9/22/2017 1 Blue Ain’t Your Color: MDD Management in the Primary Care Setting Cole Larsen, PharmD, PhC, BCPS Pharmacist Clinician University of New Mexico Hospitals October 8, 2017 Objectives Describe the incidence and costs associated with depression Discuss screening methods and diagnosis for depression Select an appropriate first-line therapy for a patient with depression based on reported symptoms and patient comorbidities Provide pharmacologic recommendations for patients with suboptimal responses to initial therapy Describe opportunities for pharmacists to assist in depression management
Transcript
9/22/2017
1
Blue Ain’t Your Color: MDD Management in the Primary Care Setting
Cole Larsen, PharmD, PhC, BCPSPharmacist ClinicianUniversity of New Mexico HospitalsOctober 8, 2017
Objectives
Describe the incidence and costs associated with depression Discuss screening methods and diagnosis for depression Select an appropriate first-line therapy for a patient with depression
based on reported symptoms and patient comorbidities Provide pharmacologic recommendations for patients with
suboptimal responses to initial therapy Describe opportunities for pharmacists to assist in depression
management
9/22/2017
2
Where Do You Practice?
A. Ambulatory CareB. Inpatient PharmacyC. Hospital floor pharmacistD. RetailE. Other?
Background
9/22/2017
3
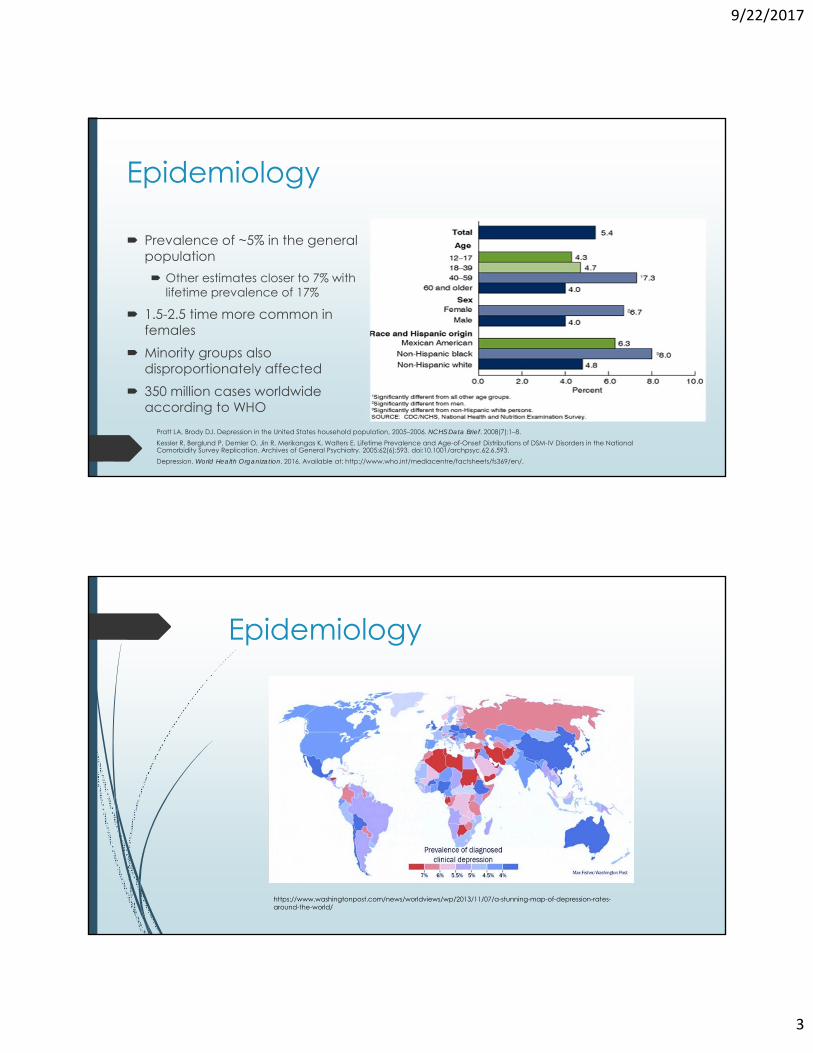
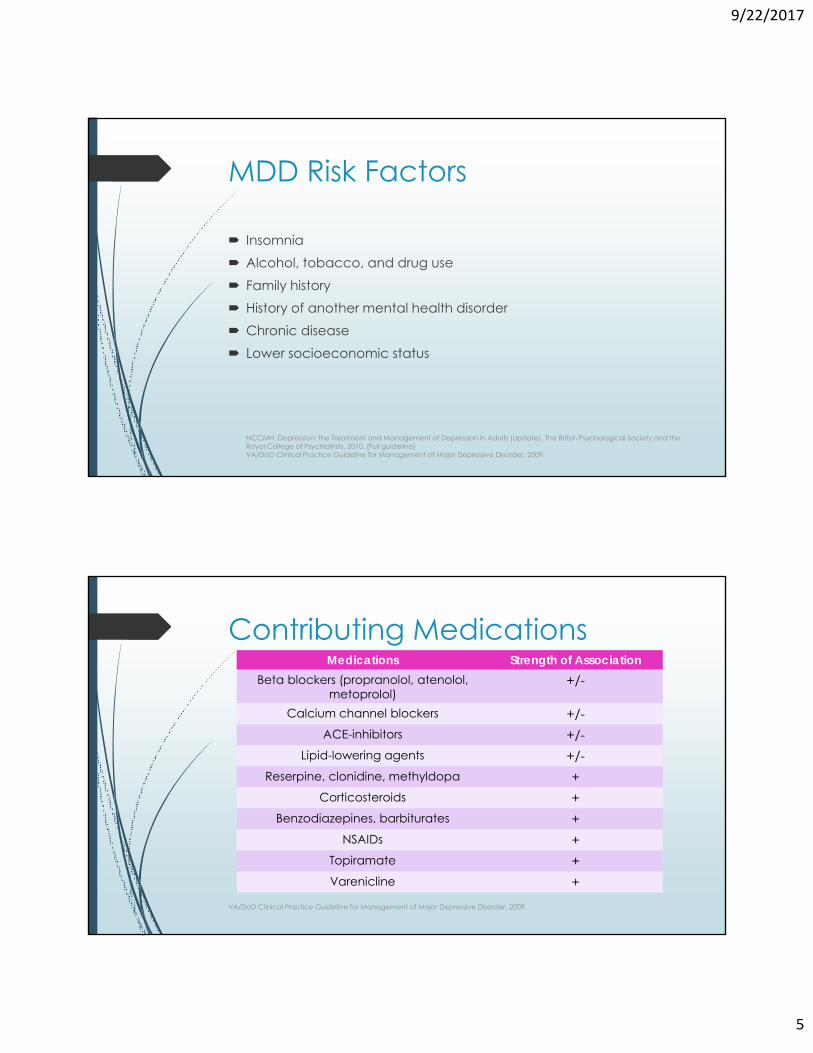
Epidemiology
Prevalence of ~5% in the general population Other estimates closer to 7% with
lifetime prevalence of 17%
1.5-2.5 time more common in females
Minority groups also disproportionately affected
350 million cases worldwide according to WHO
Pratt LA, Brody DJ. Depression in the United States household population, 2005–2006. NCHS Data Brief. 2008(7):1–8.Kessler R, Berglund P, Demler O, Jin R, Merikangas K, Walters E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry. 2005;62(6):593. doi:10.1001/archpsyc.62.6.593.Depression. World Health Organization. 2016. Available at: http://www.who.int/mediacentre/factsheets/fs369/en/.
