Bundle Primary & Community Care Committee 10 February 2020 0 AGENDA 0. Agenda PCPH P Cmt 10.2.20 v4.docx 1 PART 1 - PRELIMINARY MATTERS 1.1 Welcome & Introductions 1.2 Apologies for absence 1.3 Declarations of Interest 1.4 Unconfirmed Minutes of 30 October 2019 1.4 Draft Minutes PCCC 30.10.19 WPJ.doc 1.5 Matters Arising 1.6 Action Log 1.6 Action Log PCPHPC 10 February 2020.docx 2 PART 2 - PRESENTATIONS 3 PART 3 - ITEMS FOR APPROVAL/ENDORSEMENT 3.1 Committee Terms of Reference 3.1 Revised Committee Terms of Reference PCPHPC 10 February 2020.docx 3.2 Appointment of a Vice Chair - Oral 4 PART 4 - GOVERNANCE, PERFORMANCE AND ASSURANCE 4.1 Report of the Director of Primary, Community & Mental Health 4.1 DoPCMH PCPHPC 10 Feb 2020.docx 4.2 Committee Risk Register 4.2 Risk Register extract - PCPHP Committee Feb 2020.doc 4.3 Internal Audit Report - Primary Care Cluster Update 4.3 IA Report PC Clusters PCPHPC 10 February 2020.docx 4.3.1 Primary Care Cluster Plans Final Internal Audit- AC re.pdf 4.4 Wales Audit Office - Review of Primary Care Services 4.4 WAO Report - Review of Primary Care Services PCPPHC 10 February 2020.docx 4.5 Inverse Care Law 4.5 ICL Report PCPHPC 10 February 2020.docx 4.6 Healthy Weights Healthy Wales 4.6 Healthy Weights Healthy Wales PCPHPC 10 Feb 2020.docx 4.7 Population Health 4.7 PCPHP PHM update 10 Feb 2020_vFINAL.docx 4.7.1 Population Health Update PCPHPC 10 February 2020.docx 4.7.2 Population Health in Cwm Taf Morgannwg PCPHPC 10 February 2020.docx 4.8 Influenza Programme Report 4.8 Influenza Update PCPH&PC 10 February 2020.docx 4.9 Out of Hours Update 4.9 OOH Progress Report PCPH&PC 10 February 2020.docx 5 PART 5 - OTHER MATTERS 5.1 Primary & Community Care IMTP Quarter 3 5.1 IMTP monitoring report PCPHPC 10 February 2020.docx 5.2 Any other urgent business 5.2 Primary Care Milestones 5.2 Delivery Milestones for Primary Care Report PCPHP Feb 2020.docx 5.2.1 Annex 1 Delivery Milestones 19-20 Progress Report Jan 2020.docx 5.2.2 Annex 2 - Letter to Chairs and Vice Chairs of Local Health Boards.pdf
Transcript
Bundle Primary & Community Care Committee 10 February 2020
0 AGENDA0. Agenda PCPH P Cmt 10.2.20 v4.docx
1 PART 1 - PRELIMINARY MATTERS1.1 Welcome & Introductions1.2 Apologies for absence1.3 Declarations of Interest1.4 Unconfirmed Minutes of 30 October 2019
1.4 Draft Minutes PCCC 30.10.19 WPJ.doc
1.5 Matters Arising1.6 Action Log
1.6 Action Log PCPHPC 10 February 2020.docx
2 PART 2 - PRESENTATIONS3 PART 3 - ITEMS FOR APPROVAL/ENDORSEMENT3.1 Committee Terms of Reference
3.1 Revised Committee Terms of Reference PCPHPC 10 February 2020.docx
3.2 Appointment of a Vice Chair - Oral4 PART 4 - GOVERNANCE, PERFORMANCE AND ASSURANCE4.1 Report of the Director of Primary, Community & Mental Health
4.3 Internal Audit Report - Primary Care Cluster Update4.3 IA Report PC Clusters PCPHPC 10 February 2020.docx
4.3.1 Primary Care Cluster Plans Final Internal Audit- AC re.pdf
4.4 Wales Audit Office - Review of Primary Care Services4.4 WAO Report - Review of Primary Care Services PCPPHC 10 February 2020.docx
4.5 Inverse Care Law4.5 ICL Report PCPHPC 10 February 2020.docx
4.6 Healthy Weights Healthy Wales4.6 Healthy Weights Healthy Wales PCPHPC 10 Feb 2020.docx
4.7 Population Health4.7 PCPHP PHM update 10 Feb 2020_vFINAL.docx
4.7.1 Population Health Update PCPHPC 10 February 2020.docx
4.7.2 Population Health in Cwm Taf Morgannwg PCPHPC 10 February 2020.docx
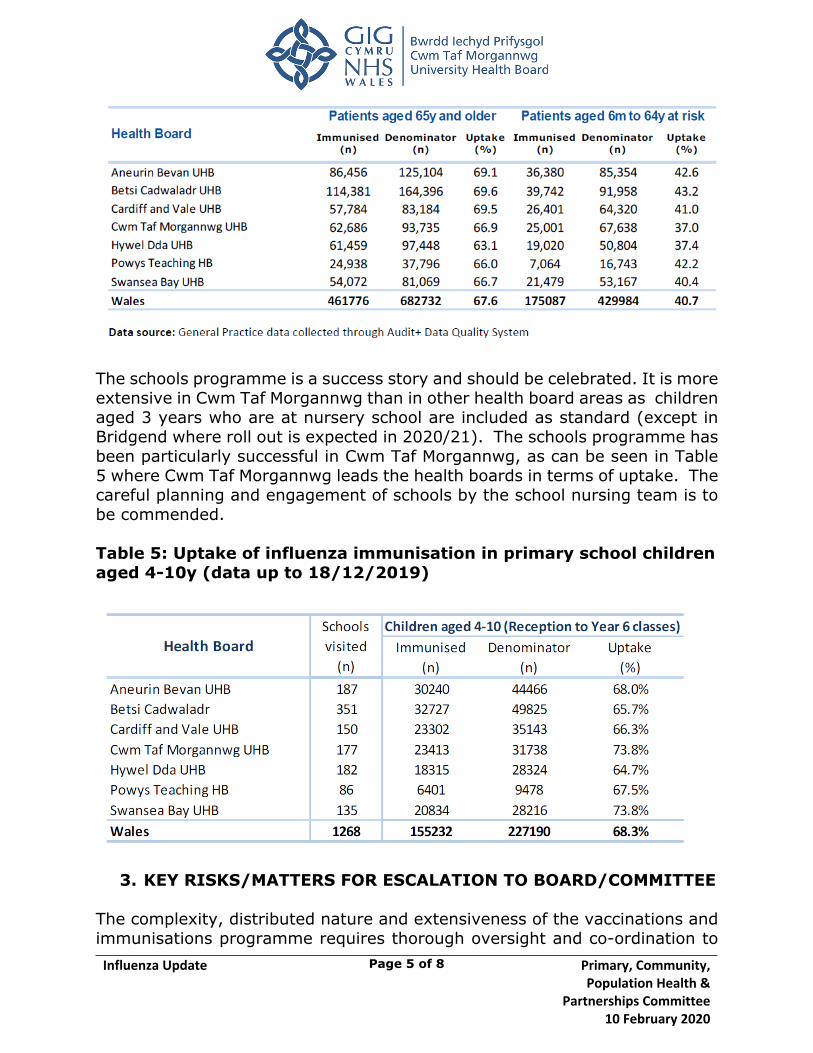
4.8 Influenza Programme Report4.8 Influenza Update PCPH&PC 10 February 2020.docx
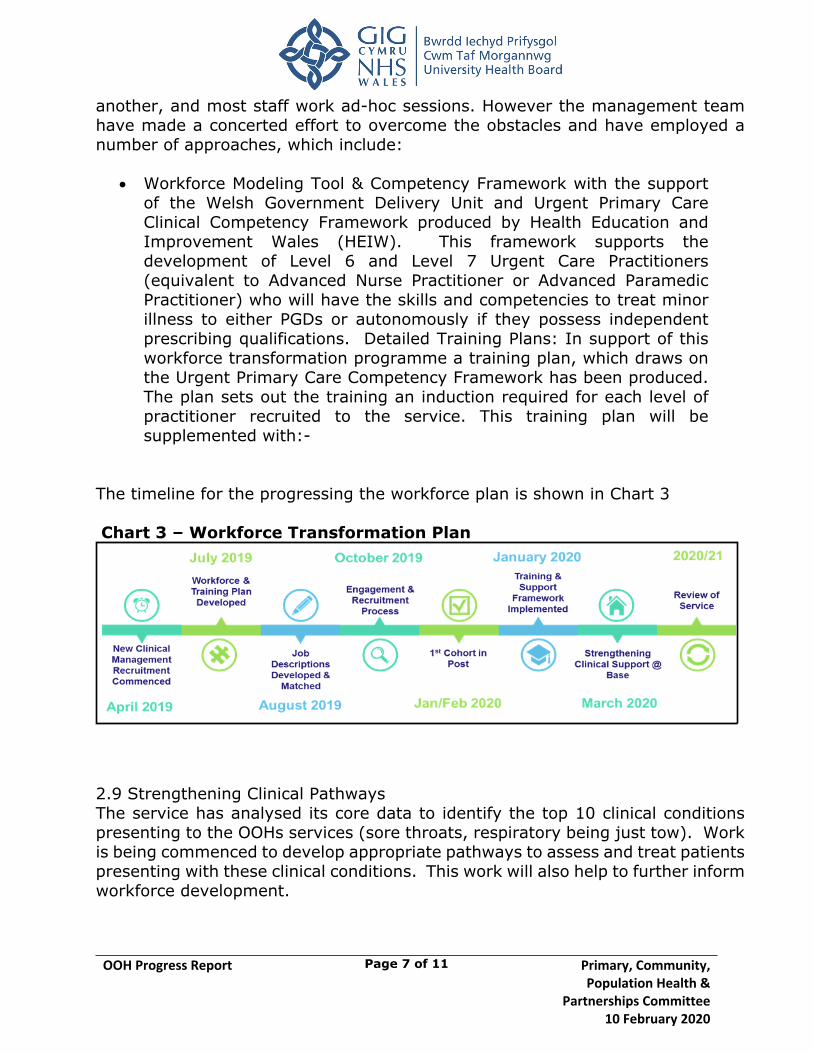
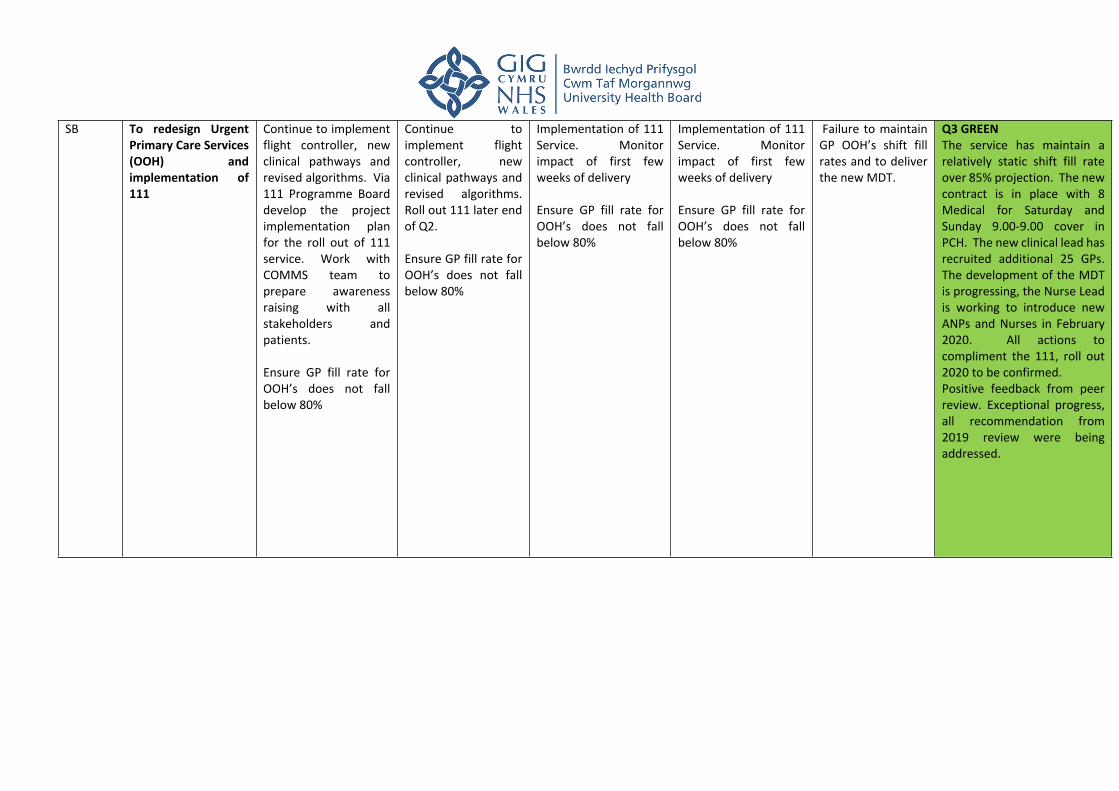
4.9 Out of Hours Update4.9 OOH Progress Report PCPH&PC 10 February 2020.docx
5 PART 5 - OTHER MATTERS5.1 Primary & Community Care IMTP Quarter 3
5.1 IMTP monitoring report PCPHPC 10 February 2020.docx
5.2 Any other urgent business5.2 Primary Care Milestones
5.2 Delivery Milestones for Primary Care Report PCPHP Feb 2020.docx
5.2.1 Annex 1 Delivery Milestones 19-20 Progress Report Jan 2020.docx
5.2.2 Annex 2 - Letter to Chairs and Vice Chairs of Local Health Boards.pdf
5.3 Date of Next Meeting5.3 National Primary Care Board Update
5.3 NPCB Communique December 2019.docx
5.3.1 Appendix 1 - Strategic Programme Update5.3.1 Strategic Programme Update for NPCB PCPHPC 10 February 2020.docx
6 PART 6 - OTHER MATTERS6.1 Comittee Highlight Report
6.1 Committe Highlight Report v1 - inc. guidance notes.docx
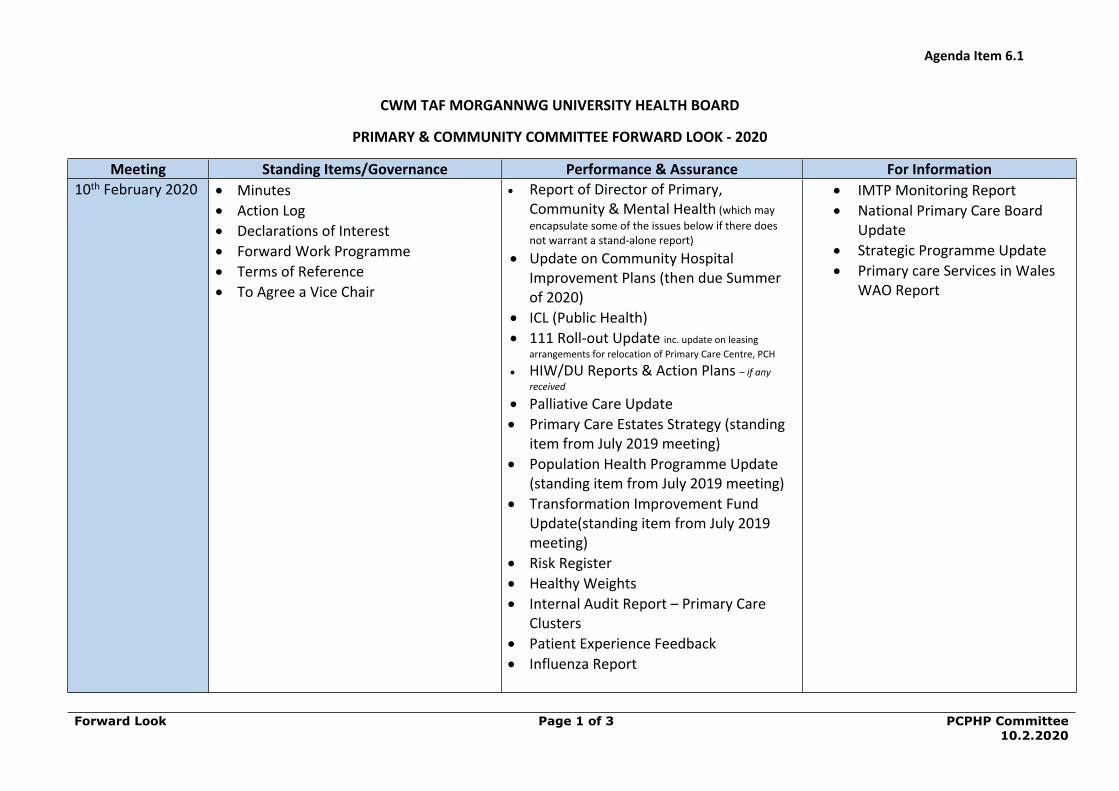
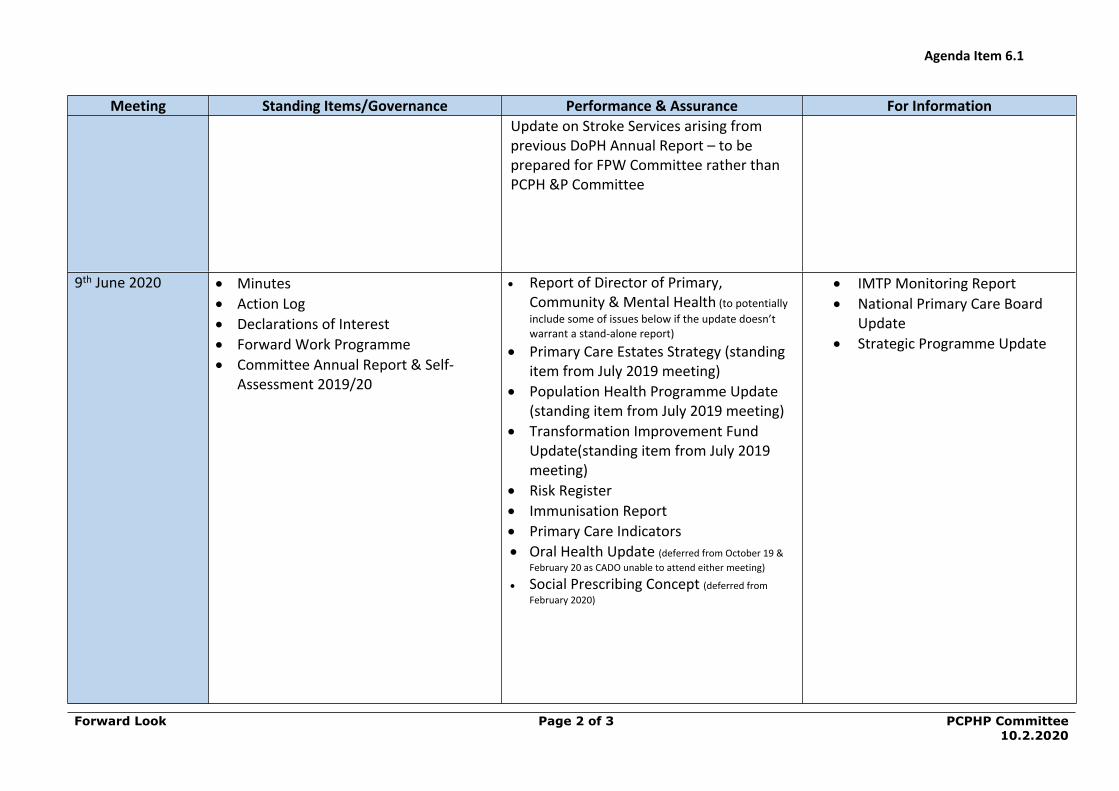
6.2 Forward Look6.2 Forward Look PCPHPC 10 February 2020.docx
6.3 Any Other Urgent Business
0 AGENDA
1 0. Agenda PCPH P Cmt 10.2.20 v4.docx
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEEMonday 10 February
Training Room 10, Royal Glamorgan HospitalCommencing at 09.30 am
AGENDALead / Attachment
PART 1 - PRELIMINARY MATTERS
1.1 Welcome and Introductions Chair / Oral
1.2 Apologies for Absence Chair / Oral
1.3 Declaration of Interests Chair / Oral
1.4 Unconfirmed Minutes of the meeting of the Primary Care Committee held on 30 October 2019
Chair Attachment
1.5 Matters Arising Chair / Oral
1.6 Action Log Chair Attachment
PART 2 – PRESENTATIONSNilPART 3 - ITEMS FOR APPROVAL / ENDORSEMENT3.1 Committee Terms of Reference Chair
Attachment
3.2 Appointment of a Vice Chair ChairOral
PART 4 - GOVERNANCE, PERFORMANCE AND ASSURANCE
4.1 Report of the Director of Primary, Community and Mental Health
Director of Primary, Community & Mental Health
Attachment
4.2 Committee Risk Register Director of Primary, Community & Mental Health
Attachment
4.3 Internal Audit Report – Primary Care Cluster Update Head of Primary CareAttachment
4.4 Wales Audit Office Report – Review of Primary Care Services
Director of Primary, Community & Mental Health
Attachment
4.5
4.6
Inverse Care Law Report
Healthy Weights Report
Director of Public Health
AttachmentDirector of Public Health
Attachment
4.7 Population Health Updates Director of Public Health Attachments
4.8 Influenza Programme Report Director of Public HealthAttachment
4.9 Out of Hours Update Director of Primary, Community & Mental Health
Attachment
PART 5 - FOR INFORMATION (Items will only to be discussed if raised with the Chair in advance of the meeting)
5.1 Primary & Community Care - IMTP Quarter 3 Review Directorate Manager, Community Services
Attachment
5.2 Primary Care Milestones Director of Primary, Community & Mental Health
Attachment5.3 National Primary Care Board Update
5.3.1 Strategic Programme Update
Director of Primary, Community & Mental Health Attachments
PART 6 – OTHER MATTERS
6.1 Committee Highlight Report ChairAttachment
6.2 Forward Look Chair Attachment
6.2 Any other urgent business Chair / Oral
Date of Next Meeting: 9 June 2020 – 1.00 pm (YMH)
7 October 2020 – 1.00 pm (YMH)
1.4 Unconfirmed Minutes of 30 October 2019
1 1.4 Draft Minutes PCCC 30.10.19 WPJ.doc
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 1 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
CWM TAF MORGANNWG UNIVERSITY HEALTH BOARD
MINUTES OF THE MEETING OF THE PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE HELD ON
30 OCTOBER 2019 IN SEMINAR ROOMS 1&2, MULTI-PROFESSIONAL EDUCATION CENTRE (MPEC), PRINCESS OF
WALES HOSPITAL, BRIDGEND
PRESENT:Maria K Thomas Vice Chair of the Health Board (Chair)Nicola MilliganDilys Jouvenat
Independent Member Independent Member
James Hehir Independent Member
IN ATTENDANCE:Alan Lawrie Director Primary, Community &
Mental HealthKelechi Nnoaham - Director of Public HealthRuth Treharne
Greg Dix
Kevin ThomasJayne HowardSuzanne Scott-ThomasGareth JordanSarah Bradley
Gwenan RobertsEmma WaltersDavid Jenkins
Director of Planning & Performance
Director of Nursing, Midwifery and Patient Services
Local Medical Committee Community Pharmacy Wales Head of Medicines Management Locality Clinical Manager Locality Manager/Head of Primary
Care Head of Corporate Services Secretariat Independent Advisor to Health
Board Chair
PCCC/19/060 WELCOME & INTRODUCTIONS Maria Thomas welcomed everyone to the meeting, and referenced the new name of the Committee. Members were advised that the Terms of Reference being revised to be brought back to the next meeting.
David Jenkins was given a warm welcome. Members were advised that the Chair had been having discussions with David Jenkins on the scrutiny and assurance that needs to be undertaken moving forward.
PCCC/19/061 APOLOGIES FOR ABSENCEApologies were RECEIVED from Keiron Montague, Nick Lyons, Anne Phillimore, Hywel Daniel, Paul Jones, Ian Jones, Steve Webster, Ian Jones, Stuart Hackwell, Sara Thomas, Georgina Galletly and Wendy Penrhyn-Jones.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 2 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
PCCC/19/062 DECLARATIONS OF INTERESTSThere were no declarations of interests.
PCCC/19/063 MINUTES OF THE PREVIOUS MEETINGThe minutes of the meeting held on 24 July 2019 were RECEIVED and confirmed as an ACCURATE record, subject to the following amendments:
Page 6, paragraph 6, 5th line – typographical error – should have read “Lymphoedema”.
PCCC/19/064 MATTERS ARISINGPCCC/19/043 - Maria Thomas advised Members that the Committee’s Terms of Reference (TOR) were due to be revised to reflect the fact its remit had been broadened. The Terms of Reference would be brought to the next meeting for consideration prior to being referred to the Board for final approval.
PCCC/19/065 ACTION LOGMembers RECEIVED and discussed the action log and NOTED that:
19/027 – Stroke Annual Report. Kelechi Nnoaham noted that this was not on the agenda. It was agreed that this be added to the agenda for the next meeting.
18/067 – Risk Register (Anticoagulation) - Sarah advised that discussions had been held and it had been agreed that this would be processed via the Directorate Clinical Business Meeting. Work was currently being undertaken to replicate the model in the Royal Glamorgan Hospital. Members AGREED for this item to be removed from the action log.
19/047 – GP sustainability - Alan Lawrie advised that his report provided an update on this issue.
050 – Improvement Plans Ysbyty Cwm Cynon and Ysbyty Cwm Rhondda - Alan Lawrie informed Members that an update would be brought to the February 2020 meeting with any issues requiring escalation being referred to the Quality & Safety Committee.
19/052 – Delivery Unit Ophthalmic Diagnostic Treatment Centre - Alan Lawrie advised Members that this work was being undertaken via the wider programme of work currently being rolled-out in Ophthalmology and that once completed an update would be brought back to the Committee.
18/051 – Transformation Fund Implementation Plan – Alan Lawrie undertook to provide an update for the February 2020 meeting.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 3 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
PCCC/19/066 PRESENTATIONSMembers NOTED that there were no presentations today, however consideration would be given to how patient experience could be reported upon at future meetings and issue needed to be captured in the revised terms of reference (TOR) for the committee.
PCCC/19/067 COMMITTEE CHAIR’S REPORT The Chair informed members that no specific Chair’s report would be presented to future meetings.
ITEMS FOR APPROVAL/ENDORSEMENT
PCCC/19/068 PRIMARY & COMMUNITY CARE COMMITTEE FINAL SELF-ASSESSMENTMembers RECEIVED the final version of the report which was presented by Gwenan Roberts. Members NOTED that the scope of the Committee had been broadened since the assessment had been undertaken and hence the work required to revise the TOR.
Members NOTED that discussions on the membership were being undertaken to review Independent Member membership and local authority representation.
Members were advised that further training was planned for the Board as a whole, as well as training for staff with regard to report writing with a view to ensuring that Independent Members were provided with the information they required.
Kelechi Nnoaham sought clarification on section 1 of the Terms of Reference, where the Committee would be known as the Primary, Community, Population Health and Partnerships Committee. It was confirmed that the ‘()’ around Population Health were an error and would be amended.
Members RESOLVED to:
ENDORSED the report for Health Board approval.
PCCC/19/069 ORGANISATIONAL RISK REGISTERMembers RECEIVED the Organisational Risk Register report, presented by Gwenan Roberts.
Members NOTED that following on from the Board Development Sessions, the Director of Governance/Board Secretary was reviewing the Risk Register, and would be meeting with Executive Directors to review each of their risks. The Board had agreed to receive the risk
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 4 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
register at each of its public Board meetings, and the Audit Committee would be undertaking scrutiny of all the risks on behalf of the Board.
Members NOTED that currently two risks had been assigned to the Committee, namely, “Primary Care Workforce – recruitment and sustainability” and “Failure to continue to provide GP out-of-hours services as currently configured”. Members were advised that the Director of Workforce & Organisational Development was reviewing all risks in relation to workforce.
Nicola Milligan referred to page five, first bullet point in the report, and queried whether it was necessary for the reference to “adequate” to be there. It was confirmed that all risk descriptions were currently under review in order to separate ‘risks’ from ‘issues’.
Ruth Treharne informed the members that if was determined that the Transformation Programme was a corporate risk, this would be included on the Risk Register.
Alan Lawrie stated that a review of the level of risk in respect of out-of-hours services was planned and an update would be provided at the February 2020 meeting.
Kevin Thomas queried whether the Primary Care Workforce risk was reflective of the existing picture or the position going forward. Sarah Bradley responded that it covered both. Greg Dix stated that the calculation could only be made on existing circumstances not anticipated positions. Sarah Bradley stated that to date, there had not been any sustainability applications.
David Jenkins advised that although the Register was being reviewed there was a need to consider whether there were truly only two risks relevant to this Committee particularly in light of its extended remit.
Alan Lawrie advised that he chaired the monthly Clinical Business meetings, and the Directorate risk register was a standing item.
Members RESOLVED to:
NOTE the report and the current risks assigned to the Committee;
AGREE that risk scoring should reflect the actual position rather than an anticipated position.
NOTE that following the planned review any new items be added to the Risk Register
NOTED that an update on the level of risk in respect of GP Out-of-Hours services would be provided at the next meeting.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 5 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
GOVERNANCE, PERFORMANCE AND ASSURANCE
PCCC/19/070 REPORT OF THE DIRECTOR OF PRIMARY, COMMUNITY AND MENTAL HEALTHMembers RECEIVED the report which was presented by Alan Lawrie.
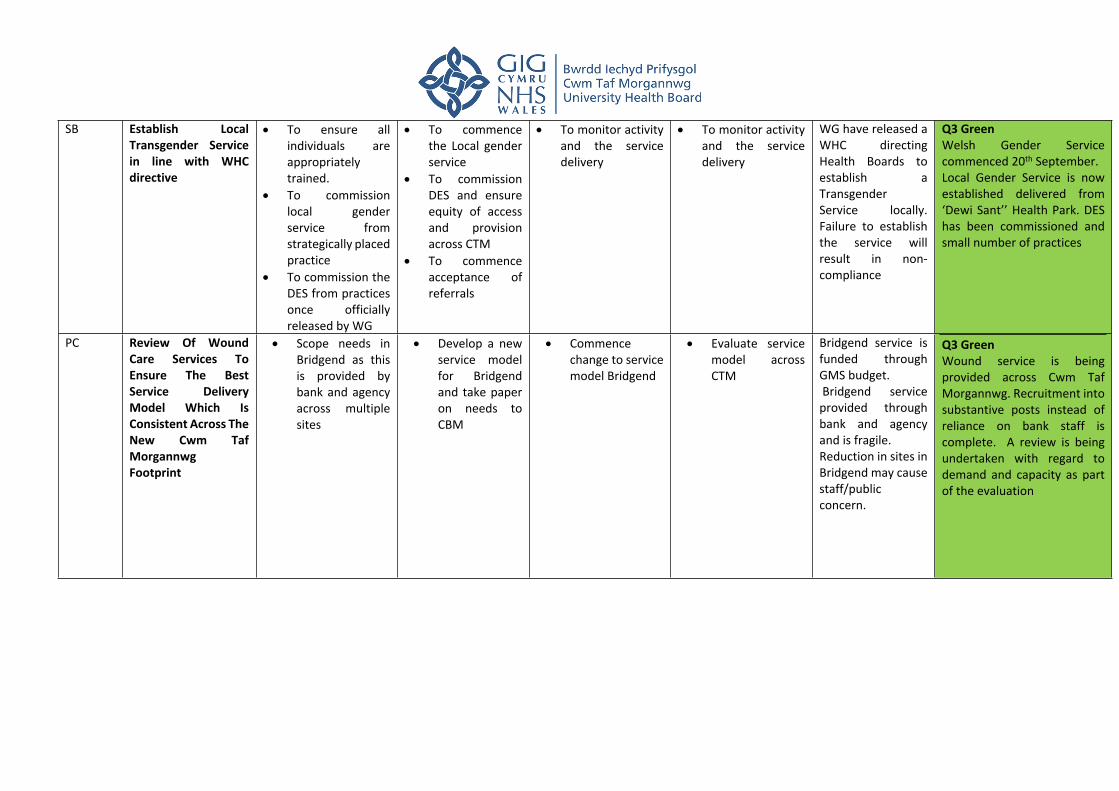
Y Bwthyn Members NOTED that the new MacMillan Unit had been operational since 20 September 2019 at six beds which would be increasing to eight once the work relating to the link corridor was completed.
Maesteg HospitalMembers were advised that the Health Board inherited the site on the 1st April 2019, as part of the boundary change transition arrangements. Members NOTED that the former Abertawe Bro Morgannwg University Health Board (ABMUHB) had commenced consultation on the closure of the Day Unit but that its future was under consideration with the possibility of it being developed into a Health Park.
