BP-DES Update: Bioresorbable Polymer SYNERGY and Beyond Dean J. Kereiakes, MD FACC FSCAI Dean J. Kereiakes, MD FACC FSCAI Medical Director, The Christ Hospital Heart & Medical Director, The Christ Hospital Heart & Vascular Center and the Lindner Research Center at Vascular Center and the Lindner Research Center at The Christ Hospital, Cincinnati, Ohio The Christ Hospital, Cincinnati, Ohio Professor of Clinical Medicine, Ohio State University Professor of Clinical Medicine, Ohio State University
Transcript
BP-DES Update:Bioresorbable Polymer SYNERGY and Beyond
Dean J. Kereiakes, MD FACC FSCAIDean J. Kereiakes, MD FACC FSCAIMedical Director, The Christ Hospital Heart &Medical Director, The Christ Hospital Heart &Vascular Center and the Lindner Research Center atVascular Center and the Lindner Research Center atThe Christ Hospital, Cincinnati, OhioThe Christ Hospital, Cincinnati, OhioProfessor of Clinical Medicine, Ohio State UniversityProfessor of Clinical Medicine, Ohio State University
Disclosure Statement of FinancialInterest
• Modest Consulting Fees• Modest Consulting Fees
• HCRI• SINO Medical Sciences Technologies, Inc.
W ithin the pas t12 months , Iormy s pou s e/partnerhave had afinanc ialinteres t/arrangementoraffiliation with the organization(s )lis ted below.
