BlueAdvantage (PPO) SM Summary of Benefits 2018 bcbstmedicare.com BlueAdvantage Diamond (PPO) SM BlueAdvantage Ruby (PPO) SM BlueAdvantage Sapphire (PPO) SM BlueAdvantage Garnet (PPO) SM H7917_18_SB Accepted 09012017
This is a summary of drug and health services covered by BlueAdvantage (PPO) health plans January 1, 2018 - December 31, 2018.
BlueCross BlueShield of Tennessee, Inc., is a PPO plan with a Medicare contract. Enrollment in BlueCross BlueShield of Tennessee, Inc. depends on contract renewal. These plans do not require referrals to see specialists.
The benefit information provided is a summary of what we cover and what you pay. It does not list every service that we cover or list every limitation or exclusion. To get a complete list of services we cover, please request the "Evidence of Coverage" by contacting member service or access it online by visiting bcbstmedicare.com.
To join BlueAdvantage (PPO), you must be entitled to Medicare Part A, be enrolled in Medicare Part B, and live in our service area. Our service area includes the Tennessee counties listed on the next two pages organized by region.
There is more than one plan listed in this Summary of Benefits. BlueAdvantage Preferred Provider Organization (PPO) plans have a network of doctors, hospitals, pharmacies, and other providers. If you use the providers in our network, you may pay less for your covered services. But if you want to, you can use providers that are not in our network as long as they participate in Medicare.
Out-of-network/non-contracted providers are under no obligation to treat BlueAdvantageSM
members, except in emergency situations. For a decision about whether we will cover an out-of-network service, we encourage you or your provider to ask us for a preservice organization determination before you receive the service. Please call our customer service number or see your Evidence of Coverage for more information, including the cost-sharing that applies to outof-network services.
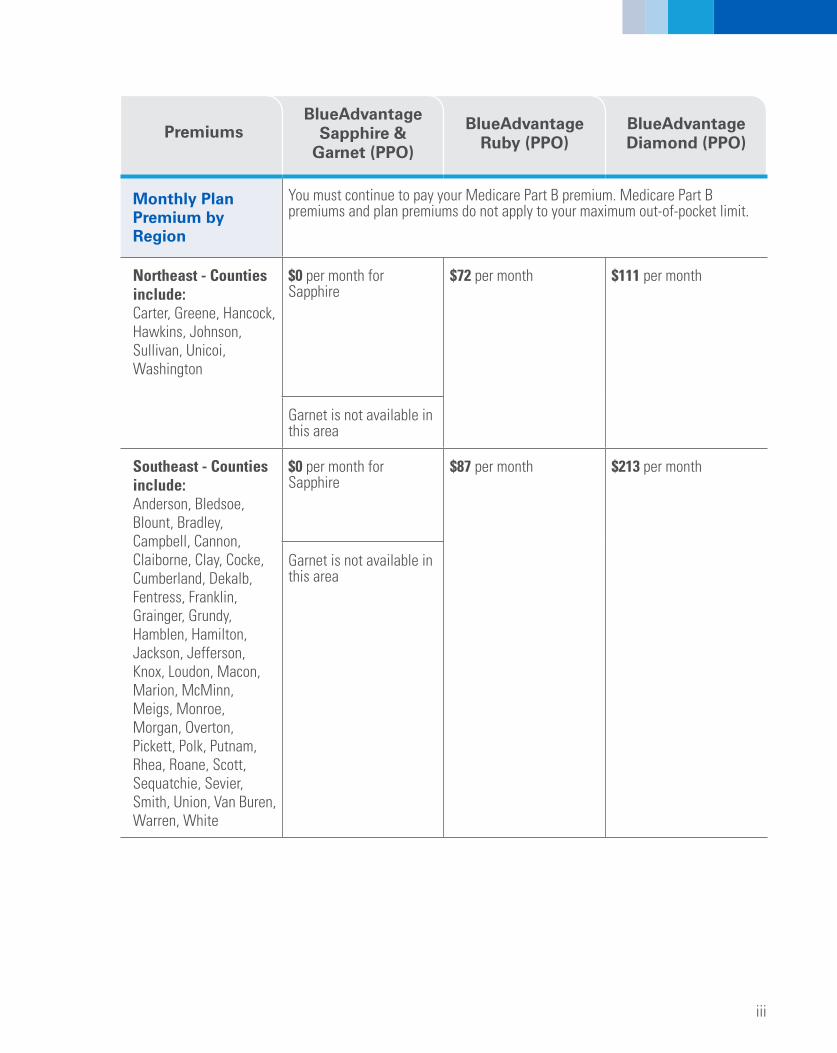
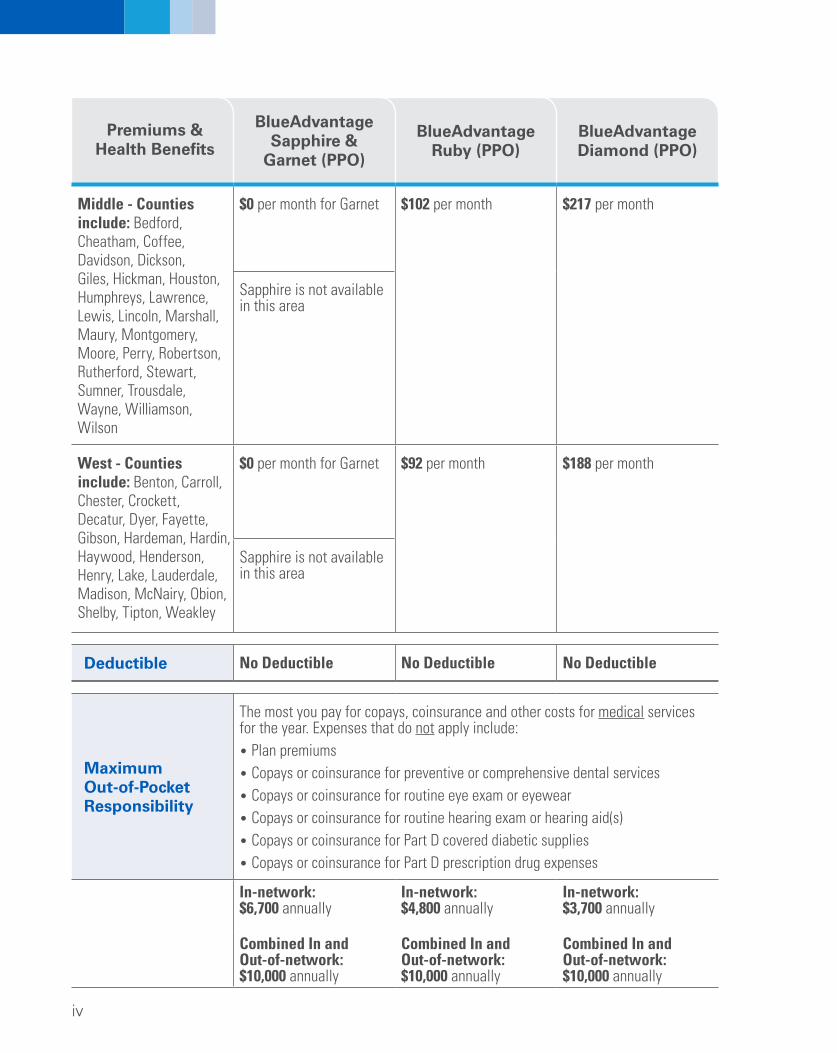
$0 per month for Garnet $92 per month $188 per month
Sapphire is not available in this area
Premiums & Health Benefits
BlueAdvantage Sapphire &
Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
Deductible No Deductible No Deductible No Deductible
Maximum Out-of-Pocket Responsibility
The most you pay for copays, coinsurance and other costs for medical services for the year. Expenses that do not apply include: • Plan premiums • Copays or coinsurance for preventive or comprehensive dental services • Copays or coinsurance for routine eye exam or eyewear • Copays or coinsurance for routine hearing exam or hearing aid(s) • Copays or coinsurance for Part D covered diabetic supplies • Copays or coinsurance for Part D prescription drug expenses
Combined In and Combined In and Combined In and Out-of-network: Out-of-network: Out-of-network: $10,000 annually $10,000 annually $10,000 annually
v
Health Benefits
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
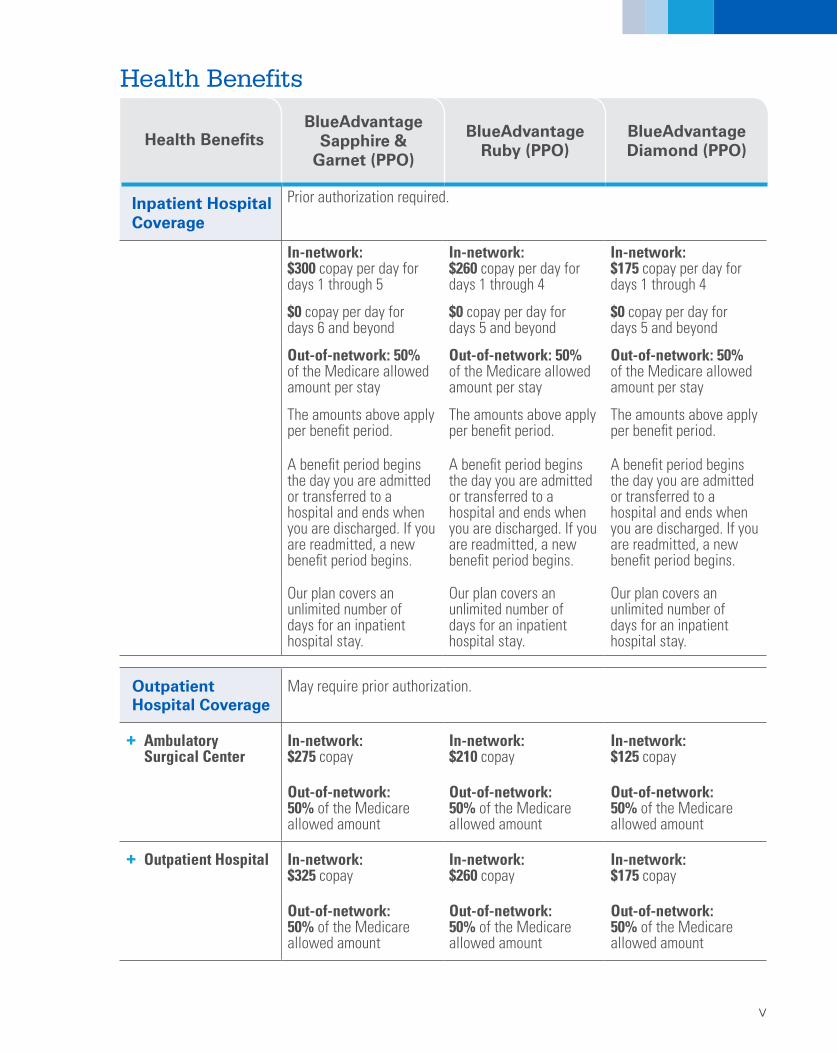
Inpatient Hospital Coverage
Prior authorization required.