SunnysideMembers NOTED that this facility had also be part of the transition arrangements and its configuration was under review. Members AGREED to receive further updates on the activity of both Maesteg Hospital and Sunnyside at future meetings.
GP Out-of-Hours (OOH)Members NOTED that a full report would be provided to the February 2020 meeting of the Committee.
Members were advised that a new Clinical Lead, Harry Hunt, had been appointed and had managed to recruit ten new GPs into the service for improved coverage at weekends.
Members NOTED that Andrea Dorrington had been appointed as Senior Nurse for urgent Primary Care and a number of events had been held for nurses looking to work within the service.
Members were advised that the Welsh Ambulance Services Trust (WAST) would be attending the Quality & Safety Committee meeting the following week to discuss the pressures upon the Emergency Departments. The Chair advised members that any issues of service performance would be a matter for the Finance, Performance and Workforce Committee.
Members NOTED that the plans were in place to roll-out the 111 service within CTM by March 2020.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 6 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Porth Farm SurgeryMembers NOTED that the surgery would be closing on 31 December 2019 due to the retirement of GPs. Communications had been challenging, but a managed process was in place, with letters having been sent out to all patients asking for their preferred GP.
Members were advised that there were a number of practices in Aberdare were looking to merge.
Members NOTED that Internal Audit had been asked to review primary care cluster plans which had received a reasonable assurance rating. The Chair advised that the Audit Committee had asked for the report to be referred for information.
Lymphoedema ServiceMembers were advised that the report had been received by the Quality and Safety Committee regarding risks relating to the service. The Chair queried whether there was any assurance that could be provided to the Quality & Safety Committee with regard to waiting times reduction and service delivery. Alan Lawrie confirmed that he would prepare a report in that regard. Members AGREED to refer back to Quality & Safety Committee.
Dental UpdateMembers NOTED the update which was provided in the report. Members NOTED that the Royal Glamorgan Hospital would shortly be able to provide paediatric general anaesthetic.
Members RESOLVED to: NOTE the report NOTE that a report regarding the Lymphoedema service
performance would be submitted to the Quality & Safety Committee
PCCC/19/071 CLUSTER UPDATE Members RECEIVED a report on Cynon North and South locality Clusters presented by Sarah Bradley.
Members were advised that the approach to the cluster plans was slightly different but many of the themes were common.
The Chair advised that the report needed to be more explicit regarding activity and outcomes, however there had been some good work undertaken within the cluster. Maria Thomas said the Committee needed to be assured that the work being undertaken was benefiting the community. Sarah Bradley confirmed that she would seek
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 7 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
outcomes and analysis in order that this could be included in future reports.
Members NOTED that the GPs were focused on low level mental health, MIND Active Monitoring, and Valley Steps. The Chair expressed an interest in seeing how many patients had accessed the services or support.
Kelechi Nnoaham stated that there was a need to support practices to identify initiatives and for there to be a clear path for evaluation.
Members were advised that this was a Welsh Government directive for practices to develop clusters and cluster plans. It was difficult for the Primary Care team to advise them on what areas to focus on, however they could provide advice and guidance.
Kevin Thomas advised that most things that come up were driven by unmet demand, where there was a patient need for the service.
James Hehir stated that the discussions highlighted that data analysis was showing that there were skills-gaps. Greg Dix advised that universities were really keen to work with CTM on service evaluation, and it was agreed contact information would be shared with Sarah Bradley outside the meeting.
Members NOTED that new services had been introduced into the area and practices were spending all their budgets and, despite being separate entities, they were working well together.
Members discussed the good work being undertaken and suggested that it would be good to look at submitting some abstracts in the Health Service Journal.
Members RESOLVED to NOTE the report.
PCCC/19/072 DELIVERY AGREEMENTS FOR 2019/20
Members RECEIVED a verbal update from Sarah Bradley.
Members NOTED that the funding was £4.382M with an underspend position being reported. Identification of how this could be spent on a non-recurrent basis had been made, with the potential recruitment of pharmacists to support Medicines Management and reviews.
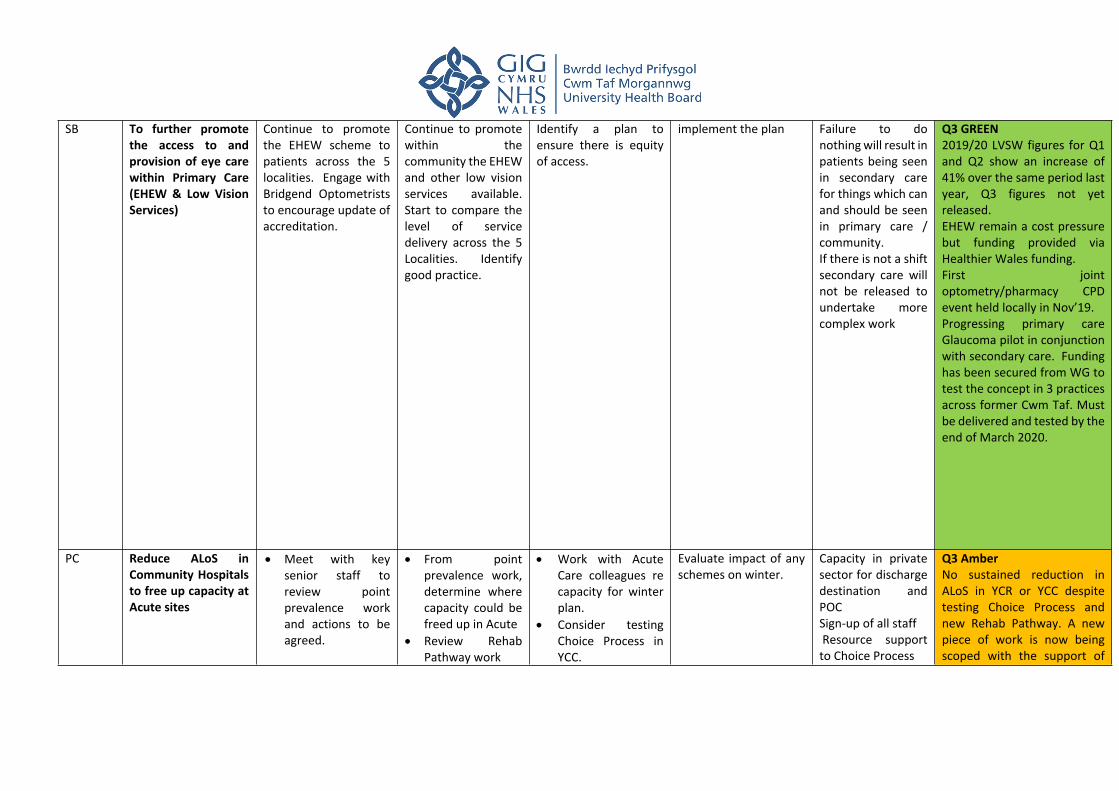
Members were advised that plans had been submitted to Welsh Government to reinvest any underspend on eye health, eye evaluation
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 8 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
and strategic programme plan. Sarah Bradley confirmed there was a tracker in place as regards spending to ensure all available funds were used.
Members NOTED that there was currently one service was being reviewed – the Chronic Obstructive Pulmonary Disease (COPD) in Bridgend.
The Chair queried the sustainability of plans, Sarah Bradley confirmed that these had all been included in the IMTP.
Members RESOLVED to NOTE the report
PCCC/19/073 POPULATION HEALTH PROGRAMME PROGRESS REPORT
Members RECEIVED the report which was presented by Kelechi Nnoaham.
Members were advised that there were three elements to the work: (1) Population Health Management (PHM) which was being piloted in the Rhondda primary care cluster - Phase 1 of the pilot assessed the feasibility of this approach and was currently being evaluated. Members NOTED that Phase 2 was in development and focussed on how this approach would support the new models of care being implemented as part of the Transformation Fund. Members were advised that there was agreement in principal for funding from Welsh Government to implement this approach across other Health Boards following submission of a Business Case from the National Primary Care Board. This was pending more detailed financial profiling.
Members NOTED that with regard to social prescribing, the paper made several recommendations which would realise the potential of social prescribing to positively impact on individual and community health and wellbeing across the Health Board. Members were advised that the recommendations had been endorsed by CTM Regional Partnership Board, Transformation Leadership Group and the Cwm Taf and Bridgend Public Service Boards. The recommendations were being progressed by a CTM multi-agency, cross sector group under leadership of Consultant Public Health.
The Chair thanked Kelechi Nnoaham for the report, and stated that there was a need to triangulate initiatives in relation to transformation and cluster initiatives. In terms of population health, Maria Thomas said the Committee would need to know risks to be identified along with what outcomes were being sought.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 9 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Members RESOLVED to
NOTE the report; ENDORSE the approach; NOTE that further work is to be undertaken
PCCC/19/074 TRANSFORMATION FUND PROGRESS REPORT
Members RECEIVED the report presented by Sarah Bradley.
Members were advised that a significant amount of work had been undertaken, with a governance structure established and regular meetings taking place with stakeholders. Members NOTED there was process on the risks relating to underspends and the various workstreams, describing the model and how the model would work.
Members NOTED that the biggest risk was recruitment, with a need to finalised job descriptions for Mental Health staff, with an implementation date of 1 January 2020 to establish the initial cluster team.
Ruth Treharne welcomed the update, and commented that it would be useful to build in the update into the forward work programme within the overall transformation programme. This had been discussed at the Transforming Leadership Group.
The Chair advised that assurance was required on the delivery, what the risks were, and whether there was any matters that required escalation to the Committee.
The Chair expressed her disappointment that the Committee had not received the financial information on the whole programme. Alan Lawrie suggested that for the February 2020 Committee meeting, the report that was prepared for the Transforming Leadership Group would be considered by this meeting. Ruth Treharne AGREED to circulate the reports from the Transforming Leadership Group meeting to Members.
Maria Thomas thanked Sarah Bradley for the report which it was agreed would be provided in a revised format for the next meeting.
Members RESOLVED to NOTE the report
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 10 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
PCCC/19/075 WELSH GOVERNMENT PRIMARY CARE MILESTONES REPORT
Members RECEIVED the report which was presented by Alan Lawrie.
Members were advised that there was no cover report with this document, and although there were a number of items contained within the strategic programme that needed to be reported on, this was presented to the Committee for information purposes only.
Sarah Bradley informed Members that many of the indicators were currently showing as amber and only partially compliant, with still further work to do on others.
Members RESOLVED to: NOTE the report;
PCCC/19/076 PRIMARY CARE ESTATES STRATEGY PROGRESS REPORT
Members RECEIVED a verbal report from Sarah Bradley.
Members NOTED that a draft outline plan had been developed, and a team member had been identified to take this forward.
Members RESOLVED to NOTE the report;
FOR INFORMATION
PCCC/19/077
PCCC/19/078
PCCC/19/079
PCCC/19/080
IMTP QUARTER 2 REVIEW
Members RECEIVED and NOTED the monitoring report arising from the Primary & Community Care Delivery Plan Integrated Medium Term Plan.
NATIONAL PRIMARY CARE BOARD UPDATE
Members RECEIVED and NOTED the report for information.
STRATEGIC PROGRAMME UPDATE
Members RECEIVED and NOTED the report for information.
AUDITOR GENERAL REPORT – PRIMARY CARE SERVICES IN WALES
Members RECEIVED and NOTED the report for information.
Agenda Item 1.4
Unconfirmed minutes of the Primary and Community Care Committee30 October 2019
Page 11 of 11 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Maria Thomas informed the members that the report had been received by the Audit Committee at their meeting on 28 October 2019 but had not yet been discussed at Management Board.
PCCC/19/081
OTHER MATTERS
TO REVIEW THE FORWARD LOOK FOR 2019/20
Members RECEIVED the forward look NOTING that this was due to be further discussed outside the meeting.
PCCC/19/082 ANY OTHER URGENT BUSINESS
The chair extended a fond farewell to Gwenan Roberts as this was her last meeting. Members NOTED that Gwenan had been a great support to the Committee and extended their good wishes for her new post.
PCCC/19/083 DATES OF 2020 MEETINGS
10 February 2020, 9.30 am 9 June 2020, 1.00 pm 7th October 2020, 1.00 pm
SIGNED …………………………………………………….MARIA THOMAS, CHAIR
DATE ……………………………………………………
1.6 Action Log
1 1.6 Action Log PCPHPC 10 February 2020.docx
AGENDA ITEM 1.6
Action Log update from 30.10.19 Page 1 of 5 PCPHP Committee Meeting10 February 2020
PRIMARY AND COMMUNITY CARE COMMITTEE ACTION LOG UPDATE FOR FEBRUARY 2020 MEETING
No MEETINGDATE
SUBJECT KEY ACTIONS/DECISIONS RESPONSIBLE OFFICER
COMPLETED/updated
PCC/19/45 24 July 19
30 October 2019
Organisational Risk Register
Risk rating for 036 (Primary Care Workforce) to be recalculated due to level of risk having diminished to determine if this would be appropriate for retention on the organisational risk register or local risk register. Risk Register scoring to be calculated on the basis of current circumstances for given issues. Consideration being given to whether Transformational Programme/Fund to be included as a new risk.
Update on OOH GP service risks to be reported to February 2020 meeting
Alan Lawrie
On Agenda 10.2.20
To be addressed in the Director of
PC&MH report to Committee 10.2.2020
On Agenda 10.2.20
PCC/19/052 24 July 2019
(Update 30.10.19)
DU Report - Ophthalmic Diagnostic & Treatment Centres
Actions required to address the DU report being taken forward as part of a wider programme of work within the specialty and would be brought back to the Committee upon completion
Alan Lawrie AL to provide oral update at
Committee meeting
10.2.2020.
AGENDA ITEM 1.6
Action Log update from 30.10.19 Page 2 of 5 PCPHP Committee Meeting10 February 2020
No MEETINGDATE
SUBJECT KEY ACTIONS/DECISIONS RESPONSIBLE OFFICER
COMPLETED/updated
PCCC/19/023 3 April 2019
Oral Health Update on dental contracts Alan Lawrie Update originally due to October
2019 meeting but Colette Bridgeman
(Chief Dental Officer) unable
attend. Also unable to attend
Committee meeting 10.2.2020
Matter deferred to June 2020 pending
discussions between Dir of PC & MH and CADO
PCCC/18/070
PCCC/19/030
10 October 2018) 3 April 2019
Inverse Care Law
Cardiovascular health check programme – receive evaluation report (with SAIL analysis).Next update - April 2020
Kelechi Nnoaham
On Agenda 10.2.2020
PCCC/19/027 3 April 2019
DPH Annual Report – Stroke
Agreed to receive an update on the work being undertaken in six months.
Kelechi Nnoaham
Update to be provided to FPW
Committee in place of PCPH & P Committee
PCC/19/50 24 July 2019
Improvement Plans YCC & YCR Hospitals
Update report to be prepared for consideration in six months-time.
Paul Crank On Agenda in DPC&MH report
10.2.2020
PCC/19/53 24 July 2019
HIW reports and action plans –
Regulator Reports and associated action plans to be brought to the Committee as soon as practical following receipt.
Alan Lawrie None received for February 2020
meeting
AGENDA ITEM 1.6
Action Log update from 30.10.19 Page 3 of 5 PCPHP Committee Meeting10 February 2020
No MEETINGDATE
SUBJECT KEY ACTIONS/DECISIONS RESPONSIBLE OFFICER
COMPLETED/updated
PCC/19/042 24 July 2019
Committee - Terms of Reference (TOR)
Endorse the need for further review of existing terms of reference for PCCC including consideration being given to local authority representation
Maria Thomas/Alan
Lawrie
TOR to be reviewed following
broadening of scope of the
Committee – on Agenda 10.2.20
PCC/19/051 24 July 2019
Transformation Fund Implementation Plan
Update reports to be prepared for all future meetings.
Ruth Treharne On Agenda for meeting 10.2.20
and added to Work Programme as Standing Item
PCC/19/054 24 July 2019
Primary Care Implementation Plan & OOH
Update to be brought to the next meeting in regard to issues with OOH Centre - leasing arrangements at PCH.
Sarah Bradley On Agenda for meeting 10.2.20
COMPLETED ITEMS
PCCC/18/068
PCC/19/51
10 October 2018 (also 9th January 2019, 3rd April 2019)
24 July 2019
Cwm Taf Transformation plan
CTM Transformation Plan
Update on financial sustainability and links with the Transformation plan.
Update reports to be prepared for all future meetings
Ana Riley
Alan Lawrie
Due To April 2019 but deferred to July meeting
Added to Forward Work Programme as standing item
PCCC/19/026 3 April 2019
Primary Care Estates Strategy
Draft Primary Care Estates Strategy to be shared with the Committee once the internal processes have been ratified.
Alan Lawrie Added to Future Work Programme as Standing Item
AGENDA ITEM 1.6
Action Log update from 30.10.19 Page 4 of 5 PCPHP Committee Meeting10 February 2020
No MEETINGDATE
SUBJECT KEY ACTIONS/DECISIONS RESPONSIBLE OFFICER
COMPLETED/updated
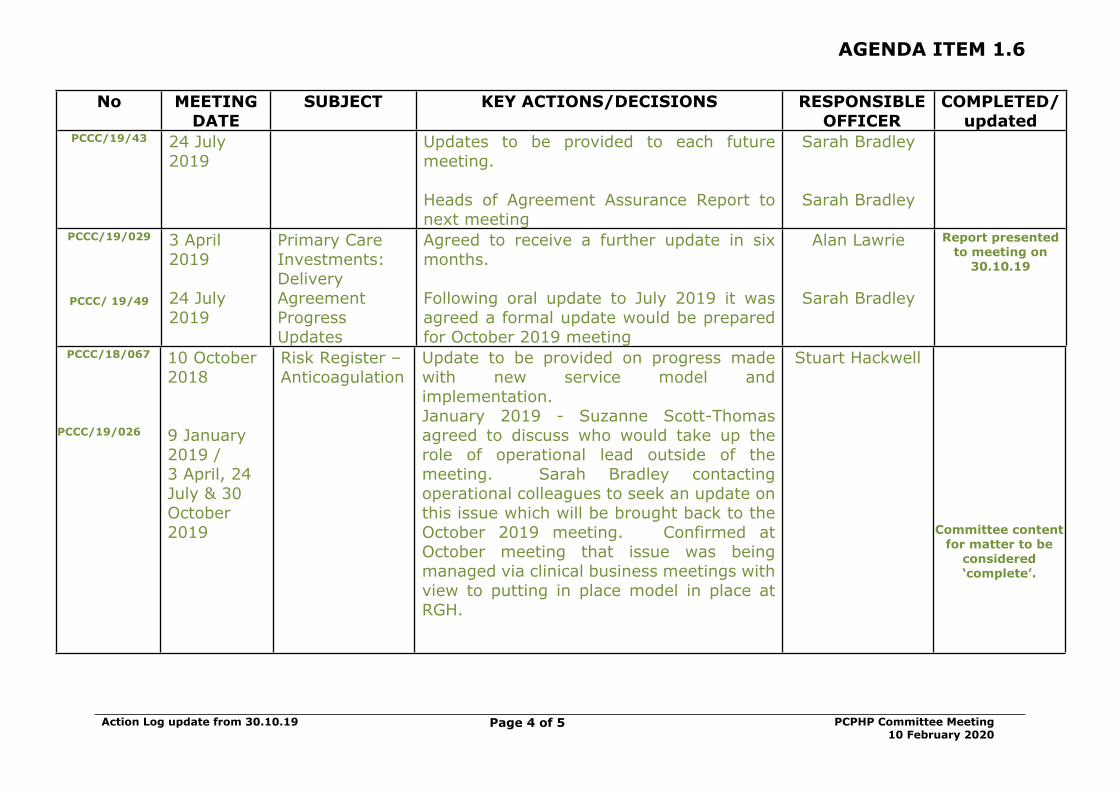
PCCC/19/43 24 July 2019
Updates to be provided to each future meeting.
Heads of Agreement Assurance Report to next meeting
Sarah Bradley
Sarah Bradley
PCCC/19/029
PCCC/ 19/49
3 April 2019
24 July 2019
Primary Care Investments: Delivery Agreement Progress Updates
Agreed to receive a further update in six months.
Following oral update to July 2019 it was agreed a formal update would be prepared for October 2019 meeting
Alan Lawrie
Sarah Bradley
Report presented to meeting on
30.10.19
PCCC/18/067
PCCC/19/026
10 October 2018
9 January 2019 / 3 April, 24 July & 30 October 2019
Risk Register –Anticoagulation
Update to be provided on progress made with new service model and implementation.January 2019 - Suzanne Scott-Thomas agreed to discuss who would take up the role of operational lead outside of the meeting. Sarah Bradley contacting operational colleagues to seek an update on this issue which will be brought back to the October 2019 meeting. Confirmed at October meeting that issue was being managed via clinical business meetings with view to putting in place model in place at RGH.
Stuart Hackwell
Committee content for matter to be
considered ‘complete’.
AGENDA ITEM 1.6
Action Log update from 30.10.19 Page 5 of 5 PCPHP Committee Meeting10 February 2020
CC/19/44 24 July 2019
Committee Draft Annual Report 2018/19
Draft Annual Report approved for submission to Health Board pending further discussion of TOR (including membership arrangements possibly including a local authority representative) and completion of self-assessment (which were to be discussed outside of the meeting)
Wendy Penrhyn-Jones/ Maria Thomas/ Alan
Lawrie
Approved by HB at its meeting 28.11.19
PCC/19/46 24 July 2019
Population Health Programme
Reports to be prepared for each future meeting
Rhondda Primary Care Pilot – Endorsed
Keletchi Nnoaham
Added to Future Work Programme as Standing Item
PCC/19/47 24 July 2019
GP Sustainability Update to be prepared for next meeting Sarah Bradley Update provided at meeting on 30.10.19
PCC/19/037 24 July 2019
Membership arrangements
Consideration to be given to the membership arrangements, including the appointment of another Independent Member
Maria Thomas/ Alan Lawrie
Phil White appointed to the Committee from November 2019
3.1 Committee Terms of Reference
1 3.1 Revised Committee Terms of Reference PCPHPC 10 February 2020.docx
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 1 of 7 PC,PH & P Committee – 10.2.2020
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
REVISED TERMS OF REFERENCE
INTRODUCTION
The Cwm Taf Morgannwg (CTM) University Health Board (UHB) standing orders provide that “The Board may and, where directed by the Welsh Government must, appoint Committees of the UHB either to undertake specific functions on the Board’s behalf or to provide advice and assurance to the Board in the exercise of its functions. The Board’s commitment to openness and transparency in the conduct of all its business extends equally to the work carried out on its behalf by committees”.
The detailed terms of reference and operating arrangements set by the Board in respect of this Committee are set out below.
CONSTITUTION AND PURPOSE
The Board hereby resolves to establish a Committee of the Board to be known as the Primary (Care), Community (Care), Population Health & Partnerships Committee (The Committee).
The Committee is an Independent Member Committee of the Board and has no executive powers, other than those specifically delegated in these Terms of Reference.
The Committee embraces the values of the Health Board and the objectives outlined within its Integrated Medium Term Plan (IMTP) which are:
To improve quality, safety and patient experience. To protect and improve population health. To ensure that the services provided are accessible and
sustainable into the future. To provide strong governance and assurance. To ensure good value based care and treatment for our
patients in line with the resources made available to the Health Board.
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 2 of 7 PC,PH & P Committee – 10.2.2020
SCOPE AND DUTIES
The Committee will: Put the needs of patients, carers and the public at the centre of
all its business. Oversee the development, implementation and monitoring of
the Primary and Community Care Delivery Plan within CTM UHB in line with the agreed direction identified within the Health Board IMTP having due regard for the Clusters IMTP.
Oversee the development, implementation and monitoring of a system-wide approach to wellbeing and population health in CTMUHB.
Ensure that primary and community care is delivered in accordance with the Health & Care Standards for Health Services in Wales.
Act as the main driver for the oversight and scrutiny of all issues relating to Primary Care, Community Care, Population Health and Partnerships on behalf of the Board.
Provide evidence based and timely advice to the Board, based on local need, to assist in discharging its functions and meeting its responsibilities
Specifically:Primary and Community Care Delivery Plan /IMTP
Support officers and clinicians in developing, implementing and monitoring the overarching Primary and Community Care Delivery Plan for the organisation. This work will be aligned and inform the UHB’s three year Integrated medium term plan (IMTP) as well as other key strategies. The GP Cluster Plans IMTPs and the UHB three year Integrated Plan will be key planning vehicles to support this work and set the local direction for services aligned with National Strategy and guidance.
Contractor Professions Advise the Board on progress, risks and key deliverables
associated with all areas of Primary and Community Care, including including for example all contractor professions, estates and out-of-hours services. Committee Members will commit to supporting and promoting the Primary and Community Care agenda and will ensure that these elements of service have a high profile within the organisations agenda.
Setting the Direction Strategic Programme for Primary Care
Provide assurance to the Board that Primary and Community Care services that are delivered and further developed are of a
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 3 of 7 PC,PH & P Committee – 10.2.2020
high quality, sustainable and are in line with Welsh Government strategy and issued primary care milestones. .
Receive reports from the Primary Care and Localities Quality and Safety Group where much of the detailed work will take place. This delivery group in delivering its functions are currently supported by service specific steering groups.
The committee will receive reports about work ongoing at community level aligned to ‘Building a Healthier Wales’ which seeks to prevent ill-health, protect good health and promote better health and wellbeing with a view to inform the case for diverting more resources into prevention and population health management activities. In this regard the Committee will provide advice and assurance in relation to any proposed service reconfigurations.
In accordance with strategic direction confirmed by Welsh Government, the committee will play a key role in driving the shift of resources towards prevention and population health management activities and service reconfigurations toward prevention and population health management.
Reports on progress made regarding the delivery of the CTM Regional Partnership Board and both the Cwm Taf Public Service Board and the Bridgend Public Service Board agendas. In particular, the Committee will receive updates on progress where delivery impacts upon health board services.
AUTHORITY
The Committee is authorised by the Board to:
investigate or have investigated any activity within its Terms of Reference and in performing these duties shall have the right, at all reasonable times, to inspect any books, records or documents of the UHB. It can seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee
obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary, subject to the Board’s budgetary and other requirements
by giving reasonable notice, require the attendance of any of the officers or employees and auditors of the Board at any meeting of the Committee.
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 4 of 7 PC,PH & P Committee – 10.2.2020
Footnotes: Patient Experience related issues are reported through the Quality and Safety Committee Primary & Community care related quality & safety issues are routed through the Quality &
Safety committee with any specific risk or service issues being brought to the attention of the PC,PH & P Committee as necessary via the Committee Referral process.
MEMBERSHIP
Vice Chair (and Chair of the Committee) Four Independent Members
In attendance Director of Primary Community and Mental Health (Lead Director) Director of Public Health Director of Planning & Performance Medical Director Director of Workforce and Organisational Development Director of Finance & Procurement Director of Governance / Board Secretary Head of Nursing, Primary & Community Care Senior representative of finance team Associate Member / Chair of Healthcare Professionals Forum Assistant Director Operations (with responsibility for Primary
Care) Assistant Medical Director with responsibility for Primary Care Consultant in Public Health from local Public Health Team Senior Member of the Local Public Health Wales team Community Health Council Head of Medicines Management Representative of the Local Dental Committee Representative of Community Pharmacy Wales Representative of the Local Medical Committee Representative of the Local Optometry Committee Assistant Director of Therapies and Health Sciences Partnerships representatives TBC
Notwithstanding the requirement to maintain quorum, Directors may on occasion nominate a suitably senior deputy to attend the Committee on their behalf, but should ensure that they are fully aware and briefed on the issues to be discussed.
Members of the Operational Locality Management Team, Population Health or Partnerships Team will attend the meeting as required, agreed in advance by the Chair or the lead Director.
The Chair of the Health Board shall not be a member of the Committee but may choose to attend any meeting as an observer.
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 5 of 7 PC,PH & P Committee – 10.2.2020
Co-opted membersThe Committee may also co-opt additional independent external members from outside the organisation to provide specialist skills, knowledge and experience as appropriate. These key individuals may be asked to attend the committee either for specific agenda items or for an agreed period of time as part of discrete pieces of work. This is to be agreed in advance by the Chair and Lead Director
Support for Committee Members
The Director of Governance / Board Secretary, on behalf of the Committee Chair, shall:
Arrange the provision of advice and support to Committee Members on any aspect related to the conduct of their role, and
Co-ordinate the provision of a programme of training, specific support or organisational development for Committee Members particularly when new.
COMMITTEE MEETINGS
QUORUM A quorum for the meetings shall be a minimum of two three Independent Members (one could include the Chair of the Committee) and at least half of those in attendance.
CHAIRThe Vice Chair of the Health Board shall Chair the Committee.
The Committee will appoint a Vice Chair from the Independent / Associate Board Member representatives on the Committee.
ATTENDANCEThe Director of Governance / Board Secretary will attend meetings periodically, ensuring governance support and advice is available to the Committee Chair.
Other Directors and senior staff of the Health Board will be required to attend when the Committee is discussing areas of risk or operational which are the responsibility of that Director or manager.
SECRETARIATThe Director of Governance / Board Secretary will determine the secretarial support and support arrangements for the Committee.
FREQUENCY OF MEETINGS Meetings shall be held not less than four times a year.
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 6 of 7 PC,PH & P Committee – 10.2.2020
WITHDRAWAL OF INDIVIDUALS IN ATTENDANCEThe Committee may ask any or all of those who normally attend but who are not Members to withdraw to facilitate open and frank discussion of particular matters.
CIRCULATION OF PAPERSThe Lead Director in conjunction with the Board Secretary will ensure that all papers are distributed at least five working days prior to the meeting.
REPORTING AND ASSURANCE ARRANGEMENTS
The Committee Chair shall:
report formally, regularly and on a timely basis to the Board on the Committee’s activities. This includes verbal updates on activity, the submission of committee minutes and written reports.
bring to the Board’s specific attention any significant matters under consideration by the Committee.
ensure appropriate escalation arrangements are in place to alert the UHB Chair, Chief Executive or Chairs of other relevant committees of any urgent/critical matters that may affect the operation and/or reputation of the UHB.
The Committee shall provide a written, annual report to the Board on its work in support of the Annual Governance Statement specifically commenting on the adequacy of the assurance arrangements, the extent to which risk management is comprehensively embedded throughout the organisation, the integration of governance arrangements and the appropriateness of self-assessment activity against relevant standards. The Board may also require the Committee Chair to report upon the activities at public meetings or to community partners and other stakeholders, where this is considered appropriate e.g. where the Committee’s assurance role relates to a joint or shared responsibility.
RELATIONSHIP WITH THE BOARD AND ITS COMMITTEES / GROUPS
PRACTICE
The Director of Governance / Board Secretary, on behalf of the Board, shall oversee a process of rigorous self-assessment and evaluation of the Committee’s performance and operation. A standard agenda must be used as the basis for discussion at each meeting of the Committee.
Minutes prepared following the Primary, Community, Population
Terms of Reference for Primary, Community, Population Health and Partnerships Committee
Page 7 of 7 PC,PH & P Committee – 10.2.2020
Health & Partnerships Committee meetings shall be circulated to members within 7 working days and shall be retained by the Head of Corporate Services as a formal record for a period of seven years.
The Committee Chair and the Director of Primary, Community and Mental Health will meet with their counterparts on the Quality & Safety Committee, Finance & Performance Committee and the Mental Health Act Monitoring Committee on a regular basis.
The Committee, through the Committee Chair and members, shall maximise cohesion and integration across all aspects of governance and assurance through the:
joint planning and co-ordination of Board and Committee business, and
sharing of information, as appropriate.
The Committee shall embed the UHB’s corporate standards, priorities and requirements, e.g. equality and human rights through the conduct of its business.
APPLICABILITY OF STANDING ORDERS TO COMMITTEE BUSINESS
The requirements for the conduct of business as set out in the UHB’s Standing Orders are equally applicable to the operation of the Committee, except in the following areas: Quorum
REVIEW
These Terms of Reference shall be adopted by the Committee after first meeting and subject to review at least on an annual basis thereafter.
Annual review - date of next review is February 2021 however updates may be required following the implementation of operational model arrangements in April 2020.
4.1 Report of the Director of Primary, Community & Mental Health
1 4.1 DoPCMH PCPHPC 10 Feb 2020.docx
AGENDA ITEM
4.1
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
REPORT OF THE DIRECTOR OF PRIMARY, COMMUNITY & MENTAL hEALTH
Date of meeting (10/02/20)
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by Alan Lawrie, Director of Primary Care Community & Mental Health Services
Presented by Alan Lawrie, Director of Primary Care Community & Mental Health Services
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(Insert Name) (DD/MM/YYYY) Choose an item.
