Breast Cancer Adapted From: SEER’s Training Web Site http://training.seer.cancer.gov.index.html MCR Staff Supported by a Cooperative Agreement between DHSS and the Centers for Disease Control and Prevention (CDC) and a Surveillance Contract between DHSS and MU
Transcript
Breast CancerAdapted From: SEER’s Training Web Sitehttp://training.seer.cancer.gov.index.htmlMCR StaffSupported by a Cooperative Agreement between DHSS and the Centers for Disease Control and Prevention (CDC) and a Surveillance Contract between DHSS and MU
Background Excluding cancers of the skin, breast cancer is
the most common type of cancer in women in the United States. Accounts for one of every three cancer diagnoses.
An estimated 174,480 new invasive cases of breast cancer were expected to occur among women in the United States during 2007.
About 2,030 new male cases of breast cancer were expected in 2007.
Background The incidence of breast cancer rises after age
40. highest incidence (approximately 80% of invasive
cases) occurs in women over age 50. 62,030 new cases of in situ breast cancer were
expected to occur among women during 2007. Approximately 88% will be classified as
ductal carcinoma in situ (DCIS).
Background 2007 - estimated 40,910 deaths (40,460
women, 450 men) Ranks second among cancer deaths in
women. Mortality rates steadily decreased since 1990
Larger decrease in women under 50 Due to combination of earlier detection &
