47
| Date post: | 20-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | sarosem |
| View: | 4,347 times |
| Download: | 1 times |


THIS WEEK
BMJ | 16 MARCH 2013 | VOLUME 346
!NEWS, p "
NEWS1 Antimicrobial resistance presents an “apocalyptic”
threat, CMO warns
Financial strains must not risk work of volunteers in the NHS
2 Judge rules that decision to close three children’s heart units was unfair
New rules on competition are still a concern
3 Case against doctor from Stafford hospital set to start next week
Britons are making healthier lifestyle choices than 40 years ago
4 More than a third of GPs on CCG boards have conflicts of interest
Articles appearing in this print journal have already been published on bmj.com, and the version in print may have been shortened. bmj.com also contains material that is supplementary to articles: this will be indicated in the text (references are given as w!, w", etc) and be labelled as extra on bmj.com. Please cite all articles by year, volume, and elocator (rather than page number), eg BMJ "#!$; $%&:f"'&. A note on how to cite each article appears at the end of each article, and this is the form the reference will take in PubMed and other indexes.
COMMENTEDITORIALS
7 Is an EMA review on hormonal contraception and thrombosis needed?Frans M Helmerhorst and Frits R Rosendaal
8 Cognitive deficits and mild traumatic brain injury V F J Newcombe and D K Menon ! RESEARCH, p #$
9 Regulating the NHS market in EnglandChris Ham
10 The new UK antimicrobial resistance strategy and action planAnthony S Kessel and Mike Sharland
FEATURES16 The hospital bed: on its way out?
John Appleby examines trends in the number of hospital beds and wonders how low we can go
HEAD TO HEAD18 Should GPs be fined for rises in avoidable
emergency admissions to hospital?Commissioning organisations in England face losing a quarter of the “quality premium” if they do not keep down their emergency admissions for speci(c conditions. Martin McShane supports the plan, but Chaand Nagpaul worries about possible unintended consequences
ANALYSIS20 Antimicrobial resistance: the true cost
Richard Smith and Joanna Coast argue that current estimates of the cost of antibiotic resistance are misleading and may result in inadequate investment in tackling the problem
MAL
COLM
WIL
LET
RESEARCHRESEARCH NEWS
11 All you need to read in the other general journals
RESEARCH PAPERS12 Influence of initial severity of depression on
effectiveness of low intensity interventions: meta-analysis of individual patient dataPeter Bower et al
13 Comparative effect sizes in randomised trials from less developed and more developed countries: meta-epidemiological assessment Orestis A Panagiotou et al
14 Features of effective computerised clinical decision support systems: meta-regression of 162 randomised trialsPavel S Roshanov et al
15 Cognitive function and other risk factors for mild traumatic brain injury in young men: nationwide cohort study Anna Nordström et al! EDITORIAL, p %
Caption, p xx
Sufficient evidence for the oral pill exists,p &
UK smoking, p '
More new antibiotics needed, p ()
King’s Fund reports on volunteers in the NHS p #

THIS WEEK
BMJ | 16 MARCH 2013 | VOLUME 346
LAST WORDS41 Scrap the royal colleges’ fellowships
Des Spence On first name terms
Oliver Ellis
EDUCATION CLINICAL REVIEW
29 Achilles tendon disordersChad A Asplund and Thomas M Best
PRACTICEQUALITY IMPROVEMENT REPORT
34 Maximising opportunities for increased antiretroviral treatment in children in an existing HIV programme in rural South AfricaRuth M Bland et al
ENDGAMES40 Quiz page for doctors in training
MINERVA42 Generating energy from crematoriums, and other
stories
COMMENTLETTERS
23 Predicted fracture risk; Bisphosphonates and GI cancers
24 Paracetamol hepatotoxicity; Cap on social care in England
OBSERVATIONSMEDICINE AND THE MEDIA
25 Hype and the HIV cureMargaret McCartney
PERSONAL VIEW
26 After Mid Staffs: NHS must look to care of its own staffAnonymous
OBITUARIES27 Ian Greville Tait
Pioneering polymath and Benjamin Britten’s general practitioner
28 Joseph Footitt; Alan William Fowler; Frank Neville Garratt; Athol Noble Hepburn; William Philip Dowie Logan; Muhammad Shafiq
Time for a break?Refresh yourself.
masterclasses.bmj.com
Angry NHS staff, p (*
An infected heel ulcer, p "(

THIS WEEK
BMJ | 16 MARCH 2013 | VOLUME 346
!."%".#%
$.%%
&.'%
Eschericha coli - %$%Klebsiella spp - ".(%Other Gram negative - $.&%Pseudomonas spp - &.%%Proteus spp - %.#%Enterobacter spp - '.'%Bacteroides spp - #.)%Serratia spp - #.*%Acinetobacter spp - *."%
&.'%
Gram negative
Gram positive
#.$%#.&%#.&%#.'%
%$%
".(%
$.&%
&.%%
%.#%
'.'%#.)%
#.*%*."%
Staphylococcus aureus (MRSA) - !."%Non-pyogenic streptococci - ".#%Enterococcus spp - $.%%Streptococcus pneumoniae - &.'%Other Gram positive - &.'%Staphylococcus aureus (MRSA) - #.$%Group B streptococci - #.&%Group A streptococci - #.&%Diphtheroids - #.'%
GRAPHIC OF THE WEEK Gram negative bacteria such as Klebsiella and Escherichia coli (E coli) have overtaken Gram positive bacteria such as Staphylococcus aureus to become the main organisms causing bloodstream infections in adults in England, Wales, and Northern Ireland, according to the recent annual report of the chief medical officer for England (data from the English National Point Prevalence Survey on Healthcare Related Infections and Antimicrobial Use, 2011, HPA England, 2012). The report points out that the threat to health posed by Enterobacteriaceae (E coli and Klebsiella related species), which are now the most frequent agents of hospital acquired infection (36% and 7.8% respectively), is substantial. Kessel and Sharland warn, in their editorial, that 10-20% of these Gram negative bloodstream infections are antibiotic resistant and 30% of patients who acquire a multidrug resistant Gram negative bloodstream infection are likely to die.
!SEE NEWS , p ", EDITORIAL, p "#, ANALYSIS, p $#
16 March 2013 Vol 346The Editor, BMJ BMA House, Tavistock Square, London WC!H "JR Email: [email protected] Tel: +!! (")#" $%&$ !!'" Fax: +!! (")#" $%&% (!'& BMA MEMBERS’ INQUIRIES Email: [email protected] Tel: +!! (")#" $%&% ((!# BMJ CAREERS ADVERTISING Email: [email protected] Tel: +!! (")#" $%&% ()%' DISPLAY ADVERTISING Email: [email protected] Tel: +!! (")#" $%&% (%&( REPRINTS UK/Rest of worldEmail: [email protected]: +!! (")#" &!!) )&#) USAEmail: [email protected]: + ' (&)() !&* !!!( SUBSCRIPTIONS BMA Members Email: [email protected] Tel: +!! (")#" $%&% ((!# Non-BMA Members Email: [email protected] Tel: +!! (")#" $%&% (#$" OTHER RESOURCES For all other contacts: resources.bmj.com/bmj/contact-us For advice to authors:resources.bmj.com/bmj/authorsTo submit an article:submit.bmj.com
The BMJ is published by BMJ Publishing Group Ltd, a wholly owned subsidiary of the British Medical Association.The BMA grants editorial freedom to the Editor of the BMJ. The views expressed in the journal are those of the authors and may not necessarily comply with BMA policy. The BMJ follows guidelines on editorial independence produced by the World Association of Medical Editors (www.wame.org/wamestmt.htm#independence) and the code on good publication practice produced by the Committee on Publication Ethics (www.publicationethics.org.uk/guidelines/).The BMJ is intended for medical professionals and is provided without warranty, express or implied. Statements in the journal are the responsibility of their authors and advertisers and not authors’ institutions, the BMJ Publishing Group, or the BMA unless otherwise specified or determined by law. Acceptance of advertising does not imply endorsement.To the fullest extent permitted by law, the BMJ Publishing Group shall not be liable for any loss, injury, or damage resulting from the use of the BMJ or any information in it whether based on contract, tort, or otherwise. Readers are advised to verify any information they choose to rely on.©BMJ Publishing Group Ltd #"'# All Rights Reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any other means, electronic, mechanical, photocopying, recording, or otherwise, without prior permission, in writing, of the BMJPublished weekly. US periodicals class postage paid at Rahway, NJ. Postmaster: send address changes to BMJ, c/o Mercury Airfreight International Ltd Inc, %() Blair Road, Avenel, NJ "$""', USA. +$*(. WeeklyPrinted by Polestar Limited
RESPONSE OF THE WEEKIt may be significant that students, lowest in the medical hierarchy, are able to break into our over-regulated NHS culture with the simple question ‘What can I do to improve your stay?’ While following prescribed guidelines will almost always be necessary in modern practice, it’s vital that all staff—not just learners—retain their authority to attend directly to patient experience while doing so. And sometimes the protocol misleads. As George Orwell said about his own guidance for writing good English, ‘Break any of these rules sooner than say anything outright barbarous.’
Sebastian Kraemer, child and adolescent psychiatrist, Whittington Hospital, London, UK, in response to “IHI Open School’s quality improvement initiative” (BMJ 2013;346:f1371)
BMJ.COM POLLLast week’s poll asked: “Should GPs be fined for rises in avoidable emergency admissions?”
65% voted no (total 858 votes cast)
!BMJ #"'%;%!(:f'%&* and BMJ #"'%;%!(:f'%*'
This week’s poll asks:“Are the dangers of antibiotic resistance exaggerated?”
!BMJ #"'%;%!(:f'!*% !Vote now on bmj.com
MOST SHAREDLocum GP from India is jailed for manslaughter in UK after failing to spot diabetic ketoacidosis Health reform alone is pointless Francis interview: what doctors must learn from my report Drug company gifts to medical students: the hidden curriculum Winding back the harms of too much medicine
BMJ | 16 MARCH 2013 | VOLUME 346
THIS WEEK
At the end of the !"#$s, the then US surgeon general William H Steward famously declared: “The war against infectious diseases has been won.” His optimism might well have been justi%ed at the time. The discovery of antibiotics and their widespread introduction had transformed both medical practice and life expectancy.
Antibiotics still transform lives, but—as with so many of the world’s resources—we now know that they are not limitless, and that unless we are careful, their bene%cial e&ects will run out. We have become so accustomed to the availability of antibiotics that a world without them is almost inconceivable. Yet this is the world that England’s chief medical o'cer, Sally Davies, demands we contemplate in the second volume of her annual report (p !). The causes of this unfolding catastrophe are many: overuse of existing antibiotics, increasing resistance to them, a “discovery void” regarding new drugs, and a change in the types of organisms presenting the greatest threat. “If we don’t get this right we will %nd ourselves in a health system not dissimilar to the early !"th century,” she says.
Is Davies being overdramatic? Sadly not. Her decision to focus on antimicrobial resistance has been broadly welcomed. And this week we publish a report from Richard Smith and Joanna Coast, long term analysts of the economics of resistance (p ($). They suggest that the picture she paints may even be too rosy. “Resistance is said to present a risk that we will fall back into the pre-antibiotic era,” they say. “However, this is perhaps optimistic.”
Their argument is that we have badly underestimated the cost of resistance. Studies that have tried to estimate the economic impact have looked at the extra cost of treating a resistant infection compared with a susceptible one. But this ignores the bigger picture. The
whole of modern healthcare, including invasive surgery and immunosuppressive chemotherapy, is based on the assumption that infections can be prevented or treated. ”Resistance is not just an infectious disease issue,” they say. “It is a surgical issue, a cancer issue, a health system issue.”
Their revised assessment of the economic burden of resistance encompasses the possibility of not having any e&ective antimicrobial drugs. Under these circumstances they estimate that infection rates a)er hip replacement would increase from about !% to *$-+$%, and that about a third of people with an infection would die. It seems likely that rates of hip replacement would fall, bringing an increased burden of morbidity from hip pain.
The CMO’s !, recommendations include better hygiene measures and surveillance, greater e&orts to preserve the e&ectiveness of existing drugs, and encouragement to develop new ones. As Anthony Kessel and Mike Sharland point out, only one or two new antibiotics that target Gram negative organisms are likely to be marketed in the next decade (p !$). Recognising this as a global problem, the CMO’s report also calls for antimicrobial resistance to be put on the national risk register and taken seriously by politicians internationally.
As for the cost of such action, Smith and Coast see it as an essential insurance policy against a catastrophe that we hope will never happen. And they share the CMO’s urgency. “Waiting for the burden to become substantial before taking action may mean waiting until it is too late.”Fiona Godlee, editor, [email protected] this as: BMJ "#$%;%&':f$''%
EDITOR’S CHOICE
Drug resistance!an unfolding catastrophe“Resistance is said to present a risk that we will fall back into the pre-antibiotic era . . . However, this is perhaps optimistic”
Sign up today using your smartphone —follow these steps:
(Download a free QR reader from your handset's app store
(Hold your smartphone over the QR code
(You will then be forwarded to the email sign up page
bmj.com/archiveVisit
The archiveDates from 1840
Delve into the complete back archive from the first issue and read BMJ articles written by eminent authors such as David Livingstone, Joseph Lister, Arthur Conan Doyle, Florence Nightingale, Richard Doll, and Alice Stewart.
(To receive Editor’s Choice by email each week, visit www.bmj.com/newaccount
Twitter (Follow the editor, Fiona
Godlee, at twitter.com/fgodlee, and the BMJ at twitter.com/bmj_latest

NEWS
BMJ | 16 MARCH 2013 | VOLUME 346 1
Ingrid Torjesen LONDONAction is needed at both a national and interna-tional level to avert the “ticking time bomb” of antimicrobial resistance, which presents a threat as grave as climate change, the chief medical o!cer for England has warned.
In the second volume of her annual report for "#$$, Infections and the rise of antimicrobial resistance,$ Sally Davies spelt out the threat—overuse of existing antibiotics and increasing resistance to them, a “discovery void” of new antibiotics, a change in the types of organism presenting the greatest threat, and the need for better training of NHS sta% in hygiene and infection control.
“If we don’t get this right we will &nd our-selves in a health system not dissimilar to the early $'th century,” where deaths from infec-tions will be commonplace because of a lack of e%ective treatments, Davies told a press brie&ng at the Department of Health. The department would publish a &ve year strategy for action in the next couple of weeks, she said.
At the chief medical o!cer’s recommenda-tion, the Department of Health and the Depart-ment for Environment, Food, and Rural A%airs have added antimicrobial resistance to their strategic risk registers. Davies has also requested that it be added to the National Security Risk Assessment, alongside pandemic flu and t errorism, to ensure cross government action.
“Governments and organisations across the world, including the World Health Organization and G(, need to take this seriously,” she said. This included &nding some way of incentivis-ing the pharmaceutical industry to develop new antibiotics. No new antibiotic classes have been discovered since $'(), and Davies said that no pharmaceutical companies had any new anti-biotic classes in their pipeline, and that there were few new antibiotics of existing classes in development.
With the pipeline drying up, stewardship of antibiotics in health, &sheries, and farming had become increasingly important, she said. In health, that meant prescribing antibiotics only when appropriate and ensuring that the patient completed the course. Cite this as: BMJ !"#$;$%&:f#'()
Zosia Kmietowicz BMJCommissioners and service providers need to better plan the role of volunteers in both the health and social care sectors if they are to avoid alienating the swathes of people who provide their time for free and ease growing tensions with those in paid jobs, a report from a leading think tank has said.1
An estimated three million people in England volunteer in the NHS, health charities, and social care organisations—the same number in paid employment in the NHS and social care systems, says the report from the King’s Fund. Volunteers play a vital role in delivering services such as assisting with mealtimes, providing support for bereaved families, and befriending older people in care homes.
The Institute for Volunteering Research has suggested that volunteers are worth around £700 000 a year to hospital
trusts, £500 000 a year to mental health trusts, and £250 000 a year to a primary care trust.
The latest report was commissioned by the Department of Health to look at the effect of the current changes to health and social care sectors on volunteering. The government sees volunteering as helping to achieve its wider ambitions to decentralise power, reduce reliance on the state, and encourage people to take an active role in their communities.
However, the current economic climate means that some “tensions have already emerged,” said the report. Some people are questioning the value of volunteers, and research has shown that staff are sometimes unclear about what volunteers do. Financial pressures also risk creating strains with paid employees who are concerned about their jobs.
It is for these reasons, the report said, that commissioners
and service providers need to focus on how volunteers will help improve quality and bring benefits to organisations, patients, and communities.
To make the most of volunteers, commissioners and providers must acknowledge the value of volunteers, develop a clear vision of how volunteers can help organisations and patients, measure their input, and clarify the boundaries between professional and volunteer roles to allay concerns of job substitution.
The report said, “It is more important than ever to think strategically about the role of volunteering. The health and social care system will find it increasingly difficult to meet its objectives without doing so.”
Chris Naylor, fellow at the King’s Fund, said that volunteering should be used to improve quality and not to reduce short term costs.Cite this as: BMJ !"#$;$%&:f#'('
Without volunteers the NHS will find it increasingly difficult to meet its objectives, said the King’s Fund
Financial strains must not risk work of volunteers in the NHS
Antimicrobial resistance presents an “apocalyptic” threat, CMO warns
LIFE
IN V
IEW
/SPL
UK news First case against doctor from Stafford hospital set to start next week, p ! BMJ investigation More than a third of GPs on CCG boards have conflicts of interest, p "
* References on news stories are in the versions on bmj.com
bmj.com * Judge overturns
New York’s ban on supersize sweet drinks

NEWS
2 BMJ | 16 MARCH 2013 | VOLUME 346
Clare Dyer BMJCampaigners !ghting the decision to close the children’s heart surgery unit in Leeds as part of an exercise to concentrate operations in fewer but larger centres have scored a comprehensive victory at the High Court in London.
Mrs Justice Nicola Davies ruled that the “Safe and Sustainable” consultation that recommended closing three units was flawed by procedural unfairness and a failure to take into account mate-rial considerations.
The success for the campaigning group, Save our Surgery Limited, on both grounds of its challenge is a signi!cant setback for the plans to concentrate surgery at only seven sites: Bristol, Birmingham, Southampton, Liverpool, Newcastle, and two in London. Units in Leeds and Leicester and at London’s Royal Brompton Hospital in London would be axed under the consultation recommendations."
The judge ruled that the consultation process was unlawful in the !rst instance because the Joint Committee of Primary Care Trusts, which
Zosia Kmietowicz BMJThe UK government has redra#ed regulations on procurement, in an attempt to allay concerns raised by several medical bodies and MPs in the past few weeks that clinical commissioners would be forced to put out to competitive tender most of the services they wanted for their patients.
However, both the BMA and the Royal College of General Practitioners are still concerned that commissioners are not completely free to choose when to use competition and when not to.
The revised regulations, which were laid before parliament on "" March, mean that the position on competition is unchanged from now, said the Department of Health—commissioners are able to o$er contracts to a single provider where only that provider is capable of providing the services.
In explanatory notes, it said, “We have removed the words that inadvertently created the impression that there were only very narrow cir-cumstances in which commissioners could award a contract without a competition.”
The department said that the rewording makes it clear that Monitor, the economic regulator of the NHS, has no power to force the competitive ten-dering of services when the regulations come into force on " April, and that decisions about how and when to introduce competition are solely up
to doctors and nurses in clinical commissioning groups. It added, “Competition should not trump integration—commissioners are free to commis-sion an integrated service where it is in the inter-est of patients.”
The UK Labour Party and the new National Health party criticised the original secondary leg-islation published in February." More than "%%% doctors also urged MPs to force a debate on the regulations& and the Academy of Medical Royal Colleges expressed “considerable concern” at the regulations, which were published to supplement section '( of the Health and Social Care Act.
Clare Gerada, chair of the Royal College of General Practitioners, said the revised regulations were “a step in the right direction but . . . do not go far enough in ensuring that commissioners are genuinely free to decide whether or not to expose services to competition.”
Mark Porter, chair of the BMA Council, said, “It is vital that competition is not allowed to under-mine integration, innovation, or clinical auton-omy. There still needs to be a full parliamentary debate to provide absolute clarity that CCGs [clini-cal commissioning groups] will have the freedom to decide how best to secure high quality services for local populations,” he said.Cite this as: BMJ !"#$;$%&:f#&$%
Judge rules that decision to close three children’s heart units was unfair
New rules on competition are still a concern
Campaigners to keep services in Leeds said the reform process had been “flawed and unjust”
SDS
PHOT
O/DE
MOT
IX/P
A
Services are failing people with dementia: People with dementia who live in care homes in England are more likely than similar people without dementia to go to hospital with avoidable conditions such as urinary infections, the Care Quality Commission has said. Once admitted, people with dementia are more likely than those without dementia to stay in hospital longer, be readmitted, and die in hospital.
Disclosure of pharma sponsorship made compulsory in Portugal: A law that was enacted on !" February requires doctors, scienti#c societies, and patient associations in Portugal to publicly disclose all sponsorship from the pharmaceutical industry to the national drug regulator (Infarmed). Failure to disclose conflicts of interests could result in #nes of $%&&& ('!()&) to $)" &&&.
Regulator rules that advertisements on plain packs are misleading: The Advertising Standards Authority has ruled that ads run by Japan Tobacco International—against the introduction of plain, standard packaging—are misleading and must not be published again. The ads, placed in the national press in %&!%, stated that in %&&* the government had “rejected” plain packaging for tobacco because “there was no credible evidence” to support such a policy. The regulator concluded that the claim breached the advertising code of practice.
Smoking to be banned from all Dutch cafes: Dutch health minister Martin van Rijn has con#rmed to MPs that he will bring forward changes to the law enforcing a smoking ban throughout the Netherlands’ hospitality industry. Most MPs recently voted for a total ban. Currently some smaller cafés are exempt. Last year, smoking increased from %"% to %+% in adults.
Partners agree to vaccinate 400 million children: The Global Alliance for Vaccines and Immunisation (GAVI) and the Islamic Development Bank (IDB) have signed a memorandum of understanding to help save children’s lives by accelerating the introduction of vaccines in IDB member countries. By %&%&, GAVI plans to vaccinate more than )&& million children in at least %, member countries with the aim of preventing -.% million deaths at an estimated cost of .(bn. Cite this as: BMJ !"#$;$%&:f#&!!
IN BRIEF
took the decision, had refused to disclose the sub-scores that an expert committee had given in a scoring exercise. Units were given only the overall scores.
“I am satis!ed that fairness did require disclo-sure of the sub-scores to enable Leeds to provide a properly focused and meaningful response,” said the judge, who described the committee’s refusal to hand over the sub-scores as “ill judged.”
In addition, the joint committee also failed to take into account the sub-scores when carrying out the consultation, although the overall scores were acknowledged to be close, she said. The sub-

NEWS
BMJ | 16 MARCH 2013 | VOLUME 346 3
Ingrid Torjesen LONDONBritish adults are half as likely to smoke as they were four decades ago and are drinking less heavily and less frequently, show data from the O!ce for National Statistics (ONS) "#$$ General Lifestyle Survey.
The survey’s report, launched at a press con-ference in London on % March, also shows that despite the ageing population, the proportion of people in Great Britain living with a longstanding illness or disability has remained steady over the past "# years at just under a third.$
The "#$$ report marks &# years of the survey. When the ONS survey 'rst included questions about smoking in $(%&, it found that &)% of adults smoked ()$% of men, &$% of women). Since then, smoking has more than halved and the gap in prevalence of smoking between men and women has narrowed; in "#$$, "#% of adults smoked ("$% of men, $(% of women).
Although fewer people smoke now than in the $(%#s, women who still do smoke consume similar numbers of cigarettes ($" per day in "#$$ compared with $* in $(%&), and consumption has fallen only slightly in men—from $+ ciga-rettes per day in $(%& to $* in "#$$.
Alongside smoking, the proportion of adults drinking heavily or frequently has also fallen.
Among $,-"& year olds, the proportion of men drinking more than eight units (double the rec-ommended maximum for men) in one day in the past week fell by almost a third in four years (from *"% in "##% to ""% in "#$$). The proportion of women drink-ing more than six units (double the recommended maximum for women) in any one day fell by a quarter over the same time period, from "&% to $+%.
The proportion of men drinking on five or more days in a week fell from "*% in $((+ to $,% in "#$$, while the proportion of women drinking at least 've times per week fell from $*% to (%. However, the survey found that older people were far more likely than younger people to drink frequently. In "#$$, men aged &) years or more
were more than twice as likely to drink 've times or more per week as those aged $,-&& years.
While lifestyle has improved the population has aged. Between $(%$ and "#$$, the pro-portion of the population aged ,) years or over
increased from $*.*% to $,.)%." However, this ageing has not been reflected in the overall
prevalence of longstand-ing illness or disability. In $(%", "$% of the popula-tion reported living with a longstanding illness or disability. This proportion
rose to *"% in $(($ and has remained steady. The most common longstand-ing illnesses reported were musculoskeletal illnesses, followed by heart and cir-culatory conditions, respira-tory illnesses, and endocrine
and metabolic conditions. How-ever, the proportion of people living with a longstanding ill-
ness or disability has increased from $)% in $(%) to $(% in "#$$.Cite this as: BMJ !"#$;$%&:f#'($
Clare Dyer BMJA surgeon who worked at Stafford Hospital, where inquiries uncovered hundreds of excess deaths and “appalling” standards of care between "##) and "##+, is to face a 'tness to practise hearing at the Medical Practitioners Tribunal Service next week.
Roderic Hutchinson faces allegations of de'-cient professional performance at a $# day hear-ing, which opens at the tribunal in Manchester on $+ March.
Three medically quali'ed managers at Mid Sta-ordshire NHS Foundation Trust are also set to appear before the tribunal, although no dates have yet been 'xed. They have been named as John Gibson, medical director from "##* to "##,; his successor, Valerie Suarez, who was appointed in September "##, and stepped down in March "##(; and their deputy, David Durrans.
The hearings follow investigations by the General Medical Council (GMC) into &" doctors who worked for Mid Sta-s trust at the time. $ Hutchinson’s case is the 'rst to be sent for a hearing.
A consultant general surgeon and colorectal surgeon, he underwent a GMC assessment of his professional performance in June "#$$. The charges allege that his performance was “unac-ceptable in the area of working with colleagues, and a cause for concern in the areas of other good clinical care and relationships with patients.”
The surgeon was allowed to continue work-ing under conditions including supervision by a named consultant, but the conditions were li.ed in October "#$$. He le. Mid Sta-s in September "#$".
A review of the general surgery department at Stafford Hospital by the Royal College of Surgeons in "##( concluded that the service provided was “inadequate, unsafe, and at times frankly dangerous.”"
NHS managers who are not doctors are not subject to regulation, but GMC guidance makes it clear that those who are medically quali'ed may be held to account on how they ful'l their management roles. Cite this as: BMJ !"#$;$%&:f#&$!
Case against doctor from Stafford hospital set to start next week
scores provided the basis for what was ultimately the di-erence of one point in the critical quality scoring between Leeds and Newcastle.
“In my view, and commensurate with their duty to properly scrutinise and assess all relevant evidence, the JCPCT [the joint committee] should have considered the sub-scores,” she said.
At a further hearing on "% March to decide what remedy should be granted, the Leeds cam-paigners are expected to argue that the decision on & July "#$" to concentrate children’s heart sur-gery at the seven sites should be quashed. The joint committee is expected to seek an appeal.
The Royal Brompton initially succeeded in a High Court challenge to the plans but lost on appeal."
If the decision is quashed, the Leeds campaign-ers would argue that surgery should continue at Leeds and Newcastle, the judge said.
Last October the health secretary, Jeremy Hunt, referred the decision to close the three units to the independent recon'guration panel, which advises on contested changes to health services in England. The panel was expected to deliver its decision by the end of March.*
The units earmarked for closure have argued that the consultation, which began in "##+, has been working with outdated 'gures.Cite this as: BMJ !"#$;$%&:f#')'
Britons are making healthier lifestyle choices than 40 years ago
In 1974 the survey found that 41% of women smoked; in 2011 it was 19%

