67
THE BONE SCAN You have to know what is normal before you determine what is ABNORMAL! Presented by Dr. Amol Gulhane DNB resident
| Date post: | 07-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | amol-gulhane |
| View: | 77 times |
| Download: | 1 times |
THE BONE SCAN
You have to know what is normal before you determine what is ABNORMAL!
Presented by Dr. Amol Gulhane DNB resident

A nuclear medicine procedure, such as a bone scan. The term is derived from the decay of the radionuclide and its resultant gamma radiation or scintillations. The number of scintillations corresponds to the concentration of the isotope.
Scintigraphy

Nuclear Medicine
Images are generated as the uptake and distribution of administered radiopharmaceuticals are detected
Provides vital information regarding tissue perfusion, physiology, and biochemistry
Physiologic and metabolic changes often precede gross structural alteration of diseased tissue by hours, days or even weeks
Key factor in determining early diagnosis and proper treatment protocols and in establishing an accurate prognosis
Radionuclide Bone Scanning Most frequently performed nuclear
medicine technique Used to evaluate soft tissue, bone and
joint disorders Fractures, infections, arthritides, tumors
and osteonecrosis
History
Skeletal scintigraphy radiopharmaceuticals were first introduced in the early 1960s
1971 Technitium 99-MDP polyphosphate compounds were introduced
Today we use diphosphonates which have faster blood clearance and higher skeletal uptake
Radiopharmaceutical Agents Dozens are employed Earlier technetium pyrophosphate was
used which is now replaced by the Tc-based
diphosphonates, primarily Tc-99m-MDP (methylene diphosphonate).
6 hour half-life Principal photon energy of 140 keV

Tc-99m-MDP is administered intravenously and is delivered to the skeletal system based on vascular distribution.
Vigorous osteoblastic activity in the growth plates of juvenile skeletons, healing fractures,pathologic conditions stimulating skeletal blood flow, and bone repair increase the bone labeling.

In the normal adult, skeletal tracer uptake is fairly uniform and symmetric.
Uptake is greater in the axial skeleton (pelvis, spine) than in the appendicular skeleton (skull and extremities).Mild,uniform soft tissue uptake is noted in the background. The kidneys should be slightly hotter than the soft tissues and should be symmetric and normal anatomically.
The renal collecting system,ureters, and bladder activity appear very intense.
NORMAL "HOT" AREAS... • SI Joints
• Acromioclavicular joints
• Hip joints
• Sternoclavicular joints
• Ends of long bones
• Growing epiphysis (in pediatric patients)
• Fractures and orthopedic surgery produce uptake for 1 or more
years • Variations in spine uptake are casued by normal curvature of the
spine
Image generation
Radiopharmaceutical emits gamma rays that are detected by an instrument and transformed into electrical signals that ultimately generate a computer image of the tracer agent activity and concentration

Examination Procedure
Three phases which represent the distribution of the tracer over the course of time Phase 1 – Flow phase or radionuclide angiogram
- tracer is intravascular – images are obtained every 2-3 seconds for 30 seconds
Phase 2 – Blood pool phase – the tracer is located in the extravascular space – the body is imaged 5 minutes after injection
Phase 3 – Bone scan phase – 2-4 hours after injection – represents clearance of the tracer from the vessels and soft tissues and concentration into the skeleton

Phase 4- can be acquired the following morning if better skeletal detail is needed, usually when the patient has poor renal function, such as in the diabetic foot.

Blood Flow Phase
Show radionuclide in the arterial, capillary, and venous phases
Variations may occur in the blood flow to the extremities depending on the vascular status and activity

Blood Pool Phase
Shows radionuclide in the extravascular space
Vascular structures such as kidneys, liver, spleen and uterus are seen and should not be mistaken for sites of abnormality

Bone Scan Phase
Show radionuclide in the skeleton and soft tissue
Metaphyseal regions of long bones show higher uptake than diaphyses – due to higher bone turnover rate in the metaphyses
Areas of highest uptake are the sternum and SI joints
The anterior wings of the iliac bones and the coracoid processes normally show considerable uptake of the radionuclide
Scoliosis – the concave side of the spine appears hotter than the convex

3 phase bone scan
Patient Presentation
Children have high diffuse bone uptake and prominent uptake around the growth plates
Elderly patients tend to have poor-quality bone scans
Heavy patients have poor quality bone scans owing to the greater amount of soft tissue, which causes more scatter and higher attenuation of the photons in the soft tissues because of the greater distance of the detectors from the skeleton
Poor hydration prevents optimal clearance of the radionuclide from the soft tissues
Renal failure prevents good soft tissue clearance Corticosteroids may produce generalized
decreased skeletal uptake
Absorbed Patient Dose
Exact dose is difficult to determine Influenced by:
Tracer biodistribution Organ pathology Renal function

Dose
Approximately 50% of the injected dose is taken up by the skeleton within 2-6 hours
The Tc agents are excreted by glomerular filtration from the kidneys. In a normal subject, 50% is excreted by 4
hours, and up to 80% of the injected diphosphonate will be excreted by 24 hours
Normal renal function clears soft tissue activity, thus
improving the quality of bone images because of improved target-to background ratios.
Decreased renal function from any cause degrades image quality.