ACRONYMSWAORGHCTMUHBABMUHBSLA
Wales Audit OfficeRoyal Glamorgan HospitalCwm Taf Morgannwg University Health BoardAbertawe Bro Morgannwg University Health Board Service Level Agreement
DoPCMH Report Page 2 of 10 Primary, Community, Population Health &
Heath Care Assistant Ysbyty Cwm Cynon Digital Enhanced Communications Technology Information and Communications Technology Ysbyty Cwm RhonddaInfection Prevention & ControlPrince Charles HospitalWelsh Government Full Business CaseExtended Cluster Community Team Stay Well in Your Community Programme Dental Contract Reform Units of Dental ActivityClinical Oral Risk & Need Form
1. SITUATION/BACKGROUND
1.1 The following report has been prepared to update Committee members on a range of issues that are currently live across primary and community care services within Cwm Taf Morgannwg University Health Board (CTMUHB). It is not an exhaustive list, but provides update on issues that have been previously reported to the committee as well as information on matters that committee members may find of interest.
In all cases there is further detail that can be made available to members in addition to a series of visits to services. The main agenda has very specific and detailed reports in regard to the Urgent Primary Care Services and NHS 111 roll-out, as well as papers in regard to recent Wales Audit Office and Internal Audit reviews of services. There is also a substantive item in regard to Primary Care milestones and progress with the deployment of the new teams as part of the Transformation Fund.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 SPECIALIST PALLIATIVE CARE: ROYAL GLAMORGAN HOSPITAL(RGH) SITE
a) The link corridor was completed (internally) on 27 January 2020 with a small amount of work to catch-up on externally due to the wet
DoPCMH Report Page 3 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
weather. Decisions about when to open up the extra two beds which are contingent on the extra Health Care Assistants to cover the nights being appointed will be made by 14 February 2020 through the Executive Team.
b) There is a concern in regard to the lack of mobile phone network in the building and the impact on professionals being able to contact them. This has been raised with to determine a long-term solution. Staff do have access to phones.
c) As part of the inaugural operational workings there is a concern about the timeliness of the out-of-hours cover now being provided from the medical team within Royal Glamorgan Hospital. A meeting has been setup to resolve this.
d) There is one middle grade doctor due to go on maternity leave in February 2020 and a further one in June 2020. An advert for a replacement post to cover both maternity posts is in circulation.
e) Arrangements are being made between CTMUHB and Macmillan in regard to a formal opening which is due to take place in April / May 2020.
2.2 MARIE CURIE SLA
There have been a series of meetings both in-house and with Marie Curie colleagues to consider the two Service Level Agreements in place. Both are for renewal in March 2020. Currently there are different operating models between the former Cwm Taf (CT) and Bridgend and work is underway on alignment. The current contract will be extended for six months only to allow time to work through what is actually needed. The information below gives headlines of both contracts.
Former CWM TAF UHB TOTAL CONTRACT VALUE £156,707
BREAKDOWN OF CONTRACT VALUEClinical Co-ordination (0.5 WTE HCA) = £14,000Nursing Costs = £142, 707Hours Commissioned = 921 per month (11, 052 per annum)Population Size: 300,314
TOTAL CONTRACT VALUE = £ 154, 397
BRIDGEND
BREAKDOWN OF CONTRACT VALUE
DoPCMH Report Page 4 of 10 Primary, Community, Population Health &
There is still a sustained need to provide cohort and/or 1:1 nursing for patients on both sites. At the time of reporting there are 4 cohort patients in Ysbyty Cwm Cynon (YCC) and 8 cohort and 3 x 1:1 patients on site in Ysbyty Cwm Rhondda (YCR). The numbers of these patients change frequently but is lower in recent weeks than it has been for some time. There is now an established focus on reviewing the 1:1 patients and the Senior Nurses on each site are personally supporting this on a daily basis. There are also ongoing discussions with Mental Health colleagues about support from them due to a significant number of these supervised patients having behavior issues which the ward staff find challenging and outside of their usual skill set.
Winter Pressures
The hospitals have been providing an intensive response to the current winter pressures and issues with flow. The Community Hospitals are all represented on the daily 10.30am Conference Call. Daily deep dives are in place and robust escalation of delays to the Local Authority is happening via the Senior Nurses and Deputy/Head of Nursing. Work is also on-going with the site management team at Prince Charles Hospital (PCH) in particular, about the high numbers of patients on the Transfer List. Most colleagues now have an acknowledgment that the list is an inaccurate reflection of those acute patients needing care in YCC/YCR and collaborative work is now taking place to find a sustainable solution. At present this remains a challenge but will be worked through.
In order to support the current level of escalation on the acute sites we have opened all of our Day Rooms (x 8) at YCC and YCR. Patients are risk assessed to be nursed in these rooms due to them not having nurse call bells, oxygen, suction and hand-washing facilities. For a one week trial we have also redirected our Nurse Assessor resource out to the acute and community sites. Their remit is to intensively support the
DoPCMH Report Page 5 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Discharge Liaison Nurses in terms of identifying and facilitating discharges. We are also in the process of securing the support of an ex-LA colleague who will work one day per week to support the high number of patients currently in the “choice” process.
Nursing
The current level of Registered Nurse vacant posts across the community hospital sites has reduced since last report. There are now 5.0 whole time equivalent (wte) Band 5 posts in YCR and 3.0 wte at YCC. As always, the sites are proactively advertising all our nursing vacancies and the Senior Nurses are very positively promoting the three sites to prospective candidates. The two vacancies for Ward Manager posts at YCR have been filled and both staff are on site in their roles.
2.4 MAESTEG HOSPITAL
Development of the Site
What we have done so far:A Stakeholder Event was arranged at Maesteg Hospital. There were a number of areas of care provision that were highlighted as having room for improvement and a summary of the discussions were captured around the key themes. Output from this event is being put together, with a plan back to the March 2020 Project Board.
Discussions are ongoing with colleagues from Acute Services in the Princess of Wales Hospital to look at increasing outpatient capacity at Maesteg Hospital. In addition, we are looking at capital plans to upgrade the existing X-ray facility and to install an automated booking system for Outpatients.
We have made some other changes. For example, a new hospital welcome sign is in situ, procurement of pressure relieving bedside chairs and comfortable visitor chairs. There is new flooring in the main Outpatient Department and new wheelchairs. Ward corridor flooring is to be replaced over the coming months. Way finding signage is being reviewed and there is an ongoing, dementia friendly decoration programme in place. Moreover, a first addition newsletter has also been developed and circulated, highlighting what has been achieved so far.
DoPCMH Report Page 6 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
A full site risk assessment was undertaken (both internally and externally) and security has been enhanced. That is, new digilocks installed and brighter exterior lighting.
What we will be doing over the next few months:We will be liaising with colleagues from the Local Authority on arrangements for updating the local community around the hospital developments, to include the possibility of accessing community transport. We will be looking to introduce a community café at the hospital and allocating room space for voluntary organisations at the hospital. By the end of January 2020, the Directorate will be updating the Health Board’s Communication Team and the Community Health Council on progress. There will also be the first meeting of the Hospital Project Steering Group Meeting
Current Environmental Challenges:As there is asbestos in the hospital roof space, the Directorate in conjunction with senior colleagues from Estates and Capital are working through a removal plan. This will require an area on Llynfi Ward to be decanted into the vacated day Hospital space. It is estimated that this will be around April 2020 and could take around three months to complete,
In addition, recent water sampling in the hospital has produced failed results from the outlets in the old Day Hospital area. All affected outlets (taps, pipes, etc.) have now been changed. The area has been resampled with results expected in around two to three weeks’ time. The area remains closed until then IPC, Estates and Facilities to discuss the findings and agree responsibilities going forward.
2.5 DISTRICT NURSING PRINCIPLES (DNP)
The all-Wales Interim District Nursing Principles submission was made in December 2019 , this was the first CTMUHB submission to include the Bridgend Networks which were previously aligned to the former Abertawe Bro Morgannwg University Health Board (ABMUHB). Initial informal feedback from Welsh Government (WG) has been positive as we have made further advances against those specific principles where our compliance was lower. A more detailed paper on the principles and our adherence along with the future roll-out of the Neighbourhood Nursing Pilot will be brought to the next committee.
DoPCMH Report Page 7 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
2.6 LYMPHOEDEMA SERVICE
The national recommendations have been accepted by CTMUHB and these are progressing alongside the development of the local Business Case. Phase 1 staff are now in post and undertaking induction and training. The team are initially focused on addressing the current backlog of patients who have been awaiting specialist assessment. A further update will be provided through the Quality and Safety Committee in March 2020 reviewing the waiting times and their improvement
There is a Service Level Agreement (SLA) with Swansea Bay University Health Board (SBUHB) for the provision of service to Bridgend at a cost of £238,394. This service will fully transfer back to CTM as of April 2021. This provides a year to develop the CTM element into a sustainable service and work through the workforce and recruitment issues to establish a new team to take on Bridgend.
2.7 PRIMARY CARE
Estates
a) Mountain Ash
The Ground Breaking Ceremony took place on the 6 December 2019 and contractors are on site. Network Rail are still insisting on further site investigations but Apollo have decided to continue at risk unless an enforcement notice is imposed. Meeting taking place with the practices through January and February 2020 to discuss practice merger plans.
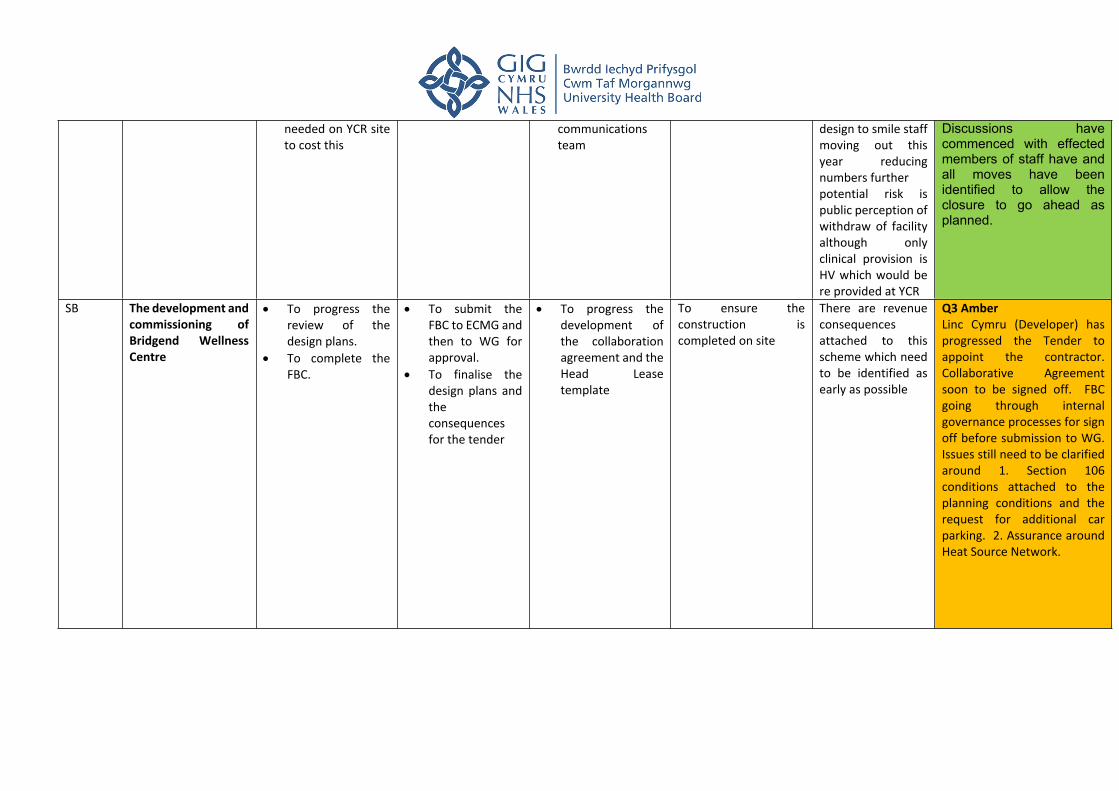
b) Bridgend Health and Wellness Centre
The Full Business Case (FBC) has been finalised and was approved by Health Board on 30 January 2020 for submission to Welsh Government. The collaboration agreement is being finalised with Linc will need to be signed prior to a contract start go at the same time.
c) Pontnewydd
The expansion work is completed and the additional patients from Porth Farm have been accommodated. The revised lease for the building between Assura and the GP Partner has been completed. Porth Farm Surgery (Rhondda Surgery) is now officially closed and all patients have
DoPCMH Report Page 8 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
been safely registered at alternative practices. No significant issues were raised during the process. The Process was managed extremely well by the primary care team and neighboring practices.
d) Estates Strategy
The work on this is progressing, the five facet survey is essential prior to any consideration by Welsh Government. This will be commissioned prior to the end of March 2020 which will allow completion of the estates strategy and programme plan in quarter 1 of 2020/21 although this is a challenging timescale.
2.8 TRANSFORMATION PLANS
Extended Cluster Community Team (ECCT) for the Stay Well in Your Community Programme (SWIYC) progressing well.
Outstanding posts for recruitment are mental health practitioners and pharmacists
Workshops held with each of the clusters to agree how the multidisciplinary team will function.
The order of implementation will be as follows:
Week commencing:- 24 February 2020 Rhondda 16 March 2020 Taff Ely 6 April 2020 Merthyr & Cynon
South* *Cynon North is already live.
3 Ambitions for the Bridgend Localities
Recruiting the following for each cluster Network teams: Occupational Therapy, Physiotherapy, Speech and Language Therapy, Community Psychiatric Nursing, Pharmacy Techs and Care Navigators and Therapy Techs.
For the single access point to district nursing, plans to move to 8.00 am – 8.00 pm Monday to Friday in January 2020, and will operate over seven days from April.
Care navigation – all posts have been recruited to.
DoPCMH Report Page 9 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
2.9 DENTAL
Dental Contract ReformWelsh Government are expecting Health Boards to have at least 50% of dental practices participating in Dental Contract Reform by the end of 2020/21. For CTM that would be 29 practices so another 8 practices would need to be approved during the next financial year. Then the intention is that all dental practices would be participating by the end of 2021/22 but a number of practices do not wish to change how they are currently working so this may need legislative changes to ‘force’ practices to participate.
Currently there are 21 dental practices (36%) in CTM participating in the Dental Contract Reform (DCR) programme, (i.e. 19 practices at Stage 1 & 2 practices in Stage 2).
Stage 1 is when 10% of annual contracted Units of Dental Activity (UDAs) are reduced in return for practices completing an Assessment of Clinical Oral Risk & Need form (ACORN) annually for each patient plus applying fluoride varnish to at least 50% of children and to adults with decay. Patient access rates must be maintained & must not reduce more than 5%. Practices still have to achieve a minimum of 95% of the reduced UDAs to avoid repayment to the Health Board. If all Stage
3. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Link to Main Strategic Objective To Improve Quality, Safety & Patient
Experience
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
4. RECOMMENDATION
4.1 Members of the Primary, Community, Population Health & Partnerships Committee are asked to:
NOTE the report
4.2 Committee Risk Register
1 4.2 Risk Register extract - PCPHP Committee Feb 2020.doc
Organisational Risk Register Page 1 of 6 Primary, Community, Population Health & Partnerships Committee
10 02 2020
AGENDA ITEM
4.2
Primary, Community, Public Health & Parterships Committee
ORGANISATIONAL RISK REGISTER
Date of meeting (10/02/2020)
FOI Status Open/Public
If closed please indicate reason Choose an item.
Prepared by Wendy Penrhyn-Jones, Head of Corporate Administration
Presented by Wendy Penrhyn-Jones, Head of Corporate Administration
Approving Executive Sponsor Director of Corporate Governance
Report purpose FOR DISCUSSION
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
Received by the Health Board 30/01/2020 ENDORSED FOR APPROVAL
Reviewed at Management Board 16/01/2020 DISCUSSEDReviewed at Audit & Risk Committee 20/02/2020 DISCUSSED
ACRONYMS
1. SITUATION/BACKGROUND
1.1 The purpose of this report is for the Committee to review the organisational risk register entries and discuss those relevant to the remit of the Committee The Organisational Risk Register was last considered by the Management Board on 16 January 2020.
1.2 The Executive Team have made a commitment to reviewing the risks allocated individually following the Board Development session held on Risk Management in August 2019.
Organisational Risk Register Page 2 of 6 Primary, Community, Population Health & Partnerships Committee
10 02 2020
1.3 Changes have been made to the Committee arrangements where the scrutiny of the risk register and risk management will now be undertaken at the Audit and Risk Committee from the Quality and Safety Committee.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 Discussions between the Director of Corporate Governance and lead directors have started to comprehensively review the Organisational Risk Register with an aim for a new approach to be finalised as soon as possible.
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 There are currently two risks being monitored by the Committee in relation to Failure to continue to provide and sustain GP Out-of-Hours Services as currently configured (030) and Recruitment and sustainability of the primary care workforce. (036). The following appendix shows the original scores both of which have since reduced.
4. IMPACT ASSESSMENT
Yes (Please see detail below)Quality/Safety/Patient Experience implications
Aim to mitigate risks to patients and staff
Governance, Leadership and AccountabilityRelated Health and Care standard(s)
All Health and Care Standards are included
No (Include further detail below)Equality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
There is no direct impact on resources as a result of the activity outlined in this report.
Link to Main Strategic Objective To provide strong governance and assurance
Link to Main WBFG Act Objective
Service delivery will be innovative, reflect the principles of prudent health care and promote better value for users
Organisational Risk Register Page 3 of 6 Primary, Community, Population Health & Partnerships Committee
10 02 2020
4.1 RECOMMENDATION
4.2 The Committee is asked to DISCUSS and REVIEW the Organisational Risk Register entries relevant to the Committee as set out in the appendix to this report.
Organisational Risk Register Page 4 of 6 Primary, Community, Population Health & Partnerships Committee
10 02 2020
Strategic Objective
Risk Ref
Description of risk identified
Initial Score
Current Score
Trend(from last report)
Last Reviewed
ScrutinyCommittee
036DPCMH
Primary Care Workforce - Recruitment and sustainability
20 16 November2019
Primary, Community
Population Health and Partnerships
030DPCMH
Failure to continue to provide and sustain GP Out of Hours Services as currently configured.
20 12 January
2020
Primary, Community
Population Health and Partnerships
Organisational Risk Register Page 5 of 6 Primary, Community, Population Health & Partnershi[ps Committee 10th February 2020
Objective: Setting the Direction & Performance & Operational Delivery Director Lead: Director of Primary, Community and Mental Health (DPCMH)Assuring Committee: Primary, Community Population Health and Partnerships Committee
Risk: Failure to continue to provide GP out of hours services as currently configured
Date last reviewed: January 2020
Risk Rating Rationale for current score:(consequence x
likelihood):Initial: 5 x 4 = 20
Current: 5 x 3 = 12Target: 4 x 3 =12Level of Control
=60%Date added to the
risk registerNovember 2014
The Out of Hours team is encouraging GPs to fill shifts. However, many sessions are filled via Locum Agency Doctors, which is
expensive and flexible sessions are offered. However, the fill rate remains variable and is challenging to maintain services. The effect
of the HMRC tax implications is now having an impact.Rationale for target score:
There are ongoing and developing Primary Care recruitment problems (reflecting a National problem). It is becoming increasingly
difficult to secure GP sessions for the GP Out of Hours Service and many sessions especially on the weekend remain unfilled putting
additional demand on both existing A&E departments.
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
Action Lead DeadlineThe out of hours team continuing to work with GPs and other primary care staff, in a flexible way for the best shift fill rates.
DPCMH Ongoing
All Wales approach being progressed to mitigate variability of approaches across NHS Wales Health Boards
Directors of W&OD/ Directors of PC&MH
Ongoing
OOHs services reconfigured and number of centres reduced from 4 to 2 in order to sustain services. An evaluation update considered by the Board in July 2016, agreed to continue with the current service which is scrutinized and monitored by the Primary, Community Population Health and Partnerships Committee.
There continues to be ongoing engagement and discussions with those practitioners currently supporting the revised model.
There continues to be engagement with key stakeholders including the Community Health Council, GPs and patients.
Further options are being considered in order to address ongoing sustainability issues with the current service configuration
Peer review undertaken providing assurance of significant improvement
Regular dialogue with OOHs service and Primary Care Clusters to ensure OOHs cover is strengthened and supported.
DPCMH Ongoing
Assurances (How do we know if the things we are doing are having an impact?)
Gaps in assurance(What additional assurances should we seek?)
Shift fill rates; patient experience surveys The current service model is not sustainable and alternative solutions are required.
Current Risk Rating Additional Comments
Current Risk Rating : 4 x 3 = 12 Lack of an All Wales Approach results in HBs competing with each other on GP sessional pay rates.
Ref No.030
05
10152025
Nov
-18
Dec-
18
Jan-
19
Feb-
19
Mar
-19
Apr-
19
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec-
19
Jan-
20
Trend
Risk Score
Organisational Risk Register Page 6 of 6 Primary, Community, Population Health & Partnershi[ps Committee 10th February 2020
Objective: Setting the Direction & Performance & Operational Delivery Director Lead: Director of Primary, Community and Mental Health (DPCMH)Assuring Committee: Primary, Community Population Health and Partnerships
Risk: Primary Care Workforce – recruitment and sustainability Date last reviewed: November 2019
Risk Rating Rationale for current score:(consequence x
likelihood):Initial: 5 x 4 = 20
Current: 4 x 4 = 16Target: 4 x 3 =12Level of Control
=60%Date added to the
risk registerAugust 2016
An increasing number of practices across the UHB are advertising for GP sessions currently due to (and other staff groups) vacancies.
Rationale for target score:Recruitment to Primary Care for GPs and some other professional
groups across Cwm Taf UHB remains challenging (reflecting a National problem).
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
Action Lead DeadlineDevelopment of the Cluster arrangements maturing, working with Primary Care and localities to develop solutions;
DPCMH Ongoing
The UHB has been successful following submission of bids against non-recurring Primary Care monies;
DPCMH Complete
Where possible the Primary Care Team is working with the practices to find solutions, which include practice mergers; considering where possible directly managing solutions and/or working to recruit on behalf of the practices.
Primary, Community Population Health and Partnerships Committee in place to scrutinise delivery of the IMTP.
Local and National recruitment campaigns progressed, with some reported success. The Board has developed its Strategy for
Primary Care aligned with its Integrated 3 Year Plan and National guidance. This includes milestones for addressing some of the related reported risks.
DPCMH
Ongoing milestones being monitored
Assurances (How do we know if the things we are doing are having an impact?)
Gaps in assurance (What additional assurances should we seek?)
Recruitment and retention data.Current Risk Rating Additional Comments
Current Risk Rating : 4 x 4 = 16
Ref No.036
4.3 Internal Audit Report - Primary Care Cluster Update
1 4.3 IA Report PC Clusters PCPHPC 10 February 2020.docx
AGENDA ITEM
(4.3)
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Internal audit report on primary care cluster plans
Date of meeting 10/02/2020
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by Sarah Bradley, Directorate Manager for Primary Care
Presented by Sarah Bradley, Directorate Manager for Primary Care
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
Audit Committee (28/10/2019) NOTED
ACRONYMS
Internal Audit Report - Primary Care Clusters
Page 2 of 3 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
1. SITUATION/BACKGROUND
1.1 In 2019 Internal Audit undertook a review of Primary Care Cluster Plans, attached in Annex 1, as part of the 2019/20 Internal Audit Plan. The objective of the audit was to evaluate and determine the adequacy of the systems and controls in place in relation to the Health Board’s management of processes in relation to Primary Care cluster plans.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 The Health Board initially had four Primary Care Clusters (Rhondda, Cynon, Merthyr Tydfil and Taff Ely) and in April 2019, it took over the responsibility for the provision of three further clusters in the Bridgend area (Bridgend East, West and North). It is important to note that at the time the audit was undertaken, which were the summer months of 2019, the clusters were still working to their historic arrangements and processes which were in place prior to the boundary change. Alignment of cluster processes had not at that point been addressed as the Health Board was just three or four months into the transition.
2.2 Despite this, the outcome of the evaluation was positive and the key finding was ‘The Board can take reasonable assurance that arrangements to secure governance, risk management and internal control, within those areas under review, are suitably designed and applied effectively. Some matters require management attention in control design or compliance with low to moderate impact on residual risk.
2.3 Areas of good practice were identified and are detailed in the report in section 6, Summary of Audit Findings.
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 Out of 5 recommendations, one was deemed by the auditors to be ‘high’ risk and this related to lack of robust process for the identification of risks at the cluster level because there was no evidence in some clusters of risks being identified. Historically the clusters have always worked well to spend their allocation in a timely manner and to prioritise wisely in line with the ‘rules’. However, the risk was accepted and was addressed by the introduction of: revised ‘terms of reference’ for the cluster meetings; the development and use of ‘risk log’ templates; agreement from the cluster to record risks on Datix; and an agreed process for clusters to report risks into the Primary Care, Quality and Risk Committee.
Internal Audit Report - Primary Care Clusters
Page 3 of 3 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
3.2 The 4 other recommendations were ranked ‘medium’ risks. The committee can be assured that all risks have been addressed by the introduction of the ‘terms of reference’, introduction of a set agenda for cluster meetings which includes ‘IMTP’ and evidencing attendance and membership of other multi-professionals.
4. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Governance, Leadership and AccountabilityRelated Health and Care
standard(s) If more than one Healthcare Standard applies please list below:
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
There is no direct impact on resources as a result of the activity outlined in this report.
Link to Main Strategic Objective To provide strong governance and
assurance
Link to Main WBFG Act Objective
Service delivery will be innovative, reflect the principles of prudent health care and promote better value for users
5. RECOMMENDATION
5.1 The Committee is asked to:5.2 NOTE the positive report findings and the actions taken to comply with
the recommendations.
1 4.3.1 Primary Care Cluster Plans Final Internal Audit- AC re.pdf
Primary Care Cluster Plans
Internal Audit Report
2019/20
Cwm Taf Morgannwg University Health Board
October 2019
NHS Wales Shared Services Partnership
Audit & Assurance Services
Primary Care cluster plans Contents
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services
Contents Page
1. Introduction and Background 4
2. Scope and Objectives 4
3. Associated Risks 5
Opinion and key findings
4. Overall Assurance Opinion 6
5. Assurance Summary 7
6. Summary of Audit Findings 8
7. Summary of Recommendations 9
Review reference: CTMU-1920-35
Report status: Internal Audit Report
Fieldwork commencement: 24 July 2019
Fieldwork completion: 30 September 2019
Draft report issued: 7 October 2019
Management response received: 17 October 2019
Final report issued: 18 October 2019
Auditors: Emma Samways, Deputy Head of Internal Audit
Ken Hughes, Audit Manager
Executive sign off: Alan Lawrie, Director of Primary,
Community and Mental Health
Distribution: Sarah Bradley, Directorate Manager for
Primary Care and Localities
Mark Gall, Deputy Directorate Manager
for Primary Care
Committee: Audit Committee
Appendix A Appendix B
Management Action Plan Assurance opinion and action plan risk rating
Primary Care cluster plans Contents
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services
Audit & Assurance Services conform with all Public Sector Internal Audit Standards as
validated through the external quality assessment undertaken by the Institute of
Internal Auditors.
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership - Audit &
Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf Morgannwg
University Health Board, no responsibility is taken by the Audit & Assurance Services Internal
Auditors to any director or officer in their individual capacity, or to any third party.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 4 of 20
1. Introduction and Background
The review of Primary Care cluster plans was completed in line with the 2019/20 Internal Audit Plan. The review sought to provide Cwm Taf
Morgannwg University Health Board (the ‘UHB’ or the ‘Health Board’) with assurance regarding the process for the production and oversight of Primary
Care cluster plans.
The Health Board initially had four Primary Care clusters (Cynon, Merthyr
Tydfil, Taff Ely, Rhondda), with a cluster being defined as the bringing together of ‘all local services involved in health and care across a
geographical area, typically serving a population between 25,000 and
100,000. Working as a cluster ensures care is better co-ordinated to
promote the wellbeing of individuals and communities.’
Primary Care services are often the first point of contact that a person has with the NHS in Wales. This can be through General Practices, pharmacy,
dentistry or optometry services. The community services delivered through the clusters can include a wide range of staff such as community and district
nurses, midwives, health visitors, mental health teams, health promotion teams, physiotherapists, occupational therapists, podiatrists, phlebotomists
and paramedics.
Each cluster will have a three-year plan in place outlining the co-ordination
of activities in its geographical area. Plans should be developed around nine strategic aims and detail the cluster’s objectives under each of those aims.
They outline who the key partners are in achieving listed objectives, target completion dates and the expected outcome for the patient of achieving the
objective. Updates and RAG ratings are also provided on the progress that
has already been made in achieving each objective.
Cluster plans should both shape and underpin the Health Board’s integrated
medium term plans (IMTPs) and embrace the key Health Board priorities
for the forthcoming three years.
In April 2019, the Health Board took over responsibility for the provision of health care services to the population of Bridgend. As a consequence there
are now three more clusters that fall under the remit of the larger Health Board (Bridgend East, West and North). As such, the Bridgend clusters have
been considered in this review.
The relevant lead Executive for the assignment is the Director of Primary
Community and Mental Health.
2. Scope and Objectives
The overall objective of this audit was to evaluate and determine the adequacy of the systems and controls in place in relation to the Health
Board’s management of processes in relation to Primary Care cluster plans.
The review sought to provide assurance to the Health Board’s Audit Committee that risks material to achieving the system’s objectives were
managed appropriately.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 5 of 20
The areas that the review sought to provide assurance on were:
• Alignment of cluster plans with Primary Care and Localities directorate
IMTPs, the Health Board IMTP and Welsh Government objectives.
• The processes followed for the development of cluster plans, ensuring all relevant parties are involved and resultant plans are meaningful
with achievable targets.
• Monitoring arrangements are in place at both a cluster level and
directorate level to ensure the achievement of objectives.
• Governance arrangements are in place for the management of the
clusters and any expenditure incurred in line with agreed objectives.
• Risks identified in the delivery of cluster plans are captured and there is a process to ensure relevant risks feed into the wider Health Board
risk management process.
3. Associated Risks
The potential risks considered in this review were as follows:
• Welsh Government and Health Board objectives are not achieved
where plans are not aligned or developed with due consideration.
• Budgets are exceeded where proper monitoring arrangements are not
in place.
• The Health Board is exposed to un-necessary risks if process are not in
place to identify and manage risk.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 6 of 20
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness
of the system of internal control under review. The opinion is based on the work performed as set out in the scope and objectives within this report.
An overall assurance rating is provided describing the effectiveness of the system of internal control in place to manage the identified risks associated
with the objectives covered in this review.
The level of assurance given as to the effectiveness of the system of internal
control in place to manage the risks associated with Primary Care cluster
plans is reasonable assurance.
RATING INDICATOR DEFINITION
Reasonable assurance
The Board can take reasonable assurance that arrangements to secure
governance, risk management and internal control, within those areas under
review, are suitably designed and applied effectively. Some matters require
management attention in control design or compliance with low to moderate
impact on residual risk exposure until
resolved.
Our review of Primary Care cluster plans showed an alignment between the
Primary Care and Localities Directorate and Health Board IMTPs, and Welsh Government Objectives. This supports the drive to further develop localities
and transfer more services from secondary to primary care. However, in line with the Welsh Government’s new Quality Assurance and Improvement
Framework, new Cluster Group IMTPs were being developed during the course of our audit, which will replace the existing Primary Care cluster
plans. In developing these plans it is important that there is clear alignment
and links to directorate and Health Board objectives.
Our review of the cluster plan development process identified that good use was being made of data and information provided by Public Health Wales
NHS Trust (PHW), and there was evidence of GP input into the planning
process through the submission of their individual Practice Development Plans. However, there was no evidence that other cluster group
stakeholders such as the Local Authority, Dentists, Pharmacists, Optometrists and third sector representatives had contributed directly to
the plans.
We also identified that arrangements for the management of cluster group
risks, and their potential escalation to the Health Board, were in the early
stages of development and consequently were not currently effective.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 7 of 20
The overall level of assurance that can be assigned to a review is dependent
on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
5. Assurance Summary
The summary of assurance given against the individual objectives is
described in the table below:
Assurance Summary
1 Alignment of cluster
plans
2
Process for development of
cluster plans
3
Monitoring and
reporting
arrangements
4
Governance and
finance
arrangements
5 Risk Management
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Design of Systems/Controls
The findings from the review have highlighted one issue that is classified as
a weakness in the system control / design for Primary Care Cluster Plans.
Operation of System/Controls
The findings from the review have highlighted three issues that are classified as weaknesses in the operation of the designed system / control
for Primary Care Cluster Plans.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 8 of 20
6. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during our review. We also summarise the findings made during our audit
fieldwork. The detailed findings are reported in the Management Action Plan
(Appendix A).