Poor concentration and decreased functionality Significant economic costs
Lost employment and productivity 23 times greater than direct costs to healthcare system
Those with depression 3X more likely to miss work
Decreased productivity while at work
Feelings of isolation from others Negative effects on relationships Suicide
Risk is quadrupled in Major Depressive Disorder (MDD) population
NCCMH. Depression: the Treatment and Management of Depression in Adults (Update). The British Psychological Society and the Royal College of Psychiatrists. 2010. [Full guideline]
>41,000completed
suicidesper year
9.3 million reported suicidal
thoughts in the past year
10th leading cause of death in
the U.S
3rd leading cause of death for
ages 15-24Males
account for 78% of all suicides
SuicideThe Ultimate Cost of Depression
Centers for Disease Control and Prevention (CDC). Web-based Injury Statistics Query and Reporting System (WISQARS) [Online]. (2013, 2011) National Center for Injury Prevention and Control, CDC (producer). Available from http://www.cdc.gov/injury/wisqars/index.html.
9/22/2017
5
MDD Risk Factors
Insomnia Alcohol, tobacco, and drug use Family history History of another mental health disorder Chronic disease Lower socioeconomic status
NCCMH. Depression: the Treatment and Management of Depression in Adults (Update). The British Psychological Society and the Royal College of Psychiatrists. 2010. [Full guideline] VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
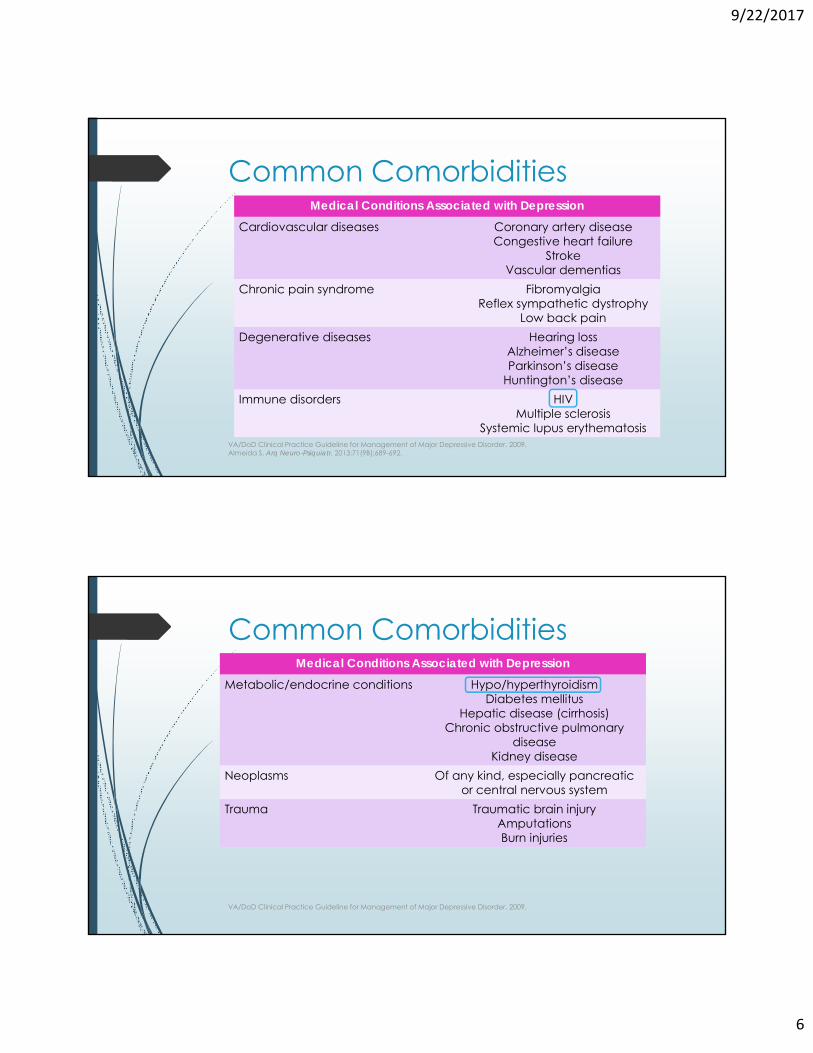
Contributing Medications
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
Medications Strength of AssociationBeta blockers (propranolol, atenolol,
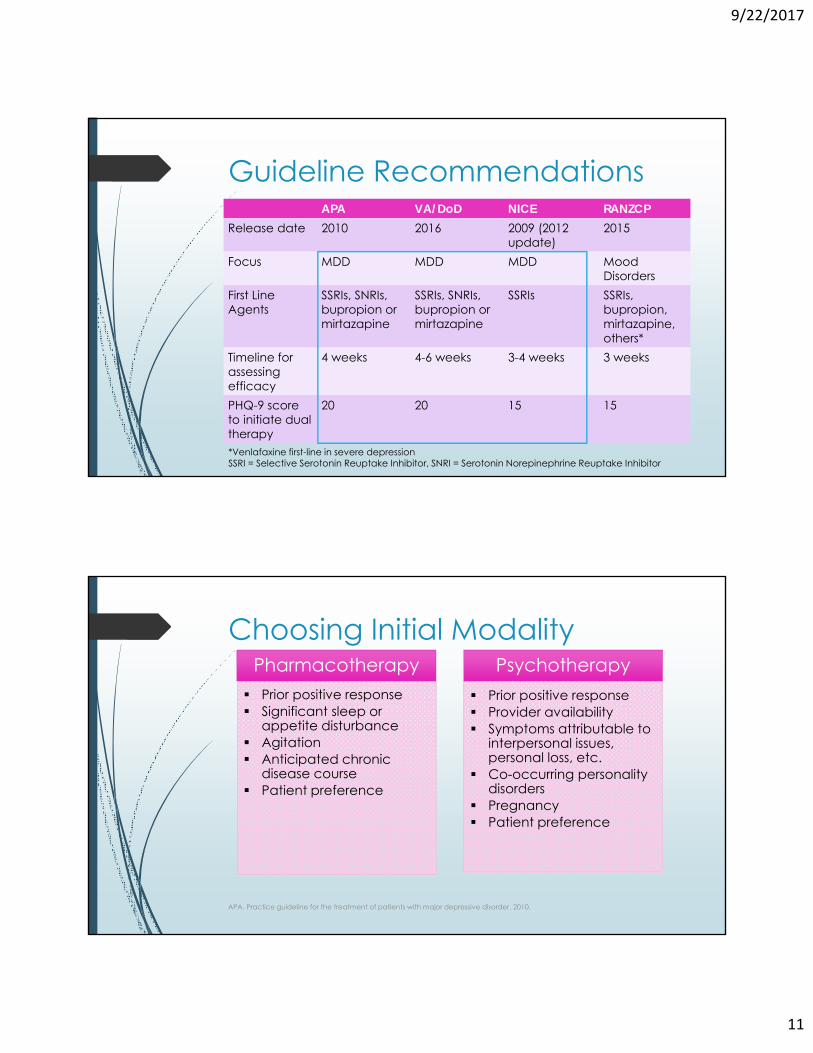
Psychotherapy Prior positive response Provider availability Symptoms attributable to
interpersonal issues, personal loss, etc.
