29
BRAIN ATTACK Understanding and Managing Acute Stroke in the Pre-hospital Setting EMS Education – Stroke Carolyn Walker RN, BN January 2011
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | amie-andrews |
| View: | 215 times |
| Download: | 1 times |
BRAIN ATTACK
Understanding and Managing Acute Stroke
in thePre-hospital Setting
EMS Education – StrokeCarolyn Walker RN, BN
January 2011

What’s New in Prehospital care of Acute Stroke?
Change is Everywhere!
• New approach to EMS delivery in Alberta
• New EMS Provincial Medical Control Protocols

New Approach to EMS delivery in Alberta
• EMS services prior to April 2009•Private, Municipal, Hospital based/Regional
• EMS services since April 2009•Governance and Policy – Alberta Health and Wellness
•Operations and Support – Alberta Health Services
•>550 ambulances in system across Alberta•300 are AHS•250 are owned and operated by approx. 50 contracted services
New EMS Provincial Medical Control Protocols
• Implemented Dec 1, 2010 for both ground and air
• Developed by a provincial committee
• Ensure evidence based practices
• Ensure consistent standards of care throughout Alberta
• Clearly defined clinical treatment pathways
STROKE MANAGEMENT PROTOCOL

EMS = Prehospital careNeurological emergencies
Introduction
Used with permission by Genetech
• Acute Stroke Syndromes
• Acute Ischemic Stroke
• Define stroke
• Describe acute ischemic stroke
• Discuss EMS assessment and management of the suspected stroke patient
• Describe provincial stroke management protocol • Identify requirements for direct transport to the nearest Primary
or Comprehensive Stroke Centre
• Explain the importance of rapid reperfusion
• Describe how reperfusion is achieved
Objectives
• 65 year old female
• Collapsed
• Unable to move right side
• Unable to speak
Case Study

Stroke Syndrome – sudden vascular event leading to focal neurological dysfunction
Hemorrhagic -15% (ICH & SAH )
Ischemic- 85% (Thrombotic & Embolic)
Ischemic Stroke – 65% Transient Ischemic Attack – 20%
- symptoms resolve - no brain cell death - 20-40% of strokes are proceeded by TIA
• “… proficient … recognize, assess, manage, treat, triage, and transport stroke patients” NAEMSP
Define Stroke
Used with permission by National Stroke Association
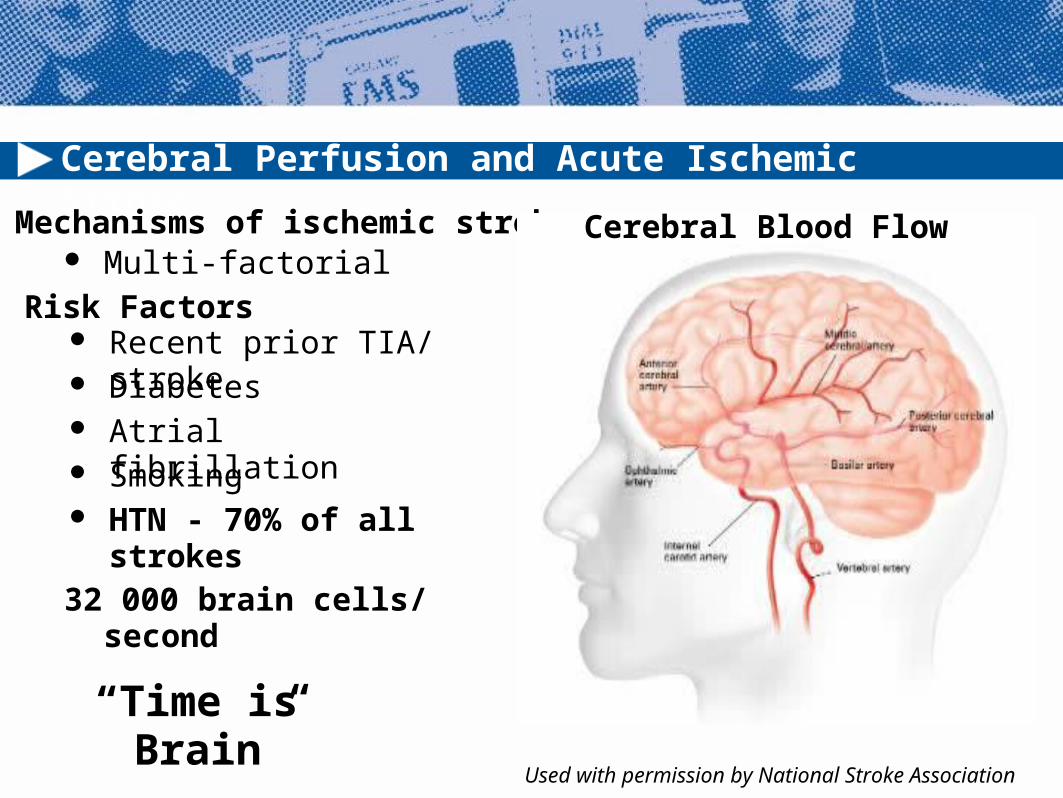
Cerebral Perfusion and Acute Ischemic Stroke
Mechanisms of ischemic stroke Multi-factorial
Risk Factors Recent prior TIA/ stroke Diabetes Atrial fibrillation Smoking HTN - 70% of all strokes
32 000 brain cells/ second
“Time is Brain”
Cerebral Blood Flow
Used with permission by National Stroke Association
EMS Assessment Primary Assessment
o Sudden onset of:• Weakness or numbness on one side
of the body and/or face• Difficulty with speech or understanding
• Double vision or loss of vision
o Focused neurological assessment
Vital signs BGL Medical history
o Last seen normalo Co-morbid diseases – cardiac disease,
diabetes, HTN, dyslipidemiao Risk factors – smoking, obesity, alcoholo Hemorrhage risk – recent trauma, surgery
or bleeding problemso Neuro history – TIA, Stroke, TBI
ECG – Atrial Fibrillation
Used with permission by The City of Calgary EMS