BMJ INVESTIGATION
commissioners who run their own private com-panies” and called on GP commissioners to “be barred from being involved in companies that they are giving contracts to.” !
But others have said that conflicts are an inevitable by-product of allowing more clini-cians into management positions and said that focusing too much on the issue may prevent commissioners redesigning services e" ectively.
The BMJ analysed the registered interests of #$% of the !## commissioning group boards, obtained through requests made under free-dom of information legislation and from CCG websites. The remaining groups were not able to disclose their lists, though they must main-tain and publish them from # April. &
Our analysis also showed that '% of GPs on CCG boards were consultants to or advised private health or pharmaceutical companies, while (% were employed by a private health company as well as working as a GP.
Some #!% of GPs declared links with not for pro) t voluntary or social enterprise providers that represented a con* ict of interest with their commissioning role, while +% of GPs declared a con* ict of interest through a family member.
More than a third of GPs on the boards of the new clinical commissioning groups (CCGs) in England have a con* ict of interest resulting from director-ships or shares held in private companies, a new analysis by the BMJ has shown.
An examination of the registered interests of almost !(,, board members across #$% CCGs provides the clearest evidence to date of the con-* icts that many doctors will have to manage from # April, when the GP led groups are handed stat-utory responsibility for commissioning around -%,bn of NHS healthcare services.
Our investigation shows that con* icts of inter-est are rife on CCG governing bodies, with '!% (&%%) of the ##$+ GPs in executive positions having a ) nancial interest in a for-pro) t private provider beyond their own general practice—a provider from which their CCG could potentially commission services.
The interests range from senior directorships in local for-pro) t ) rms set up to provide services such as diagnostics, minor surgery, out of hours GP services, and pharmacy to shareholdings in large private sector health ) rms that provide care in conjunction with local doctors, such as H armoni and Circle Health.
May !"#" Coalition government is elected. Andrew Lansley (right), who had served as the Conservatives’ shadow health secretary for six and a half years, is appointed secretary of state for health. But it is understood that the Conservatives’ policy chief, Oliver Letwin, and the Liberal Democrat MP Danny Alexander drew up the new government’s health policy as part of their hastily devised “programme for government” ( BMJ 2012;345:e4833).
July !"#" Government publishes its NHS white paper Equity and Excellence: Liberating the NHS . This proposes handing sweeping powers to GPs in a major shake-up of the NHS. The radical proposals include the abolition of primary care trusts and the establishment of new consortiums, led by GPs, to manage NHS commissioning budgets ( BMJ 2010;341:c3796) .
January !"## Department of Health pub-lishes the Health and Social Care Bill, outlining its vision for healthcare. An accom-panying impact assessment identifi es potential confl icts of interest as a key risk associated with the proposed changes ( BMJ 2011;342:d507).
April !"## Government announces “pause” in the passage of the Health and Social Care Bill, prompted by concerns
from the Liberal Democrats, the Labour Party, and the medical profession. Steve Field, former RCGP chairman (below), is put in charge of the Future Forum set up to hear such concerns during the pause ( BMJ 2011;342:d2216).
June !"## After the listening exercise conducted during the “pause” the government announces that the GP consortiums will be renamed clinical commissioning groups (CCGs) to refl ect the wider clinical involvement beyond GPs. It says that each CCG must have at least two other clinicians on its governing body, including at least one secondary care specialist doctor ( BMJ 2011;342:d3777).
In some cases most of the GPs on the CCG gov-erning body have ) nancial interests in the same private healthcare provider.
Some doctors have relinquished interests in private enterprises because of their new roles as commissioners. These include GPs linked to Richard Branson’s Virgin Care, which announced in October !,#! that it planned to end its joint venture partnerships with over &,, GPs in Eng-land, # a. er admitting that many were becoming “increasingly worried about the perception of potential con* icts of interest.”
Calls for doctors with interests to step down But our analysis found that, in total, ((( (!&%) of !'!% clinical, lay, and managerial members of CCG governing bodies had a ) nancial stake in a for-pro) t company.
Leading GPs, including a senior government adviser on commissioning, have called for doc-tors with con* icts that were “too great” to step down and have urged the NHS Commissioning Board to o" er tougher guidance to those with multiple interests. Last week the BMA’s UK con-sultants’ conference passed a motion expressing concern at “the clear con* ict of interest of GP
More than a third of GPs on CCG boards have conflicts of interest
4 BMJ | 16 MARCH 2013 | VOLUME 346
On the eve of one of the biggest upheavals in the history of the NHS, Gareth Iacobucci looks at the conflicts at the heart of clinical commissioning groups
Membership of CCG governing bodies
GPs (n=!!"#)
Other (n=$")
Total number of board members in !"# CCGs analysed (n=$%$#)
Lay andmanagerialmembers (n=#!%)
Other clinicalmembers (n=&'%)
3%
49%38%
10%
!"#" !"##COMMISSIONING$WHAT HAPPENED WHEN
>>> >>> >>> >>> >>>>

No o
f GPs
!
"!!
#!!
$!!
%!!
Consult with or advise a private company or drug company
&!! Key
Types of interests registered by GPs on CCG boards
Employed by a private company (aside from their GP practice)
Declared a conflict of interest relating to a family member
Personal links with not for pro't voluntary or social enterprise organisations
Directors or have shares in privatecompanies
426
144
106
55 43
BMJ INVESTIGATION
The NHS Commissioning Board has issued rules to CCGs stating that board members must remove themselves from decisions from which they could materially bene! t. "
Some CCGs have responded to this by includ-ing a provision to co-opt additional members if doctors on the governing body have to remove themselves from decisions. Others have increased the number of lay members on boards to try to alleviate potential con# icts.
But doctors’ leaders have expressed concern that clinical input into commissioning deci-sions might become diluted if too many doc-tors were forced to remove themselves from particular decisions.
CCGs with notable conflicts Governing bodies with notable con# icts include NHS Leicester City CCG, where seven GPs on the board have a financial interest in the LLR (L eicester, Leicestershire and Rutland) GP Provider Company; NHS Oldham CCG, where ! ve of the eight GPs have an interest in the provider Primary Care Oldham LLP; and NHS Blackpool CCG, where six of the eight GPs have an interest in the local out of hours provider Fylde Coast Medical Services.
Ian Wilkinson, a GP and chief clinical o$ cer at NHS Oldham CCG, who does not have a ! nan-cial stake in a private provider company, said that the CCG’s board had also recruited addi-tional lay and clinical members to ensure that decisions could be made if members needed to remove themselves. He added that so far no voting members had removed themselves from governing body or committee proceedings.
Richard Gibbs, a lay board member at NHS Southwark CCG, told the BMJ that his CCG had attempted to deal with con# icts by appointing him as a “guardian” who would judge when it might be appropriate for members to remove themselves from decisions (box).
A spokeswoman for Leicester City CCG said that a signi! cant proportion of its local general practices were members of the LLR GP Provider Company and said that it would co-opt mem-bers from neighbouring CCGs if its governing body were con# icted. She said, “They have to remain neutral, so we would bring in members from our fellow CCGs—East Leicestershire and Rutland/West Leicestershire—or bring in a GP member from a neighbouring county such as Northamptonshire.”
In NHS Chiltern CCG, in Buckinghamshire, two of the three GPs on the governing body hold shares in the for-pro! t provider Chiltern Health, while in NHS Aylesbury Vale CCG, also in Buck-inghamshire, both GP voting members of the board have interests in the private provider Vale Health. In NHS Southwark CCG, in London, ! ve of nine GPs on the governing body have a stake in various for-pro! t provider companies.
All these CCGs told the BMJ that they had robust systems in place for managing potential con# icts, including publishing their policies on con# icts of interest and regularly updating mem-bers’ declarations of interest.
Amanda Doyle, a GP and chief clinical o$ cer at NHS Blackpool CCG, told the BMJ that her CCG had sought to tackle potential con# icts by opting to double the number of lay members on its governing body from the minimum set by the government, including a lay chairperson (box).
Doyle acknowledged that most of the GPs on the board would have to “step away” if the local out of hours service were to be retendered. But she warned that the bene! ts of having doctors leading commissioning might be lost if con# icts of interest gained too much attention.
BMJ | 16 MARCH 2013 | VOLUME 346 5
September !"## RCGP and NHS Confederation, the membership body for organisations that commission and provide NHS services, publish joint guidance on “managing confl icts of interest in clinical commissioning groups” (BMJ Careers, http://bit.ly/W7y9wK ).
!"#! !"#$>>> >>> >>> >>> >>>>
February !"#! House of Lords agrees amendments to the Health and Social Care Bill stating that CCGs would have to publish registers of board members’ interests ( http://bit.ly/ wqDqVP ).
June !"#! NHS Commissioning Board Authority publishes a code of conduct. This states that members must remove themselves from decisions from which they could materially benefi t
October !"#!
The private sector company Virgin Care, owned by Richard Branson (top right), announces plans to dissolve its joint venture provider partnerships
with GPs, in response to concerns from GPs over confl icts of interest in the new commissioning landscape ( BMJ 2012;345:e7227).
November !"#!
NHS Commissioning Board rejects a call from GP commissioning leaders for confl icts of interest to be treated with leniency ( BMJ 2012;345:e7967).
February !"#$ In its response to its consultation “Securing the Best Value for Patients,” health department says that it will strengthen the powers of Monitor, headed by David Bennett (right), to act where confl icts “may affect the integrity of a commissioner’s decision.”

6 BMJ | 16 MARCH 2013 | VOLUME 346
BMJ INVESTIGATION
A spokesman for NHS Chiltern CCG said that the group had co-opted additional members to a decision making panel for the recent procure-ment of a GP led minor illness and injury unit where there was “potential for perceived con!ict of interest,” while NHS Aylesbury Vale CCG said that it had written the ability to co-opt members into its constitution.
Declaring an interest “not enough”However, despite the measures being taken, James Kingsland, the government’s national clinical lead for NHS clinical commissioning and a GP on Merseyside, said that he believed some doctors on local commissioning boards should step down from one of their roles if they had a substantial stake in a local private healthcare company, because their con!icts were too acute.
He said, “If it is somebody who has got a major stake in some of the provider services which the CCG commissions, I don’t think excluding [himself or herself] or declaring an interest is enough—not for the public. I think they have got to step down.”
Kingsland said that his stance had been criti-cised by some doctors, who were concerned that forcing people to step down could lead to a short-age of clinicians willing to sit on CCG boards.
But he said, “That isn’t an excuse to allow con-!ict to go. If they are enthusiasts as both senior provider and senior commissioner, my answer would be: make your choice and be accountable for that choice.
“If you can justify a marginal amount of con-!ict that can be declared and managed, then "ne. If you can’t marginalise a con!ict, and you are excluding yourself from the board week in, week out because you’ve got an interest, ultimately it becomes unaccountable. Where you draw the line is di#cult; if somebody is going to be the arbiter of that, it should be the public.”
The “local newspaper test”Michael Dixon, chairman of the NHS Alliance, which represents organisations and individual professionals in primary care, has previously called for “more leniency” in handling con!icts of interest in the new system.$ He warned that placing too much emphasis on the issue might prevent clinical commissioners from bringing more care into community settings.
He said, “The priority is to move services out of hospital and into primary care. The reason this hasn’t happened to date is because of blocks in the system. It’s more important to remove those blocks than be preoccupied with conflicts of interest. Dixon said that he believed that “trans-parency is all you need” to handle con!icts and urged doctors to use “the local newspaper test” when assessing their own interests: “You have
got to be happy for everything you do as a GP and a commissioner to appear on the front page.”
Chaand Nagpaul, the BMA’s lead GP negotia-tor on commissioning and a GP in Harrow, called for the NHS Commissioning Board to issue more robust guidance on handling con!icts.
“The Commissioning Board’s guidance has not gone far enough. Their guidance is all about declaring and managing con!icts, rather than recognising that some con!icts of interest are too great,” he said.
Nagpaul said that he supported the idea of CCGs co-opting additional members to help make decisions where con!icts existed, but he said that it was crucial that this extra help did not just focus on lay members, as it could “dilute” clinical commissioning.
“It would undermine the whole concept of clinically led commissioning to not have clinical input,” he warned.
A spokeswoman for the NHS Commissioning Board said that it had already published “com-prehensive guidance” on managing con!icts of interest, which “clearly sets out that the decision on whether an individual’s con!icts of interest are likely to be so great as to preclude them from taking a role on the governing body should be made by the CCG.”
But she said that the board was reviewing its
existing guidance and would shortly be publish-ing “"nal, comprehensive guidance on managing con!ict of interest.”
Strengthening the rulesThe Department of Health acknowledged in its response to its consultation “Securing the Best Value for Patients” that concerns about con-!icts needed to be answered, and it pledged to strengthen the power of the healthcare regula-tor Monitor to act where con!icts “may a%ect the integrity of a commissioner’s decision.”&
The department said that this would mean that “Monitor is able to take action where con-flicts have not been managed appropriately in awarding a contract, and not only where M onitor is able to establish that the decision to award a contract was the result of an interest in the p rovider.”
Niall Dickson, chief executive of the General Medical Council, said that there were “no new principles involved” as far as doctors’ ethical conduct was concerned. He added, “The con-siderable additional responsibilities about to be undertaken by GPs does mean that some face con!icts of interests more o'en than in the past. We expect doctors to be open about any "nancial and commercial interests linked to their work.”Cite this as: BMJ !"#$;$%&:f#'&(
NHS Blackpool CCG
NHS Southwark CCGRichard Gibbs, lay member of the board of the NHS Southwark CCG, said that his group had tried to tackle potential conflicts by appointing him as a “guardian”—with the remit of exercising judgment on when it might be appropriate for members to remove themselves from decisions.
Gibbs, who has no financial interests in any private providers, said that the CCG had also set up a three person evaluation
panel, comprising himself, the chief officer, and the director of public health, to arbitrate on commissioning decisions where two or more members have to remove themselves from decisions because of conflicts.
“We have convened the panel on three or four occasions,” Gibbs said. “If we needed to get additional expertise then we would co-opt in someone who isn’t conflicted, presumably from outside Southwark.”
Amanda Doyle, chief clinical officer at NHS Blackpool CCG, who has declared an interest in the local provider of out of hours services, said that her CCG had sought to deal with potential conflicts by opting to have four lay members on its governing body—double the minimum set by the government—including a lay chairperson.
“We were very conscious of the need to demonstrate that we were not letting conflicts interfere with our decisions,”
she explained.But Doyle added that it was
important to strike a “balance” between managing conflicts appropriately and “ensuring that we get a full range of clinical input into service redesign and commissioning decisions.”
She warned, “There is a risk of getting so tied up with worrying about conflicts of interest that you don’t go ahead and reap the benefits of having clinicians leading commissioning.”
Doyle acknowledged that most
GPs on the board would have to step away if the local out of hours service were to be retendered. She said that it was “unlikely” that the board would co-opt additional clinicians onto the board in such a case but said that it may take “clinical input and advice” from outside the area if this was needed.
TACKLING THE ISSUE OF CONFLICTS OF INTEREST

BMJ | 16 MARCH 2013 | VOLUME 346 7
Editorials are usually commissioned. We are, however, happy to consider and peer review unsolicited editorials ! See http://resources.bmj.com/bmj/authors/types-of-article/editorials for more details
EDITORIALS
Is an EMA review of hormonal contraception and thrombosis needed?Sufficient evidence exists to recommend lightest tolerable second generation pill for all indications
Frans M Helmerhorst professor in clinical epidemiology of fertility [email protected] R Rosendaal professor in clinical epidemiology, Leiden University Medical Center, !"## RC Leiden, Netherlands
Four recently reported deaths in women using the Diane-35 contraceptive and a lawsuit against the French drug authority (L’Agence Nationale de Sécurité du Médicament) a#er it banned Diane-35 led the authority to request that the European Medicines Agency (EMA) review the safety of combined oral contraceptives.1 2 Of particular concern were third and fourth generation drugs, including Diane-35 and its generics. This review was granted on 7 February 2013.3 4 The Dutch College for the Evaluation of Medicines (Dutch “EMA”) decided that a new study on Diane-35 was in order.
Most oral contraceptives are combination preparations, containing a progestogen, to prevent ovulation, and an oestrogen to prevent breakthrough bleeding. Since the introduction of the pill, the oestrogen dose, in the form of ethinyl estradiol, has been reduced (heavy v light pills) and the type of progestogen has changed several times (indicating the generation). The categorisation is imprecise and incomplete. For example, cyproterone acetate, the progestogen in Diane-35, does not belong to a generation. Furthermore, the categorisation assumes that all side e*ects of oral contraceptives are class e*ects. In our recent network meta-analysis of all combined oral contraceptives (unpublished data), we found that the risk of venous thrombo-sis depended on the dose of oestrogen and the type of progestogen, even within generations.
Many studies have shown that oral contra-ceptive users have an increased risk of venous thrombosis (deep vein thrombosis, pulmonary embolism) and arterial thrombosis.5 6 Venous thrombosis is more common than arterial throm-bosis, but in young women the incidence of these side e*ects is low. Even the “safest” oral contra-ceptive increases the risk of venous thrombosis, however, and the risk is twice as high for oral
contraceptives containing a third generation progestogen, drospirenone (sometimes called fourth generation), or cyproterone acetate.5 This knowledge is not new—the increased risk for pills containing third generation progestogens, cyproterone acetate, and drospirenone has been known since 1995, 2001,7 and 2003, respec-tively.8
The EMA’s public report at the beginning of the review states that Diane “works by blocking the e*ects of a class of hormones called androgens,”3 and that this is responsible for its supposed ben-e.ts on acne and hirsutism. However, as early as 2004 (and in three updates) a systematic review concluded that all types of monophasic com-bined oral contraceptives are e*ective against acne.9
All combined oral contraceptives are equally effective in preventing pregnancy. Their side e*ects (such as weight gain10) and bene.ts (in terms of acne and hirsutism) are also similar, so the only rational strategy is to use the safest one with regard to venous thrombosis. The common arguments that the risk of thrombosis is low or that the risk of thrombosis during pregnancy is higher than when using oral contraceptives are flawed. Millions of women in Europe use oral contraceptives, so use of the pill with the best safety pro.le in terms of thrombosis would
probably prevent thousands of thrombotic events and hundreds of deaths a year. Because the pill with the safest thrombosis pro.le is as e*ective at preventing pregnancy as the less safe ones, the risk of thrombosis in pregnancy is irrelevant in the choice of oral contraceptive. The safest oral contraceptive is one that contains the low-est tolerable dose of ethinylestradiol (lowest dose that prevents breakthrough bleeding—30 μg11) together with the second generation pro-gestogen, levonorgestrel.
Sufficient evidence is already available on which clinicians and regulatory agencies can base their decisions, so lengthy evaluations, let alone new studies, are not needed.
In his 2011 BMJ editorial, Nick Dunn recom-mended prescribing an oral contraceptive that contains levonorgestrel unless “there is a persist-ent reason to use another type.”12 Because oral contraceptives containing levonorgestrel and the lowest tolerable dose of oestrogen are also adequate for the treatment of acne or hirsutism, we can see no reason to use another type. Third and fourth generation oral contraceptives are widely overprescribed.Competing interests: None declared.Provenance and peer review: Commissioned; not externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ "#$%;%&':f$&'&
Response on bmj.com“It is wise to consider all of the many serious conditions caused by use of hormonal contraception including the increased risks of suicide and breast cancer.” Ellen CG Grant, retired medical gynaecologist, Kingston-upon-Thames, Surrey
! Visit the article online and click “Respond to this article” to have your say.
French drug authority L’Agence Nationale de Sécurité du Médicament recently banned Diane-35
BSIP
, B B
OISS
ONNE
T/SP
L

8 BMJ | 16 MARCH 2013 | VOLUME 346
EDITORIALS
Cognitive deficits and mild traumatic brain injury New study identifies risk factors and raises questions about the nature of any implied causal association
V F J Newcombe academic clinical fellow in emergency and intensive care medicine D K Menon professor of anaesthesia, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge CB! !QQ, UK
Between !% and ""% of patients who have “mild” traumatic brain injury (sometimes called concussion) develop persistent post-concussion syndrome, which may last weeks to months a#er injury.$ More than $%% have a measurable cognitive de&cit at one year.' " There is grow-ing interest in the syndrome of post-traumatic encephalopathy,( % which may follow a blast injury or repeated sports related concussion. However, despite this growing literature on the cognitive consequences of mild traumatic brain injury, our knowledge of risk factors that predis-pose people to sustaining such injury is limited.
In a linked paper, Nordström and colleagues examine the associations and temporal associa-tions between a history of concussion, cognitive function, academic achievement, and measures of social wellbeing in a cohort of more than ")) ))) Swedish conscripts.* Given the paucity of data on premorbid neurocognitive testing in traumatic brain injury, this paper draws on an impressively large dataset that allows comparison of neurocognitive function before and a#er such injury in a nationwide cohort of Swedish men.
The results complement an earlier study from the same group, which examined the association between cognitive performance and incidence of a subdural haematoma.That study concluded that low global intelligence in adolescence was a risk factor for subsequent development of a subdural haematoma.
Although the current study investigates a more common diagnosis, case ascertainment was probably less precise than the more clearly de&nable endpoint of subdural haematoma. The case ascertainment of “concussion” that the authors used was based on the International Classi!cation of Diseases and probably repre-sents the best epidemiological approximation achievable in the administrative databases that were searched. However, a substantial propor-tion of patients with mild traumatic brain injury are never admitted to hospital or seen in the outpatient setting. Therefore, this study prob-ably underestimated the incidence of this con-
dition in the study population. Conversely, the approaches used may not have fully excluded subjects who sustained a moderate or severe injury. Cross correlating multiple sources of data could mitigate against this source of confound-ing, which is common when administrative data-sets are analysed.+
Despite these caveats related to case ascertain-ment, Nordström and colleagues’ study provides unique insights into the epidemiology of mild traumatic brain injury. Unsurprisingly, poor cog-nitive function, low educational status, and other risk factors were associated with mild traumatic brain injury. However, surprisingly, the associa-tion between cognitive function and concussion did not depend on the temporal association between the two and was just as common when poor cognitive performance preceded concus-sion. In addition, similar cognitive scores were seen before and a#er injury in twins discordant for mild traumatic brain injury, which suggests that both genetic and environmental in,uences contributed to the low cognitive function found. Other strong independent (but not unexpected) risk factors for development of mild traumatic brain injury included a previous episode of brain injury, hospital admission for intoxication, and low education and socioeconomic status. Sur-prisingly, the analysis found no signi&cant di-er-ences in cognitive performance before and a#er
the index event in men who sustained an injury.These results are important for several rea-
sons. Firstly, they identify potential risk factors for mild traumatic brain injury and could help guide attempts to investigate prevention strate-gies, perhaps through education initiatives (par-ticularly in accessible populations such as the military conscripts investigated here). Secondly, they provide a context for interpreting studies that measure cognitive function a#er injury only and compare it with matched controls from the general population, with the assumption that those with brain injury have similar pre-injury characteristics to the general population. The results of this study suggest that such assump-tions may be incorrect. Finally, those who subse-quently sustained a mild traumatic brain injury had similar cognitive performance to that of those who had previously sustained such an injury, which implies that the injury itself may not reduce cognitive function. However, the tests used (word recollection; visuospatial geometric perception; logical and inductive performance; and mathematical and physics problem solving) have not been validated as sensitive measures of changing performance in cognitive areas thought to be a-ected by mild traumatic brain injury. These tests may therefore have missed important changes.
It is important that additional studies attempt to replicate these &ndings. Suitable populations for such studies include other military cohorts and cohorts of people who practise contact sports, which are associated with a relatively high incidence of mild traumatic brain injury. Such studies must take account of “gaming” by soldiers and sportspeople, who allegedly choose to perform suboptimally on pre-injury cognitive screening to hide evidence of any post-injury cognitive decrement, thus enabling them to stay with their units and teams. Although it may not be easy to control for such confounding, more studies like the current one will increase our understanding of the epidemiology, patho-physiology, and outcome impact of traumatic brain injury.Competing interests: None declared.Provenance and peer review: Commissioned; not externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#'!!
bmj.com ( Neurology updates from BMJ Group are at www.bmj.com/specialties/neurology
Poor cognitive performance linked to concussion
JAM
ES D
AVIE
S/AL
AMY

BMJ | 16 MARCH 2013 | VOLUME 346 9
EDITORIALS
Regulating the NHS market in EnglandThe government must make its intentions clear as it rewrites the regulations on competition
Chris Ham chief executive, King’s Fund, London W!G "AN, UK [email protected]
The government’s dra! regulations on procure-ment, patient choice, and competition, pub-lished in February, have opened up old wounds in the debate about NHS reform. The regulations set out in detail how commissioners should pro-cure NHS services under section 75 of the Health and Social Care Act 2012. The stated aim of the regulations, which will be enforced by Monitor as the economic regulator, is to ensure that the NHS Commissioning Board and clinical commis-sioning groups act to protect patients’ rights and to prevent anti-competitive behaviour.1
The government claims that the regulations follow from commitments given during the passage of the 2012 act and are consistent with the “Principles and rules for cooperation and competition” put in place by the previous administration. Its critics contend that they go much further and represent a major extension of market principles in the NHS. In this they are supported by legal advice, which argues that commissioners of NHS services will be expected to make greater use of tendering, with competition becoming “the norm for placing NHS c ontracts.”2
The government’s critics comprise general practitioner leaders who are worried that clini-cal commissioning groups will have to use ten-dering to procure all services; Liberal Democrat MPs and peers who fear this will make it more di'cult to promote integrated care; and oppo-sition politicians who interpret the regulations as con(rmation that ministers are hell bent on opening the NHS up to the private sector. In the face of these concerns, the government has announced that it will amend the regulations to ensure that they are not open to misinterpre-tation. Statements made by ministers indicate that this means commissioners will not have to tender all services, Monitor will not force com-missioners to tender competitively, and compe-tition will not take precedence over cooperation and integration.3
The decision to make these changes less than a month before the provisions of the 2012 act come into e*ect is embarrassing for the govern-ment. It re+ects both the in+uence of the Liberal
Democrats within the coalition and the need to retain the support of GP leaders, who will play a key role in the work of clinical commission-ing groups. If these leaders had walked away at this stage, the edi(ce on which the reforms are based might well have crumbled to the ground even before it had come into being.
Underlying the debate about the precise wording of the regulations is the more impor-tant question of the government’s intentions regarding the role of markets in the NHS. On this question there is room for legitimate doubt in the light of the debate on the 2012 act and the amendments made a!er the work of the NHS Future Forum. Particularly important was the change to Monitor’s role from an original duty to promote competition to a revised duty to pro-tect and promote the interests of people who use healthcare services, and in so doing to prevent anti-competitive behaviour.
These amendments may have watered down Andrew Lansley’s ambitious plans to apply market principles to the NHS, but the architec-ture of economic regulation set out in part 3 of the 2012 act remains in place. A key element in this architecture is the role that the O'ce of Fair Trading (OFT) and the Competition Commission will play in the future NHS. In the debate about the regulations, the involvement of the OFT in assessing the proposed merger of two NHS foun-dation trusts in the south of England has gone largely unnoticed. The OFT is also investigating the proposed merger of an NHS foundation trust and an NHS trust in Torbay, which is designed to bring about closer integration of services in an area well known for its innovative approach to the care of older people.
The question this raises is whether this kind of market regulation is needed in the NHS in addition to the new role of Monitor? There are many di*erences between healthcare and the industries that OFT and the Competition Com-mission regulate, and there is a danger that regulators with experience in other sectors will adopt an approach that is not sensitive to these di*erences. Overexuberant regulation of merg-ers could delay the implementation of service changes that may bene(t patients—for example, by preventing the full integration of care as is being proposed in Torbay.
It is worrying that fundamental questions of this kind are unresolved so close to the date of implementation of the reforms. Evidence that competition in healthcare is bene(cial is both equivocal and contested.4 5 Even where bene(ts can be delivered, these have to be set against the considerable transaction costs involved in con-tract negotiations between commissioners and providers and the work of the regulators. The well known limits to markets in healthcare mean that planning, collaboration, and clinical networks6 should also play a major role in bringing about improvements in care.
Where markets are used, regulators need to be sensitive to the di*erent forms of competition in healthcare. Competition in the market has a role in situations where patients have the time and inclination to decide where to obtain treatment—for example, when receiving planned care. Com-petition for the market should be the preferred approach when commissioners want di*erent providers to work together under long term con-tracts to deliver integrated urgent care and care for groups such as older people and those with complex needs.7 A nuanced approach that com-bines the right kind of competition alongside planning, collaboration, and clinical networks, where appropriate, is most likely to deliver the desired results.
If GP leaders and Liberal Democrats are to withdraw their opposition, the government needs to provide reassurance on its intentions with regard to regulating the NHS market. To avoid doubt, ministers must be explicit about the place of markets in the NHS, including the role of the OFT and Competition Commission, when they publish the revised regulations. Without absolute clarity on these questions, there is a risk of uncertainty and misinterpretation by the com-missioners and regulators tasked with making the regulations and the 2012 act work in practice.
There is also every possibility that old wounds will not heal and will cause even deeper ri!s within the coalition, which will create politi-cal difficulties for the government as well as u nwelcome confusion for the NHS.Competing interests: None declared.Provenance and peer review: Commissioned; not externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#&"'
Underlying the debate about the precise wording of the regulations is the much more important question as to the government’s intentions on the role of markets in the NHS