Bladder receives the highest dose
May be reduced by pre-examination hydration and frequent voiding after exam
Whole-body dose is approximately 0.13 rad (average dose for CT scan of the L/S is 3-5 rad.
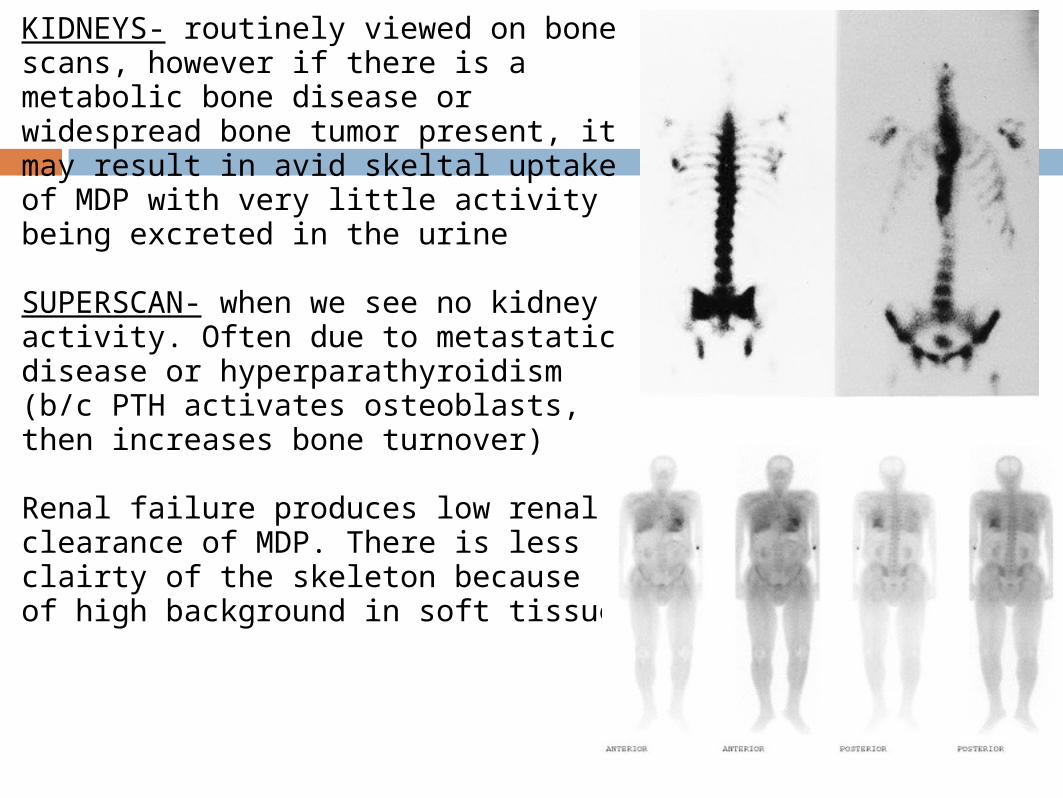
KIDNEYS- routinely viewed on bone scans, however if there is a metabolic bone disease or widespread bone tumor present, it may result in avid skeltal uptake of MDP with very little activity being excreted in the urine SUPERSCAN- when we see no kidney activity. Often due to metastatic disease or hyperparathyroidism (b/c PTH activates osteoblasts, then increases bone turnover) Renal failure produces low renal clearance of MDP. There is less clairty of the skeleton because of high background in soft tissue

Contraindications
Pregnancy because transplacental transmission of radiopharmaceuticals is possible
Breast milk will carry isotope activity for several days after the study

Several Bone Scan Uses
Insufficiency fractures in metabolic disease
Trauma Metastatic Disease Disuse osteoporosis Osteomalacia Osteonecrosis Osteomyelitis
Insufficiency fractures in metabolic disease Pubic rami Femoral necks Femoral condyles Metaphyses of the proximal and distal
portions of the tibias, sacrum and calcaneus
Tend to be bilaterally symmetric and occur in the metaphyses of long bones of the lower extremities

Trauma to the skeleton may be undetectable on standard radiographic examinations.
The classic stress fracture may be caused by overuse of the normal skeleton, or an insufficiency fracture may result from normal use of weakened bone.
Scintigraphically demonstrated trauma precedes radiographically detectable fracture healing by approximately 10 days.
Decreased or normal osteoblastic activity is seen at the fracture site in this first phase of repair.
The subsequent osteoblastic activity then shows as a hot spot weeks before the calcified callus appears on a radiograph