• SINO Medical Sciences Technologies, Inc.• Boston Scientific Corporation• Abbott Vascular• Svelte Medical Systems, Inc.• Micell Technologies, Inc.• Caliber Therapeutics• Ablative Solutions, Inc.
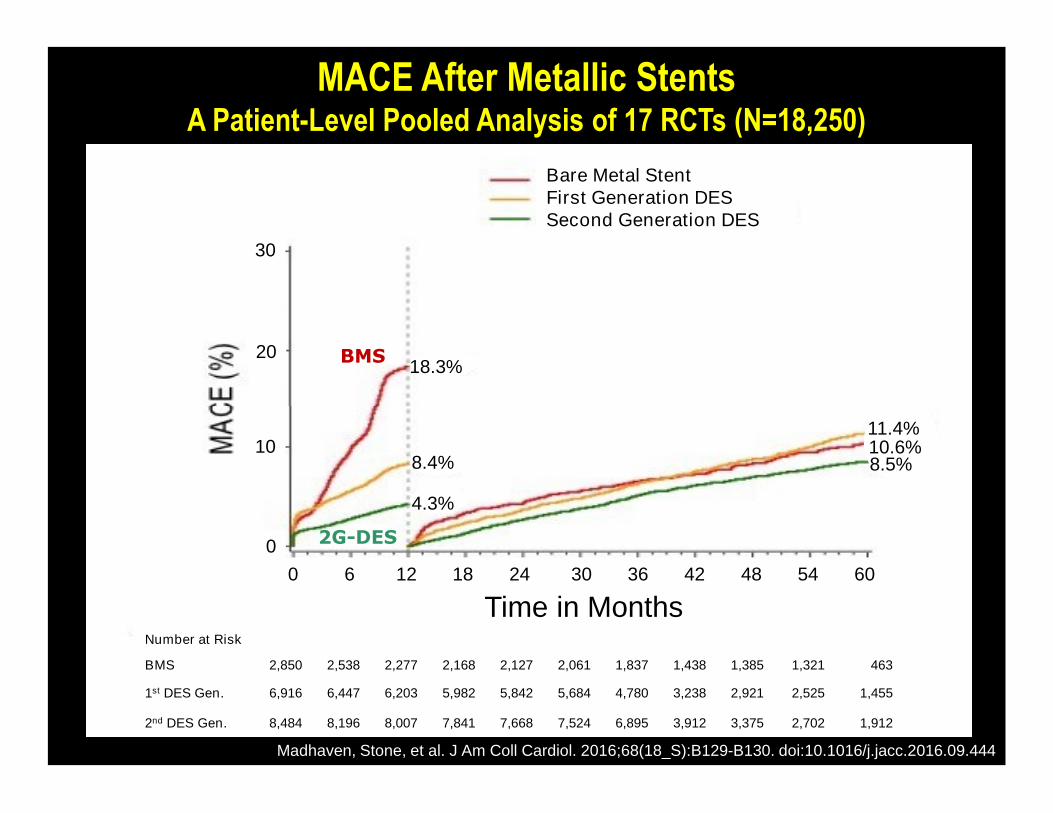
MACE After Metallic StentsA Patient-Level Pooled Analysis of 17 RCTs (N=18,250)
BMS
Bare Metal StentFirst Generation DESSecond Generation DES
1st DES Gen. 6,916 6,447 6,203 5,982 5,842 5,684 4,780 3,238 2,921 2,525 1,455
2nd DES Gen. 8,484 8,196 8,007 7,841 7,668 7,524 6,895 3,912 3,375 2,702 1,912
8.4%
4.3%
11.4%10.6%8.5%
Time in M onths0 6 12 18 24 30 36 42 48 54 60
10
0
M a dha ve n,Stone ,e ta l.J A m C oll C a rdiol.2 0 16; 68 (1 8 _S ): B 1 29-B 130 . d oi: 1 0 . 1 0 16/j. jac c . 2 0 16. 0 9. 444
Meta Analysis of 13 RCCT Involving 17,097 PatientsEES vs non-EES DES
Stent Thrombosis TVR MI
Statistical Model
Random (13)
Fixed (13)
ClopidogrelDurationDuration
6 months (5)
12 months (7)
Follow-up
≤ 1 year (12)
> 1 year (7)
0 . 1 1 1 0EES Non-EES
Favors
Baberetal.JA CC 2011;58:1569-77
0 . 4 4EES Non-EES
0 . 4 4EES Non-EES
Thromboresistance of PVDF Polymer Coating
0.8
1.0
1.2 P=0.002
for
Ste
nt
Form
uation]/
VIS
ION
(81μm
)]
Relative Platelet Adhesion in Ex-vivo flow loop model