10 BMJ | 16 MARCH 2013 | VOLUME 346
EDITORIALS
The new UK antimicrobial resistance strategy and action planA major societal, political, clinical, and research challenge
New challenges will include screening (by rec-tal swab) and isolation of any patient admitted to the NHS who has received inpatient care outside the UK, with rigorous control of any outbreaks of multidrug resistant infection inside the NHS. Acute trusts and their boards will need to con-sider how to strengthen infection prevention and control practice using new methods of organisa-tional and behavioural change.
Antimicrobial prescribing needs to be more evidence based and more e!ciently targeted. New NHS initiatives to provide antimicrobial stewardship guidance in secondary care (Start Smart then Focus) and primary care (TARGET antimicrobial toolkit)" need to develop into more formal quality indicators.
This strategy makes the UK the #rst country to explicitly announce its intention to develop national outcome measures in AMR using speci#c drug-bug combination resistance rates (for example, rates of E coli resistance to third generation cephalosporins). This is a brave move and should be welcomed. The chief medical o!cer has taken a clear leadership role by tackling the international dimensions of the problem, adding AMR to the Department of Health risk register and calling for AMR to be added to the national risk register (National Security Risk Assess-ment) to promote cross government action. Impor-tant areas that will be covered include antimicrobial use in animals and new initiatives to encourage the development of novel antimicrobials.$
The wider application of molecular microbiol-ogy, particularly whole genome sequencing, to detect clonal spread of MDR Gram negative bacteria within hospitals is providing a rapid explosion of new data. It is still unclear if this will lead to e%ec-tive new control policies. The research agenda is extensive, but the NHS information technology and National Institute of Health Research infrastruc-tures are well placed to provide global leadership in this area.& New technology focusing on rapid diagnosis of speci#c bacteria and resistance genes, along with combination biomarkers indicating bacterial or viral infections, especially if adapted to near patient testing, could have a major impact on targeting appropriate antibiotic treatment. Improved surveillance by Public Health England, using large dataset linkage combined e!ciently with observational studies focused on clinical out-comes, including all infection related deaths, will also help to de#ne new targets for intervention.Competing interests are in the version on bmj.com.Provenance and peer review: Not commissioned; externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#&"#
Anthony S Kessel honorary professor, Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, UK Mike Sharland professor in paediatric infectious diseases, Paediatric Infectious Diseases Research Group, St George’s University London, London SW!" #RE, UK [email protected]
This week the chief medical o!cer highlighted in her report how the rise of antimicrobial resistance (AMR) poses a threat to healthcare delivery in the United Kingdom.$ This will be followed shortly by the Department of Health’s new UK Five Year Anti-microbial Resistance Strategy and Action Plan, which will re'ect the need for a clear change in the understanding and response to AMR by the public, the NHS, and the government in the UK. The rise of AMR as a serious health threat is due to the inter-national spread of multidrug resistant (MDR) Gram negative bacteria, the global overuse of antibiotics in humans and animals, and the almost complete lack of new antibiotic development.( All of these are now of direct concern to the NHS.
The ")% reduction in rates of meticillin resistant Staphylococcus aureus (MRSA) bloodstream infec-tions seen in England between (**+ and (*$$ has been remarkable. MRSA is now responsible for less than (% of all bloodstream infections in England. Less remarked on has been the inexora-ble rise in the number of bloodstream infections attributable to Gram negative organisms (particu-larly Escherichia coli), which now comprise more than half of the around $** *** of these infections reported in England annually.+ Most large NHS hospitals now identify )*-$** times more patients with Gram negative bloodstream infections than those with MRSA, with antibiotic resistance rates of $*-(*% and mortality rates of +*% reported for MDR forms., In England the successful introduc-tion of conjugate pneumococcal vaccine means that the number of reported Klebsiella pneumoniae bloodstream infections in England is now higher than for Streptococcus pneumoniae.
In many European countries AMR rates are much worse. In (*$$ the European Centre for Disease Pre-vention and Control reported a signi#cant increase in multidrug resistant E coli and K pneumoniae (for example, resistance to third generation cepha-losporins, 'uoroquinolones, and aminoglycosides) in more than a third of European Union/European Economic Area countries.) Klebsiella is an impor-tant pathogen in the spread of resistance. Many anti-biotic resistance genes group together in plasmids easily transferred between bacteria, with particular clones carrying multiple resistance genes (for exam-ple, OXA-," and CTX-M$)). Many EU countries are now reporting Klebsiella MDR rates of ()-,*%.
Globally, rates of MDR Gram negative bacterial infection can be even higher.- This has inevita-bly led to a rapid rise in the use of carbapenem antibiotics (for example, meropenem) as empiri-cal treatment for suspected sepsis. In turn, this has led to a rapid increase in hospital outbreaks of carbapenemase producing organisms, which are usually sensitive to only one or two older less e%ective antibiotics. In the UK, there has also been a sharp rise in meropenem use and increasing reports of carbapenemase producing organisms. Only one or two new antibiotics that target Gram negative organisms are likely to be marketed in the next decade (http://antibiotic-action.com), which raises the concern that virtually untreatable i nfections will threaten routine NHS care..
The new UK strategy is an important step in rec-ognising and responding to these concerns. At its core the strategy recognises that AMR, infection prevention and control, and antimicrobial steward-ship are closely interconnected and all need to be strengthened. The seven aims (table) re'ect that all individuals and organisations have unique roles and responsibilities. Enhanced infection preven-tion and control are crucial to limiting the spread of MDR Gram negative bacteria, both into and across the NHS.
UK antimicrobial resistance strategy: seven action areas and likely stakeholder involvement in the health sectorSeven key areas of focus StakeholdersPromote responsible evidence based prescribing
Individual prescribers, NHS providers, national and local commissioning boards, ARHAI, PHE, Department of Health, professional bodies
Improve infection prevention and control
Individual clinical staff, NHS providers, national and local commissioning boards, ARHAI, Department of Health, PHE, professional bodies
Raise public and professional awareness of antimicrobial resistance threat and promote behaviour change
Professional bodies, Department of Health, ARHAI, patient groups
Research programme into new diagnostics, alternatives to antibiotics (such as antiseptics), pathogenesis, effective behavioural change to improve infection prevention and control and prescribing practice
NIHR, universities, Department of Health, ARHAI
Facilitate development of new antimicrobials, vaccines, and immunomodulators
Department of Health, drug industry, European Union
Improve surveillance and data linkage
PHE, ARHAI, Department of Health
Encourage international collaboration and data sharing and learning from best practice internationally
Department of Health, PHE
ARHAI=Department of Health Expert Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection; PHE=Public Health England. NIHR=National Institute for Health Research.

BMJ | 16 MARCH 2013 | VOLUME 346 11
The BMJ is an Open Access journal. We set no word limits on BMJ research articles, but they are abridged for print. The full text of each BMJ research article is freely available on bmj.com
Scan this image with your smartphone to read our instructions for authorsRESEARCH
RESEARCH NEWS
RESEARCH NEWS All you need to read in the other general medical journals Alison Tonks, associate editor, BMJ [email protected]
violence has le! us without the means to "nd out. These authors did what they could with the data available, but the data are woefully inadequate in the face of an epidemic of gun violence that has killed more than #$$ $$$ US citizens since %$$& and seems to be intensifying. No more than a handful of researchers are currently working in the "eld, thanks to a concerted political e'ort by the National Ri(e Association in the early &))$s, says the editorial. Research must resume now, to deepen our understanding of this complex prob-lem and "nd ways to "x it.JAMA Intern Med !"#$; doi:#".#""#/jamainternmed.!"#$.#!%&Cite this as: BMJ !"#$;$%&:f#'("
Six women pilot deep brain stimulation for anorexia nervosa
Six women with intractable and life threatening anorexia nervosa have been treated with deep brain stimulation in a preliminary study from Toronto, Canada. Doctors selected the women for deep brain stimulation a!er many years of unsuc-cessful conventional management. They had average body mass indices (BMIs) of && to &* in the years leading up to the study, accompanied by multiple medical complications of chronic starva-tion. Five had psychiatric comorbidities, most o!enmajor depression and obsessive compulsive disorder.
Surgeons placed electrodes just beneath the corpus callosum. One patient had a self limiting panic attack during the local anaesthetic phase of the procedure and one developed a cardiac air embolus that resolved within "ve minutes a!er the operating table was repositioned. A third patient had a seizure during device programming two weeks a!er the procedure. It was switched o' then restarted one week later with no further problems.
Three of the six women gained weight during nine months of stimulation (BMIs increased from &&.& to %&, &+.% to &,, and &*.& to %$). They also reported improved quality of life. Symptom scores measuring mood, anxiety, and anorexia nervosa related obsessions and compulsions improved in four patients.
The pilot was designed to assess safety, not e'ectiveness. The authors judge deep brain stim-ulation to be safe enough for further evaluation.Lancet !"#$; doi:#".#"#&/S"#'"-&($&(#!)&!#%%-&Cite this as: BMJ !"#$;$%&:f#'&&
Treating depression after acute coronary syndrome
Depression is common a!er hospital admission for acute coronary syndrome and international guidelines recommend screening and treat-ment. A recent trial tested a programme of care that allowed people with depression symptoms to choose between psychotherapy, antidepres-sant drugs, or a combination of the two. The programme worked well, reducing symptoms signi"cantly more than usual care over six months (an extra #.* point drop in Beck depression inven-tory score, )*% CI -,.& to -$..).
All &*$ participants had symptoms of depression two to six months a!er treatment for acute coronary syndrome. Among .# assigned to the new programme, +& chose psychotherapy, nine chose drugs, and &. chose the combina-tion. Their care was organised by a remote team of mental health professionals who met once a week to discuss cases and advise a local doctor or nurse prescriber. A centralised team also provided psychotherapy (problem solving therapy) over the telephone or by video link and followed a stepped care algorithm that intensi"ed treatment every six to eight weeks if required.
This programme contained all the elements known to work from previous trials and intro-duced the idea that organisation, coordination, and support does not have to be local to be suc-cessful, says a linked comment (doi:&$.&$$&/jamainternalmed.%$&#.)%*).JAMA Intern Med !"#$;doi:#".#""#/jamainternalmed.!"#$.)#*Cite this as: BMJ !"#$;$%&:f#'&(
“Whole mummy” scans confirm ancient atherosclerosis
An international team of researchers has found clear evidence of atherosclerosis among &#. mummies from diverse ancient cultures. Com-puted tomography showed vascular calci"cation in %) of ., mummies from ancient Egypt, &# of *& from ancient Peru, two of "ve mummies from a Puebloan people who lived in south west America between &*$$ BC and AD &*$$, and three of "ve mummies from a population of hunter gatherers who lived more recently on remote islands *$$ miles o' modern day Alaska.
Overall, a third of the mummies examined had de"nite or probable atherosclerosis in at least one vascular bed, usually more. Two mummies had disease in all "ve vascular beds—an ancient Egyptian princess, Ahmose-Meritamun, who died in early middle age, and a slightly older woman from the Aleutian islands who would have been a hunter gatherer eating mainly "sh and shell "sh.
The researchers and a linked comment agree that atherosclerosis is not as modern as we think it is (doi:&$.&$&,/S$&+$-,.#,(&#),$,#)-X). Sim-ilar disease was common in geographically and culturally di'erent populations that spanned at least +$$$ years of human history.Lancet !"#$; doi:#".#"#&/S"#'"-&($&(#$)&"*)%-XCite this as: BMJ !"#$;$%&:f#')#
Stronger gun laws, fewer deaths
US states with the strongest gun laws have the lowest rates of death caused by "rearms, accord-ing to a nationwide cross sectional analysis. The authors ranked *$ states using a score of legis-lative strength that counted then weighted gun control laws up to a maximum score of %/. States in the highest quarter, such as Massachusetts and Illinois, had ,., fewer deaths per &$$ $$$ each year than states in the lowest quarter, such as Louisiana and Utah (incident rate ratio $.*/, )*% CI $.#. to $.)%). The di'erence survived multiple adjustments for state demographics, including poverty and population density.
Did gun control save those extra lives? It’s impos-sible to say, says a linked editorial (doi:&$.&$$&/jamainternmed.%$&#.&%)%). The systematic and deliberate erosion of funding for research into gun
Adapted from JAMA Intern Med !"#$; doi:#".#""#/jamainternmed.!"#$.#!%&
Legislative strength and mortality by state
!.'-%." %.#-#".# #".!-#$." #$.#-#%."
III
III
III IIIIII
III
III
III
IIII
I
I
I
II
IIII
IIIII
III
IIIIII
II
II
II
II
II
II
I
I I I
I
II I
IIIV
IVIV
IVIVIV
IVIVIVIV
IV
IVI
II
Hawaii
Mortality rate per !"" """, mean
First quarter: "-# lawsSecond quarter: $-% laws
Third quarter: &-' lawsFourth quarter: (-#% laws
Legislative strength score, median
Alaska
IV
I
I

12 BMJ | 16 MARCH 2013 | VOLUME 346
RESEARCH
Correspondence to: P Bower, NIHR School for Primary Care Research, Manchester Academic Health Science Centre, University of Manchester, Manchester M!" #PL, UK [email protected] this as: BMJ !"#$;$%&:f'%"doi: !$.!!"%/bmj.f&'$
Details of the authors’ affiliations are given in the full article on bmj.comThis is a summary of a paper that was published on bmj.com as BMJ ($!";"'%:f&'$
STUDY QUESTION Do patients with more severe depression benefit less from “low intensity” psychological therapy than those with milder depression?
SUMMARY ANSWER No, patients with more severe depression show at least as much clinical benefit from low intensity interventions as less depressed patients.
WHAT IS KNOWN AND WHAT THIS PAPER ADDS To better manage the high prevalence of depression in the community, many services seek to provide simple forms of psychological therapy (low intensity interventions), but whether patients with more severe depression are suitable for such interventions is not known. We found no clinically meaningful differences in treatment effects between more and less severely ill patients receiving low intensity interventions.
SELECTION CRITERIA FOR STUDIES We searched published systematic reviews, updated with a search of the Cochrane Library, for randomised controlled trials of low intensity interventions (such as interventions provided through written materials or the internet with limited professional support) in patients with depression.
Primary outcome(s)Our primary outcome was the relation between initial depression severity (measured with the Beck Depression Inventory or Center for Epidemiologic Studies Depres-sion Scale) and the amount of clinical bene!t (change in depression score) that patients received from low intensity interventions.
Main results and role of chanceWe used individual patient data from "# trials including $%&' patients. We found a signi!cant interaction between baseline severity and treatment e(ect (coe)cient *'." (+,% CI *'."+ to *'.''$)), suggesting that patients who are more severely depressed at baseline demonstrate larger treatment e(ects from low intensity interventions than those who are less severely depressed. However, the magnitude of the interaction was small and may not be clinically signi!cant.
Bias, confounding, and other reasons for cautionWe were unable to access all published data on low inten-sity interventions, obtaining individual patient data from just over half of the $+ eligible studies. Although we found no clinically meaningful di(erences in treatment e(ects between more and less severely ill patients receiving low intensity interventions, patients with more severe depres-sion are more likely to continue to show clinically signi!-cant levels of distress a-er low intensity treatments and may require additional care.
Study funding/potential competing interestsThe study was funded as part of the UK National Insti-tute of Health Research (NIHR) School for Primary Care Research. BM is an employee of GAIA AG, Hamburg, which owns one of the low intensity interventions considered in this paper. PB has been a paid consultant to the British Association for Counselling and Psychotherapy.
Influence of initial severity of depression on effectiveness of low intensity interventions: meta-analysis of individual patient dataPeter Bower, Evangelos Kontopantelis, Alex Sutton, Tony Kendrick, David A Richards, Simon Gilbody, Sarah Knowles, Pim Cuijpers, Gerhard Andersson, Helen Christensen, Björn Meyer, Marcus Huibers, Filip Smit, Annemieke van Straten, Lisanne Warmerdam, Michael Barkham, Linda Bilich, Karina Lovell, Emily Tung-Hsueh Liu
Interactions between baseline severity of depression ande!ect of low intensity interventions
CBT=cognitive behavioural therapy; TAU=treatment as usual;PST=problem solving therapy; Edu=education
Mead !""# Willemse !""$ Warmerdam !""% CBT Warmerdam !""% PST Lovell !""% Christensen !""$ CBT Christensen !""$ Edu Van Straten !""% Meyer !""& Richards !""' Andersson !""# Vernmark !"(" De Graaf !""& CBT+TAU De Graaf !""& CBT Liu !""& Bilich !""%Overall e)ectPooled coe*cient-".( (-".(& to -".""!)
-(." -".# " ".# (." (.#E!ect size ("#% CI) for interaction e!ect
bmj.com ( Psychiatry updates from BMJ Group are at www.bmj.com/specialties/psychiatry

BMJ | 16 MARCH 2013 | VOLUME 346 13
RESEARCH
STUDY QUESTION Do randomised trials in less developed countries give different results from those in more developed countries and, if so, to what extent?
SUMMARY ANSWER Randomised trials from less developed countries occasionally show significantly different treatment effects from those from more developed countries, and on average treatment effects are more favourable in the less developed countries.
WHAT IS KNOWN AND WHAT THIS PAPER ADDS An increasing number of trials are performed in less developed countries with no longstanding tradition of clinical research. Discrepancies in treatment effects between trials from more developed versus less developed countries may often reflect biases as well as genuine differences and should be taken into account when generalising evidence across different settings.
Selection criteria for studiesA meta-epidemiological assessment was performed of trials from less and more developed countries identi!ed through the Cochrane database of systematic reviews. We selected Cochrane meta-analyses with mortality outcomes including quantitative data from at least one randomised trial from a less developed country and at least one trial from a more developed country. For each meta-analysis we compared the relative risk estimates of more developed versus less devel-oped countries by calculating the relative relative risk (RRR) for each topic and the summary relative relative risk (sRRR) across all topics. Additionally, we performed similar analy-ses for the primary binary outcome of each eligible topic.
Primary outcomeThe primary outcome of the current study was the discrep-ancy in e"ect estimates on mortality between trials from less developed and more developed countries.
Main results and role of chance#$% meta-analyses with mortality outcomes were eligible. No nominally signi!cant di"erences between the country types were found for #&' (%&%) meta-analyses. However, di"erences were beyond chance in ## ('%) cases (ante-natal corticosteroids, preventive antioxidants, admissions to hospital for bed rest in multiple pregnancy, steroids in sepsis, antioxidants for the prevention of gastrointestinal cancer, antifungals for critically ill patients, postopera-tive radiotherapy for non-small cell lung cancer, calcium antagonists in aneurysmal subarachnoid haemorrhage, intravenous immunoglobulin for preventing infection in preterm or low birthweight infants, transarterial emboli-sation in unresectable hepatocellular carcinoma, and altered fractionation radiotherapy for oral cavity and oropharyngeal cancer), always showing more favourable treatment e"ects in trials from less developed countries. The sRRR was #.#& (%(% con!dence interval #.)* to #.#'; P<).))#; I&=)%), suggesting signi!cantly more favourable mortality e"ects in trials from less developed countries. Results were similar when focusing on meta-analyses with nominally signi!cant treatment e"ects for mortality (sRRR #.#(), excluding meta-analyses of old trials (#.#+), and excluding trials from less developed countries subse-quently becoming more developed (#.#&). For the primary meta-analysis binary outcomes (#&, eligible meta-anal-yses), &) topics had di"erences in treatment e"ects in more developed versus less developed countries beyond chance (more favourable in less developed countries in #(/&) cases).
Bias, confounding, and other reasons for cautionPublication bias or selective analysis and outcome report-ing biases may be in-uential in shaping these !ndings. A higher barrier to publication for authors from less devel-oped countries with no longstanding tradition in clinical research may further boost selective reporting. Large, well conducted trials are needed to probe the claims for coun-try speci!c major bene!ts and they may show that many of these claims are spurious. Moreover, di"erences in treat-ment e"ects between less developed and more developed countries may also be due to genuine di"erences rather than to biases. Low income and middle income countries face substantial !nancial barriers to their total healthcare budget, which may limit the implementation of expensive interventions. However, we did not identify any discrepan-cies where the implicated intervention was expensive or di.cult to administer and its e.cacy may have depended largely on sophisticated background standards of care. Nevertheless, di"erentiating between bias and genuine di"erences in baseline risks or treatment implementa-tion might be di.cult. These concerns should be taken into account when generalising evidence across di"erent settings.
Comparative effect sizes in randomised trials from less developed and more developed countries: meta-epidemiological assessmentOrestis A Panagiotou,! Despina G Contopoulos-Ioannidis," # John P A Ioannidis$ %
!Clinical Trials and Evidence-Based Medicine Unit, Department of Hygiene and Epidemiology, University of Ioannina School of Medicine, University Campus, Ioannina, Greece"Division of Infectious Diseases, Department of Pediatrics, Stanford University School of Medicine, Stanford, CA, USA#Health Policy Research, Palo Alto Medical Foundation Research Institute, Palo Alto, CA, USA$Stanford Prevention Research Center, Department of Medicine%Department of Health Research and Policy, Stanford University School of Medicine, Stanford, CA &$#'%, USACorrespondence to: J P A Ioannidis [email protected] this as: BMJ !"#$;$%&:f'"'doi: !'.!!#(/bmj.f)')
This is a summary of a paper that was published on bmj.com as BMJ "'!#;#$(:f)')
Statistically significant differences in treatment effects on mortality between trials from less developed and more developed countries
TopicExperimental intervention Outcome
Relative relative risk (()% CI) for more v less developed countries
Antenatal prevention in preterm birth Corticosteroids Fetal and neonatal deaths ".'* (!.#' to #.##)Antioxidant supplements for prevention Antioxidants Mortality !.!# (!.'! to !."))Multiple pregnancy Admission to
hospital for bed rest Perinatal death $.$" (!.'# to !*.&&)
Treatment of sepsis and septic shock Corticosteroids All cause mortality at "* days ".%* (!.'! to (.(#)Prevention of gastrointestinal cancers Antioxidants Mortality !.!% (!.'# to !."&)Non-neutropenic critically ill patients Systemic antifungals Mortality #.!* (!.'* to &.$')Treatment of non-small cell lung cancer
Postoperative radiotherapy
Mortality !.(! (!.'# to ".%#)
Aneurysmal subarachnoid haemorrhage
Calcium antagonists alone
Case fatality %.)# (!.!# to "*.#)
Prevention of infection in preterm or low birthweight infants
Intravenous immunoglobulin
All cause mortality !.&# (!.'! to #.(()
Unresectable hepatocellular carcinoma
Transarterial (chemo)embolisation
All cause mortality !.)( (!.'% to ".&))
Oral cavity and oropharyngeal cancer Altered fractionation radiotherapy
Total mortality !.(' (!.'# to ".$*)

14 BMJ | 16 MARCH 2013 | VOLUME 346
RESEARCH
Features of effective computerised clinical decision support systems: meta-regression of 162 randomised trialsPavel S Roshanov,! Natasha Fernandes," Jeff M Wilczynski,# Brian J Hemens,$ John J You,$ % & Steven M Handler,' Robby Nieuwlaat,$ ' Nathan M Souza,$ Joseph Beyene,$ ' Harriette G C Van Spall,% & Amit X Garg,$ ( ) R Brian Haynes$ & !*
STUDY QUESTION What characteristics differentiate computerised clinical decision support systems that successfully improve clinical care or patient outcomes from those that do not?
SUMMARY ANSWER Presenting advice within electronic charting or order entry systems is not sufficient to derive clinical benefit and is associated with failure, perhaps from alert fatigue. Demanding reasons from clinicians before they can over-ride advice and also providing recommendations to patients might improve chances of success.
WHAT IS KNOWN AND WHAT THIS PAPER ADDS Computerised clinical decision support systems often fail to improve the process of care and are even less likely to improve patient outcomes. Our study found that presenting decision support within electronic charting or order entry systems is not sufficient to derive clinical benefit and is associated with failure. Demanding reasons from clinicians before they can over-ride electronic advice and providing advice to patients and clinicians might improve chances of success. Most evaluations have been conducted by the developers of the systems and such evaluations are more likely to show benefit than those conducted externally.
Studies and settingWe created a database of characteristics and e!ectiveness of computerised support systems in "#$ randomised control-led trials from a recent systematic review.
DesignIn this cross sectional study, we conducted logistic regres-sion analyses to determine the association between charac-teristics and e!ectiveness of computerised clinical decision support systems. We used several statistical methods for sensitivity analysis.
Primary outcomesWe defined effectiveness as a significant difference in favour of the system over control for process of care (such as adherence to prescribing recommendations) or patient outcomes (such as reduction in blood pressure, mortal-
ity). In a multivariable model, we looked for associations between system e!ectiveness and whether the system pro-vided advice that was automatically within clinical work-%ow, given at the time of care, presented in an electronic charting or order entry system, required reasons to be given for over-riding advice, and was also given to patients, and whether some of the study’s authors were also the system’s developers.
Main results and the role of chanceComputerised clinical decision support systems presenting advice in electronic charting or order entry interfaces were less likely to succeed than their counterparts (odds ratio &.'(, )*% con+dence interval &."( to &.,&). Systems more likely to succeed than their counterparts provided advice for patients in addition to practitioners ($.((, ".&( to (."(), required practitioners to give a reason when over-riding advice ("".$', ".), to #'.($), or were evaluated by their developers (-.'*, ".## to "".--).
Bias, confounding, and other reasons for cautionThough our study was based on data from randomised con-trolled trials, our analyses were observational. We did not +nd signi+cant associations for the remaining "( factors tested in exploratory analyses but cannot rule out confound-ing by factors that we could not test directly, such as leader-ship and a culture of quality improvement. Our +ndings were generally robust across di!erent statistical methods and in internal validation, but the estimates of e!ect were imprecise. Additional studies are needed—ideally randomised control-led trials directly comparing di!erent features.
Generalisability to other populationsCommercial products represent only $"% of systems tested in our trials but will account for nearly all systems clinicians will use. While we found no association between commercial status and success, we did not have su.cient data to test interactions between commercial status and system features and cannot determine if the associations we discovered are generalisable to commercial products. Over a third ('(%) of trials were conducted at institutions with an academic his-tory in medical informatics, but we found no link between this and e!ectiveness.
!Schulich School of Medicine and Dentistry, University of Western Ontario, !!'! Richmond St, London, ON, Canada N%A #K&"Faculty of Medicine, University of Ottawa, $'! Smyth Rd, Ottawa, ON, Canada K!H (M'#Department of Health, Aging, and Society, McMaster University, !"(* Main St W, Hamilton, ON, Canada L(S $K!$Department of Clinical Epidemiology and Biostatistics, McMaster University, !"(* Main St W, Hamilton, ON, Canada L(S $K!'Department of Biomedical Informatics, University of Pittsburgh, Pittsburgh, USA%Population Health Research Institute, "#& Barton St E, Hamilton, Canada L(L "X"&Department of Medicine, McMaster University, !"(* Main St W, Hamilton, ON, Canada L(S $K!(Department of Medicine, University of Western Ontario, !!'! Richmond St, London, ON, Canada N%A #K&)Department of Epidemiology and Biostatistics, University of Western Ontario, !!'! Richmond St, London, ON, Canada N%A #K&!*Health Information Research Unit, McMaster University, !"(* Main St W, Hamilton, ON, Canada L(S $K!Correspondence to: R B Haynes, McMaster University, Department of Clinical Epidemiology and Biostatistics, !"(* Main Street West, CRL-!##, Hamilton, Ontario, Canada L(S $K! [email protected] this as: BMJ !"#$;$%&:f&'(doi: !*.!!#%/bmj.f%'&
This is a summary of a paper that was published on bmj.com as BMJ "*!#;#$%:f%'&
Odds ratios ()'% confidence intervals) and P values for adjusted associations between effectiveness and features of computerised clinical decision support systemsFactors Prespecified model (#%* trials) Final primary model (#'" trials)Developed by authors #.'" (!.#$ to )."&), *.**( $.#' (!.%% to !!.$$), *.**"Advice automatically in workflow !.$( (*.%" to #.'"), *.#( —Advice at time of care *.%! (*."! to !.&&), *.#' —Advice presented in electronic charting or order entry *.## (*.!$ to *.&%), *.**( *.#& (*.!& to *.(*), *.*!Provides advice for patients ".'$ (*.)( to %.'&), *.*' ".&& (!.*& to &.!&), *.*#Requires reason for over-ride !*.%) (!.(& to %!.*"), *.**! !!."# (!.)( to %#.&"), <*.**!
Response on bmj.com“Can the authors provide a list of excluded articles? For example, why was the positive study by Kucher et al not included?”Robert G Badgett, physician, Kansas
+ Visit the article online and click “Respond to this article” to have your say.bmj.com
+ Editorial:The road to e+ective clinical decision support: are we there yet? (BMJ "*!#;#$%:f!%!%)