Risk Factors Age—more prevalent in older women Exposure to natural estrogens
First childbirth after age 30 Age at menopause Obesity—estrogens stored in body fat
Affluence High-fat diet Alcohol consumption
Genetics/family history
Reducing Risk Having children at early age Breast feeding Healthy body weight Exercise Anti-estrogens
Symptoms New lump or mass
painless, hard, uneven edges sometimes tender, soft, or rounded
Swelling Skin irritation or dimpling Nipple pain or nipple turning inward Redness or scaliness of the nipple or breast skin Nipple discharge (other than milk) A lump in the underarm area
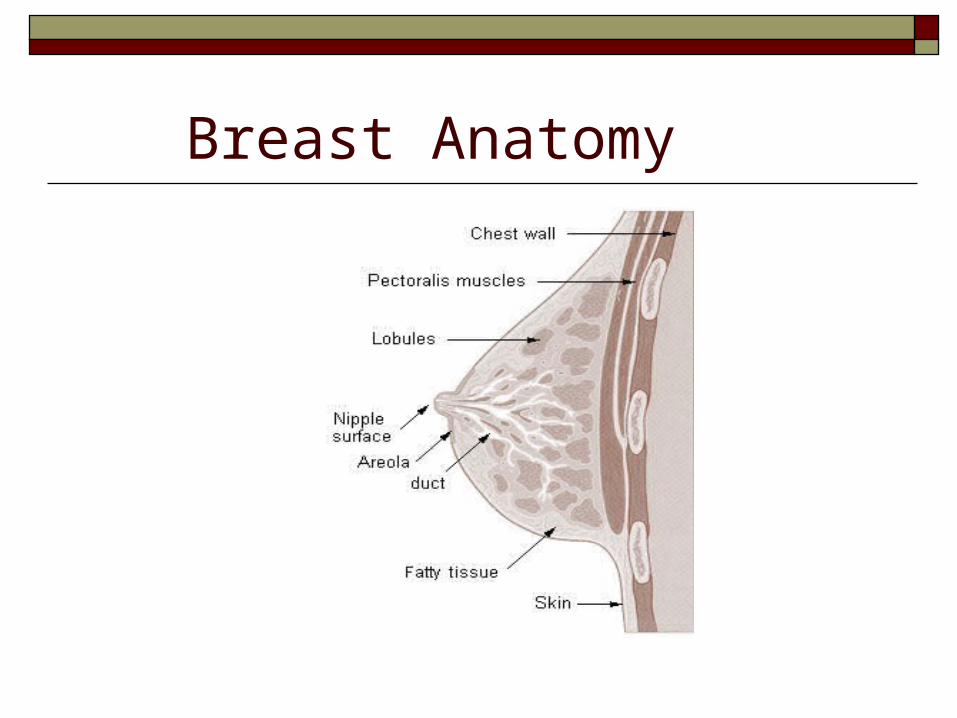
Breast Anatomy
Breast Made up of milk-producing glands Supported and attached to the chest wall by ligaments Rests on pectoralis major muscle No muscle tissue Layer of fat surrounds the glands and extends
throughout breast
Three major hormones affect the breast Estrogen, progesterone, and prolactin
Breast Anatomy
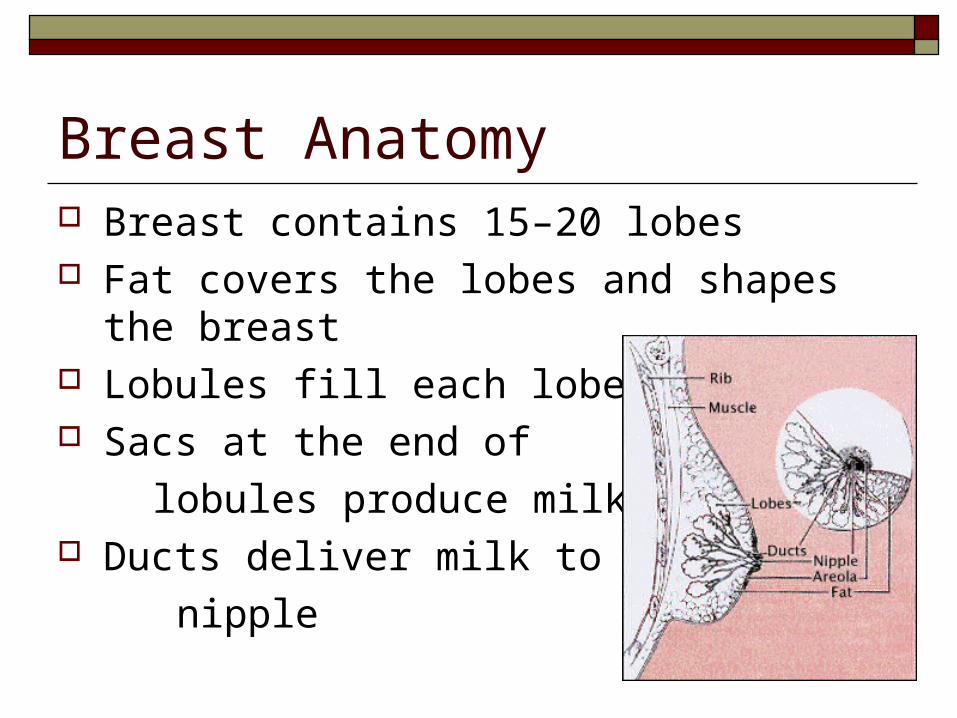
Breast Anatomy Breast contains 15–20 lobes Fat covers the lobes and shapes the breast Lobules fill each lobe Sacs at the end of
lobules produce milk Ducts deliver milk to the
nipple
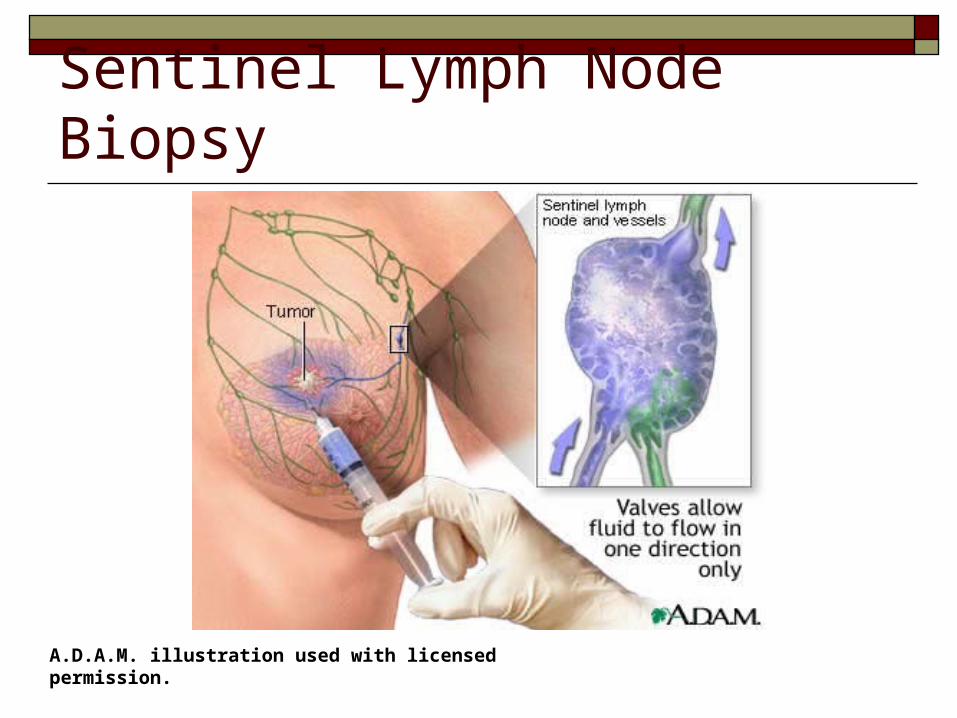
Anatomy – the lymphatic system
Important to know if cancer has spread to the lymph nodes
The more nodes involved, the more likely it is that the cancer may involve other organs.
