32
Board Review: Genetics January 2008
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | kylie-cartlidge |
| View: | 219 times |
| Download: | 0 times |
Board Review:Genetics
January 2008

TRUST US….
We’re BOARD CERTIFIED!
Karyotypes
• Diagnosis?
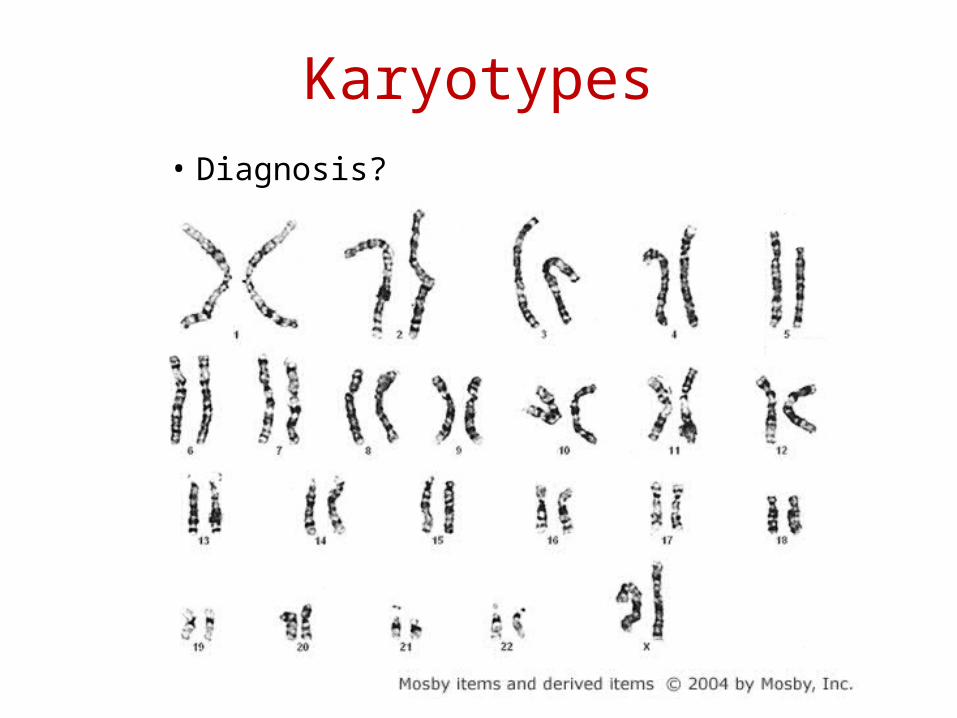
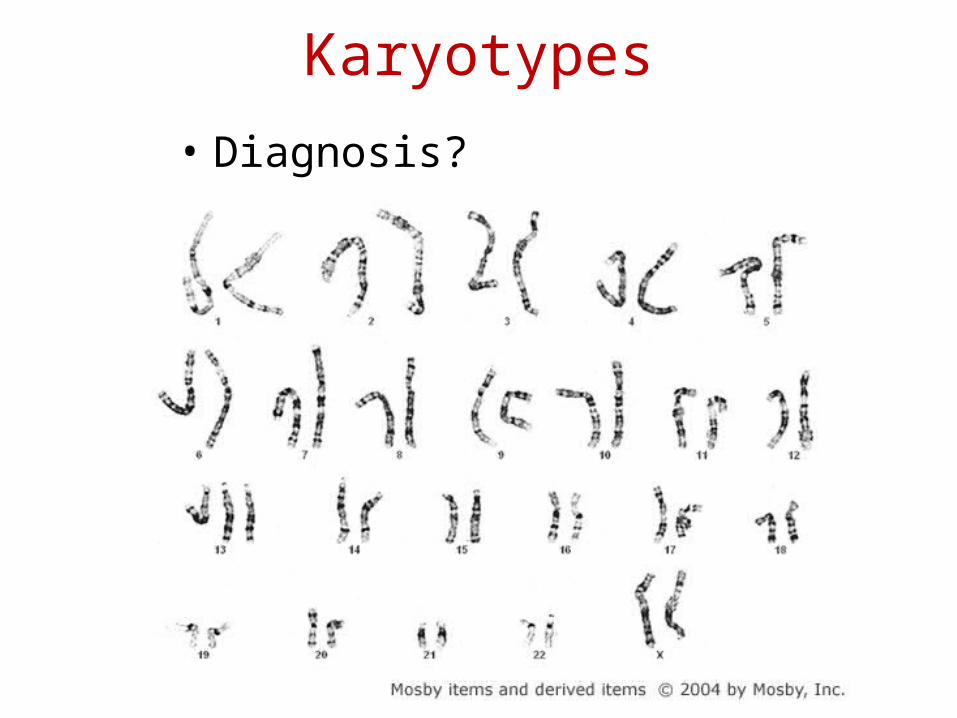
Karyotypes• Diagnosis?

