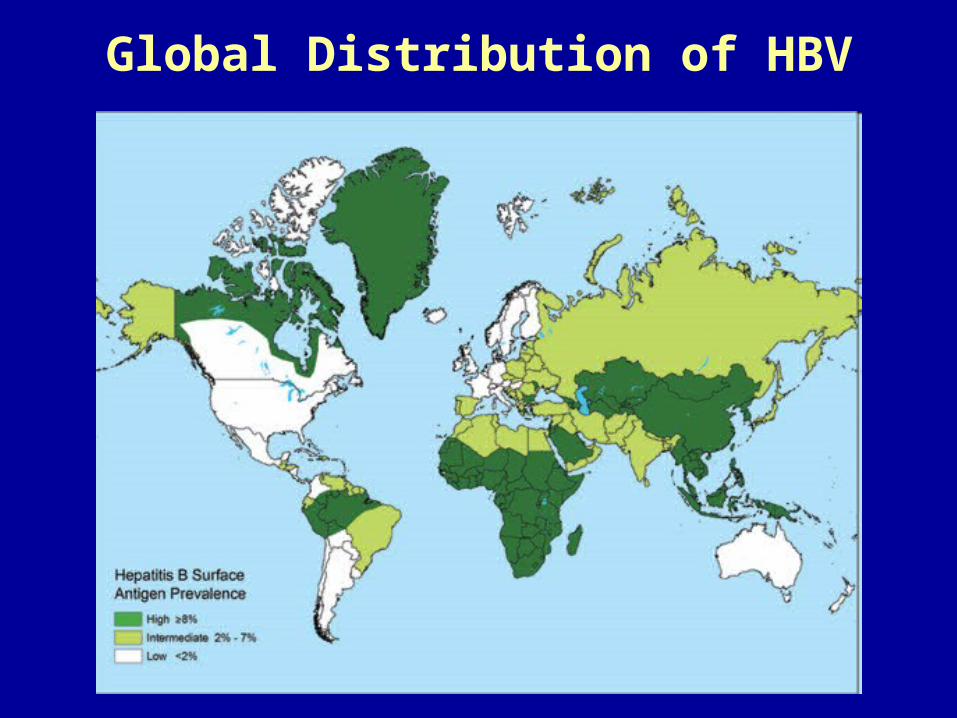
Global Distribution of HBV
8% - High

Global Patterns of Chronic HBV Infection
• High (>8%): 45% of global population– lifetime risk of infection >60%– early childhood infections common
• Intermediate (2%-7%): 43% of global population– lifetime risk of infection 20%-60%– infections occur in all age groups
• Low (<2%): 12% of global population– lifetime risk of infection <20%– most infections occur in adult risk groups

Hepatitis B Incidence

Blood transfusion 0%
Other* 15%
Unknown 32%
Hemodialysis 0%Multiple sex partners 17%
Injection drug use 14%
Men who have sex with men 6%
Sexual contact with hepatitis B patient 13%
Medical Employee 1%
Household contact of hepatitis B patient 2%
Risk Factors Associated with Reported Hepatitis B, 1990-2000,
United States
Source: NNDSS/VHSP *Other: Surgery, dental surgery, acupuncture, tattoo, other percutaneous injury

Transmission of HBV
• Concentration of HBV in various body fluids– High: Blood, serum, wound exudates– Medium: saliva, semen, and vaginal secretions– Low/not detectable: urine, feces, sweat, tears,
breastmilk
• Household transmission – less risk than percutaneous but significant - can occur in settings such as shared toothbrushes, razors, combs, washcloths
Transmission of HBV
• Likelihood of becoming a carrier varies inversely with the age at which infection occurs.
• Pool of carriers in U.S. is 1-1.25 million persons.
• ~5000 persons die/yr. from HBV-related cirrhosis.

Prevention & Treatment
• “Advisory Committee on Immunization Practices (ACIP) recommends that all children receive their first dose of hepatitis B vaccine at birth and complete the vaccine series by age 6–18 months” (CDC)
– Adults where deficient
• Acute Infection– no medication is available; treatment is supportive
• Chronic Infection– several antiviral drug – require regular monitoring to determine whether
disease is progressing and to identify liver damage or hepatocellular carcinoma.