In an uncomplicated fracture, repaired bone returns to normal appearance as the callus at the fracture site remodels over a period of months
A complicated fracture in a weight-bearing bone may take many years to return to normal bone scan activity.
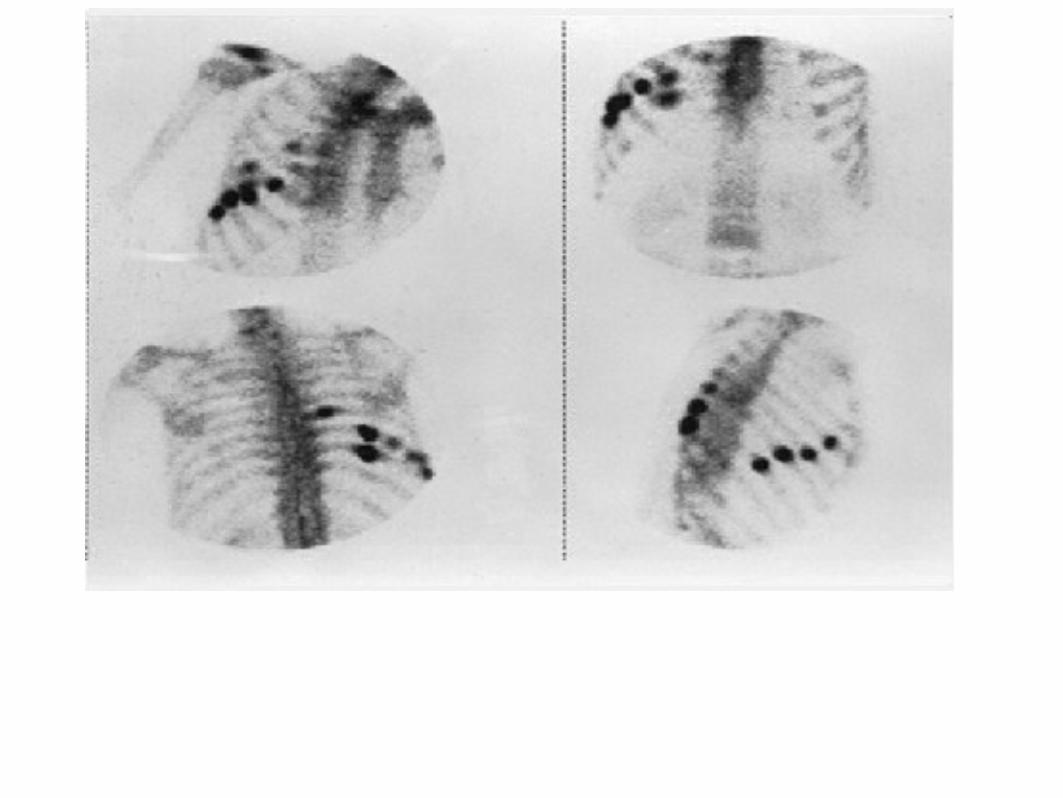
Multiple Rib Fractures. Vigorous osteoblasticrepair activity is seen in two rows of fractures, which were notvisible on radiographs.
Trauma
Increased blood flow associated with bone repair results in marked radiopharmaceutical accumulation
Occult fractures demonstrate an increased perfusion
Important for follow up to assess for fracture non-union
Compression fractures of the spine reveal a horizontal band of increased tracer activity, typically affecting the superior endplate

Serial bone scans of the lower thoracic and lumbar spine at intervals of months show a normal spine followed by a compression fracture of L1, which gradually heals, only to be replaced by new fractures at T9 and T12. Note the horizontal, linear pattern of a simple vertebral compressionfracture

Recent studies have shown that a pinhole bone scan is more sensitive than plain film or CT for scaphoid and other fractures of the wrist.
Whole-body bone scans are useful in detecting unsuspected fractures following severe cases of multiple trauma.

Prosthetic joint replacements may loosen and/or become infected.
For about 6 months after hip replacement surgery, the bone around the prosthesis is expected to have increased osteoblastic activity.
Thereafter, increased labeling correlates with infection, loosening,and heterotopic bone formation
Radiographs and, occasionally, radiolabeled white blood cell scans may be required to further diagnose abnormal findings