Down Syndrome/Trisomy 21
Full trisomy 21 94%
Mosaic trisomy 21 2.4%
Translocation 3.3%
Translocations
Parent carrier t(21q;21q) 100% recurrence
Parent carrier t(14q;21q) 1/3 chance of having affectedchild
Heart defect: Endocardial cushion defect
Special Olympics: Atlantoaxial instability
IF THE PATIENT HAS A TRANSLOCATION THE PARENTS KARYOTYPE SHOULD BE CHECKED
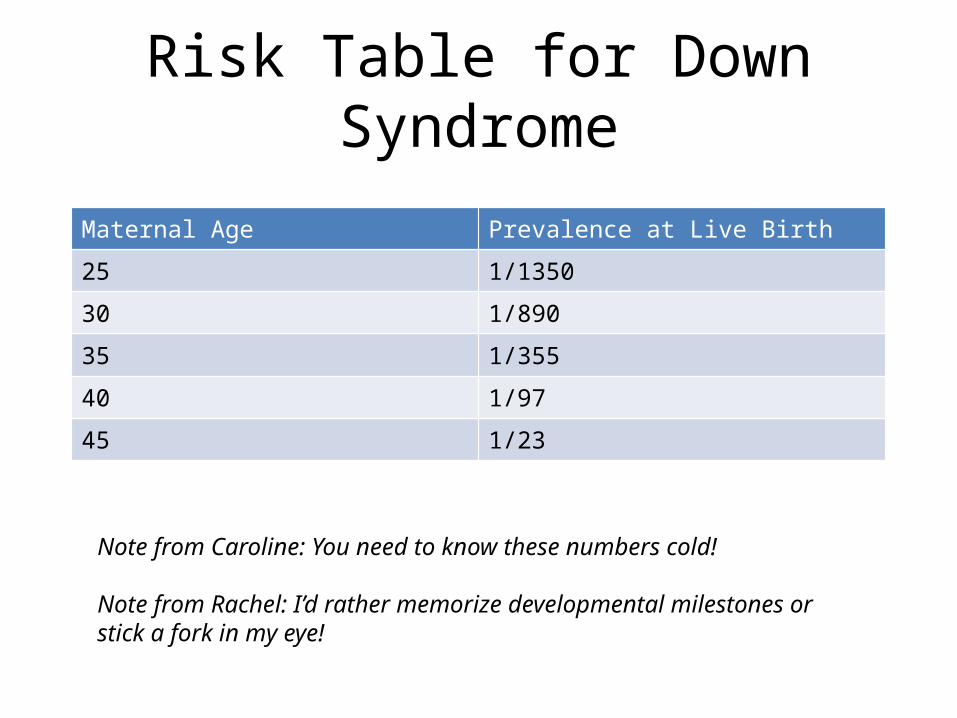
Risk Table for Down Syndrome
Maternal Age Prevalence at Live Birth
25 1/1350
30 1/89035 1/355
40 1/97
45 1/23
Note from Caroline: You need to know these numbers cold!
Note from Rachel: I’d rather memorize developmental milestones or stick a fork in my eye!
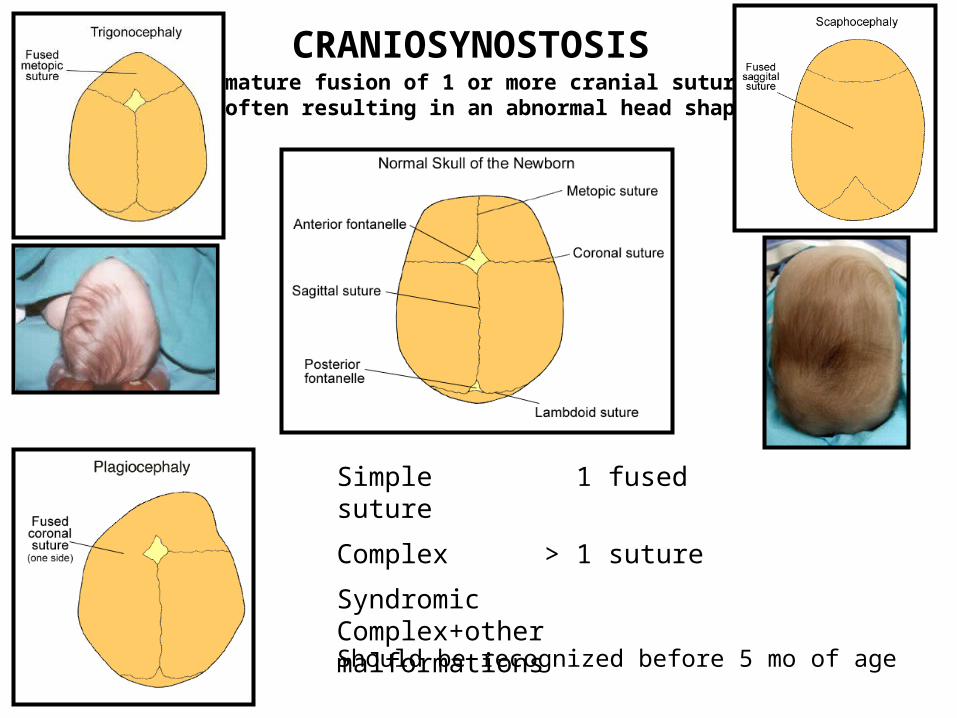
CRANIOSYNOSTOSISpremature fusion of 1 or more cranial sutures,
often resulting in an abnormal head shape
Simple 1 fused suture
Complex > 1 suture
Syndromic Complex+other malformations
Should be recognized before 5 mo of age