Co-occurring personality disorders
Pregnancy Patient preference
9/22/2017
12
Agent selection
All antidepressants are considered equally efficacious
Use patient-specific factors to choose agent based on: Side effect profile Medical and psychiatric comorbidities Drug interactions Prior response Response for family members
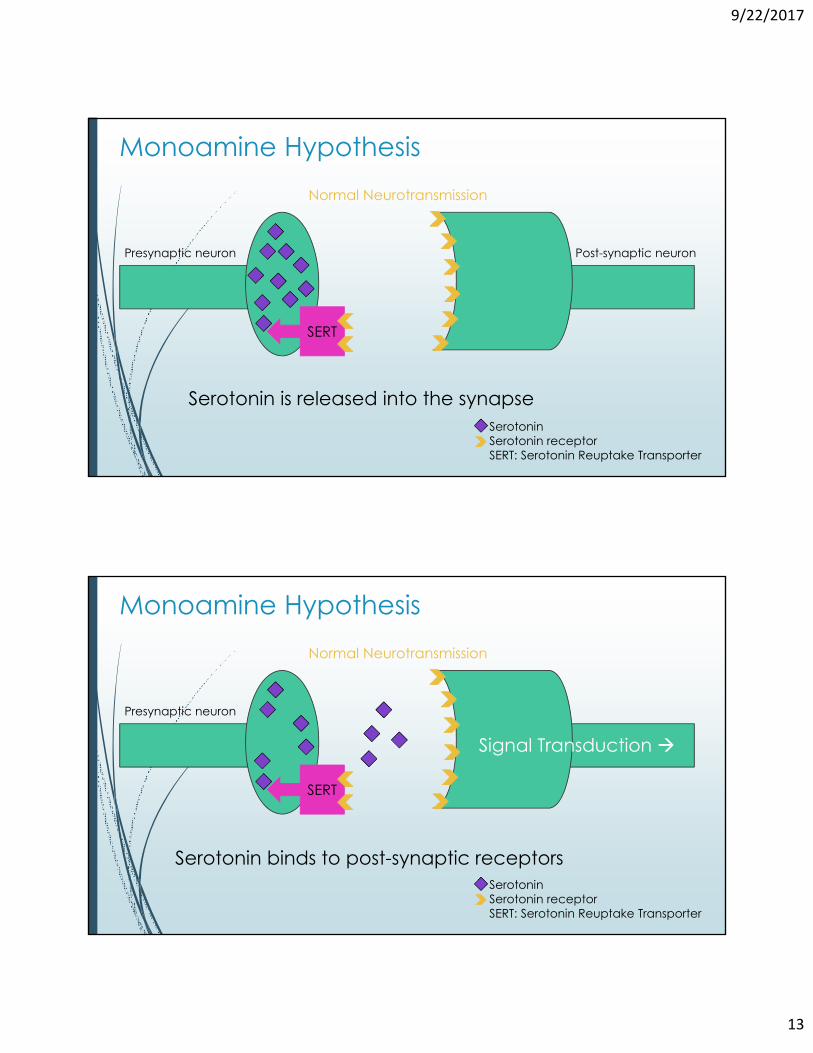
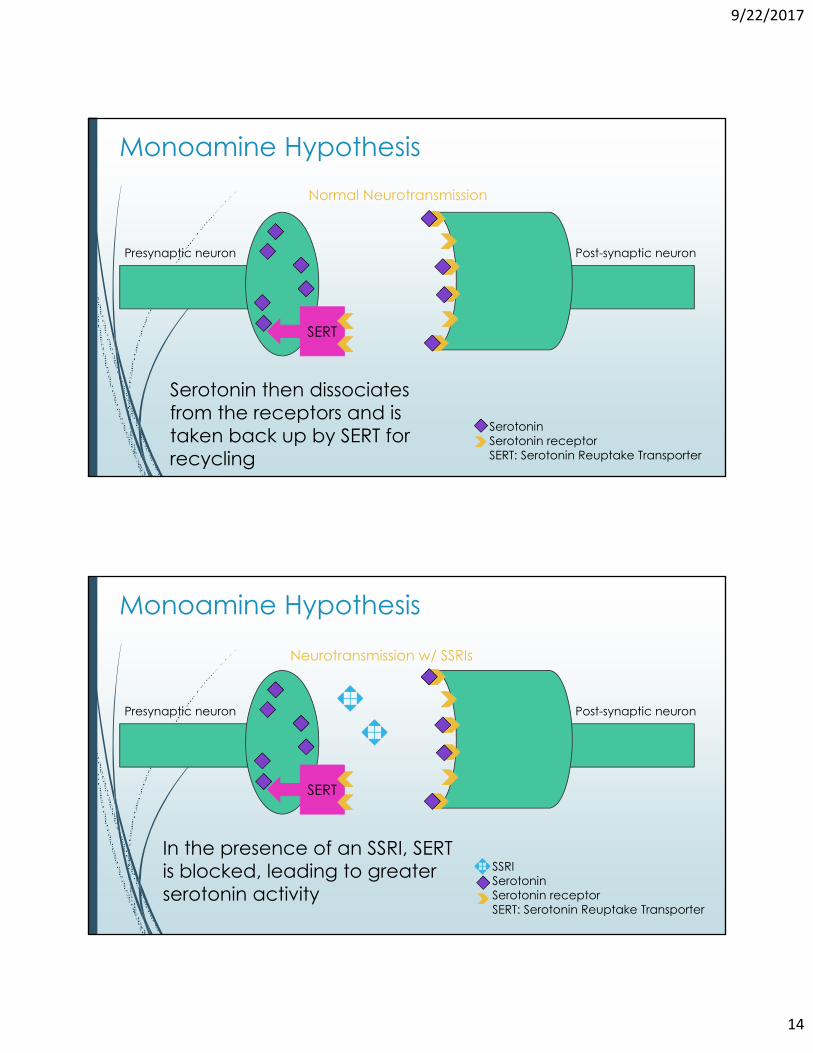
In the presence of an SSRI, SERT is blocked, leading to greater serotonin activity
Signal Transduction
Neurotransmission w/ SSRIs
Presynaptic neuron Post-synaptic neuron
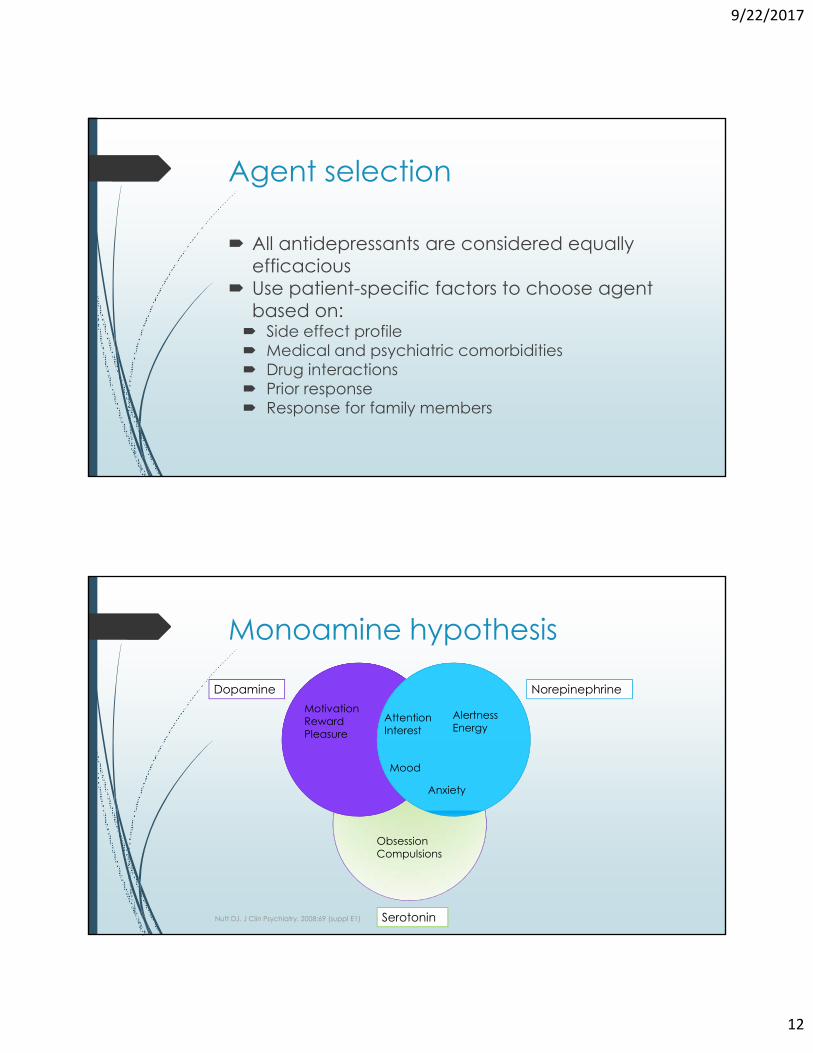
Monoamine Hypothesis
Pharmacotherapy Options
9/22/2017
16
SSRIs
Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
•Concern for QTc prolongation•More sedating due to antihistaminergic activity
Citalopram (Celexa)Citalopram (Celexa)
•“Purest” SSRI •Less cardiotoxicity•Fewest drug interactions
Escitalopram (Lexapro)Escitalopram (Lexapro)
QTc Prolongation Recommendations Concern for Torsades de pointes if QTc >500 milliseconds Ensure potassium and magnesium levels are within the normal range Perform ECG prior to initiating citalopram if any of the following present:
Congestive heart failure
Bradyarrhythmias
Concomitant QTc-prolonging agentsCrediblemeds.org
VHA PBM Bulletin. Updated Guidance: Citalopram hydrobromide and dose-dependent QT interval prolongation. September 29, 2011.
9/22/2017
17
SSRIs
Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
•May be more activating•No tapering required due to long half-life
Fluoxetine (Prozac)Fluoxetine (Prozac)
•Not officially labeled for MDD•Only approved for OCD, off-label use in
eating disorders•Multiple drug interactions
Fluvoxamine (Luvox)Fluvoxamine (Luvox)
SSRIs
Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
•Anticholinergic activity•Only SSRI that requires renal dose adjustments•Worst discontinuation symptoms
Paroxetine (Paxil) Paroxetine (Paxil)
•Weak dopamine reuptake inhibition believed to enhance activity
Sertraline (Zoloft)Sertraline (Zoloft)
9/22/2017
18
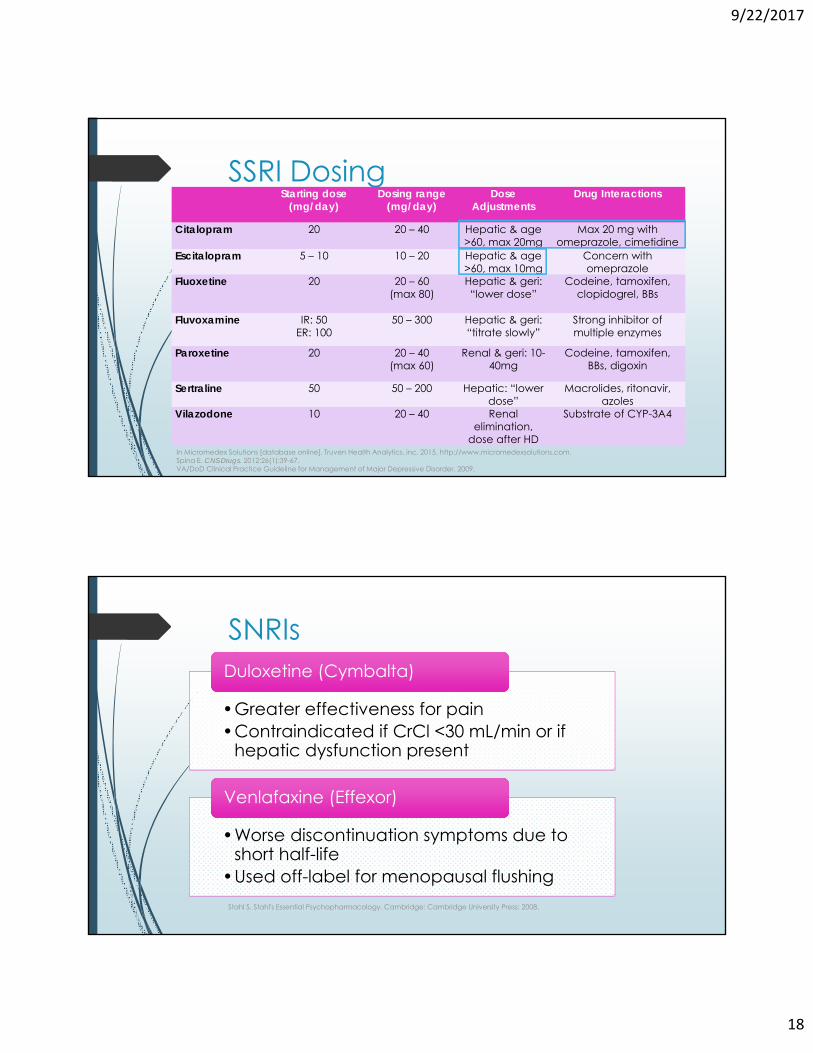
SSRI Dosing Starting dose
(mg/day)Dosing range
(mg/day)Dose
AdjustmentsDrug Interactions