Hip Prosthesis Loosening. Anterior images ofthe pelvis, hips, and femurs show intense labeling around thefemoral (long arrows) and acetabular (wide arrows) componentsof a 2-year-old total hip arthroplasty. Both had loosened withoutinfection.
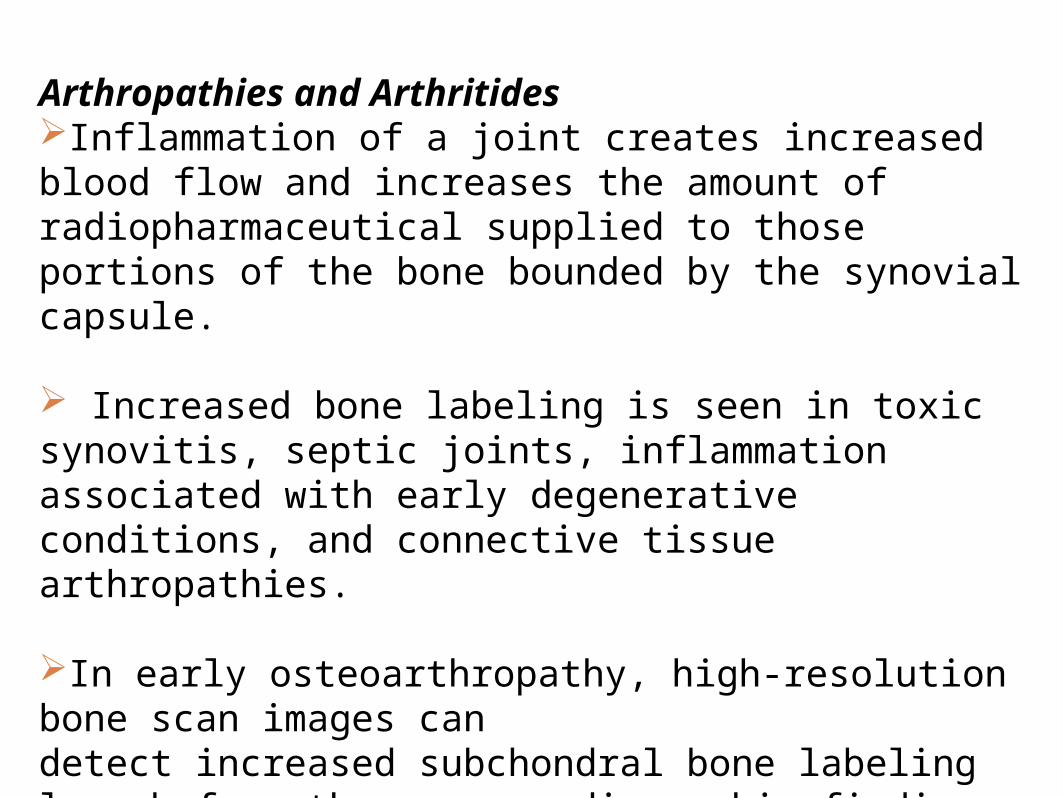
Arthropathies and ArthritidesInflammation of a joint creates increased blood flow and increases the amount of radiopharmaceutical supplied to those portions of the bone bounded by the synovial capsule.
Increased bone labeling is seen in toxic synovitis, septic joints, inflammation associated with early degenerative conditions, and connective tissue arthropathies.
In early osteoarthropathy, high-resolution bone scan images candetect increased subchondral bone labeling long before there are radiographic findings.
Intense, abnormal labeling also is seen in neuropathic jointslong before the abnormality is detected by radiographs
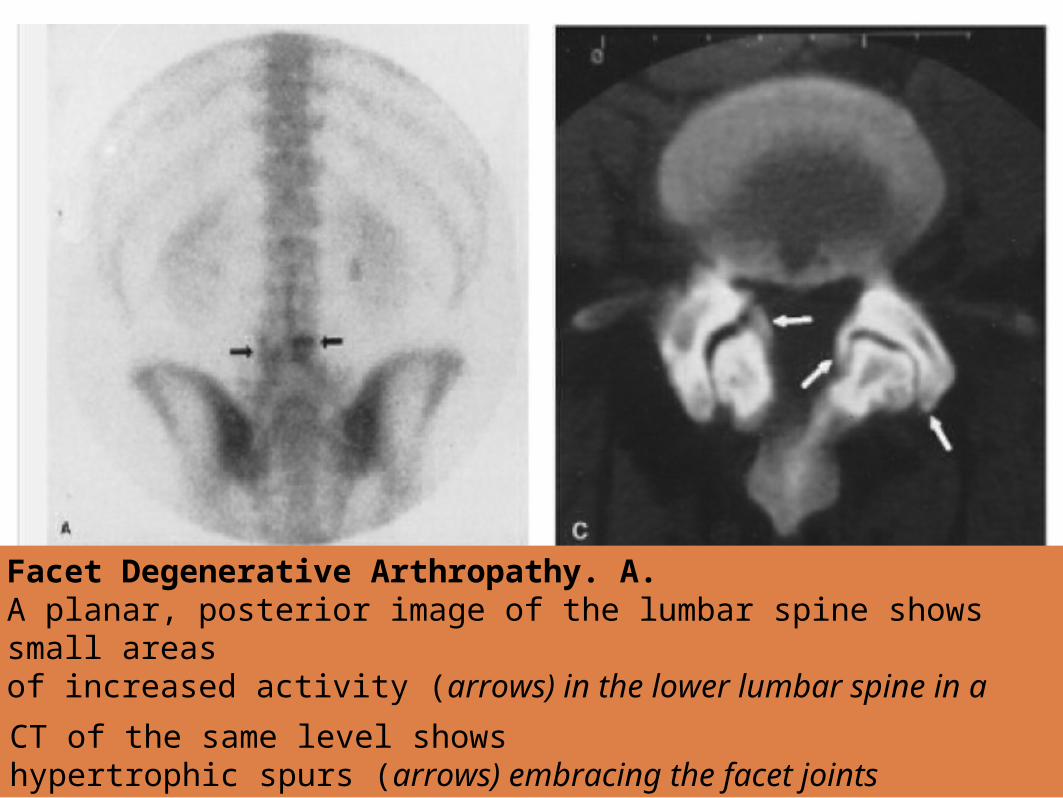
Facet Degenerative Arthropathy. A.A planar, posterior image of the lumbar spine shows small areasof increased activity (arrows) in the lower lumbar spine in apatient with chronic low back pain.
CT of the same level showshypertrophic spurs (arrows) embracing the facet joints

Metastatic Disease
The most common use of the bone scan is for the detection andmonitoring of metastatic tumor involving the skeleton.
tumors monitored prostate, lung, breast, thyroid, and renalCarcinoma
Majority of metastases affect the axial skeleton in a pattern that reflects the distribution of the erythropoietic marrow.
Most metastases are multiple at the time of discovery.

a solitary hot spot in the skull or a rib has a low probability of being a metastatic lesion.
Comparison bone scans at intervals of 3 to 6 months allow an accurate assessment of tumor spread.
Because of its sensitivity, the bone scan can be utilized when a cancer patient has new backpain or bone pain.

superscan - Numerous prostate cancermetastases produce â hot spots of intense isotopeaccumulation that leave little or none of the radiopharmaceuticalfor renal excretion or soft tissue uptake.