• The craniofacial syndrome associated with cervical spine fusion, OM, and syndactyly.– Aperts
• 71% of patients with this CFS have Chiari I type malformations and hydrocephalus– Crouzon
• What cutaneous finding is associated with Crouzon syndrome?– Acanthosis nigricans
• Which CFS is associated with medially deviated great toes & broad radial thumbs?– Pfeiffer Syndrome

SYNDROMIC
CRANIOSYNOSTOSIS
Pfeiffer syndrome
Apert Syndrome
Crouzon Syndrome

What genetic syndrome would this make you think of?•Trisomy 13What is the most common congenital heart defect?•VSD
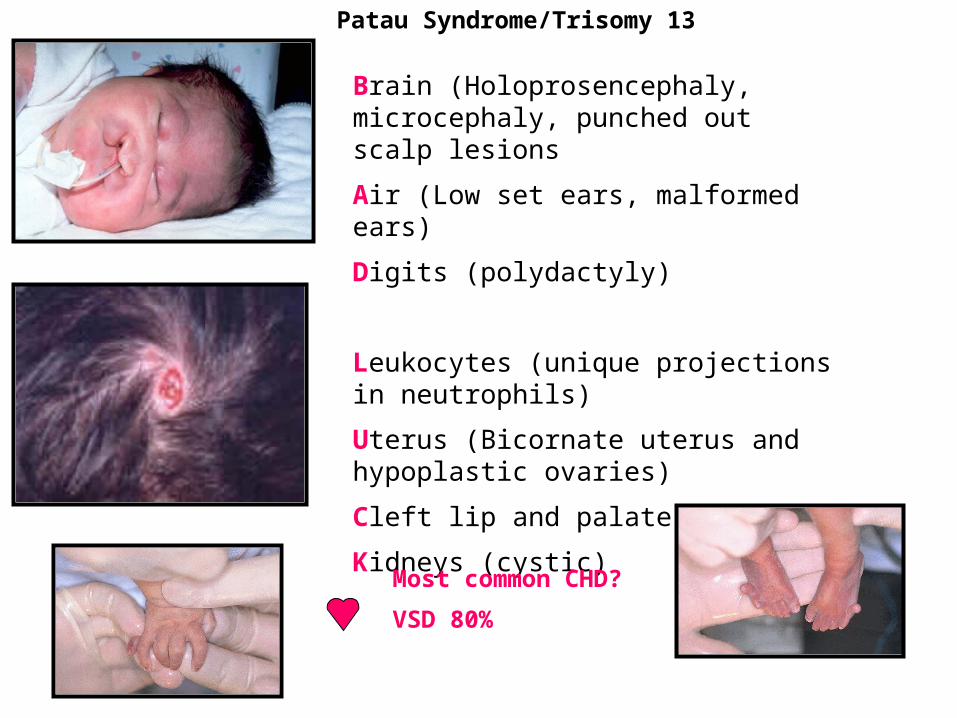
Patau Syndrome/Trisomy 13
Brain (Holoprosencephaly, microcephaly, punched out scalp lesions
Air (Low set ears, malformed ears)
Digits (polydactyly)
Leukocytes (unique projections in neutrophils)
Uterus (Bicornate uterus and hypoplastic ovaries)
Cleft lip and palate
Kidneys (cystic)
Most common CHD?