In-network: $300 copay per day for days 1 through 5
$0 copay per day for days 6 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Our plan covers an unlimited number of days for an inpatient hospital stay.
In-network: $260 copay per day for days 1 through 4
$0 copay per day for days 5 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Our plan covers an unlimited number of days for an inpatient hospital stay.
In-network: $175 copay per day for days 1 through 4
$0 copay per day for days 5 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Our plan covers an unlimited number of days for an inpatient hospital stay.
Outpatient Hospital Coverage
May require prior authorization.
+ Ambulatory Surgical Center
In-network: $275 copay
In-network: $210 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: $125 copay
Out-of-network: 50% of the Medicare allowed amount
+ Outpatient Hospital In-network: $325 copay
In-network: $260 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: $175 copay
Out-of-network: 50% of the Medicare allowed amount
vi
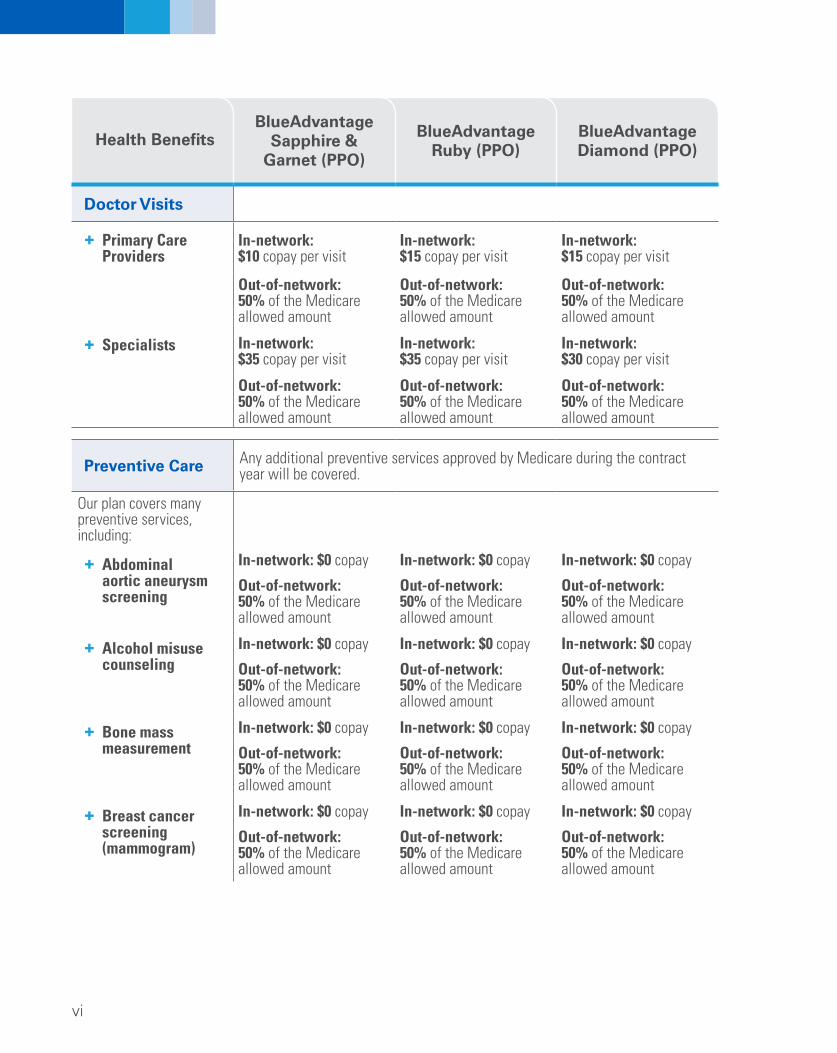
Doctor Visits
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
+ Primary Care Providers
+ Specialists
In-network: $10 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $35 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $15 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $35 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $15 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $30 copay per visit
Out-of-network: 50% of the Medicare allowed amount
Preventive Care
Our plan covers many preventive services, including:
+ Abdominal aortic aneurysm screening
+ Alcohol misuse counseling
+ Bone mass measurement
+ Breast cancer screening (mammogram)
Any additional preventive services approved by Medicare during the contract year will be covered.
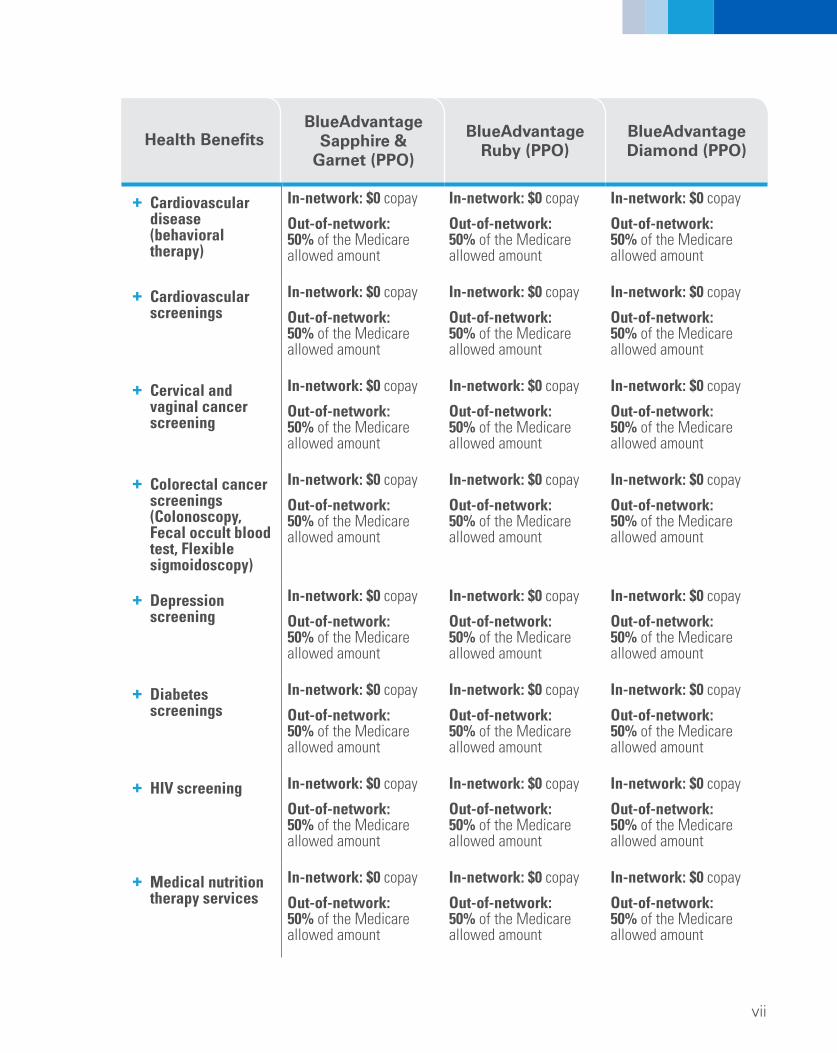
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
viii
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
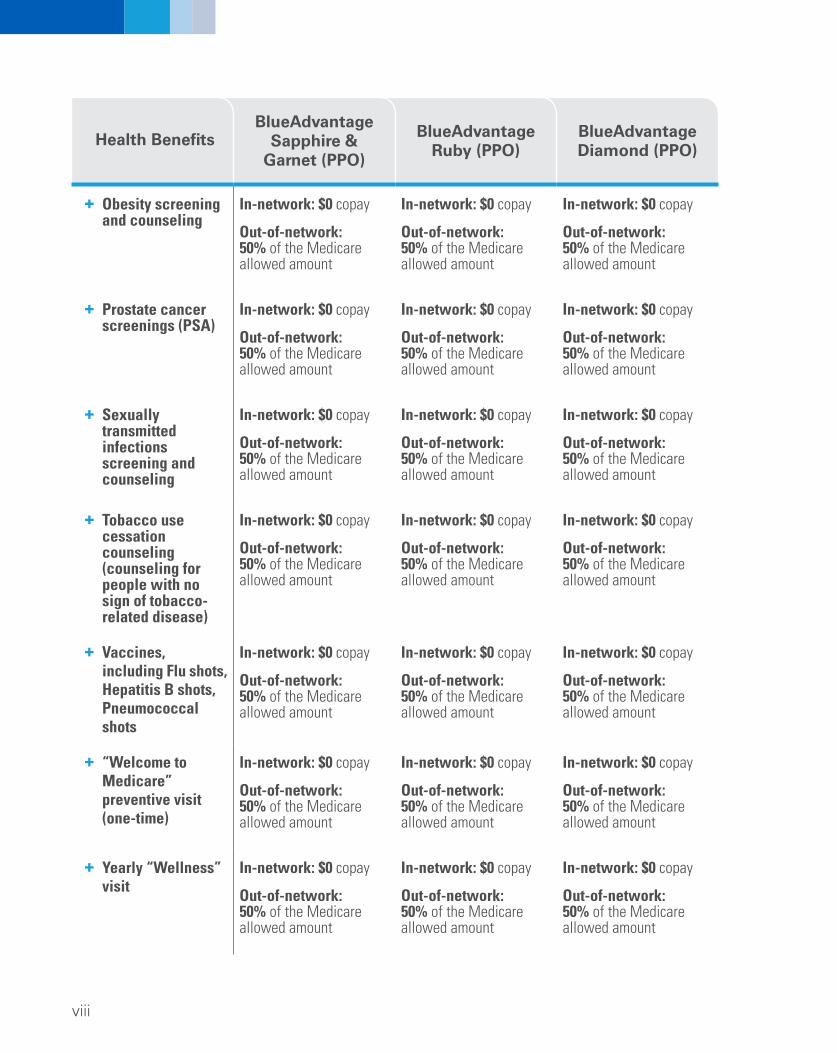
+ Obesity screening and counseling
+ Prostate cancer screenings (PSA)
+ Sexually transmitted infections screening and counseling
+ Tobacco use cessation counseling (counseling for people with no sign of tobacco-related disease)
+ Vaccines, including Flu shots, Hepatitis B shots, Pneumococcal shots
+ “Welcome to Medicare” preventive visit (one-time)
+ Yearly “Wellness” visit
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
ix
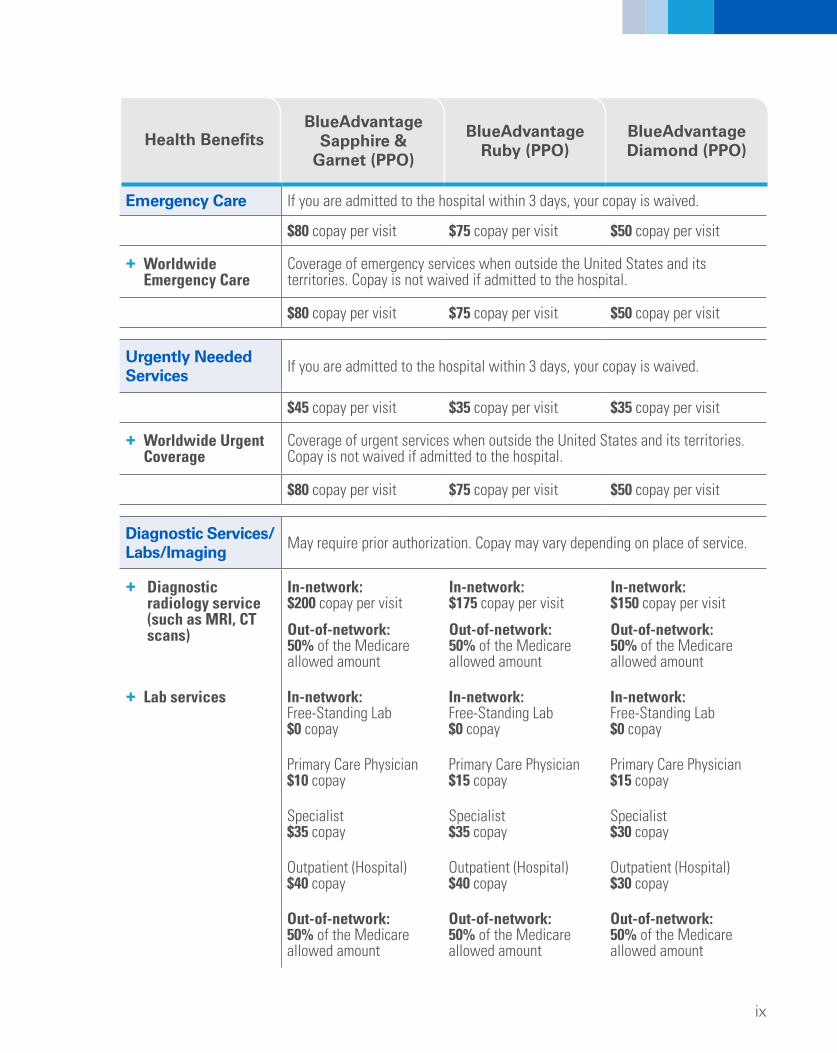
Emergency Care If you are admitted to the hospital within 3 days, your copay is waived.
$80 copay per visit $75 copay per visit $50 copay per visit
+ Worldwide Emergency Care
Coverage of emergency services when outside the United States and its territories. Copay is not waived if admitted to the hospital.