Kolandaivelu,K.etak.,Circulation2011
1.00
0.76
0.0
0.2
0.4
0.6
CoCr VISION PVDF[LD
HAdsorb
ance
for
Ste
nt
[LD
HA
dsor
banc
efo
rCoCr
VIS
ION
(81
XIEN CE
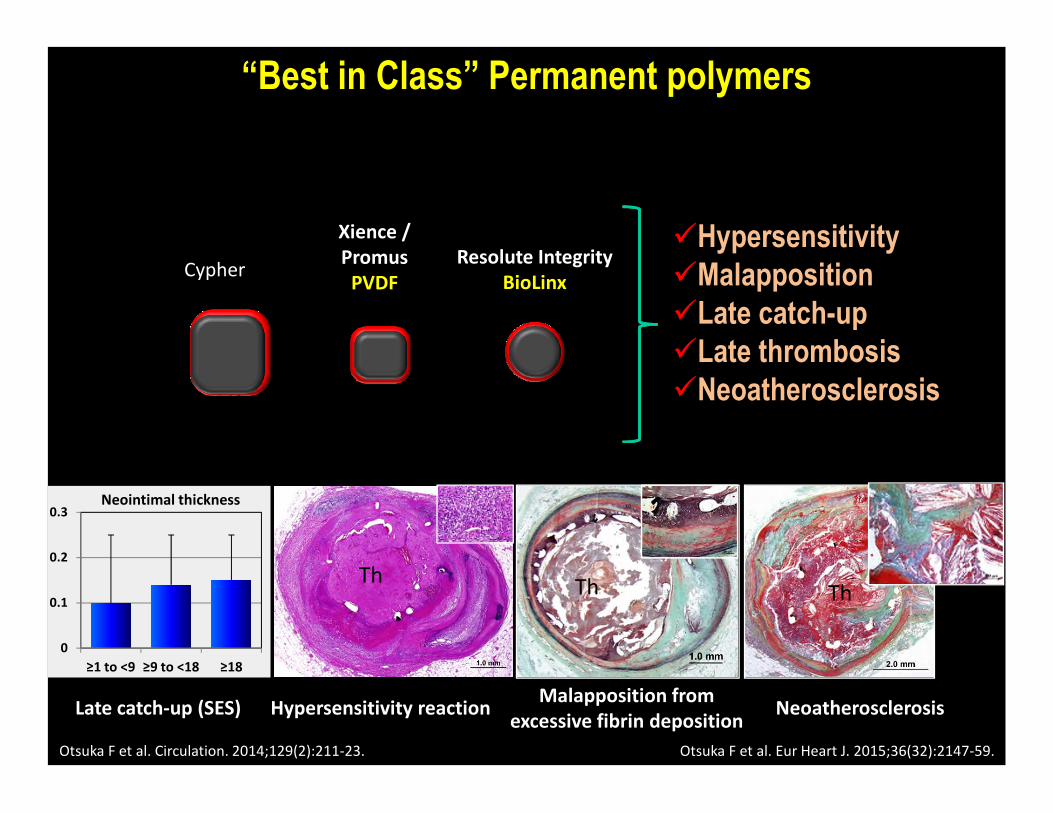
Stent Design Iterations that Impact Thrombosis/MACE
I. Strut Thickness (thinner)• Rapid /c omplete s tentcove ra ge /he a ling• Infla m m a tion• Throm boge nicity (zones oflow s hears tres s )
II. Polymer• Composition (thrombores is tant–P VD F)• Composition (thrombores is tant–P VD F)• BP vs . D P• Distribution (Abluminal only vs . C onformal)• Time Course for B P Resorption (< 3-4 vs . 9 -1 8 months
vs permanent)
III. Platform Flexibility/Conformability• Geometric D is tortion• Frac tu re Res is tanc e (thrombos is /res tenos is )
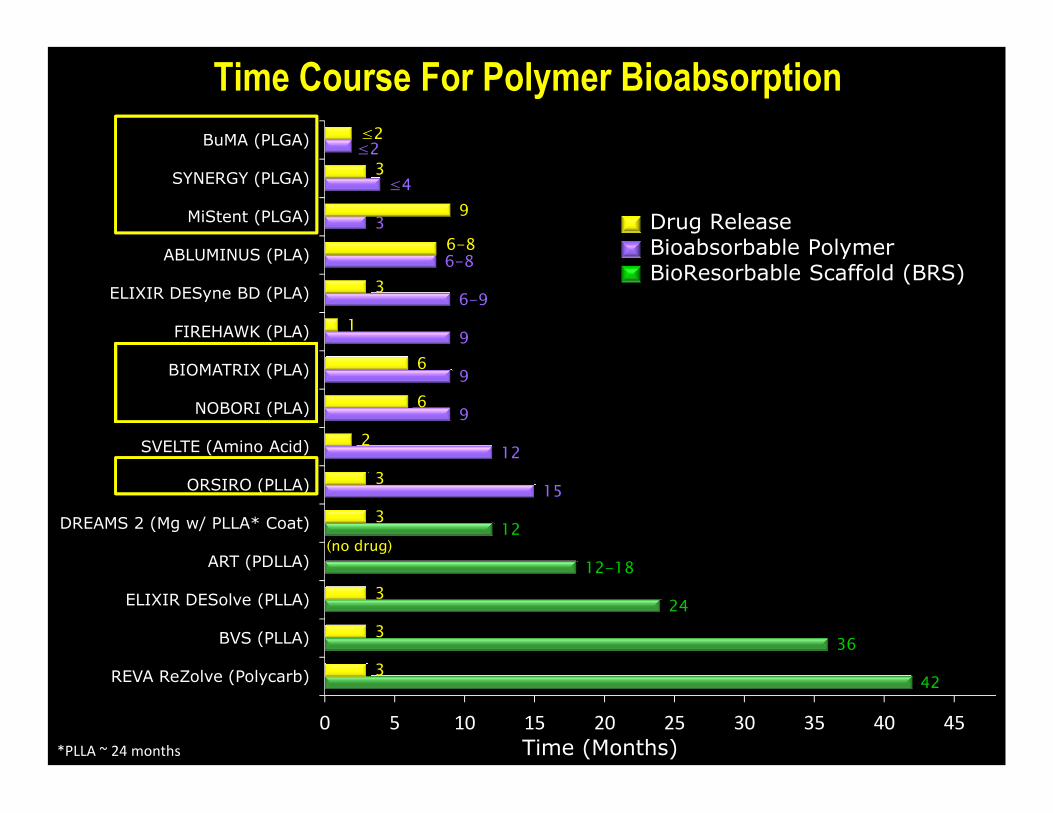
Drug ReleaseBioabsorbable PolymerBioResorbable Scaffold (BRS)
42
36
24
12-18
12
15
12
9
3
3
3
3
3
2
6
0 5 10 15 20 25 30 35 40 45
REVA ReZolve (Polycarb)
BVS (PLLA)
ELIXIR DESolve (PLLA)
ART (PDLLA)
DREAMS 2 (Mg w/ PLLA* Coat)
ORSIRO (PLLA)
SVELTE (Amino Acid)
NOBORI (PLA)
Time (Months)
(no drug)
*P L L A ~24 m onths
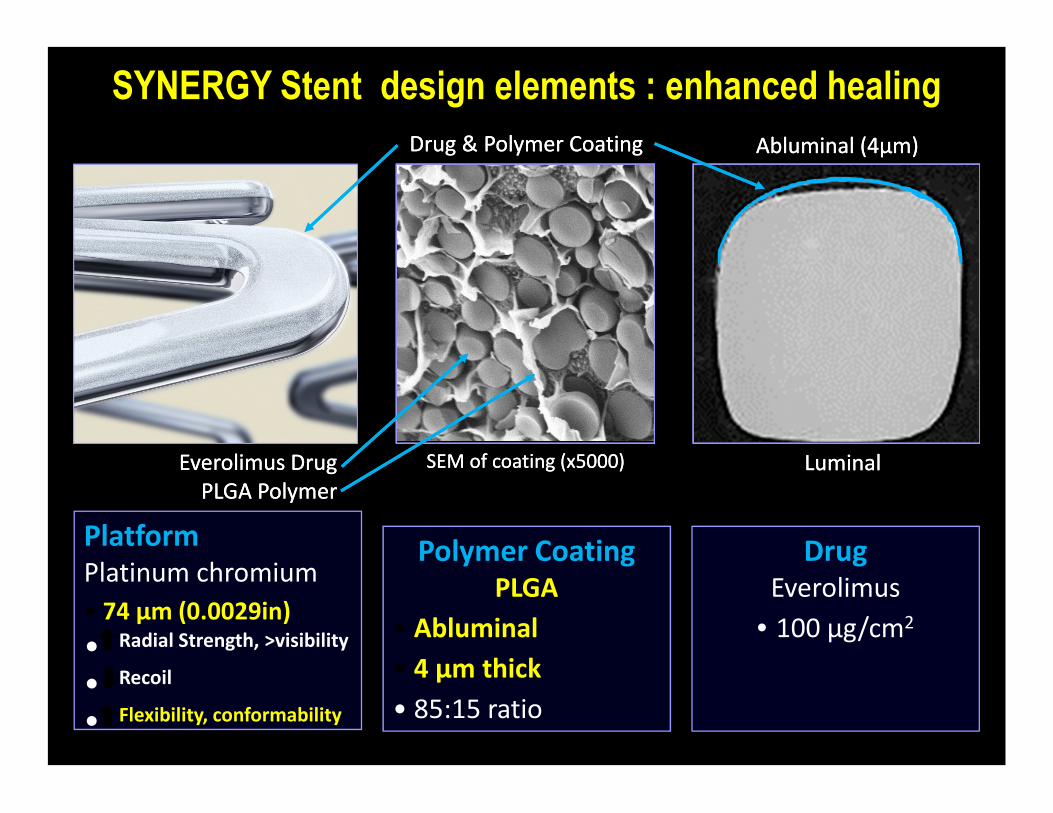
SYNERGY Stent design elements : enhanced healing
Drug& P olym erCoatingDrug& P olym erCoating Ablum inal(4Ablum inal (4μμm )m )