Objective 1: Alignment of cluster plans with Primary Care and Localities directorate IMTPs, the Health Board IMTP and Welsh
Government objectives.
We identified the following area of good practice:
Priorities in the cluster plans broadly aligned to those in the
directorate and Health Board IMTPs.
We did not identify any findings relating to this objective.
Objective 2: The processes followed for the development of cluster plans, ensuring all relevant parties are involved and resultant plans
are meaningful with achievable targets.
We identified the following areas of good practice:
Responsibility for coordinating and preparing cluster group plans had been specifically assigned to the Cluster Development Managers with
leadership, direction and support from the Cluster Leads.
A GP Practice Development Plan template has been provided to each
GP Practice and its use has ensured the consistency of information
provided to inform the cluster plan.
We identified the following findings:
Due to poor attendance at cluster meeting by some stakeholder
groups, there was no evidence that all stakeholders had input into the
development of cluster plans, nor was there evidence that draft
cluster plans were reviewed by respective cluster groups.
Not all plans that we reviewed contained SMART objectives, and not all plans specifically assigned a lead with responsibility for achieving
objectives.
Objective 3: Monitoring arrangements are in place at both a cluster
level and directorate level to ensure the achievement of objectives.
We identified the following area of good practice:
The Bridgend West cluster group recorded actions arising from cluster group meetings in an action log. This showed the action to be taken,
the responsible lead and completion of the outstanding action. All other clusters undertook monitoring via the minutes of their
meetings.
No findings were identified under this objective.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board
NHS Wales Audit & Assurance Services Page 9 of 20
Objective 4: Governance arrangements are in place for the
management of the clusters and any expenditure incurred in line
with agreed objectives.
We identified the following area of good practice:
Cluster group expenditure and budgets are monitored centrally by the
Development Managers and Cluster Leads with input from Health Board’s finance team, as appropriate. Clusters also undertake their
own additional monitoring and cluster expenditure is a regular agenda
item at Cluster Meetings.
We identified the following finding:
All cluster group terms of reference were in need of updating.
Objective 5: Risks identified in the delivery of cluster plans are
captured and there is a process to ensure relevant risks feed into
the wider Health Board risk management process.
We identified the following finding:
Risk management processes and procedures are not currently
effective and in need of development across all of the cluster groups
that we reviewed.
7. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A
together with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Number of
recommendations 1 3 0 4
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 10 of 20
We reviewed the risk management arrangements at six cluster groups to ensure
there were adequate processes and procedures in place for the identification, recording and monitoring of cluster group risks, and for the escalation of
‘significant’ risks to the Health Board. During our discussions with the Cluster
Development Managers it was apparent that there are some risk registers and risk logs in place, however, risk management processes were generally not well
established, and in some cases were in the very early stages of development.
Our testing identified the following:
There was no standard risk assessment methodology in place.
There were no risk assessment forms in use.
Risks were not assessed for impact and likelihood on five of the six risk
registers or logs that we reviewed, therefore the risk score is unknown.
There was no standard format risk register or risk log in use.
None of the risks on any of the risk registers or risk logs that we reviewed
had an individual, unique risk identification number.
The date risks were added to the risk register or risk log was not recorded.
Responsibility for undertaking actions designed to mitigate risks was not
recorded.
There was no evidence on any of the risk registers or logs that we reviewed
that they had been updated.
Potential risks to the successful
achievement of cluster plans are not being identified and mitigated
against.
The Health Board is exposed to
unnecessary risks if processes are not in place to identify and manage
risk.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 11 of 20
To date no risks had been escalated to the Health Board. There was no
established approach for clusters to identify risks for escalation to the
Health Board.
Recommendation Priority level
The Health Board should ensure that adequate risk management processes and
procedures are put in place for all cluster groups. These should include:
A documented risk assessment methodology underpinned by a standard
risk assessment form.
A standard risk register for use by all cluster groups.
Assigning each risk a unique risk reference and recording the date the risk
was accepted onto the risk register.
Assigning a lead for each risk responsible for undertaking risk mitigating
actions for that risk.
Ensuring risk registers are regularly reviewed and updated, and reviews
are evidenced.
A process for identifying and escalating qualifying risks to the Health Board.
It may also be beneficial for the Cluster Development Managers to undertake risk
management training.
High
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 12 of 20
Management Response Responsible Officer/ Deadline
We disagree that this is a HIGH Priority. Cluster Risks are very low however ToRs
will be amended to reflect the requirement to assess and record risk appropriately. From a timescale point of view we will recommend that Clusters
review the recommendations at the next Cluster Meeting and amend the ToRs as
appropriate.
Audit note: We acknowledge the management response including
management’s view of our judgement of the priority level set against the recommendation. It is our view that, given the level of maturity of the risk
management process within cluster groups and the work to be done, the high
priority assessment was appropriate at the time of our fieldwork.
Development Managers/Spring
2020
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 13 of 20
Finding 2 - Development of cluster plans (Operating effectiveness) Risk
We held discussions with six of the seven Cluster Development Managers to
review the process for developing the Primary Care Cluster Group Plans. There was good evidence of GP input to cluster group plans through the submission of
their Practice Development Plans. However, there was no documentary evidence
from other primary care providers such as dentists, pharmacists, optometrists and stakeholders such as the Local Authority, third sector and Public Health
Wales.
Our review of the minutes from the last year for the six cluster groups also
identified very little discussion about the cluster group plans during the meetings or any input to the plan preparation process from these groups. We also
identified:
The two Bridgend clusters reviewed held six meetings each over the last
year. PHW was not represented at any of these meetings. The Local
Authority was only represented at 4/12 of the meetings.
The minutes of the four meetings held by the Cynon cluster did not provide
enough detail to determine which organisations were represented.
The Merthyr, Taff Ely and Rhondda cluster held 13 meetings in total over the last year. There was no Local Authority representative at any of these
meetings, and the third sector representation was poor for the Rhondda
cluster, with only 1/4 meetings attended.
Welsh Government and Health
Board objectives are not achieved where plans are not aligned or
developed with due consideration.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 14 of 20
There appears to be some ambiguity around cluster group membership and those
groups that are deemed as stakeholders as opposed to cluster members. The
terms of reference that we reviewed does not make this distinction.
Draft plans are submitted to the Primary and Localities Directorate Manager, but
there is no timeframe for this, other than they need to be submitted in time for
the development of the Primary Care directorate’s IMTP.
We also identified that feedback on plans was not sought or encouraged from
patients or patient groups.
Recommendation Priority level
1. All members of the cluster groups should be encouraged to attend their
cluster group meetings and have input to the development and refresh of their cluster group plans. The cluster groups should also encourage
attendance at cluster group meetings by representatives from all stakeholder
groups.
2. Cluster group plans should be subject to approval and sign-off from the cluster group during their meetings, prior to being submitted to the Health
Board and published on the Health Board website.
3. Consideration should be given to feedback being provided to the Cluster
Development Managers on their plans in order for best practice to be shared
amongst the clusters.
Medium
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 15 of 20
Management Response Responsible Officer/ Deadline
1. Cluster membership is not prescribed therefore attendance continues to be
non-mandatory. Cluster Development Managers communicate details of
meetings widely. Clusters cannot be held accountable for attendance.
2. Cluster Plans are approved at Cluster meetings however it is noted that this action should be clearly documented via ToR, Agenda’s and Minutes of
meetings. IMTPs have clearly documented participation requirements as set
out in the revised GMS contract effective October 1st 2019.
3. Cluster Plans are shared at Cluster Leads Meetings however the introduction of IMTPs has clearly documented requirements for each Cluster GP Practice
member.
Development Managers/December
2019 (for discussion/action at next
Cluster Meeting as appropriate)
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 16 of 20
Finding 3 - Content of cluster plans (Operating effectiveness) Risk
We reviewed all seven cluster plans and noted that there were two basic plan
templates used, but these had been altered and not used consistently as clusters can choose their reporting style. The two templates related to the former Cwm
Taf clusters and the former Abertawe Bro Morgannwg University Health Board
(ABMUHB) clusters, which is inevitable during this period of transition.
Within the ‘Action Plan’ section of the cluster plans, we identified:
The targets, aims and objectives were not always measurable or time-bound.
In some cases the lead assigned responsible for implementation was not
specific and just stated ‘Health Board’.
All cluster plans included a RAG rating in the 'Action Plan' section but four did
not include a key as to what each colour rating referred to. Of the three that did provide a key, there was consistency in the descriptors in two of the plans,
with the third one using a different set of descriptors.
Welsh Government and Health
Board objectives are not achieved where plans are not aligned or
developed with due consideration.
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 17 of 20
Recommendation Priority level
1. Cluster plans (or IMTPs) should include targets that are measurable and time-
bound, and responsibility for achieving them should be specifically assigned
within the cluster group.
2. A standard template should be used for all Cluster Group Plans. Where
objectives and targets are RAG rated a key should be included in the plan.
Medium
Management Response Responsible Officer/ Deadline
1. SMART Objectives will be set.
2. The introduction of IMTP’s has addressed this item with a common template
being adopted by all Clusters.
Development Managers/January
2020
Completed September 2019
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 18 of 20
Finding 4 – Cluster group terms of reference (Operating effectiveness) Risk
We reviewed the terms of reference for six of the seven Cluster Groups and
identified the following issues:
The terms of reference for the Bridgend clusters made several references to
ABMUHB, (now Swansea Bay), for example compliance with ABMUHB
Financial Regulations and Standing Orders.
The terms of reference for Cynon, Taff Ely and Rhondda cluster groups did
not include the monitoring of cluster expenditure and ensuring the efficient
use of financial resources. This is inconsistent with the other cluster groups.
The terms of reference for the three Bridgend clusters and the Merthyr cluster did not include the responsibility for the management of cluster
group risks. This is inconsistent with the other cluster groups.
Welsh Government and Health
Board objectives are not achieved where plans are not aligned or
developed with due consideration.
Recommendation Priority level
Consideration should be given to the impact of the boundary change and the period of transition to acknowledge and amend inconsistencies created by the
processes and procedures followed by former ABMUHB colleagues. With
consideration to any published Welsh Government guidance:
1. The terms of reference for the Bridgend cluster groups should be amended to ensure all references to ABMUHB are replaced with Cwm Taf Morgannwg
UHB.
Medium
Primary Care cluster plans Internal Audit Report
Cwm Taf Morgannwg University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 19 of 20
2. The terms of reference for the Cynon, Taff Ely and Merthyr cluster groups
should be updated to ensure they include financial responsibility and the need to ensure efficient use of their budget in compliance with the Health Board’s
Financial Regulations and Standing Orders.
3. The terms of reference for the Bridgend and Merthyr cluster groups should be updated to include responsibility for the effective management of Cluster
Group risks.
Management Response Responsible Officer/ Deadline
1. All ToRs will be reviewed to reflect CTMUHB.
2. All ToRs will be reviewed to ensure that clear financial controls are
documented and Finances are formally reviewed throughout the year.
3. All ToRs will be reviewed to ensure that Risks are acknowledged, reported,
assessed and reviewed.
Development Managers/Next
Cluster Meeting
Development Managers/Next
Cluster Meeting
Development Managers/Next
Cluster Meeting
Primary Care cluster plans Internal Audit report
NHS Wales Audit & Assurance Services Page 20 of 20
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.4 Wales Audit Office - Review of Primary Care Services
1 4.4 WAO Report - Review of Primary Care Services PCPPHC 10 February 2020.docx
AGENDA ITEM
(4.4)
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Welsh Audit Office Report on Primary Care Services in Wales
Date of meeting 10.02.20
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by SARAH BRADLEY, DIRECTORATE MANAGER FOR PRIMARY CARE
Presented by Alan Lawrie, Director of Primary Community and Mental Health
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR DISCUSSION / REVIEW
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(Insert Name) (DD/MM/YYYY) Choose an item.
ACRONYMSIMTPWAODPCCAMDJET
Intermediate Medium Term PlanWelsh Audit OfficeExecutive Director for Manager for Primary and CommunityAssistant Medical Director Joint Executive Team
Wales Audit Office Report – Review of Primary Care Services
Page 2 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
1. SITUATION/BACKGROUND
1.1 The Wales Audit Office (WAO) has recently carried out a national review of primary care services. ..\..\..\..\WAO Reports\Primary Care in Wales 2019-english version.pdf. The aim was to assess and report on progress being made with the planning and the delivery of the Primary Care Model for Wales. The Primary Care Model for Wales has evolved and promotes multi-professional teams to reduce the pressures on GPs, to improve access and services to patients and deliver care in a more collaborative way closer to people’s homes. It is also a core element of the Welsh Government’s plan for a sustainable service model as described in the ‘A Healthier Wales’ policy.
1.2 The report sets out National level recommendations, although they are mainly aimed at Welsh Government and the National Primary Care Board. The Director General Health and Social Care Services has accepted the WAO’s recommendations that they ‘need to do better’ but in turn there will be greater scrutiny on health boards to ‘do more’ to ensure that the pace and scale of change is achieved at a local level.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 The WAO report concludes that;
‘despite considerable investment and many plans for primary care transformation over the years, change has not happened as quickly or as widely as intended’.
From a Cwm Taf Morgannwg perspective a considerable amount of work has already been undertaken since 2016 to support new ways of working, innovation and the implementation of the new primary care model. This has been achieved through;
1. GP Sustainability workshops to identify the roles required for ab effective wider extended primary care team.
2. Cluster development and implementation of new initiatives3. National Primary Care Fund. Introduced in 2015/16 to specifically
fund the national primary care model, the increased in 2016 to support cluster funding, workforce developments and pacesetter projects. This totals £8.414m.
Wales Audit Office Report – Review of Primary Care Services
Page 3 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
4. Raising the profile and supporting the professional development of services provided by other contractor professions, such as Dental, Optometry and Pharmacy.
5. Development of the multi-disciplinary team, important elements of the ‘Stay well in your community’ (SWIYC) Programme for Rhondda, Cynon, Taff and Merthyr Tydfil Localities and 3 Ambitions within Bridgend Locality.
2.2 Previous Audit ReportsTwo previous Audit Reports on Primary Care Services have been undertaken and have provided the Board in both instances with reasonable assurance with regard to progress of the implementation of the primary care model. The first audit was a WAO ‘Report into Primary Care Services for 2017-18’ for the former Cwm Taf Health Board and it concluded that;‘The Health Board has a sound plan for primary care and is making reasonable progress towards implementing key elements of the national vision. Oversight arrangements are strong and performance against some indicators is above average. However, there is further scope to raise the profile of primary care, shift more resources towards primary care and to address workforce challenges.’ The full report is available at ..\..\..\..\WAO Reports\2018 WAO Review CT Primary Care Services
The recommendations were:
Strategic planning: the Health Board has a strong primary care plan aligned to national priorities and whilst clusters are at an early stage of development, the Health Board is taking steps to support their ongoing development
Investment: the Health Board has some examples of resources shifting to primary care but there are barriers to large-scale change, and the available data make it difficult to accurately calculate the overall investment in primary care
Workforce: workforce challenges are threatening the sustainability of some practices but the Health Board has begun workforce modelling and is in the early stages of testing solutions
Oversight and leadership: strong leadership and monitoring arrangements are in place and the Health Board is taking steps to improve primary care data, however, there is further scope to raise the profile of primary care
Wales Audit Office Report – Review of Primary Care Services
Page 4 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Performance and monitoring: the Health Board is making reasonable progress in delivering its primary care and localities plan and some aspects of performance are better than the Wales average, although a number of difficult challenges remainA second audit was undertaken very recently in 2019 by Internal Audit and focused on Cluster Plans across the newly formed Cwm Taf Morgannwg Health Board area. It sought to provide the Board with assurance regarding the process for the production and oversight of Primary Care cluster plans. It concluded that;‘Our review of Primary Care cluster plans showed an alignment between the Primary Care and Localities Directorate and Health Board IMTPs, and Welsh Government Objectives. This supports the drive to further develop localities and transfer more services from secondary to primary care.’This report is available at ..\..\..\GMS\Internal Audit Reports\Cluster Audit 2019\Primary Care Cluster Plans draft audit report for issue CTMUHB Response update v2.docx
2.3 Welsh Audit Office Recommendations
The WAO report makes specific recommendations and for ease these have been collated in table 1 below. Although the recommendations have been identified for Welsh Government and for the National Primary Care Board the Directors of Primary Community Care and the National Director of Primary Care are going to formulate a response to ensure there is a consistent approach across the 7 Health Boards. Our local response has been identified in the same table but also include actions which are already being taken forward by the health board and by the national work-streams as part of the Strategic Programme for Primary Care.
There is a lot of similarity in the recommendations made in the WAO report from 2018 and this National Report.
Table 1 – Recommendations
Improving Primary Care DataMonitoring of primary care performance and activity is limited. Current performance measures do not give an effective overview of whether patient outcomes are improved by primary care. Activity monitoring and planning is complicated by difficulties obtaining standardised data from independent contractors.
Wales Audit Office Report – Review of Primary Care Services
Page 5 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Local Actions TimescaleRecommendation 1. The Welsh Government should work with the National Primary Care Board to agree robust measures of patient outcomes in their suite of performance measures for primary care and in doing so they should look to collaborate with experts in measuring whole systems change outcomes.
1. Whole system outcome measures have been identified as part of the Stay Well in Your Community (SWIYC) transformation programme. These will be shared with the DPCC to help inform the suite of measures.
April 2020
Recommendation 2.The Welsh Government should work with independent primary care contractors to ensure the NHS in Wales has ongoing access to standardised information about their activity, to contribute to better planning and design of services.
1. There is a national procurement of a demand and capacity tool and this will be implemented as part of the new GMS Access standards.
2. National Workforce Tool will also help support this.
To be confirmed
Implementing the Primary Care Model for WalesThe Primary Care Model for Wales and the Strategic Programme for Primary Care provide a direction of travel but there is not yet a clear approach to quantifying the extent of progress in implementing these changes, and data on the numbers and the roles employed in primary care is limited. The Welsh Government should:
Local actions TimescaleRecommendation 3. Strengthen its performance management of primary care within health boards by developing a method for quantifying each health board’s progress in implementing the primary care model
1. Cluster IMTPs form a vehicle for measuring progress against the primary care model
2. National GMS workforce toolkit has been procured but not fully functional. Primary Care team already taking steps to continue to collect the data regarding roles and workforce manually from practices. Baseline to be reported in IMTP
Baseline February 2020By DM for Primary Care
Baseline February 2020By DM for Primary Care
July 2020
Wales Audit Office Report – Review of Primary Care Services
Page 6 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
3. Further work to be undertaken to gather similar data for other contractor professions
By DM for Primary Care
Recommendation 4.Collect and regularly publish data on the number and type of staff working as part of multi-disciplinary primary care practice teams, with a view to monitoring the implementation of the multi-professional model
1. Report bi-annually (mid and end of year) to Primary Community and Population health and Partnerships Committee the data on the multi-disciplinary teams. Details on WTE and types of roles
July 2020By DM for Primary Care
Keeping the Strategy Under Review The Strategic Programme for Primary Care is in its infancy and partnership with social care and the third sector, through Regional Partnership Boards, will be crucial to transformation. The National Primary Care Board should:
Local Actions TimescaleRecommendation 5. Publish a review of progress in delivering the strategic programme in 2020-21. The review should seek opinions on progress from all key partners, including the Regional Partnership Boards
1. Report bi-annually (mid and end of year) to the Regional Partnership Board
2. Present on the progress by the Primary Care Strategic Programme and the deliverables from the various the work streams to the Executive Management Board
July 2020By DPCC & AMD for Primary Care
April 2020By DPCC & AMD for Primary Care
Strengthening ClustersThe Health, Social Care and Support Committee’s cluster inquiry made 16 recommendations. Public Health Wales subsequently led the development of a good practice guide for cluster governance. Much work remains to be done to ensure clusters have a clear remit, broad membership and are able to drive change at pace and scale. The Welsh Government should:
Local Actions TimescaleRecommendation 6. Undertake and publish a stock take of progress against the recommendations from the cluster inquiry and in implementing the cluster governance framework, with
1. Cluster Leads and Cluster Development Managers to undertake review of the inquiry recommendations and ensure compliance and detail actions to be undertaken where compliance is not met.
April 2010By Deputy Manager for Primary Care
Wales Audit Office Report – Review of Primary Care Services
Page 7 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
a view to supporting further development and maturity of clusters.
2. Undertaken review of the recommendations and progress made by the previous two reports, WAO report for Cwm Taf on Primary Care clusters and the Internal Audit report on clusters.
3. Promote the use of cluster toolkit with independent contractors
April 2010By Deputy Manager for Primary Care
April 2010By Deputy Manager for Primary Care
Shifting resources to primary careFrom the existing data, it is difficult to quantify exactly how much the NHS in Wales is spending on primary care, and to assess whether health boards are succeeding in shifting resources towards primary and community care. A Welsh Health Circular from July 2018 set out a new financial framework for supporting such shifts
Local actions TimescaleRecommendation 7The Welsh Government should consult with health boards, to agree an approach to clarifying and standardising the way that primary care expenditure is recorded and reported.
1. Await national guidance TBCWG and JET
Recommendation 8The Welsh Government should work with health boards to evaluate, and if necessary, improve the effectiveness of the financial framework in supporting the shift in resources towards primary and community care.
1. Mainstream current cluster initiatives to release cluster funding to continue to innovate for new roles and initiatives. This is reliant on no CRES or other expectations to reduce the existing Primary Care Budget.
2. Historically there is a reliance on ‘new’ primary care funding or core GMS funding to support primary care developments rather transfer of resource from other parts of the system.
TBCBy Executive Team
TBC By Executive Team
Wales Audit Office Report – Review of Primary Care Services
Page 8 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
3. Support from finance and performance partners to identify the impact of primary care initiatives on secondary care to identify the efficiency and productivity across the whole system and to resultant resource shift required.
Recommendation 9As part of the Joint Executive Team process, the Welsh Government should require health boards to report annual on their progress in shifting resources towards primary care. The coverage of these reports should not be limited to financial resources and should include other resources such as staff and services. Through this process, the Welsh Government should hold to account the entire executive team of health boards, not just the executive directors of primary care.
1. To await the guidance on the JET reporting template
TBCBy Executive Team
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 In December 2019, Andrew Goodall, Director General for Health and Social Care, wrote out to all Health Boards informing them of his decision to allocate additional £10million across Wales to support cluster funding on a recurrent basis. ..\..\..\GMS\cluster plans\Cluster Funding\Andrew Goodall letter to CEOs on cluster working Dec 2019.pdf. This demonstrates the ongoing confidence and commitment to cluster development. The letter also reminds Health Boards of the expectations, that they;
Provide planning, HR and finance support so clusters can plan for the use of this funding as recurrent funding
Must provide support to clusters to enable reasonable and proportionate evaluation for innovative use of this funding and must plan to adopt and adapt proven service models with core funding, across the health board and not just in the cluster hosting
Wales Audit Office Report – Review of Primary Care Services
Page 9 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
that innovation, via the health board IMTP process. This also then releases cluster funding for reinvestment
Look to re-provide any underspend (planned or unplanned) from your core funding the following year to enable as much flexibility as possible
Include action in your IMTPs to delegate more and more decisions and core funding and other resources to cluster level.
3.2 Welsh Government will be assessing the progress of Health Boards against the recommendations through the scrutiny of the Integrated Medium Term Plans (IMTP) for 2020-23 and via Joint Executive Team (JET) meetings. A specific template will be issued to support reporting arrangements. In addition to this there is a requirement, as outlined in Recommendation 9, for Health Boards to report on the shift in resources, financial, workforce and services on an annual basis.
Welsh Government wish to see a ‘real’ increase in the level of investment being made into primary care services. The development and implementation of the Primary Care Model for Wales is not just limited to General Medical Services but essentially but also incorporates the wider development and upskilling of multi-professional teams across all primary care services. The challenge of achieving further development, and importantly, pace and scale will be made harder and near impossible in the event that cash releasing efficiency savings (CRES) targets are applied to the Primary Care Investment Fund and/or to ‘core’ Primary Care, including all Dental, Optometry and General Medical Services, budgets.
4. IMPACT ASSESSMENT
Yes (Please see detail below)
Quality/Safety/Patient Experience implications
The implementation of the Primary Care Model for Wales will ultimately result in the delivery of high quality, safe and timely care for patients delivered in a prudent manner by an appropriate professional.
Effective CareRelated Health and Care standard(s)
Wales Audit Office Report – Review of Primary Care Services
Page 10 of 10 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
Yes (Include further detail below)Resource (Capital/Revenue £/Workforce) implications / Impact
There will be a resource impact resulting from the mainstreaming of cluster initiatives and shift of activity to primary care
Link to Main Strategic Objective To ensure that services provided are
accessible and sustainable into the future
Link to Main WBFG Act Objective
Work collaboratively with our public service partners and a broader range of partners to join up health and other services where this potentially represents better value for our residents and care users
5. RECOMMENDATION
5.1 The Primary, Community, Population Health & Partnerships Committee is asked to:
5.2 NOTE and discuss the report.
4.5 Inverse Care Law
1 4.5 ICL Report PCPHPC 10 February 2020.docx
AGENDA ITEM
(4.5)
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Inverse care law programme
Date of meeting 10/02/2020
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by
Gillian Day, Wellbeing Development Manager, Primary Care, Gemma Northey, Specialty Registrar and Sara Thomas, Consultant Public Health
Presented by Sarah Bradley, Head of Primary Care
Approving Executive Sponsor Executive Director of Public Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(Insert Name) (DD/MM/YYYY) Choose an item.
ACRONYMS
ICL Inverse Care Law
CTMUHB Cwm Taf Morgannwg University Health Board
Inverse Care Law Report Page 2 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
1. SITUATION/BACKGROUND
This paper provides an update on the Inverse Care Law (ICL) Cardiovascular Health Check Programme in CTMUHB. The programme has been developed to tackle inequalities in health, initially with a focus on cardiovascular disease. The Cwm Taf Health check has been operational since 2015 with specific focus on targeting our most deprived communities.
The Committee has received previous reports which provided the background logic model and early outcomes of this high profile Welsh Government funded Programme which uses CTMUHB and Aneurin Bevan UHB as its pilot sites.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
A National ICL Programme update report was produced for Welsh Government in 2019. The activity and outcome data contained within this report was presented to the Cwm Taf Primary Care Committee (April 2019). The executive summary of this report is attached as Appendix 1.
Valuable learning has been gained from undertaking this programme to date. It has demonstrated an ability to reach more deprived populations, in an effort to mitigate the effects of poverty on health and close the inequality gap. Despite good uptake and promising early outputs, there is more work to be done to encourage wider population engagement with this programme. In addition, greater focus is needed on the availability and sustainability of support services as well as refining the method of evaluating the impact of this approach over time. Of particular concern was the lack of low level weight management support service to individuals receiving a health check.
The report made three recommendations which are being progressed under the leadership of CTMUHB Consultant Public Health in partnership with the ICL Teams in CTMUHB and Aneurin Bevan UHB.
Recommendation1:Establish a detailed next phase of the national Inverse Care Law Programme in Wales that consolidates the model framework based on the valuable learning to date; the re-focused programme will inform the Primary Care Strategic Programme and contribute to the realisation of the prevention vision set out in a Healthier Wales.
Inverse Care Law Report Page 3 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Recommendation 2:Explore the challenges posed by the evaluation of the programme with particular focus on addressing the weaknesses in the data architecture underpinning the programme.
Recommendation 3:Explore opportunities for health economic evaluation of the programme and longitudinal research drawing on the strength of the SAIL database. The CTMUHB Public Health and Primary Care ICL team partnership are working with the ABUHB Team to progress recommendation 1 which will inform the future development of the programme locally.
A further analyses of data will be available from SAIL during summer 2020 which will inform the next report to Welsh Government. This will be shared with the committee in due course.
Current Position:The CTM ICL Health Check team currently has 1 manager, 1 Registered lead nurse, 1.3WTE part time Lifestyle advisors and 7 WTE advisors.
By the end of March 2020, the team will have worked with 36 GP practices of the previous Cwm Taf footprint, who engaged with the programme. Bridgend North Cluster were part of a health check pilot in the previous ABMUHB. Going forward, the CTMUHB CVD Health Check Programme will be rolled out to Bridgend practices commencing in March/April in Bridgend west Cluster.
The team has undertaken in excess of 17,000 health checks which has enabled identification of people at most risk and provide them with the information and advice they need to support changes in their lifestyle. Please see headline activity page 6.
A service review was undertaken at the end of 2018 with new management in post and as a result the programme is implementing changes to meet the challenges raised from the data and the review by identifying people who need support to make change. The team are implementing the best evidence, and using prudent approaches to co-produce improved pathways. This has enabled cost savings identified from the review and available evidence to introduce Lifestyle Advisor roles and other improvements in process for an improved patient experience and service.
The 1.3 WTE Lifestyle Adviser posts are a new and exciting addition to the programme in January 2020, the posts are being tried as a proof of concept in response to the high numbers of patients requesting and in need of further
Inverse Care Law Report Page 4 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
support. The Lifestyle Advisers support people to access opportunities and set goals they would not be able to do unaided.
Participants are supported with goal setting and behaviour change for up to 6 months in a way that matters to them. The impact of the posts will be measured by performance and patient outcomes/experience which will be collated and evaluated in October 2020.
Next Steps:The programme is currently now in the second phase of delivery which entails:
1- Inviting the people who have turned 40 since the team was in the practice previously
2- inviting original participants and non-attenders3- Possibility of investing in the development of a community module to
allow health checks to be undertaken in other venues but still being linked to GP systems to mitigate any risk to follow up of patients.
4- Identified patients offered referral for the support of a lifestyle advisor for up to 6 months to support their behaviour change journey.
5- Evaluating the lifestyle Advisor roles and implementing recommended changes October 2020
6- Evaluating Bridgend North Cluster lifestyle approach completed by April 2020
7- MSc Research project underway to understand lack of engagement with the Health Check offer (up to 50%). Explore reasons for variable attendance across the area.
8- Implementing pre-diabetes training and screening research project in South Cynon Cluster.
9- Implementing Diabetes case finding into the programme to support NICE guidance in identifying people who are not currently part of the inclusion criteria- this is an essential and natural addition to the programme which will involve investment in further staff by Public Health prevention monies.
10- Undertake further service review to ensure we are meeting the needs of the patients, clusters and staff development.
Type 2 Diabetes Prevention ProgrammeDiabetes mellitus is one of the most common chronic diseases in Cwm Taf Morgannwg University Health Board (CTM UHB) and the project work aims to prevent or delay the development of type 2 diabetes in patients at high risk who are identified as having ‘pre-diabetes’.
The Health Board has identified in its “Prevention and Early Years” funding, an allocation to undertake this project utilising the expertise of the CVD Health Check team. The project will be piloted in Cynon South Cluster and delivered
Inverse Care Law Report Page 5 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
in two phases, the first is a ‘pre-diabetes’ lifestyle intervention in GP practices. The programme will offer a 20-minute appointment for patients identified as having a high blood glucose by their GP but who are not already on the diabetes register. The appointment will be run by trained health care support workers who will:
Discuss test results and current risk of type 2 diabetes if no lifestyle changes are made
Discuss ‘pre-diabetes’ Measure height, weight and body mass index (BMI) Discuss diet Discuss importance of increasing physical activity levels Provide an information pack including Diabetes UK ‘high risk of
type 2 diabetes’ leaflet, a dietary sheet and information about the community coordinator
Patients will be recalled after one year and offered a repeat blood test and BMI, then if results are still high will be offered a repeat lifestyle appointment. The programme feasibility will be tested initially in the South Cynon cluster and will be evaluated by Swansea University Medical School in collaboration with CTM UHB. Supported by evaluation evidence, an assessment on general rollout to practices across the UHB will be made.
The second phase aims to identify people at high risk of diabetes in CTM UHB who do not meet the Inverse Care Law (ICL) health check criteria (or who did not attend for their health check appointment) and offer them an assessment. This will allow identification of patients under the age of 40 who would not normally be called for a check. Second phase feasibility will again be tested in the South Cynon cluster and a process evaluation undertaken.
Headlines
98% of smokers referred to Smoking Cessation services70% of people seen
overweight or obese
Undertaking a brief intervention in primary care to increase physical activity is more
cost effective than prescribing statins
25% had high
blood pressure
68% of people were inactive
Inverse Care Law Report Page 6 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
The programme is funded by Welsh Government Primary Care Delivery Agreement money and so any associated risk with this.
4. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Staying HealthyRelated Health and Care standard(s) If more than one Healthcare Standard
applies please list below:
“The health check changed my life- I lost 4 stone and exercise regularly, I never realized how at risk I was ” 49 male Rhondda
“ Until I had the health check I had no idea how high my cholesterol was- I have improved it and will now enjoy my retirement health” 61 GP Practice Manager
“ The advice and information I received off the nurse was excellent- I only wish I could see her again ” 60 female Taf Ely
“I made my husband have his health check after having mine and I think it should be available to everyone not just 40-74 age ” 65 female Merthyr Tydfil
57% had raised cholesterol over 5 mmols
Inverse Care Law Report Page 7 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
Yes (Include further detail below)Resource (Capital/Revenue £/Workforce) implications / Impact £445k Welsh Government Primary Care
Delivery Agreement funding
Link to Main Strategic Objective To protect and improve population health
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
5. RECOMMENDATION
5.1 The Committee is asked to: 5.2 NOTE the report.
Inverse Care Law Report Page 8 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Appendix 1
1. Executive Summary
2.1 The Programme
The Inverse Care Law (ICL) Programme in Wales was conceived in 2013 with expert
input from eminent primary care academics including Professor Julian Tudor Hart. It was
predicated on a logical extension of the law - that eliminating the deficit in access to
healthcare for needier populations would reduce their excess of morbidity/mortality. It was
an expression of Julian Tudor Hart’s hope that “pre symptomatic diagnosis and screening,
which can be best done at primary care level, is possible within NHS General Practice”.
As a national initiative, the ICL programme (2013) was intended to accelerate the
development of innovative and effective models of primary care services in the areas of
Wales where the impact of poverty was most marked. This linked directly with the Welsh
Government’s commitment to tackle poverty, by clearly understanding local needs and
developing service provision accordingly. An Inverse Care Law Programme Timeline
identifies key phases in its development.
The two University Health Boards with the highest premature mortality rates and health
inequalities (Cwm Taf UHB and Aneurin Bevan UHB) were invited to develop a
programme of work to achieve measureable improvement in health and wellbeing, for
defined populations, with a reduction in variation in life expectancy between
socioeconomic groups as a key priority. This would include actions to improve the
prevention and management of chronic conditions and reduce premature mortality.
2.2 The Cardiovascular Risk Assessment (CVRA) Model
The Cardiovascular Risk Assessment (CVRA) aspect of the programme which
commenced in 2015 (also known as Living Well, Living Longer in ABUHB and Cwm Taf
Health Check), has identified and supported individuals to reduce their risk of
Inverse Care Law Report Page 9 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
cardiovascular disease through engagement, information and access to good clinical care
and lifestyle support.
The CVRA model invites eligible GP registered patients (aged 40-74 (64 in ABUHB), not
otherwise known to have cardiovascular disease (CVD)) to attend a health check or
assessment with a trained Health Care Support Worker. During the consultation a 10 year
risk of Cardiovascular Disease (QRisk2 score) is calculated from measurements and
information provided by the individual; the results are discussed with the patient together
with advice on how to reduce the risk and any support available to achieve this. Whilst
the main focus of the approach is lifestyle risk reduction, there are safeguards in place to
pick up previously undetected risk factors that would trigger an immediate clinical referral.
The logic model of the ICL programme captures the end goal of impacting CVD-related
morbidity and mortality, and also through proximal risk factor management all-cause
mortality.
The model has been shared with other health boards through the NHS Wales
Cardiovascular Risk Assessment Programme (under the auspices of the national ICL
Programme). Abertawe Bro Morgannwg and Hywel Dda University Health Boards
successfully established pilot programmes during 2017/18.
2.3 Learning from the Programme
Much has been learned from undertaking this programme and key points are captured in
this report. The programme demonstrated:
• the feasibility and value of utilising an affordable, and readily available and
appropriately-trained primary care-based workforce resource to enhance the
identification of previously unrecognised cardiovascular disease risk and signpost
into existing lifestyle and/or clinical interventions aiming to modify such risk
• that many preventive activities that were traditionally performed by registered
primary care staff can be successfully taken on by Healthcare Support Workers (or
other similar roles) working within a prudent, robust framework of governance,
Inverse Care Law Report Page 10 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
training and management. The success of this approach has possible application
to many other areas of primary care transformation through the primary care
strategic programme
• successful development and delivery of a social model of CVRA delivered by
appropriately trained Health Care Support Workers, providing capability and
capacity to GP practices to implement national guidance (NICE CG181) with pace
and at scale
• ability to link into Clinical Pathways with appropriate clinical governance
arrangements
• (from patient feedback) that those who attend the 40 minute CVRA appointment
like the experience, although as many as 50% of those invited do not take up the
offer, which is a key area for further exploration
• feasibility of undertaking CVRA with full use of software in GP practice premises,
other health care settings and community venues with minimal difference in uptake
• that models developed in one health board can be adapted and implemented
successfully in other health boards. However, the imperative to roll out the
programme before a full evaluation had been conducted meant that opportunities
were missed to strengthen the programme at its foundation and in its linkages with
services/initiatives aimed at changing disease risk
• development of a range of products:
o Training programmes and operational manuals for Health Care Support
Workers undertaking CVRA in conjunction with the British Heart Foundation
(BHF).
o CVRA Software tailored for Wales – for use in both Practice and Community
settings
o Publicity and patient materials
• Primary care and public health working together with wider partners with shared
objective of improving population health; providing opportunity for practices to
make contact with patients who otherwise wouldn’t attend the surgery or take
interest in their health and wellbeing; providing additional capacity to practices
enabled them to take an active interest in CVD prevention and social referral
Inverse Care Law Report Page 11 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
• that the availability of services to support lifestyle change is key – lack of low level
weight management support service being a serious concern
2.4 The evaluation of impact
The programme has:
• provided an unique experience of using SAIL to evaluate a complex intervention
where:
o Parallel local monitoring of data provided comparison
o Data governance agreement with practices and data transmission posed
challenges
• identified challenges in accessing data at individual patient level from lifestyle
support services e.g. NERS which limited realisation of the unique data linkage
feature of the SAIL technology
• delivered in excess of 25,000 cardiovascular risk assessments between February
2015 and May 2018.
• successfully targeted inverse care by reaching more deprived populations. For
example, 94% patients attending CVRA live in areas that fall into deprivation
quintiles 1,2 or 3
• successfully identified lifestyle and clinical risk factors and advised or directed
patients to further assessment, accordingly. Offer of access to good quality risk
modifying health care has been demonstrated but there are gaps in the availability
and consistency of services across health boards
• whilst indications are good, longitudinal outcome data at individual patient and
population level will be required to establish whether the programme has
successfully modified risk of CVD and led to reduced CVD (and all cause)
morbidity and mortality in those individuals.
• at this time, we are not able to capture the results /risk modification outcomes from
lifestyle referrals and activity including;
o Weight loss following referral to and participation in a weight management
programme
Inverse Care Law Report Page 12 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
o Number of people who have quit smoking following referral to Help Me Quit
or other programmes including Community Pharmacy and self-help
o Increased physical activity/weight loss following referral and participation in
the NERS programme or other local programme.
Recommendations
Valuable learning has been gained from undertaking this programme to date. It has
demonstrated an ability to reach more deprived populations, in an effort to mitigate the
effects of poverty on health and close the inequality gap. Despite good uptake and
promising early outputs, there is more work to be done to encourage wider population
engagement with this programme. In addition, greater focus is needed on the availability
and sustainability of support services as well as refining the method of evaluating the
impact of this approach over time.
Recommendation 1:Establish a detailed next phase of the national Inverse Care Law Programme in Wales
that consolidates the model based on the valuable learning to date; the re-focused
programme will inform the Primary Care Strategic Programme and contribute to the
realisation of the prevention vision set out in a Healthier Wales. Progressed by National Inverse Care Law Programme Board by end September 2020
Recommendation 2:Explore the challenges posed by the evaluation of the programme with particular focus
on addressing the weaknesses in the data architecture underpinning the programme.
Progressed by National Inverse Care Law Programme Board, PHW and Swansea University (SAIL) by end December 2019
Inverse Care Law Report Page 13 of 13 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Recommendation 3:Explore opportunities for health economic evaluation of the programme and longitudinal
research drawing on the strength of the SAIL database. Progressed by the National Inverse Care Law Board by March 2020
4.6 Healthy Weights Healthy Wales
1 4.6 Healthy Weights Healthy Wales PCPHPC 10 Feb 2020.docx
AGENDA ITEM
(4.6)
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
HEALTHY WEIGHT:HEALTHY wALES STRATEGY
Date of meeting (10/02/2020)
FOI Status Open/Public
If closed please indicate reason Choose an item.
Prepared by Ann Unitt, Principal Public Health Practitioner
Presented by Executive Director of Public Health
Approving Executive Sponsor Executive Director of Public Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date OutcomeThe public health team convened a multi-agency workshop to inform the health board’s response to the draft HW:HW strategy consultation
27/03/2019 Choose an item.
ACRONYMSHW:HWMECC
Healthy Weight: Healthy WalesMaking Every Contact Count
Healthy Weights: Healthy Wales
Page 2 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
PSBCTMUHBWBFG
Public Services BoardCwm Taf Morgannwg University Health Board Well Being & Future Generations Act
1. SITUATION/BACKGROUND
1.1 Preventing obesity is a complex challenge, with many contributing factors at individual, community and societal levels. The Healthy Weight: Healthy Wales (HW: HW) strategy (Appendix 1) was published on 17 October 2019, having been developed as an outcome of the Public Health (Wales) Act 2017. It sets out a whole system approach to ensure a sustained and long-term approach to prevention, early intervention and support to those who need help.
Healthy Weight: Healthy Wales themes
1.2 It is acknowledged that the strategy cannot be delivered by a single organisation, and it will require strong leadership and commitment from a range of public, private and third sector organisations to achieve change. The strategy will be monitored via five, two-yearly delivery plans from 2020-2030; the first of these will be published in January
Healthy Weights: Healthy Wales
Page 3 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
2020. A National Implementation Board, chaired by the Minister for Health and Social Care, will oversee delivery of the strategy.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 All four themes of HW: HW have implications for the health board.Healthy environments: An increase in the promotion of healthier alternatives and
incentivising products, which support positive choices. Procurement and contracting in the public sector supporting the
purchasing and selling of healthier food and drink. A Refill Nation, where access to free drinking water is commonplace. Healthy settings: All food and drink provision for patients, staff and visitors to adhere
to strict healthy criteria, including within canteens, vending and retail outlets on NHS sites. The public health team have led work on the removal of added sugar drinks from health board and other PSB partners’ premises.
A clear active travel plan for all sites, which will promote easy access and use of sustainable transport links.
Local Health Boards evidencing progress to support health and activity within their workforces, including availability of weight management services for staff.
Healthy people: In terms of prevention, the strategy focuses on early years to ensure
that children are well nourished and start school at a healthy weight. Early years and health care professionals will receive Making Every Contact Count (MECC) training to support parents, carers and families, with a specific focus on diet and nutrition.
Increased support for the promotion of breastfeeding; Cwm Taf Morgannwg has the lowest rates of breastfeeding at birth, 10 days and six weeks in Wales.
The strategy has a range of approaches to support positive behaviour change:
o Health care professionals routinely holding conversations with people and raising the issue about weight sensitively.
o A range of behavioural science informed early intervention weight management support and physical activity based services delivered within local communities, which draw upon local assets for children, families and adults linked through social prescribing.
Healthy Weights: Healthy Wales
Page 4 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
With regard to specialist weight management for adults and children, all health boards will be monitored on their plans to evidence how targeted and specialist services are in place across a clinical obesity pathway; this will be measured and accountable through NHS planning frameworks. The clinical obesity pathway is outlined in Figure 2 below. Health boards will be responsible for the delivery of services at Levels 2 and 3.
Figure 2. Clinical obesity pathway
Leadership and enabling change: Accountability will be built into the NHS planning framework for the
delivery of services. A set of annual indicators will assess delivery. The longer-term focus is to shift the focus of NHS and other public
services towards prevention and wider population health.
Note: The delivery plan 2020-2022 is due to be published in January 2020. It will include: Standards and definitions of the clinical obesity pathway A set of national outcome measures Indicative funding for health boards and partners to support the
delivery of the strategy.
2.2 Obesity context in CTMUHBCTMUHB has among the highest rates of overweight and obesity in adults and children in Wales.
Healthy Weights: Healthy Wales
Page 5 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Source: Public Health Wales Observatory
Source: National Survey for Wales
Source: Child Measurement Programme for Wales
For both adults and children, Bridgend has similar rates of overweight and obesity to the Wales average, whereas Rhondda Cynon Taf and Merthyr Tydfil have statistically significantly higher rates.
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 Across the levels of the current All Wales Obesity Pathway, the health board has: Very limited Level 2 services for adults
Adult obesity numbers in Cwm Taf Morgannwg, by BMI classification
Page 6 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
No Level 3 specialist MDT weight management service for adults. This limits patient access to Level 4 bariatric surgery, as weight management at Level 3 is a pre-requisite.
No Level 2 or Level 3 services for children3.2 The health board is facing increasing costs of obesity related illnesses.
These include: Pharmacological treatments Costs associated with in-patient care Bariatric equipment
3.3 The health board now need to agree: A mechanism for developing and implementing a clinical obesity
pathway for children and families, and adults in Cwm Taf Morgannwg Which directorate(s) will host any weight management services for
children and families, and adults The local governance arrangements for reporting progress to Welsh
governmentA further paper will be submitted to Executive Board for a decision on the above.
4. IMPACT ASSESSMENT
Yes (Please see detail below)
Quality/Safety/Patient Experience implications
HW:HW promotes prevention and early intervention to address obesity and reduce associated ill health, as well as the provision of appropriate services for those who need support to achieve and maintain a healthy weight.
Staying Healthy
Related Health and Care standard(s) If more than one Healthcare Standard
applies please list below:Staff and resources, Effective care.
Not requiredEquality impact assessment completed
Healthy Weights: Healthy Wales
Page 7 of 7 Primary, Community, Population Health &
Partnerships Committee10 February 2020
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
Obesity is placing a large financial burden on our services in clinical service provision, specialist equipment costs and staff health and safety. Investment in prevention and weight management services is a requirement of HW:HW.
Link to Main Strategic Objective To protect and improve population health
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
5. RECOMMENDATION
5.1 The Primary, Community, Population Health & Partnerships Committee are asked to: NOTE the Healthy Weight: Healthy Wales strategy DISCUSS the implications for health board services
4.7 Population Health
1 4.7 PCPHP PHM update 10 Feb 2020_vFINAL.docx
AGENDA ITEM
4.7
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Population health Management: update
Date of meeting 10/02/2020
FOI Status Open/Public
If closed please indicate reason Choose an item.
Prepared by Kimberley Cann, Consultant in Public Health
Presented by Kelechi Nnoaham, Director of Public Health
Approving Executive Sponsor Executive Director of Public Health
Report purpose ENDORSE FOR COMMITTEE APPROVAL
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
Choose an item.
ACRONYMS
CTMUHB Cwm Taf Morgannwg University Health Board
PSRS Population Segmentation and Risk Stratification
Population Health Page 2 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
NWIS NHS Wales Informatics Service
SWIYC Stay Well in Your Community
GP General Practitioner
1. SITUATION/BACKGROUND
1.1 This report provides an update on the population segmentation and risk stratification (PSRS) approach to Population Health Management in Cwm Taf Morgannwg University Health Board (CTMUHB) for the committee to review, discuss and endorse.
1.2 Population Health Management seeks to understand patient populations, groups or clusters by characteristics related to their need and use of health care resources which can help Primary Care Clusters and GPs to decide how best to use limited time and resources to deliver anticipatory and pre-emptive care for patients. Segmenting the population based on a range of factors can identify groups by their holistic need and ability to benefit from anticipatory care.
1.3 The feasibility of the population segmentation and risk stratification (PSRS) approach was previously piloted in the Rhondda primary care cluster. The roll out of this approach forms one workstream of the Stay Well in Your Community (SWIYC) Programme of work supported by Transformation funding by the Welsh Government. The aims and objectives of the workstream are available in Annex A and will form part of a wider Population Health Management strategy for CTMUHB. PSRS supports new models of care being implemented within the other workstreams of SWIYC, in particular, the Enhanced Community Cluster Teams and Assistive Technology. As part of the work, PSRS is being fully evaluated. Progress on implementation across CTMUHB and evaluation is provided in this update.
1.4 There has been an agreement in principal for funding from the Welsh Government to implement this approach across other Health Boards following submission of a Business Case from the National Primary Care Board. This is pending and no further update on this element is provided in this report.
Population Health Page 3 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
Implementation of PSRS for CTMUHB
2.1 Following obtaining permission to utilise primary care data from practices in Merthyr and RCT, a Data Quality Submission application was submitted prior to seeking permission from Bridgend practices, using the same format as for the pilot. The Data Quality Group and GPC Wales requested that roll out of the approach uses data from the SAIL Databank rather than create a new integrated dataset as done in the pilot.
2.2 This approach benefits from the well-developed information governance framework surrounding the SAIL Databank. However, SAIL was developed for research purposes and holds anonymised patient data, in addition it does not currently provide data back to practices. A technical solution (see Figure 1) has been agreed with all partners and the Local Public Health Team (LPHT) are currently working through the technical and legal details and processes that would enable this to happen with partners SAIL, NHS Wales Informatics Service (NWIS) and the commercial provider of the platform through which primary care would access the data - Sollis.
2.3 In summary, the Sollis system will be hosted within the SAIL environment. SAIL will make a location available to host the tool and provide a subset of SAIL data. The PSRS analysis will take place within the SAIL environment using algorithms run by Sollis. Patient level data will only be accessible to GP practices using the Sollis Clarity application, following a de-anonymisation process after the data leaves the SAIL environment.
2.4 The primary care data currently available within the SAIL Databank is available from SAIL consenting practices via Informatica and NWIS who complete the linkage and initial encryption and anonymisation of the data to SAIL. This translates into an anonymised linkage field (ALF) within SAIL which is an encrypted unique patient identifier (ID). This patient ID is completely anonymous and has no meaning to practices or secondary users of practice data. A mapping table will be provided to Sollis which will map the Audit+ patient ID to the clinical system patient ID once the data leaves the SAIL environment. The clinical system patient ID can only be used by practices to identify their own patients and has no meaning to external users outside the practice. SAIL data will therefore remain anonymous but contain an identifier that practices
Population Health Page 4 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
can use in data fed back to the practice. This process will rely on implied consent as the basis for processing at common law as this will be used for direct care purposes.
2.5 Further approval from the Secretary of State via the Confidentiality Advisory Group under Section 251 of the National Health Services Act 2006 will not be required. An application to the Data Quality System (DQS) governance group will be made. Small number suppression will be applied at practice level in line with standard data disclosure processes. This will be lawful at common law without any further approvals. Should any data be identifiable on its own or in combination with other data held in the dashboard at any point in future, a legal basis at common law will be established with the health bodies accessing the data.
2.6 A separate research project has been proposed to be conducted by the LPHT in parallel, and will be submitted and approved via its own separate IGRP application, to enable evaluation using standard SAIL anonymised data. Outputs from SAIL will be aggregated for incorporation into an evaluation report. These will be subject to SAIL standard disclosure controls policy.
2.7 Provision of the intelligence is planned for June 2020. A detailed project plan based on the new data flows is available in Annex B. The full project document agreed with partners is available upon request.
Evaluation
2.8 The potential for using utilisation-based cluster analyses to segment a local General Practice-registered population in the Rhondda cluster was assessed as a pilot during April 2018 – July 2019. A process evaluation assessed the feasibility of the approach and compared the use of a traditional expert-driven segmentation approach with data-driven utilisation analysis. The findings have previously been presented and are available upon request.
2.9 A Principal Public Health Intelligence Analyst has been recruited within the LPHT to lead on evaluation for PSRS, with support from a statistician within Cardiff University. Logic models have been developed in collaboration with Cardiff University. The PSRS workstream aims to evaluate the effectiveness of PSRS in identifying the health and care needs of the CTMUHB primary care-registered population. This is supported by two objectives:
(1) To evaluate the predictive ability of population segmentation.
Population Health Page 5 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
(2) To undertake a process evaluation to inform wider roll out of this approach, to other clusters and to other Health Boards.
2.10 There are three components of the evaluation of the workstream to support these two objectives (see Table 1). The predictive ability of segmentation will be assessed as a separate research project in collaboration with SAIL and is underway. Further analysis of healthcare use post-PSRS implementation will be undertaken in future using SAIL data. Findings from a process evaluation will support quality improvement cycles of the work within CTMUHB and any future roll out of the work across other Health Boards.
2.11 The evaluation does not include evaluation of specific interventions which are implemented using the findings of the segmentation, over and above identifying the added benefit that segmentation offers. For example, the Enhanced Community Cluster MDTs which are being implemented as a separate workstream within the SWIYC programme. These will be evaluated separately. However, this evaluation will work closely with this workstream to ensure any outcomes which support evaluation of segmentation are measured using a prudent, coordinated approach.
Next steps
Continue roll out of PSRS across CTMUHB using the proposed technical solution aiming for provision of data to primary care in June 2020.
Continue evaluation of PSRS and use this to inform delivery. Await a decision from the Welsh Government regarding provision across
Wales.
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
There are none.
4. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Related Health and Care standard(s) Effective Care
Population Health Page 6 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
If more than one Healthcare Standard applies please list below:
No (Include further detail below)Equality impact assessment completed Completed for pilot; currently being
completed for roll out.There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
There is no direct impact on resources as a result of the activity outlined in this report.
Link to Main Strategic Objective To protect and improve population health
Link to Main WBFG Act Objective
Work collaboratively with our public service partners and a broader range of partners to join up health and other services where this potentially represents better value for our residents and care users
5. RECOMMENDATION
5.1 The Primary, Community, Population Health and Partnerships Committee is asked to:
5.2 ENDORSE the approach to Population Health Management outlined in this report.
Population Health Page 7 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Figure 1: Data flow for the proposed technical solution
Population Health Page 8 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Note: this map of data flow does not distinguish between current process that are already in place (data flows from GP to NWIS, and NWIS to SAIL) and processes that will be adapted as part of this project (data flows within SAIL and out to GP and LPHT via the Sollis application (operating within and outside the SAIL environment)). It also does not depict the project actions e.g. IGRP and DQS applications (please see project action plan).
Population Health Page 9 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Table 1: Elements of the evaluation of the PSRS workstream
Evaluation aspect
Timescales Aim(s) Objective(s) Data source(s)
1. Predictive ability of segmen-tation
TBC (as soon as data becomes available – it is hoped this will be prior to June 2020 data provision)
To assess whether and to what extent segmentation can predict future health care use
a) To assess the predictive ability of traditional versus data-driven segmentation in relation to healthcare use (combined settings and individual measures)
b) To determine the rates of transition between segments (stability of segmentation over time) and underlying factors driving this.
c) To assess whether segmentation at cluster or Health Board level is different.
d) To determine whether a new combination of existing variables in the segmentation could improve prediction of future healthcare need.
SAIL Databank
2. Analysis of healthcare use post segmentation and risk stratify-cation implement-tation
TBC (will require a follow-up period of approxi-mately 1 year post-June 2020)
TBC TBC SAIL Databank
3. Process evaluation of implement-tation
Ongoing to support quality improve-ment cycles
To learn from the imple-mentation of PS and use it to inform delivery
a) To assess the feasibility and practicality of using SAIL as a data source
b) To determine the most effective data flow processes
c) To determine whether GP practices can access the outputs of PSRS
d) To estimate the resource demands on GP practices of using this approach
e) To determine whether the LPHT has sufficient information to support primary care clusters in taking action on the outputs from PSRS
f) To determine whether PSRS offers added benefit over population segmentation alone
g) To determine whether the patients identified by PSRS would have been identified without PSRS and any resource implications this may have
h) To establish the resource implications of this approach
TBC - multiple
Population Health Page 10 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
ANNEX A: AIMS AND OBJECTIVES OF THE PSRS SWIYC WORKSTREAM
Aims
a) To undertake population segmentation and risk stratification for the primary care-registered population of CTMUHB using data from the SAIL Databank.
b) To provide GP practices with patient-level identifiable information on the health and care needs of patients registered in their practice using individually-assigned segments and risk stratification scores.
c) To evaluate the effectiveness of population segmentation and risk stratification in identifying the health and care needs of the CTMUHB primary care-registered population.
Objectives
i. To establish the processes by which data will flow in the project.
ii. To set out the roles and responsibilities of all parties collaborating on this project.
iii. To ensure all legal and information governance requirements for data sharing, processing and dissemination are met.
iv. To ensure GP practices are provided with information on the segmentation and risk stratification of individual patients in a format that allows that information to be easily linked to patient records.
v. To ensure the Local Public Health Team (LPHT) are provided with sufficient information to: (1) support GP practices in the interpretation and use of the data; and (2) to consider, advise and/or initiate effective interventions for patient segments and risk strata in their population.
vi. To ensure that this project closely aligns, and that outputs produced are compatible, with any separate research projects undertaken by the LPHT to evaluate the effectiveness of population segmentation and risk stratification.
vii. To undertake a process evaluation to inform wider roll out of this approach, to other clusters and to other Health Boards.
viii. To evaluate the predictive ability of population segmentation.
ANNEX B: PSRS WORKSTREAM PROJECT PLAN
PHM Data ManagementTask No Week beginning - Update as Necessary Owner Start End
Refine Data process inc. Information Governance
DF/NS/AF- Accountable People
R1 Confirm viability of using SAIL AA 04.11.19 04.11.19
R2Produce Project Brief to clarify requirements KC, JK, AG 05.11.19 06.12.19
R3Confirm data flow & technical requirements for using SAIL AA, SH, JP, AF 06.12.19 20.12.19
R4Sign off on data flow and technical requirements KC, SN, DF, AF 20.12.19 20.12.19
R5SAIL /Sollis draw up aligned agreement on access. DF, RL, NS 04.12.19 20.12.19
R6Complete & submit application to SAILs IGRP KC, JK 20.12.19 17.01.19
R9 Gain approval of SAILs IGRP SAIL IGRP 10.04.20 10.04.20After approval R9 – the SAIL Analytical Services Team will need to provision the data within the IGRP and filter and clean/prepare it based on the Sollis requirements. The initial element is up to 30 days, the latter will dependant on the contents of the document and Sollis data ingest requirements.
SAIL Analytical Services Team
R10Complete the CTMUHB Data Impact Assessment KC, JK 17.01.20 14.02.20
R11 Gain approval of the CTMUHB DIA KC, JK 14.02.19 10.04.20
R12Update existing Data Disclosure Agreements in line IGR Panel KC, JK 14.02.20 10.04.20
R13Draft Data Disclosure Agreements for Bridgend KC, JK 14.02.20 10.04.20
R14 Gain sign offs for Rhondda EC, JK 13.04.20 14.05.20
R15 Gain sign offs for Cynon North EC, JK 13.04.20 14.05.20
R16 Gain sign offs for Cynon South EC, JK 13.04.20 14.05.20
R17 Gain sign offs for Taff Ely EC, JK 13.04.20 14.05.20
R18 Gain sign offs for Merthyr EC, JK 13.04.20 14.05.20
R19 Gain sign offs for Bridgend EC, JK 13.04.20 14.05.20
Population Health Page 12 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
R20Make new application to the NWIS DQS Gov Group
KC, JK 14.05.20 31.05.20
R21Gain approval from the NWIS DQS Gov Group KC, JK 14.05.20 31.05.20
Implement Refined Data Process
DF/NS/KC/JK - Accountable People
IM1SAIL grant Sollis access to the SAIL environment
SAIL Analytical Services Team 10.04.20 17.04.20
IM3SAIL format/clean data to allow ingest
SAIL Analytical Services Team 10.04.20 01.05.20
IM2
SAIL provision data to requirements of the Sollis Tool, and enable access to Sollis named analyst
SAIL Analytical Services Team 01.05.20 On going
SAIL to setup environment and config for Sollis Tool
SAIL Technical Team
IM4Sollis/SAIL set up the Sollis Tool inside SAIL
JP, SAIL Technical Team 10.04.20 01.05.20
IM5Sollis build the data processing functionality as per agreed brief. JP 01.05.20 15.05.20
IM6
Sollis conduct technical testing to demo full functionality inc Clarity, with SAIL support JP 15.05.20 20.05.20
IM7Any Test issues will be addressed
JP, SAIL Technical Team 20.05.20 22.05.20
IM8
Sollis conduct testing to demo the processing/access via Clarity in situ/pilot surgeries, with SAIL support JP 25.05.20 27.05.20
IM9Any Test issues will be addressed
JP, SAIL Technical Team 27.05.20 29.05.20
IM 10
Sollis will conduct user acceptance and gain sign off JP 01.06.20 05.06.20
IM11
Any Test issues will be addressed JP, SAIL Technical Team 03.06.20 05.06.20
IM12
The system to run with the first Qtrly data to be processed in June 2020 JP 08.06.20 ON GOING
Key to Initials Initial Name Organisation DF David Ford SAIL RL Ronan Lyons SAIL
Population Health Page 13 of 13 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
AA Ashley Akbari SAIL SH Sharon Heys SAILSAT SAIL Analystical Services Team SAILSTT SAIL Technical Team SAILNS Nigel Slone Sollis JP Jaivir Pall SollisAF Andrew Fletcher NWIS KC Kim Cann LPHTJK Julie Kelly LPHTAG Andrea Gartner LPHTEC Emma Cahill LPHT
1 4.7.1 Population Health Update PCPHPC 10 February 2020.docx
AGENDA ITEM
4.7.1
CTM MANAGEMENT BOARD
PoPulation Health in cwm Taf Morgannwg
Date of meeting (10/02/2020)
FOI Status Open/Public
If closed please indicate reason Choose an item.
Prepared byEmma Cahill (Principal Public Health Practitioner) and Sara Thomas (Consultant in Public Health)
Presented by Kelechi Nnoaham Executive Director of Public Health
Approving Executive Sponsor Executive Director of Public Health
Report purpose FOR DISCUSSION / REVIEW
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
Choose an item.
ACRONYMSDALYsCVDLTCMECCPHM
Disability adjusted life yearsCardiovascular diseaseLong term conditionsMaking Every Contact CountPopulation Health Management
Population Health Page 2 of 3 Primary, Community, Population Health &
Partnerships Committee10 February 2020
1. SITUATION/BACKGROUND
1.1 Population Health is an approach aimed at improving the health and wellbeing of an entire population, while reducing health inequalities. This includes the health outcomes of a group of individuals, including the distribution of such outcomes within a group. To achieve this, actions and interventions are required to reduce the occurrence of ill health, deliver appropriate health and care services as well as target the wider determinants of health.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 The purpose of this paper to provide a common definition and understanding of Population Health. The paper will set out what population health means, what we currently deliver to improve population health and next steps to further adopt a population health approach across Cwm Taf Morgannwg (CTM). This will allow for partners to develop a common understanding of the terminology used and vison for improving Population Health outcomes.
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 Ensuring a common understanding of Population Health across the system ensures a coordinated approach to tackling inequalities in health.
3.2 This paper outlines the opportunities available to Cwm Taf Morgannwg to adopt a Population Health approach, for which requires Committee support.
4. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Staying HealthyRelated Health and Care standard(s) If more than one Healthcare Standard
applies please list below:
Population Health Page 3 of 3 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Not requiredEquality impact assessment completed
Yes (Include further detail below)
Legal implications / impact Elements of the Public Health Act included in the paper (pg. 9) have legal obligations for the Health BoardThere is no direct impact on resources as a result of the activity outlined in this report.
Link to Main Strategic Objective To protect and improve population health
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
5. RECOMMENDATION
5.1 The Primary, Community, Population Health & Partnerships Committee are asked to:
5.2 NOTE the current work, as well as support opportunities to further adopt the definitions of Population Health and to ensure a Population Health approach is adopted.
1 4.7.2 Population Health in Cwm Taf Morgannwg PCPHPC 10 February 2020.docx
Population Health in Cwm Taf MorgannwgA paper for Primary Care, Population Health and Partnerships Committee
Purpose The purpose of this paper is to provide a common definition and understanding of Population Health. The paper will set out what Population Health means, what we currently deliver and next steps to further adopt a population health approach across Cwm Taf Morgannwg. This will support partners to develop a common understanding of the terminology used, and vison for improving Population Health outcomes.
Definition of termsHealth: A person's physical and mental condition relates to their health. Wellbeing is the subjective state of being healthy, happy, contented, comfortable and satisfied with one's quality of life. Mental wellbeing relates to a person's emotional and psychological wellbeing. It also includes being able to develop potential, work productively and creatively, build strong and positive relationships with others and contribute to the community.
Population Health: Population Health is an approach aimed at improving the health and wellbeing of an entire population, while reducing health inequalities. This includes the health outcomes of a group of individuals, including the distribution of such outcomes within a group1. To achieve this, actions are required to reduce the occurrence of ill health, deliver appropriate health and care services as well as target the wider determinants of health.
Public Health: The public health system looks to support people to live healthily (such as smoking cessation, weight loss support and sexual health services) as well as some elements of what the NHS delivers (such as immunisation and vaccination against preventable diseases). The public health profession is trained to plan, design and deliver preventive policies and interventions.