A cold spot within the femoral head is highly specific for avascular necrosis (AVN) and is the earliest scintigraphic evidence of this disease.
This finding is usually seen 7-10 days after the ischemic event.
Over a period of weeks to months, increased uptake representing revascularization and repair surrounds and eventually replaces the region of photopenia.
The central region of photopenia with surrounding zone of increased uptake is termed the doughnut sign.
Osteonecrosis
Initially, uptake is decreased in all phases, which represents the early ischemic event.
Later, uptake is decreased within the femoral head in the perfusion phase and increased around the cold region in the bone scan phase.
It represents the reactive zone around the infarcted segment. The increased uptake from the reparative zone eventually replaces the photopenic region.


Osteomyelitis
In a large bone such as a tibia, acute hematogenous infection of bone that precedes radiographic abnormality can be sensitively andspecifically diagnosed by three-phase bone scans.
early infection Early arterial flow seen seconds after injection (first phase)increased blood pool (second phase) for a few minutes intense labeling in third phase

Radiographic changes may not be seen for 10 to 14 days.
The scan is more difficult to read and not as specific when the target is small (e.g., the bones of the foot)
In the small bones it is difficult to differentiate between an infection adjacent to a bone with increased soft tissue and increased periosteal labeling from an infection within the bone.
Bone scans may take months to normalize after infections of bone are sterilized, and thus a white blood cell scan may be useful for follow-up.

Osteomyelitis of the Second Toe andMetatarsal and Septic Second Metatarsal Phalangeal Joint.A. A plantar bone scan shows increased activity in the secondproximal phalanx (, metatarsal phalangeal joint and second metatarsal indicating reactive bone stimulated by the infection. Decreased activity distal to that pointcorresponds with necrotic tissue. B. A radiograph shows destructive changes in the second proximal phalanx but the foot appears normal in the second metatarsal phalangeal joint and metatarsal phalangeal shaft.
Primary bone tumors
Benign lesions do not show typically increased activity in the early phases, and even if there is a detectable late phase activity, it is moderate (except for osteoid osteoma, osteoblastoma, fibrotic dysplasia and aggressively growing bone cysts, or lesions that are associated with pathologic fractures.)
Malignant tumors (osteosarcoma, Ewing sarcoma) as opposed to benign tumors, have an increased blood supply and a more intense osteoblast activity
MDP bone scan highly sensitive in the diagnosis of osteoid osteoma.
Initial vascular blush followed by a focal avid tracer uptake in the delayed skeletal phase
The double density sign is the diagnostic feature of the central nidus on a bone scan.
SPECT localizes the nidus as a focal avid uptake in the middle of the lesion, with a decremental uptake toward the periphery.
Osteoid Osteoma
DD of osteoid osteoma includes a healing stress fracture, and osteomyelitis due to the similarity of symptoms, presentation, and overlapping radiological features.
Plain radiography and CT find it difficult to localize the nidus due to varying degrees of bony sclerosis masking the central nidus.
On SPECT Osteoid osteoma has characteristic features of central avid focus with decremental activity toward the periphery, differentiating it from osteomyelitis and stress fracture, which appear more diffuse and linearly oriented along the long axis of the bone,

Radioisotope bone scan in a 6-year-old child who presented with left hip pain demonstrates intense uptake in the left proximal femur.

OsteosarcomasTypically show increased uptake of radioisotope on bone scans
Bone scans are most useful in excluding multifocal disease.
Skip lesions and pulmonary metastases may also take up the radioisotope, but skip lesions are most reliably excluded by MRI.
Lateral isotope bone scan reveals intense uptake in the calcaneal region. The remainder of the skeleton appeared normal.