VSD 80%
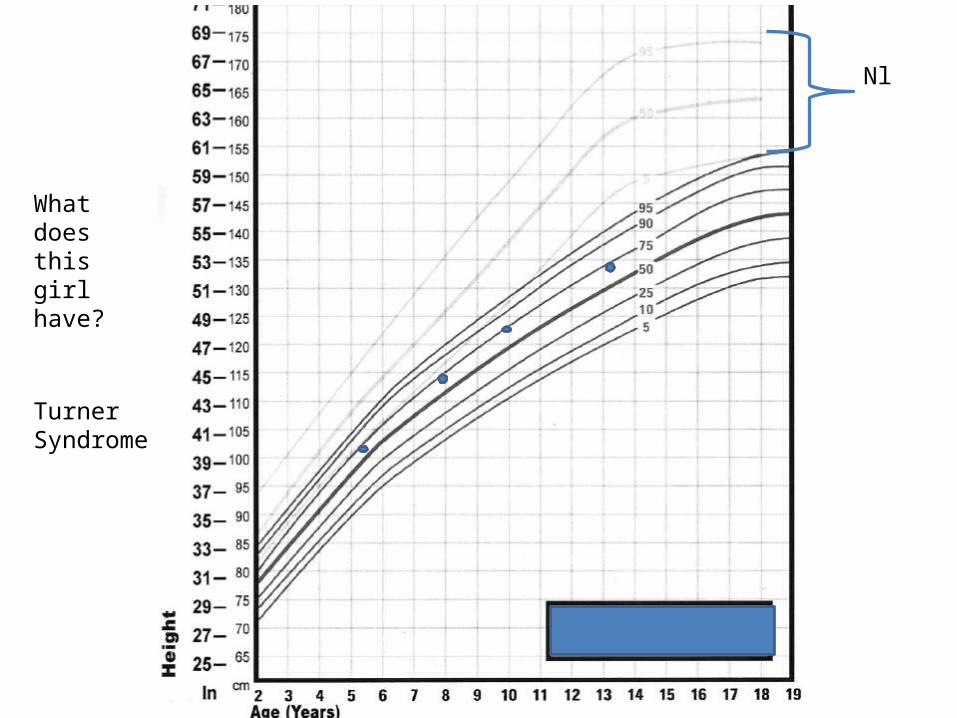
Nl
What does this girl have?
Turner Syndrome
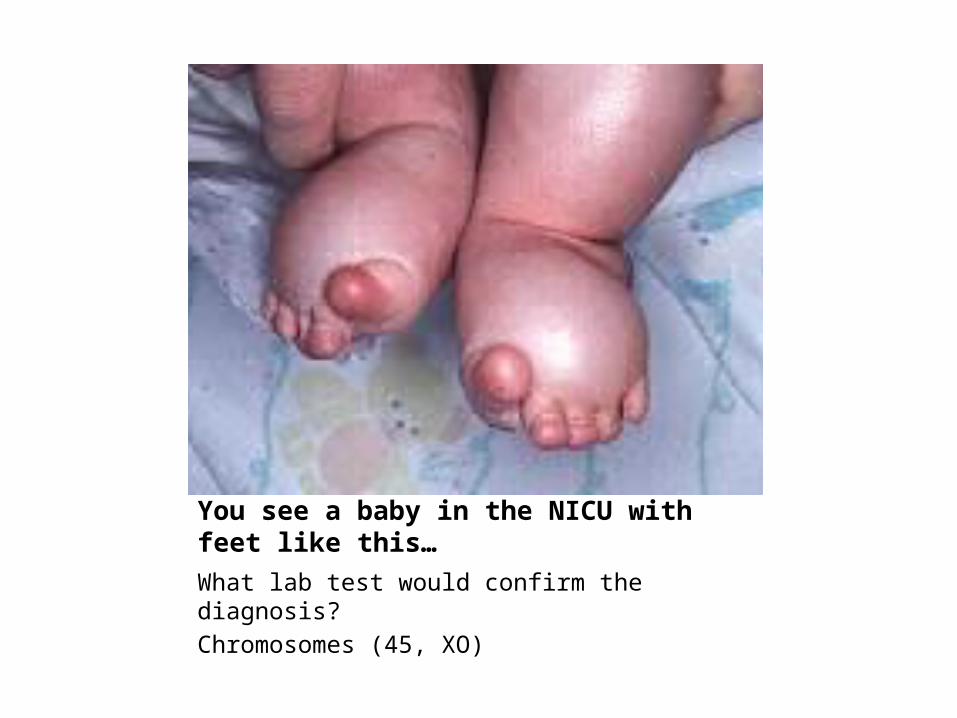
You see a baby in the NICU with feet like this…What lab test would confirm the diagnosis?Chromosomes (45, XO)

Turner Syndrome / 45,X0
It is the most common chromosomal defect in spontaneous abortions
Short stature, webbed neck, delayed secondary sexual characteristics, short 4th-5th metacarpals, widely space nipples, pedal edema, cubitus valgus
Most common cardiac defect in TS Coarctation of the aorta.

Edwards Syndrome/Trisomy 18
Rocker bottom
feet
Clenched fists, hypoplastic nails
Short sternum, prominent occiput, microcephaly.