Population Health Management utilises data in the planning and delivery of health care to improve population health outcomes. This includes techniques such as population segmentation and risk stratification to identify groups at risk of ill-health to focus specific interventions. This approach looks to ensure the appropriate allocation of resources to different groups of patients as required.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
1
1. What is Population Health?Population Health has been defined as ‘the health outcomes of a group of individuals, including the distribution of such outcomes within a group1. Health outcomes include measures such as mortality, life expectancy, morbidity, disability adjusted life years (DALYs) and health related quality of life. These outcomes vary across the population depending on a number of factors including; age, sex, socioeconomic status and geography. By focussing on the specific needs of different population groups we can improve population health outcomes across Cwm Taf Morgannwg University Health Board (CTMUHB).
People living in more deprived areas have poorer health outcomes than those living in less deprived areas, this is termed an inequality. The Kings Fund Population Health2 report identifies socio-economic and environmental determinants of health as the primary drivers for health, followed by health behaviours; socio-economic factors such as income, accounting for 50% of health outcomes. Within Cwm Taf Morgannwg there is a 6.4 years difference in life expectancy for men and a 5 year difference for women between those living in the most and least deprived areas (figure 1)
Figure 1. Life expectancy and gap in life expectancy in Cwm Taf Morgannwg 2015-17 Source: Public Health Observatory
The factors which lead to these inequalities are not just related to the decisions people make or healthcare they receive, but a number of external factors. The wider determinants of health, as presented by Dahlgren and Whitehead’s model (1991)3 which maps the relationships between the individual, their environment and their health. With the individual at the centre, surrounding them are the various external factors which impacts on health. This highlights that the choices a person makes regarding their health is influenced by a range of factors including living and working conditions, access to services, health literacy, family influence as well as legislation. A number of the factors are outside of on an individual’s control.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
2
Figure 2 presents the Dahlgren and Whitehead model and highlights the population health impacts of such wider determinants on health. People living in deprived areas are disproportionately affected by the negative impact of these wider determinants.
Figure 2. The population health impacts in relation to the wider determinants model (4,5,6,7)
Achieving good Population Health outcomes is not just the role of the National Health Service (NHS). Taking a Population Health approach, the whole system around and including the individual or citizen must work together to improve wellbeing as well as reducing the risk of ill-health.
2. Background to Population Health in CTMUHBThe need for a Population Health approach in Cwm Taf Morgannwg was identified in the Director of Public Health’s Fifth Wave Annual report (2016/17). Urging an agreement across partnerships to define a common direction of travel, to harness collective resource and maximise opportunities in new and innovative ways; ensuring that the whole society contribution is greater than the sum of its parts. This led to three key elements to improving the health and wellbeing of people in Cwm Taf Morgannwg (figure 3).
Environment: areas with more accessible green space are associated with better mental and physical health among the local population and with reducing the impact of income inequalities
Employment: Unemployment leads to a higher rate of mortalitythrough cardio vascular disease, lung cancer and suicide1
Housing: death rates rise by 2.8% for every Celsius-degree drop in the external temperature for those in the coldest 10% of homes, compared with 0.9% in the warmest homes.1
Individual Lifestyle factors: The Caerphilly Cohort Study found that if a population of men adopted four or five healthy behaviours it would reduce their rates of diabetes and vascular disease by 69% each, dementia by 58% and cancers by 33%.
Education: four more years of
education reduces mortality rates by 16% and reduces the risk of heart
disease and diabetes
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
3
Figure 3: Society wide approach to wellbeing
In the three years since its publication, progress has been made in each area and continues.
2.1 Strategic plan for Population Well-beingThe Wellbeing of Future Generations Act required each Local Authority in Wales to undertake a Wellbeing Needs Assessments and develop Wellbeing Plans to improve the health and wellbeing of the local population. Across Cwm Taf Morgannwg there are two plans with identified priority areas:
- The Cwm Taf Wellbeing Plan (2018-23) prioritises tackling loneliness and isolation, ensuring thriving communities, healthy people and a strong economy.
- The Bridgend Public Services Board Wellbeing Plan whose priorities include; ensuring the best start in life, supporting communities to be safe and cohesive, reducing social and economic inequalities and supporting healthy choices in a healthy environment.
Both plans involve a range of organisations as well as the communities themselves to address a number of wider determinant of health. It is anticipated that updates on actions within the plans will be provided to the committee.
2.2 Population Health ManagementOver the past two years, the use of population segmentation and risk stratification techniques have been piloted within the Health Board. This consists of 3 elements of work:
1. Analysis of the Rhondda population using population segmentation and risk stratification to segment the population by health care usage
2. Roll out of the analysis across CTMUHB as part of the Transformation programme
3. Agreement in principal for funding from the Welsh Government to implement this approach across other Health Boards
Further updates on progress will be provided to the Committee.
2.3 Well-being Research FrameworkIt is essential that actions undertaken to improve the well-being of the population are evidence-based. Research is a useful tool to develop and test theories for what might work and demonstrate that we are using funding effectively. The Population Well-being
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
4
Research Framework aims to address gaps in our knowledge around understanding our population and addressing key population health challenges. Developing the framework involved extensive stakeholder engagement and prioritisation methodologies.
3. Health outcomes in Cwm Taf Morgannwg population
In addition to inequalities in life expectancy between geographical areas, inequalities are also apparent in specific health topics, from lifestyle behaviours to chronic conditions and disease.
3.1 Lifestyle behavioursThe lifestyle behaviours of an individual can reduce the risk of ill-health and disease. Healthy behaviours for good health and wellbeing include not smoking, being physically active, eating a healthy diet, not exceeding alcohol guidelines and maintaining a healthy weight. Supporting the population to adopt healthy behaviours can reduce the risk of a number of long term conditions, shown in figure 4
Figure 4. Link between behaviours and ischemic heart disease7
If the population adopt four or five of the health behaviours rates of diabetes, heart disease, dementia and cancers would be reduced7. Figure 5 shows the percentage of adults reporting fewer than two behaviours, showing all local authority areas within Cwm Taf Morgannwg are above than the Welsh average. Meaning that a higher proportion of our population adopt less than two behaviours and increase their risk of ill health.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
5
Figure 5 Percentage of adults who reported fewer than 2 healthy lifestyle behaviors (National Survey for Wales, 2019)
Of all of the behaviours, smoking has been identified as the most predominant behavioural risk factor in the contribution to disability adjusted life years8(DALYs). Smoking prevalence in Wales ranges from 11% in the least deprived fifth, to 28% in the most deprived fifth, showing an inequality which will further widen the population health outcome gap.
Figure 6. Percentage of adults who smoked or used e-cigarettes, 2017-18 and 2018-19(Source: National Survey Wales)
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
6
Figure 6 shows the high prevalence of smoking within Cwm Taf Morgannwg and it has been shown that 75% of lung cancer cases in Wales are attributable to smoking9. People identified as living in the most deprived quintile of Wales are 2.5 times more likely to be diagnosed with lung cancer when compared to those living in the least deprived quintile10. Data showing the incidence of lung cancer shows Cwm Taf Morgannwg to be the highest across Wales, high levels of deprivation as well as high smoking rates may explain this pattern.
3.2 Long term conditions and diseaseLifestyle behaviours are just one factor that can lead to ill health, many others impact on individual health. This is shown by the Global Burden of Disease Study11, which identifies the common factors that contribute to DALYs for certain conditions. Figure 8 shows three examples, for chronic respiratory disease, smoking is identified as the primary risk factor accounting for 66% of all DALYs related to the condition. However, occupation risk and air pollution together can account for over 20%.
Figure 8 Global burden of disease identified risks for three causes with the largest attributable DALYs, percentage, all persons, all ages, Wales, 2016. Source: Public Health Wales Observatory using Global Health Data Exchange.
In addition to single long term conditions, co-morbidities must also be considered. This is where an individual has more than one long term condition. The Rhondda population segmentation pilot identified that over half of the population (53%) in the Rhondda cluster had one or more long term conditions (LTC). Of those with a LTC, 31% had two or more. For example, of the patients with COPD, 94% also had at least one other LTC.
This analysis also identified the cost of such conditions on the local health care systems. It was found that the degree of multi-morbidity was a greater driver of cost than age in the population. By taking a preventative approach to population health, Cwm Taf Morgannwg can reduce the risk of developing long term conditions by supporting individuals and communities to adopt and maintain a healthy lifestyle from an early age.
4. Existing Population Health interventionsAcross organisations in Cwm Taf Morgannwg there are already a large number of interventions in place to support the population to live a healthy lifestyle and further improve their health and wellbeing. Some interventions, such as education in schools, focus on primary prevention, such as stopping people starting smoking, to secondary prevention such as the Health Check programme identifying patients which may be pre-diabetic to receive lifestyle advice to reduce the risk of diabetes developing. Figure 9 shows some examples of interventions in place, of which there are many more, such as
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
7
the many community groups and activities which support a healthy lifestyle as well as organisations such as housing associations and the interventions they undertake to support residents.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
8
Figure 9. Examples of population health interventions already in place across Cwm Taf Morgannwg
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
9
There are a number of ways to classify population health interventions; in figure 9 they have been classified by lifestyle behaviour and the setting in which they are delivered. As such, some interventions which encompass a range of topics and settings are not presented, these include:
Making Every Contact CountMaking Every Contact Count (MECC) is an approach to behaviour change that supports staff to more routinely and effectively incorporate health behaviour change conversations into their interactions with other people. These conversations, based on brief advice and brief intervention methodology, help support individuals to make positive changes to their lifestyle by empowering them to consider the changes that they want to make, as well as how they may achieve them. As part of this, individuals are signposted and referred to avenues of local support.
The Inverse Care Law programme (Health Checks)The Health Checks programme invites members of the public aged 40-74yrs at risk of cardiovascular disease, who are not already on a CVD register, into practice to review their health and wellbeing. A partnership between Primary Care and Public Health, this provides an opportunity for individuals to discuss lifestyle choices and also looks to identify any health concerns which may require further investigation. Named the Inverse Care Law, the programme looks to intervene and support those in need to reduce the gap in inequalities. Updates on this programme will be provided to the committee.
Social PrescribingThere is increasing acceptance that sources of support in local communities have an important role to play alongside clinical care or even as an alternative in improving health and wellbeing. Social prescribing can reduce social isolation and loneliness, improve individual emotional and physical wellbeing. The Cwm Taf Morgannwg Social Prescribing group will work collectively across statutory and third sector organisations to realise the potential of social prescribing, enabling citizens to build or re-build friendships, community connections and a sense of belonging to reduce isolation and improve wellbeing.
4.2 The role of Welsh Government and Policy on local deliveryThe outer most circle of figure 9 highlights the policies/interventions of Welsh Government and local statutory organisations. Welsh Government has the authority to set aspects of health and wellbeing service delivery into law. Two Acts have been passed which highlight Welsh Government’s use of legislation as tool to improve Population Health, the role of local organisations is to ensure that these are met and delivered.
Wellbeing of Future Generations (Wales) Act 2015The Well-being of Future Generations (Wales) Act requires public bodies to think about the long-term impact of their decisions, to work better with people, communities and each other, and to prevent persistent problems such as poverty, health inequalities and climate change. Public bodies are required to ensure that when making decisions they
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
10
take into account the impact they could have on people living their lives in Wales in the future, using the 5 sustainable development principles:
- Long Term: The importance of balancing short term needs with the need to safeguard the ability to also meet long term needs
- Prevention: How acting to prevent problems occurring or getting worse may help public bodies meet their objectives
- Integration: Considering how the public body’s well-being objectives may impact upon each of the well-being goals, on their other objectives, or on the objectives of other public bodies.
- Collaboration: Acting in collaboration with any other person (or different parts of the body itself) that could help the body to meet its well-being objectives.
- Involvement: The importance of involving people with an interest in achieving the well-being goals, and ensuring that those people reflect the diversity of the area which the body serves.
Public Health (Wales) Act 2017The Public Health (Wales) Act aims to address a number of specific public health concerns, and to create social conditions that are conducive to good health and where avoidable harms can be prevented. It includes provisions relating to obesity, tobacco, intimate piercing, health impact assessments, pharmaceutical services, and toilets for public use. The Welsh Government has emphasised that the Public Health (Wales) Act is intended to sit alongside a broader suite of actions for improving public health. Examples of identified actions include:
- Part 3 Tobacco: re-states restrictions on smoking in enclosed and substantially enclosed public and work places. Additionally, it places restrictions on smoking in outdoor care settings for children, school grounds, hospital grounds and public playgrounds to contribute to the de-normalisation of smoking.
- Part 6 Health Impact Assessments: The Act places a duty on the Welsh Ministers to make regulations which require public bodies to carry out health impact assessments in specified circumstances
- Part 7 Pharmaceutical services: Anyone wishing to provide NHS pharmaceutical or dispensing services must apply to the relevant Health Board for inclusion on that Health Board’s pharmaceutical list. Under the Act, Health Boards will be required to prepare and publish ‘pharmaceutical needs assessments’ for their areas.
Both the Wellbeing of Future Generations (Wales) Act and Public Health (Wales) Act both provide a national context and requirement for the local delivery of Population Health.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
11
5. Population Health OpportunitiesTo continue to drive a shift towards a population health approach, opportunities must be sought to continue to deliver preventative services sustainably, ensuring they are accessible to all. Opportunities to further support Population Health in Cwm Taf Morgannwg include:
- Integrating the Welsh Government Prevention and Early Years funding into service delivery
- A continued partnership approach across Cwm Taf Morgannwg- Use of Population Health Management tools, such as population segmentation,
to ensure services meet the specific needs of population groups.
5.1 Prevention and early years fundingThe need to focus on prevention specifically has been raised at the NHS Wales Collaborative Leadership Group. The Welsh Government definition of prevention is “working in partnership to co-produce the best outcomes possible, utilising the strengths and assets people and places have to contribute.” This led to the multi-agency Building a Healthier Wales Programme Board and discussion paper, proposing the following priority areas of focus across Wales:
- Tackling the wider determinants- Ensuring the best start in life: optimising early years- Enabling healthy behaviours- Minimising the impact of clinical risk factors- Enabling transformational change
A partnership approach was taken to identify areas in need to offer support for sustainability which the funding may bring, as well as opportunities for innovation in areas of need. This funding has proposed the following areas of work:
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
12
PREVENTION AND EARLY YEARS FUNDINGTackling the wider determinants of healthTo meet this priority, partners across Cwm Taf Morgannwg will:
- Complement the Health Board Transformation Programme Enhanced Community Cluster Team by funding community assets to meet the gaps in provision identified to support social prescribing.
- Take a coordinated approach to tackle housing as a wider determinant of health, including undertaking a rapid health needs assessment, reduce inequalities in access to health services, and explore interventions to promote housing improvements for people with respiratory health conditions.
Ensuring the best start in life: optimising our early yearsTo meet this priority, partners across Cwm Taf Morgannwg will:
- Deliver the Bump-start programme across Cwm Taf Morgannwg supporting pregnant women who are obese to ensure healthy weight gain during pregnancy.
- Support pregnant smokers to quit through 1-2-1 support through the roll out of the MAMMS programme across Cwm Taf Morgannwg.
- Develop and implement the CHOICE programme for vulnerable women to access contraceptive and sexual health services through an outreach service.
- Support community interventions for play to increase the opportunities to deliver free, unstructured play.
Enabling healthy behavioursTo meet this priority, partners across Cwm Taf Morgannwg will:
- Deliver the MECC programme to PSB and RPB partners, ensuring healthy conversations take place across the system and not solely within the Health Board.
- Deliver the Help Me Quit: In hospital service (and mental health services) across Cwm Taf Morgannwg, providing further smoking cessation support alongside community and pharmacy services.
Minimising the impact of clinical risk factorsTo meet this priority partners across Cwm Taf Morgannwg will:
- Pilot the development of an integrated chronic disease prevention programme (based initially on diabetes prevention), to include the implementation of a pre-diabetes intervention within primary care as well as case-finding of adults at high risk of type 2 diabetes based on NICE guidelines.
- Develop and implement a childhood obesity prevention programme, to include a communication intervention to share key public health messages with the population, and a family-based obesity prevention programme to stimulate positive behaviour change.
These programmes will be delivered across Cwm Taf Morgannwg together with partners and will be closely monitored and scrutinised by the Regional Partnership Board as well
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
13
as updates provided to the Primary Care, Population Health and Partnerships Committee.
5.2 Continued Partnership approachesTo ensure population health is integrated across the whole system we must continue to take a partnership approach. This can be achieved strategically through partnership groups such as the Public Service Board and Regional Partnership Board. Health Board programmes relating to Population Health will also be scrutinised by the Primary Care, Population Health and Partnerships Committee.
Over the past two years, a preventative focus had also been integrated into the Health Board Directorates’ Integrated Medium Term plans (IMTPs). Directorates are allocated Public Health partners to support the integration of preventive actions into their plans. This includes actions from supporting staff health and wellbeing, and promotion of the staff flu campaign, to ensuring high quality public health messages are available to patients by embedding a MECC approach.
5.3 Taking a Population Health Management ApproachHealthcare services were identified by Dahlgren and Whitehead as a wider determinant of health. It has been widely accepted that this accounts for approximately a 15% contribution to individual health. However, evidence has been presented that if healthcare services were focussed on prevention and population health approaches, this could be increased to up to 43%. Population Health Management is one approach to support a healthcare system to deliver population health.
Over the past 2 years Cwm Taf Morgannwg has piloted the use of population segmentation and risk stratification in the Rhondda Population. This has resulted in a number of population groups each with different needs based on healthcare usage. By better understanding these healthcare needs, services can be more effectively tailored to increase the opportunity of improve health outcomes.
Over 2020, population segmentation will be undertaken across the Health Board to provide insight to all primary care clusters as part of the primary care transformation strategy. However, this is just one use of the tool; by understanding the characteristics and needs of the remaining population groups, evidence based interventions can be developed and targeted. Figure 12 is an example of a population health management system; in the case of transformation, segmentation provides a tool to identify the top segment of the population for which a multi-disciplinary approach (MDT) has shown to be beneficial.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
14
Figure 12. A Population Health Management approach to health care planning
Further analysis and evidence reviews focused on remaining segments will result in additional interventions. Figure 12 identifies the ‘early loss of health’ population group. With the understanding that people often experience more than one long term condition, interventions may focus on a patient centred multi-morbidity service, resulting in patient centred care as opposed to attending different health services for each condition experienced.
SummaryThis paper has provided an overview of what Population Health means as well as providing examples of actions already in place to improve population health outcomes across Cwm Taf Morgannwg. It is recognised that our communities still presents poor health outcomes. The opportunities identified provide a preventative approach to ensure sources are fully utilised and target those in need to reduce health inequalities.
The Wellbeing of Future Generations (Wales) Act identifies the five principles of working, one of which is Involvement. We must be sure to involve and engage the population in Cwm Taf Morgannwg. Both to ensure services meet their specific needs but also to encourage a culture of wellbeing. As identified by the multi-agency social prescribing group, our communities can provide the opportunities to reduce isolation, re-connect individuals and improve health and wellbeing and in doing so increase Population Health outcomes.
Population Health in Cwm Taf MorgannwgPrimary Care, Population Health and Partnerships Committee (10th February 2020)
15
Recommendations- The committee to agree and adopt the definitions of Population Health- Note the current work, as well as support opportunities to further adopt a
Population Health approach- Agree to scrutinise future papers to this committee to ensure a Population Health
approach is adopted
References1 Kindig, D., & Stottart, G. 2002. What is population health. American Journal of Public Health, 93: 380-3832 The Kings Fund, 2018. A vision for population health. Available at https://www.kingsfund.org.uk/publications/vision-population-health3 Dahlgren, G. and Whitehead, M. Policies and strategies to promote social equity in health. 1991. Stockholm: Institute for Policy Studies4 Royal College of Physicians and Royal College of Paediatrics and Child Health (2016). Every breath we take: the lifelong impact of air pollution. Available at https://www.rcplondon.ac.uk/projects/outputs/every-breath-we-take-lifelong-impact-air-pollution5 Public Health England and Institute of Health Equity (2015). Psychosocial pathways and health outcomes: Informing action on health inequalities. Available at: http://www.instituteofhealthequity.org/resources-reports/psychosocial-pathways-and-health-outcomes-informing-action-on-health-inequalities6 National Institute Clinical Excellence (2015). Excess winter deaths and illness and the health risks associated with cold homes (NG15). Available at: https://www.nice.org.uk/guidance/ng6
7 Elwood P, Galante J, Pickering J, Palmer S, Bayer A, Ben-Shlomo Y, et al. (2013) Healthy Lifestyles Reduce the Incidence of Chronic Diseases and Dementia: Evidence from the Caerphilly Cohort Study8 Benzige., C Roth, G.,& Moran, a., 2016 The Global Burden of Disease study and preventable burden of NCD. Available at: https://doi.org/10.1016/j.gheart.2016.10.0249 Brown et al, (2018). The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. British Journal of Cancer, 118(8), pp.1130-114110 Welsh Cancer Intelligence and Surveillance Unit, Health Intelligence, Public Health Wales, 201611 Benzige., C Roth, G.,& Moran, a., 2016 The Global Burden of Disease study and preventable burden of NCD. Available at: https://doi.org/10.1016/j.gheart.2016.10.024
4.8 Influenza Programme Report
1 4.8 Influenza Update PCPH&PC 10 February 2020.docx
AGENDA ITEM
4.8
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
INFluenza UPDate JaNuary 2020
Date of meeting 10/02/2020
FOI Status Open/Public
If closed please indicate reason Choose an item.
Prepared by Claire Beynon, Consultant in Public Health
Presented by Claire Beynon, Consultant in Public Health
Approving Executive Sponsor Executive Director of Public Health
Report purpose FOR DISCUSSION / REVIEW
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(Insert Name) (DD/MM/YYYY) Choose an item.
ACRONYMS
Influenza Update Page 2 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
1. SITUATION/BACKGROUND
Immunisation is one of the most successful and cost-effective health protection interventions and is a cornerstone of public health.
High immunisation rates are key to preventing the spread of infectious disease, complications and possible early death among individuals and protecting the population’s health through both individual and herd immunity.
It is widely acknowledged that vaccination programmes have an enormous positive economic impact. Though vaccines require funding, they lead to long-term savings through reduction in health costs and avoidance of loss of productivity from the workforce. Estimates of the savings from vaccination are in the order of tens of billions of pounds (Royal Society of Public Health, Moving the Needle 2018).
Cwm Taf Morgannwg University Health Board (CTMUHB) is responsible for the delivery of influenza vaccinations to protect the health of the local population. This is an extensive programme to immunise the following groups:
children over the age of 6 months with a long-term health condition children aged 2 and 3 years children in primary school adults over 65 years pregnant women anyone with a serious long-term health condition, e.g. chronic
respiratory diseases, heart disease, kidney disease, liver disease, neurological conditions, diabetes and people with obesity
There are several Welsh Government targets for influenza vaccinations: 75% uptake for those aged 65 years and older 75% uptake for pregnant women 55% uptake for those aged six months to 64 years in clinical risk group 60% uptake for healthcare workers providing direct patient care
Cwm Taf* has never met any of these targets and did not meet any of the targets for influenza vaccination in 2018/19, as outlined below in Table 1.
Table 1: Influenza targets and performance for Cwm Taf* (2018/19)Welsh Government targets for influenza Target Actual
(2018/19)65 years and older 75% 67.1%Pregnant women 75% 54.0%6 months to 64 years in clinical risk groups 55% 40.0%Healthcare workers providing direct care 60% 50.9%
Influenza Update Page 3 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
*note all data for Cwm Taf area only in 2018/19
In 2019 a strategic review of the immunisation programme was undertaken and this provided a comprehensive review of the current service and a series of recommendations for improvement over the next three years. The implementation of the actions recommended commenced immediately to deliver improvements.
2.SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
This year the programme across the UK has been plagued by difficulties in obtaining the influenza vaccinations due to issues with supply from the pharmaceutical companies. The delivery of supplies to GP practices, pharmacists, the health board (for staff) and the school nursing team (for children) have all been disrupted and delayed this season. Despite this the influenza vaccine has been delivered to the target groups.
This report gives the latest data on the Cwm Taf Morgannwg status against the national influenza immunisation uptake targets (based on the latest available information -January 2020), see Table 2 for summary figures.
Table 2: Influenza targets and actual performance for Cwm Taf Morgannwg in 2019/20 as at January 2020 (season not complete)Welsh Government targets for influenza Target Actual 65 years and older 75% 66.9%Pregnant women 75% *6 months to 64 years in clinical risk groups 55% 37.0%Healthcare workers providing direct care 60% 60.3%
*note- no data available yet, this is determined by point of delivery survey in January each year.
The improvement in the healthcare workers providing direct care to meet the target is pleasing, and is based on several factors, greater impetus from the Director of Nursing and Heads of Nursing and the move away from only providing occupational health led influenza vaccination clinics to the peer vaccinator model (staff vaccinating other members of staff), which brings vaccinators to every area of the health board, and specifically to front line staff. Cwm Taf Morgannwg is the first health board to meet the frontline healthcare workers target this year, see Table 3.
Influenza Update Page 4 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Table 3: Uptake of influenza immunisation in Welsh Health Board and NHS Trust staff until the end of December 2019
The need to deliver additional training to the peer vaccinators has however had consequences on the demands on the small core immunisation team. For example in 2018/19 26 peer vaccinators were trained and in 2019/20 this increased to over 200. This has limited time for the other activities. In previous years members of the core immunisation team have gone out to visit GP practices that are not meeting the influenza target to work with them to develop actions that boost uptake, this has not been possible this season due to the increased demands on the core immunisation team and the increased numbers of GP practices, health visitors, school nurses and peer vaccinators which are requiring support (e.g. queries and questions on supply issues; review of clinical incidents etc.). This can be seen in the data for GP practices in Cwm Taf Morgannwg in Table 4.
Table 4: Uptake of influenza immunisation in patients aged 65y and older and in those aged 6m to 64y at clinical risk (12/01/2020).
Influenza Update Page 5 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
The schools programme is a success story and should be celebrated. It is more extensive in Cwm Taf Morgannwg than in other health board areas as children aged 3 years who are at nursery school are included as standard (except in Bridgend where roll out is expected in 2020/21). The schools programme has been particularly successful in Cwm Taf Morgannwg, as can be seen in Table 5 where Cwm Taf Morgannwg leads the health boards in terms of uptake. The careful planning and engagement of schools by the school nursing team is to be commended.
Table 5: Uptake of influenza immunisation in primary school children aged 4-10y (data up to 18/12/2019)
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
The complexity, distributed nature and extensiveness of the vaccinations and immunisations programme requires thorough oversight and co-ordination to
Influenza Update Page 6 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
reduce healthcare harm. This season more than 117,580 vaccines have been provided by hundreds of Cwm Taf Morgannwg employees in primary and secondary care at hundreds of locations including GP practices, schools and nurseries.
This extensive immunisations programme, which extends far beyond just influenza vaccination is coordinated by a small core team consisting of a part-time Band 7 Immunisation Coordinator (2 days per week) a Band 6 Immunisation Nurse (4 days per week) and a Band 3 administrator (2.5 days per week). The additional workload that the team are now responsible for with the boundary change has not been able to be absorbed by the team and this is a risk to the organisation in not being able to provide sufficient support to deliver services of high quality across the whole patch. No additional resource has been applied to the team since the boundary change. There is an urgent need to increase the staffing in this team in order to cope with the additional demands placed on the team which is affecting staff well-being. The team has been under severe pressure this season and as a result the current staff are seeking alternative roles.
It is recommended that the core immunisation team should be expanded, to add capacity to cope with:• the complexity of the programme and aspirations to achieve the targets
set by the Welsh Government.• the additional workload arising from the Bridgend merger.
This should include funding to make the Immunisations Coordinator full time (i.e. increase of 0.6 WTE). Further support for the additional primary and secondary care services administering vaccinations is required from an additional full time Band 6 Immunisation Nurse Facilitator, and in addition a further 0.6 Band 3 administrator is required to manage the increased liaison with the directorates that needs to result of the drive to empower the directorates to take the lead for staff influenza uptake, and provide regular and timely information to primary and secondary care.
Staff cost (including on costs)0.6 Band 7 Immunisation Co-ordinator £28,4021.0 Band 6 Immunisation Nurse Facilitator £40,6560.6 Band 3 Administrator £13,883TOTAL Annual costs £82,941
4. IMPACT ASSESSMENT
Influenza Update Page 7 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Yes (Please see detail below)
Quality/Safety/Patient Experience implications
Staff must be trained regularly to ensure compliance and maintain competence in vaccination procedures and management of any adverse reactions.Vaccinating healthcare workers offers protection to vulnerable patients, especially neonates, paediatrics and pregnant mothers.
Staying Healthy
Related Health and Care standard(s)
If more than one Healthcare Standard applies please list below: Staff and Resources –staff absences due to flu and colds in 2018/19 cost the health board more than £500,000 Safe Care – staff must be competent to deliver vaccinations this requires training
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
This report raises the risks associated with the limited capacity of the team to deliver all the support services required. The cost to bring staffing to a level able to cope with existing demand is £82,941.
Link to Main Strategic Objective To protect and improve population health
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
Influenza Update Page 8 of 8 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
5. RECOMMENDATIONS
The Committee are asked to: NOTE the success in reaching the influenza target for the first time for
front line staff. NOTE the improvements required in primary care, especially in high
risk groups. NOTE the high rates of uptake in the schools programme. NOTE the funding requirement which has been put forward to the
organisation’s Executives which is being considered alongside other organisational priorities.
4.9 Out of Hours Update
1 4.9 OOH Progress Report PCPH&PC 10 February 2020.docx
AGENDA ITEM
(4.9)
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Urgent Primary Care (GP Out of HOurs) Service transformation programme
Date of meeting (10/02/2020)
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by Martine Randall – Senior Manager, GP Out of Hours
Presented by Sarah Bradley, Head of Primary Care
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(Insert Name) (DD/MM/YYYY) Choose an item.
ACRONYMSOOHPGDPCCPCHRGH
Out of HoursPatient Group DirectivesPrimary Care CentresPrince Charles HospitalRoyal Glamorgan Hospital
OOH Progress Report Page 2 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
1. SITUATION/BACKGROUND
During 2018, a national peer review process was implemented to support delivering a quality improvement and transformational process for the urgent primary care services (out of hours) by each health board. A number of recommendations were made and this together with a drive to comply with the new welsh government performance standards for GP Out of Hours (OOH) services provided the basis and focus for our local transformation programme.
The aims of the transformation programme are:-
To develop a more robust management structure with strong clinical leadership;
To develop engagement strategies for GPs and to ensure they feel the service offers a supported and attractive working environment;
To transform the workforce by expanding the professional skill mix and competencies within the service and reduce reliance on GPs;
To test the market by tendering the Prince Charles Hospital weekend face-to-face service;
To develop new clinical pathways to ensure patients are guided to the most appropriate professional or service to meet their needs;
To align service delivery with the new 111 service for Wales; To accelerate development of the Clinical Support Hub in
partnership with the 111 Team; To work to ensure OOHs is fully integrated with Cwm Taf
Morgannwg (CTM) UHB other urgent care and out of hours services.
The Primary Care Urgent Care Out of Hours Service has made tremendous improvements over the past 12 months. This paper provides an update with regard to the progress during the past 12 months and identifies the priorities for the coming year.
2. PROGRESS REPORT
2.1 Clinical Leadership
A number of key appointments have been made which include; New Clinical Director appointed July 2019 New Senior Nurse appointed July 2019 (new post) Clinical Shift Lead role introduced during OOH period
OOH Progress Report Page 3 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Critical to the success of the transformation programme was the development of a strong clinical leadership team. This is to ensure there is a clear, clinically driven service strategy and an operating environment which is conducive to providing effective mentorship, training and support for new staff. The Clinical Director has focused efforts on service improvement, service redesign, clinical reviews and governance and staff recruitment. Strengthened clinical engagement and GP induction processes have been implemented as part of this work.
The Senior Nurse is focused on developing the non-GP clinical workforce (Urgent Care Practitioners) and to provide assurance that the OOHs service is operating in a clinically safe and effective manner for those practitioners. She is implementing training, supervision, mentoring & audit processes for the new workforce and will ensure that staff are approved as competent to issue medications under a Patient Group Direction (PGD). As part of the future development the senior nurse will be supported by two part-time (1WTE) Advanced Nurse Practitioners who will undertake a supporting nurse educator role which will be pivotal to providing on-shift mentoring, guidance and audit for newly recruited Urgent Care Practitioners.