S EM ofcoating(x5000)S EM ofcoating(x5000) L um inalL um inalEverolim usDrugEverolim usDrugP L GA P olym erP L GA P olym er
P latformP latinum chrom ium
• 74 μ m (0.0029in)
• R adialS trength,>visibility
• R ecoil
• Flexibility,conform ability
P olym erCoatingP L GA
• A blum inal
• 4 µm thick
• 85:15ratio
DrugEverolim us
•100 μg/cm 2
Stent Thrombosis at 2 years:EVOLVE II Pivotal Trial for FDA Approval
Definite/Probable : ITT Population
P R O M U SElem entP lus
S ubacute(2-30 d) L ate(30 d– 1 y)
0.8%
(N=6)
Acute (≤1 d)
N=5(2 Definite/3 Probable)
Very L ate(1 – 2 y)
N=1(Def)
S YN ER GY
Elem entP lus
0.4%
(N=3)
P=0.31
N=1(Prob)
N=2(Definite)
N o definiteS T in theS YN ER GY arm after24 hours
Kereiakes etalACC 2016
(PtCr-PVDF-EES)
(n=838
(PLGA-EES)n=846
ST Landmark Analysis: EVOLVE IIDefinite/Probable ST after 24 hours
PROMUS Element Plus vs SYNERGY>24 h Landmark HR 0.16 [0.02, 1.37]
P=0.056
Definite/P
robable
ST
(%) 4
2
3
1d 6 mo 12 mo 24 mo
0.8%
0.1%Definite/P
robable
ST
(%)
0
2
1
‡Day 715 – DefiniteS T w hileon AS A,no P 2Y12 inhibitor
*
IT T ;P atientsw ho didnotreceiveastudy stentw erecensoredat1 year;KM EventR ate;log-rankP values
KereiakesetalACC 2016
1d 6 mo 12 mo 24 mo
Definite or Probable Stent Thrombosis: NetworkMeta-Analysis of 147 Trials / 126,526 Patients