Horseshoe Kidney
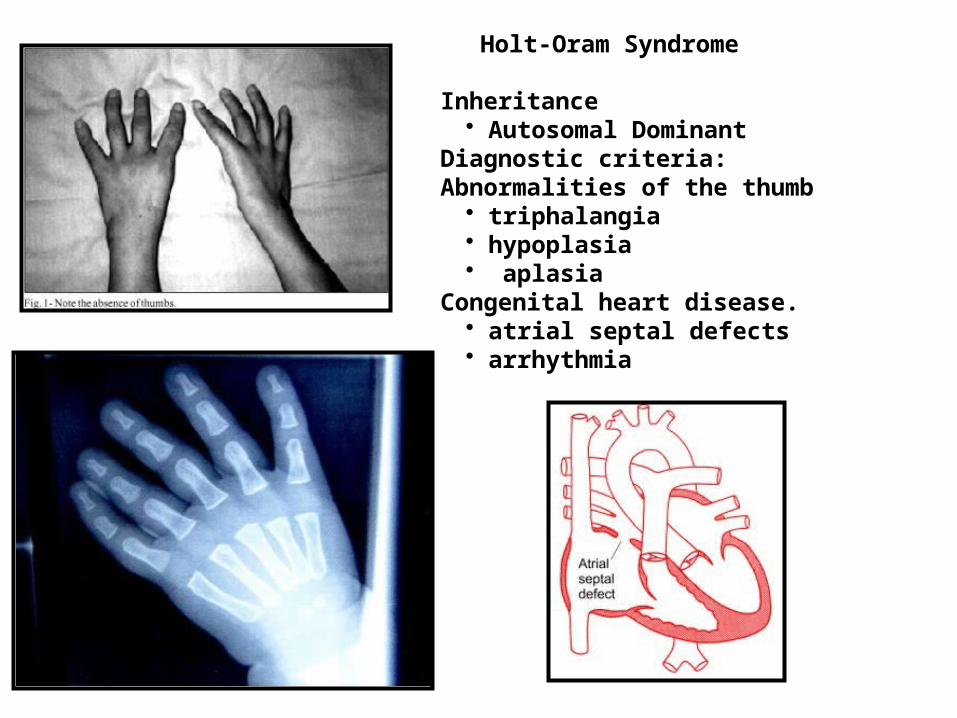
Inheritance • Autosomal Dominant
Diagnostic criteria:Abnormalities of the thumb
• triphalangia • hypoplasia• aplasia
Congenital heart disease. • atrial septal defects • arrhythmia
Holt-Oram Syndrome
• A 4 year old boy presents because he’s been falling a lot per his parents. His dad is mad because the child “walks like a girl on his tippy toes.”
• What diagnosis should you suspect?– Duchenne’s Muscular Dystrophy
• Can someone demonstrate a physical exam finding seen in this disease?– Gower sign
• What would be the diagnostic finding on muscle biopsy?– Absence of dystrophin
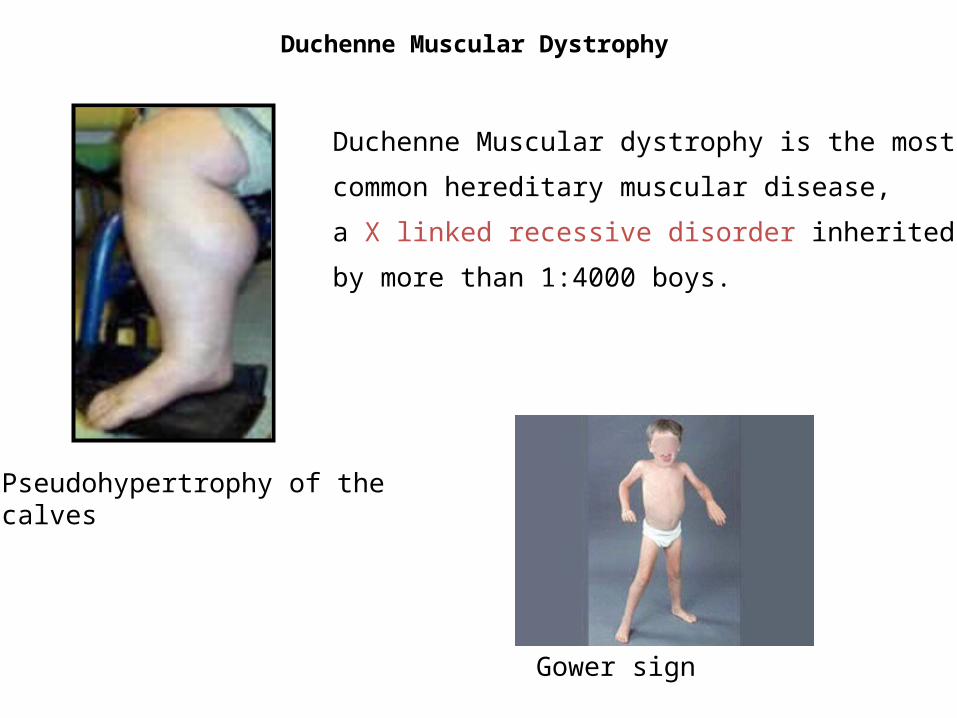
Duchenne Muscular Dystrophy
Gower sign
Pseudohypertrophy of the calves
Duchenne Muscular dystrophy is the most
common hereditary muscular disease,
a X linked recessive disorder inherited
by more than 1:4000 boys.