$80 copay per visit $75 copay per visit $50 copay per visit
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
Urgently Needed Services If you are admitted to the hospital within 3 days, your copay is waived.
$45 copay per visit $35 copay per visit $35 copay per visit
+ Worldwide Urgent Coverage
Coverage of urgent services when outside the United States and its territories. Copay is not waived if admitted to the hospital.
$80 copay per visit $75 copay per visit $50 copay per visit
Diagnostic Services/ Labs/Imaging
+ Diagnostic radiology service (such as MRI, CT scans)
+ Lab services
May require prior authorization. Copay may vary depending on place of service.
In-network: $200 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: Free-Standing Lab $0 copay
Primary Care Physician $10 copay
Specialist $35 copay
Outpatient (Hospital) $40 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $175 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: Free-Standing Lab $0 copay
Primary Care Physician $15 copay
Specialist $35 copay
Outpatient (Hospital) $40 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $150 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: Free-Standing Lab $0 copay
Primary Care Physician $15 copay
Specialist $30 copay
Outpatient (Hospital) $30 copay
Out-of-network: 50% of the Medicare allowed amount
x
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
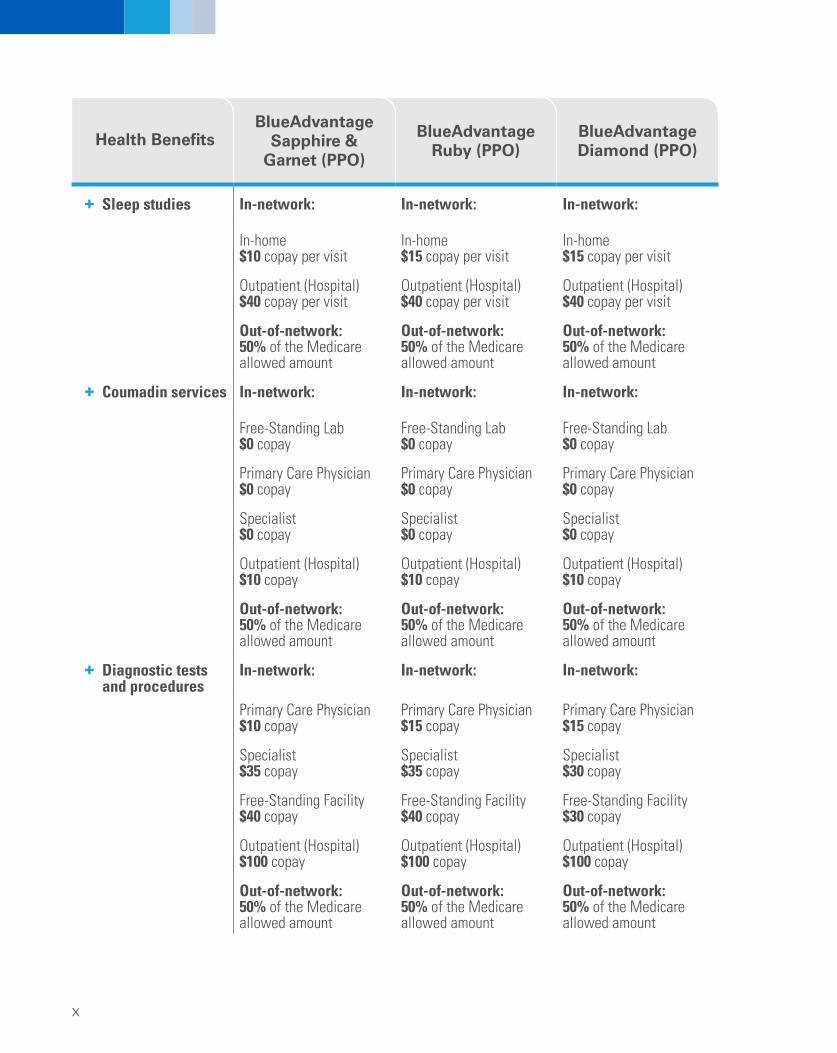
+ Sleep studies
+ Coumadin services
+ Diagnostic tests and procedures
In-network:
In-home $10 copay per visit
Outpatient (Hospital) $40 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network:
Free-Standing Lab $0 copay
Primary Care Physician $0 copay
Specialist $0 copay
Outpatient (Hospital) $10 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
Primary Care Physician $10 copay
Specialist $35 copay
Free-Standing Facility $40 copay
Outpatient (Hospital) $100 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
In-home $15 copay per visit
Outpatient (Hospital) $40 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network:
Free-Standing Lab $0 copay
Primary Care Physician $0 copay
Specialist $0 copay
Outpatient (Hospital) $10 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
Primary Care Physician $15 copay
Specialist $35 copay
Free-Standing Facility $40 copay
Outpatient (Hospital) $100 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
In-home $15 copay per visit
Outpatient (Hospital) $40 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network:
Free-Standing Lab $0 copay
Primary Care Physician $0 copay
Specialist $0 copay
Outpatient (Hospital) $10 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
Primary Care Physician $15 copay
Specialist $30 copay
Free-Standing Facility $30 copay
Outpatient (Hospital) $100 copay
Out-of-network: 50% of the Medicare allowed amount
xi