Citalopram 20 20 – 40 Hepatic & age >60, max 20mg
Max 20 mg with omeprazole, cimetidine
Escitalopram 5 – 10 10 – 20 Hepatic & age >60, max 10mg
Concern with omeprazole
Fluoxetine 20 20 – 60(max 80)
Hepatic & geri: “lower dose”
Codeine, tamoxifen,clopidogrel, BBs
Fluvoxamine IR: 50 ER: 100
50 – 300 Hepatic & geri: “titrate slowly”
Strong inhibitor of multiple enzymes
Paroxetine 20 20 – 40(max 60)
Renal & geri: 10-40mg
Codeine, tamoxifen,BBs, digoxin
Sertraline 50 50 – 200 Hepatic: “lower dose”
Macrolides, ritonavir, azoles
Vilazodone 10 20 – 40 Renalelimination,
dose after HD
Substrate of CYP-3A4
In Micromedex Solutions [database online]. Truven Health Analytics, inc. 2015. http://www.micromedexsolutions.com. Spina E. CNS Drugs. 2012;26(1):39-67. VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
SNRIs
Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
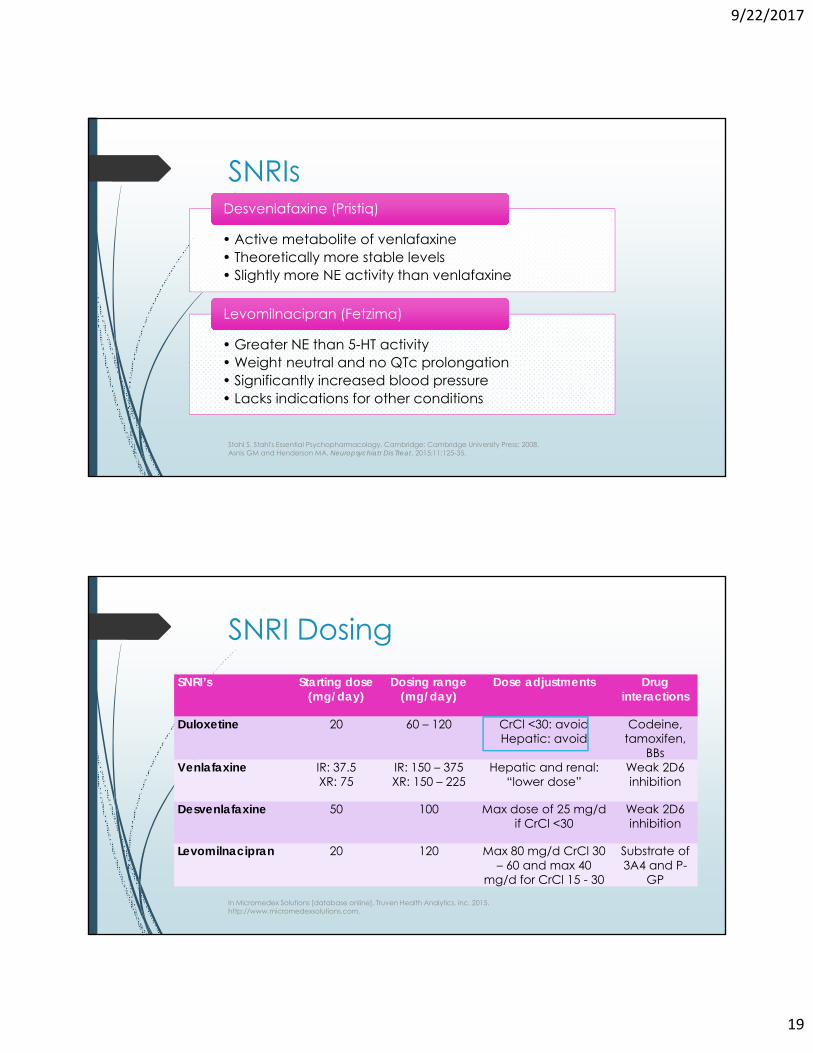
•Greater effectiveness for pain•Contraindicated if CrCl <30 mL/min or if
hepatic dysfunction present
Duloxetine (Cymbalta)Duloxetine (Cymbalta)
•Worse discontinuation symptoms due to short half-life
•Used off-label for menopausal flushing
Venlafaxine (Effexor)Venlafaxine (Effexor)
9/22/2017
19
SNRIs
Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.Asnis GM and Henderson MA. Neuropsychiatr Dis Treat. 2015;11:125-35.
• Active metabolite of venlafaxine• Theoretically more stable levels• Slightly more NE activity than venlafaxine
Desvenlafaxine (Pristiq)Desvenlafaxine (Pristiq)
• Greater NE than 5-HT activity• Weight neutral and no QTc prolongation• Significantly increased blood pressure• Lacks indications for other conditions
Desvenlafaxine 50 100 Max dose of 25 mg/d if CrCl <30
Weak 2D6 inhibition
Levomilnacipran 20 120 Max 80 mg/d CrCl 30 – 60 and max 40
mg/d for CrCl 15 - 30
Substrate of 3A4 and P-
GP
In Micromedex Solutions [database online]. Truven Health Analytics, inc. 2015. http://www.micromedexsolutions.com.
9/22/2017
20
Mixed Activity SERTs
Boulenger et al. International Clinical Psychopharmacology. 2014. 29:138-149. Grant JE et al. 2017 May;32(3):121-126.Wang et al. Chonnam Med J. 2016. 52:91-100.Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