Patient started having difficulties in school when he was eight years old. His teacher noted that he seemed to be irritable and impulsive; she raised the possibility of attention deficit disorder. In addition, Ronnie was noted to have mild difficulties with spelling and composition. Although he was requiring some additional help with these tasks, his IQ was normal (104) and he had been progressing academically with his peer group. He was tall for his age (95th percentile in height). He had no physical or medical problems. A detailed evaluation by a psychologist revealed some impulsivity, but insufficient findings to support a diagnosis of attention deficit disorder. Tutoring was arranged, and he continued to progress adequately in school. At age 14 years, he develops gynecomastia. At this point, he is seen by an endocrinologist.What is the diagnosis ?
Klinefelter Syndrome
Treatment: TESTOSTERONE
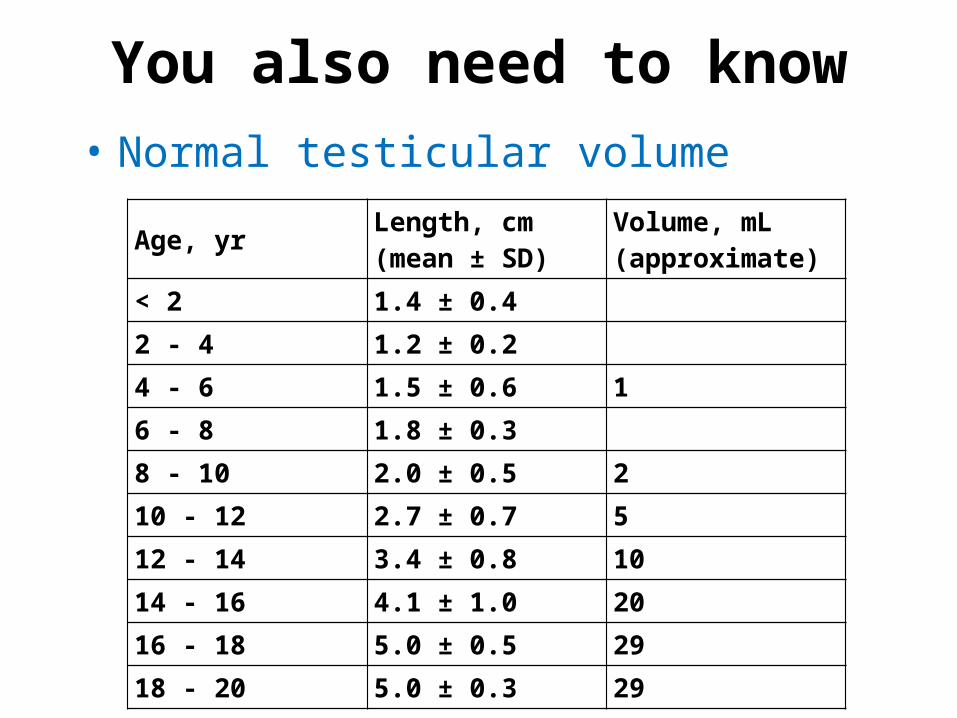
You also need to know• Normal testicular volume
Age, yr Length, cm (mean ± SD)
Volume, mL (approximate)
< 2 1.4 ± 0.4
2 - 4 1.2 ± 0.2
4 - 6 1.5 ± 0.6 1
6 - 8 1.8 ± 0.3
8 - 10 2.0 ± 0.5 2
10 - 12 2.7 ± 0.7 5
12 - 14 3.4 ± 0.8 10
14 - 16 4.1 ± 1.0 20
16 - 18 5.0 ± 0.5 29
18 - 20 5.0 ± 0.3 29
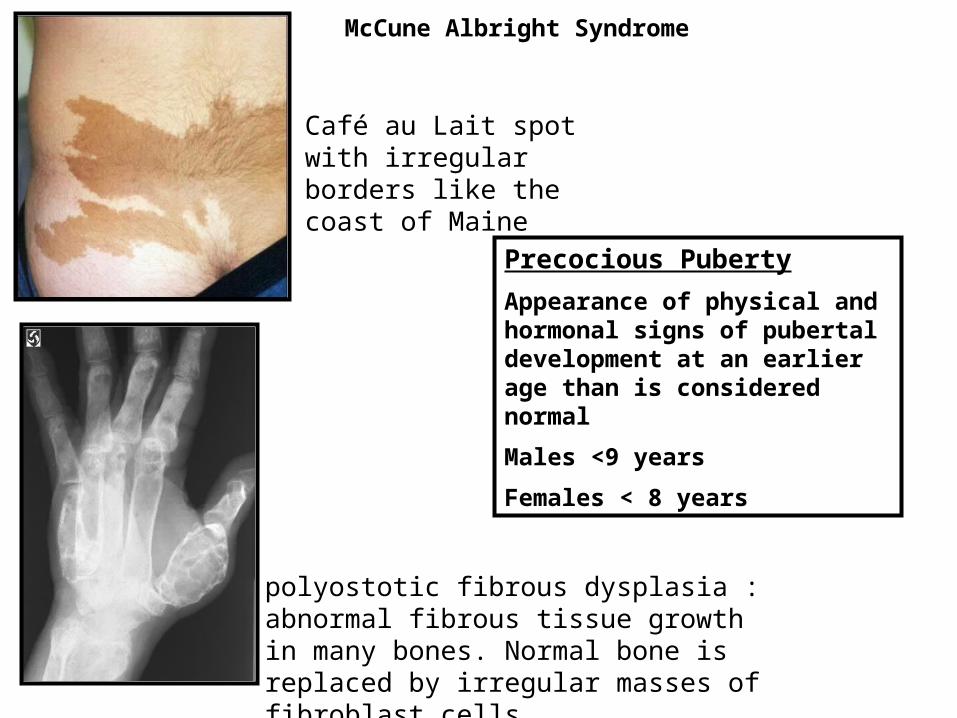
McCune Albright Syndrome
Café au Lait spot with irregular borders like the coast of Maine
polyostotic fibrous dysplasia :abnormal fibrous tissue growth in many bones. Normal bone is replaced by irregular masses of fibroblast cells.