BMJ | 16 MARCH 2013 | VOLUME 346 15
RESEARCH
STUDY QUESTION Does a mild traumatic brain injury result in lower cognitive function?
SUMMARY ANSWER Cognitive function was similar in men with mild traumatic brain injuries before and after cognitive testing.
WHAT IS KNOWN AND WHAT THIS PAPER ADDS Previous retrospective studies have found lower cognitive function after a mild traumatic brain injury in several areas including attention, working memory, episodic memory, verbal learning, and processing speed. Low cognitive function was found in men who later sustained mild traumatic brain injuries, suggesting that low cognitive function may be a risk factor rather than the long term consequence of such injuries.
Participants and settingWe studied a nationwide cohort of !"# $$# men con-scripted for mandatory Swedish military service between %&$& and %&&' at a mean age of %$ years.
Design, size, and durationWe constructed a measure of overall cognitive function from the four di(erent tests used at conscription. We inves-tigated mild traumatic brain injuries occurring before and
a)er conscription in relation to cognitive function and other potential risk factors assessed at conscription and follow-up.
Main results and the role of chanceIn the cohort, '*%! men had sustained one mild trau-matic brain injury before the tests of cognitive function. In the rest of the cohort, %% +%* men sustained one mild traumatic brain injury, and *&# men sustained at least two such injuries a)er cognitive testing, during a median follow-up period of %& (range "–++) years. Men with one injury within two years before (n=%&$$) or a)er cognitive testing (n=++%') had about #.#% lower overall cognitive function scores than men with no injury during follow-up (P<".""% for both). Men with at least two injuries a)er cognitive testing (n=*&#) had %#% lower overall cogni-tive function scores than those with none (P<".""%). Men with a mild traumatic brain injury within three months before cognitive testing had similar cognitive function scores to men with an injury within two years a)er the cognitive tests. Independent strong risk factors (P<%,%"-%") for at least one mild traumatic brain injury a)er cognitive testing (n=%+ '&' events) included low overall cognitive function, a previous mild traumatic brain injury, hospital admission for intoxications, and low education and socio-economic status. In a sub-cohort of twin pairs in which one twin had a mild traumatic brain injury before cognitive testing (n=.!), both twins had lower logical performance and technical performance compared with men in the total cohort with no injury (P<"."# for all). These results may suggest a genetic component to the low cognitive function associated with mild traumatic brain injury.
Bias, confounding, and other reasons for cautionWe evaluated only younger men with mild traumatic brain injury, so our results are not applicable to women, older men, or people with more severe traumatic brain injuries.
Generalisability to other populationsThe large well characterised nationwide cohort studied including more than %. """ diagnosed mild traumatic brain injuries increases external validity.
Study funding/potential competing interestsThe study was funded by the Swedish Research Council.
Cognitive function and other risk factors for mild traumatic brain injury in young men: nationwide cohort studyAnna Nordström,! Benoni B Edin," Sara Lindström,# Peter Nordström$
!Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, SE-%&! '( Umeå, Sweden"Department of Integrative Medical Biology, Physiology Section, Umeå University#Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA$Department of Community Medicine and Rehabilitation, Geriatric Medicine, Umeå UniversityCorrespondence to: A Nordström [email protected] this as: BMJ !"#$;$%&:f'!$doi: !&.!!#)/bmj.f("#
This is a summary of a paper that was published on bmj.com as BMJ "&!#;#$):f("#
(EDITORIAL by Newcombe and Menon
Cognitive function at conscription for total cohort based on mild traumatic brain injurystatus at follow-up
No of mild traumatic brain injuries
Cogn
itive
func
tion
scor
e
! beforetesting
* Signi"cantly lower (P<#.#!) for speci"c test compared with men with one mild traumatic brain injury before cognitive testing (n=$%!&)† Signi"cantly di'erent (P<#.#!) for speci"c cognitive test compared with all other groups
!(
!%
!)
*!
*&Overall functionLogical function
Visuospatial functionTechnical function
Word recollection
! within* yearsbeforetesting
! within& months
beforetesting
**
*
*
*
†† †
†
†
††
†
†
! a+ertesting
! within* years
a+ertesting
>! a+ertesting
None
bmj.com ( Neurology updates from BMJ Group are at www.bmj.com/specialties/neurology

16 BMJ | 16 MARCH 2013 | VOLUME 346
DATA BRIEFING
In !"#$ the King Edward’s Hospital Fund for London, now known as the King’s Fund, published a new specification for the design of a “hospital bedstead.”! This had followed an evaluation of various bed designs in collaboration with Bruce Archer, an engineering designer at London’s Royal College of Art.% As Lawrence notes, the evaluation was intensive and “relied on extensive data collection, mathematical modelling of solutions, and field trials . . . !&&& hospitals completed a televisual survey on beds, and . . . %& prototype beds were installed for three months at Chase Farm Hospital, Enfield. Trained observers recorded all bed-related activities from &#&& h to %%&& h daily.” The project cost '() &&&—over ')&& &&& (*)+& &&&; ,$)& &&&) at today’s prices.( Over time the King’s Fund bed came to replace the many hundreds of different bed designs used in the NHS.
Fig ! | Hospital beds by type: English NHS: !"#"-$% to &%!!-!&'-( Design classic: the King’s Fund bed
0
1979
-80
1981
-82
1983
-84
1985
-86
1987
-88
1989
-90
1991
-92
1993
-94
1995
-96
1997
-98
1999
-00
2001
-02
2003
-04
2005
-06
2007
-08
2009
-10
2011
-12
Tota
l No
of b
eds
(000
s)
300
350
400
250
200
150
100
50
1979-2012All beds
59%
AcuteGeriatricMental illnessLearning disabilityMaternity
Previous articles in this series ) Rises in healthcare spending: where will it end? (BMJ !"#!;$%&:e'#!') ) Hospitals: what do they do and how much does it cost? (BMJ !"#!;$%%:e#'&() ) How long can we expect to live? (BMJ !"#$;$%):f$$#)
THE HOSPITAL BED: ON ITS WAY OUT?John Appleby examines trends in the number of hospital beds and wonders how low we can go
Coincidentally, just as the King’s Fund embarked on its bed redesign project in !"#%, concern was being raised by the then minister of health, Enoch Powell, and others at the Ministry of Health about the need to save money and improve labour efficiency in the light of a shortage of nurses and general pressures on health service budgets.(
As Lawrence reports Enoch Powell at the time, a key question was “what mechanical and powered assistance would be necessary if the same quantity of care and attention had to be given with half the present quantity of woman-hours?”( Standardising the hospital bed to improve nurse productivity and reduce procurement costs was one project on his list that, fortuitously, the King’s Fund had started to address.
Nearly half a century later, concerns about productivity remain—as does, to an extent, the King’s Fund bed, modified and
redesigned. What has changed— and not just in the English NHS but in most countries—is the number of beds in use in hospitals.
In England, for example, over the (( years since !"$", beds used for acute care fell by ()%, for maternity by )+%, for geriatric care by #)%, and for mental illness and learning disability by $-% and "#%, respectively (fig !). If allowance is made for increases in population, these bed reductions are proportionately higher—a drop of -%% in the number of acute beds per !&&& population, for example. And over the decade to %&&", the US and UK have experienced similar proportionate reductions in acute beds.
The fact that the number of hospital beds has fallen in almost all countries in the Organisation for Economic Cooperation and Development (fig %) provides some clue to the reasons for these trends. Changes in medical practice have shortened the time patients
“With more patients being treated but fewer beds, there’s no doubt that beds are being used more efficiently. But more intensive use could be a problem”

BMJ | 16 MARCH 2013 | VOLUME 346 17
DATA BRIEFING
Design classic: the King’s Fund bed
Fig ! | Average annual changes in acute care beds per "### population (calculated from total change from "$$%-!#"#) in selected OECD countries&
KoreaTurkey (2000-10)
Greece (1995-2009)Netherlands
MexicoPortugal
IsraelGermanyBelgiumAustria
SpainAustralia (1995-2008)Slovenia (1996-2010)
France (1997-2010)United States (1995-2009)
PolandIreland
Slovak RepublicNorway
Denmark (1997-2010)Czech Republic
JapanSweden
Switzerland (1998-2010)United Kingdom (2000-10)
FinlandItaly
Estonia-3.0 -2.0 -1.0 0.0 1.0 2.0 3.0 4.0 5.0
% change
Fig ' | Daily bed occupancy (%) in English NHS, !#""-"!(
80
95
95
80
75
65
60
70
April
May
June July
Augu
st
Sept
embe
r
Octo
ber
Nove
mbe
r
Dece
mbe
r
Janu
ary
Febr
uary
Mar
ch
Peaks: Midnight Tuesday
Troughs: Midnight Saturday
Good Friday
New Year’s Eve
Boxing Day
Christmas DayChristmas Eve
Public holidays
% o
ccup
ancy
spend in hospital—the average length of stay for an acute case in England has shrunk from around !." days in #!$! to about three days in %&##. And new practices, drugs, and diagnostic procedures have helped shift care from the ward to the outpatient department and beyond the walls of hospitals.
The introduction of deliberate policies to move some types of care out of hospital and into the community has had a dramatic effect on hospital beds too. In England, for example, care in the community policies have changed the proportion of the hospital bed stock taken up by mental health, learning disability, and geriatric services from around '"% to (&% in just over (& years (fig #).
With more patients being treated but fewer beds, there’s no doubt that beds are being used more efficiently. But more intensive use could be a problem. Daily bed occupancy data for England in %&##-#% reveal that average occupancy across all hospitals reached over !&% on several days (fig (). Such high occupancy rates reduce the time available for cleaning between patients and increase the chances of infection.
Is the hospital slowly but inexorably on its way out to be replaced perhaps by “virtual wards”! and new configurations of care facilities? Or are we already close to the limit of substitution and technology development that would allow significant further reductions?John Appleby chief economist, King’s Fund, London, UK [email protected] interests: None declared. Provenance and peer review: Commissioned; externally peer reviewed.! King Edward’s Hospital Fund for London. Design of
hospital bedsteads. KEHFL, !"#$.% Lawrence G. King’s Fund beds. Lancet %&&!;'():)*).' Lawrence G. Hospital beds by design: a sociohistorical
account of the “King’s Fund bed,” !"#&-!"$(. PhD thesis. University of London, %&&!. http://chrisrust.wordpress.com/%&&!/!%/'!/lawrence-hospital-beds-by-design/.
* Department of Health. NHS hospital activity statistics for England: !"$"-!""&-"!. Stat Bull !""%;%(!):"%.
( Department of Health. Bed availability and occupancy—overnight: Time series !")$/) to %&&"/!&. %&!%. http://transparency.dh.gov.uk/?p=!"$*(.
# Department of Health. Bed availability and occupancy— overnight: Time series %&!&/!! onwards. %&!%. http://transparency.dh.gov.uk/?p=!"$*(.
$ Organisation for Economic Cooperation and Development. OECD health data %&!%: frequently requested data. www.oecd.org/els/health-systems/oecdhealthdata%&!%-frequentlyrequesteddata.htm.
) Campbell D. Dr Foster’s report: how does hospital bed availability change throughout the year? Guardian. %&!% Dec '. www.guardian.co.uk/news/datablog/%&!%/dec/&'/dr-foster-report-nhs-hospital-bed-occupancy-data.
" Department of Health. Hospital organisation, specialty mix and MRSA. %&&$. www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_&)!%"%.pdf.
Cite this as: BMJ !#"';')*:f"%*'

18 BMJ | 16 MARCH 2013 | VOLUME 346
HEAD TO HEAD
Reducing avoidable emergency admissions is undoubtedly a desirable and worthy aim,
not least because it will bene!t patients. Additionally, emergency admissions are a considerable drain on NHS resources, representing about "#% of hospital bed days in England, at an annual cost of $%%bn (&%'bn; (%)bn).% The health data company Dr Foster estimated that *+% of these admissions are potentially avoidable and amenable to interventions in the community.* Emergency admissions also have an adverse e,ect on provision of other hospital services—for example, by causing cancellation of elective operations at short notice—and Dr Foster says that overoccupancy of hospital beds is at “breaking point,” risking patient safety.*
Annual emergency hospital admissions have increased by ')% over the past %- years.' The NHS is required to save $*-bn by *-%#, and avoiding emergency admissions is a key policy to deliver this. Currently, commissioners use local referral incentive schemes to encourage general practitioners to reduce their emergency admissions. Furthermore, the recently announced quality premium. will reward clinical commissioning groups if they are able to reduce
or prevent an increase in emergency admissions within a !scal year. Given the !nancially challenged budgets of commissioning groups, and reductions in GPs’ incomes, failing to hit such targets will in e,ect be a !nancial penalty.
Unfortunately, there is scant evidence, if any, that such !nancial levers will have any real e,ect on emergency admission rates. We know that !nancial incentives paid to GPs as part of practice based commissioning during *--#-%% were unable to stem the rise in emergency admission rates. Nor is there any conclusive evidence that the tools currently used by GPs and commissioners, such as risk strati!cation and case management, are e,ective in reducing emergency admissions.#
Solutions go beyond general practiceThe fundamental /aw in linking !nancial payments to GPs to emergency hospital admissions is that the GP is only one player in a multiplicity of factors that in/uence such admissions. It is therefore inappropriate for GPs themselves to be held responsible for emergency admission rates. Evidence has shown that increasing age, social deprivation, morbidity, area of residence, self management, provision of community and social care services, hospital supply, and internal hospital organisation and admission policies will all in/uence emergency admissions."
Major changes have occurred in healthcare over the past '- years. I remember, as a
house o0cer, having to admit patients for sev-eral days just to start them on a new drug—the angiotensin converting enzyme inhibitor cap-topril. As a surgeon I became adept at perform-ing vagotomy and pyloroplasty for duodenal ulcer and recently winced when a colleague pointed out that, in e,ect, we used to perform surgery for an infectious condition. While a general practitioner, I witnessed the closure of long stay geriatric wards and the proliferation of large residential and nursing home facilities for which GPs were expected to provide medi-cal care, looking a1er frail elderly patients with complex comorbidities. We have seen startling decreases in mortality and morbidity in cardiovascular disease and improvements in cancer treatments and survival. Despite this we have also seen an inexorable rise in emergency admissions. Financial incentives will help bring about the changes required to reverse this trend.
Narrow thinkingAs a clinician working in commissioning I have been struck by how “siloed” professional and organisational thinking can be. Emergency admissions account for a relatively small pro-portion of overall activity in specialist care, yet a large proportion of cost. If you look across the health and care system most activity occurs out-side hospital but most of the cost is consumed by hospital services.%
For a long time there has been the mantra of “moving care closer to home,” yet, except in a few isolated instances, this has not happened. Talking to a specialist recently, I asked why. His response was that there is no consistency out-side hospital. “I don’t know if my patients will be safe or get the care they need delivered,” he told me. I was also taken aback by the response a practice gave me recently when I asked when it last looked at its emergency admissions. The staff proudly told me that they had done an audit—a year previously.
Many emergency admissions are the result of exacerbations of long term conditions, failure of coordinated care, and, increasingly, frail eld-erly people with comorbidities needing proac-tive care from primary, community, and social
Should GPs be fined for rises in avoidable emergency admissions to hospital?Commissioning organisations in England face losing a quarter of the “quality premium” if they do not keep down their emergency admissions for specific conditions. Martin McShane supports this, but Chaand Nagpaul worries about possible unintended consequences
Martin McShane director for domain !, National Commissioning Board, Leeds LS! "UE, UK [email protected]
Chaand Nagpaul general practitioner , Stanmore, London, UK [email protected]

BMJ | 16 MARCH 2013 | VOLUME 346 19
HEAD TO HEAD
Furthermore, the 2004 GP contract transferred the responsibility for out of hours care to primary care trusts, and therefore hospital admissions during the out of hours period (70% of weekly hours) fall outside the control of general practices. Additionally, numerous other primary care access points, from telephone advice via NHS Direct, to other unscheduled care settings such as walk-in centres and new 111 urgent care services will also refer patients directly to hospitals, bypassing GPs. Similarly, GPs have no control of direct patient admissions from emergencies such as road tra&c incidents. And some increases in admission rates could re'ect national policies—for example, e(orts by emergency departments to avoid breaches of the target of a four hour maximum wait may have increased short term hospital admissions.5
Another problem is that the relatively small number of patients in general practice lists could result in variations in admission rates by chance or volatility in the external environment (for example, infection outbreaks). Providing *nancial rewards or penalties to GPs as a result of erroneous interpretation of admission rates will unfairly discriminate against patients.
Unwanted effectsThe division of GPs and hospital specialists into commissioners and providers, with payment
of an activity tari( to hospitals, provides no incentive to hospitals to reduce emergency admissions, nor to collaborate with GPs. This creates the perverse e(ect of supplier induced demand.5
Making payments to GPs to reduce emergency admissions may also cause patients to mistrust the motives of GPs in managing their care, and risks breaching General Medical Council principles of good medical practice by adding a perverse *nancial incentive not to refer patients to hospital. Overzealous attempts to reduce hospital admissions could have unintended consequences. For instance, two recently published high quality randomised controlled trials of interventions designed to keep people out of hospital showed increased deaths among the intervention groups.7 8 Nor can we assume that avoiding admission is always cost e(ective, since the expense of keeping patients in the community may not necessarily re'ect a cost saving.
The logical way forward should be a whole system approach, bringing together all stakeholders so that all in'uences on hospital admissions are aligned. There is evidence that hospital admissions can be reduced by integration between health and social care, as well as between primary and secondary care, and by improved internal hospital organisation of admission units sta(ed by
more senior doctors.6 9 10 We need to jettison the current unhelpful competitive purchaser-provider spit between primary and secondary care and replace the tari( system of payment by results with a system of collaboration and shared *nancial ownership with goals aligned across primary, secondary, and social care. Wider determinants that in'uence hospital admissions must be addressed.6 9
Proposals to *nancially reward or penalise GPs as either providers or commissioners in their own right on the basis of emergency admission rates is likely to squander precious public resources on unproved ideology at a time of harsh *scal austerity. It also carries the possibility of counterproductive e(ects and potential to do harm through unintended consequences.Competing interests: I have read and understood the BMJ Group policy on declaration of interests and declare I am a negotiator for the BMA General Practitioners Committee with lead roles in commissioning and IT and a member of BMA Council.Read the opposing side in the debate by Martin McShane, doi:!".!!#$/bmj.f!#%&. Provenance and peer review: Commissioned; not externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#$'#
care.1 2 How many practices systematically ana-lyse the root causes of emergency admissions?
Opportunity for changeThe advent of clinical commissioning groups and health and wellbeing boards presents an opportunity to tackle the complex issues rel-evant to emergency admissions. The recent analysis of trends in emergency admissions by Bardsley and colleagues tells us one thing—we need to ask more and better questions and work collectively across the continuum of health and social care, if we are to move care closer to home and reverse the trend in acute admissions.3
Clinical commissioning groups will be com-missioning the community and mental health care that can support that move, as well as the acute services, which are under pressure. To avert emergency admissions to hospital they will need to work in partnership with social care and some of the wider services that frail elderly people and their carers are so dependent on. The construct of health and wellbeing boards
provides an opportunity to foster and forge a coherent and consistent common purpose across primary care. The responsibility of com-missioning groups and the NHS Commission-ing Board to improve the quality of primary care creates a new dynamic in the system which, if approached in the right way, can build on the potential of general practice to support collabo-rative coordinated care and reduce emergency admissions, especially if aligned with commis-sioning in the rest of the health system.
Success will require a range of enablers, levers, and incentives to help leaders to change attitudes, behaviours, and ways of working right across the system. The fact that colleagues say that most emergency admissions are out of hours or self referrals, as if that absolves them from any responsibility, is worrying. Clinicians have a responsibility to improve care no matter where a patient is on a pathway. There is no bet-ter way of articulating the role of primary care than to quote from the Francis report: “It will be important for the future that all GPs undertake a monitoring role on behalf of their patients who receive acute hospital and other specialist services . . . A GP’s duty does not end on refer-ral to hospital but is a continuing relationship.
They will need to take this continuing partner-ship with their patients seriously if they are to be successful commissioners of services. They should exploit to the full this new role in ensur-ing their patients get safe and e(ective care.”4
No part of the system is an island. In my expe-rience, through better use of data, planning, service redesign, contracting, and monitoring performance—that is, good commissioning—it will be possible to improve quality while man-aging costs. The quality premium is one instru-ment in the toolbox to support new thinking and ways of tackling deep rooted problems. To consider the premium in isolation, or to label it as a *ne, perpetuates a fragmented view of a complex adaptive system in which clinicians have now got a real opportunity to lead change and improve outcomes for patients.Competing interests: I have read and understood the BMJ Group policy on declaration of interests and declare that I work for the NHS Commissioning Board and one of my key objectives is supporting clinical commissioning groups to reduce emergency admissions. Read the opposing side in the debate by Chaand Nagpaul, doi:!".!!#$/bmj.f!#&!.Provenance and peer review: Commissioned; not externally peer reviewed.References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#$('
Clinicians have a responsibility to improve care no matter where a patient is on a pathway
The GP is only one player in a multiplicity of factors that influence emergency admissions

20 BMJ | 16 MARCH 2013 | VOLUME 346
ANALYSIS
Antimicrobial resistance: the true costRichard Smith and Joanna Coast argue that current estimates of the cost of antibiotic resistance are misleading and may result in inadequate investment in tackling the problem
Almost as soon as antibiotics were dis-covered, we knew that bacteria were able to develop resistance to them.! This is not necessarily a problem, as long as there are other antimicrobi-
als to take their place. During the latter half of the "#th century this was the predominant situation, but no longer." A rapid decrease in the number of new drugs approved and numerous withdrawals on quality and safety grounds have le$ the well dry, and it is clear that “the existing classes of anti-biotics are probably the best we will ever have.”%
In light of this, there have been e&orts to sup-port interventions that encourage the more con-servative and appropriate use of antibiotics in a bid to halt or slow the progress of resistance.' However, this action is o$en too little and may be too late.
Given that the dangers of resistance are widely acknowledged, why isn’t more being done? One reason is that antibiotic resistance has fallen victim to evidence based policy making, which prioritises health problems by economic burden and cost e&ectiveness of interventions.( Health economists have been unable to show that antibi-otic resistance costs enough to be a health priority.
Limitations of health economic researchTen years ago we published a systematic review on the economics of resistance.) We asked two questions: what is the cost of resistance and what is the cost e&ectiveness of interventions to reduce
KEY MESSAGESAn increase in resistant organisms coupled with a big fall in the number of new antimicrobial drugs suggests an apocalyptic scenario may be loomingCurrent estimates suggest antimicrobial resistance has a low economic impactSuch estimates do not take into account that antimicrobials are integral to modern healthcare We may not ever be able to make an accurate forecast of the costsWe should view greater investment in antibiotic resistance as an insurance policy
bmj.com !This week’s poll asks: “Are the dangers of antibiotic resistance exaggerated?” Cast your vote on bmj.com
! Editorial: Improving antimicrobial stewardship and surveillance: the Chennai Declaration (BMJ !"#$;$%&:f'(#) ! Research: E)ectiveness of multifaceted educational programme to reduce antibiotic dispensing in primary care (BMJ !"#!;$%%:d*#+$)
their estimates of the actual economic impact may not be accurate because the research used to produce these estimates is limited in its scope. For example, economic estimates are based on the incremental costs and focus on a speci*c infectious disease or set of diseases: estimates are based on the cost of extra treatment of a resistant infection compared with susceptible infection, such as costs of additional inves-tigations, more expensive drugs, side e&ects from extra treatments, longer hospital stay, and greater mortality.+ Some may also include costs associated with surveillance and activities associated with trying to control resistance. Most studies were from the United States and based
it? The lack of research meant we could investi-gate only the second question., And even here we concluded that the evidence for the cost e&ec-tiveness of interventions for resistance was poor.
We have just performed a rapid review at the Department of Health’s request to take into account newer information on the *rst question. The box summarises our methods and further details are available in the full report.- Estimates of additional cost varied from less than .( (/%; 0') to more than .(( ### per patient episode. This might be explained by type of resistance and how productivity losses are dealt with.
Although there was little intrinsically wrong with these papers, we became concerned that

BMJ | 16 MARCH 2013 | VOLUME 346 21
ANALYSIS
Annual cost of illness for selected conditions in US
Health problem Societal cost (!bn, "##$)
Cardiovascular diseasew! "#$Musculoskeletal conditionsw% "$$Motor vehicle accidentsw" %&$Occupational injury and illnessw' %((Mental disordersw) %($Substance abusew( !*)Cancer (all)w& !#)Diabetesw# !')Alzheimer’s diseasew* &$Antimicrobial resistancew!$ ))Skin diseasew!! '#Urinary incontinencew!% %"Asthmaw!" !(
in hospitals and included the costs related to additional hospital stay and treatment but not early mortality.
None of the studies considered the bigger picture—a world in which there are no e!ective antibiotics for situations where they are cur-rently used routinely, such as in hip replacement or cancer patients. Our concern is that today’s limited estimates will be used to project future costs. Will the current worst case scenario place antibiotics high enough up on the health agenda to ensure adequate action?
Current worst case scenario is still an underestimateWe took the study that found the highest cost of antimicrobial resistance, of "##bn ("$%bn in health service costs and "&#bn in lost produc-tivity) per year overall to the US, and compared it with economic burden 'gures for other health problems in the US. These burden 'gures are taken from a variety of studies, and the dates range considerably, but it is clear that resistance rates fairly low down (table).
However, the costs of resistance could be much higher than these estimates suggest. As
an example we estimated the consequences of having no antibiotics for patients having a total hip replacement. Because antibiotics have been used as prophylaxis and treatment for hos-pital acquired infection since hip replacements were 'rst performed we looked at information relating to limb amputation as a proxy for what infection rates might have been with and with-out antimicrobials.
The figure shows the care pathway for patients requiring hip replacement. Currently, prophylaxis is standard practice, and infection rates are about %.#-$%, so most patients recover without infection, and those who get an infec-tion have it successfully treated. We estimate that without antimicrobials, the rate of post-operative infection is (%-#%% and about &%% of those with an infection will die.w)(-w)* Thus, removal of antibiotics would increase postoper-ative infection by )-#%% and deaths by %-&%%. Of course, at such rates it is likely that the rates of hip replacement would fall, which would increase the burden of morbidity from hip pain.
We recognise that this is a simplistic analy-sis, with many of the data obtained from litera-ture relating to amputation as a proxy for hip
replacement. However, we use it as an example to illustrate and provoke, to emphasise the point that infection rates and their consequences in terms of health service costs and human health may be unimaginable. As we struggle to imagine the clinical consequences, it is easy to see why the economic burden is at present inestimable.
A world without antibioticsModern healthcare was built over the past century on the basis that infections can be pre-vented or treated using antimicrobials (exem-plified by the US surgeon general famously proclaiming in )+,- that “the war against dis-eases has been won”).)%
Resistance is said to present a risk that we will fall back into the pre-antibiotic era.)) How-ever, this is perhaps optimistic. Our health system is now designed to treat more chronic conditions. Healthcare has become increas-ingly technological and invasive, improving mortality and morbidity significantly, and antimicrobials have become integrated in many aspects of such care. For example, antimicro-bials are given as standard to prevent iatro-genic infection in surgical care,)) to women
Poor symptoms
Bad outcome Recover Bad outcome Recover Recover
Severe painand reduction
in QALYs
Treatment with antibiotics No antibiotic treatment available
No total hip arthroplastyTotal hip arthroplasty
No antibioticsAntibiotic prophylaxis
No infectionInfection No infectionInfection
Bad outcome Recover Bad outcome Recover Recover
Treatment with antibiotics No antibiotic treatment available
Before surgery
A!er surgery
Care pathway for total hip arthroplasty with and without antimicrobials
Box % | Methods used in the review&
We searched for the combinations of terms relating to resistance, antimicrobial and costs. Some papers did not refer to antimicrobial resistance generally but only to particular drugs or micro-organisms. We extended the search terms to focus on meticillin resistant Staphylococcus aureus and vancomycin resistant enterococci, two of the most studied and potentially serious current resistant infections.
We included English language
studies (empirical or modelling) with data on costs associated with resistance, since !""". For empirical studies, we selected studies that included a control group with a susceptible infection because the aim was to focus on costs of resistance, rather than costs of infection.
Data extracted included: study design; sample size/modelling approach; relevant micro-organism and drug; cost perspective, year, currency, time frame, discounting approach;
resource use included; valuation methods; summary of results.We identified #$! possible papers, from which !% were eventually included in our analyses.
Vancomycin resistant enterococci
JANI
CE C
ARR/
SPL