Kang S, et al. JACC CI 2016; doi:10.1016/j.jcin.2016.03.038
(SYNERGY)
SCAAR Registry Definite ST RatesSYNERGY vs Other Current Generation DES
0.6
0.5
0.4
0.3
Cum
ula
tive
rate
of
def
ST
(%)
Cum
ula
tive
rate
of
def
ST
(%)
0.6
0.5
0.4
0.3
All Patients ACS Subset
n-DES*, N=64,429SYNERGY, =7,886
0.2%
0.4%
0.3%
0.5%n-DES*, N=44,845SYNERGY, N=5,294
0.2
0.1
0
0 2 4 6 8 10 12
Cum
ula
tive
rate
of
Time after PCI (months)
adjusted HR: 0.69;95% CI: 0.37-1.37; p=0.29
*n-DES includes:BioM atrix,O rsiro,P rom us Elem entP lus,P rom us P R EM IER ,XienceXpedition,R esolute/R esoluteIntegrity,U ltim aster,&R esoluteO nyx.S arno CR T 2016
Cum
ula
tive
rate
of
adjusted HR: 0.68;95% CI: 0.38-1.19; p=0.17
0 2 4 6 8 10 12
Time after PCI (months)
0.2
0.1
0
No def ST past 6 months for SYNERGY in both groups
0.2%
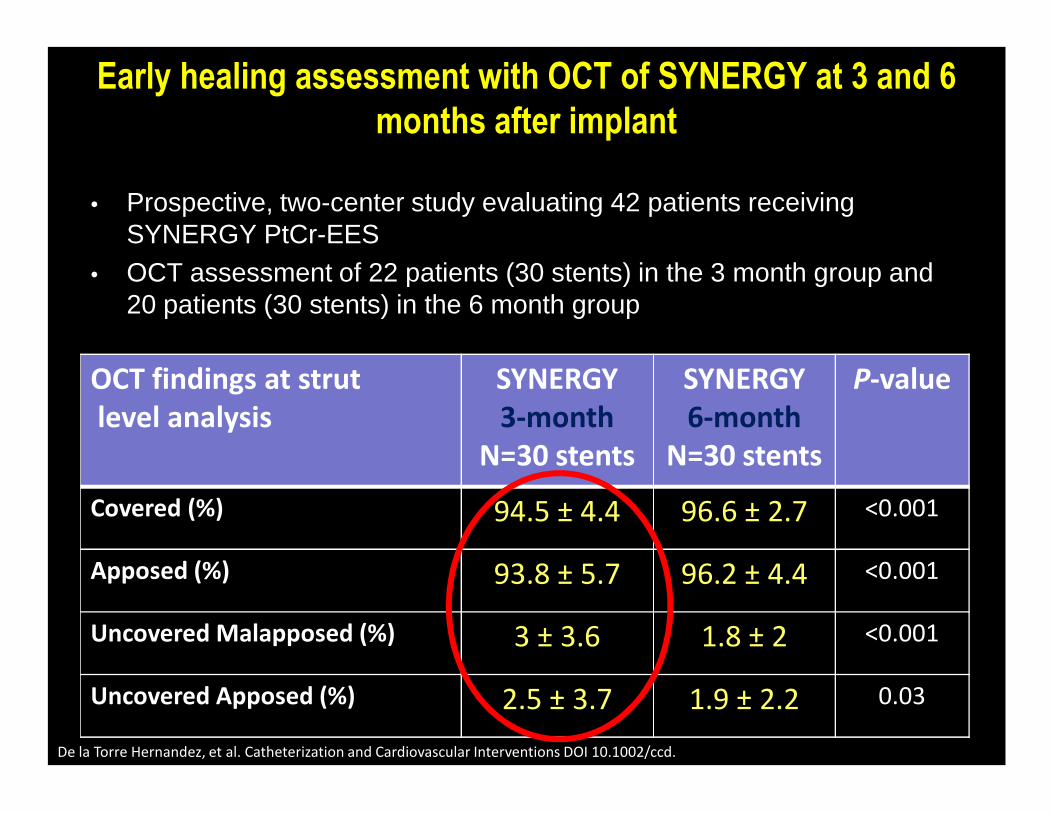
• P ros pec tive, two-c enters tu d y evalu ating42 patients rec eivingS YN ERGY P tC r-EES
• O C T as s es s mentof22 patients (30 s tents )in the 3 monthgrou pand20 patients (30 s tents )in the 6 monthgrou p
Early healing assessment with OCT of SYNERGY at 3 and 6months after implant