The primary tumor of Ewing sarcoma is usually depicted as a focal area of increased radionuclide activity.
Whole-body bone scans can provide information about the primary lesion and depict skip lesions.
Bone scintigraphy can be used to localize distant metastases during tumor staging.
Three-phase dynamic bone scintigraphy (TPBS) can help in the assessment of treatment effects
In cases that respond to treatment, a reduction of both flow and tracer uptake can be observed.
Ewing sarcoma
In addition to technetium-99m (99m Tc), other tracers, such as thallium-201 (201Tl) & Gallium-67 (67 Ga) are used to assess the therapeutic response.
However (PET) scanning with (FDG) is currently usedFDG is used as a marker of tumor viability, and it may help to detect lesions that are not depicted on conventional bone scans.
In addition, PET scanning is the most sensitive modality for therapeutic follow-up, and this modality can reveal early changes in tumor metabolism, which is an indicator of the therapeutic effect.
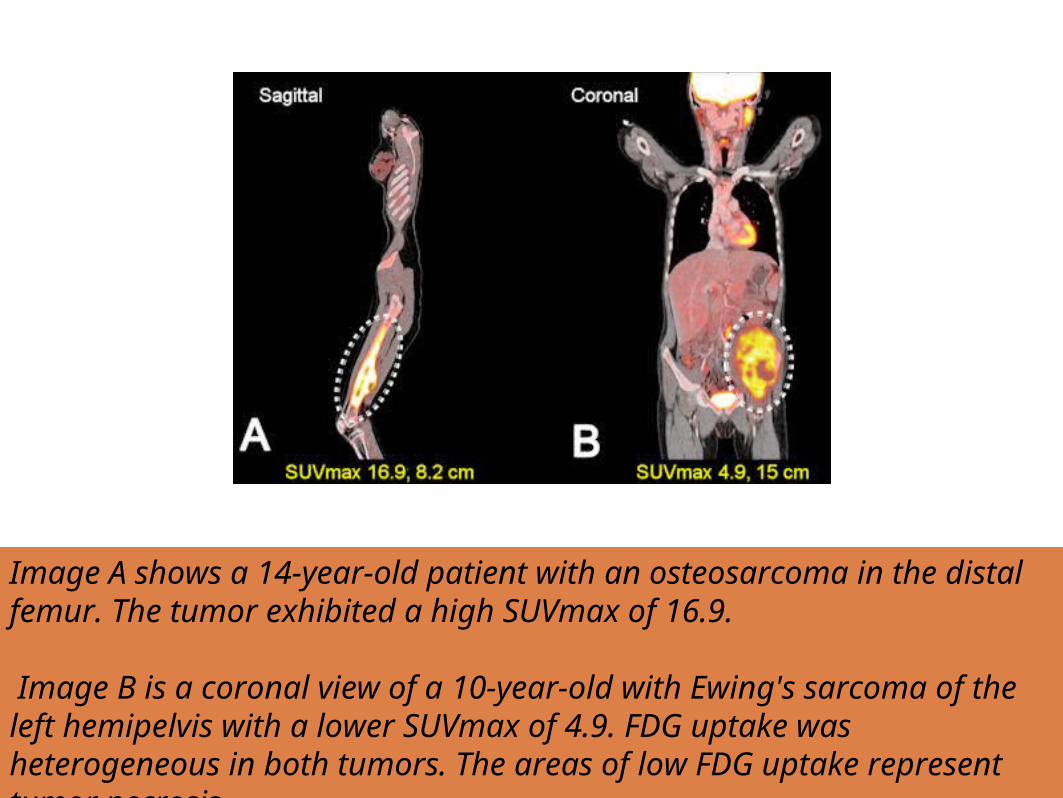
Image A shows a 14-year-old patient with an osteosarcoma in the distal femur. The tumor exhibited a high SUVmax of 16.9.
Image B is a coronal view of a 10-year-old with Ewing's sarcoma of the left hemipelvis with a lower SUVmax of 4.9. FDG uptake was heterogeneous in both tumors. The areas of low FDG uptake represent tumor necrosis.

Vascular Phenomena
There is a strong vascular influence on the labeling of bones.Increased blood flow stimulates increased osteoblastic andosteoclastic activity.
Tumor and trauma cause hyperemia and increased bloodpooling, with increased delivery of radiopharmaceuticals to thebone's osteoblasts.
In Reflex sympathetic dystrophy release of sympathetic vascular tone causes arteries to dilate .

A bone scan is also a simple test of the vascular status of a bone or bone graft.
If osteoblasts are labeled, the blood supply must be intact.
Bone subjected to radiation therapy may lose blood supply and osteoblastic activity.