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
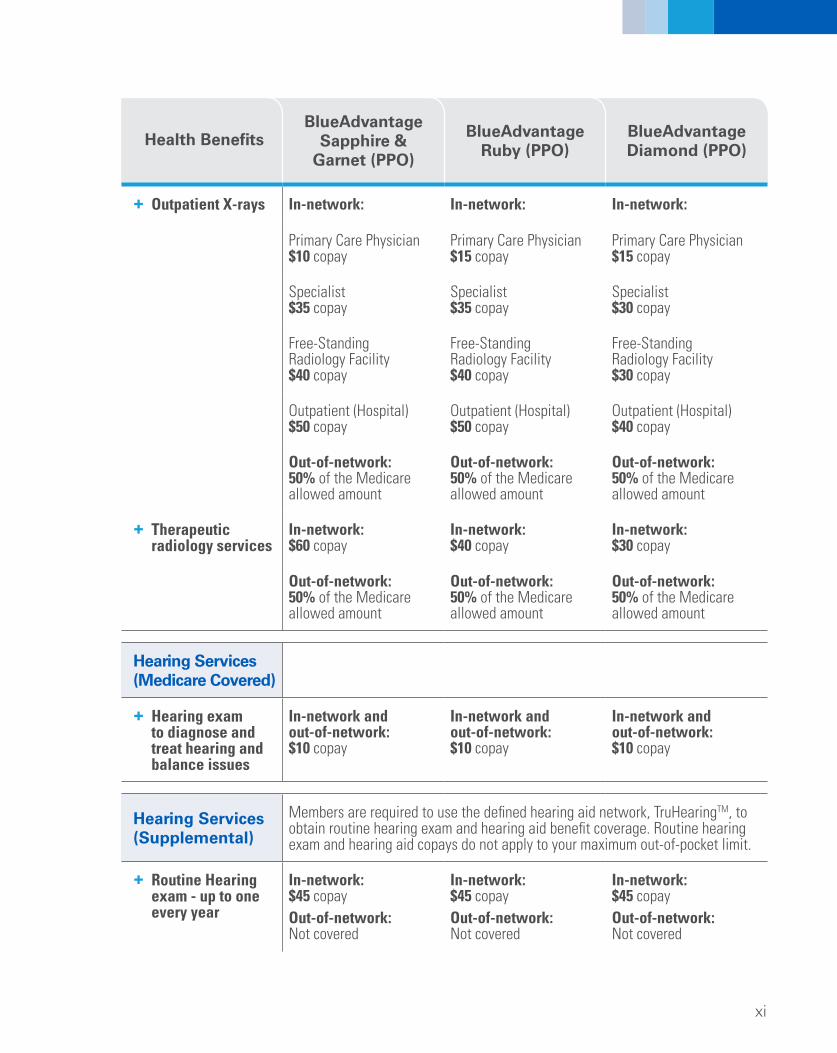
+ Outpatient X-rays
+ Therapeutic radiology services
In-network:
Primary Care Physician $10 copay
Specialist $35 copay
Free-Standing Radiology Facility $40 copay
Outpatient (Hospital) $50 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $60 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
Primary Care Physician $15 copay
Specialist $35 copay
Free-Standing Radiology Facility $40 copay
Outpatient (Hospital) $50 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $40 copay
Out-of-network: 50% of the Medicare allowed amount
In-network:
Primary Care Physician $15 copay
Specialist $30 copay
Free-Standing Radiology Facility $30 copay
Outpatient (Hospital) $40 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $30 copay
Out-of-network: 50% of the Medicare allowed amount
Hearing Services (Medicare Covered)
+ Hearing exam to diagnose and treat hearing and balance issues
In-network and out-of-network: $10 copay
In-network and out-of-network: $10 copay
In-network and out-of-network: $10 copay
Members are required to use the defined hearing aid network, TruHearingTM, to obtain routine hearing exam and hearing aid benefit coverage. Routine hearing exam and hearing aid copays do not apply to your maximum out-of-pocket limit.
In-network: In-network: In-network: $45 copay $45 copay $45 copay Out-of-network: Out-of-network: Out-of-network: Not covered Not covered Not covered
Hearing Services (Supplemental)
+ Routine Hearing exam - up to one every year
xii
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
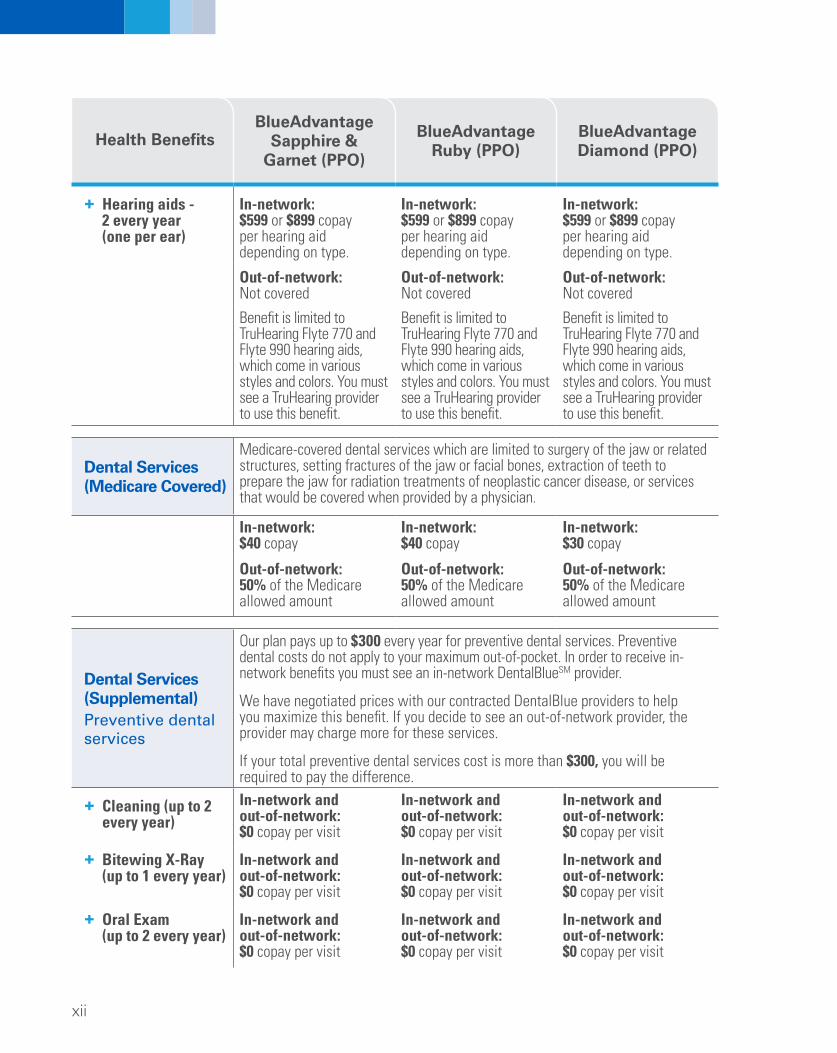
+ Hearing aids 2 every year (one per ear)
In-network: $599 or $899 copay per hearing aid depending on type.
Out-of-network: Not covered
Benefit is limited to TruHearing Flyte 770 and Flyte 990 hearing aids, which come in various styles and colors. You must see a TruHearing provider to use this benefit.
In-network: $599 or $899 copay per hearing aid depending on type.
Out-of-network: Not covered
Benefit is limited to TruHearing Flyte 770 and Flyte 990 hearing aids, which come in various styles and colors. You must see a TruHearing provider to use this benefit.
In-network: $599 or $899 copay per hearing aid depending on type.
Out-of-network: Not covered
Benefit is limited to TruHearing Flyte 770 and Flyte 990 hearing aids, which come in various styles and colors. You must see a TruHearing provider to use this benefit.
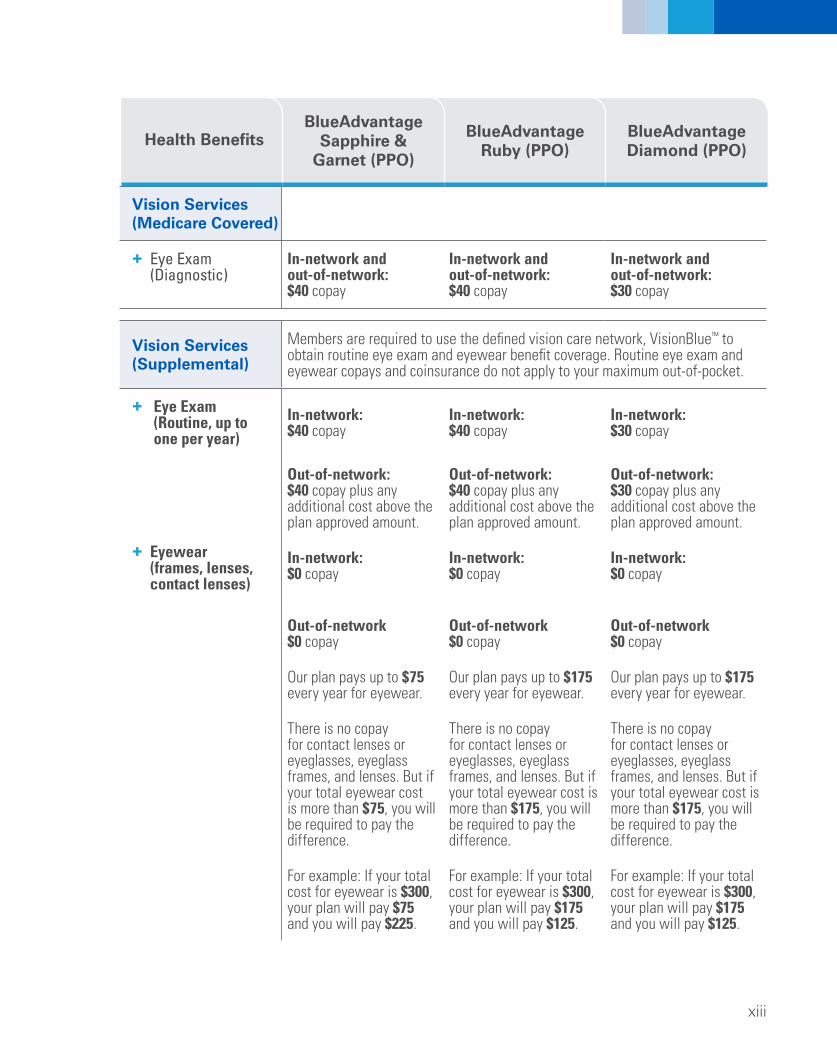
Dental Services (Medicare Covered)
Medicare-covered dental services which are limited to surgery of the jaw or related structures, setting fractures of the jaw or facial bones, extraction of teeth to prepare the jaw for radiation treatments of neoplastic cancer disease, or services that would be covered when provided by a physician.