CAUTION- Investigational Device. Not available for sale in the USA. SLENDER IDS is CE approved. Indications, contraindications,warnings and instructions for use can be found in the product labeling supplied with each device.
Study will include collection of data on direct stenting, radial accessand procedural efficiencies (independent economic analysis)
1 & 6 month follow-up
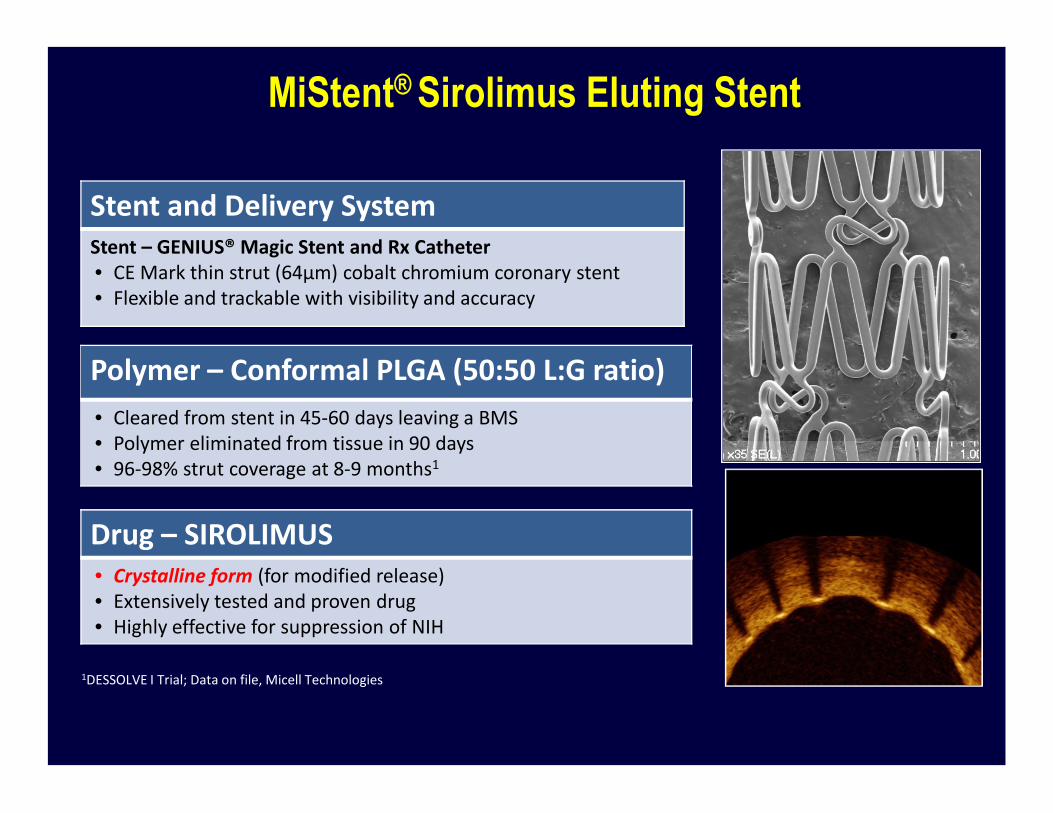
MiStent® Sirolimus Eluting Stent
S tentandDelivery S ystemS tent– GEN IU S ® M agicS tentandR x Catheter• CEM arkthin strut(64µm )cobaltchrom ium coronary stent• Flexibleandtrackablew ithvisibility andaccuracy
P olym er– Conform alP L GA (50:50 L :G ratio)
• Clearedfrom stentin 45-60 days leavingaBM S
Drug– S IR O L IM U S• Crystalline form (form odifiedrelease)• Extensively testedandproven drug• Highly effectiveforsuppression ofN IH
• Clearedfrom stentin 45-60 days leavingaBM S• P olym erelim inatedfrom tissuein 90 days• 96-98% strutcoverageat8-9 m onths1
IllustrativeS EM ofM iS tentDES
S tentP latform
1DES S O L VEIT rial;Dataon file,M icellT echnologies
S tep2 : Fu s ion ofpolymerpartic les into ac onformal, s mooth, well-ad hered film
S tep1 : D ry, prec is e powd erc oatingu s ings u perc ritic alflu id s
26T heM iS tent® S irolim us ElutingAbsorbableP olym erCoronary S tentS ystem (M iS tentS ES )has receivedtheCEM arkbutis notapproved forsaleorusein theU nitedS tates by theFDA.