• 5-HT1A Partial Agonist and Reuptake Inhibitor (SPARI)• Proposed benefits of faster onset, less sexual side
effects and greater efficacy*• Primary side effect of GI upset
Vilazodone (Viibryd)Vilazodone (Viibryd)
Mixed Activity SERTs
Kostrubsky SEet al. Inhibition of hepatobiliary transport as a predictive method for clinical hepatotoxicity of nefazodone. Toxicol Sci 2006; 90: 451-9)Stahl S. Stahl's Essential Psychopharmacology. Cambridge: Cambridge University Press; 2008.
• 5-HT2A antagonist/reuptake inhibitor (SARI)• Less potently inhibits NE reuptake
• Use severely limited due to hepatotoxicity• Less sedating than trazodone
Nefazodone (Serzone)Nefazodone (Serzone)
• Use limited by sedation
TrazodoneTrazodone
9/22/2017
21
Mixed Activity SERTsStarting dose
(mg/day)Dosing range
(mg/day)Dose
AdjustmentsDrug Interactions
Vortioxetine
Vilazodone 10 20 – 40 Renalelimination,
dose after HD
Substrate of CYP-3A4
Nefazodone
Trazodone
In Micromedex Solutions [database online]. Truven Health Analytics, inc. 2015. http://www.micromedexsolutions.com. Spina E. CNS Drugs. 2012;26(1):39-67. VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
Comparative Data
Citrome L. Journal of Affective Disorders. 2016. 196:225-233.
4.3 4.6 1.8 1.2 1.4 3.3 5.1
9/22/2017
22
Tolerability
Common adverse effects include headache, GI upset, dry mouth, agitation, insomnia, sexual dysfunction, diaphoresis, and weight gain
SNRIs also pose risk of hypertension, tremor and tachyarrhythmia's Other risks
Bleeding
Hyponatremia
Osteoporosis (elderly)
Moret C et al. Journal of Psychopharmacology. 2009;23: 967–974.
Serotonin Syndrome
Rare but serious Counsel patients to discontinue medication and seek care if
Diaphoresis, delirium, agitation, muscle rigidity, clonus, or mydriasis
Higher risk in patients with multiple serotonergic agents Linezolid, tramadol, valproate, triptans, dextromethorphan, L-
tryptophan and other antidepressants (especially MAOIs)
Management largely supportive Cyproheptadine considered treatment of choice
Benzodiazepines for agitation/clonus
Boyer E, Shannon M. New England Journal of Medicine. 2005;352(11):1112-1120.