In-network: $40 copay
In-network: $40 copay
In-network: $30 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Our plan pays up to $300 every year for preventive dental services. Preventive dental costs do not apply to your maximum out-of-pocket. In order to receive in-network benefits you must see an in-network DentalBlueSM provider.
We have negotiated prices with our contracted DentalBlue providers to help you maximize this benefit. If you decide to see an out-of-network provider, the provider may charge more for these services.
If your total preventive dental services cost is more than $300, you will be required to pay the difference. In-network and In-network and In-network and out-of-network: out-of-network: out-of-network: $0 copay per visit $0 copay per visit $0 copay per visit
In-network and In-network and In-network and out-of-network: out-of-network: out-of-network: $0 copay per visit $0 copay per visit $0 copay per visit
In-network and In-network and In-network and out-of-network: out-of-network: out-of-network: $0 copay per visit $0 copay per visit $0 copay per visit
Members are required to use the defined vision care network, VisionBlue™ to obtain routine eye exam and eyewear benefit coverage. Routine eye exam and eyewear copays and coinsurance do not apply to your maximum out-of-pocket.
In-network: $40 copay
Out-of-network: $40 copay plus any additional cost above the plan approved amount.
In-network: $0 copay
Out-of-network $0 copay
Our plan pays up to $75 every year for eyewear.
There is no copay for contact lenses or eyeglasses, eyeglass frames, and lenses. But if your total eyewear cost is more than $75, you will be required to pay the difference.
For example: If your total cost for eyewear is $300, your plan will pay $75 and you will pay $225.
In-network: $40 copay
Out-of-network: $40 copay plus any additional cost above the plan approved amount.
In-network: $0 copay
Out-of-network $0 copay
Our plan pays up to $175 every year for eyewear.
There is no copay for contact lenses or eyeglasses, eyeglass frames, and lenses. But if your total eyewear cost is more than $175, you will be required to pay the difference.
For example: If your total cost for eyewear is $300, your plan will pay $175 and you will pay $125.
In-network: $30 copay
Out-of-network: $30 copay plus any additional cost above the plan approved amount.
In-network: $0 copay
Out-of-network $0 copay
Our plan pays up to $175 every year for eyewear.
There is no copay for contact lenses or eyeglasses, eyeglass frames, and lenses. But if your total eyewear cost is more than $175, you will be required to pay the difference.
For example: If your total cost for eyewear is $300, your plan will pay $175 and you will pay $125.
xiv
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
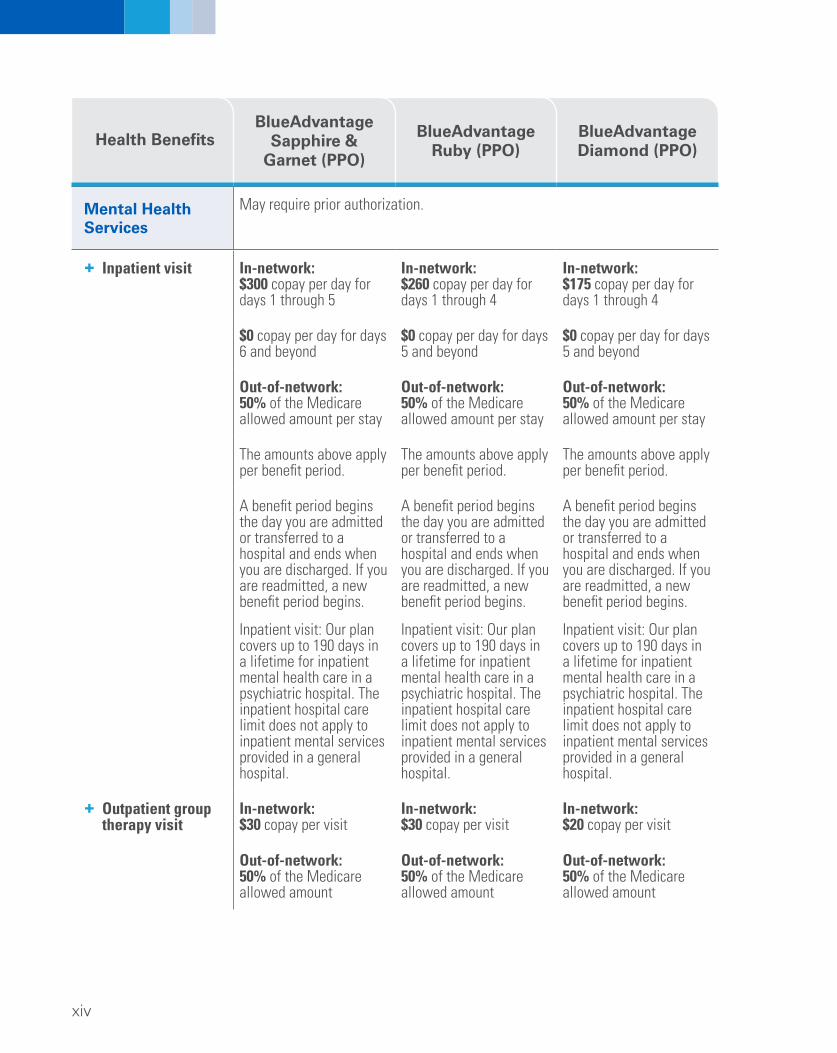
Mental Health Services
+ Inpatient visit
+ Outpatient group therapy visit
May require prior authorization.
In-network: $300 copay per day for days 1 through 5
$0 copay per day for days 6 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Inpatient visit: Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services provided in a general hospital.
In-network: $30 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $260 copay per day for days 1 through 4
$0 copay per day for days 5 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Inpatient visit: Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services provided in a general hospital.
In-network: $30 copay per visit
Out-of-network: 50% of the Medicare allowed amount
In-network: $175 copay per day for days 1 through 4
$0 copay per day for days 5 and beyond
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
A benefit period begins the day you are admitted or transferred to a hospital and ends when you are discharged. If you are readmitted, a new benefit period begins.
Inpatient visit: Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services provided in a general hospital.
In-network: $20 copay per visit
Out-of-network: 50% of the Medicare allowed amount
xv
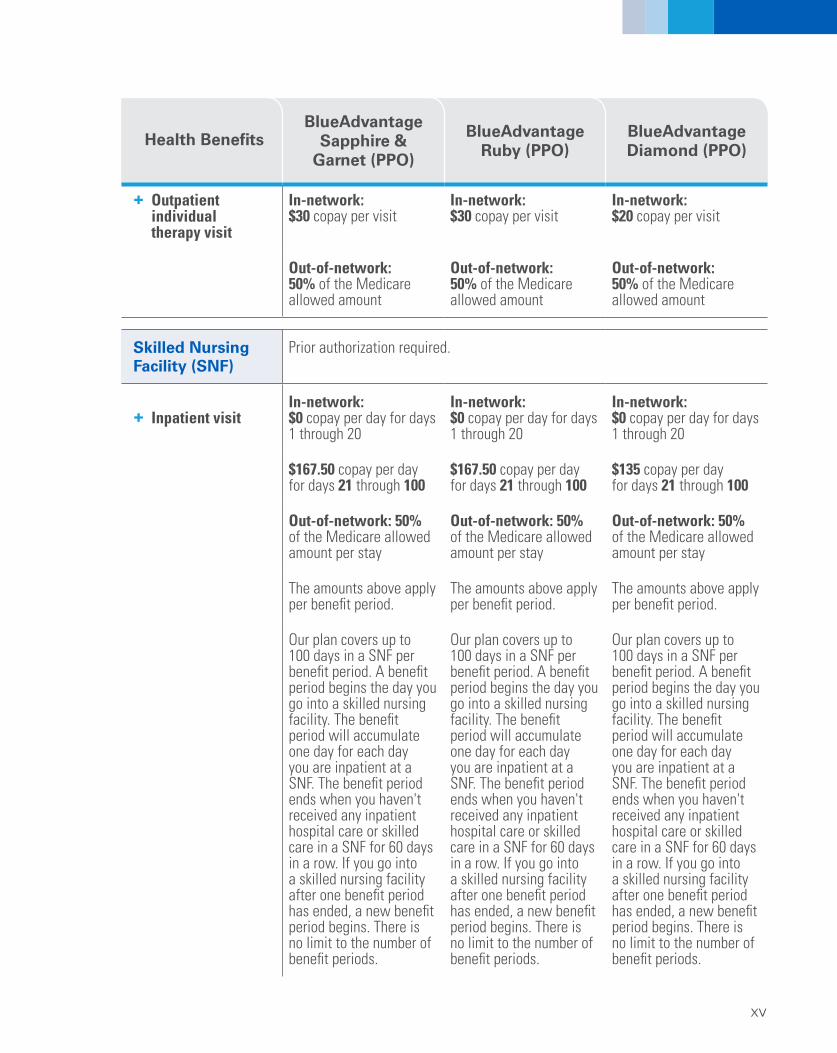
+ Outpatient individual therapy visit
In-network: $30 copay per visit
In-network: $30 copay per visit
In-network: $20 copay per visit
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
Out-of-network: Out-of-network: Out-of-network: 50% of the Medicare 50% of the Medicare 50% of the Medicare allowed amount allowed amount allowed amount
Skilled Nursing Facility (SNF)
+ Inpatient visit
Prior authorization required.
In-network: $0 copay per day for days 1 through 20
$167.50 copay per day for days 21 through 100
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
Our plan covers up to 100 days in a SNF per benefit period. A benefit period begins the day you go into a skilled nursing facility. The benefit period will accumulate one day for each day you are inpatient at a SNF. The benefit period ends when you haven't received any inpatient hospital care or skilled care in a SNF for 60 days in a row. If you go into a skilled nursing facility after one benefit period has ended, a new benefit period begins. There is no limit to the number of benefit periods.