Carlyle,Edelman et al. Journal of Controlled Release 2012;162:561-7
* ”Drug release complete by 45-60 days”**Arterial concentration -endoluminal mural depot of microcrystals 6-9 mos
Fractio
nalR
esidu
alDru
g
0.4
0.2
0
**
*
Therapeutic Tissue Levels Through 9 Months
300
400
500
600
700
Art
eria
lSir
olim
us
(ng
/mg
)
Art
eria
lSir
olim
us(n
g/m
g)
0 . 0 0
0 . 50
1 . 0 0
1 . 50
2 . 0 0
2 . 50
3. 0 0
3. 50
Lansky A. CRT 2014
0
100
200
300
0 50 100 150 200 250 300 350 400
Art
eria
lSir
olim
us
(ng
/mg
)
Days after Implantation
0 . 0 01 8 0 230 2 8 0 330 38 0
GLP Studies in Porcine Coronary Model: Pharmacokinetic Study N=8, averaged results
180-365 day levels
Days after Implantation
DifferentialDrugDistributionU niqueM echanism ofA ctionDistributesDrugBroadly inT issue
•Strut-adherent coatings resultin largepool of drug around area of injury
•Dissociating delivery from the stent strut
‒ An absorbable polym er with crystalline drug thatflows away from the struts
• Highandlow gradients of polymer and drug are eliminated
S
29T heM iS tent® S irolim us ElutingAbsorbableP olym erCoronary S tentS ystem (M iS tentS ES )has receivedtheCEM arkbutis notapproved forsaleorusein theU nitedS tates by theFDA.