Precocious Puberty
Appearance of physical and hormonal signs of pubertal development at an earlier age than is considered normal
Males <9 years
Females < 8 years

Cri du Chat/ Deletion 5p
One of the most common human deletion syndromes with an incidence 1 in 20,000 to 1 in 50,000 births
The syndrome was discovered in France in 1963 by a team headed by the late Jerome Lejeune.
The peculiar cry of affected infants sounded to Lejeune like the meowing of a Parisian cat.
The syndrome involves severe developmental and mental retardation and a characteristic constellation of congenital malformations:
microcephaly round face hypertelorismmicrognathia epicanthal folds low-set ears hypotonia motor and mental retardation
Although the majority of patients die in early childhood, some survive into adulthood and exhibit an IQ below 20.

This girl has hearing problems but otherwise does well in school.
What is her diagnosis?•Treacher CollinsWhat might clue you in on family history?•Multiple family members with hearing aids
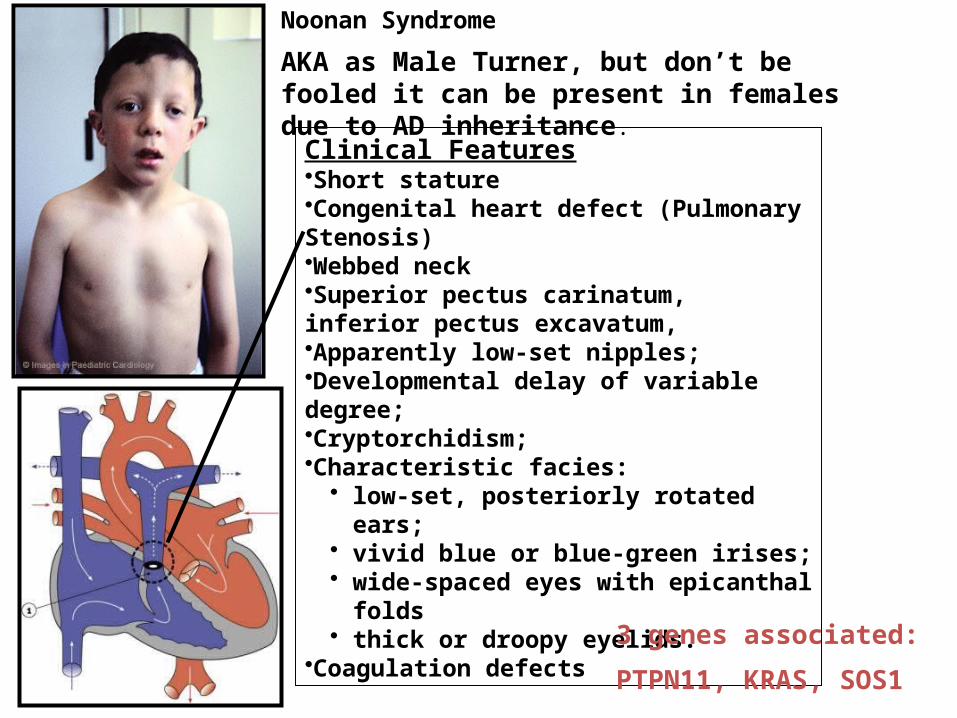
Noonan Syndrome
Clinical Features•Short stature•Congenital heart defect (Pulmonary Stenosis)•Webbed neck•Superior pectus carinatum, inferior pectus excavatum, •Apparently low-set nipples;•Developmental delay of variable degree; •Cryptorchidism; •Characteristic facies:
• low-set, posteriorly rotated ears; • vivid blue or blue-green irises; • wide-spaced eyes with epicanthal folds• thick or droopy eyelids.