To strengthen clinical leadership during operational hours the role of Clinical Shift Lead was introduced on Saturdays/Sundays & Bank Holidays. This is a senior clinician who undertakes the following functions:-
• Manages the triage pool creating a more timely and safer service • Improves service performance against Welsh Government standards• Provides senior clinical support for the team• Provides advice and development of staff• Helps mitigates the limitations within the existing Decision Support Tools
The role is not just helping to stabilise the service during its busiest periods but is also helping to provide a more structured career pathways for GPs working in the Urgent Primary Care service.
2.2 GP Recruitment and EngagementThe service has historically been reliant on GP workforce and yet GP recruitment over the past few years has been sporadic and not in sufficient numbers to sustain the service. Since the summer of 2019 the service has attracted 25 new GPs to which has considerably improved the shift fill rate. This recruitment success is, in part, due to new forms of engagement with the GP population. The Clinical Director has led this and introduced the following strategies:-
New strengthened clinical induction process Refresh and re-engagement of the Clinical Reference Group Engagement with GP Specialty Trainees
OOH Progress Report Page 4 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
2.3 Shift fillShift of OOH posed one of the Directorate’s biggest risks and was reporting red on the risk register for a number of years. However, as a result of all the combined changes and efforts made by the management team the shift fill rate has continued to steadily improve and is now reporting the lowest escalation level 1.
Chart 1 - Shift Fill Rate
Of note, there have been no overnight shifts unfilled since June 2019 and the service is looking to introduce twilight shifts (until 2am) to provide additional capacity and support for the overnight service.
2.4 PCH Contract The shift fill rate at Prince Charles Hospital (PCH), has historically been problematic and the reason is the proximity away from the M4 corridor and the environment at Accident & Emergency (A&E). A different approach has been taken to test the market by inviting offers to tender for delivery of the face to face service at PCH on weekends and Bank Holidays. The contract was awarded to a consortium of GPs called ‘8 Medical’ in December 2019 and delivery commenced on the 18th January 2020. As part of the tender exercise there was a requirement to issue a formal lease for the dedicated rooms and shared spaces at PCH for the sole use of the contractor between 9.00am and 9.00pm on weekends. Albeit the new arrangement has only been in place for a couple of weeks no issues have been reported.
2.5 Assurance – Welsh Government StandardsIn January 2016 the Chief Executive of NHS Wales wrote to all UHBs indicating an expectation of delivery of the Welsh Government Standards for OOHs service by March 2018. The standards provide a minimum benchmarking dataset for
OOH Progress Report Page 5 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
OOHs services across Wales and are based on the three core elements of the service:-
Call handling Telephone assessment / triage Face-to-face consultations at home or in a primary care centre
Since the launch of the Standards, GP OOHs services have completed a self-assessment against the standards, which was followed up by a desk top assurance exercise undertaken by the NHS Wales Delivery Unit. Health Boards are required to report on the performance of GP OOHs services to the Urgent and Unscheduled Care Board and as part of their performance management reviews with Welsh Government. GP OOHs services report performance on a monthly basis to Welsh Government.
In order to improve assurance for the Board internal reporting mechanisms have been strengthened with the following:-
• Weekly reporting on shift fill nationally and to Welsh Government • Weekly performance produced and shared with the Executive Team,
example attached in Annex 1. • Dashboard reported and discussed at Clinical Business Meetings • Future forecasting of service demand provided on a weekly basis• Improved monitoring of trends in performance – identifying strengths and
weaknesses• Monitoring is showing improvements towards meeting the WG standards• Using the reports to inform capacity planning
2.6 Patient Satisfaction 2019The Welsh Government Standards for GP Out-of-Hours Services also requires the undertaking of an annual Patient Satisfaction Survey and the reporting of actions to Board. The results of the 2019 survey are shown in Chart 2. Ninety-six Questionnaires were collected between May and July 2019 which show an overall improvement in patient experience. Key actions for improvement have been identified with results circulated to all staff the findings reported through governance channels.
OOH Progress Report Page 6 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Chart 2 – Patient Satisfaction Survey
2.7 On-line Rota ManagementAs recommended by the 2018 Peer Review, a new online e-rostering system has been implemented (RotaMaster) to enable GPs to directly book shifts remotely without having to contact Ty Elai. The new system was procured and implementation completed in April 2019. This has allowed for:
• Quicker and more accurate running of payroll• Fairer allocation of shifts• Inbuilt reporting and audit tools• All staff can now book into their own shifts rather than contacting
an administrator; • Daily operational reports are simple to produce;• Texting function can be used via the system to inform staff and GPs
of vacant shifts
Building on this improvement a mobile app will be rolled out to all staff during February 2020.
2.8 Workforce Transformation In recent years numerous attempts to expand the professional skill mix within the service has been met with limited success, due to the unsociable hours, the fact that PCCs and the call centre are not integrated but dispersed from one
OOH Progress Report Page 7 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
another, and most staff work ad-hoc sessions. However the management team have made a concerted effort to overcome the obstacles and have employed a number of approaches, which include:
Workforce Modeling Tool & Competency Framework with the support of the Welsh Government Delivery Unit and Urgent Primary Care Clinical Competency Framework produced by Health Education and Improvement Wales (HEIW). This framework supports the development of Level 6 and Level 7 Urgent Care Practitioners (equivalent to Advanced Nurse Practitioner or Advanced Paramedic Practitioner) who will have the skills and competencies to treat minor illness to either PGDs or autonomously if they possess independent prescribing qualifications. Detailed Training Plans: In support of this workforce transformation programme a training plan, which draws on the Urgent Primary Care Competency Framework has been produced. The plan sets out the training an induction required for each level of practitioner recruited to the service. This training plan will be supplemented with:-
The timeline for the progressing the workforce plan is shown in Chart 3
Chart 3 – Workforce Transformation Plan
2.9 Strengthening Clinical PathwaysThe service has analysed its core data to identify the top 10 clinical conditions presenting to the OOHs services (sore throats, respiratory being just tow). Work is being commenced to develop appropriate pathways to assess and treat patients presenting with these clinical conditions. This work will also help to further inform workforce development.
OOH Progress Report Page 8 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
2.10 National 111 ImplementationThis workforce transformation plan comes at a time when the new NHS 111 Wales model of care urgent care is being rolled out across Wales. During the out of hours period the 111 service continues to rely on the GP OOHs service for clinical consultation, face-to-face consultations in primary care centres and home visiting services. It is expected that 111 will roll out to CTM during the summer of 2020 (The Bridgend County Borough is already covered by the 111 service). At present the roll out has been delayed due to capacity pressures from Welsh Ambulance Services NHS Trust (WAST) call handling perspective. This Health Board is ready in its preparedness plans and is in a position to implement.
2.11 Clinical Support Hub A component part of the National 111 Programme for Wales has been the development of Regional Clinical Support Hubs. These hubs comprise mainly of GPs and pharmacists and are responsible for maintaining the oversight of the calls coming into the clinical advice queue following call handling and nurse triage. The 111 team have provided weekend pharmacy support from the Hub since November 2018 and a Clinical Shift Lead as been rostered on weekends since September 2018.
2.12 Accommodation To support the multi-disciplinary workforce model a single site option for call handling and primary care centre would be the ideal. Valuable clinical support and advice could be provided to call handlers and also would solve the issue around dispensing of controlled drugs. It would also release financial resources if the lease on Ty Elai could be terminated. Discussions are underway regarding the identification of suitable accommodation for relocation.
2.13 Bridgend OOH ProvisionBridgend OOH is currently being delivered under a Service Level Agreement (SLA) with Swansea Bay UHB. It is planned that the SLA will continue through 2020/2021 with a plan to transfer the service in line with implementation of the new 111 Salus IT system. There is regular communication of shift fill rates between the two services. Engagement processes have started with clinical staff in Bridgend and further meetings are planned.
2.14 Governance arrangementsThe governance arrangements have been reviewed and strengthened. There is regular OOH Clinical Governance Meetings as well as participation in Significant Incident Reviews and harm review processes. All issues and exceptions are reported into the Primary Care Quality Safety and Risk Group which reports into
OOH Progress Report Page 9 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
the wider Primary Care and Localities Quality, Safety and Risk Group. A concerted effort has also been made to ensure that training has been undertaken by team members and reporting of incidents and risks are escalated in a timely manner via the Datix Risk system.
2. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
The main risks identified with this plan are:-
For weekday provision and RGH weekends the service is still reliant on ad-hoc GP sessions although currently the shift fill continues to be very good. It is not known how many practitioners will convert into a regular pattern of OOHs work.
Service change with the roll-out of national 111 programme has the potential to drive additional demand, however feedback from other Health Boards who have implemented has been that there has been no adverse implications.
Co-location of the call handling function with the PCC will provide a more robust infrastructure and alternative accommodation needs to be found in the Royal Glamorgan Hospital.
3. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Safe CareRelated Health and Care standard(s) If more than one Healthcare Standard
applies please list below:
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
OOH Progress Report Page 10 of 11 Primary, Community, Population Health &
Partnerships Committee10 February 2020
Choose an item.Resource (Capital/Revenue £/Workforce) implications / Impact
Link to Main Strategic Objective To Improve Quality, Safety & Patient
Experience
Link to Main WBFG Act Objective
Service delivery will be innovative, reflect the principles of prudent health care and promote better value for users
4. RECOMMENDATION
4.1 The Primary, Community, Population Health & Partnerships Committee is asked to:
4.2 NOTE and discuss the report.
5.1 Primary & Community Care IMTP Quarter 3
1 5.1 IMTP monitoring report PCPHPC 10 February 2020.docx
AGENDA ITEM
5.1
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
PRIMARY AND COMMUNITY CARE IMTP MONITORING REPORT
Date of meeting 10/02/2020
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by Mrs Alison Lagier, Directorate Manager Community Services
Presented byExecutive Director of Primary, Community & Mental Health
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome Primary Care & Localities
Management Team. GP cluster leads. Executive Directors Wider directorate staff in
Primary, Community and Secondary care inclusive of directorate managers.
Engagement sought on a continual
basis.
SUPPORTED
IMTP Quarter 3 Review Page 2 of 16 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Clinical Business meeting Primary, Community,
Population Health & Partnerships Committee
ACRONYMSIMTP – Integrated Medium Term Plan CTMUHB – Cwm Taf Morgannwg University Health Board RAG – Red, Amber, GreenRCT – Rhondda, Cynon, Taf SLA - Service Level Agreement NEWS – National Early Warning ScoreOOH – Out Of Hours
1. SITUATION/BACKGROUND
The purpose of this paper is to receive and NOTE the Quarter 3 report for the Primary and Community Care IMTP. The full report is available online at:http://cwmtaf.wales/Docs/Board_Papers/Legacy%202015-2016/15-11%20November%202015/AI%20%203%202%20Appendix%201%20Primary%20and%20Community%20Care%20Delivery%20Plan%20UHB%204%20Nov%202015.pdf.
The development of the Integrated Medium Term Plan (IMTP) has provided the opportunity to align the planning and delivery of primary and community care services as an integral part of the Health Board’s overall strategic direction. The Primary and Community IMTP is a key feature of the Cwm Taf Morgannwg UHB (CTMUHB) IMTP, along with emphasis on addressing health inequalities, strengthening prevention and building capacity and managing demand. We constantly aim to secure and sustain progress made in the previous year, whilst refreshing our plan to reflect new national requirements, our local priorities and the desire to ‘fast track’ innovation/ modernisation and new models of delivery in Primary Care and Community Services. This plan will be supported over the next two years by the addition of the Transformation funding from Welsh Government.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
The Monitoring Report as outlined in Appendix 1 is used by the directorate to track and report on progress of all the key elements that are within the Primary and Community Care IMTP. The report is updated for each new
IMTP Quarter 3 Review Page 3 of 16 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
financial year and reflects the current priorities within the IMTP for 2019/20. A new plan has now been developed for 2020/21 and will be reported to the next committee.
This is a live document that is up-dated quarterly by the directorate and used to report progress. Any key risks are also highlighted and are then included within our own risk register for monitoring. Key elements of the plan would also feature via designated papers to the directorates Quality and Safety Meetings and any other committees within CTMUHB as appropriate.
The 19 top areas for development / action are outlined within our plan. They are currently RAG rated as below with the updates on delivery outlined within the attached plan:
Key Priority AreasRED No Areas rating REDAMBER
7
Development and implementation of the transformation Multi-Disciplinary Team model
Expansion of the Lymphoedema team in RCT and Merthyr Tydfil in order to meet existing demand and become an effective and responsive service. (Bridgend service provided by SLA with Swansea Bay)
Reduce Average Length of Stay in Community Hospitals to free up capacity at acute sites
Implement the All Wales District Nursing Principles. The development and commissioning of Bridgend Wellness
Centre NEWS - National Early Warning Score Community Dental Service and Design 2 Smile redesign for
alignment across all 5 Localities GREEN
12
Implement the Neighbourhood Nursing Pilot within District Nursing including piloting 'Malinko' software.
To redesign Urgent Primary Care Services (OOH) and implementation of 111
To support the development and commissioning of the new Mountain Ash Primary Community Facility
Re-provide the current Y Bwthyn on the Royal Glamorgan site Continue to develop @Home alignment to Stay Well @Home
Phase 2 and the Extended Community Cluster Teams Closure of Ystrad Clinic Continuing Health Care Cost Containment Establish Local Transgender Service Review Of Wound Care Services to ensure the best service
delivery model which is consistent across CTMUHB
IMTP Quarter 3 Review Page 4 of 16 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Lindsay Leg club - Roll out program across CTMUHB Development of Maesteg Hospital To further promote the access to and provision of eye care
within Primary Care (EHEW & Low Vision Services)
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
Updates on the Amber areas are outlined within the attached plan (Appendix 1). There are no key risks identified with the areas currently, they mainly relate to timing of specific pieces of work or outstanding decisions on finance. We will continue to monitor the actions and will bring back any key issues at Quarter 4 that have impacted on delivery of year end targets.
4. IMPACT ASSESSMENT
Quality/Safety/Patient Experience implications
There are no specific quality and safety implications related to the activity outined in this report.
Related Health and Care standard(s) Staying Healthy
Equality impact assessment completed Not required
Legal implications / impactThere are no specific legal implications related to the activity outlined in this report.
Some of the above priority areas will require investment however the appropriate documentation has been complete and included within the IMTP.
Link to Main Strategic Objective
To Improve Quality, Safety & Patient Experience
To protect and improve population health
To ensure that services provided are accessible and sustainable into the future
IMTP Quarter 3 Review Page 5 of 16 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
Link to Main WBFG Act Objective
Work with communities to prevent ill-health, protect good health and promote better health and well-being
Service delivery will be innovative, reflect the principles of prudent health care and promote better value for users
Work collaboratively with our public service partners and a broader range of partners to join up health and other services where this potentially represents better value for our residents and care users
5. RECOMMENDATION
5.1 The Primary, Community, Population Health and Partnerships Committee are asked to:
NOTE the Monitoring Report for the Primary and Community Care IMTP
APPENDIX 1DIRECTORATE IMTP MONITORING REPORT (Quarter 3 up-dated January 2020)
SB Development and implementation of the transformation MDT model
Recruitment of staff. Review and refine processes and protocols.
Induction, training and team building.
Further engage Cluster Leads and other stakeholders.
Continue recruitment of staff, induction, training and team building.
Continue engagement with key stakeholders.
Set up project structure to feed into Programme Board.
Commence phased implementation
Continue with team building and recruitment as needed.
Commenced implementation on phased basis across Clusters.
Review data across each Cluster area.
Produce monitoring reports.
Continue to recruit as needed.
Refine the model based on ongoing review.
Ability to recruit significant numbers of staff. Ability to delivery within agreed timescale of 18 months. Gaining full commitment from the existing primary care workforce and wider MDT team. Sustaining the service after the funding period. Public acceptance of the new model and workforce.
Q3 AmberCommitment from Clusters to support the MDT. Workshops have taken place with all of the clusters with regard to the models which will operate. Recruitment of Staff almost complete, only mental health practitioner outstanding. Staff inductions have been organised for February. Dates for implementation have been agreed with all of the clusters. Rhondda end of February, Taff Ely March and South Cynon and Merthyr April.
SB – CDS and D2S redesign for alignment across all 5 Localities
Project Initiation Document completed and approved
Steering Group membership established and dates agreed for 2019/ 20
Task and Finish Groups membership agreed
Priorities for service redesign agreed
Engage with teams across CDS and D2S
Engage with external stakeholders
Set up Task and Finish Groups to feed into Steering Group
Continue engagement with all CDS/ D2S staff groups
Establish broad timelines for project priorities
Commence phased review of Fluoride Varnish and Tooth brushing programme
Commence phased review of existing posts and structures
Commence phased review of GA and sedation services
Evaluate activity data including utilisation, DNA’s and demand and capacity for all clinics
Undertake full review of Fluoride Varnish and Tooth Brushing programme
Undertake full review of posts and structures
Fully review skill mix and undertake TNA for all clinical staff
Commence phased review of application of WHC Feb 2016 throughout CDS
Fully review GA and sedation services
Submit any recommendations for change to structures to Steering Group for approval
Implement any HR processes associated with organisational change (if required) following approval from Steering Group
Fully review clinic structure following evaluation of all activity data
Fully review WHC application throughout CDS
Ability to deliver within agreed timescale by June 2020. Ability to engage with clinicians around clinical commitments. Being able to fully engage with existing staff with any proposed changes. Public acceptance of any proposed changes to the service.
Q3– AMBER 1st Draft of review of C2S is complete. Project Draft proposal for alignment of D2S across all localities is being compiled. Established work streams being reviewed. Review of paediatric GA service underway, discussions will include the need for CTMHB to identify additional capacity in RGH to accommodate Bridgend dental GA patients (currently treated in Swansea Bay via SLA). Awaiting on Theatres to confirm the additional monthly theatre session. Scope for full review of CDS has been drafted and work will commence in February.
AL/PC Expansion of the Lymphoedema team in RCT and Merthyr in order to meet existing demand and become an effective and responsive service(Bridgend service provided by SLA with Swansea Bay)
Meeting of WG/CEO and Leads to discuss resources needed
Recruit via TRAC the additional staff required. Provide additional clinics to meet demand.
Scope the needs and clinical risks against the WG report – Q1
Report to CBM – Q1
Review pathways with the wound and tissue viability clinics
Implement more robust service.
Continue to report improving position into WG
Commence evaluation of the service
Breaching the All Wales standards. The recommended patient to clinician ratio is 220:1. The CTUHB ratio is 1,054:1. Inability to meet increasing demand will lead to increasing length of time patients have to wait to be seen and or treated with potential deterioration in clinical condition.
Q3 AMBERAll Q1, 2 & 3 actions complete and new staff are in post. We have reduced this risk from a Red to an Amber with the new staffing in place but this remains Amber until such time we are confident that the new capacity has reduced the waiting times. We have undertaken a table top exercise to look at the potential capacity release based on the Welsh Government business case.
SB To support the development and commissioning of the new Mountain Ash Primary Community Facility
Detailed project plan in place
Detailed project plan in place
Detailed Project Plan in place
Detailed Project Plan in place
Failure to build and commission the building within the funding timeframe provided by WG due to unforeseen circumstances
Q3 GreenNow in construction phase. Development is on track for March 2021 with completion end of November 2020. Discussions with art consultant regarding the commissioning of art work. Agreement to lease in place with practices and Apollo. 2 practices merging just prior to occupation of the building.
SB To redesign Urgent Primary Care Services (OOH) and implementation of 111
Continue to implement flight controller, new clinical pathways and revised algorithms. Via 111 Programme Board develop the project implementation plan for the roll out of 111 service. Work with COMMS team to prepare awareness raising with all stakeholders and patients.
Ensure GP fill rate for OOH’s does not fall below 80%
Continue to implement flight controller, new clinical pathways and revised algorithms. Roll out 111 later end of Q2.
Ensure GP fill rate for OOH’s does not fall below 80%
Implementation of 111 Service. Monitor impact of first few weeks of delivery
Ensure GP fill rate for OOH’s does not fall below 80%
Implementation of 111 Service. Monitor impact of first few weeks of delivery
Ensure GP fill rate for OOH’s does not fall below 80%
Failure to maintain GP OOH’s shift fill rates and to deliver the new MDT.
Q3 GREENThe service has maintain a relatively static shift fill rate over 85% projection. The new contract is in place with 8 Medical for Saturday and Sunday 9.00-9.00 cover in PCH. The new clinical lead has recruited additional 25 GPs. The development of the MDT is progressing, the Nurse Lead is working to introduce new ANPs and Nurses in February 2020. All actions to compliment the 111, roll out 2020 to be confirmed. Positive feedback from peer review. Exceptional progress, all recommendation from 2019 review were being addressed.
SB To further promote the access to and provision of eye care within Primary Care (EHEW & Low Vision Services)
Continue to promote the EHEW scheme to patients across the 5 localities. Engage with Bridgend Optometrists to encourage update of accreditation.
Continue to promote within the community the EHEW and other low vision services available. Start to compare the level of service delivery across the 5 Localities. Identify good practice.
Identify a plan to ensure there is equity of access.
implement the plan Failure to do nothing will result in patients being seen in secondary care for things which can and should be seen in primary care / community. If there is not a shift secondary care will not be released to undertake more complex work
Q3 GREEN2019/20 LVSW figures for Q1 and Q2 show an increase of 41% over the same period last year, Q3 figures not yet released. EHEW remain a cost pressure but funding provided via Healthier Wales funding.First joint optometry/pharmacy CPD event held locally in Nov’19.Progressing primary care Glaucoma pilot in conjunction with secondary care. Funding has been secured from WG to test the concept in 3 practices across former Cwm Taf. Must be delivered and tested by the end of March 2020.
PC Reduce ALoS in Community Hospitals to free up capacity at Acute sites
Meet with key senior staff to review point prevalence work and actions to be agreed.
From point prevalence work, determine where capacity could be freed up in Acute
Review Rehab Pathway work
Work with Acute Care colleagues re capacity for winter plan.
Consider testing Choice Process in YCC.
Evaluate impact of any schemes on winter.
Capacity in private sector for discharge destination and POC Sign-up of all staff Resource support to Choice Process
Q3 AmberNo sustained reduction in ALoS in YCR or YCC despite testing Choice Process and new Rehab Pathway. A new piece of work is now being scoped with the support of
Review support for families for choice
Patients remain longer than needed in hospital
the PMO this will form part of the plan from 2020/21. ALoS in Maesteg has reduced since the Community Directorate have managed the site.
AL Re-provide the current Y Bwthyn on the Royal Glamorgan site
Communication with staff
Operational Policy to be signed off
Support Capital works
Move date agreed and plan progressed
Ongoing communication
Commissioning of Unit i.e.: * furniture * equipment * staff familiarisation while link corridor is being built
Ongoing communication
Patients and service transfer - service is operational
Monitor any changes/ impacts
Review service change and impacts
Additional HCA at Night once 8 beds commissioned
Link corridor complete
Any changes to capital scheme re weather Any identified commissioning issues that might arise Staff patient concerns that may arise re the move Increased HCA needed by night
Q3 GreenAll actions complete and the service moved to the new unit on the RGH site in September 2019. Key positive outcomes already experienced. Paper on additional HCSW’s to support extra 2 beds presented to Executives
PC Implement the Neighbourhood Nursing Pilot within District Nursing including piloting 'Malinko' software. Consider roll out of Malinko to all other DN's
Review recruitment and training
Malinko outputs to date to be measured
Report to Project Board on action plan
Evaluate Malinko to date
Review action plan and report to Project Board
Review actions Report to Project
Board Outcome of
Malinko to consider roll out to other DN’s
End of year evaluation and report to include recommendations re Malinko for all DN’s if data supports priorities in IMTP
Ability to progress in a timely manner to ensure WG funding is spent
Support of wider Primary Care Team
Q3 Green Recruited HEIW support for Malinko evaluation. Developed a slippage bid to RCTM Transformation for Malinko role out to RCTM. Working with Bridgend on this also
PC Implement the All Wales District Nursing Principles. We are compliant on several within RCT and Merthyr Tydfil - to consider those outstanding.Review Bridgend
Detailed paper prepared and presented already re RCT & MT.
Await outcome of IMTP funding proposals re RCT and MT
Start scoping Bridgend
If agreed, develop plan for recruitment and change re RCT and MT
Develop a case for CBM for Bridgend
Implement staff changes and change process re RCT and MT if funding agreed
Scope plan for Bridgend
Evaluate changes if funding agreed re RCT and MT
Bridgend to be prioritised in IMTP
Not implementing reputation with Welsh Government Qualified staff continue to undertake admin tasks re RCT and MTNo consistency across CTM
Q3 AmberDetailed paper presented for RCT and MT, no additional funding received from IMTP. Impact of Bridgend scoped and included in the return to Welsh Government. To be included in 2020/21 IMTP. The impacts / gaps for Bridgend due to the complexity of the Integrated Model.
AL Continue to develop @Home alignment to SW@Home Phase 2 and the ECCT (Transformation Agenda)
Review meetings with staff to outline new model re transformation
Consider Pathway from @Home into new Transformation Model
Ensure @Home are involved in relevant Transformation meetings
Agree any changes to @Home to align
Develop new Pathways/ Protocols to align with Transformation Model
Review alignment with new Transformation Model
Q3 GreenStaff from @Home actively engaged in the Transformation work to ensure alignment of the developing models.
AL Closure of Ystrad Clinic
Scope needs Secure alternative
accommodation at YCR and other sites
Work with Capital/Facilities on any changes
Based on capital being available start engagement with staff and CHC
Based on capital availability commence engagement with community supported by
Commence move once any work is complete.
current building is in need of repair minimum numbers of staff currently based at site causing some lone worker issues
Q3 GreenThe new office accommodation is being developed in the old Radiology store YCR this is scheduled to be completed by the end of March 2019.
needed on YCR site to cost this
communications team
design to smile staff moving out this year reducing numbers further potential risk is public perception of withdraw of facility although only clinical provision is HV which would be re provided at YCR
Discussions have commenced with effected members of staff have and all moves have been identified to allow the closure to go ahead as planned.
SB The development and commissioning of Bridgend Wellness Centre
To progress the review of the design plans.
To complete the FBC.
To submit the FBC to ECMG and then to WG for approval.
To finalise the design plans and the consequences for the tender
To progress the development of the collaboration agreement and the Head Lease template
To ensure the construction is completed on site
There are revenue consequences attached to this scheme which need to be identified as early as possible
Q3 AmberLinc Cymru (Developer) has progressed the Tender to appoint the contractor. Collaborative Agreement soon to be signed off. FBC going through internal governance processes for sign off before submission to WG. Issues still need to be clarified around 1. Section 106 conditions attached to the planning conditions and the request for additional car parking. 2. Assurance around Heat Source Network.
SB Establish Local Transgender Service in line with WHC directive
To ensure all individuals are appropriately trained.
To commission local gender service from strategically placed practice
To commission the DES from practices once officially released by WG
To commence the Local gender service
To commission DES and ensure equity of access and provision across CTM
To commence acceptance of referrals
To monitor activity and the service delivery
To monitor activity and the service delivery
WG have released a WHC directing Health Boards to establish a Transgender Service locally. Failure to establish the service will result in non-compliance
Q3 GreenWelsh Gender Service commenced 20th September.Local Gender Service is now established delivered from ‘Dewi Sant’’ Health Park. DES has been commissioned and small number of practices
PC Review Of Wound Care Services To Ensure The Best Service Delivery Model Which Is Consistent Across The New Cwm Taf Morgannwg Footprint
Scope needs in Bridgend as this is provided by bank and agency across multiple sites
Develop a new service model for Bridgend and take paper on needs to CBM
Commence change to service model Bridgend
Evaluate service model across CTM
Bridgend service is funded through GMS budget. Bridgend service provided through bank and agency and is fragile.Reduction in sites in Bridgend may cause staff/public concern.
Q3 Green Wound service is being provided across Cwm Taf Morgannwg. Recruitment into substantive posts instead of reliance on bank staff is complete. A review is being undertaken with regard to demand and capacity as part of the evaluation
PC Lindsay Leg club - Roll out the delivery of services the new Cwm Taf Morgannwg Footprint
Learn from Rhondda Development and agree roll out programme across CTM
Develop business case, identify areas and commence phased roll out
Agreed action plans in place with Leads for each scheme and project approach
Evaluate and review roll out programme and patient impact
Capacity to deliver as set up is labour intensiveCommunity Champions to Chair are scarceAppropriate venues available
Q 3 GreenScoping completed and a phased approach across the patch has been outlined.
AL Development of Maesteg Hospital
Scope potential new model for Maesteg
Test model with key partners informally
Meet with key partners formally to agree model
Take paper to UHB Executive Board for sign off
Develop project approach with support from HR/Planning and Communications/Capital
Commence engagement
Commence implementation of plan
Report through project scheme
Continue implementation of plan
Evaluate plan to date
Report through project scheme
Public engagementStaff engagementCapital fundingCapital works
Q3 GreenModel scoped.Support informally gained from CHC, Friends of Maesteg and BCBC. Executive Board Paper presented. Project Structure outlined and commencing Jan 2020.
AL CHC Cost Containment
Scope and understand Bridgend element
Work with Procurement on contracts with Nursing Homes and Community Care providers
Continue to progress work with Procurement Team
Work with Finance to develop more robust monitoring reports to take to CBM
Work with Procurement on a detailed phased plan to tackle any issues that they advise might reduce cost
Review impact of work with Procurement
Review improved data/information
Procurement resource is short term funded to give extra capacity and expertise to this work
Q3 Green We have established a baseline and have outlined a plan with procurement.
PC NEWS - National Early Warning Score
Scope need for equipment and maintenance across whole of CTM
Purchase of appropriate equipment to support across all Localities
Roll out across the CTMUHB communities
Evaluate impact Q3 AmberScope complete across CTM. RCTM areas completed. Still looking at solutions for Bridgend due to finance implications.
5.2 Primary Care Milestones
1 5.2 Delivery Milestones for Primary Care Report PCPHP Feb 2020.docx
AGENDA ITEM
(5.2)
OTHER
PRIMARY, COMMUNITY, POPULATION HEALTH & PARTNERSHIPS COMMITTEE
Primary care Delivery milestones
Date of meeting (10/02/2020)
FOI Status Open/Public
If closed please indicate reason Not Applicable - Public Report
Prepared by Sarah Bradley, Directorate Manager for Primary Care
Presented by Sarah Bradley, Directorate Manager for Primary Care
Approving Executive Sponsor Executive Director of Primary, Community & Mental Health
Report purpose FOR NOTING
Engagement (internal/external) undertaken to date (including receipt/consideration at Committee/group) Committee/Group/Individuals Date Outcome
(DD/MM/YYYY) Choose an item.
ACRONYMSIMTPWAST
Intermediate Medium Term PlanWelsh Ambulance Services Trust
Primary Care Milestones Page 2 of 4 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
1. SITUATION/BACKGROUND
1.1 A key element of A Healthier Wales is the implementation of the Primary Care Model for Wales. The Strategic Programme for Primary Care is progressing a number of work steams to support the delivery of the model and each year the Minister for Health and Social Care issues a set of delivery milestones for Health Boards to adopt locally. He has specifically charged Vice Chairs of Health Boards with a key leadership role in promoting the implementation of these milestones and the adoption of the New Primary Care Model.
1.2 This paper and Annex A outlines the progress made against the 2019/20 milestones, and also introduces the new 2020/21 milestones.
2. SPECIFIC MATTERS FOR CONSIDERATION BY THIS MEETING (ASSESSMENT)
2.1 Progress has been made against the 2019/20 milestones and this is detail in Annex 1. Although we are achieving and reporting green against a number of the milestones there are a number which remain amber. There are two reasons behind the lack of ability to achieve: Firstly, the Primary Care team is reliant on other agencies and parts of the Health Board to collaborate and to contribute to the delivery of the initiatives and this has proved difficult at times. Secondly, a couple of the indicators are reliant on work being concluded on a National basis, such as the implementation of the All Wales Workforce Reporting Tool and the Demand and Capacity Audits. Once these are in place the milestones should will be reached. Further actions have been identified in the last column of the report indicating what needs to be done for the Health Board to reach compliance.
2.2 The 2020/21 milestones and covering letter from the Minister for Health is attached in Annex 2
3. KEY RISKS/MATTERS FOR ESCALATION TO BOARD/COMMITTEE
3.1 There are no red risks identified for the 2019/20 delivery milestones. The Primary Care team will endeavor to ensure that work continues to ensure compliance against the milestones which are reporting as amber by the end of March 2020.
3.2 The milestones for 2020/21. The covering letter the Minister for health and Social Care has clearly set out his expectations that going forward
Primary Care Milestones Page 3 of 4 Primary, Community, Population Health &
Partnerships Committee 10 February 2020
the responsibility for the achievement of the milestones rests with the entire leadership team of the Health Board and not just with the Director of Primary and Community Care and the actions should be reflected in the 2020-21 IMTP. Planning and delivery at a cluster level is now emphasised and is supported by the additional allocation of cluster funding (£10 million across Wales which equates to £1.5 Million for Cwm Taff Morgannwg Health Board). As well as this, the Minister also states that he expects Health Boards to allocate additional funding, workforce and other resources at a cluster level. This is a new challenge for the Health Board.