In-network: $0 copay per day for days 1 through 20
$167.50 copay per day for days 21 through 100
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
Our plan covers up to 100 days in a SNF per benefit period. A benefit period begins the day you go into a skilled nursing facility. The benefit period will accumulate one day for each day you are inpatient at a SNF. The benefit period ends when you haven't received any inpatient hospital care or skilled care in a SNF for 60 days in a row. If you go into a skilled nursing facility after one benefit period has ended, a new benefit period begins. There is no limit to the number of benefit periods.
In-network: $0 copay per day for days 1 through 20
$135 copay per day for days 21 through 100
Out-of-network: 50% of the Medicare allowed amount per stay
The amounts above apply per benefit period.
Our plan covers up to 100 days in a SNF per benefit period. A benefit period begins the day you go into a skilled nursing facility. The benefit period will accumulate one day for each day you are inpatient at a SNF. The benefit period ends when you haven't received any inpatient hospital care or skilled care in a SNF for 60 days in a row. If you go into a skilled nursing facility after one benefit period has ended, a new benefit period begins. There is no limit to the number of benefit periods.
xvi
+
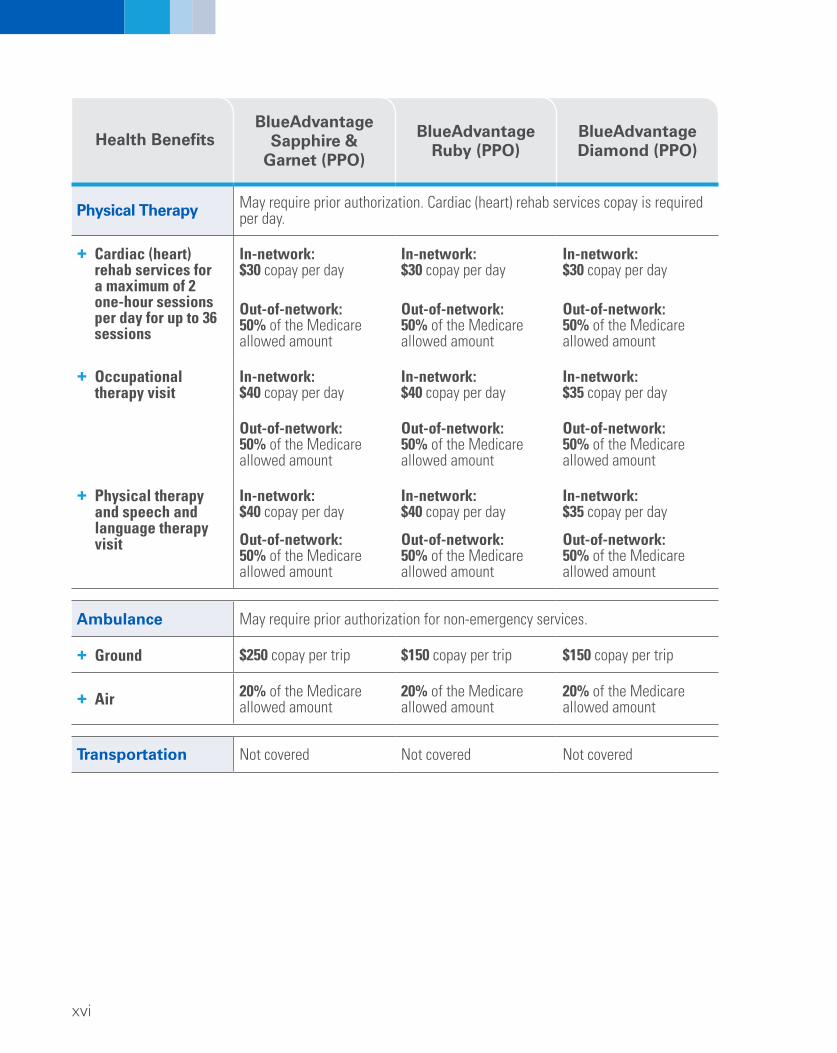
Physical Therapy per day.
In-network: $30 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $40 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $40 copay per day
Out-of-network: 50% of the Medicare allowed amount
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
May require prior authorization. Cardiac (heart) rehab services copay is required
+ Cardiac (heart) rehab services for a maximum of 2 one-hour sessions per day for up to 36 sessions
+ Occupational therapy visit
+ Physical therapy and speech and language therapy visit
In-network: $30 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $40 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $40 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $30 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $35 copay per day
Out-of-network: 50% of the Medicare allowed amount
In-network: $35 copay per day
Out-of-network: 50% of the Medicare allowed amount
Ambulance May require prior authorization for non-emergency services.
+ Ground $250 copay per trip $150 copay per trip $150 copay per trip
Air 20% of the Medicare allowed amount
20% of the Medicare allowed amount
20% of the Medicare allowed amount
Transportation Not covered Not covered Not covered
xvii
Health Benefits BlueAdvantage
Sapphire & Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
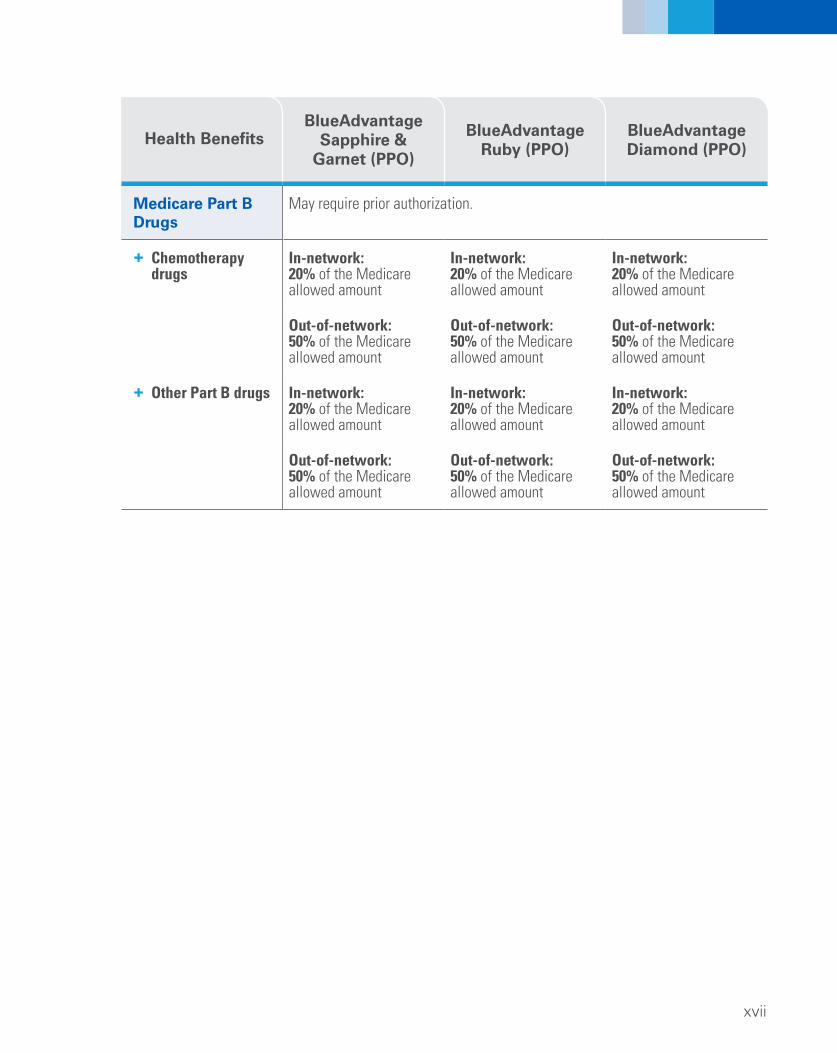
Medicare Part B Drugs
+ Chemotherapy drugs
+ Other Part B drugs
May require prior authorization.
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
xviii
Prescription Drug Benefits
1. Deductible Stage
These plans do not have deductibles for drug benefits. Prescription drug copays and coinsurance do not apply to the maximum out-of-pocket.
2. Initial Coverage Stage
What you pay for: Preferred Retail and Mail Order Pharmacy OR Standard Retail and Mail Order Pharmacy
You pay the following until total yearly drug cost (including what our plan paid and what you have paid) reaches $3,750.
Total yearly drug costs are the total drug costs paid by both you and our Part D plan. You may get your drugs at preferred retail pharmacies and through the preferred mail order pharmacy program managed by Express Scripts®. Or you can get your drugs from standard retail pharmacies or the standard mail order pharmacy, DrugSource, Inc. Your prescription drug copay will typically be less at a preferred network pharmacy because it has an agreement with BlueAdvantage. Some medications may require prior authorization, please see the formulary (drug list).