B. The early blood poolimage (left) shows greater blood pooling (arrows) in the left foot. The 3-hour delayed images show a generalized increase inbone labeling.
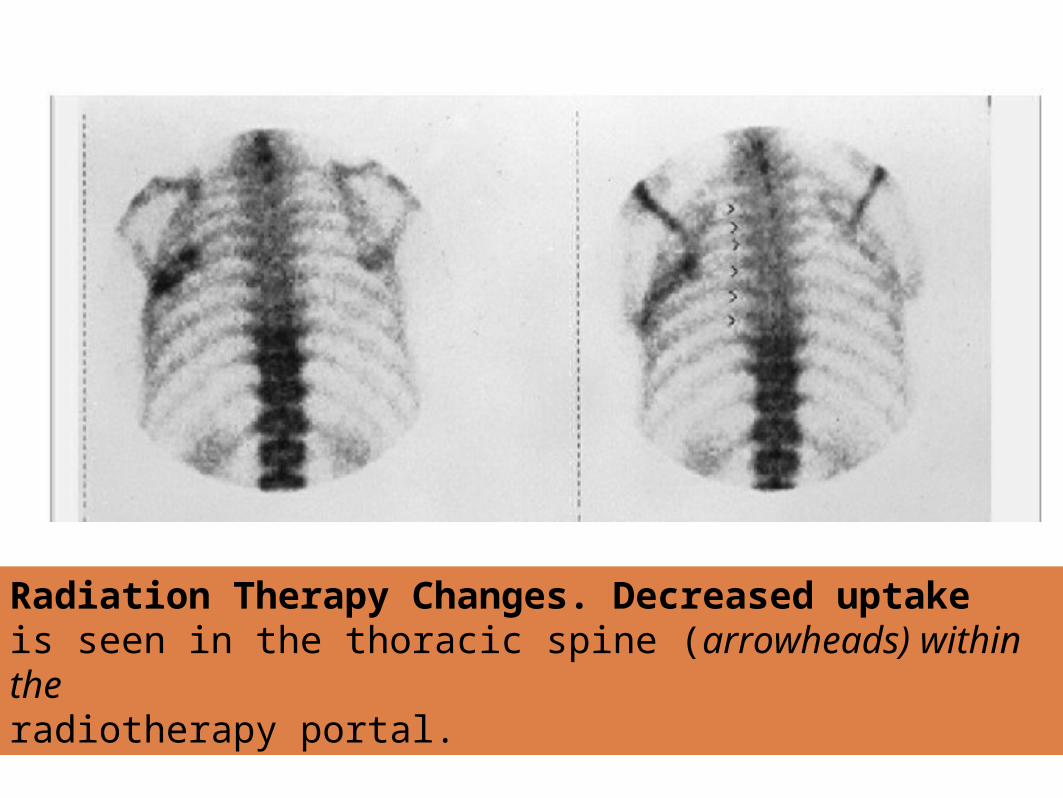
Radiation Therapy Changes. Decreased uptakeis seen in the thoracic spine (arrowheads) within theradiotherapy portal.

Heterotopic BoneRepair of soft tissue injuries sometimes leads to the formation of heterotopic bone.
Muscle crush injuries healing with the formation of heterotopic bone (myositis ossificans) are readily labeled on bone scans, weeks before a plain film will show signs of calcification.
The restricting area may be safely released orresected after the blood pool phase becomes inactive.
Soft tissues around joint prostheses, in paralyzed limbs, and in burn injuries are common sites of heterotopic bone formation.
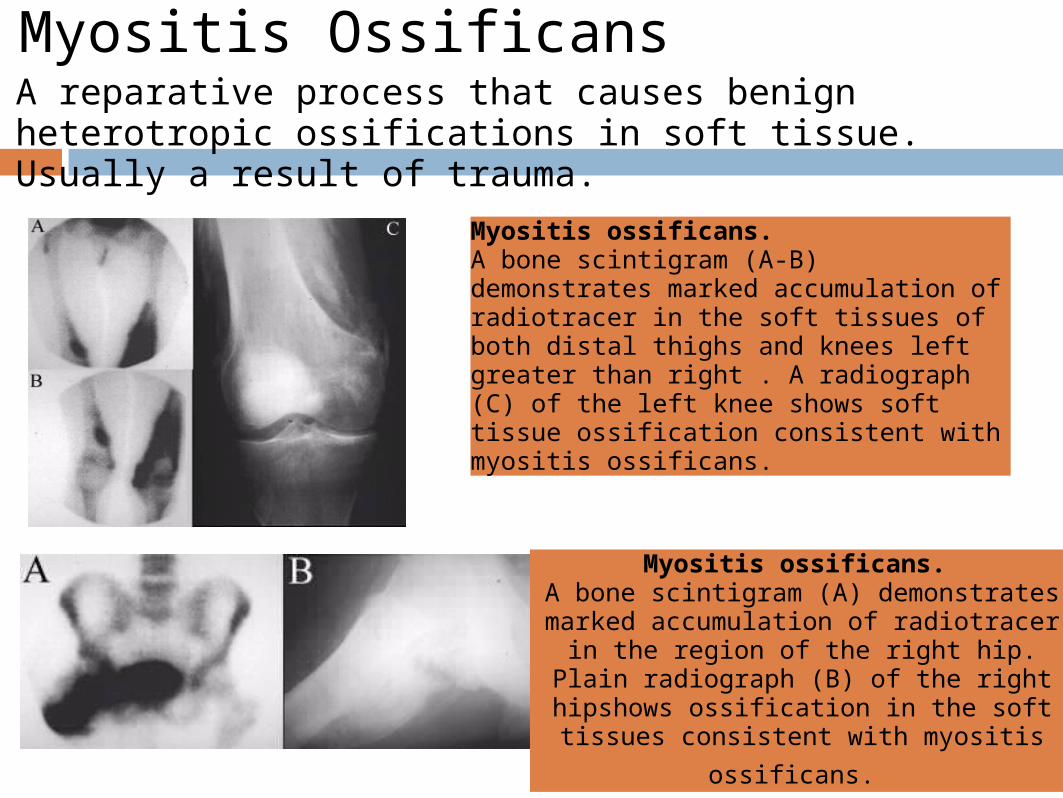
Myositis OssificansA reparative process that causes benign heterotropic ossifications in soft tissue. Usually a result of trauma. Myositis ossificans.
A bone scintigram (A-B) demonstrates marked accumulation of radiotracer in the soft tissues of both distal thighs and knees left greater than right . A radiograph (C) of the left knee shows soft tissue ossification consistent with myositis ossificans.
Myositis ossificans. A bone scintigram (A) demonstrates marked
accumulation of radiotracer in the region of the right hip. Plain radiograph (B) of the right hipshows ossification in the soft tissues
consistent with myositis ossificans.