4. IMPACT ASSESSMENT
There are no specific quality and safety implications related to the activity outined in this report.
Quality/Safety/Patient Experience implications
Governance, Leadership and AccountabilityRelated Health and Care
standard(s) If more than one Healthcare Standard applies please list below:
Not requiredEquality impact assessment completed
There are no specific legal implications related to the activity outlined in this report.Legal implications / impact
There is no direct impact on resources as a result of the activity outlined in this report.
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
1
DELIVERY MILESTONE BY WHEN RAG RATING REPORTING Actions required to meet Compliance
STRATEGIC PLANNINGCluster workingCluster IMTPs for 2020-2023 complete, using nationally agreed template and underpinned by cluster workforce development plans
End Sept 2019 GREEN Cluster IMTP’s have been completed by all 8 clusters in Cwm Taf Morgannwg.
They have been shared with Welsh Government.
None
PREVENTION AND WELLBEINGPreventing FallsFalls prevention awareness programmes (IStumble or equivalent) are rolled out to care homes
End Mar 2019
AMBER
Initiative with WAST
IStumble tool developed to make it ‘fit’ for purpose in care homes (residential and nursing)Care homes have been provided with Magar Elk fitting cushion.
All care homes within the old Cwm Taf footprint have received training in Istumble. We have requested information on the roll out in the Bridgend area. Awaiting data from WAST on outcomes of implementing the tool on calls to homes for falls and hospital transfers.
Further engagement required with WAST colleagues and Health Board continuing health care team.
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
2
Preventative careCare home residents routinely receiving assessments and care planning in line with the 2017 directed enhanced service for care home residents
People with 3 or more chronic conditions living in their own homes agree and receive care and support in line with an individual anticipatory/advanced care plan
End Nov 2019
End Mar 2020
We have received data from WAST with regard to the number of calls to each home and the reasons for them. The data is currently being organised into a meaningful format that can be used to support further work.
Good uptake of care home enhanced service. 92% in Rhondda, 100% in North Cynon, 83% South Cynon, 57% Taff Ely, 100% Bridgend Clusters. Clusters to be approached with regard to providing the enhanced service cluster wider via a network arrangement where practices have not signed up to deliver it.
Segmentation programme is being implemented across CTM to help GPs identify patients with co-morbidities and to plan anticipatory approach to care. Supporting this programme is the implementation of a MDT team wrapped around GPs and Clusters.
Bridgend North Cluster invested in a Chronic Conditions Nursing Team to support review of housebound patients living with
Large number of nursing homes in Taff Ely and practices are not keen to take up the DES due to the workload involved. Discussions to take place at Cluster level to find a solution and practice which will do this on behalf of others.
Segmentation data has been provided to the Rhondda cluster as they were part of initial pilot. The plan is to roll this out across Cwm Taf Morgannwg as part of the wider transformation programme with data
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
3
chronic conditions and provide proactive and relevant support to help individuals to manage their conditions
The Enhanced Cluster Team – Discussions with Rhondda, Taff Ely, Cynon and Merthyr clusters were held in 2018 to help inform decisions around the skill-mix and workforce for the multi-disciplinary team. The cluster-based Multi-Disciplinary Team, tentatively called the “Enhanced Cluster Team”, will help people to maintain patients health and independence at home. The teams will consist of GP time, Nursing, Therapies, Social Care and Third Sector professionals, and the day-to-day co-ordination will be carried out by a dedicated operational support manager and administrative support. The MDT professionals will work together to provide holistic assessments and a range of social and healthcare interventions for patients that MDT interventions are deemed appropriate. Patients will be identified through:
- Health and social care professionals
- Population segmentation and risk stratification
being provided to the remaining clusters June 2020
MDT team to become embedded as part of the wider Primary Care Team to support patients with Chronic diseases.
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
4
A very similar model is also being implemented within the Bridgend Cluster areas. The model was agreed whilst Bridgend was still part of ABMU but the model does consist of a multi-disciplinary care team providing holistic care to patients.
The ECT teams in Rhondda are due to go live week commencing 24th February 2020, Taff week commencing 16th March and Merthyr & Cynon week commencing 6th April 2020.
24/7 SERVICEAccess to GP practices and 111/Out of Hours ServicesPeople contacting GP practices and 111/Out of Hours services are responded to in line with national standards for access to each of these services.
In line with timescales set separately by Welsh Government for each set of standards
AMBERStandards monitored regularly at our CBM and OOH Project Board. The new standards published in April 2019 have been developed based on the configuration of the 111 pacesetter project, therefore not all targets can be reported on until the health board has moved to 111 or the Adastra system has been re-configured to reflect the new parameters (which will be at a cost). It has been agreed with WG that CTM are able to report on the targets in their current configuration due to the
Achieving of the full set of OOH standards is dependent on the implementation of 111
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
5
impending launch date of CTM 111 in Autumn 2019.
Shift fill across the board has improved dramatically due to the tender for 8 Medical and also 25 new GPs have signed up to provide OOH sessions. This is assisting in the achievement of the standards.
Very positive response from the follow up national peer review team following visit in December. Reported that they were impressed that all actions identified in 2018 review has been addressed and significant improvement overall made.
Governance has been strengthened and harm reviews and Significant Incidents are reviewed regularly.
In line with the new Access to In Hours GMS Services Standards that were introduced in March 2019, the Primary Care Access & Sustainability Forum has been established with representation from all parties as specified within the guidance issued by Welsh Government. The remit of the
The expectation is all Practices will have achieved these national standards by March 2021
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
6
group is to “ review and monitor performance against standards, share best practice and assist with the development of good access initiatives through clusters”.
A baseline assessment of all practices against the standards has been completed and the baseline revealed a good position This was reviewed at the first meeting held in January 2020.
DATA & DIGITAL TECHNOLOGY
Reporting escalating pressuresUse of nationally agreed system for reporting escalating pressures on GP practices and 111/Out of Hours Services commenced.
Oct 2019 onwards GREEN
OOH escalation process is robust and established. OOH Performance reported on weekly basis to Executive Team. Reporting to CBM and quality and safety committee monthly. Harm reviews and Significant Incidents reviews in place.
An escalation tool for primary Care has been agreed and has been circulated to all GP practices. This is currently a hard copy that is completed by practices and attached to an email that is then submitted to the health board on a weekly basis. The tool has 4 levels for the practices to report against with
No further action
Encourage all practices to report. Collate feedback from practices with regard to the usefulness of the tool in order to inform further refinement.
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
7
Level 1 being no pressures and level 4 being extreme pressures. Directors of Primary Care have tasked NWIS colleagues with developing this into an online tool.
36 out of 52 practices reported. There was an excellent rate of submissions from practices to date with the majority recording level 1 or level 2. 5 reported level 3 and 1 reported level 4.
WORKFORCE & OD
Workforce capacity and capabilityCluster workforce development plans for 2020-2023 complete, using nationally agreed tools for workforce planning and analysing service demand and capacity
End Sept 2019
AMBER
The 2019-2020 GMS Contract confirmed the introduction of the Wales National Workforce & Reporting System (WNWRS) and its mandatory completion by GP
The WNWRS will be developed into a secure web based tool that will support workforce planning at both practice & cluster level.
A demand and capacity tool is being procured by one of the national strategic work streams. Demand and capacity audit is a requirement of the Quality Assurance and Improvement
The agreed workforce tool only just been released for practices to populate, and needs to be completed by the 14th February.
Still awaiting the a nationally agreed tool for analysing demand and capacity. Expected to be commissioned in 2020.
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
8
Framework in the GMS contract. .
COMMUNICATION & ENGAGEMENT
Use of local positive stories to engage community April 2019
onwards GREEN
Dedicated communications officer for primary care and localities has been appointed. Clusters utilise the communications officer to ensure messages about services being developed within clusters are relayed to patients.
Cluster leads and development managers have attended numerous public events to provide information to the public on what services to support them are available and to engage with the public on service developments. The ‘Know your team’ campaign continues to be implemented and will include new roles as part of the wider MDT being delivered from the transformation programme.
We are running a series of public engagement events in February across all cluster areas to invite members of the public to come along and meet people from
“Know your Team” campaigns are ongoing.
Cluster engagement continues with community groups and at community events.
Annex 1
PRIMARY CARE MODEL FOR WALES – DELIVERY MILESTONES 2019-2020 – PROGRESS REPORT JANUARY 2020
9
different services and provide information on the services available to them within the area.
1 5.2.2 Annex 2 - Letter to Chairs and Vice Chairs of Local Health Boards.pdf
Vaughan Gething AC/AM Y Gweinidog Iechyd a Gwasanaethau Cymdeithasol Minister for Health and Social Services
To: Chairs and Vice Chairs of Local Health Boards
CC: NHS Trust Chairs, Chair of HEIW, Chairs of Regional Partnership Boards, National Director and Strategic lead for Primary Care
8 January 2020 Dear Chairs and Vice Chairs, Primary Care Model for Wales - Delivery Milestones 2020-21 I am writing to set the national delivery milestones for the Primary Care Model for Wales to be achieved in 2020-21. These delivery milestones are set out at Annex A. The Primary Care Model for Wales is one my 5 priorities in the NHS Planning Framework. I note that previously Health Boards have assumed that the delivery milestones are the responsibility of Directors of Primary and Community Care. I would like to remind you that as part of A Healthier Wales, the implementation of the Primary Care Model is part of the development of whole system working. I therefore expect the entire leadership team of the Health Board to consider their responsibilities in delivering these milestones and for this to be reflected in the actions in your 2020-23 IMTP or annual plan. To help make a real leap forward on this, I have set two ‘whole system ‘delivery milestones for urgent care. The Strategic Programme for Primary Care already has action underway or planned on a suite of resources to support you in achieving these delivery milestones. To help your wider leadership team become fully engaged and involved, Judith Paget, Chair of the National Primary Care Board will write to Health Board Chief Executives setting out in more detail how the Strategic Programme supports each delivery milestone. Cluster led planning and delivery is here to stay and is core to the Primary Care Model for Wales. To reinforce my commitment to this, I have set delivery milestones at cluster level. I am pleased to allocate an additional £10 million recurrent funding from 2020-21 for clusters to decide how to invest in implementing the Primary Care Model for Wales. I expect Health Boards to follow my lead and delegate more funding, workforce and other resources to cluster level. When I met cluster leads at the primary care conference on 7 November, it was clear there are still issues with the arrangements for the current £10 million cluster funding and Andrew Goodall has since written to Health Board Chief Executives. The National Director of Primary Care and the Chair of the Directors of Primary Care have a planned discussion with the Directors of Finance on the key issues. I expect each Health Board to review its own arrangements against each of the key issues to ensure the existing and additional funding I allocate for cluster determination is optimised.
I will continue to monitor progress with the Primary Care Model for Wales through my regular meetings with Vice Chairs, with a particular focus on the input from the entire Health Board leadership team. In view of the impact of the Primary Care Model for Wales on the whole system and the vision in A Healthier Wales, I am also copying this letter to the chairs of the Regional Partnership Boards. Yours sincerely,
Vaughan Gething AC/AM Y Gweinidog Iechyd a Gwasanaethau Cymdeithasol Minister for Health and Social Services
Annex A Primary Care Model for Wales - Delivery Milestones 2020-21
Delivery Milestone When
Each cluster IMTP for 2021-24 includes action in clinical settings to address risk factors for preventable poor health and wellbeing.
By end September 2020
Each cluster has achieved increased vaccination and screening uptake rates for its population.
By end March 2021
Each Health Board to be proactively monitoring urgent care activity, and collaboratively developing methods to better manage changing demand in the community during peaks in pressure, leading appropriate whole system action to address escalating pressures’
From April 2020 on
Each Health Board has:
shared a detailed self-assessment of and learning from local delivery against each of the seven winter themes;
for 2019-20 with the Welsh Government and other NHS Wales bodies,
used this self-assessment and learning to develop plans to improve the year round resilience of the urgent
care system further
By end April 2020 By end August 2020
Each cluster has analysed demand on:
Community pharmacy
Dental and oral health services
Optometry and eye health services
Community nursing (including children’s)
Community health and social care services
By end September 2020
Each cluster IMTP for 2021-24 includes action to plan and deliver appropriate Enhanced Services at cluster level.
By end September 2020
Each Health Board is using the reformed dental contract for 50% of the practices it contracts dental services from.
By end October 2020
A nationally agreed approach to monitoring time spent at home (or equivalent measure) is in operation locally.
By end March 2021
People contacting GP practices are responded to in line with Access to In-Hours General Medical Services National Standards.
By end March 2021
Out of Hours care pathways have been adapted for local use and are available to 111/Out of Hours for:
Urgent Dental pathway
Mental health crisis services pathway Palliative Care pathway access to pain relief.
By end March 2021
The 111 service, integrating with the Out of Hours Service, to be rolled out in 6 health board, and by September 2021, to be rolled out in Betsi Cadwaladr University Health Board
By end March 2021, By end September 2021 for Betsi Cadwaladr University Health Board
Each cluster IMTP for 2021-2024 includes action relating to facilities, premises and estates.
By end September 2020
Each cluster IMTP for 2021-24 includes actions to move eye care services out of hospital and provide them in the community, specifically action to include at least one optometrist in the cluster with advanced training for:
Professional certificate in medical retina
Professional certificate in glaucoma.
Higher certificate in glaucoma.
Independent prescribing.
By end September 2020
Each Health Board has begun:
rolling out the national primary care campaign locally
developing internal communications aimed at all primary and secondary care staff to improve awareness of the Primary Care Model for Wales
By end September 2020
5.3 National Primary Care Board Update
1 5.3 NPCB Communique December 2019.docx
NATIONAL PRIMARY CARE BOARDCOMMUNIQUE FROM MEETING HELD ON 12 DECEMBER 2019
Strategic Programme for Primary Care
The Strategic Programme is progressing at an increased pace with two appointments made to national roles as follows:
Dr Alastair Roeves who takes up the role of Clinical Lead and will have a phased start in the New Year.
Kerrie Phipps who has been appointed as Lead AHP and will take up the post on 20 January 2020.
Overall the Highlight report for the period of 1 September 2019 to 30 November 2019 is rated as Amber. This is due to two reasons. Firstly, changes in timescales for some deliverables and secondly, new deliverables are being scoped for inclusion into the work streams. The Highlight Report is attached as Appendix 5.3.1.
The achievements over the last quarter include: the completion of the first edition of the cluster IMTP the issuing of the winter planning framework (with five of the seven themes proposed
by the Directors of Primary Care). the publication of the Cluster Year Book, providing a wealth of information and
recognising the work of the cluster teams on the ground. The document can be found here Cluster Year Book
A handbook on the Strategic Programme is now available and can be accessed via the link Strategic Programme Handbook
For further details on the Strategic Programme, contact [email protected]
Wales Audit Office Report on Primary Care Services
The Wales Audit Office have published a report on primary are and Welsh Government have subsequently issued a response. It is important to note that the report is an accurate representation of the issues at the time of the field research and much progress has been made against the issues described.
There are key recommendations and issues which will be considered by the National Primary Care Board and many of the recommendations are being addressed through the Strategic Programme for Primary Care.
One of the emerging themes is to ensure that the wider executive team within Health Boards take a leadership role on primary care as part of the whole system.
The action plan will be drafted for consideration by Health Board Chief Executives and will be discussed at the next National Primary Care Board meeting.
Update from the Directors of Primary & Community Care
Pacesetter Report
Two themes have emerged from the most recent pacesetter proposals:- workforce- quality improvement.The theme of workforce has been well received and is being developed in partnership with Health Education & Improvement Wales (HEIW) and the theme of quality improvement will be taken forward by the National Clinical Lead for the Strategic Programme. The proposals will
be finalised for approval by Directors of Primary Care and Chairs action will be undertaken in order to submit to Welsh Government in January 2020.
Winter PlanningFollowing the work undertaken by the Directors of Primary Care to inform the Winter Planning Framework for 2019/20, a review of primary care schemes in each of the Health Boards had been undertaken with key themes emerging such as domiciliary care, advanced care planning and out of hours resilience. The impact of these schemes will be measured and will inform the learning for next year’s winter planning.
Update from the Primary Care Hub
National Primary Care Conference Full details from the conference are now available in Welsh and the hyperlink to the supporting papers and videos is below:National Primary Care Conference 2019
Over 400 delegates attended the conference with a focus on showcasing the development of clusters and the primary care model for Wales. Feedback has been positive.
Closed sessions with the Cluster Leads and Practice Managers were undertaken with the Minister and Andrew Goodall. Common themes raised in all of the sessions were:
- Funding arrangements- Workforce - IM&T- Evaluation expertise- The need for All Wales polies and procedures at practice level
Actions are in place to address the issues raised.
Care Model For Wales Evaluation Tender ProgressThe Consortium have finalised their report confirming the components of the Primary Care Model for Wales (PCMW) as the theory of change, and concluded workshops designed to inform logic models for each component of the model. These models incorporate maturity level descriptors and associated measures, a prioritised selection of which will contribute to the PCMW evaluation plan. The tender is on track within both cost envelope and slippage tolerances, with the final two deliverables (evaluation plan and reporting pro forma) expected before end March 2020.
Cluster Working in Wales HandbooksA series of digital handbooks on Cluster Working in Wales have been developed and are now available to view online or download via the primary care one website. (http://www.primarycareone.wales.nhs.uk/news/51916). The handbooks provide practical advice and ideas and signpost additional resources for anyone new to a cluster leadership role, or who wants to become involved in cluster working. Although presented as three separate handbooks to enable focussed reading, they are designed to complement each other and will be most effective if used collectively.
The next meeting is 9.30am on 14 February 2020.
5.3.1 Appendix 1 - Strategic Programme Update
1 5.3.1 Strategic Programme Update for NPCB PCPHPC 10 February 2020.docx
Appendix A
Page 1
Strategic Programme for Primary Care
Programme Highlight Report: November 2019(Reporting period: 1 September 2019 to 30 November 2019)
An overall programme rating of AMBER has been assigned by the Strategic Programme Board.
This rating reflects that: a library of resources have been successfully delivered and progress in specific areas is being made at an increased pace and scale; however a number of deliverables will require modifications to the original project plans to enable delivery.
Intervention / adjustment required to deliver on time / to specification.
On track to deliver on time / as per specification.
Nov 19
Appendix A
Page 2
Work Stream Updates:
RAG (Previous / Current / Predicted)
Key Activities and Achievements Key Issues, Exceptions and Risks Priorities for Next Quarter
1. Prevention and Wellbeing
G A A Launch of resources which outline the Public Health Wales system offer to clusters in addressing immunisation and screening.
Development and promotion of smoking infographics for primary care (Help Me Quit) at National Primary Care Conference Nov 19.
Presentation and positive engagement with All-Wales Directors of Public Health Leadership Group (DPH) (15 Nov.)
The BP self-measurement pilot is live.
Continuous improvement of the PCNA tool
A change to work stream scope is proposed: inclusion of the Inverse Care Law programme (ICL).
Timeline slippage and data challenges with obtaining centralised Make Every Contact Count (MECC) data (to inform the setting of targets across Wales).
Framework to support prevention in clinical settings scheduled for release Jan 20 (was Dec 19).
Working group meetings planned. To undertake remedial actions to
support and progress the MECC deliverable.
Launch of the framework to support prevention in clinical settings.
Hosting of an All-Wales Social Prescribing workshop (9 Dec).
Review of all Cluster IMTP Prevention & Wellbeing chapters.
To maintain contact with Building A Healthier Wales in order to shape deliverable.
(Subject to Exception Report approval) To produce a management plan for the Inverse Care Law activity.
2. 24/7 Model G A G Launch of Winter Planning Framework 2019-20 (2nd Sept.).
First round out of hours (OOH) peer reviews and on-site visits completed; learning shared and improvement action plans issued.
Second round OOH reviews are underway.
Draft ‘OOH’ Urgent Dental and Mental Health crisis pathways produced.
All-Wales Escalation Levels agreed and draft process issued (Nov 19).
Risk: Health Boards not being responsive to the new winter themes and defaulting to previous year plans.
Issue: Limited Health Board engagement to support winter theme implementation, learning and good practice.
Issue: OOH Mental Health tool was agreed in principle over two years ago but there were difficulties operationalising it.
Issue: Escalation tool not formally launched in Nov 19 as scheduled; although guidance issued and pressure levels agreed. Escalation requires a set
To provide the National Unscheduled Care Board with an overview of each primary and community care key actions for winter planning.
Monthly winter teleconferences to be established and evaluation framework to be developed.
Completion of second round OOH peer reviews and on-site visits.
Draft OOH Dental and Mental Health pathways subjected to Primary Care Reference Group and Strategic Programme Board review.
Production of draft All-Wales OOH Palliative Care Pathway.
Appendix A
Page 3
of supporting questions which will be assigned to the Data & Digital group to develop. Handover of digital solution to Digital & Data group also made.
Issue: The mapping of Primary Care contracted services (in a locality) requires a modification to timeline and potentially scope.
Partnership working with Data & Digital group to:
o Develop a set of supporting, Escalation questions
o test feasibility of digital solution
Continuous, strategic work with Welsh Government on potential national, alternative escalation system.
To gather further intelligence and data to inform:
o mapping of direct access Primary Care contracted services in a locality
o Development of clinical triage toolkito Regional Partnership Board Peer
Review Tool.Work Stream Updates: Key Activities and Achievements Live Issues and Risks Priorities for Next Quarter
3. Data and Digital Technology
G R A Task & Finish groups established; specific deliverables assigned.
A survey to compile Cluster IT system requirements has been developed.
A once-for-Wales template to report Health Board progress against access standards has been agreed.
GP contact data validation exercise being undertaken in 26 general practice sites across Wales.
Scoping of Time Spent at Home is underway.
Issue: System improvement recommendations will not be presented to the Strategic Programme Board in Dec 19. Modification of timeline required.
Issue: The agreed access standard template requires two digital solutions: o online solution for practice–level
inputo a tool to compile/ analyse
information at Health Board level. Issue: Digital solutions require NWIS
resource. This has recently been prioritised to meet QAIF requirements.
Issue: Developing guidance for stakeholders on work requests for the National Informatics plan has been deprioritised. Modification to timeline may be required.
Development of digital solutions to support:o Access Standardso ‘In hours’ Escalation process
Go-live of Cluster IT survey; feedback to be analysed.
Review results of the GP Contact Data validation exercise. Next steps (to support roll out of data across Wales) to be determined.
To conclude scoping of Time Spent at Home and present a whole system measure for use across Wales.
To develop WG Delivery Milestones measures and data sources (2019-20, 2020-21) and proactive planning to support 2021-22.
To assign the new WG Digital Director as the technology
Appendix A
Page 4
Issue: GP contact data validation exercise signals large variance between local and nationally gathered data. Modification to timeline and additional actions are required.
Issue: Camden CCG no longer use Time Spent at Home (rationale unknown). An alternative measure may need to be implemented.
Issue: Welsh Government Delivery Milestones are not developed in line with the WISB standard development processes. The work stream is working reactively to identify pragmatic and consistent measures and data sources accordingly.
Issue: The technology deliverable has made very little progress.
deliverable lead and to explore linkages with the Technology Enhanced Care Programme.
Work Stream Updates: Key Activities and Achievements Live Issues and Risks Priorities for Next Quarter
4. Workforce and Organisational Development
G A G Re-focussing of deliverables to meet four key areas:1. Workforce shape2. Resources3. Efficiency; and 4. Leadership
Development of a visual, depicting the ‘Primary Care Workforce Model’.
Wales National Workforce Reporting System (WNWRS) is operational across Wales.
Population-based Workforce Planning Approach (guidance) issued to all Health Boards. Webinars also in development.
New web content launched:
Issue: Timeline for WNWRS data extraction (which will enable reporting at All-Wales, Cluster and Health Board levels, to inform workforce planning) requires modification.
Risk: Any once-for-Wales demand and capacity model/tool will require funding.
Risk: Maintenance and content management of the newly launched OOH website will be subject to a change of ownership in March 2020.
Issue: An agreed timeline to deliver a once-for-Wales demand and capacity model/tool is required.
Issue: Delivery of training for ‘GP trainers’ is being negatively impacted by lack of physical space.
Using the ‘Primary Care Workforce Model’ as a basis for gap analysis and fresh ideas e.g. gaps present opportunities for potentially new interdisciplinary roles.
To overcome WNWRS barriers; enabling data extraction in Jan 20.
To develop a workforce planning template (for Clusters) and launch via most effective communication mechanism.
To highlight and ensure inclusion of the primary care offer/functions within the NHS Wales Learning & Development Framework being developed by HEIW.
Appendix A
Page 5
o recruitment portal ‘GP Wales’; and
o Urgent Primary Care (OOH) website and a digital marketing campaign.
‘Demand and capacity’ tool scoping is making progress; including feasibility of ‘in-house’ development versus external procurement.
Positive response from GPs wanting to become trainers (109 applications to date).
14 optometrists enrolled and studying Independent Prescribing (enabling more patents to be managed in optometry practices.)
Issue: The timeline and communication mechanism to deliver a workforce planning template (for Clusters) requires modification.
Issue: HEIW are establishing a group to coordinate administration of training for multiple professions in primary care learning environments. Governance and reporting arrangements to be explored.
Issue: Discrepancy between relocation expenses for returning GPs in England versus Wales exists.
Work Stream Updates: Key Activities and Achievements Live Issues and Risks Priorities for Next Quarter
5. Communication and Engagement
G R A Collaborative working with PR agency to design an effective national primary care campaign.
Range of engagement activities held with Health Board communication leads.
Raising awareness of the Primary Care Model (via the promotion of the Strategic Programme) via:
o Strategic Programme Handbook
o Webpages; and o a social media
channel (Twitter)
Issue: Early collaborative working with Health Boards has signalled that further investment and time to prepare local campaigns for national message inclusion is required; this will result in modification to the national campaign approach and launch date.
Issue: The following deliverables (assigned from work stream 6) were deprioritised and will require modification to delivery timelines:o refreshed PCM visual;o refreshed descriptor for the vision for
Clusters. Risk: Communications staff (WG and
Health Boards) may have different priorities and resources available to
Engagement with the All-Wales Health Board communication leads to produce ‘Newsletter’ text for all Health Boards to adapt locally.
Appendix A
Page 6
support national campaign (e.g. Brexit preparedness).
Work Stream Updates: Key Activities and Achievements Live Issues and Risks Priorities for Next Quarter
6. Transformation and the Vision for Clusters.
G A G Clusters used the Strategic Programme produced IMTP reporting template.
Completion of first cluster development review (reconciling the findings from a bespoke sample review of clusters, with challenges listed on the cluster register).
The National Primary Care Conference (7 Nov 19) was successful in profiling the development of clusters and the sharing of best practice. The day included:o Ministerial session with
Cluster leads.o A dedicated practice
manager’s session with the Director General for Health and Social Services/CEO of NHS Wales.
o Launch of a Cluster ‘year-book’
The register of Cluster challenges has been made available on-line.
Continuous engagement with wider stakeholders and alignment with national programmes.
Issue: Engagement with the All-Wales Health Board communication leads to create shared vision and draft a descriptor.
Issue: Timeline for a refreshed descriptor remains as ‘TBC’. This work will be inlfuenced by:o HB Comms Leads inputo A reflection of learning, intelligence
gathering and cluster feedback provided at the National Primary Care Conference 2019
o Input from the King’s Fund regarding advice on simplying the vision.
Cluster IMTP responses to be compiled and analysed. Findings from across Wales to help understand current landscape and inform next steps.
Cluster Yearbooks to be made available online.
Working to ensure timely achievement of actions as prescribed within the cluster register of challenges.
To complete the development of the Primary Care Model evaluation framework.
Release of the Cluster Leads Handbook – Cluster Working in Wales.
Results of Primary Care Model insight work to inform next steps and other relevant areas of work.
Appendix A
Page 7
Work with Northern Ireland, resulting in further two-way MDT development learning.
Development of the evaluation framework to assess delivery of the Primary Care Model is underway. Health Board stakeholder events held.
Funding has been secured to commission insight work with primary health care professionals, to gain their understanding of the barriers and facilitators to how they communicate the Primary Care Model to patients.
6.1 Comittee Highlight Report
1 6.1 Committe Highlight Report v1 - inc. guidance notes.docx
Choose an item.
Choose an item.
DATE OF MEETING (DD/MM/YYYY)
PUBLIC OR PRIVATE REPORT Choose an item.
IF PRIVATE PLEASE INDICATE REASON Choose an item.
PREPARED BY (Please Include Name and Title)
PRESENTED BY
EXECUTIVE SPONSOR APPROVED Choose an item.
REPORT PURPOSE FOR NOTING
ACRONYMS
1. PURPOSE
1.1 This paper had been prepared to provide the Board with details of the key issues considered by the (INSERT MEETING NAME) at its meeting on the (INSERT DATE).
1.2 Key highlights from the meeting are reported in section 2.
1.3 The Board is requested to NOTE the contents of the report and actions being taken.
2. HIGHLIGHT REPORT
Page 2 of 2
ALERT / ESCALATE
To include where applicable:
Explicit references to any items on the risk register that needs to be escalated.
Items endorsed by Committee for further consideration by the full Board e.g. policies, business cases, reports.
ADVISE
To include where applicable:
External/Independent Reports/Reviews (e.g. WAO reports, HIW, WG Policies/Initiatives.
Internal Control Issues (e.g. Internal Audit Reports, system effectiveness, resource management)
Corporate Risk Register - (explicit reference should be made to the risks discussed and any direction agreed by the committee to help mitigate/reduce the risk)
ASSURE
To include where applicable:
External/Independent Reports/Reviews (e.g. WAO reports, HIW, WG Policies/Initiatives.
Internal Control Issues (e.g. Internal Audit Reports, system effectiveness, and resource management).
INFORM
Choose an item.APPENDICES
6.2 Forward Look
1 6.2 Forward Look PCPHPC 10 February 2020.docx
Agenda Item 6.1
Forward Look Page 1 of 3 PCPHP Committee10.2.2020
CWM TAF MORGANNWG UNIVERSITY HEALTH BOARD
PRIMARY & COMMUNITY COMMITTEE FORWARD LOOK - 2020
Meeting Standing Items/Governance Performance & Assurance For Information10th February 2020 Minutes
Action Log Declarations of Interest Forward Work Programme Terms of Reference To Agree a Vice Chair
Report of Director of Primary, Community & Mental Health (which may encapsulate some of the issues below if there does not warrant a stand-alone report)
Update on Community Hospital Improvement Plans (then due Summer of 2020)
ICL (Public Health) 111 Roll-out Update inc. update on leasing
arrangements for relocation of Primary Care Centre, PCH HIW/DU Reports & Action Plans – if any
received
Palliative Care Update Primary Care Estates Strategy (standing
item from July 2019 meeting) Population Health Programme Update
(standing item from July 2019 meeting) Transformation Improvement Fund
Update(standing item from July 2019 meeting)
Risk Register Healthy Weights Internal Audit Report – Primary Care
IMTP Monitoring Report National Primary Care Board
Update Strategic Programme Update Primary care Services in Wales
WAO Report
Agenda Item 6.1
Forward Look Page 2 of 3 PCPHP Committee10.2.2020
Meeting Standing Items/Governance Performance & Assurance For InformationUpdate on Stroke Services arising from previous DoPH Annual Report – to be prepared for FPW Committee rather than PCPH &P Committee
9th June 2020 Minutes Action Log Declarations of Interest Forward Work Programme Committee Annual Report & Self-
Assessment 2019/20
Report of Director of Primary, Community & Mental Health (to potentially include some of issues below if the update doesn’t warrant a stand-alone report)
Primary Care Estates Strategy (standing item from July 2019 meeting)
Population Health Programme Update (standing item from July 2019 meeting)
Transformation Improvement Fund Update(standing item from July 2019 meeting)
Risk Register Immunisation Report Primary Care Indicators Oral Health Update (deferred from October 19 &
February 20 as CADO unable to attend either meeting)
Social Prescribing Concept (deferred from February 2020)
IMTP Monitoring Report National Primary Care Board
Update Strategic Programme Update
Agenda Item 6.1
Forward Look Page 3 of 3 PCPHP Committee10.2.2020
Meeting Standing Items/Governance Performance & Assurance For Information
7th October 2020 Minutes Action Log Declarations of Interest Forward Work Programme
Report of Director of Primary, Community & Mental Health (which may encapsulate some of the issues below if there does not warrant a stand-alone report)
Primary Care Estates Strategy (standing item from July 2019 meeting)
Population Health Programme Update (standing item from July 2019 meeting)
Transformation Improvement Fund Update(standing item from July 2019 meeting)
Risk Register
IMTP Monitoring Report National Primary Care Board