9/22/2017
23
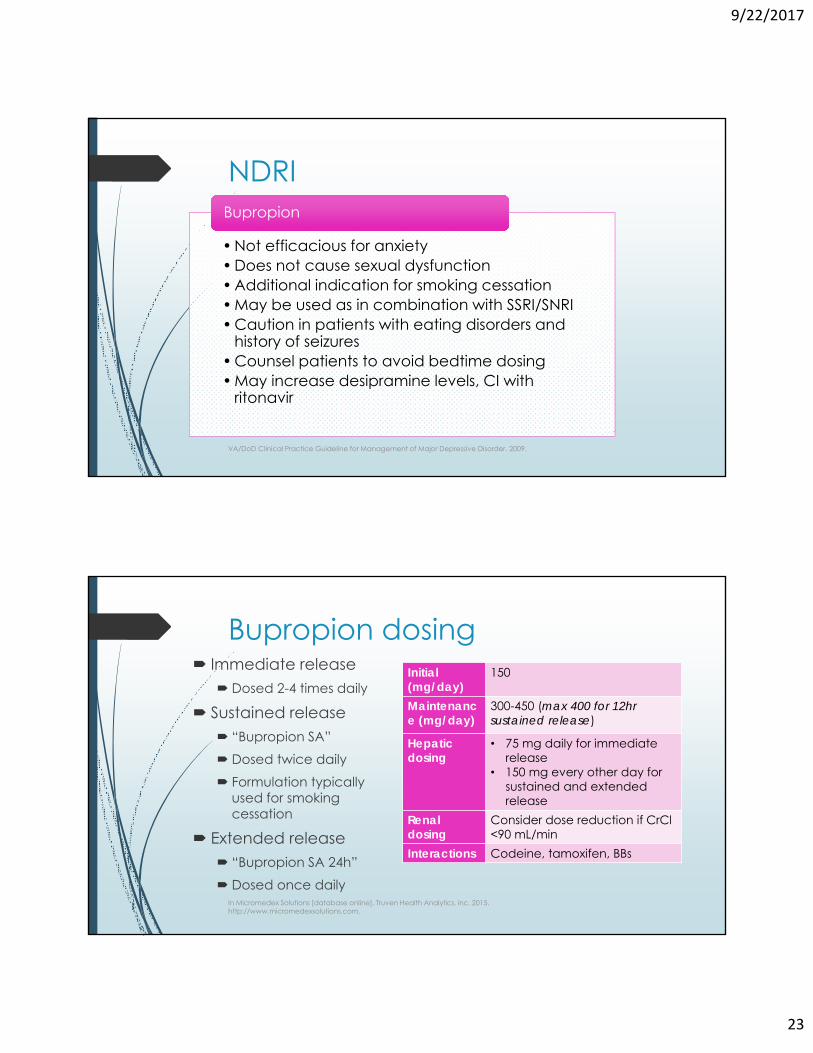
NDRI
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
• Not efficacious for anxiety• Does not cause sexual dysfunction• Additional indication for smoking cessation• May be used as in combination with SSRI/SNRI• Caution in patients with eating disorders and
history of seizures• Counsel patients to avoid bedtime dosing• May increase desipramine levels, CI with
ritonavir
BupropionBupropion
Bupropion dosing Immediate release
Dosed 2-4 times daily
Sustained release “Bupropion SA” Dosed twice daily Formulation typically
used for smoking cessation
Extended release “Bupropion SA 24h” Dosed once daily
In Micromedex Solutions [database online]. Truven Health Analytics, inc. 2015. http://www.micromedexsolutions.com.
Initial (mg/day)
150
Maintenance (mg/day)
300-450 (max 400 for 12hr sustained release)
Hepaticdosing
• 75 mg daily for immediate release
• 150 mg every other day for sustained and extended release
Renal dosing
Consider dose reduction if CrCl<90 mL/min
Interactions Codeine, tamoxifen, BBs
9/22/2017
24
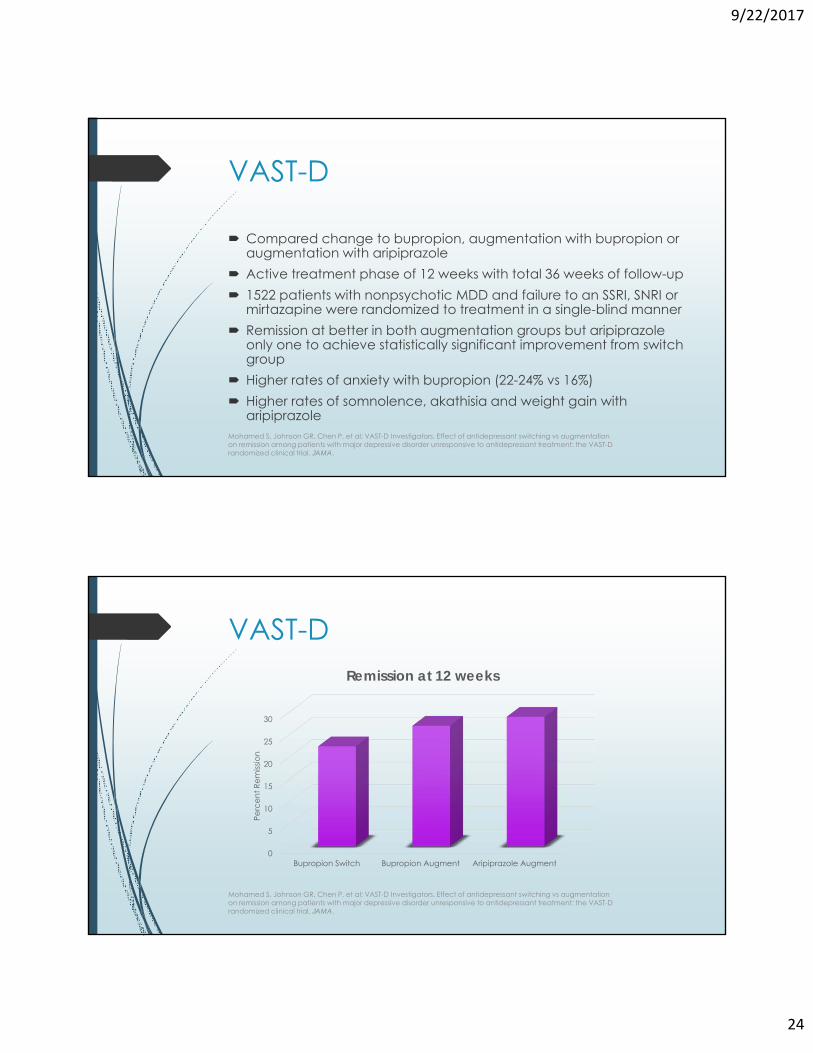
VAST-D
Compared change to bupropion, augmentation with bupropion or augmentation with aripiprazole
Active treatment phase of 12 weeks with total 36 weeks of follow-up 1522 patients with nonpsychotic MDD and failure to an SSRI, SNRI or
mirtazapine were randomized to treatment in a single-blind manner Remission at better in both augmentation groups but aripiprazole
only one to achieve statistically significant improvement from switch group
Higher rates of anxiety with bupropion (22-24% vs 16%) Higher rates of somnolence, akathisia and weight gain with
aripiprazoleMohamed S, Johnson GR, Chen P, et al; VAST-D Investigators. Effect of antidepressant switching vs augmentation on remission among patients with major depressive disorder unresponsive to antidepressant treatment: the VAST-D randomized clinical trial. JAMA.