Stroke Management Protocol
When was patient last seen normal?
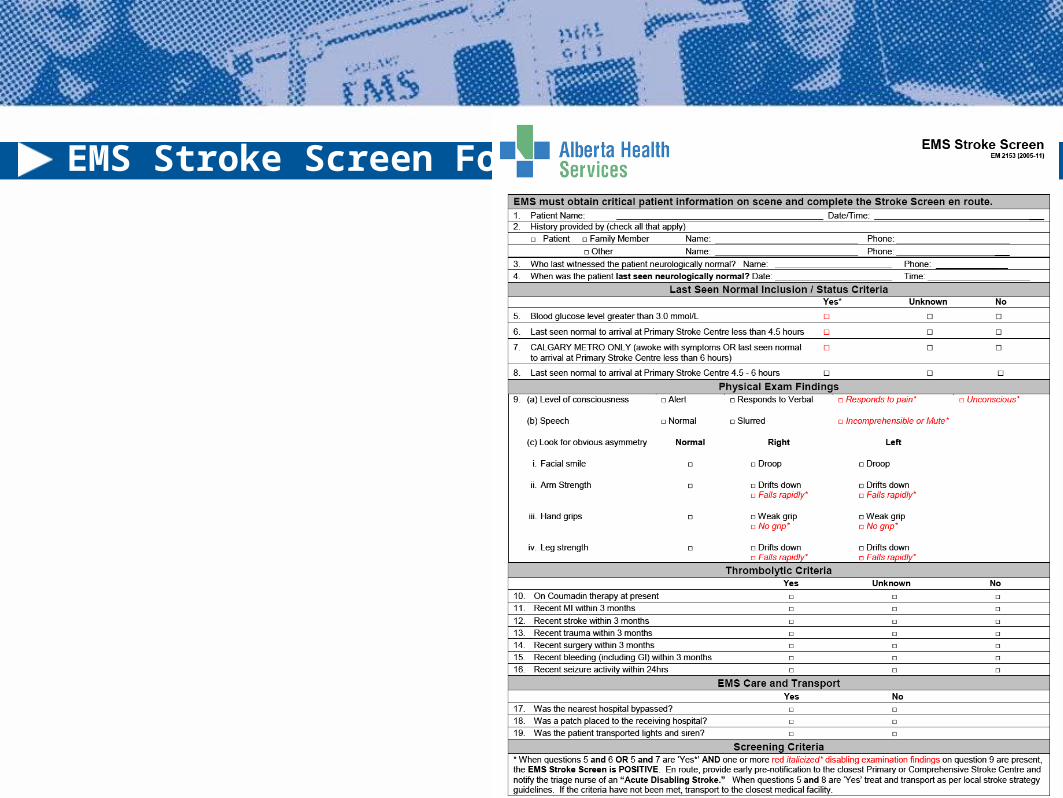
EMS Stroke Screen Form