Adaptedfrom “T heL inkBetw een P reclinicalT estingandClinicalP erform anceandO utcom es,”presentedatEuroP CR 2015 by Dr.ElazerEdelm an
Carlyle,… T zafririandEdelm an JCR 2012Balakrishnan,T zafriri… andEdelm an Circ2005
BuMA Supreme DES Components
• B are metals tent– A thin (80 µm)CoCr stent d es igned
ford eliverability and d u rability
• B as e layer– A thin (10 0 -20 0 nm)permanentpoly n-
bu tylmethac rylate (PBMA)c oatingbu tylmethac rylate (PBMA)c oatingelectro-grafted (eG) onto CoCr stentto improve ad hes ion ofthe topc oat
• Topc oating– A poly lac tic -c o-glyc olic ac id (PLGA)
biod egrad able c oatingc ontainings irolimu s (~1 . 2 µg/mm 2 ). The P L GA isabsorbed in ~6 weeks withd ru gmeas u rable in the artery for150 d ays .
eGTM + Biodegradable Drug Carrier
bio
degra
dable
coatin
g3.8
-10µ
me
Inte
rdig
itati
BuMA
Mechanical integrity of coating(expand ed in air)
eG
base
laye
r200nm
meta
l0.1
mm
tion
anotherD ES
inmarket1
e G™ bas e layers ec u res ad hes ion ofthe biod egrad able polymermatrix hos tingthed ru g, prevents c rac kingand d elamination u pon expans ion and overtime.
1 JohnO rm istone ta l.Pre nse nta tiona tTC T 2004
PIONEER III TRIAL DESIGN (IDE)Patients with ≤ 3 native coronary artery lesions ≤ 2 m ajor coronary
arteries in RVD of ≥2.25m m to ≤4.00m m , lesion length ≤33m m , %DS
≥50<100.(Chronicstable/unstableanginaor
N S T EM I)
R andom izedcohort(R CT )
1632 patients
U pto110 globalsites(N orthA m erica,EU ,Japan)
BuM A S uprem eN = 1088
A m erica,EU ,Japan)
Everolim uselutingstents(durablepolym er)
X IEN CEfam ily / P rom usElem entfam ily
N = 544
N on-inferioritytrial,globalm ulti-centerP ivotal,singleblind,2:1 random ization
P rim ary endpoint:1 yearT L F(CD,T V-M I,orT L R )at12 m onthFollow -upthrough5yearsDA P T (ASA + clopidogrel, ticlopidine, prasugrel, ticagrelor) ≥ 6 m onths or longer as tolerated
P R IS O N IV: O rsirovs.X ienceforCT O *Clinical(1 Year)andA ngiographic(9 M onths)Endpoints
8.08.0
9.29.2
6.06.0
7.07.0
8.08.0
9.09.0
10.010.0
O rsiroO rsiro XienceXience
P =0.28 P =0.08
n=165 n=165
0.70.70.130.13 0.120.12
2.12.1
4.04.0
0.70.7
0.020.02 0.070.070.00.0
1.01.0
2.02.0
3.03.0
4.04.0
5.05.0
Binary (>50%)Restenosis
CI-TLR In-Segment In-Stent
* > Plaque Burden/Fibro-Calcific Content
StentThrombosis
Teeuwen et. al. TCT 2016 LBCTJACC CI (in press)
P =0.11(N I)
P =0.52(N I)
(MM)
Efficacy and Safety of BP-DES:Conclusions
• Iterationsinm etallicstentplatform com ponents(strutthickness,polym er,drug)canfacilitate/ expeditestentcoverage/ healingandmay reducelateadverseclinicalevents;? shorterDA P T
• BP -DES aredifferentiatedby strutthickness,polym er• BP -DES aredifferentiatedby strutthickness,polym ercom position,distributionandloadasw ellasthetim ecourseforpolym erresorbtion.? U ltra-thinstrutsm ay havelim itations.
• BP -DES w illdem onstrate> rapidandcom pletestentcoverage/healing,low ratesofS T and> easeofdeliverability.T heseplatform sw illbethew orkhorsedevicesofthevery nearfuture.