22 BMJ | 16 MARCH 2013 | VOLUME 346
ANALYSIS
de livering by caesarean section,!" and to those having cancer treatment.!# From cradle to grave, antimicrobials have become pivotal in safe-guarding the overall health of human societies.
When viewed in this broader way, the costs of resistance are not limited to those associ-ated with additional treatment for a primary infection , such as a “strep throat.” Rather, they must encompass the costs that might relate to the loss of modern healthcare. In the same way that health systems need adequate and e$ective health workers to function, they also require e$ective antimicrobials. Resistance is not just an infectious disease issue; it is a surgical issue, a cancer issue, a health system issue.
To calculate the true economic burden of resist-ance we therefore have to consider the burden associated with not having any e$ective antimi-crobial drugs. And, as witnessed when there are outbreaks of hospital acquired infection, the sys-tem can very quickly come to a standstill.!% In the future we may need to rethink how the health sys-tem is developed—for instance, redesigning many facilities or reintroducing sanatoriums if e$ective antibiotic treatments are no longer available.
Planning for an uncertain futureAlthough we now have more empirical information on the economic burden of resistance than was available a decade ago, it is unlikely to help us plan for the future. Even the highest current estimates of the costs of resistance provide false reassurance and this may mean that inadequate attention and resources are devoted to resolving the problem. Our illustrative example for hip replacement with-out antibiotics shows how di&cult it is to forecast the likely economic burden of resistance. And we have explained how resistance has the potential to undermine modern health systems.
Full health systems analyses seem a more appropriate means to assess the potential impact of resistance and evaluate measures to stem it. Although this approach is complex, understand-ing the threat to the health system overall, not just for speci'c diseases, could be the single most important step in better understanding the eco-nomic burden that resistance presents. Analysing outbreaks of resistant infections and the cost of dis-ruption to the healthcare system may help produce future estimates.!(
A change in culture and action is needed to plan for a future with more antibiotic resistance. Con-siderable inertia remains regarding radical change in our stewardship of antimicrobials, precisely because there is a focus on current economic bur-den. The same is true with climate change and, to a degree, the 'nancial system. A major driver of this inertia is likely to be collective uncertainty about the clinical and 'nancial implications of increasing resistance. But there is a tried and trusted way to
deal with such uncertainty—insurance. Waiting for the burden to become substantial before taking action may mean waiting until it is too late. Rather than see expenditure on antimicrobial policies as a cost, we should think of it as an insurance policy against a catastrophe; albeit one which we hope will never happen.)
Richard Smith professor of health system economics , London School of Hygiene and Tropical Medicine, London WC!H "SH, UKJoanna Coast professor of health economics, School of Health and Population Sciences, University of Birmingham. Birmingham, UKCorrespondence to: R Smith [email protected] thank Callum Hodge, Joseph Gri!n, and Daniel Haynes for help with literature searching and Anthony So, Ursula Wells, Claire Boville, Sally Wellsteed, Ross Leach, Peter Bennett, John Henderson, David Cohen, Miranda Mugford, and Huseyin Naci for their comments. This report is independent research commissioned and funded by the Department of Health Policy Research Programme (Economic burden of antimicrobial resistance: a rapid paper, #$!##%&). The views expressed in this publication are those of the authors and not necessarily those of the Department of Health.Contributors and sources: Both authors have been health economists for over '# years and have worked together on aspects related to antimicrobial resistance for more than !& years. This article is a culmination of experiences over that time, and is based particularly on a rapid review, and interaction with colleagues who commissioned this review at the Department of Health. Both authors contributed equally to the writing of the paper. RS is guarantor.Competing interests: None declared.Provenance and peer review: Not commissioned; externally peer reviewed.! Courvalin P. Predictable and unpredictable evolution of
antibiotic resistance. J Intern Med '##(;')$:$-!).' So AD, Ruiz-Esparza Q, Gupta N, Cars O. %Rs for innovating
novel antibiotics: sharing resources, risks, and rewards. BMJ '#!':%$$:e!*('.
% Cormican M, Vellinga A. Existing classes of antibiotics are probably the best we will ever have. BMJ '#!';%$$:e%%)".
$ World Health Organization. The evolving threat of antimicrobial resistance: options for action. WHO, '#!'.
& Coast J, Smith RD, Millar MR. Disentangling value: assessing the benefits of containing antimicrobial resistance. In: Roberts J, ed. The economics of infectious disease. Oxford University Press, '##):'#!-!$.
) Smith RD, Coast J, Millar MR, Wilton P, Karcher A-M. Interventions against anti-microbial resistance: a review of the literature and exploration of modelling cost-effectiveness. WHO, '##!
* Wilton P, Smith RD, Coast J, Millar M. Strategies to contain the emergence of antimicrobial resistance: a systematic review of effectiveness and cost-effectiveness. J Health Serv Res Policy '##';*:!!!-*.
( Smith R, Coast J. The economic burden of antimicrobial resistance. Why it is more serious than current studies suggest. '#!%. www.lshtm.ac.uk/php/economics/assets/dh_amr_report.pdf.
" Coast J, Smith RD, Karcher AM, Wilton P, Millar M. Superbugs II: how should economic evaluation be conducted for interventions which aim to reduce antimicrobial resistance? Health Econ '##';!!:)%*-*.
!# Gregor M. Bird flu: a virus of our own hatching. New York, '##):(&.
!! Cars O, Hogberg LD, Murray M, Jasper W, Nordberg O, Sivaraman S, et al. Meeting the challenge of antibiotic resistance. BMJ '##(;%%*:*')-(.
!' Bratzer DW, Houck PM. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis '##$;%(:!*#)-!&.
!% Wild SM. Antibiotic prophylaxis at caesarean section. Lancet '##';%)#:*'$.
!$ Plowman RP, Graves N, Griffin M, Roberts JA, Swan AV, Cookson BC, et al. The socioecomic burden of hospital acquired infection. Public Health Laboratory Service, !""".
!& Kanerva M, Blom M, Tuominen U, Kolho E, Anttila VJ, Vaara M, et al. Costs of an outbreak of methicillin-resistant Staphylococcus aureus. Hosp Infect '##*;)):''-(.
Cite this as: BMJ !"#$;$%&:f#%'$
BMJ BLOG Elizabeth Loder
How can journals help stop disease mongering?How can medical journals address their role in selling sickness and disease mongering? I suggested two possible strategies at the "#$% Selling Sickness conference held in Washington last month.
First, why not quarantine apparently groundbreaking studies about new treatments or interventions in a special journal until the findings are replicated and long term consequences explored? Print copies of the journal would arrive in plain brown wrappers that, undone, would show the journal’s cover logo of a skull and crossbones. During quarantine, any news stories or summaries of research from this journal would travel with a sternly worded disclaimer, along the lines of those that accompany investment company advertisements. Something like the following would do nicely:
“Warning! Taking any action on the basis of this research could result in injury or death. The results described in this study have not been replicated and the long term effects of this treatment are unknown. Past performance is no guarantee of future results. When subjected to further investigation, most published research findings turn out to be false.”
To fill the void, medical journals deprived of these sensational research studies could instead devote themselves to the promotion and prioritisation of the less glamorous medical research that really matters: replication studies, comparative effectiveness trials, and long term pharmacosurveillance and safety studies.
My second suggestion was that several parts of a typical research paper are too important to be written by the researchers or anyone else with a vested interest in the outcome of the research. These include the portions where “spin” is mostly likely to enter into the paper—namely, the title, abstract, results, and conclusion sections, and any summary or “what this study adds” statements that authors are now sometimes asked to supply. These portions of research papers should instead be written by disinterested parties with subject matter expertise.
I have no illusion that these things will come to pass, but I can dream, can’t I?Elizabeth Loder is US research editor, BMJ
+ Read this blog in full and other blogs at bmj.com/blogs.

BMJ | 16 MARCH 2013 | VOLUME 346 23
LETTERS Letters are selected from rapid responses posted on bmj.com. A!er editing, all letters are published online (www.bmj.com/archive/sevendays) and about half are published in print ! To submit a rapid response go to any article on bmj.com and click “respond to this article”
judgment that prompted our analysis. We suggest that the most clinically useful starting point is to provide doctors and older patients with three to five year fracture risk estimates unadjusted for mortality risk, so that consultations can realistically cover the projected benefits of treatment for the patient concerned.Mark J Bolland senior research fellow [email protected] Jackson professor of epidemiologyGreg Gamble research fellowAndrew Grey associate professor of medicine, University of Auckland, Private Bag "#$%", Auckland %%&#, New ZealandCompeting interests: None declared.% Leslie WD, Lix LM, Wu X. Competing mortality and fracture
risk assessment. Osteoporos Int #$%';#&:()%-).# Collins GS, Michaelsson K. Fracture risk assessment: state of
the art, methodologically unsound, or poorly reported? Curr Osteoporos Rep #$%#;%$:%""-#$*.
' Steurer J, Haller C, Hauselmann H, Brunner F, Bachmann LM. Clinical value of prognostic instruments to identify patients with an increased risk for osteoporotic fractures: systematic review. PLoS One #$%%;(:e%"""&.
.Cite this as: BMJ "#$%;%&':f$&&#
BISPHOSPHONATES AND GI CANCERS
A misinterpretationVinogradova and colleagues misinterpreted the findings of our Danish national cohort study on the risk of colon cancer in bisphosphonate users.1,2 Moreover, they did not account for possible bias due to the longer survival of bisphosphonate users in the type of case-control studies that they performed.
Risk was reduced in long term bisphosphonate users (more than six months) in our study. We reported a 31% reduced risk of colon cancer and a 38% reduced risk of colon cancer mortality at five years, both of which were significant before and after adjustment for confounding (table 2). The authors must have misunderstood our dose-response analysis, which was not a comparison with the background population but a comparison of bisphosphonate users with different degrees of exposure.
The case-control design is problematic when survival is linked to exposure. This is perhaps not immediately obvious, but case-control studies only include runners in the race if they make it to the finish line, whereas cohort studies follow each runner from the start of the race.
Several studies have shown that bisphosphonate users as a group have lower mortality,3-5 thus contributing more patient years to analyses. This is accurately captured in cohort
PREDICTED FRACTURE RISK
Confused thinking Bolland and colleagues argue that estimates of fracture in older people should use a short time horizon of three to five years yet ignore competing mortality because it precludes effective treatment of these patients.1
They assume that adjustment for mortality risk in FRAX is based only on average mortality rates for the population, but the tool accommodates the fact that many risk factors that predict fracture risk also influence mortality (older age, previous fracture, low body mass index, smoking).2 The incorporation of competing mortality directly addresses the concerns raised over the time horizon used; a three to five year time horizon in older people is exactly what FRAX produces (table 2 of the article). If life expectancy is less than 10 years, then the fracture probability equals the remaining lifetime risk of fracture (table 2).
The authors ignore well recognised systematic differences in the output of the fracture prediction tools (fig 2), reflecting differences in calibration, input risk variables, outcome fractures, and incorporation of competing mortality. It is nonsensical to compare the tools against intervention thresholds that have been derived for only one of the tools (FRAX).
The real problem is not FRAX, but the setting of intervention thresholds and the complexities therein, which Bolland and colleagues do not address. Fracture rates alone as an outcome show an exponential rise with age so that treatment is indicated in all older people. Like Bolland and colleagues, we are keen to ensure optimal and appropriate use of osteoporosis drugs at all ages, but there are risks of both undertreatment and overtreatment. The authors also fail to acknowledge the importance of clinical judgment. An intervention threshold is a guideline not an absolute; clinical judgment is espoused within all guidelines, including that of the National Osteoporosis Guideline Group.Eugene McCloskey professor of adult bone diseases and honorary consultant physician, University of She+eld, Metabolic Bone Centre, Northern General Hospital, She+eld S, *AU, UK [email protected]
Juliet Compston professor of bone medicine and honorary consultant physician, University of Cambridge School of Clinical Medicine, Addenbrooke’s Hospital, Cambridge, UK John Kanis emeritus professor, University of She+eld Medical School, Beech Hill Road, She+eld S%$ #RXCompeting interests: The authors were involved in the development of FRAX or the NOGG guideline.% Bolland MJ, Jackson R, Gamble GD, Grey A. Discrepancies
in predicted fracture risk in elderly people. BMJ #$%';'&(:e)((". (#% January.)
# Kanis JA, on behalf of the WHO Scientific Group. Assessment of osteoporosis at the primary health-care level. Technical report. University of Sheffield, #$$). www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf.
Cite this as: BMJ "#$%;%&':f$&"(
Authors’ reply McCloskey and colleagues seem to misunderstand our analysis and its key messages. Firstly, fracture risk estimates should be generated for clinically relevant time frames—we suggest a three to five year interval because available interventions are effective within that time frame and it aligns with recommendations for an initial course of osteoporosis treatment. Despite their argument, FRAX generates only 10 year risk estimates. Providing patients with estimates of “remaining lifetime risk” is clinically useful only if accompanied by accurate estimates of remaining lifespan.
Secondly, adjusting for competing mortality risk is unnecessary when risk estimates are generated over short time frames because it has little impact.1
Thirdly, predicting fracture risk estimates in older patients over a 10 year time frame using calculators that incorporate competing mortality risk can obscure important short term fracture risks and treatment benefits. Because none of these messages are influenced by specific intervention thresholds or practice guidelines, the comments on those matters are not relevant.
As developers of FRAX, the correspondents can easily correct misunderstandings about FRAX methodology by publishing its equations and algorithms. This deficiency in the development of FRAX has been criticised,2 3 has hindered research,3 and differs from the approach taken for other risk calculators. The decision to charge SFr4000 (£2824; €3266; $4246) a month to use FRAX for research purposes (www.who-frax.org/) further limits accessibility.
We agree that misdirection of treatment and clinical judgment are important aspects of osteoporosis management. It was clinical

24 BMJ | 16 MARCH 2013 | VOLUME 346
LETTERS
studies, which measure event rates, but not in case-control studies, which estimate relative risk.
Cohort studies certainly have lower resolving power for rare outcomes, but they are at much lower risk of bias and provide clinicians and researchers with meaningful absolute risk estimates.Bo Abrahamsen professor, University of Southern Denmark, DK !""", Odense C, Denmark [email protected] Pazianas visiting senior fellowR Graham G Russell professor, Oxford University Institute of Musculoskeletal Sciences, Nu#eld Department of Orthopaedics, Rheumatology and Musculoskeletal Diseases, Oxford, UKCompeting interests: See www.bmj.com/content/$%&/bmj.f''%/rr/&()%)$.' Vinogradova Y, Coupland C, Hippisley-Cox J. Exposure to
bisphosphonates and risk of gastrointestinal cancers: series of nested case-control studies with QResearch and CPRD data. BMJ ("'$;$%&:f''%. ('& January.)
( Pazianas M, Abrahamsen B, Eiken PA, Eastell R, Russell RGG. Reduced colon cancer incidence and mortality in postmenopausal women treated with an oral bisphosphonate—Danish National Register Based Cohort Study. Osteoporos Int ("'(;($:(&*$-+"'.
$ Bolland MJ, Grey AB, Gamble GD, Reid IR. Effect of osteoporosis treatment on mortality: a meta-analysis. J Clin Endocrinol Metab ("'";*!:''+%-)'.
% Bondo L, Eiken P, Abrahamsen B. Analysis of the association between bisphosphonate treatment and survival in Danish hip fracture patients—a nationwide register-based open cohort study. Osteoporos Int ("'$;(%:(%!-!(.
! Lyles KW, Colon-Emeric CS, Magaziner JS, Adachi JD, Pieper CF, Mautalen C, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med (""+;$!+:'+**-)"*.
Cite this as: BMJ !"#$;$%&:f#'#%
Authors’ reply Pazianas and colleagues’ study did show a 31% reduced risk of incident colorectal cancer in alendronate users compared with non-users (adjusted hazard ratio 0.69, 95% CI 0.60 to 0.79), as we noted. The alendronate group in table 2, however, included all women with one or more prescription for alendronate, and mean follow-up was 3.4 years, so the analysis seemed to look at any duration of alendronate use, not five or more years, as the authors’ response implied. There was also no significant dose-response association in their analysis restricted to alendronate users (0.89, 0.66 to 1.22 when comparing users exposed to more or fewer than 180 defined daily doses).
We used a nested case-control design because this can better quantify time dependent exposures.1 To account for longer survival for bisphosphonate users, we matched cases and controls by age and calendar time, and required all controls to be alive and registered with the practice at the date of the first recorded diagnosis of cancer in their matched case. This ensured that survival up to the point of the case diagnosis of cancer would be equivalent between the two groups, so that the potential for bisphosphonate exposure would be comparable. All patients
with initial cancer diagnoses were included in the analysis, whether or not diagnosis was after death. To ensure an unbiased estimate of relative risk, our study was based on an underlying cohort structure, where matched controls are randomly selected from all remaining subjects at risk, including potential future cancer cases (incidence density sampling).2Yana Vinogradova research fellow in medical statistics [email protected] Coupland associate professor and reader in medical statistics Julia Hippisley-Cox professor of clinical epidemiology and general practice, Division of Primary Care, University Park, Nottingham NG( +RD, UKCompeting interests: None declared.' Etminan M. Pharmacoepidemiology II: the nested case-
control study—a novel approach in pharmacoepidemiologic research. Pharmacotherapy (""%;(%:''"!-*.
( Lubin JH, Gail MH. Biased selection of controls for case-control analyses of cohort studies. Biometrics '*)%;%":&$-+!.
Cite this as: BMJ !"#$;$%&:f#'#(
PARACETAMOL HEPATOTOXICITY
Is paracetamol ever safe?We note that the number of registrations for hepatic transplantation for paracetamol overdose found in SALT (Study of Acute Liver Transplantation) in the UK1—63 cases in 2005-07 (5.25 cases per quarter)—was the same as that reported by Hawton and colleagues.2
However, in the UK and the other European countries included in the SALT study, paracetamol had been used in the 30 days before the first symptoms in several acute liver failures that led to registration for transplantation (ALFT) not related to overdose. There were 24 cases in the UK and 49 in France, for example. Using the same criteria as for other “known hepatotoxic agents,” such as non-steroidal anti-inflammatory drugs (NSAIDs), we found that non-overdose paracetamol was associated with a three times higher rate of ALFT than all NSAIDs pooled, or individual NSAIDs such as diclofenac or nimesulide. This was true whether the denominator was in patient years or individual patients.3
Perhaps we should start looking into hepatotoxicity associated with paracetamol at normal doses? Does this have anything to do with chronic glutathione depletion and increased risk from other toxins, as was hypothesised for asthma?4Nicholas D Moore clinical pharmacologist [email protected] Gulmez associate professor in pharmacoepidemiologyPatrick Blin senior scienti,c o#cer, Department of Pharmacology, University of Bordeaux, Inserm U&!+-CIC-P""!, $$"+& Bordeaux, FranceCompeting interests: The SALT study was requested and approved by the European Medicines Agency and funded by Helsin Healthcare, which had no part in its performance, publications, or this reply.' Gulmez SE, Larrey D, Pageaux GP, Lignot S, Lassalle R, Jove J, et
al. Transplantation for acute liver failure in patients exposed to
NSAIDs or paracetamol (acetaminophen): the multinational case-population SALT study. Drug Saf ("'$;$&:'$!-%%.
( Hawton K, Bergen H, Simkin S, Dodd S, Pocock P, Bernal W, Gunnell D, Kapur N. Long term effect of reduced pack sizes of paracetamol on poisoning deaths and liver transplant activity in England and Wales: interrupted time series analyses. BMJ ("'$;$%&:f%"$. (+ February.)
$ Moore N, Gulmez SE, Larrey D, Pageaux GP, Lignot S, Lassalle R, et al. Choice of the denominator in case population studies: event rates for registration for liver transplantation after exposure to NSAIDs in the SALT study in France. Pharmacoepidemiol Drug Saf ("'$;((:'&"-+.
% Shaheen S, Potts J, Gnatiuc L, Makowska J, Kowalski ML, Joos G, et al. The relation between paracetamol use and asthma: a GA(LEN European case-control study. Eur Resp J ("");$(:'($'-&.
Cite this as: BMJ !"#$;$%&:f#'#)
CAP ON SOCIAL CARE IN ENGLAND
The perfect storm for a lawyer?The secretary of state for health, Jeremy Hunt, considers it a scandal that 30 000-40 000 people have to sell their home each year to pay for their care costs.1 2 The real scandal is that many of those people paying for “social” means tested care should be receiving free care paid for by the NHS to meet their “health” needs. Health and social needs have been defined by the Department of Health.3
The Department of Health’s latest figures show that there is a postcode lottery for NHS continuing healthcare funding.4 Recently, many primary care trusts and local authorities have simply been ignoring the law and the Coughlan ruling. The further blurring of the boundary between health and social care with the push towards integration has allowed the costs of care to be passed from primary care trusts to individual self funders (and local authorities when the assets run out). The forthcoming legislation introducing the £75 000 (€86 767; $113 175) cap should set a clear and consistent boundary between means tested social care and state funded healthcare.
Those facing a £75 000, rather than £35 000, bill for “social” care would be justified in seeking legal advice at an early stage when moving to a care home. This would help ensure that those making funding decisions on behalf of the secretary of state—clinical commissioning groups—are not acting unlawfully and thereby depriving vulnerable, frail, often demented older people of their right to fully funded NHS continuing healthcare.Nigel Dudley consultant in elderly medicine, St James’s University Hospital, Leeds LS* +TF, UK [email protected] interests: A relative of ND applied for continuing healthcare funding.' Torjesen I. Government sets -+! """ cap on social care in
England. BMJ ("'$;$%&:f*)$. ('( February.)( Watt N. Inheritance tax freeze to fund social care cap of
-+! """. Guardian ("'$ Feb ''. $ Department of Health. National framework for NHS continuing
healthcare and NHS funded care. ("'(.% Department of Health. Individuals in receipt of NHS continuing
care. ("'$. Cite this as: BMJ !"#$;$%&:f#'%$

BMJ | 16 MARCH 2013 | VOLUME 346 25
OBSERVATIONS
MEDICINE AND THE MEDIA
Hype and the HIV cure Some media reports exaggerated the significance of the recent case of a functional cure of a baby with HIV, but that’s a result of publicising unpublished, non-peer reviewed research, says Margaret McCartney
Atul Gawande, the surgeon and author, was one of the ! rst to react. “This is huge, stunning, world changing,” he tweeted, linking to a story of a “startling development” in the New York Times titled “In medical ! rst, a baby with HIV is deemed cured.” " The article explained how a baby in the United States had been treated with antiretrovirals #$ hours a% er birth, and by "& months of age the baby had no detectable viral load. The New York Times article explained that this demonstrated “proof of principle . . . if we can replicate this case.”
It also reported that other experts would need “convincing that the baby had truly been infected” and that this may have been a case of prevention of transmission rather than cure, as the BMJ also pointed out. ' It described this development in the context of other knowledge, such as the now established prophylactic treatment of babies born to infected mothers, and it called on seven experts in the article for their views, two of whom were coauthors of the original paper. Although the arti-cle acknowledged potential for excitement, it was also clear that deep uncertainty existed.
The same couldn’t be said for much of the UK media. Paper (&LB from the '$th Conference on Retroviruses and Opportunistic Infections, titled “Functional HIV cure a% er very early ART of an infected infant,” was presented in Atlanta at "$ am on ( March '$"#. # However, the press release was issued on # March, ( the same day the New York Times ran its report, before the abstract had been presented. The press release made it clear that researchers would “continue to follow the case” and that they thought that “further research is needed to understand whether the experience of the child can be replicated in clinical trials involv-ing other HIV-exposed children.”
The press release also hinted that the case was unusual because the mother had received no ante-natal care or antiretrovirals when she gave birth prematurely; additionally, treatment was stopped when the child was "& months old for “reasons that are unclear.” The press release had the sub-heading, “Discovery provides clues for potentially eliminating HIV infection in other children.” The uncertainties—the unusual nature of this case and that the ! ndings are yet to be replicated—were not
spelt out, but a quotation from one author did say that this was a “promising lead.”
This important nuance seems to have been eroded in several news reports. The Guardian ’s headline was “US doctors make history by curing child born with HIV.” It continued, “Doctors in the US have made medical history by e) ectively curing a child born with HIV . . . the child has a normal life expectancy and is highly unlikely to be infectious to others, doctors believe.” The researcher was described as “stunned” at this “extraordinary” out-come. * The story ended with a note that patients should not stop taking antiretrovirals and that
preventive treatments for preg-nant, HIV positive women were of proved e) ectiveness. There was no reminder of the unpub-lished nature of the report and its lack of peer review or the lack of replication.
Sarah Boseley in the same newspaper the next day explained the limitations of the research: “Is this the big one? Have doctors stumbled across the cure for HIV? Unfortunately not. This is progress . . . but the implications for those already infected or even the still signi! cant numbers of babies born with the virus in the developing world are sadly probably slight.” +
The Daily Mail , meanwhile, asked, “Have we found a cure for HIV? Child born with virus is now free of infection a% er ‘miraculous’ treat-ment,” and commented, “There is no guarantee that the baby will remain disease free, but early signs do look positive.” , The Telegraph hosted a video from a press conference in Atlanta, with one of the researchers, Deborah Persaud, saying that the work “sets the stage for a paediatric cure.” &
However, the Telegraph also ran another video fea-turing the HIV researcher John Frater from Oxford University, who explained the research, its limita-tions and uncertainties, and the need for patients taking antiretrovirals to continue taking them. -
Jon Snow, on Channel ! News, was right to ask straight away, “How sure are you? Has it been peer reviewed? Are you sustainably excited?” Another of the researchers answered that the development had not been published or peer reviewed but that “other researchers need to know.”
Publicising conference presentations can have problems. The abstract had not been peer reviewed and was presented after the press release. The press release did not spell out the inherent uncertainties in the meaning of this case report. It was le% to doctors not involved in the case, including many interviewed by the New York Times , and journalists to unpick the details and ask harder questions.
The risks of hype expand when unchecked enthusiasm seeks coverage before publication. Although research should be published with-out undue delay, generating press coverage is not always useful for the research community, patients, or citizens. Many comparisons in the press were made with the case of the “Berlin patient,” a man with HIV who had a bone marrow transplantation in '$$- and was subsequently found to have been functionally cured of HIV. Yet this has not, so far, been repeated. - Margaret McCartney is a general practitioner, Glasgow [email protected] Competing interests: None declared. Provenance and peer review: Commissioned; not externally peer reviewed. References are in the version on bmj.com. Cite this as: BMJ !"#$;$%&:f#'((
The abstract had not been peer reviewed and was presented after the press release. The press release did not spell out the inherent uncertainties in the meaning of this case report
Some stories had more nuance than others: Guardian (top), New York Times (left), and Daily MailSome stories had more nuance than others: Guardian (top), Guardian (top), Guardian New York Times (left), and Daily Mail

26 BMJ | 16 MARCH 2013 | VOLUME 346
PERSONAL VIEW
After Mid Staffs: NHS must look to care of its own staffNHS staff can be brutalised by severe pressure of work, which is exacerbated by the poor management exemplified by Mid Staffs, an anonymous occupational health physician believes
I worked for many years in several NHS trusts before the problems at Mid Staffordshire emerged. I was a consultant occupational physician, tasked with looking a!er the health and welfare of some "# $$$ NHS sta%. Other
consultant NHS physicians I have met have had similar experiences.
I came to the NHS as an outsider, having trained and specialised in occupational medi-cine abroad. The &rst post I held in occupational medicine in the UK, while undertaking training for membership of the faculty, was in indus-try. I found that line managers in engineering regarded the workforce in a similar way to how they view other parts of the production process: if someone was getting worn out or damaged, then the underlying cause should be &xed to prevent it happening again. Although they were not happy to see reports on new cases of work related ill health, they saw them as just as necessary as the plant engineer’s report on machine maintenance.
When I started working in the NHS I was taken aback by the resentment and anger that sta% expressed toward their employer. However, their feelings became understandable when I tried to present anonymised statistics about work related ill health to management, as I had done in industry. Managers saw my reports as likely to cause them trouble and to provide ammunition for sta% who were thinking of making compensa-tion claims. I was told that no other NHS occupa-tional health department produced such reports, and they were “&led” in the bin. NHS managers seemed not to understand that it had a duty to protect its sta% from the pressures of work. This was a callous disregard for sta% wellbeing.
As I persisted in trying to get trusts to tackle this problem over several years, I was investi-gated for spurious reasons such as “not getting on with others” and had to leave my position with a pay-o% and a gagging clause. I have applied for six other consultant posts in the NHS since. On each occasion I have been interviewed but failed to secure the post for unexplained reasons.
After leaving the NHS I analysed national statistics to see how work related ill health in healthcare sta% compared with that in workers in other industries. What I found con&rmed my impression that work related ill health was worse in the NHS. I presented a paper on this topic at a conference in the early #$$$s. It was recorded in the proceedings, which were brought to the atten-tion of the Health and Safety Executive, with no response to tackling the causes.
I found that healthcare workers were some '$% more likely to have developed work related stress, depression, or anxiety than was the general work-force at that time ("()/'$*) (#."%) v +"+/),"'- (".,%) cases; odds ratio ".'' (-*% con&dence interval ".(+ to #."#))." This odds ratio has wors-ened since then, and it is now #."$: the #$"# prev-alence of work related mental health problems in health professionals was ""$% higher than in the general workforce, as shown in recent government statistics (#*)$ v "##$ per "$$ $$$ employees).# Why is this?
Firstly, the NHS is a labour intensive indus-try that is not easily mechanised. Manual han-dling while maintaining patient dignity in o!en cramped conditions and under time pressure is di.cult. The environment is highly emotive, with near limitless demands but &nite resources.
Secondly, there were more occupational health resources available in industry compared with the NHS, despite a much higher requirement in the NHS—such as for immunisations and dealing with exposure to body /uids. For example, when I worked in industry there was one occupational health physician for every '$$$ employees, compared with one for every "" $$$ employees in the NHS; and there was one occupational health nurse for every "$$$ industry employees but one for every #'$$ NHS employees (personal observations).
The #$$- Boorman report into what health interventions would improve the wellbeing of NHS staff was a lost opportunity., The recom-mendations dealt only with the need to tackle sta% sickness absences and with providing counselling and lifestyle changes, none of which have credible evidence bases. Tackling the underlying causes of ill health (understa.ng, poor people manage-ment, inappropriate targets) was not emphasised.
Thirdly, in most organisations occupational physicians can appeal to senior management’s
altruism to try to obtain resources to promote employee health and welfare. This does not work when you are directly competing with the urgent needs of ill patients and with ongoing government initiatives to reduce waiting lists.
Fourthly, in the NHS trusts in which I worked, responsibilities for overseeing safe working prac-tices were not delegated to people who had the necessary authority. The board did not consider any statistics related to work-related ill health; no director was held responsible.
Fi!hly, a!er working in these trusts for several years I realised that most senior managers moved to new positions in three to four years. Managers seemed prepared to take the chance that they would not be in post when the results of their deci-sions became apparent.
Sixthly, the ability of an organisation to learn from its mistakes and take corrective action to prevent recurrence is essential for its survival. When shown evidence of escalating cases of work related ill health, senior NHS managers usually put the increase down to greater awareness of cases. No action was taken to prevent recurrence. Eventually, the bearer of bad news was shot.
NHS managers have not grasped the enormity of this waste. Work related ill health leads not only to the loss of sta% who provide services but also to then having to treat them as patients. The fac-tors I have identi&ed have led to the brutalisation of some NHS sta% so that they no longer respond appropriately to distress in their patients, as recorded in the inquiry in what happened at Mid Sta%s. If we wish healthcare sta% to behave with compassion they must be treated with such. References are in the version on bmj.com.Cite this as: BMJ !"#$;$%&:f#'"$
bmj ipad ( BMJ Mid Sta!s iPad special issue:
download from iTunes
When I started working in the NHS I was taken aback by the resentment and anger that staff expressed toward their employer