xix
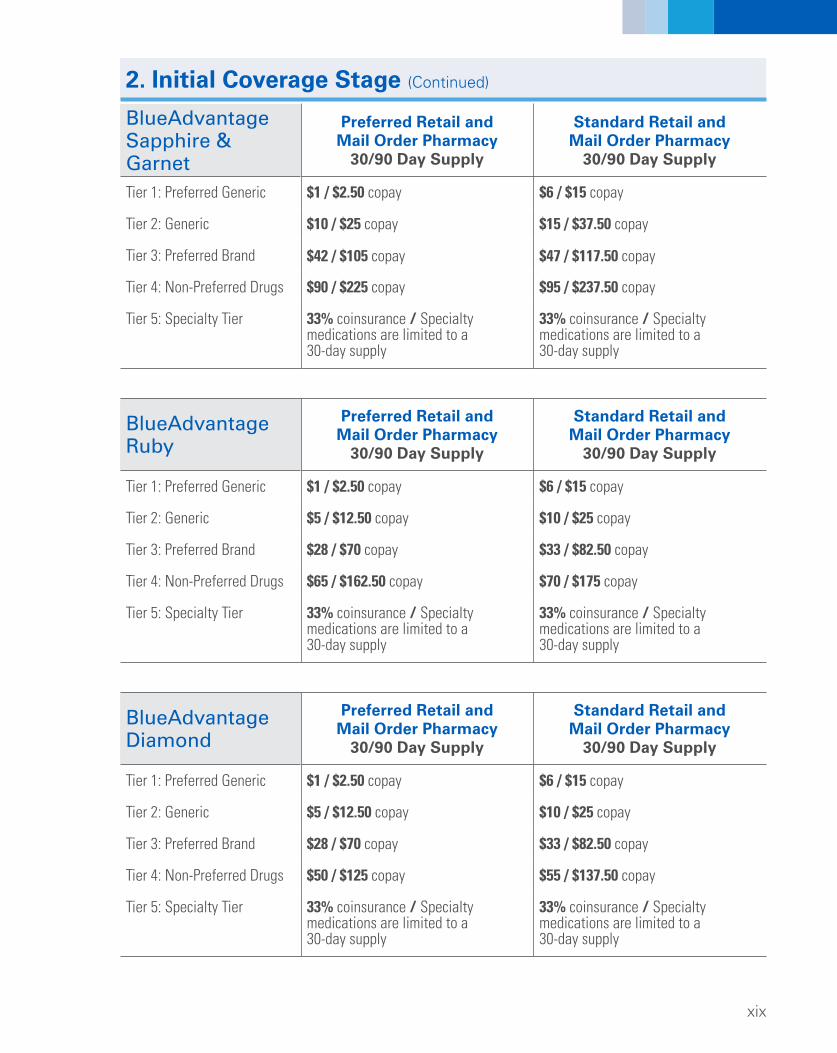
2. Initial Coverage Stage (Continued)
BlueAdvantage Sapphire & Garnet
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drugs
Tier 5: Specialty Tier
$1 / $2.50 copay
$10 / $25 copay
$42 / $105 copay
$90 / $225 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
$6 / $15 copay
$15 / $37.50 copay
$47 / $117.50 copay
$95 / $237.50 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
BlueAdvantage Ruby
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drugs
Tier 5: Specialty Tier
$1 / $2.50 copay
$5 / $12.50 copay
$28 / $70 copay
$65 / $162.50 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
$6 / $15 copay
$10 / $25 copay
$33 / $82.50 copay
$70 / $175 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
BlueAdvantage Diamond
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drugs
Tier 5: Specialty Tier
$1 / $2.50 copay
$5 / $12.50 copay
$28 / $70 copay
$50 / $125 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
$6 / $15 copay
$10 / $25 copay
$33 / $82.50 copay
$55 / $137.50 copay
33% coinsurance / Specialty medications are limited to a 30-day supply
xx
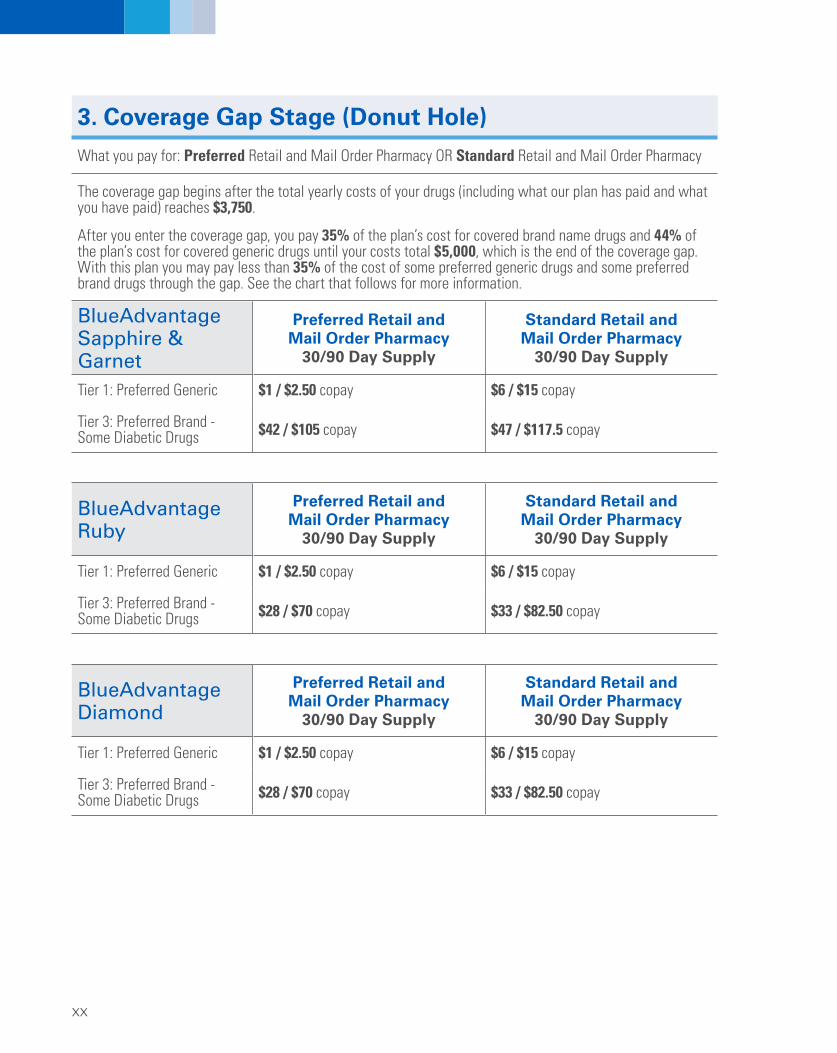
3. Coverage Gap Stage (Donut Hole)
What you pay for: Preferred Retail and Mail Order Pharmacy OR Standard Retail and Mail Order Pharmacy
The coverage gap begins after the total yearly costs of your drugs (including what our plan has paid and what you have paid) reaches $3,750.
After you enter the coverage gap, you pay 35% of the plan’s cost for covered brand name drugs and 44% of the plan’s cost for covered generic drugs until your costs total $5,000, which is the end of the coverage gap. With this plan you may pay less than 35% of the cost of some preferred generic drugs and some preferred brand drugs through the gap. See the chart that follows for more information.
BlueAdvantage Sapphire & Garnet
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 3: Preferred Brand - Some Diabetic Drugs
$1 / $2.50 copay
$42 / $105 copay
$6 / $15 copay
$47 / $117.5 copay
BlueAdvantage Ruby
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 3: Preferred Brand - Some Diabetic Drugs
$1 / $2.50 copay
$28 / $70 copay
$6 / $15 copay
$33 / $82.50 copay
BlueAdvantage Diamond
Preferred Retail and Mail Order Pharmacy
30/90 Day Supply
Standard Retail and Mail Order Pharmacy
30/90 Day Supply
Tier 1: Preferred Generic
Tier 3: Preferred Brand - Some Diabetic Drugs
$1 / $2.50 copay
$28 / $70 copay
$6 / $15 copay
$33 / $82.50 copay
xxi
4. Catastrophic Coverage Stage
After your yearly out-of-pocket drug costs (including drugs purchased through your retail pharmacy and through mail order) reach $5,000, until 12/31/18, you pay the greater of:
5% of the cost, or $3.35 copay for generic (including brand drugs treated as generic) $8.35 copay for all other drugs.
xxii
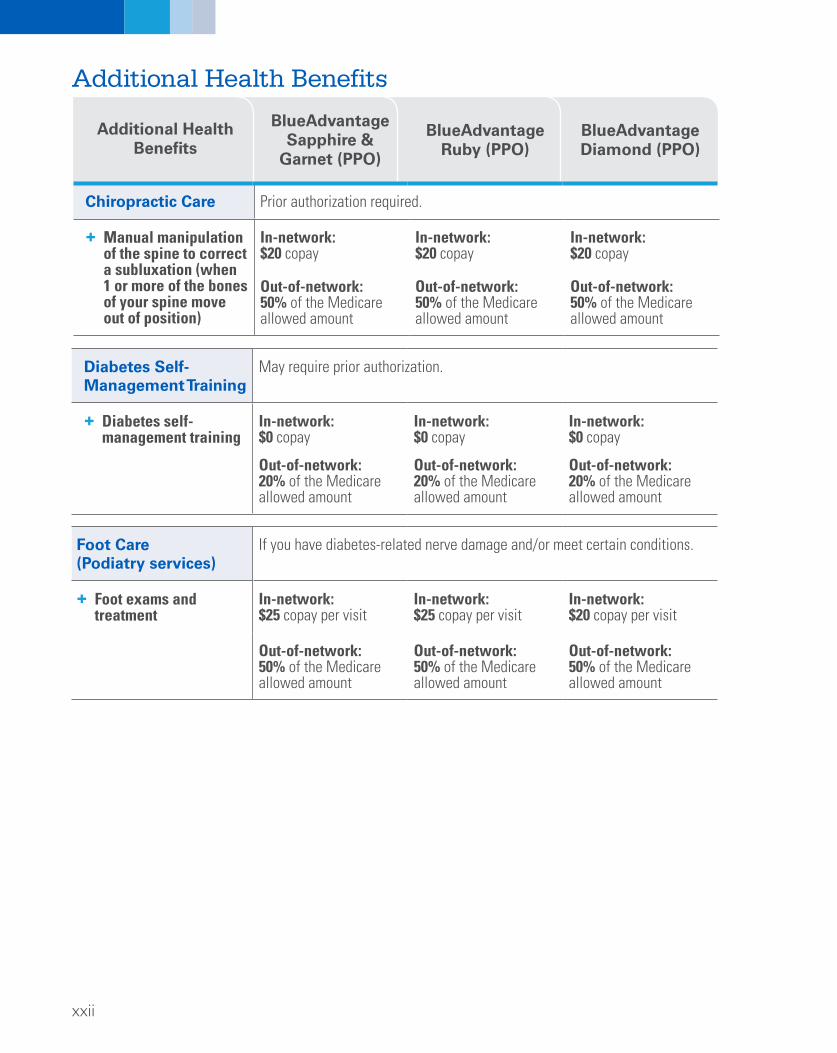
Additional Health Benefits
Chiropractic Care Prior authorization required.
Additional Health Benefits
BlueAdvantage Sapphire &
Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
+ Manual manipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position)
In-network: $20 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $20 copay
Out-of-network: 50% of the Medicare allowed amount
In-network: $20 copay
Out-of-network: 50% of the Medicare allowed amount
Diabetes Self-Management Training
May require prior authorization.
