38
Burns, Bites and Stings of Animals and Insects Patrick C. Obasi
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | jeremiah-manners |
| View: | 217 times |
| Download: | 0 times |

Burns, Bites and Stings of Animals and Insects
Patrick C. Obasi

Rabies
Wild animals constitute the most potential source of infection for both humans and domestic animals in US
About 10,000 pts receive post exposure prophylaxis for rabies annually
Most domestic animal bites are provoked by attack.
Post exposure prophylaxis combining local wound treatment, passive immunization, and vaccination is very effective
Any wild animal that bites or scratches a person should be killed at once

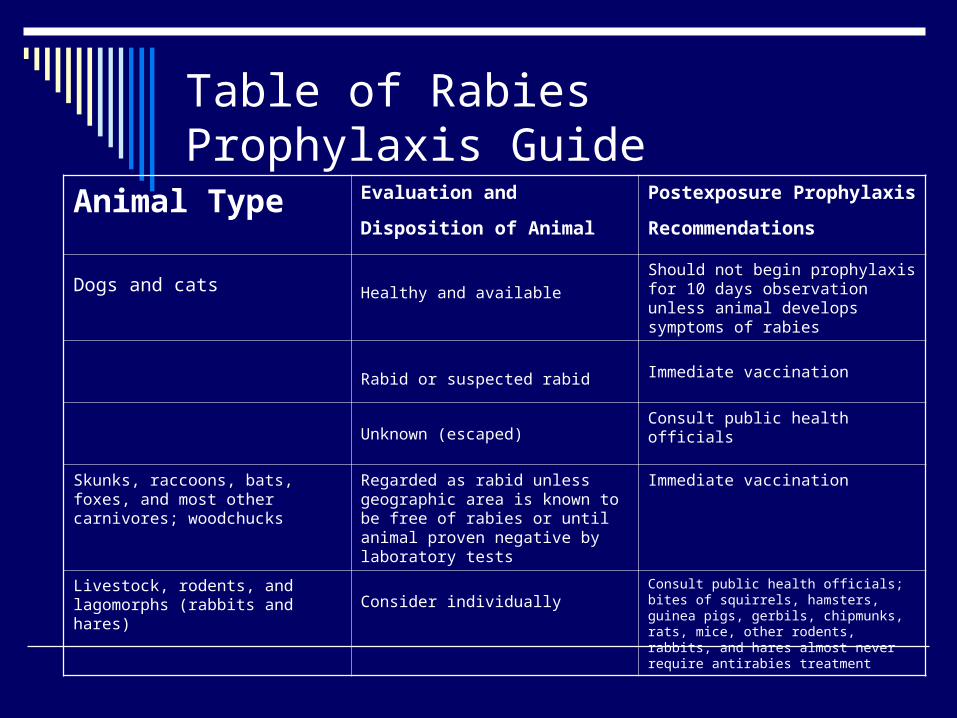
Table of Rabies Prophylaxis Guide
Animal Type Evaluation and Disposition of
Animal Postexposure Prophylaxis
Recommendations
Dogs and cats Healthy and available
Should not begin prophylaxis for 10 days observation unless animal develops symptoms of rabies
Rabid or suspected rabid Immediate vaccination
Unknown (escaped) Consult public health officials
Skunks, raccoons, bats, foxes, and most other carnivores; woodchucks
Regarded as rabid unless geographic area is known to be free of rabies or until animal proven negative by laboratory tests
Immediate vaccination
Livestock, rodents, and lagomorphs (rabbits and hares) Consider individually
Consult public health officials; bites of squirrels, hamsters, guinea pigs, gerbils, chipmunks, rats, mice, other rodents, rabbits, and hares almost never require antirabies treatment

Rabies:Local Care of Animal Bites
Thorough irrigation Cleansing with soap solution Debridement Administration of tetanus toxoid Abx

Rabies Vaccination
2 rabies vaccines currently available in US Rabies vaccine adsorbed (RVA) (Imovax) Human diploid cell rabies vaccine (HDCV)
Either administered with HRIG (Imogan rabies)
Vaccine administered intramuscularly in deltoid area for adult and anterolateral aspect of thigh for children

SFX of Vaccines
Muscle aches Headache Nausea Abdominal pain Pain, erythema, swelling, itching at
injection site Neurologic illness Note: Steroids can interfere with the
development of active immunity

Manifestations of Rabies
Paresthesia Headache Stiff neck Lethargy Pulmonary sxs Maniacal behavior Muscle spasm of throat with dysphasia Convulsion →coma →paralysis →death