MAKING A DIAGNOSIS...
• Increased activity is not diagnositc of neoplastic process • Positive bone scan findings does NOT differentiate between
malignant or benign • Final diagnosis is made by correlating bone scan images
with clinical data and other imaging modalities ( SPECT CT)
PITFALLS IN BONE SCANS
• Epiphyeal plates in kids will appear hot due to increased blood flow and metabolism in growing bones
• Bone images may be negative when bony healing is
completed (healed fx's, cured osteo, treated bone mets). However, this may take 1+ years.
• Ga-67 or In-111 used with Tc-99m MDP for osteomyelitis.
They help define active osteomyelitis and may detect deep soft tissue infection

• MDP may concentrate at sites of soft tissue pathologic conditions such as breast CA, malignant pleural effusions, ascites, soft tissue malignancies, myositis ossificans, MI, electrical burns, ectopic calcification, splenic infarction, IM injections
• Bone grafts show increased activity at the ends of the bone
graft, with little to no uptake in the middle for 6 months post sx.
INTERESTING FINDINGS

SCAR
Whole-body bone scan in anterior (A) and lateral (B) projections show linear radiotracer accumulation along the midepigastric region, where prior laparotomy scar is evident.

Urine contamination
Anterior image (A) of the bone scan shows 2 hot spots projecting over the right femur; repeat image (B) after decontamination shows disappearance of both hot spots.

Malignant Fibrohistiocytoma
Malignant fibrous histiocytoma (MFH) -most common soft tissue sarcoma of late adult life, most commonly occurring between 50-70yrs.
The bone scintigram (A) shows radionuclide accumulation in the soft tissue of the right thigh. Axial MRI (B) demonstrates an intramuscular soft tissue mass, that was biopsy-proven malignatn fibrohistiocytoma.
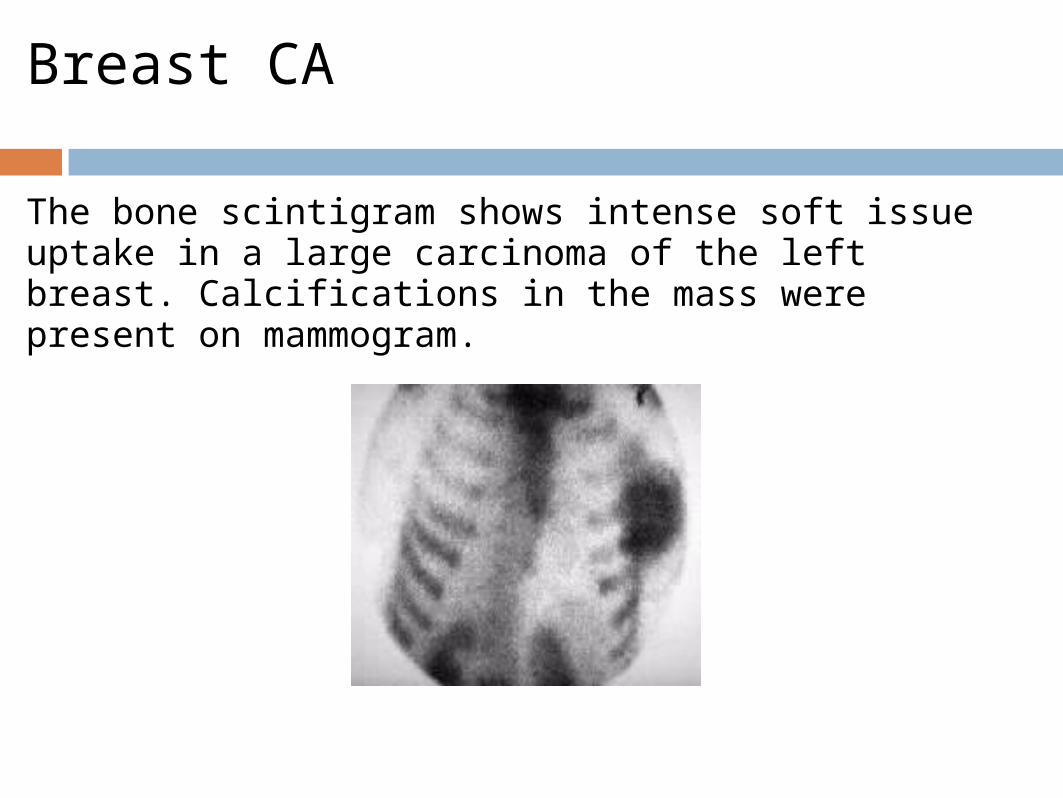
Breast CA
The bone scintigram shows intense soft issue uptake in a large carcinoma of the left breast. Calcifications in the mass were present on mammogram.

PET vs SPECT in Bone metastasis
PET often detects lesions missed on SPECT
PET has greater ability to differentiate between benign and malignant lesions (FDG is used)


