+ Diabetes self-management training
In-network: $0 copay
Out-of-network: 20% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 20% of the Medicare allowed amount
In-network: $0 copay
Out-of-network: 20% of the Medicare allowed amount
Foot Care (Podiatry services)
If you have diabetes-related nerve damage and/or meet certain conditions.
+ Foot exams and treatment
In-network: $25 copay per visit
In-network: $25 copay per visit
In-network: $20 copay per visit
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
xxiii
Additional Health
Benefits
BlueAdvantage Sapphire &
Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
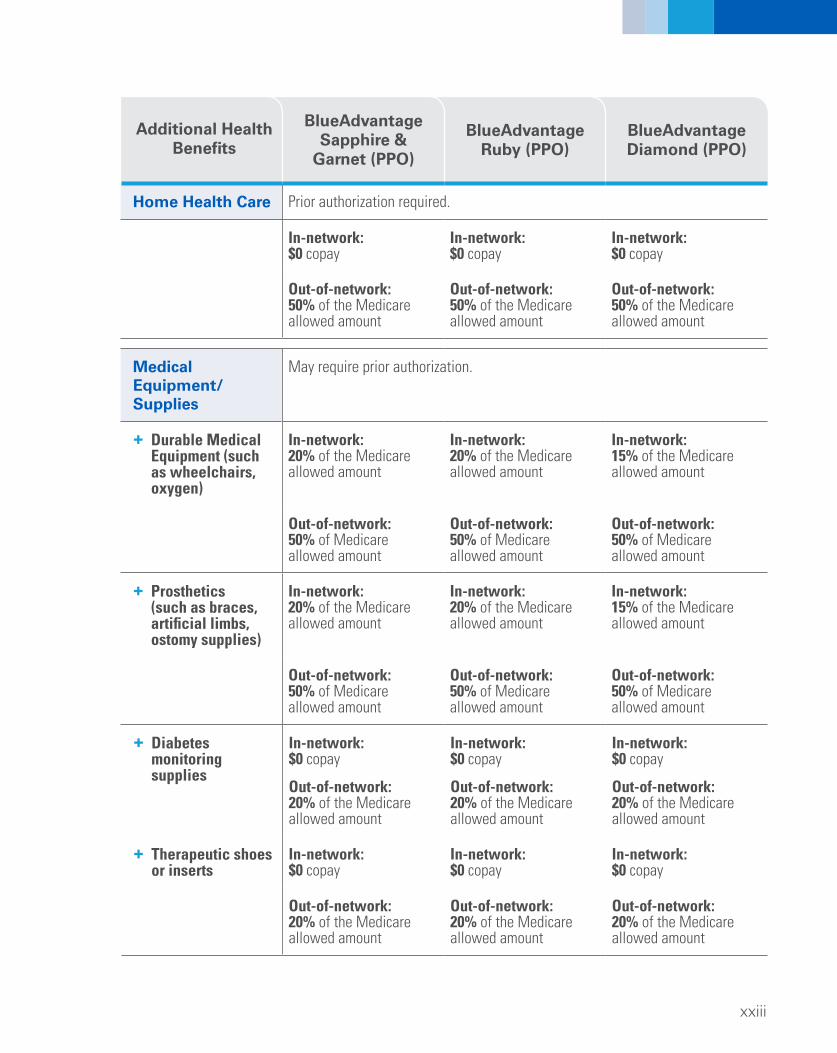
Home Health Care Prior authorization required.
In-network: $0 copay
In-network: $0 copay
In-network: $0 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Medical Equipment/ Supplies
May require prior authorization.
+ Durable Medical Equipment (such as wheelchairs, oxygen)
In-network: 20% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
In-network: 15% of the Medicare allowed amount
Out-of-network: 50% of Medicare allowed amount
Out-of-network: 50% of Medicare allowed amount
Out-of-network: 50% of Medicare allowed amount
+ Prosthetics In-network: In-network: In-network: (such as braces, 20% of the Medicare 20% of the Medicare 15% of the Medicare artificial limbs, allowed amount allowed amount allowed amount ostomy supplies)
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
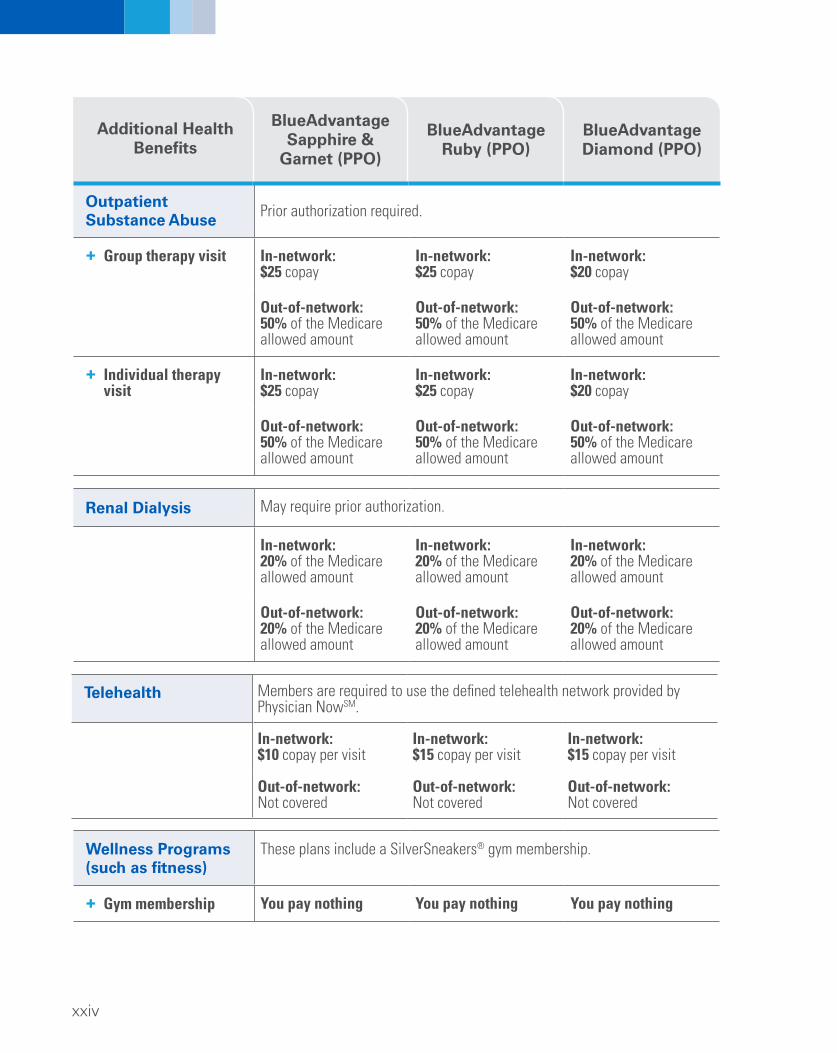
Individual therapy visit
In-network: $25 copay
In-network: $25 copay
In-network: $20 copay
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Out-of-network: 50% of the Medicare allowed amount
Additional Health Benefits
BlueAdvantage Sapphire &
Garnet (PPO)
BlueAdvantage Ruby (PPO)
BlueAdvantage Diamond (PPO)
Renal Dialysis May require prior authorization.
In-network: 20% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
In-network: 20% of the Medicare allowed amount
Out-of-network: 20% of the Medicare allowed amount
Out-of-network: 20% of the Medicare allowed amount
Out-of-network: 20% of the Medicare allowed amount
Members are required to use the defined telehealth network provided by Physician NowSM.
Telehealth
In-network: In-network: In-network: $10 copay per visit $15 copay per visit $15 copay per visit
Out-of-network: Out-of-network: Out-of-network: Not covered Not covered Not covered
Wellness Programs These plans include a SilverSneakers® gym membership. (such as fitness)
+ Gym membership You pay nothing You pay nothing You pay nothing
For more information, please call us at the phone number below or visit us at bcbstmedicare.com.
If you are a member, call toll-free 1-800-831-BLUE (2583), TTY: 711.
If you are not a member, call toll-free 1-800-292-5146, TTY: 711.
From Oct. 1 to Feb. 14, you can call us 7 days a week from 8 a.m. to 9 p.m. ET. From Feb. 15 to Sept. 30, you can call us Monday through Friday from call 8 a.m. to 9 p.m. ET. If you call us outside these hours or on a holiday, our automated system will answer your call.
You can leave a message for us, and we will call you back as soon as possible.
This information is not a complete description of benefits. Contact the plan for more information. Limitations, copayments, and restrictions may apply. Benefits, premiums and/or co-payments/co-insurance may change on January 1 of each year.
You can see our plan's provider directory at our website at bcbstmedicare.com You can see our plan's pharmacy directory at our website at bcbstmedicare.com. The formulary, pharmacy network, and/or provider network may change at any time. You will receive notice when necessary. We cover Part D drugs. In addition, we cover
Part B drugs such as chemotherapy and some drugs administered by your provider. You can see the complete plan formulary (list of Part D prescription drugs) and any
restrictions on our website at bcbstmedicare.com.
MDLive provides the PhysicianNowSM services for BlueCross BlueShield of Tennessee and is an independent internet and phone based service that allows consumers to select and interact with independent physicians and other health care providers. Physician Now does not provide BlueCross BlueShield of Tennessee branded products and services.
Tivity Health, Inc. is an independent company that provides fitness services for BlueCross BlueShield of Tennessee. Tivity Health, Inc. does not provide BlueCross BlueShield of Tennessee branded products and services.
If you want to know more about the coverage and costs of Original Medicare, look in your current "Medicare & You" handbook. View it online at http://www.medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227),
24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.
BlueCross BlueShield of Tennessee 1 Cameron Hill Circle | Chattanooga, TN 37402 bcbstmedicare.com
BLUE CROSS®, BLUE SHIELD® and the Cross and Shield Symbols are registered service marks of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans.
BlueCross BlueShield of Tennessee, an Independent Licensee of the Blue Cross Blue Shield Association