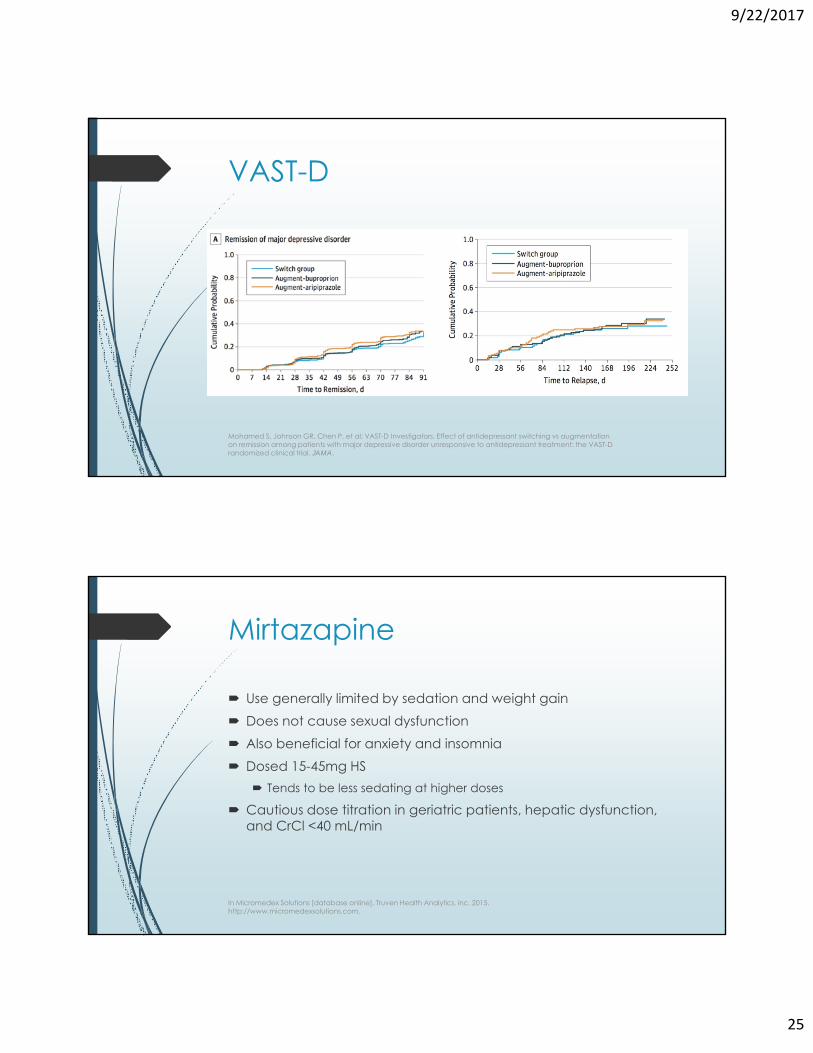
VAST-D
Mohamed S, Johnson GR, Chen P, et al; VAST-D Investigators. Effect of antidepressant switching vs augmentation on remission among patients with major depressive disorder unresponsive to antidepressant treatment: the VAST-D randomized clinical trial. JAMA.
Mohamed S, Johnson GR, Chen P, et al; VAST-D Investigators. Effect of antidepressant switching vs augmentation on remission among patients with major depressive disorder unresponsive to antidepressant treatment: the VAST-D randomized clinical trial. JAMA.
Mirtazapine
Use generally limited by sedation and weight gain Does not cause sexual dysfunction Also beneficial for anxiety and insomnia Dosed 15-45mg HS
Tends to be less sedating at higher doses
Cautious dose titration in geriatric patients, hepatic dysfunction, and CrCl <40 mL/min
In Micromedex Solutions [database online]. Truven Health Analytics, inc. 2015. http://www.micromedexsolutions.com.
9/22/2017
26
Discontinuation Symptoms
Divided into affective, gastrointestinal, neuromotor, vasomotor, neurosensory, and other neurological symptoms
Onset usually within 5 days of stopping antidepressant Counsel against abrupt cessation More pronounced with short-acting agents (paroxetine and
venlafaxine)
NCCMH. Depression: the Treatment and Management of Depression in Adults (Update). The British Psychological Society and the Royal College of Psychiatrists. 2010. [Full guideline]
A Word About Supplements Some benefit
St. Johns WortMultiple drug interactions
Risk of serotonin syndrome when combined with SSRIs
Omega-3 Recommend dietary modifications first
Consider if other indications for supplementation exist
Other dietary supplements possibly beneficial when used adjunctively
Sarris J. J Clin Psych. 2012;73:81-86.Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Australian & New Zealand Journal of Psychiatry. 2015;49(12):1087-1206.
9/22/2017
27
Monitoring
Setting Expectations
Most side effects should subside after the first 2 weeks Counsel to take with food to avoid GI upset
Not for PRN use Adequate trial of at least 4-6 weeks before adjusting dose
Increased activity, interest, and cognition in first 1-3 weeks
Mood elevation, return of pleasure, decreased hopeless feelings, and fewer suicidal thoughts in 2-4 weeks
60-70% of patients will respond to an initial antidepressant trial 30-40% will achieve remission
Nierenberg AA. A critical overview of the pharmacologic management of treatment-resistant depression. Psychiatric Clinics of North America. 2007;30:13–29.
9/22/2017
28
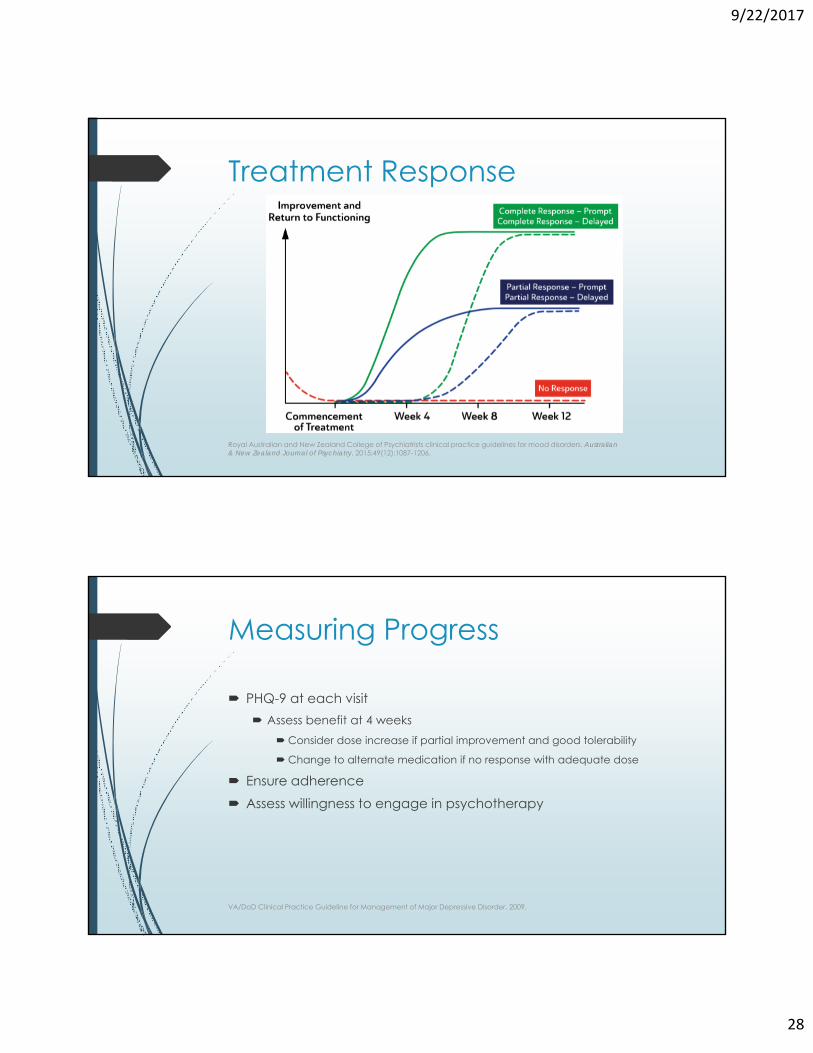
Treatment Response
Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Australian & New Zealand Journal of Psychiatry. 2015;49(12):1087-1206.