BMJ | 16 MARCH 2013 | VOLUME 346 27
OBITUARIES
Ian Greville TaitPioneering polymath and Benjamin Britten’s general practitioner
and Tait had masterminded his treatment for diverticulitis, subacute bacterial endocarditis, and aortic incompetence, liaising with Britten’s cardiologist and recruiting a superb nursing sister to look a!er him at home. Britten had encouraged him to make statements about his health, while the medical records were in the public domain—yet a recent biography had stated as a fact that his heart disease was caused by syphilis, despite the congenital defect found at operation and its histology as well as the previous negative serological tests. As somebody who had o!en dined at the composer’s house—invitations that were reciprocated—Tait was understandably upset but sadly died before the controversy had come fully into the open and the opposite case could be proved.
Tait leaves a wife, Janet, whom he met at Barts and to whom he was married for almost "# years. She also had an important role as a doctor in the practice, as well as being prominent in the Liberal Democrat Party; there were three sons and a daughter and nine grandchildren.Stephen Lock, former editor, BMJ [email protected] this as: BMJ !"#$;$%&:f##'"
a dowager’s message told him that GPs were received only on Fridays at $$ am, through the back door. Yet a few years later the practice was %rmly in the &#th century, with a national reputation. Not only had it adopted the rapid developments elsewhere (such as the practice ancillary team), but Tait had also pioneered a vocational training scheme, problem oriented medical records, and practice educational meetings. Surprisingly the location was Aldeburgh, the Su'olk seaside town that in E M Forster’s words is a “bleak little place, not beautiful.” As today, it contained a mixture of aristocrats, %shermen, former spooks, and musicians—including Benjamin Britten, who became Tait’s patient and friend.
Though on call &( hours most days, Tait also served the community outside medicine, becoming a town councillor, for example, in a (vain) attempt to stop ribbon housing development along the country roads. His other interests were wide. A published poet himself, he helped establish an international poetry festival, became an accomplished watercolour painter, and sailed as far and as o!en as possible, besides succumbing to the local addiction to golf.
Born in Sussex, Tait had wanted to go into the Royal Navy but was persuaded to follow the family tradition of general practice. During national service in the Royal Naval Volunteer Reserve (RNVR) at the end of the war, he was taught navigation in London by being given a map, a compass, and a tradesman’s bicycle adapted for selling ice cream and told to %nd speci%ed locations. He studied medicine at Cambridge and St Bartholomew’s Hospital Medical School, where he held house appointments before going for a year to internships at St Luke’s Hospital, New York. A!er a further junior post at Ipswich Hospital, his lifelong friend John Stevens invited him to join the practice at Aldeburgh, where he stayed for the rest of his life.
Firm Quaker principlesHandsome and modest, with a warm smile, and deeply concerned about the problems of others, Tait unsurprisingly became a member of the Society of Friends. Their %rm Quaker principles enabled him and his wife to stand
unembarrassed in Aldeburgh High Street, lobbying against the proposed war in Iraq. Similar principles had emerged earlier when the practice doctors decided to undertake attachments in the developing world, working for $) months in Swaziland. Tait’s obsession was general practice and how to make it ever better. He became deeply involved with the emerging college of general practitioners, becoming regional adviser for East Anglia and establishing his own trainee scheme linked to Ipswich Hospital. Later he was to hold three travelling fellowships, give the Gale Memorial Lecture, and serve as a visiting professor of general practice at University College Hospital, London, and at Canberra. His over-riding interest in medical records culminated in a general practice rarity, an MD degree. While in retirement he took the undergraduate course in medical history at the Wellcome Institute in London—subsequently playing an important part in its new faculty of &#th century medical history.
One of Tait’s last concerns was that somebody should refute a contentious claim that Benjamin Britten’s death was due to aortic syphilis. The composer had been his patient for several years,
“A published poet himself, he helped establish an international poetry festival, became an accomplished watercolour painter, and sailed as far and as often as possible”
Ian Greville Tait (b #(!&; q Cambridge #()$), died from pneumonia on % February !"#$.
When Ian Tait entered general practice in $*+*
Brick Dock from Round Hill, Aldeburgh. Tait studied painting with the Aldeburgh artist Tessa Henderson, becoming an accomplished watercolourist

28 BMJ | 16 MARCH 2013 | VOLUME 346
OBITUARIES
degeneration, which intruded on his great hobbies of reading and crosswords. He leaves his second wife, Barbara; four sons; two daughters; !" grandchildren; and four great grandchildren.Alan Logan Donald Logan Ian Logan Cite this as: BMJ !"#$;$%&:f##"'
Muhammad Shafiq
Consultant general surgeon (b #($); q Nishtar Medical College, Multan, Pakistan #()'; FRCS Edin), d #" September !"#!.After coming to England in !#"$, Muhammad Shafiq studied at the postgraduate medical school at Hammersmith and then became a senior house officer in trauma and surgery at the Princess Beatrice Hospital in Earls Court. He obtained the Hallet prize from the Royal College of Surgeons of England and the Lilly prize as a joint author in !#%&. After several other posts, he worked for the North Manchester Health Authority from !#'$ until the last few years. His repertoire included gastrointestinal and vascular surgery. He died after an accident while on holiday in France. He leaves his wife, Fay, and four children.John Clegg Cite this as: BMJ !"#$;$%&:f(#*
Joseph Footitt
Former Walport clinical lecturer infection in airway disease research group, National Heart and Lung Institute, Imperial College, London (b #('%; q Guy’s and St Thomas’ Medical School !"""; PhD), died in a road traffic accident in Bermuda on #$ June !"#!.Joseph Footitt managed to combine membership of committees of the Royal College of Physicians and British Thoracic Society with a demanding PhD. He was passionate about chronic obstructive pulmonary disease, and his research into the role of rhinovirus in exacerbations was beginning to spawn a flurry of journal articles when he died. His popularity with colleagues and patients is best illustrated by the fact that two of his research subjects, on hearing of his death, donated their participation fee to Joseph’s Breath of Life fund. He leaves his wife, Emma, and a son, Aneurin Max Joseph, who was born on () November ()!(.Simon Merritt Cite this as: BMJ !"#$;$%&:f##")
Alan William FowlerConsultant orthopaedic surgeon Bridgend (b #(!"; q UCH London, #(%$; FRCS Eng), died from a stroke on !# January !"#$. Alan William Fowler worked as an orthopaedic surgeon at Bridgend General Hospital from !#*& to his retirement in !#%". He published a technique for embedded toenails by excision of the germinal matrix in !#*% and for forefoot reconstruction (Fowler’s operation) for irreversible claw toes in !#*#. After retirement he was visiting professor of orthopaedics in Lusaka, Zambia. In !##* he published a review paper on the importance of joint movements in the treatment of fractures, in which he advocated
the conservative management of fractures using short splints, thus allowing for movement at adjacent joints. His wide ranging interest in medical research and practice is reflected in his book Modern Medicine and the Bible. Predeceased by his wife, Margaret, in ()!), he leaves seven adopted children.Joseph Fowler Cite this as: BMJ !"#$;$%&:f##"*
Frank Neville Garratt
Former director of public health Wolverhampton (b #(!*; q Birmingham #()#; PhD, FFCM), died from bronchopneumonia and Parkinson’s disease on #$ January !"#$.After house jobs at Birmingham General Hospital and national service with the Royal Army Medical Corps in Antwerp and Belgium, Frank Neville Garratt completed his PhD and worked as a lecturer, establishing his lifelong research interests in mental illness, learning disability, perinatal mortality, and their aetiologies. He was medical officer of health and then director of public health for Wolverhampton until his retirement in !#%#. The Neville Garratt Centre for Independent Living is a tribute to his efforts to improve health and wellbeing in Wolverhampton. He continued his research in retirement, as an honorary consultant in Walsall, with a ())# publication on maternal diet and pre-eclampsia. Neville leaves his wife, Mary; two sons; and three grandsons.David Garratt Anne McConville Kevin Kelleher Cite this as: BMJ !"#$;$%&:f#!%%
Athol Noble HepburnFormer occupational physician Ministry of Defence (b #($#; q Aberdeen #()%; DPH, FFOM), d $# December !"#!.
Athol Hepburn did his national service in the Royal Navy, specialising in aviation medicine with the Fleet Air Arm. He then served in the Royal Naval Reserve unit at HMS President in London. After working for the airline BOAC he became senior medical officer at the Royal Aircraft Establishment Farnborough and subsequently director of civilian medical services with the Ministry of Defence. He was a member of the Anglo-French Concorde aeromedical subcommittee. In the latter part of his career he worked part time at the Atomic Weapons Establishment in Aldermaston. He leaves his wife, Julia; two sons; and two grandsons.Alastair L N Hepburn Cite this as: BMJ !"#$;$%&:f##"(
William Philip Dowie Logan
Epidemiologist and former director of the Division of Health Statistics, World Health Organization (b #(#%; q Glasgow #($(; DPH, MD, PhD, FRCP), d ## December !"#!.William Philip Dowie Logan joined the General Register Office in !#$% as chief medical statistician. He was adviser on statistics to the Ministry of Health, head of the World Health Organization’s centre for classification of disease, and a panel member for health statistics for WHO. His statistical analysis of the consequences of the great smog of London on *-!) December !#*( contributed to the rapid implementation of the Clean Air Act !#*". In his later years he developed bilateral macular
Longer versions are on bmj.com. We are pleased to receive obituary notices of about !"# words. In most cases we will be able to publish only about $## words in the printed journal, but we can run a fuller version on bmj.com. We will take responsibility for shortening. We do not send proofs. Please give a contact telephone number, and email the obituary to [email protected]

BMJ | 16 MARCH 2013 | VOLUME 346 29
CLINICAL REVIEW
Achilles does not have a true synovial sheath but has a paratenon, which is a sheath of !exible connective tissue that allows for a gliding action. The paratenon and Achilles tendon are innervated by nerves from attached muscles and small fasciculi from cutaneous nerves, especially the sural nerve.4 The paratenon is a highly vascular structure, and along with the surrounding muscle complex supplies blood to the Achilles tendon.5
Cadaveric studies suggest that there is an area 2-6 cm above the calcaneal insertion with a relatively poor blood supply, and that this predisposes the region to chronic in!ammation and rupture.5 6 However, in vivo studies have failed to demonstrate this “watershed” area. Direct measurement of forces reveal loading in the Achilles ten-don to be as high as 9 kilonewtons (up to 12.5 times body weight) during running, which probably contributes to its high rate of injury.7
Tendinitis is a common term used with Achilles disor-ders. However, chronic overuse tendon injuries are not caused by inflammation—instead, histology typically shows tissue degeneration and disorganization.8 Tendi-nopathy or tendinosis are therefore more accurate terms, with tendinopathy the clinical term and tendinosis its pathological equivalent.
Recently, it has been proposed that tendon injury occurs along a continuum.9 Initially, reactive tendinopathy is caused by overload. This results in a non-in!ammatory response that thickens the tendon, reduces stress, and increases sti+ness in response to overload. If overload continues, this leads to tendon dysrepair and highly dis-organized tissue and, ,nally, degenerative tendinopathy, with even greater cellular disorder.9 It is unclear if this degeneration within the tendon is the source of pain because many asymptomatic tendons show degenerative changes.10 Painful tendons, however, show an increase in sensory and sympathetic nerves from the highly innervated paratenon and fat pad,11 which may be the source of pain in symptomatic tendinopathy.
Who gets Achilles tendon disorders?Achilles tendinopathy generally occurs in the midsub-stance of the tendon or less commonly at its insertion in the calcaneus; this di+erentiation is important because
Disorders of the Achilles tendon are common in active people—competitive and recreational athletes alike—but they can occur in less active people. As the largest tendon in the body, the Achilles experiences repetitive strain from running, jumping, and sudden acceleration or decelera-tion, so is susceptible to rupture and degenerative changes. This review aims to describe the anatomy and diagnostic evaluation of the Achilles tendon, and to discuss the best available evidence to help in the management of Achilles tendon disorders.
What are Achilles tendon disorders?The Achilles tendon is the strongest tendon in the body,1 serving both the gastrocnemius and soleus muscles. It begins near the mid-calf and inserts posteriorly at the calcaneus (,g 1). In the region where the tendon joins the bone, there is an amalgam called the enthesis organ, in which the tissue is a composite of bone and tendon.2 Kager’s fat pad is located anterior to the Achilles tendon and posterior to the calcaneus, forms the superior border of this enthesis organ, and protects the blood vessels of the Achilles tendon.2 The fat pad may also provide a mechani-cal advantage by increasing the lever angle of the Achilles tendon during plantar !exion.3 Unlike other tendons, the
!Department of Family Medicine, Eisenhower Army Medical Center, Fort Gordon, GA "#$#%, USA&Division of Sports Medicine, Department of Family Medicine, Ohio State University, Columbus, OH '"&&!, USACorrespondence to: C A Asplund [email protected] this as: BMJ !"#$;$%&:f#!&!doi: !#.!!"(/bmj.f!&(&
Achilles tendon disordersChad A Asplund,! Thomas M Best&
SUMMARY POINTSMidsubstance Achilles tendinopathy is more common than the insertional variantRupture is most common in men in the fourth and fifth decades of lifeEccentric exercises are the best treatment for Achilles tendinopathyOther modalities such as shock wave therapy are additive to eccentric exercises in the treatment of recalcitrant Achilles tendinopathyEarly weight bearing and progressive rehabilitation improve outcomes for the non-operative management of Achilles tendon rupture
!Follow the link from the online version of this article to obtain certi"ed continuing medical education credits
SOURCES AND SELECTION CRITERIAWe searched Medline (to include the Cochrane database) with the terms tendinopathy, Achilles tendon, tendon injuries, and Achilles tendon disorders. This was further limited to Achilles and finally to English language, human subjects within the past five years, and randomized controlled trials or evidence based reviews. The search yielded !" references. We reviewed the abstracts of these !" references and #! met the inclusion criteria. Further landmark studies were added.
Subcutaneous calcaneal bursaSubtendinous calcaneal bursa
Achilles tendon
Calcaneus
Gastrocnemius muscle
Soleus muscle
Lateral view Posterior view
Fig # | Anatomy of the Achilles tendon
bmj.com/multimedia ' Watch a video
demonstration of eccentric calf exercises

30 BMJ | 16 MARCH 2013 | VOLUME 346
CLINICAL REVIEW
the treatments di!er. Tendon rupture can be complete or partial and the treatments for both of these will also be discussed.
TendinopathyThe most common causes of Achilles disorders are mid-substance tendinopathy (55-65%), followed by insertional tendinopathy (20-25%).12 Achilles tendon disorders can a!ect anyone, but they most commonly a!ect active peo-ple, especially those who participate in running or jumping sports. In a cohort study with an 11 year follow-up, Achil-les tendon overuse injuries occurred in 29% of runners compared with 4% of non-runners; the age adjusted odds ratio was 10.0 in runners compared with controls.13
Age, male sex, and obesity have been cited as risk fac-tors for Achilles tendon disorders, but a recent study of athletes over 40 years of age found no in*uence of any of these factors.14 15 A study of military recruits found that decreased plantar *exion strength and extremes of dorsi*exion (too much or too little) were associated with Achilles disorders.16 Abnormal subtalar joint motion has also been found to contribute to midsubstance tendinopa-thy.17 A positive family history raises the risk of Achilles tendinopathy almost five times, suggesting a possible genetic link.15 Medical factors that may be associated with Achilles injury include hypertension, hyperlipidemia, and diabetes—presumably secondary to glycation or systemic in*ammation.18
Tendon ruptureIt is now recognized that most tendinopathies are rarely associated with one single factor, and the degenerative process that precedes rupture likely results from a variety of di!erent pathways and causative factors. Degenerative changes are likely over age 35 years and contribute to the increased susceptibility to tendon rupture.10 Achilles ten-don ruptures are most common in men in the fourth to ./h decade of life, perhaps because degenerative changes have started but activity levels are still high.19 The incidence of Achilles tendon rupture is seven injuries per 100 000 in the general population and 12 injuries per 100 000 in com-petitive athletes.19 Finally, a history of Achilles rupture places the person at a higher risk of injury to the contral-ateral Achilles.20 Running, jumping, or sudden explosive or eccentric activities are the usual mechanisms for rup-ture.21
Drugs may be associated with Achilles rupture in less active older adults. A population based cohort study found that *uoroquinolone antibiotics are associated with 12 epi-sodes of rupture per 100 000 treatment episodes.22 Another population based drug safety study found that use of *uor-oquinolones increased risk for tendon disorders (odds ratio 1.7, 95% con.dence interval 1.4 to 2.0) and Achilles rup-ture (4.1, 1.8 to 9.6), whereas concomitant use of *uoro-quinolones and oral corticosteroids signi.cantly increased the risk of Achilles rupture (43.2, 5.5 to 341.1).23
How are Achilles tendon disorders evaluated?A thorough history and physical examination are the .rst steps in the diagnosis of Achilles tendon disorders. The history should include pattern of symptoms—onset, dura-
tion, cessation, plus alleviating and exacerbating factors. Ascertain the level of training, previous injury, and previ-ous treatments. Also determine the presence of risk factors, such as previous injury, family history, medical history, and drug use.
TendinopathyPatients with tendinopathy generally describe pain or sti!ness in the Achilles 2-6 cm above the calcaneal inser-tion.24 Morning sti!ness is common, and the pain is usu-ally worse with activity, although it may continue into rest. Less commonly, patients will describe similar symptoms with point tenderness over the insertion of the Achilles on the calcaneus.
Inspection of the patient’s gait may elicit the presence of overt gait abnormalities. With the patient in a prone posi-tion, palpate the distal lower leg to assess areas of tender-ness. Tenderness in the body of the tendon or directly over the insertion, with or without crepitus, suggests tendin-opathy. Swelling around the tendon or crepitus with active motion may indicate inflammation of the paratenon. Tendinopathy and paratendinopathy may coexist.25 In isolated paratendinopathy, there is local thickening of the paratenon. Finally, assess range of motion (passive and active) and strength testing to plantar *exion, dorsi*ex-ion, eversion, and inversion, along with subtalar mobility to evaluate for restrictions to motion or muscle weakness, which would predispose to re-injury. It is essential to com-pare the injured limb with the contralateral non-injured limb to appreciate subtle di!erences.
Severity of tendinopathy, as well as response to treat-ment, can be assessed by using a validated outcome meas-ure such as the Victorian Institute of Sport assessment (VISA-A), which consists of eight items to assess sti!ness, pain, and function.26
RuptureClassically patients with complete tendon rupture will describe the feeling of “being shot or hit in the back of the leg,” typically while performing an explosive running or jumping maneuver, with immediate pain and an inability to continue their current activity.
Because gravity and activity of the tibialis posterior, peroneals, and long toe *exors can cause active plantar *exion, examine patients for suspected rupture while they are prone. Ecchymosis suggests tendon rupture, and a
A PATIENT’S PERSPECTIVEI am a !" year old competitive runner. When running on the beach while on vacation I suddenly felt a burning pain in my left mid-calf. This was followed by a sudden pop and I was unable to finish the run. Examination showed ecchymosis and a small palpable defect in the lateral border of the left Achilles tendon near the myotendinous junction with a negative calf squeeze test. Magnetic resonance imaging demonstrated a #$-$%% tear of the Achilles tendon at the myotendinous junction. After an initial period of limited weight bearing, ice, and compression, I underwent an ultrasound guided platelet rich plasma injection. I was placed in a walking boot for six weeks followed by a progressive rehabilitation eccentric exercise program. Four months after the initial injury, I have started running again.
bmj.com Previous articles in this series
! Malignant and premalignant lesions of the penis (BMJ !"#$;$%&:f##%')
! Postpartum management of hypertension (BMJ !"#$;$%&:f('%)
! Diagnosis and management of pulmonary embolism (BMJ !"#$;$%&:f)*))
! Anaphylaxis: the acute episode and beyond (BMJ !"#$;$%&:f&"!)
! Ulcerative colitis (BMJ !"#$;$%&:f%$!)
! Prostate cancer screening and the management of clinically localized disease (BMJ !"#$;$%&:f$!*)

BMJ | 16 MARCH 2013 | VOLUME 346 31
CLINICAL REVIEW
palpable defect may exist within the !rst hours of rupture. Tendon rupture can be con!rmed with the calf squeeze test, where the examiner gently squeezes the patient’s calf muscles with the palm of the hand—if the tendon is intact, plantar "exion will occur, if torn the ankle will remain still. Test both legs to assess for di#erences. Sensitivity and spe-ci!city of this test have been measured at 0.96 (0.91 to 0.99) and 0.93 (0.76 to 0.99), respectively.27-29
What is the differential diagnosis of posterior heel pain?Posterior heel pain can be a diagnostic challenge—consider Achilles tendinopathy (midsubstance or insertional) and tendon rupture (partial or complete). Achilles disorders will localize pain to the Achilles tendon, typically along its course from the insertion on the heel to its transition into the conjoined tendon of the gastrocnemius and soleus. However, di#erential diagnoses include retrocalcaneal bur-sitis or enthesitis, plantaris muscle injury, posterior ankle impingement, and sural nerve impingement or entrap-ment.
Retrocalcaneal bursitis may occur near the distal inser-tion of the Achilles and may mimic insertional tendin-opathy, and both disorders can occur simultaneously. In Achilles enthesitis, in addition to the tendon !ndings, an
e#usion is o+en present in the retrocalcaneal bursa. This condition can be investigated using three !nger palpation. The middle !nger and thumb are placed on each side of the Achilles while the index !nger palpates the distal tendon; "uctuation palpated with the index !nger can indicate e#usion of the retrocalcaneal bursa.30 The plantaris muscle is a vestigial rope-like structure seen in 7-20% of the popu-lation.31 It lies deep to the proximal lateral gastrocnemius muscle, travels obliquely, and inserts near the medial bor-der of the Achilles tendon; in some cases it fuses with the Achilles.32 Injury to the plantaris can mimic the symptoms seen with Achilles tendon disorders and can be diagnosed with magnetic resonance imaging (MRI) or ultrasound.33 34 Posterior impingement of the ankle refers to impingement of the posterior talus by the posterior aspect of the tibia when the ankle is in extreme plantar "exion. In this con-dition, pain occurs in the posterior ankle but increases with passive plantar "exion of the ankle, unlike in Achil-les tendinopathy, in which the pain lessens. Finally, sural nerve entrapment or impingement may cause pain in the posterior distal leg and may mimic Achilles pathology.
What is the role of imaging in Achilles tendon disorders?Most Achilles disorders are diagnosed clinically. Imaging may be useful, however, when the diagnosis is unclear or when trying to di#erentiate between complete or partial tendon rupture. Ultrasound and MRI are useful when clini-cal examination does not yield a de!nitive diagnosis.
MRI is useful in the diagnosis of tendon disorders because it can detect abnormalities in the entire locomotor unit, including the tendon, calcaneus, Achilles insertion, retrocalcaneal bursa, peritendinous tissues, and musculo-tendinous junction. MRI !ndings also correlate with !nd-ings at surgery and may be useful for surgical planning.35
Ultrasound, however, can provide a dynamic assessment of the tendon and can evaluate for tissue neovasculariza-tion. Perhaps more importantly, it can be used to guide per-cutaneous procedures and is therefore becoming a popular imaging tool. In a prospective blinded comparison study of ultrasound and MRI for identi!cation of Achilles tendinop-athy, both had similar speci!city, but MRI had better sensi-tivity (95% v 80%).36 However, a recent retrospective study comparing MRI with physical examination found that MRI was less sensitive in the diagnosis of Achilles tendon rup-ture and may be useful only for operative planning.37 In a prospective longitudinal cohort study, ultrasound was used to measure neovascularization before and a+er eccentric exercises to help predict patient outcome, with a decrease in neovascularity corresponding to patient improvement.38 It has been suggested that, in trained hands, ultrasound is better for focused examinations or for guiding intervention, whereas MRI is better for global assessment of the tendon or for operative planning.39
What are the treatment options?Figure 2 shows an algorithm for the treatment of Achilles tendon disorders. Consider conservative treatment !rst for most Achilles tendon disorders. The aims of treatment are load reduction and pain management. Advise patients with tendinopathy to reduce or discontinue the o#ending activ-ity, weight bear as tolerated, use a heel li+ to e#ectively
Patient presents with Achilles pain
Consider referral to sports medicine specialist for advanced modality(low energy shock wave treatment, injection, laser therapy)
Calf squeeze test to exclude rupture
Surgical consultation Conservative management
Begin eccentric exercise program, consider physiotherapy referral
Order imaging to better evaluate
Continue maintenance program !-" monthsConsider adding glyceryl trinitrate patch
Unclear
ResponseNo response
No response
Negative
If no improvement in #-$% days
Positive
Fig ! | Algorithm for the treatment of Achilles tendon disorders
ADDITIONAL EDUCATIONAL RESOURCES Resources for healthcare professionalsAmerican Academy of Orthopaedic Surgeons. The diagnosis and treatment of acute Achilles tendon rupture: guideline and evidence report. !""#. www.aaos.org/research/guidelines/atrguideline.pdf Carcia CR, Martin RL, Houck J, Wukich DK. Achilles pain, stiffness, and muscle power deficits: Achilles tendinitis clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther !"$":%":A$-!&. Maffuli N, Almekinders LC. The Achilles tendon. Springer, !""'Alfredson H, Cook J. A treatment algorithm for managing Achilles tendinopathy: new treatment options. Br J Sports Med !""';%$:!$$-&Resources for patientsKreher JB. Achilles tendinopathy: everything you need to know (and more). What you should know about Achilles tendinopathy to prevent its occurrence and to stop it in its tracks before it stops you. www.beginnertriathlete.com/cms/article-detail.asp?articleid=$&#% Beginnertriathlete.com (www.beginnertriathlete.com/cms/article-detail.asp?articleid=$($()—Video case study on Achilles tendonitis

32 BMJ | 16 MARCH 2013 | VOLUME 346
CLINICAL REVIEW
Insertional tendinopathyMuch of the evidence is for the treatment of midsubstance tendinopathy, and it is unclear if it directly translates to treatment of insertional tendinopathy. A systematic review of 11 studies concluded that conservative treatment, including eccentric loading exercises and shock wave therapy, should be attempted before operative interven-tion.49 A small pilot study to evaluate the e$ect of painful eccentric loading exercises without dorsi%exion (di$erent from eccentric loading exercises for midsubstance tendi-nopathy) found that two thirds of the patients who per-formed such exercises improved clinically. Interestingly, combined disease (such as tendon, bursa, or enthesitis) at the insertion does not exclude a satisfactory response to this training regimen.50 Finally, a larger RCT of people with chronic insertional tendinopathy found that low energy shock wave therapy may be superior to eccentric loading exercises in improving functional outcome scores.51 This treatment may be useful in patients with a poor initial response to eccentric loading exercises.
Achilles ruptureComplete ruptureSurgery is o(en recommended for complete Achilles rup-ture, but there is some controversy about its long term e$ec-tiveness. A meta-analysis of six RCTs comparing minimally invasive surgery with conventional approaches found no signi)cant di$erence in outcomes, although minimally invasive surgery resulted in fewer infections and greater patient satisfaction.52 In a Cochrane systematic review, open surgery was associated with a much lower rate of re-rupture than conservative treatment but had a higher rate of complications.53 If surgical repair is performed, current evidence supports a minimally invasive technique, and evi-dence supports early weight bearing to improve functional outcome scores.54
Although surgery is generally considered the gold stand-ard, two RCTs comparing surgery to conservative manage-ment with immobilization for complete tendon rupture showed no signi)cant di$erence a(er one year in func-tional outcomes.55 56 Another RCT of operative versus non-operative (accelerated functional rehabilitation program) treatment of Achilles tendon rupture found that all outcome measures, including rate of re-rupture, were similar in both groups.57 In this study, all patients wore a walking boot with a 2 cm heel li( two weeks a(er injury; early range of motion and weight bearing as tolerated started at four to six weeks and strength exercises at six to eight weeks. Finally, an RCT of early motion plus surgery versus early motion without surgery suggested that controlled early motion is an impor-tant part of treatment for a ruptured Achilles tendon.58 Therefore, recent studies indicate that good outcomes may be achieved without surgery, especially with accelerated functional rehabilitation and early motion. Maintain a high level of suspicion for deep venous thrombosis, the incidence of which is high a(er complete rupture.59
Because outcomes can be similar for conservative or surgical management, it is useful to know which patients are most suitable for surgery. Non-surgical management is generally best for older less active patients or those with poor skin integrity or wound healing problems.53 Surgical
shorten the Achilles and reduce load, and use acetami-nophen (paracetamol) as needed for pain. Refer patients with complete rupture to a surgeon for advice about treat-ment options. Additional treatments for speci)c Achil-les tendon disorders are outlined below. If conservative measures fail, refer to a sports medicine or orthopaedic specialist.
Midsubstance Achilles tendinopathyEccentric calf exercises have the most evidence and best outcomes for the treatment of midsubstance Achilles tendinopathy. A meta-analysis of 11 randomised control-led trials (RCTs) found that eccentric exercises improved pain, patient function, and satisfaction compared with control treatments, such as concentric exercises, stretch-ing, splinting, and ultrasound.40 Another systematic review of 16 RCTs of non-operative treatments for midportion Achilles tendinopathy found that eccentric exercises had the most evidence of e$ectiveness.41 Furthermore, a )ve year follow-up study of an RCT found sustained long term improvement with eccentric exercises performed according to Alfredson’s heel drop program.42 Currently, we recom-mend Alfredson’s method of performing three sets of 15 repetitions, twice a day, every day for up to 12 weeks (see video).43
Does the addition of other treatments to eccentric exer-cises improve results? Two RCTs found that the addition of low energy shock wave treatment to eccentric exercises is more e$ective than eccentric exercise alone.44 45 Finally, the addition of low level laser therapy to eccentric exer-cises accelerated clinical recovery.46 Therefore both of these treatments may be additive to eccentric exercise and may be useful in patients who do not respond to the initial eccentric exercises.
Topical glyceryl trinitrate has been used to treat tendi-nopathies, but is it e$ective for Achilles tendinopathy? A meta-analysis of seven studies showed that glyceryl trini-trate reduces pain during activities of daily living in chronic tendinopathies, with an odds ratio of 4.44 (2.34 to 8.40), and in acute and chronic phases combined, with an odds ratio of 4.86 (2.62 to 9.02).47 For the speci)c treatment of Achilles tendinopathy, another systematic review found two RCTs of topical glyceryl trinitrate alone in the treatment of chronic (more than six weeks) Achilles tendinopathy. One trial found a bene)t of glyceryl trinitrate in terms of pain on activity or at night and tendon tenderness, but the other trial found no di$erence from placebo at six months on pain at rest or with activity.47 Finally, another RCT com-paring physical therapy plus topical glyceryl trinitrate with therapy alone found that addition of glyceryl trinitrate was of questionable bene)t.48 Despite evidence at the cellular level of the role of nitric oxide in tendon healing, results of clinical studies in human Achilles tendons have been con%icting, so further validation is needed. If glyceryl trini-trate is used, we recommend cutting a 5 mg 24 hour patch into four and placing one quarter over the area of maximal tenderness or pain. Leave the patch in place for 24 hours and then replace the patch daily until pain subsides or 12 weeks of treatment have been completed, when patient centered outcomes such as pain and function should be re-evaluated.