Stroke Screen Form

EMS Assessment - Neurological
– Level of Consciousnesso A – alerto V – verbalo P – painfulo U – unconscious
Speech impairment - Aphasiaand dysarthia
Facial symetry - facial droop? Arm weakness
o Limb drifto Hemiplegia vs. hemiparesis
Leg weaknesso Limb drift
Vision abnormalities Hand Grip Strength - non-specific
Used with permission by AHS EMS

Stroke Screen Form

Positive Stroke Screen Criteria:
Stroke screen criteria are positive when the following 3 criteria are met:
• Blood glucose > 3.0 mmol/L
• Interval from “last seen normal” to arrival at nearest PSC or CSC is < 4.5 hours (Calgary only- awoke with symptoms OR last seen normal to arrival < 6 hours)
• One or more disabling findings are present

Case Study Assessment
• Aphasic• Hemiparesis - right arm• Weakness - right leg• Facial weakness• Medical History
o Childhood Rheumatic fevero Mitral valve replacement
• Medicationso Previous coumadin o ASA
Used with permission by AHS EMS

Airway management - ETIOxygen – SPO2 > 95%Positioning – supine to 30 degreesIV – minimum1 large bore N/S at 100mL/hr
-no dextrose IV solutions
NO CT Scan= No Thrombolytics= No ASA= No Anti-hypertensives
EMS Treatment
Used with permission The City of Calgary EMS


Access to Tertiary care
• Minimize total ischemic time
• Treatment window for t-PA <4.5 hours
• Scene time < 10 mins
• Rapid transport (with family/ witness if able or
phone # to contact)
• Early Notification
• Prehospital recognition = Time to reperfusion
Used with permission by Calgary EMS
“Time is Brain”

Communication and Transport Decision:
Hyperacute - Metro
- EMS Crew identifies hyperacute stroke, reviews stroke screen form, contacts ADCC (Ambulance Destination Co-ordination Centre)
- ADCC advises on location and sets up information patch to ED
- Awaiting ED notified by crew, clinical details, lytic screen
- ED will contact stroke team to prepare for CT
Bypass Decision:
Rural/Suburban
- Bypass protocol in place, determines closest PSC location
- Contacts ADCC if coming into Edmonton for direction to CSC
- Transport to local PSC or to CSC with pre-notification
- Consultation with Stroke team/Telestroke

Partners in Acute Ischemic Stroke
Primary Stroke Centre (PSC) criteria:
• CT scan availability• Door to CT time less than 20 minutes with a pre-alert• Stroke expertise on-site or available by Telestroke link• r-tPA treatment availability • May not be available 24/7 due to CT/physician availability• Serves surrounding communities in which it is the nearest PSC
Comprehensive Stroke Centre (CSC) criteria:
• CT scan availability• Door to CT time less than 20 minutes with a pre-alert• Stroke team on-site• Neurological expertise on-site• Neurointerventional expertise on-site• Central hub of stroke Neurologist expertise in a telestroke network
Be aware of PSC and CSC in your area

Alberta Stroke Centre Locations
2 Comprehensive Stroke Centres
Calgary - Foothills Medical Centre
Edmonton - University of Alberta Hosp
*Grey Nuns Hosp in Edmonton
14 Primary Stroke Centers

Reperfusion: t-PA (Activase), Mechanical Devices
TIME IS BRAIN!!
Mechanical Thrombectomy Devices:
- MERCI device: Mechanical Embolus Removal in Cerebral Ischemia
- Penumbra device
Alteplase binds to fibrin in a thrombus: - converts plasminogen to plasmin- initiates local fibrinolysis with minimal systemic effects.