Affects treatment plan.
Anatomy – the lymphatic system
Most lymphatic vessels in the breast connect to lymph nodes under the arm (axillary)
•Also internal mammary nodes•Supraclavicular or infraclavicular nodes
Types of Breast Cancer The earliest form of the disease is ductal
carcinoma in situ, comprises about 15-20% of all breast cancers and
develops solely in the milk ducts. Invasive ductal carcinoma,
develops from ductal carcinoma in situ, spreads through the duct walls, and invades the breast tissue. Most common – 70-80% of cases
Types of Breast Cancer cont’d. Cancer that begins in the lobes or lobules is
called lobular carcinoma. more likely to be found in both breasts. accounts for 10–15% of invasive breast
cancers. Both ductal and lobular carcinomas can be
either in situ, or self-contained; or infiltrating, meaning penetrating the wall of the duct or lobe and spreading to adjacent tissue.
Types of Breast Cancer cont’d. Less common types of breast cancer include the following:
Inflammatory Medullary carcinoma (originates in central breast tissue) Mucinous carcinoma (invasive; usually occurs in
postmenopausal women) Paget disease of the nipple Phyllodes tumor (tumor with a leaf-like appearance that
extends into the ducts; rarely metastasizes) and Tubular carcinoma (small tumor that is often undetectable
by palpation)
Inflammatory Carcinoma
frequently involves entire breast characterized by reddened skin
and edema caused by tumor spread to lymphatic channels of skin of breast
usually without an underlying palpable mass
Is a clinical diagnosis verified by biopsy of the tumor and overlying skin.
Key words: lymphatic involvement of skin, peau d'orange, orange-peel skin, en cuirasse
Image source: National Cancer Institute
Paget’s disease Crusty tumor of nipple
and areola, which may be associated with underlying tumor of the ducts.
www.sunmed.org/cbesk2.jpg
DCIS In Situ: Abnormal cells that have not escaped the
part of the body where they developed For Breast – abnormal cells in the lining of a milk
duct that have not invaded surrounding breast tissue Appearance of being precancerous when viewed
under a microscope, but No ability to spread as cancer cells would After DCIS, increased risk of invasive breast cancer
from 2 to more than 8 times higher than the risk found in general population
Behavior Invasive (infiltrating)
In situ (15-20% of all breast cancers)
Synonyms for carcinoma in situ: noninfiltrating, intraductal, lobular carcinoma in situ, Stage 0, TIS noninvasive, no stromal involvement, papillary intraductal, papillary non infiltrating, intracystic, lobular neoplasia, lobular noninfiltrating, confined to epithelium,
intraepithelial, intraepidermal, DCIS, LCIS
Grade (differentiation) Assigned by pathologist How close does the bx resemble normal tissue Helps predict prognosis Lower number indicates slower-growing
cancer that is less likely to spread Higher number indicates a faster-growing
cancer that is more likely to spread
Grades Grade 1 (well differentiated) cancers have
relatively normal-looking cells that do not appear to be growing rapidly and are arranged in small tubules.
Grade 2 (moderately differentiated) cancers have features between grades 1 and 3.
Grade 3 (poorly differentiated) cancers, the highest grade, lack normal features and tend to grow and spread more aggressively