BMJ | 16 MARCH 2013 | VOLUME 346 33
CLINICAL REVIEW
successful return to sports and long term outcome a!er treatment of a partial Achilles rupture with the injection of platelet-rich plasma followed by a progressive rehabili-tation program.62 63 Platelet-rich plasma may be a useful addition to the current conservative management options for partial Achilles tendon ruptures, although more de&ni-tive studies are needed before it can be recommended.
What is the prognosis?Most people who develop Achilles tendinopathy will improve with conservative treatment. In general, signi&-cant decreases in pain and improvement in function occur a!er 12 weeks of intervention.64 A long term follow-up study showed that 85% of patients with Achilles tendinopathy had full normal function and continued to be asymptomatic eight years a!er injury.65 Surgery for tendinopathy is reserved for patients who do not respond a!er six months of conservative measures. Nevertheless, 24 of the 83 patients in the long term follow-up study did not respond to conservative treat-ment and underwent surgery.65
Treatment of complete Achilles rupture is controversial, but good outcomes have been seen a!er both operative and non-operative approaches.55-57 Regardless of treat-ment approach, functional de&cits may persist for up to two years.66 It is therefore important to advise patients of the potential for a long recovery.Contributors: CA and TB conceived and designed the article. CA performed the literature search and wrote the initial dra!. TB revised this and further dra!s. All authors approved the "nal version. CA is guarantor.Competing interests: None declaredProvenance and peer review: Commissioned; externally peer reviewed.Patient consent obtained.References are in the version on bmj.com.
management is recommended for young people, active high level athletes, and those in whom non-surgical manage-ment has been unsuccessful.
Partial ruptureMuch of the research into the treatment of Achilles rupture has been performed on complete tendon rupture rather than partial rupture. It is di,cult to di-erentiate partial tears from tendinopathy. Imaging may help, but MRI &nd-ings can overlap substantially.60 Ultrasound can di-er-entiate full thickness tears from partial thickness ones or tendinosis of the Achilles tendon with 92% accuracy,36 61 so should be used in this situation.
Tendon repair can be slow and incomplete, and par-tial tendon ruptures o!en respond poorly to conservative measures. Surgery has therefore been the recommended treatment,41 even though it has a long recovery period and greater incidence of complications. Recently, despite the apparent lack of e-ectiveness of platelet-rich plasma for treating Achilles tendinopathy, two case reports found a
AREAS FOR FUTURE RESEARCHThe role of biological agents in the treatment of Achilles tendon disordersThe role of ultrasound or advanced imaging techniques as prognostic tools in Achilles disorders
TIPS FOR NON!SPECIALISTSEccentric exercise programs have the best success rate for Achilles tendinopathyConsider surgical referral if no response after six months of conservative treatment or for acute complete rupture of the Achilles tendon
ANSWERS TO ENDGAMES, p 40 For long answers go to the Education channel on bmj.com
CASE REPORTAn unexpected finding after a fall from a horse! A white blood cell count greater than "#$!#%/L is caused by a primary
haematological disease or, less commonly at such a high value, a leukemoid reaction. A leukemoid reaction may be lymphoid or myeloid in nature and is a physiological response of the bone marrow to a strong stimulus, such as infection, drugs, or an underlying solid cancer.
& The chronic phase of chronic myeloid leukaemia (CML).' In addition to blood count and differential, examination of a blood film and
bone marrow biopsy will help to exclude other differential diagnoses, such as other myeloproliferative disorders (polycythaemia rubra vera, essential thrombocytopenia, myelofibrosis) or chronic myelomonocytic leukaemia, and will help determine the stage of CML. Further confirmation can then be obtained using cytogenetics to look for the presence of the Philadelphia chromosome (t(%;&&)(q'(;q!!)) and of the BCR-ABL transcript.
( Treatments include disease control with targeted treatment—the tyrosine kinase inhibitors, such as imatinib—and potential cure with allogeneic haematopoietic stem cell transplantation.
" To reduce the risk of gout and tumour lysis syndrome in response to cytoreductive treatment.
STATISTICAL QUESTIONNormal rangesStatement b is true, whereas a and c are false.
PICTURE QUIZPeri-oral papules! This cluster of papules in a peri-oral distribution is
molluscum contagiosum.& It is unusual to find multiple molluscum lesions
on the face of a healthy adult so look for causes of immunocompromise. Investigations should include a full blood count and HIV serology.
' Treatment is not usually needed in children or young adults because molluscum contagiosum resolves spontaneously in most cases. In atypical infections topical imiquimod or cryotherapy can be used.
( Skin disease may be the first sign of HIV infection. Cutaneous infections and skin malignancies are more common in HIV positive patients.

34 BMJ | 16 MARCH 2013 | VOLUME 346
PRACTICE
!Africa Centre for Health and Population Studies, University of KwaZulu-Natal, South Africa"School of Medicine, Glasgow University, Glasgow G!" #XX, UK$Centre for Paediatric Epidemiology and Biostatistics, University College London Institute of Child Health, London WC!E %BT, UKCorrespondence to: R Bland, Africa Centre for Health and Population Studies, University of KwaZulu-Natal, PO Box !&#, Mtubatuba, KwaZulu-Natal, $&$', South Africa [email protected] this as: BMJ !"#$;$%&:f''"doi: !(.!!$%/bmj.f''(
Problem Infants and young children infected with HIV as a result of mother to child transmission are not being identi!ed or started with antiretroviral treatment (ART) in line with HIV guidelines in resource limited settings.Design Retrospective analysis of data from a paediatric cohort before and a"er an intervention strategy.Setting Rural public HIV treatment programme in the province of KwaZulu-Natal, South Africa.Key measures for improvement Increase in the number of HIV infected infants and children who start HIV treatment each year; increase in the proportion of children starting ART with less immune suppression, shown by higher CD# counts and less advanced World Health Organization clinical stages for HIV.Strategies for change Late $%%&: training in paediatric HIV for all sta' in contact with mothers and children; campaigns for increased HIV testing at immunisation and clinics; routine testing of children with tuberculosis and malnutrition for HIV, and HIV testing of all children admitted to hospital. The establishment of a family HIV clinic in late $%%(. E!ects of change The number of children () year to *)+ years) starting ART each year increased from #, in $%%# to $+# in $%)); the corresponding number of infants (<) year) starting treatment increased from $ to +-. A trend towards increasing CD# counts at the start of treatment was found.Lessons learnt It is possible to improve the identi!cation of HIV infected children and ensure a prompt start on ART where needed with relatively simple measures and limited implications for sta.ng and budgets.
The setting is an HIV treatment and care programme in Hla-bisa, a rural sub-district of the province of KwaZulu-Natal, South Africa. In 2011, the population of Hlabisa was about 220 000 people, of whom an estimated 37.8% (83 160) were children aged 1 year to ≤15 years and 2.4% (5280) infants aged <1 year. The area has a high burden of both HIV and tuberculosis,1 2 with an estimated overall HIV prevalence in 2010 of 23% among adults, with no evidence of a sub-stantive decline in HIV incidence.3 In 2011 there were about 5000 deliveries, of which an estimated 2000 were to HIV positive women (Africa Centre Surveillance, www.africa-centre.com). The noti,cation rate of adult tuberculosis in Hlabisa more than doubled between 2003 and 2008, from an estimated 707 per 100 000 a year to 1700 per 100 000; 75% of those adults were HIV positive.
Since 2004 the Africa Centre for Health and Population Studies (www.africacentre.com), funded by the Wellcome Trust, has partnered with the local Department of Health in implementing and running a comprehensive HIV pro-gramme in Hlabisa.4 From inception, additional funding was provided by PEPFAR, the United States’ President’s Emergency Plan for AIDS Relief, to support activities includ-
QUALITY IMPROVEMENT REPORT
Maximising opportunities for increased antiretroviral treatment in children in an existing HIV programme in rural South Africa Ruth M Bland,1 2 James Ndirangu,1 Marie-Louise Newell1 3
ing monitoring and evaluation, sta- training, and manage-ment of the programme. The programme was initially based at the local 250-bed hospital but rapidly decentralised, with clients accessing HIV services at their nearest clinic, along with other primary care services, including antenatal services, child growth, immunisation clinics, tuberculosis services, and management of undernutrition. Attendance at clinics for antenatal and child health monitoring in Hlabisa is high, with over 95% of pregnant women attending for at least one antenatal visit5 and primary vaccination in the ,rst 6 months of life being achieved in over 80% of children.6 The programme is led by nurses and counsellors, with doc-tors (mostly without postgraduate specialisation) visiting clinics to start antiretroviral treatment (ART) and manage clinical problems during follow-up. Most clinics are typical of small facilities in rural South Africa, with limited physical space and shortages of healthcare workers. One or two HIV counsellors and one to four primary healthcare nurses cov-ering all services are allocated to each clinic, with a ratio of 795 HIV positive patients receiving ART per nurse, and 386 per counsellor (Till Barnighausen, personal communication, 2012). Numbers of people starting ART have increased sub-stantially since the start of the programme, from 1800 at the end of 2006 to over 17 000 at the end of 2011, 73% of whom were female and 10% of whom were children aged <15 years.
The clinics in the programme follow national and pro-vincial guidelines (re/ecting international World Health Organization recommendations7) for starting and con-tinuing treatment in HIV positive children. Healthcare and medications, including antiretroviral drugs, are free for chil-dren in South Africa and are provided by the government. Testing for HIV in pregnancy is on an “opt-in” basis, with high rates of testing (>90%); HIV testing using polymer-ase chain reaction at age 6 weeks is recommended for all infants born to HIV infected mothers, with results available two weeks later. Children aged >18 months not previously tested or with clinical signs or symptoms suggestive of HIV are tested using HIV antibodies with immediate results. Antiretroviral drugs are started on the basis of a combination of clinical and immunological criteria, dependent on age. The South African guidelines for paediatric HIV treatment were updated in 20108 in response to revised WHO recom-mendations,9 including HIV treatment of all HIV infected infants (aged <12 months) irrespective of their clinical or immunological status.
In South Africa the estimated number of children starting ART each year has risen from 4200 in 2004 to 152 000 in 2011. However, assessing the proportion of eligible children who have started ART is challenging in this setting. Cover-age of HIV treatment in children in South Africa has been estimated in ongoing work by Johnson and colleagues at the Centre for Infectious Disease Epidemiology and Research,
bmj.com Previous articles in this series
( A general practitioner and nurse led approach to improving hospital care for homeless people (BMJ "(!";$)':e'&&&)
( Lessons from the Johns Hopkins Multi-Disciplinary Venous Thromboembolism (VTE) Prevention Collaborative (BMJ "(!";$)):e$&$')
( An integrated paediatric to adult clinical service for young adults with kidney failure (BMJ "(!";$)):e$*!#)
( Improving MMR vaccination rates: herd immunity is a realistic goal (BMJ "(!!;$)$:d'*($)
( Intraoperative fluid management guided by oesophageal Doppler monitoring (BMJ "(!!;$)":d$(!%)

BMJ | 16 MARCH 2013 | VOLUME 346 35
PRACTICE
aged <1 year.21 Using local facility and population based data and a deterministic model, we also calculated the number of children in need of treatment22 and estimated that by the end of 2007 only two thirds of children who were in need of treatment and were still alive had started ART; this represents a huge unmet need.
We recognised that many opportunities were missed in the existing system to identify infants and children who were HIV positive, and we postulated that this was the result of problems in the health system rather than lack of resources, unclear guidelines, or unwillingness of parents to bring their children to clinics for testing. Here we describe initiatives introduced in late 2008 to improve early detection of HIV positive infants, to increase diagnosis of older children who missed being identi&ed in infancy, and the impact of these strategies on the number and characteristics of children starting ART.
Key measures for improvementOur aim was to identify perinatally infected HIV positive children as early as possible and start ART as appropriate; to diagnose older HIV positive children who had missed being tested as infants; to start ART in children before they were clinically unwell; and to ensure sustainability of these improvements.
Key outcomes measured were:• Number of HIV positive infants (children aged <12
months) starting ART • Number of HIV positive children aged 1 to ≤15 years
starting ART• Proportion of children starting ART with higher CD4
counts or CD4% values (indicating less immune suppression) and at WHO stages 1-2 rather than stages 3-4 (indicating better health).As discussed above, providing an accurate denominator
for children eligible for ART, and thus being able to report on the proportion of eligible children receiving HIV treatment, poses a problem in our setting. It relies on accurate numbers of HIV infected pregnant women (and thus accurate num-bers of HIV exposed infants) and on accurate numbers of HIV exposed infants known to be HIV infected in utero and during delivery. We have good estimates of the proportion
University of Cape Town.10 Their models (rather than data collected from treatment sites) are available for national trends and indicate that increasing numbers of children have started ART since 2004. However, these modelled estimates cannot be split down to provincial or local level, and rural areas are probably lagging behind urban centres.
ProblemWorldwide, in 2008 an estimated 430 000 children became infected with HIV (mostly via mother to child transmission), of whom 90% live in sub-Saharan Africa.11 Without treat-ment children progress rapidly to disease, with about 20% of perinatally infected infants dying within the &rst year of life, and 50% by their second birthday.12 However, early ART leads to increased survival, improved morbidity, and immu-nological bene&ts.13-15
Despite the roll-out of prevention of mother to child trans-mission programmes and increasing availability of HIV testing with polymerase chain reaction to identify perina-tally infected infants at age 4-8 weeks, follow-up of infants remains inadequate in resource limited settings.16 17 Prob-lems cited include “vertical” systems in primary healthcare facilities and lack of integration of prevention of mother to child transmission programmes with other maternal and child health initiatives, such as immunisation and growth monitoring; missed opportunities to identify HIV positive children postnatally; poor turnaround time of results owing to lack of capacity in laboratories and transport problems from rural areas; and lack of training of primary healthcare sta/ to recognise and refer potentially HIV positive children, particularly older children, who have little routine contact with the health facilities. Although guidelines exist, putting these into practice in already overburdened health sys-tems remains an enormous challenge. As a result, outside research settings many children die before diagnosis, and those who progress more slowly are diagnosed relatively late, usually presenting with illness at an advanced stage of disease.18-20
We have previously reported on the &rst four years (2004-08) of our decentralised nurse and counsellor driven HIV treatment programme in rural South Africa, in which 477 children had started receiving ART, of whom very few were
Table ! | Children (aged "!# years) starting antiretroviral treatment (ART) each year, $%%&-!!
Year
No of children Proportion of all children (out of total No in programme) (%)
Estimated mother to child transmission rate at age ' weeks (%)
Estimated No of new paediatric cases of HIV infections*
Aged <! year
Aged ! -"!# years Total
Jun !""# to Sep !""$ ! #% #$ & '#† !("Oct !""$ to Sep !"") ' && '"" ( '# !("Oct !"") to Sep !""* ) ')' ')* ( '!‡ !#"Oct !""* to Sep !""( !" !$' !*' ( (§ ')"Oct !""( to Sep !""& )' #'# #*$ '% ) '!"Oct !""& to Sep !"'" $& !(* %#) & #¶ ("Oct !"'" to Sep !"'' $& !$# %'% * %** )"*Out of total of !""" HIV positive women. †Data from a large mother to child transmission programme in Hlabisa sub-district.!%‡Increasing numbers of HIV positive women with low CD# counts started ART between !""# and !""), resulting in an estimated decrease in the rate of mother to child transmission of HIV.§New guidelines were introduced in February !""(, including provision of zidovudine to all pregnant women not already receiving ART from !( weeks’ gestation. By this period the ART programme was well established for adults, with no waiting times for treatment, and most women with CD# counts <!"" cells/µL had started ART for life.¶Estimated further decrease in the rate of mother to child transmission of HIV as more women with low CD# counts had started ART for life, and the guidelines rolled out in February !""( had been fully implemented across the Hlabisa sub-district.**In August !"'" new guidelines for prevention of mother to child transmission were introduced, including: zidovudine for all pregnant women not already receiving ART from '# weeks’ gestation; all pregnant women with CD# counts <%$" cells/µL (rather than <!"" cells/µL) to start ART for life; and all infants aged <' year to start ART.

36 BMJ | 16 MARCH 2013 | VOLUME 346
PRACTICE
initial roll-out of the programme there have been no wait-ing lists for patients needing ART. A prevention of mother to child transmission programme had been operating in the Hlabisa area since 2001, with provision for all pregnant HIV positive women to receive appropriate management at their nearest local clinic. Before 2010 women received sin-gle dose nevirapine in labour; this was changed in August 2010 to: (a) combination ART for life for women with CD4 counts of ≤350 cells/µL, and (b) for the remaining women, zidovudine monotherapy from early pregnancy plus single dose nevirapine and a dose of emtricitabine plus tenofovir in labour and oral daily nevirapine for their infants for at least six weeks.
Analysis and interpretationIn the (rst four years of the programme (June 2004 to Sep-tember 2008) we identi(ed two problems:• Few of the children starting ART were aged <1 year
(table 1)• Children starting ART had low CD4%, low CD4
counts, high WHO clinical stages (suggesting immune compromise at start of treatment), and CD4 counts well below the eligibility criteria for treatment (table 2).Therefore, we examined the cascade of HIV care from
pregnancy to early childhood to identify why so few infants were starting ART despite our estimates of expected need.22 As clinic waiting times and the cost of antiretroviral drugs
of pregnant women who are HIV infected from anonymous surveillance at the Africa Centre and from the Department of Health. However, we do not know the exact number of HIV exposed infants who are HIV infected as some may not have been tested for HIV and others may have died before having the opportunity to be tested for HIV. Therefore, our denominator for eligible children remains an estimate based on several assumptions (table 1), and we provide our (rst two key outcomes as numbers rather than proportions.
Process of gathering informationBaseline clinical and laboratory data of all children start-ing ART in the HIV programme are collected from paper based records stored at clinics and entered into a secure, electronic database hosted at the Africa Centre. We analysed data from all children in the programme from June 2004 to September 2008 before implementing our intervention, and from October 2008 to September 2011 a+er introducing the improvement strategies. Characteristics at the start of ART included age and sex, CD4 count and CD4%, WHO clinical HIV stage, “weight for age” z score, and haemoglobin and albumin (both predictors of mortality). All analyses were performed in Stata (version 11.0).
Since the programme’s inception, all drugs and health-care have been provided free of charge in the primary health-care clinics and health workers have had access to clear guidelines for managing HIV positive children. A+er the
Table ! | Clinical markers in infants and children starting antiretroviral treatment, by age group and period in which treatment started
Age group and period in which treatment started
CD"% CD" count WHO stage # or "†Median (interquartile range)
No (%) with count missing
Median (interquartile range)
No (%) with count missing No (%)
No (%) with count missing
Infants (<$ year), n=!%&Jun !""# to Sep !""$,* n=% &' (&!-&() & (%%) )%% (#"%-&"$%) & (%%) " ! ($$)Oct !""$ to Sep !""), n=$ &# (&"-!&) & (&)) )"! (#(!-&")") & (&)) ' (*%) "Oct !"") to Sep !""*, n=!" &% (&&-!") * (#") )!& (#*'-&&%&) * (#") &$ (*") "Oct !""* to Sep !""(, n=$& !" (&$-!*) &$ (!$) &#'# (#$#-&#'#) &$ (!$) #( (*") # ())Oct !""( to Sep !"&", n='( !% (&#-%%) &' (!') *%$ (!'$-&'(') &' (!') !# (#&) &% (!!)Oct !"&" to Sep !"&&, n='( !" (&&-%&) !$ (##) &"$% (%)*-&'*$) !$ (##) !' (#!) &# (!#)Children $ to ' years, n=($#Jun !""# to Sep !""$, n=%( &# ((-&$) &" (!$) '"* (&*)-&)($) ) (&*) — —Oct !""$ to Sep !""), n=$& &!.' ().'-&$) ' (*) #'# (!*%-*%!) # ()) — —Oct !"") to Sep !""*, n=&"' &' (&&-!") &$ (&') '!# (%!!-)%)) &$ (&') — —Oct !""* to Sep !""(, n=&(% &$ (&!-!!) !" (&") $%' (#"$-&""%) !" (&") — —Oct !""( to Sep !"&", n=&&* &( (&#-!#) &# (&!) $(" (#"(-&&"#) &# (&!) — —Oct !"&" to Sep !"&&, n=() &* (&&-!#) !" (!&) $&* (!$%-&""#) &( (!") — —Children >' to )$' years, n=&*(Jun !""# to Sep !""$, n=&"% ( ('-&') &$ (&$) &*# ((!-%$") &% (&%) — —Oct !""$ to Sep !""), n=&"" &" ('-&#) &! (&!) &** (&"&-!((.') * (*) — —Oct !"") to Sep !""*, n=&#$ && ($-&$) && (*) &)' (*!-%*#) ( ($) — —Oct !""* to Sep !""(, n=!!& &% ()-!") &' ()) !(%.' (&'#.'-#*)) &% ($) — —Oct !""( to Sep !"&", n=&$( &# ((-!%) &! ()) !)$ (&%)-#$#) ( (') — —Oct !"&" to Sep !"&&, n=&') &#.' ($-!") %' (!!) !&( (&&!-#%') %# (!!) — —Children $ to )$' years, n=$'%*Jun !""# to Sep !""$, n=&#! — — — — *( ($%) &' (&&)Oct !""$ to Sep !""), n=&$& — — — — &&# ()&) &) (&&)Oct !"") to Sep !""*, n=!'& — — — — &(* ()() !" (*)Oct !""* to Sep !""(, n=#&# — — — — %%) (*&) !# ($)Oct !""( to Sep !"&", n=!*) — — — — &*( ($$) %* (&%)Oct !"&" to Sep !"&&, n=!'# — — — — &!) ('") $% (!') *The period Jun !""# to Sep !""$ is longer than the others because of small numbers of infants.†Data not currently available separately for age groups & to ' and >' to +&'.

BMJ | 16 MARCH 2013 | VOLUME 346 37
PRACTICE
One day training for lay HIV counsellors• This included the following topics:
– Immunological eligibility criteria for starting ART in children. Counsellors received charts of the CD4 counts and CD4% cut-offs for starting ART and practised reading laboratory reports to work out if children of different ages were eligible – Clinical eligibility criteria for starting ART in children. Counsellors received charts of the WHO HIV clinical stages for children; clinical scenarios were presented, and counsellors practised “staging” the children. Although staging is done by nurses and doctors, this exercise emphasised to counsellors the importance of staging children clinically and not relying only on immunological eligibility criteria. This is particularly important for children with tuberculosis, who are WHO clinical stage 3 but often have CD4 counts above the immunological threshold for treatment.
• The one day training was repeated annually, with special emphasis in 2010, when the guidelines changed to include giving ART to all infants, irrespective of immunological or clinical criteria. The counsellors received printed leaflets containing the new guidelines, and all the clinics received leaflets for their notice boards and consulting rooms.
Documentation of HIV status for all children• At all training sessions staff were trained on the
importance of ensuring that an HIV status was recorded on the clinic card of all young children (which was held by the mother). If the status was missing on the card of any HIV exposed child being seen in primary healthcare, the nurses referred the child immediately to a counsellor for testing (polymerase chain reaction if aged <18 months; rapid test if aged ≥18 months).
HIV testing during immunisation campaigns• Annual primary healthcare campaigns in KwaZulu-
Natal are organised by the Department of Health and provide opportunities for children who have missed immunisations or scheduled vitamin A supplements to receive these. The campaigns focus on the targeted task and do not consider other child health matters. Nurses and counsellors were trained to use this opportunity to check the HIV status of HIV exposed children and to ensure that HIV positive children had been referred to the HIV treatment programme. We chose immunisations and vitamin A supplements for the campaigns as these health interventions are usually targeted at children under age 5 years, are conducted at least annually, and thus provide an excellent opportunity to “catch” children whose HIV diagnosis had been missed previously.
Clinical staging for all HIV positive children• After the training mentioned above, the counsellors
were instructed to refer all HIV positive children to the clinic nurse or doctor for clinical staging without waiting (potentially for two weeks) for the results of CD4 counts. All counsellors received this instruction at every annual training meeting; the counsellor supervisor who visited the clinics to conduct inhouse training reinforced this.
Referral of all sick HIV exposed children for medical assessment• HIV exposed children were considered a vulnerable group.
Nurses and counsellors were instructed to refer all children with clinical features suggestive of HIV whose mothers were HIV positive, for immediate medical assessment (for example, for failure to thrive, oral thrush beyond the neonatal period, persistent diarrhoea, chronically discharging ears). The WHO’s Integrated Management of Childhood Illness (IMCI) strategy is a method of assessing and managing sick children in resource limited settings with a shortage of medical staff. The South African adaptation of the IMCI guidelines includes a section on identifying HIV in children and includes a list of signs and symptoms. The adapted IMCI guidelines were included in the one day training for counsellors and a similar one day training for nurses. Many of the nurses had been trained in IMCI, and this section of the course was re-emphasised.24 25
Link with tuberculosis and malnutrition programmes• Tuberculosis and malnutrition are associated with HIV,
so linking with these services and the HIV treatment programme is important. The link with the tuberculosis service was part of an initiative that encompassed both adult and paediatric tuberculosis services.26 Anyone in Hlabisa with tuberculosis had an HIV test (or confirmation of a previous HIV test) as part of their management. This was documented on the paediatric tuberculosis “initiation” card that is given to all children starting tuberculosis treatment in the province. Any child with an unknown HIV status was referred immediately for HIV testing and the subsequent result written on the child’s card.
• Nurses from all the clinics and the dietitian from the sub-district received specific training on malnutrition. Nurses were instructed to refer any children with malnutrition and an unknown HIV status to the counsellors for testing.
HIV testing for children in hospital• Hospital admissions for malnutrition, tuberculosis,
pneumonia, or chronic diarrhoea provide a good opportunity to identify children with undiagnosed HIV. Hospital staff conducted HIV testing in the children’s ward of Hlabisa Hospital, and documented HIV status for each child on admission in the case file. Results were retrieved from the laboratory for children who had been tested (with, for example, polymerase chain reaction) but whose result was not documented on their clinic card and whose mothers were unaware of the result. Children who had not been tested for HIV were tested in the ward, with appropriate consent.
Feedback of progress to clinic staff• Feedback to the clinic staff took various forms:
– Annual programme meetings: feedback on numbers of children who began ART (data similar to those in table 2) was presented to counsellors and nurses – Monthly monitoring and evaluation meetings: feedback to clinic staff on monthly and cumulative data on numbers of children and infants starting ART – Regular programme meetings: presentation of statistics stratified by clinic (meetings were attended by all programme staff).
Measures taken in late !""# to improve early identification of young children with HIV and ensure treatment of all eligible children