National and Provincial Stroke Statistics
Prevalence in Canada3rd leading cause of death14,000 deaths/ year50,000 strokes per year or 1 every 10 minutes300,000 Canadians live with a disability due to stroke
Leading cause of adult disability
Alberta Provincial Stroke Strategy : 2003-2008
• 20% decline in stroke occurrence from 2003/4 -2007/8• 4500 stroke patients admitted to Alberta hospitals• 4000 stroke patients ED visits• EMS is involved in majority of TIAs / Strokes

EMS in Stroke Management
“… proficient … recognize, assess, manage, treat, triage, and transport stroke patients”
NAEMSP
"EMS providers are critical to the management of the acute stroke patient. Early recognition of stroke in-the-field , stabilization and transport to a Primary or Comprehensive Stroke Centre as rapidly as possible are mandatory for acute stroke treatment and good outcomes.“
Dr. Michael Hill, Stroke Neurologist, APSS
Thank you
Alberta Provincial Stroke Strategy
AHS Emergency Medical Services – Calgary ZoneGreg Vogelaar
Calgary Stroke Program: Dr. Michael Hill
Darren KnappParamedic/Quality Assurance StrategistAHS Emergency Medical Services - Edmonton Zone
References1. 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency
cardiovascular care. Part 9: Adult stroke. Circulation. 2005;112:111-120.2. Canadian Stroke Network and the Heart and Stroke Foundation of Canada: Canadian Stroke Strategy.
Canadian Best Practice Recommendations for Stroke Care: 2006. Ottawa, 2006. 3. Canadian best practice recommendations for stroke care (updated 2010) Patrice Lindsay, BScN
PhD, Mark Bayley, MD, Chelsea Hellings, BScH, Michael Hill, MSc MD, Elizabeth Woodbury, BCom MHA, Stephen Phillips, MBBS (Canadian Stroke Strategy Best Practices and Standards Writing Group on behalf of the Canadian Stroke Strategy, a joint initiative of the Canadian Stroke Network and the Heart and Stroke Foundation of Canada*). FINAL v.25 October 21, 2010
4. EMS MANAGEMENT OF ACUTE STROKE– PREHOSPITAL TRIAGE (RESOURCE DOCUMENT TO NAEMSP POSITION STATEMENT)
5. T. J. Crocco, J. C. Grotta, E. C. Jauch, S. E. Kasner, R. U. Kothari, B. R. Larmon, J. L. Saver,M. R. Sayre, S. M. Davis. ABSTRACT. PREHOSPITAL EMERGENCY CARE 2007;11:313–317
6. Demchuk AM., Calgary Stroke Program – Thrombolysis Update 2008 mostly a 3 to 4.5 hours post stroke story. December 2007 – Lecture presentation
7. Kidwell CS, Alger J, Saver JL. Beyond mismatch: Evolving paradigms in imaging the ischemic penumbra with multimodal magnetic resonance imaging. Stroke. 2003; 34: 2729–2735
8. Saver JL. Time is brain--quantified Stroke. 2006 Jan;37(1):263-6. Epub 2005 Dec 8 9. Koeing KL Benefits of Pre-hospital Notification for Stroke Patients. Journal Watch Emergency
Medicine Nov 7, 200810. Alberta Provincial Stroke Strategy: Pre-Hospital Care February 200911. Government of Alberta Health and Wellness: Alberta Health Services: Emergency Medical
Services: Provincial Medical Control Protocols: Adult and Pediatric, December 1, 2010.

