•Coagulation defects
AKA as Male Turner, but don’t be fooled it can be present in females due to AD inheritance.
3 genes associated:
PTPN11, KRAS, SOS1
• You have an obese 6 year old male who was brought in because his mom is frustrated that he is always waking up and stealing food from the kitchen at night even though he’s on a diet.
• What is the mechanism of action for the diabetes he will likely develop?– It’s type 2 DM due to insulin resistance
• What other complications is he at risk for?– GH deficiency, hypogonadism, osteoporosis,
hypothyroidism, SCFE, sleep apnea….
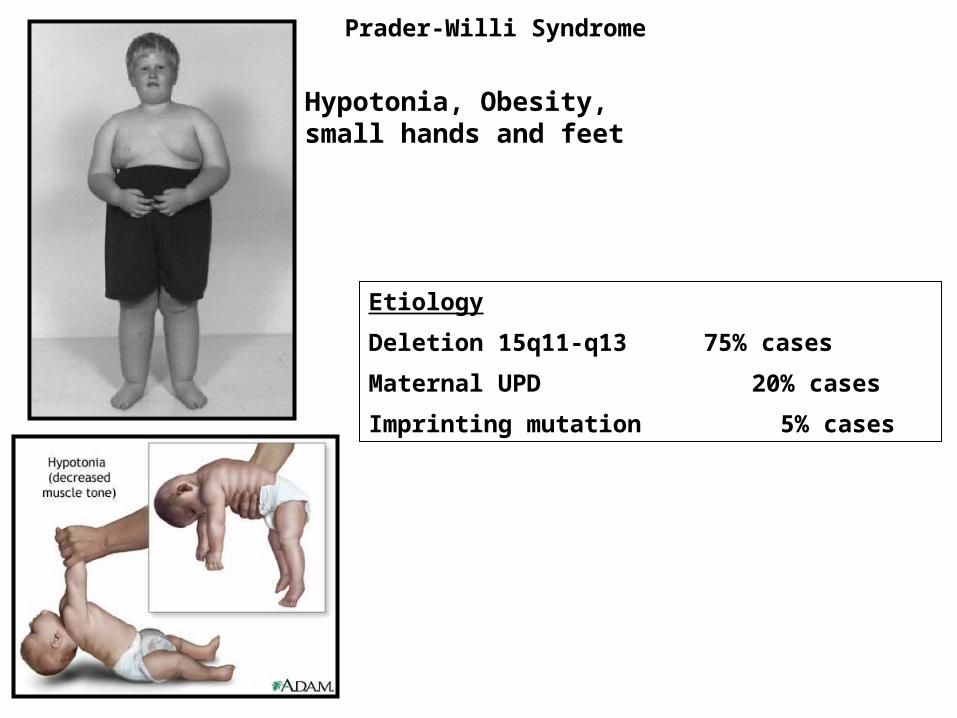
Prader-Willi Syndrome
Hypotonia, Obesity, small hands and feet
Etiology
Deletion 15q11-q13 75% cases
Maternal UPD 20% cases
Imprinting mutation 5% cases
Clinical Features
Severe DDM
Profound speech impairment
Ataxia and other movement disorders
Inappropriate laughter
Short attention span
Microcephaly and seizures
Wide spaced teeth
Hypopigmentation
Angelman Syndrome
Remember IMPRINTING
2 alleles from MOM PWS
2 alleles from DAD AS
Clinical Features
Macroglossia
Omphalocele
Macrosomia
Hypoglycemia
Hemihypertrophy
Hypospadias
Indentation on posterior helix
Beckwith Wiedemann Syndrome
Inheritance
autosomal dominant
Clinical Features
aplasia or hypoplasia of the thymus (immunodeficiency)
aplasia, or hypoplasia of the parathyroid glands (Hypocalcemia)
conotruncal cardiac defects
Hearing loss, CL/CP, velopharyngeal incompetence, prominent nose, narrow alae nasi, long face
Slender fingers
DiGeorge Syndrome/ Deletion 22q11.2/VCF
VSD (62%) R AoArch (52%), TOF (21%)
What lab test makes the diagnosis:
FISH 22q
• You would use FISH to detect all of the following syndromes except:A. Prader williB. EdwardsC. VelocardiofacialD. WilliamsE. Cri du chat
• All of them are deletions except Edwards (check chromosomes)

Mental retardation, dysmorphic facies, infantile hypercalcemia, growth deficiency, cocktail personality, hoarse voice, enamel hypoplasia
Williams Syndrome
Supravalvular Ao stenosis

Prenatal and postnatal growth delay
Neurodevelopmental deficits
Long philtrum
Thin/smooth upper lip
Short palpebral fissures
Epicanthal folds
mid face hypoplasia
Mild to moderate microcephaly
Short nose
Fetal Alcohol Syndrome

