38 BMJ | 16 MARCH 2013 | VOLUME 346
PRACTICE
year increased from 2 to 59 over the same period (table 1). Of all 1134 children and infants starting ART from Septem-ber 2008 onwards, 70 (6%) started ART at the hospital, the rest at the primary healthcare clinics. Obtaining an accu-rate denominator for the number of children eligible for treatment is problematic and relies on the number of HIV exposed infants who are estimated to be infected, rather than the number of infants actually testing HIV positive. This is because HIV infected but untreated infants are at risk of dying in the +rst month of life before there has been an opportunity to test them. Table 1 gives the estimated number of new cases of HIV infection annually in infants and the number of children who started ART.
The +gure (top panel) shows the cumulative number of children and infants starting ART, with sharp increases observed from early 2008 onwards. Similar annual increases were observed in children and infants, especially in the one year period immediately a,er the interventions were introduced (fig 1(bottom panel)). Thereafter the number of infants starting ART has stabilised at around 50 a year. With the changes in the prevention of mother to child transmission regimen for pregnant women, the mother to child transmission rate in infants at age 6 weeks has fallen from 14% in the early years of the prevention programme (2001-06)23 to 3% in 2011. With an estimated 2000 deliveries to HIV positive women annually in the Hla-bisa sub-district, fewer than 60 infants annually would be expected to be vertically infected with HIV from 2011 onwards. The number of children aged 1 year to ≤15 years starting ART peaked in 2008-09 and then declined, which we assume is a result of a large number of older children being identi+ed with HIV during the early months of the intervention, and subsequently children being picked up at a younger age. In year 7 (October 2010 to September 2011) 59 infants started ART, with an estimated 60 new paediatric HIV infections over the same period.
Most of the infants and children, both before and a,er the quality improvement interventions, were in WHO clini-cal stage 3 or 4 when they started ART, mainly owing to diagnosis with comorbid pulmonary tuberculosis (stage 3) or severe acute malnutrition (stage 4) (table 2). One of the intervention strategies was to provide HIV testing for all children admitted to the local hospital, and all those presenting to clinics with tuberculosis or malnutrition; this “mopping up” of older sick children will have accounted for many of those in WHO stage 3 or 4, and from 2009 to 2011 a trend emerged towards starting treatment in less advanced disease in children aged 1 year to ≤15 years (table 2). We cannot comment on any such trends in infants as the changing guidelines in 20108 meant that all infants were eligible for HIV treatment irrespective of their clinical or immunological stage. This is corroborated by the trend of higher CD4 counts and CD4% seen in the later years of the programme, particularly in those aged 1-5 years, suggesting that children were being identi+ed when they were in better health (table 2).
Next stepsOur results show that in a rural health district it is pos-sible to improve identi+cation of children needing ART and improve early diagnosis of HIV positive infants with
presented no barrier, we thought the problem probably resulted from missed opportunities to test and diagnose young children with HIV, rather than HIV positive children not receiving treatment; this thinking was in line with +nd-ings from other sites in sub-Saharan Africa.16 17
Strategy for changeWe implemented a series of measures from late 2008 to improve early identi+cation of HIV positive infants and fast track them for treatment, and to ensure that older children had a de+nitive HIV test result recorded on their health card and were receiving treatment if eligible (box). We employed no additional sta/, conducted all training in-house, and used no external laboratory services.
Additionally, in late 2007 one of the authors (RMB) established a weekly multidisciplinary family clinic at the busiest government clinic in the Hlabisa sub-district. It was established primarily as an HIV clinic, but other paediatric problems are also managed at the clinic, and children pre-senting with diseases such as tuberculosis and malnutri-tion can also be tested for HIV. Referrals from other clinics in the area are accepted, ART can be started immediately if necessary, discharges from hospital are followed up, and the child acts as an index case to ensure that other mem-bers of the family, particularly siblings, are tested for HIV and receive appropriate care.
Effects of changeWe compared data from the period before the interven-tion strategies with those from September 2008 onwards. The number of children (aged 1 to ≤15 years) starting ART each year increased from 43 in 2004 to 254 in 2011, with the largest increases from September 2008 onwards. The number of infants (aged <1 year) starting treatment each
No o
f chi
ldre
n an
d in
fant
s
Before Oct !"
Oct !"-M
ar !#
Apr !#-Sep !#
Oct !#-M
ar !$
Apr !$-Sep !$
Oct !$-M
ar !%
Apr !%-Sep !%
Oct !%-M
ar !&
Apr !&-Sep !&
Oct !&-M
ar !'
Apr !'-Sep !'
Oct !'-M
ar (!
Apr (!-Sep (!
Oct (!-M
ar ((
Apr ((-Sep ((
!
"!!
&!!
()!!
($!!
)!!!
No o
f chi
ldre
n an
d in
fant
s
Before Oct !"
Oct !"-Sep !#
Oct !#-Sep !$
Oct !$-Sep !%
Oct !%-Sep !&
Oct !&-Sep !'
Oct !'-Sep (!
Oct (!-Sep ((
!
(!!
)!!
*!!
"!!
#!!Age <( yearAge ( to +(# years
Top panel: Cumulative number of children and infants starting antiretroviral treatment (ART): June !""# to September !"$$. Bottom panel: Annual numbers of children and infants receiving ART June !""# to September !"$$

BMJ | 16 MARCH 2013 | VOLUME 346 39
PRACTICE
Provenance and peer review: Not commissioned; externally peer reviewed.! Houlihan CF, Mutevedzi PC, Lessells RJ, Cooke GS, Tanser FC, Newell ML.
The tuberculosis challenge in a rural South African HIV programme. BMC Infect Dis "#!#;!#:"$.
" Welz T, Hosegood V, Jaffar S, Batzing-Feigenbaum J, Herbst K, Newell ML. Continued very high prevalence of HIV infection in rural KwaZulu-Natal, South Africa: a population-based longitudinal study. AIDS "##%;"!:!&'%-%".
$ Tanser F, Bärnighausen T, Grapsa E, Newell ML. Effect of ART coverage on rate of new HIV infections in a hyper-endemic, rural population: South Africa. Conference on Retroviruses and Opportunistic Infections. Seattle, US, "#!". www.retroconference.org/"#!"b/Abstracts/&($%).htm.
& Houlihan CF, Bland RM, Mutevedzi PC, Lessells RJ, Ndirangu J, Thulare H, et al. Cohort profile: Hlabisa HIV treatment and care programme. Int J Epidemiol "#!#;&#:$!*-"'.
( Wilkinson D, Cutts F, Ntuli N, Abdool Karim SS. Maternal and child health indicators in a rural South African health district. S Afr Med J !))%;*%:&('-).
' Ndirangu J, Barnighausen T, Tanser F, Tint K, Newell ML. Levels of childhood vaccination coverage and the impact of maternal HIV status on child vaccination status in rural KwaZulu-Natal, South Africa. Trop Med Int Health "##);!&:!$*$-)$.
% World Health Organization. Antiretroviral therapy of HIV infection in infants and children in resource limited settings: towards universal access. "##'. www.who.int/hiv/pub/guidelines/WHOpaediatric.pdf.
* National Department of Health, South Africa. Guidelines for the management of HIV in children. "nd ed. "#!#. www.hivfshealth.org/document/"#!#/#*/!)/guidelines-for-the-management-of-hiv-in-children-"nd-edition-"#!#.
) World Health Organization. Antiretroviral therapy for HIV infection in infants and children: towards universal access. Recommendations for a public health approach: "#!# revision. www.who.int/hiv/pub/paediatric/infants"#!#/en/.
!# Johnson L. Access to antiretroviral treatment in South Africa, "##&-!!. Southern African Journal of HIV Medicine "#!";!$(!).
!! Joint United Nations Programme on HIV/AIDS. AIDS epidemic update "##). http://data.unaids.org/pub/Report/"##)/JC!%##_Epi_Update_"##)_en.pdf.
!" Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet "##&;$'&:!"$'-&$.
!$ Newell ML, Patel D, Goetghebuer T, Thorne C. CD& cell response to antiretroviral therapy in children with vertically acquired HIV infection: is it associated with age at initiation? J Infect Dis "##';!)$:)(&-'".
!& Prendergast A, Mphatswe W, Tudor-Williams G, Rakgotho M, Pillay V, Thobakgale C, et al. Early virological suppression with three-class antiretroviral therapy in HIV-infected African infants. AIDS "##*;"":!$$$-&$.
!( Violari A, Cotton MF, Gibb DM, Babiker AG, Steyn J, Madhi SA, et al. Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med "##*;$():""$$-&&.
!' Ginsburg AS, Hoblitzelle CW, Sripipatana TL, Wilfert CM. Provision of care following prevention of mother-to-child HIV transmission services in resource-limited settings. AIDS "##%;"!:"(")-$".
!% Rollins N, Little K, Mzolo S, Horwood C, Newell ML. Surveillance of mother-to-child transmission prevention programmes at immunization clinics: the case for universal screening. AIDS "##%;"!:!$&!-%.
!* KIDS-ART-LINC Collaboration. Low risk of death, but substantial program attrition, in pediatric HIV treatment cohorts in Sub-Saharan Africa. J Acquir Immune Defic Syndr "##*;&):("$-$!.
!) Bolton-Moore C, Mubiana-Mbewe M, Cantrell RA, Chintu N, Stringer EM, Chi BH, et al. Clinical outcomes and CD& cell response in children receiving antiretroviral therapy at primary health care facilities in Zambia. JAMA "##%;")*:!***-)).
"# Kiboneka A, Wangisi J, Nabiryo C, Tembe J, Kusemererwa S, Olupot-Olupot P, et al. Clinical and immunological outcomes of a national paediatric cohort receiving combination antiretroviral therapy in Uganda. AIDS "##*;"":"&)$-).
"! Janssen N, Ndirangu J, Newell ML, Bland RM. Successful paediatric HIV treatment in rural primary care in Africa. Arch Dis Child "#!#;)(:&!&-"!.
"" Cooke GS, Little K, Bland RM, Thulare H, Newell ML. Need for paediatric HIV treatment within primary health care in rural South Africa. PLoS ONE "##);&:e%!#!.
"$ Rollins NC, Coovadia HM, Bland RM, Coutsoudis A, Bennish ML, Patel D, et al. Pregnancy outcomes in HIV-infected and uninfected women in rural and urban South Africa. J Acquir Immune Defic Syndr "##%;&&:$"!-*.
"& Horwood C, Liebeschuetz S, Blaauw D, Cassol S, Qazi S. Diagnosis of paediatric HIV infection in a primary health care setting with a clinical algorithm. Bull World Health Organ "##$;*!:*(*-''.
"( Horwood C, Voce A, Vermaak K, Rollins N, Qazi S. Experiences of training and implementation of integrated management of childhood illness (IMCI) in South Africa: a qualitative evaluation of the IMCI case management training course. BMC Pediatr "##);):'".
"' Coovadia H, Bland R. From Alma-Ata to Agincourt: primary health care in AIDS. Lancet "##*;$%":*''-*.
Accepted: "& December "#!"
relatively simple measures and limited implications for sta!ng and budgets. Guidelines are in place, but vertical health programmes present barriers to ensuring holistic assessment of children, including early HIV diagnosis. This applies particularly to children attending tuberculosis services and presenting with malnutrition and to infants attending immunisation and growth clinics. All these points of care represent opportunities to determine the HIV status of a child and refer them for treatment and care. One of the key elements of our initiatives has been regular feedback of results to clinic and programme sta", o#en ignored in set-tings where monitoring and evaluation are under-resourced or poorly conducted.
Our $ndings show that most children still presented in WHO clinical stage % or &, which probably re'ects the high prevalence of tuberculosis in the area. However, we found suggestions of a trend towards treatment starting at lower WHO clinical stages and higher CD& counts; this trend may be linked to earlier diagnosis of HIV.
With the introduction of new regimens for prevention of mother to child transmission (including expanded eligibility criteria for ART for pregnant women) and immediate ART for all infants aged under ( year with con$rmed HIV sta-tus, there is now the real possibility to eradicate mother to child transmission of HIV and to identify and treat the few children who are HIV positive within the $rst three months of life.
In February )*(% the management of the Hlabisa HIV programme changed. The funding to South Africa by the US emergency AIDS plan PEPFAR, always intended for a limited time period, was substantially reduced, and the programme is now managed wholly by the local Department of Health. Systems are now well established to continue this optimal treatment and care of HIV infected children in Hlabisa: the Department of Health sta" are trained, integration with the paediatric tuberculosis services is in place, and the pro-gramme has followed a decentralised model from inception.
We will continue to monitor the prevention of mother to child transmission programme and the follow-up of HIV exposed infants in Hlabisa, and we are aiming to achieve virtual eradication of mother to child HIV transmission over the next $ve years and to start ART in all HIV positive infants in the $rst four months of life. Our $ndings should be encouraging to other rural areas of sub-Saharan Africa with equally high HIV prevalence and limited resources.Contributors: RMB dra+ed the manuscript; JN analysed the data; all authors contributed to interpretation of results and reviewed the manuscript.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: The Africa Centre for Health and Population Studies is supported by a core grant from the Wellcome Trust (#(#("&). The Hlabisa HIV Treatment and Care Programme is made possible through the US Agency for International Development (USAID) and the President’s Emergency Plan (PEPFAR) under the terms of Award No '%&-A-##-#*-####!-##. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID or the US government. The funders played no part in the analysis or writing of this manuscript. We declare no ,nancial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.Ethical approval: The authors obtained ethical approval from the Biomedical Ethics Committee of the University of KwaZulu-Natal for the retrospective analysis of anonymised data from the HIV Treatment and Care Programme (BE#''/#%); the Research O-ce of the KwaZulu-Natal Department of Health also granted approval.
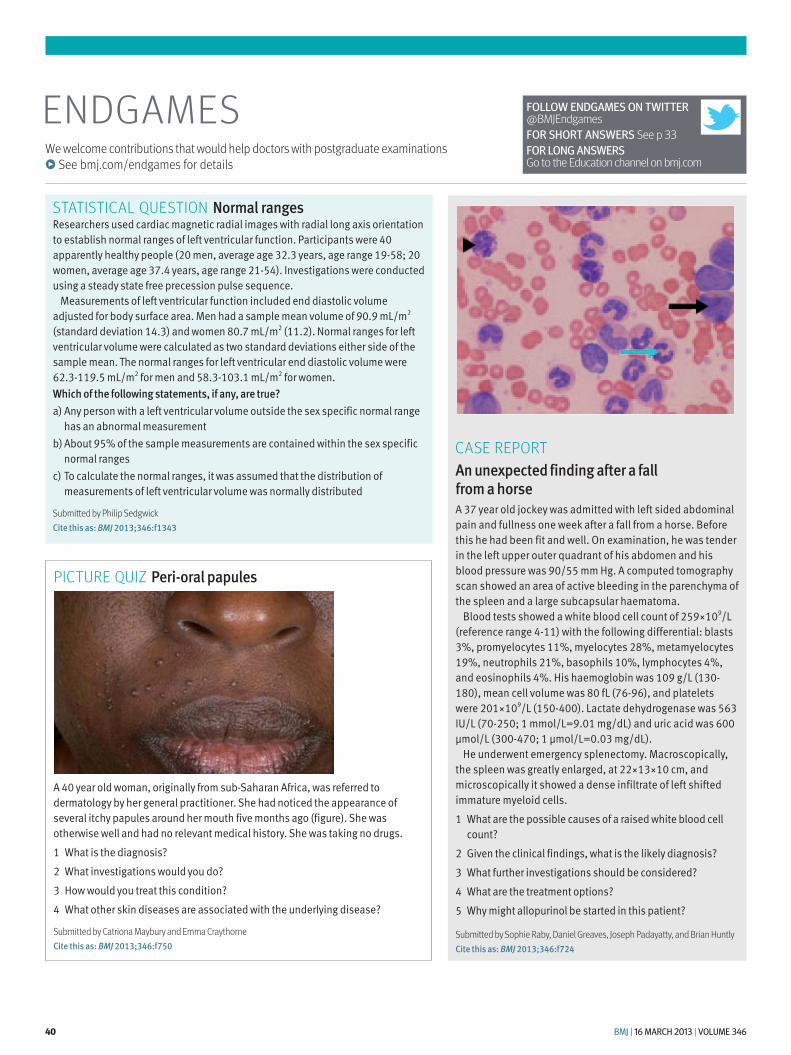
40 BMJ | 16 MARCH 2013 | VOLUME 346
ENDGAMESWe welcome contributions that would help doctors with postgraduate examinations
! See bmj.com/endgames for details
CASE REPORTAn unexpected finding after a fall from a horseA !" year old jockey was admitted with left sided abdominal pain and fullness one week after a fall from a horse. Before this he had been fit and well. On examination, he was tender in the left upper outer quadrant of his abdomen and his blood pressure was #$/%% mm Hg. A computed tomography scan showed an area of active bleeding in the parenchyma of the spleen and a large subcapsular haematoma.
Blood tests showed a white blood cell count of &%#'($#/L (reference range )-(() with the following differential: blasts !%, promyelocytes ((%, myelocytes &*%, metamyelocytes (#%, neutrophils &(%, basophils ($%, lymphocytes )%, and eosinophils )%. His haemoglobin was ($# g/L ((!$-(*$), mean cell volume was *$ fL ("+-#+), and platelets were &$('($#/L ((%$-)$$). Lactate dehydrogenase was %+! IU/L ("$-&%$; ( mmol/L=#.$( mg/dL) and uric acid was +$$ µmol/L (!$$-)"$; ( µmol/L=$.$! mg/dL).
He underwent emergency splenectomy. Macroscopically, the spleen was greatly enlarged, at &&'(!'($ cm, and microscopically it showed a dense infiltrate of left shifted immature myeloid cells.( What are the possible causes of a raised white blood cell
count?& Given the clinical findings, what is the likely diagnosis?! What further investigations should be considered?) What are the treatment options?% Why might allopurinol be started in this patient?
Submitted by Sophie Raby, Daniel Greaves, Joseph Padayatty, and Brian HuntlyCite this as: BMJ "#$%;%&':f("&
STATISTICAL QUESTION Normal rangesResearchers used cardiac magnetic radial images with radial long axis orientation to establish normal ranges of left ventricular function. Participants were )$ apparently healthy people (&$ men, average age !&.! years, age range (#-%*; &$ women, average age !".) years, age range &(-%)). Investigations were conducted using a steady state free precession pulse sequence.
Measurements of left ventricular function included end diastolic volume adjusted for body surface area. Men had a sample mean volume of #$.# mL/m& (standard deviation ().!) and women *$." mL/m& (((.&). Normal ranges for left ventricular volume were calculated as two standard deviations either side of the sample mean. The normal ranges for left ventricular end diastolic volume were +&.!-((#.% mL/m& for men and %*.!-($!.( mL/m& for women.Which of the following statements, if any, are true?a) Any person with a left ventricular volume outside the sex specific normal range
has an abnormal measurementb) About #%% of the sample measurements are contained within the sex specific
normal rangesc) To calculate the normal ranges, it was assumed that the distribution of
measurements of left ventricular volume was normally distributed
Submitted by Philip SedgwickCite this as: BMJ "#$%;%&':f$%&%
FOLLOW ENDGAMES ON TWITTER @BMJEndgamesFOR SHORT ANSWERS See p 33FOR LONG ANSWERS Go to the Education channel on bmj.com
A )$ year old woman, originally from sub-Saharan Africa, was referred to dermatology by her general practitioner. She had noticed the appearance of several itchy papules around her mouth five months ago (figure). She was otherwise well and had no relevant medical history. She was taking no drugs.( What is the diagnosis?& What investigations would you do?! How would you treat this condition?) What other skin diseases are associated with the underlying disease?
Submitted by Catriona Maybury and Emma CraythorneCite this as: BMJ "#$%;%&':f()#
PICTURE QUIZ Peri-oral papules

BMJ | 16 MARCH 2013 | VOLUME 346 41
LAST WORDS
They are a product of yesteryear’s deference, club mentality, and divisiveness, celebrating superiority and elitism, and they reinforce hierarchy
celebrating superiority and elitism, and they reinforce hierarchy.
Some doctors also complain that those who pursue their medical careers o!en do so to the detriment of their col-leagues who are le! holding the on-call pager. Some even suggest that fellow-ships are a cynical conspiracy to make money by preying on middle aged insecurity. A fellowship of the Royal College of General Practitioners, for example, costs "#$% along with some truly dreadful but expensive polyester merchandising tat. The bottom line is that many ordinary, hard working consultants and general practitioners never receive a gong or recognition.
What value do fellowships add to the profession? Aren’t fellowships a potential barrier to challenging author-ity and the establishment? Isn’t it time to review our medical honours system?Des Spence is a general practitioner, Glasgow [email protected] this as: BMJ !"#$;$%&:f#&"'
We are all a product of our time, a morass of contradictions, conflicts, and prejudices. I was raised on a iso-lated Scottish island, attended a com-prehensive school, and worked in many di&erent jobs. I pride myself on my ordinariness and the ordinariness of my medical work. Egalitarianism is branded in my psyche. I am intent on never appearing intimidated—even when I am. I am respectful but not deferential. I dislike titles, includ-ing “ Doctor,” reasoning that these are merely a weapon of intimidation. Success and contentment are not in the gi! of others, or possessions, but a purely personal perspective.
So I have mixed emotions towards honours, knighthoods, and the rest. These are from a class ridden past, mere baubles designed to a'rm sepa-ration and superiority. Today honours strive to be more egalitarian, with the odd postal worker and teacher recog-nised for their daily dedication. But
honours are still part political patron-age, closed but to a select elite few. It is the powerful and privileged, not the hardworking teacher, who have the highest honour of falling asleep in ermine and claiming expenses in the House of Lords.
What of medical gongs, the “fellow-ships” to the medical royal colleges, presented in gowns at ceremonies with curling cucumber sandwiches? Doctors are awarded these through nomination by colleagues and subject to committee review. Fellowships are seen as a tradi-tion—harmless and an important recog-nition of hard work and commitment.
I am not angry that I have never been nominated (or perhaps I am just in denial). But aren’t fellowships out-dated, just like those badly painted portraits of past presidents, all look-ing the same irrespective of sex, hang-ing on the college walls? They are a product of yesteryear’s deference, club mentality, and divisiveness,
My (rst proper job was as a salesman at a big chain of electrical shops. During my induction the manager introduced himself as John Clark. I had just le! school, and my only retail experience was from watching reruns of the )*+%s British sitcoms Are You Being Served and Open All Hours, so I had no idea whether I should call him John or Mr Clark. I spent the next week addressing him as “Excuse me” and desperately listening out for cues from my colleagues.
Seven months into my (rst job as a doctor, and a!er six years of medical school, I still feel a bit uncomfortable about how to address my seniors—especially consultants. To my ear, calling doctors by their surnames has a whi& of Are You Being Served. But calling consultants by their (rst name, without (rst being explicitly invited to, would be unthinkable.
I’ve recently been experimenting with “Boss.” It does make me sound
screw ups could have been averted if juniors had had the courage to challenge what they were being told. Perhaps more commonly, being able to question your senior’s clinical reasoning helps you to learn why they are doing what they are doing. Getting rid of the rigid interpersonal hierarchy can only help this happen.
Of course, the boss still makes the (nal call. But your seniors derive their authority from their experience and knowledge, not from outdated etiquette. The few consultants I have known who preferred to be called by their (rst names still had the full respect of their juniors.
So let’s be on (rst name terms. It’ll make work a nicer place, and it might make medicine better.Oliver Ellis is foundation year ! doctor, Mersey Deanery [email protected] interests: None declared.Cite this as: BMJ !"#$;$%&:f#%("
I’ve recently been experimenting with “Boss.” It does make me sound a bit like a doomed henchman in a 1980s action movie but has the advantage of having just one syllable
a bit like a doomed henchman in a )*,%s action movie but has the advantage of having just one syllable and being a bit less stu&y.
The world has become a less formal place. Politicians don’t wear ties, gardeners don’t do& their caps, and people use (rst names.
What patients and doctors call each other is a di&erent matter. Many patients prefer to use surnames.
But when patients aren’t in the room, why can’t our interactions catch up with the rest of the world?
As a medical student I was once given a comprehensive telling o& for the way I was standing. “When you present a patient, stand up straight, feet a shoulder width apart, hands behind your back.” Stand at ease, in other words, which was odd, because I had no memory of ever joining the army.
Doctors are increasingly recognised not to be gods. So many scandals and
FROM THE FRONTLINE Des Spence
Scrap the royal colleges’ fellowships
LAYING FOUNDATIONS Oliver Ellis
On first name terms
Twitter " Follow Des Spence on
Twitter @des_spence!
bmj.com " Previous articles by
Oliver Ellis are available at http://bit.ly/YVR#qY

42 BMJ | 16 MARCH 2013 | VOLUME 346
MINERVASend comments or suggest ideas to Minerva: [email protected]
A !" year old woman, with several itchy papules around her mouth Try the picture quiz in ENDGAMES, p!"
The installation of !"# solar panels on the roof of a crematorium in Hereford, United Kingdom, is expected to generate over !$ """ units of electricity a year, saving more than !% tonnes of carbon dioxide emissions and saving taxpayers nearly &$""" ('$(""; )*$+") per year. Solar panels are well suited to crematoriums, according to the local energy company, “because they are silent, and won’t disrupt the business of the site” (Pharos International Spring %"!,;*-:,().
Early laparoscopic cholecystectomy is encouraged for most people with acute cholecystitis. But what happens to those who are discharged on first admission without surgery? Using data from over !" """ patients who did not undergo cholecystectomy on first admission, Canadian researchers found a !-% probability of a subsequent gallstone related event or hospital visit within !% weeks of discharge. This risk increased in younger patients aged !(-,+ years (Journal of Trauma and Acute Care Surgery %"!,;*+:%#-,!, doi:!".!"-*/TA."b"!,e,!(%*((e+d).
In a comparison study of -* children with epilepsy and #- healthy children, IQ was significantly lower in children with epilepsy than in controls. However, IQ did not differ significantly between the parents of both groups. Children with epilepsy had significantly lower IQ scores than their biological parents, which was not observed in the control group. The researchers suggest that the parent-child IQ difference is a marker of the effect of epilepsy, independent of familial IQ and of the type of epilepsy (Developmental Medicine and Child Neurology %"!,;$$:%*(-(%, doi:!".!!!!/dmcn.!%"+").
The proportion of medical graduates in the United Kingdom who choose to specialise in psychiatry has remained at about $% over the past ,$ years. In a questionnaire study of nearly ,+ """ respondents, the main reasons for choosing psychiatry included experience of the subject at medical school, self appraisal of skills, and inclinations even before applying to medical school. Of graduates who did not choose psychiatry, *%% gave “job content” as their reason for rejection, compared with ,,% of those who considered but rejected
other specialties (British Journal of Psychiatry %"!,;%"%:%%(-,+, doi:!".!!-%/bjp.bp.!!%.!!!!$,).
Minerva fondly remembers the adventures of Laura Ingalls in the Little House on the Prairie, and the tears she wept when Laura’s sister Mary went blind at the age of !+. Mary’s sight loss was blamed on scarlet fever in the novels, but in Laura Ingalls Wilder’s memoirs, she recalls Mary being “taken suddenly sick with a pain in her head” and then being “delirious with an awful fever,” with her face “drawn out of shape.” It was recorded as “spinal sickness” and “brain fever,” period terms for meningoencephalitis (Pediatrics %"!,;!,!:+"+-#, doi:!".!$+%/peds.%"!%-!+,().
Postdural puncture headaches (PDPH) occur in up to +"% of people who undergo lumbar puncture, typically starting within !$ min of sitting up, and resolving within !$ min of lying down again. In a prospective study of !#" people with migraine headaches and $, matched healthy controls, risk factors for
PDPH were identified as young age and low body mass index, but not having migraines (Neurology %"!,;(":-+!-(, doi:!".!%!%/WNL."b"!,e,!(%(+"bf#). Duration of PDPH was prolonged if multiple attempts at lumbar puncture were made, and if patients perceived their lumbar puncture experience as stressful.
Men with high risk prostate cancer who undergo robot assisted radical prostatectomy could have just as good oncological outcomes as those who undergo open surgery, according to a retrospective analysis of over +"" patients at one United States institution (British Journal of Urology International %"!,, doi:!".!!!!/j.!+#+-+!"X.%"!%.!!+-,.x). Recurrence free survival was similar in both groups at two years (open procedure (+% v robot assisted procedure *-%) and four years (#(% v ##%). But robot assisted patients had less blood loss and underwent complete bilateral nerve sparing more often than patients with open surgery.
Preoperative magnetic resonance imaging (MRI) could underestimate the size of articular cartilage defects compared with what is actually found at arthroscopy. In one cohort study of ** patients undergoing knee arthroscopy, MRI scans underestimated the defect area by an average of *"%; therefore, many patients were not well informed preoperatively about the best repair strategies on offer. The authors suggest that such discrepancies are predictable, and should be reflected in the treatment strategies discussed before surgery (American Journal of Sports Medicine %"!,;+!:$-"-$, doi:!".!!**/",#,$+#$!%+*%"++).
PCV*—a seven valent, pneumococcal conjugate vaccine—was introduced in Australia in two phases, in %""! and %""$. In the five years after its introduction, admission rates for all childhood pneumonias fell significantly; however, admissions for empyema rose more than expected, although this increase was significant only among children aged !-+ years. There is a concern that empyema may have emerged as a “replacement disease,” produced by non-vaccine related serotypes of Streptococcus pneumoniae (Bulletin of the World Health Organization %"!,;-!:!#*-*,, doi:!".%+*!/blt.!%.!"-%,!). Cite this as: BMJ !"#$;$%&:f#'!&
This plain radiograph shows the right foot of a #- year old man with type % diabetes, who presented with an infected heel ulcer that did not respond to oral antibiotics. The radiograph clearly shows extensive subcutaneous emphysema of the foot. There is also a curvilinear lucency in the calcaneum extending to the cortex, with thinning of the cortex adjacent to the ulcer site. The bony changes were deemed to be secondary to osteomyelitis affecting the calcaneum.Jonathan D Evans, foundation year # trainee, Adrian M Jennings ([email protected]), consultant physician , Department of Diabetes and Endocrinology, Queen Elizabeth Hospital, King’s Lynn PE$" !ET, UKPatient consent obtained.Cite this as: BMJ !"#$;$%&:f#'!(

