Measuring Progress
PHQ-9 at each visit Assess benefit at 4 weeks
Consider dose increase if partial improvement and good tolerability
Change to alternate medication if no response with adequate dose
Ensure adherence Assess willingness to engage in psychotherapy
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
9/22/2017
29
Measuring Progress
Mann J. New England Journal of Medicine. 2005;353(17):1819-1834.
Variable ResponseNonresponse Minimal or < 25% decrease in baseline severity of
symptomsPartial response
Reduction in severity of symptoms but symptoms still evident; 26-49% decrease in baseline severity of symptoms
Response ≥ 50% reduction in baseline severity of symptomsRemission No symptoms, return to normal functioning; PHQ-9
score of ≤ 4, maintained for at least 1 month
Recovery Extended remission, PHQ-9 score of ≤ 4, maintained for at least 6 months
Measuring Progress
Assess tolerability Sexual dysfunction
Lower dose
Adjunct with bupropion, or buspirone
Trial alternative agent
Treat with PDE-5 inhibitor
Sedation/InsomniaMove dose to alternate time of day
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder. 2009.
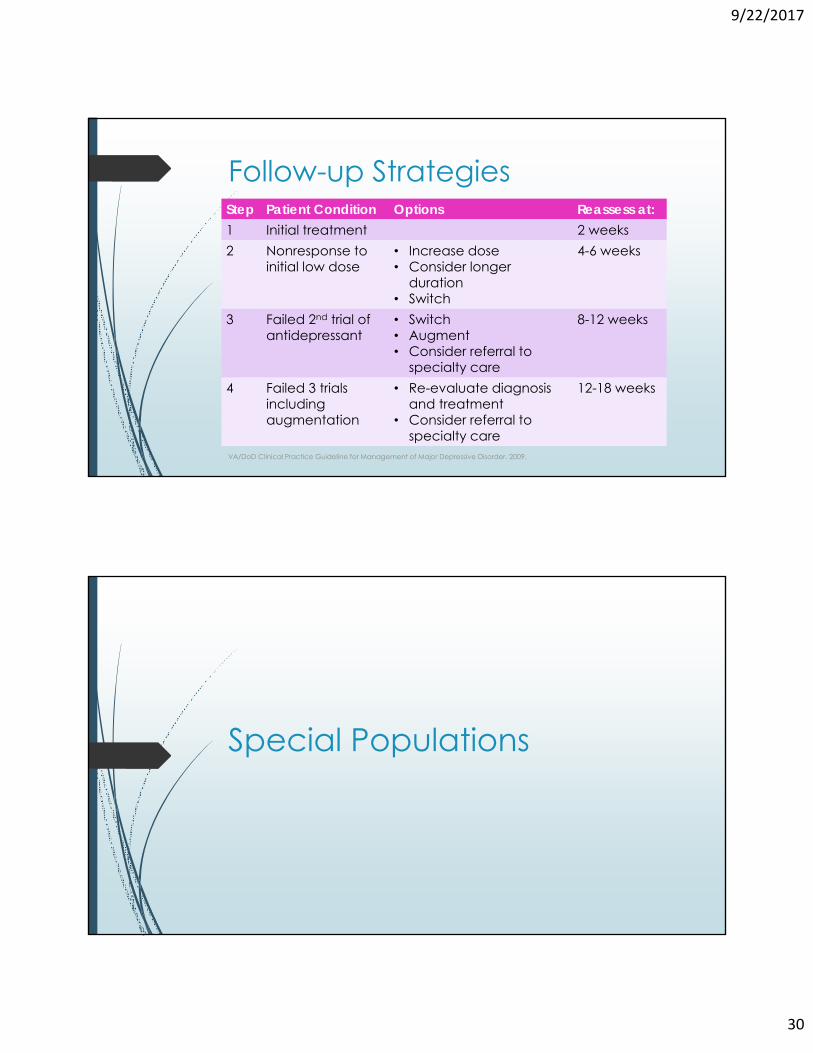
Special Populations
9/22/2017
31
Medical Co-Morbidities
Cardiovascular disease Caution with SNRIs
Avoid citalopram due to QTc prolongation
Avoid Tricyclic Antidepressants (TCAs)
Parkinson’s disease Depression present in 40-60% of patients
No evidence to suggest one agent over another
SSRIs/SNRIs may worsen tremor
APA. Practice guideline for the treatment of patients with major depressive disorder. 2010.
Medical Co-Morbidities
Seizure disorders Bupropion and TCAs lower seizure threshold No increased risk with SSRIs/SNRIs
Obesity/Diabetes Mirtazapine and TCAs can cause/contribute to weight gain SSRIs/SNRIs associated with weight gain to a lesser extent Bupropion is weight neutral and may promote modest weight loss
Traumatic Brain Injury Paroxetine and TCAs can worsen cognition via anticholinergic activity Population with lowered seizure threshold
APA. Practice guideline for the treatment of patients with major depressive disorder. 2010.
9/22/2017
32
Medical Co-Morbidities
Pain syndromes Neuropathic pain
Recommend SNRI or TCA
Migraine and tension headaches Highest quality evidence with amitryptiline, some evidence supporting SNRIs
Fibromyalgia Duloxetine (FDA approved)
Amitriptyline (off-label use)
APA. Practice guideline for the treatment of patients with major depressive disorder. 2010.
Patient-Specific Factors
Elderly patients Consider alternative to paroxetine due to anticholinergic effects
Cautious dose titration
Insomnia Consider augmenting with mirtazapine, trazodone, or hydroxyzine
Suicidality SSRIs generally least toxic in overdose
APA. Practice guideline for the treatment of patients with major depressive disorder. 2010.
9/22/2017
33
Pregnancy/Lactation
Depression rate of 10-16% Consider risk/benefit
Psychotherapy preferred for mild/moderate cases
Untreated depression is not benign (premature birth, low birth weight, postnatal complications, impaired cognitive/emotional development)
Pregnancy/lactation risk now a narrative section in package inserts Consider time of initiation and expected duration of therapy
Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Australian & New Zealand Journal of Psychiatry. 2015;49(12):1087-1206.
Pregnancy/Lactation
Paroxetine contraindicated in pregnancy Pulmonary HTN, cardiac defects, neonatal withdrawal
Venlafaxine and bupropion also associated with heart defects All other SSRIs/SNRIs previously category C Lactation
Lowest risk with fluoxetine, paroxetine, and sertraline
If pharmacotherapy selected, use lowest effective dose Sertraline preferred
O’Connor E. Primary Care Screening for and Treatment of Depression in Pregnant and Postpartum Women. JAMA. 2016;315(4):388. TOXNET. Toxnetnlmnihgov. 2016. Available at: http://toxnet.nlm.nih.gov/cgi-bin/sis/search2/d?./temp/