HEPATITIS B IN BLOOD
• SURVIVAL OUTSIDE THE BODY– In dry blood the virus can survive for up to 10 days
• QUANTITY OF VIRUS IN BLOOD– 1 mL of blood contains 100,000,000 particles of virus
• RISK OF INFECTION FOLLOWING NEEDLE STICK INJURY– Very High - 30% - 3 people in 10
• RISK OF INFECTION FOLLOWING EYE SPLASH– High.
* Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recommendations and Reports, June 29, 2001 / 50(RRll);1-42. Centers for Disease Control and Prevention

Occupational Exposure

• means reasonably anticipated skin, eye, mucous membrane, or parenteral (piercing of the skin) contact with blood or OPIM that may result from the performance of an employee's duties
Occupational Exposure
Transmission of BBPs
• is a specific contact with blood or OPIM that is capable of transmitting a bloodborne disease
Exposure Incident

Most Common Occupational Exposure
Needlestick Injuries
Over 85% of documented occupational transmissions
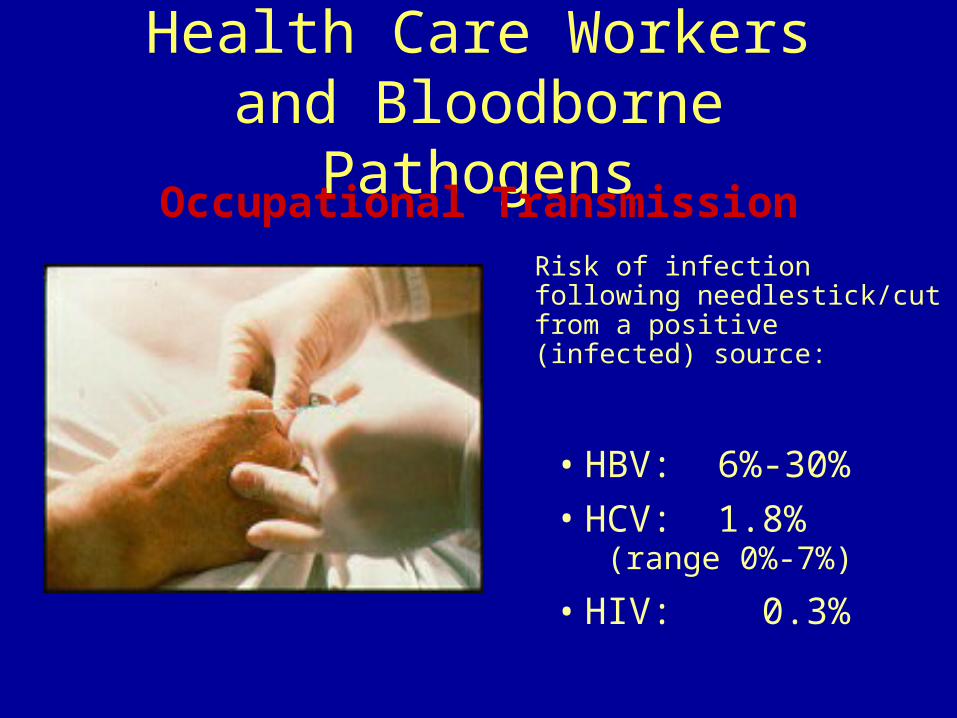
Health Care Workers and Bloodborne Pathogens
• HBV: 6%-30%
• HCV: 1.8% (range 0%-7%)
• HIV: 0.3%
Occupational Transmission
Risk of infection following needlestick/cut from a positive (infected) source:

Transmission of BBPs
Risk of infection depends on several factors:
The pathogen involved The type/route of exposure The amount of virus in the
infected blood at the time of exposure
The amount of infected blood involved in the exposure
Whether post-exposure treatment was taken
Specific immune response of the infected individual
Courtesy of Owen Mumford, Inc.

Health Care Workers and BBPs
• Most common: needlesticks
• Cuts from other contaminated sharps (scalpels, broken glass, etc.)
• Contact of mucous membranes (eye, nose, mouth) or broken (cut or abraded) skin with contaminated blood
Occupational TransmissionCauses of percutaneous injuries with hollow-
bore needles, by % total percutaneous injuries
Manipulating needle in patients
27%
IV line-related causes
8%
Handling or passing device
during or after use
10%
Recapping
5%
Clean-up
11%
Collision w/health
care worker or sharp
8%
Disposal-related causes
12%
Improperly disposed
sharp10%
Handling/transferring specimens
5%
Other4%
Source: CDC [1999]
Exposure Controls
• Universal precautions (or equivalent system*)
• Equipment and Safer Medical Devices
• Work practices
• Personal protective equipment
• Housekeeping
• Laundry handling
• Hazard communication- labeling
• Regulated Waste

Occupational Exposure Protection

Exposure Controls
Protected position
Unprotected position

Universal Precautions
• A system of infection control in
which all human blood and OPIM
are treated as if known to be
infectious with a bloodborne
disease.