Snakebites
Poisonous snakes of medical importance are of members of the family crotalidae or pit vipers
Coral snakes of the elapidae family also important
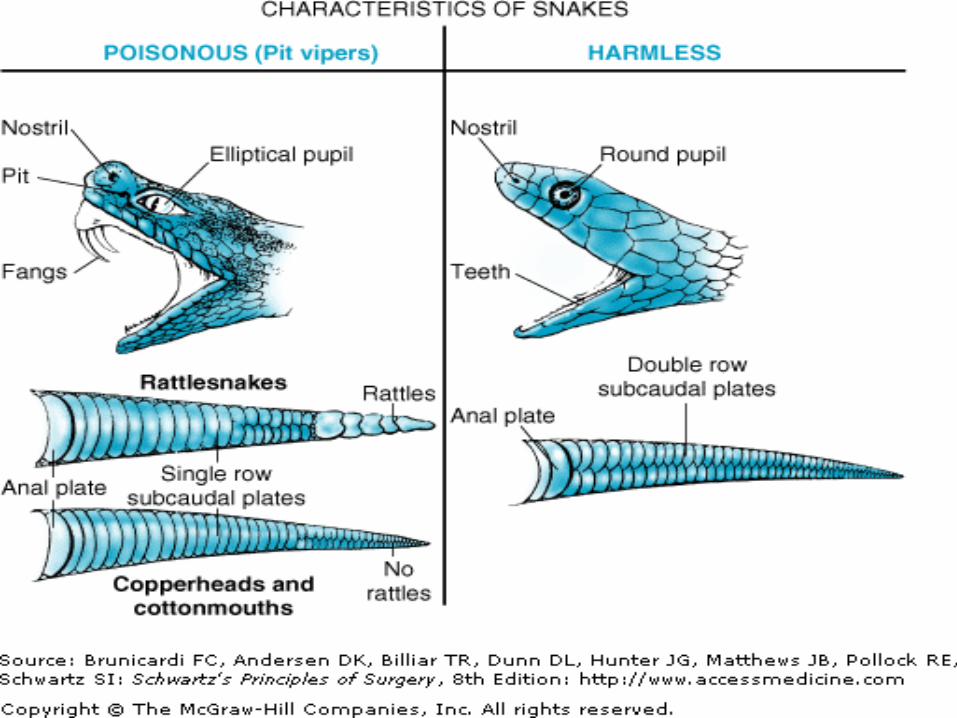
Poisonous snakes identified by their elliptical pupil
Non poisonous snakes do not have pits and fangs
Poisonous snakes have single row of sub caudal plates

Clinical Manifestation of Envenomation
Hypotension Weakness Nausea/vomiting Pain, swelling, tenderness and
ecchymosis at site of bite Paresthesia and muscle fasciculations Defect in blood coagulation Pulmonary edema

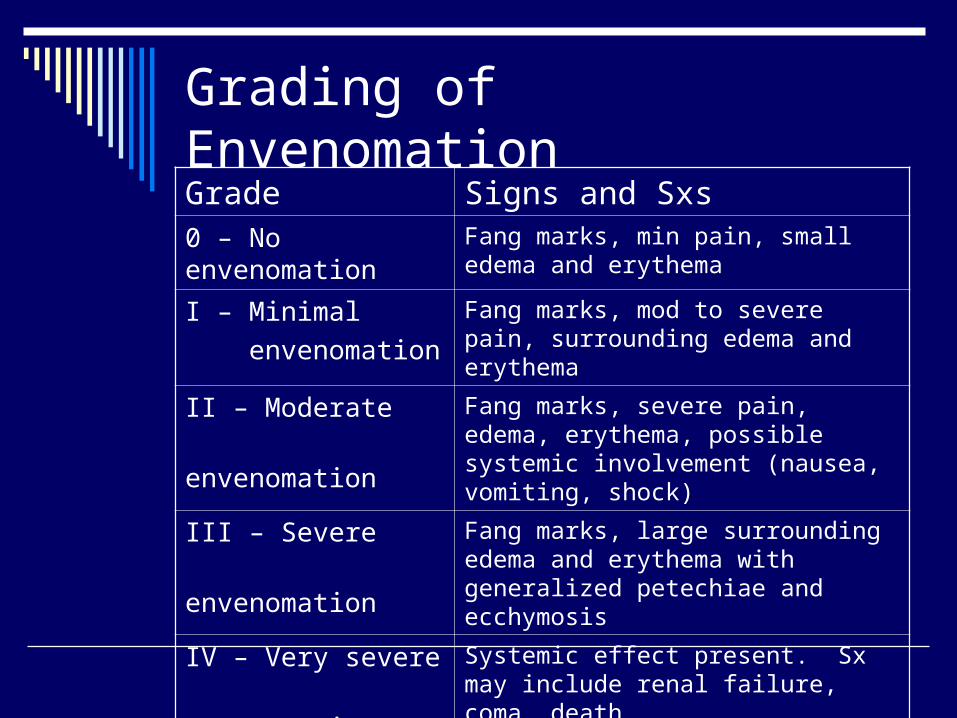
Grading of EnvenomationGrade Signs and Sxs0 – No envenomation Fang marks, min pain, small edema and
erythema
I – Minimal
envenomation
Fang marks, mod to severe pain, surrounding edema and erythema
II – Moderate
envenomation
Fang marks, severe pain, edema, erythema, possible systemic involvement (nausea, vomiting, shock)
III – Severe
envenomation
Fang marks, large surrounding edema and erythema with generalized petechiae and ecchymosis
IV – Very severe
envenomation
Systemic effect present. Sx may include renal failure, coma, death

Management of Snakebites
Application of a tourniquet, incision and suction are appropriate if done within one hour from time of bite
The most important treatment for snakebite is antivenin (crotalidae polyvalent immune fab)
IVF required to replace the decreased extra cellular fluid volume resulting from edema formation
Fascial planes may become tense with obstruction of venoms and later arterial flow, requiring fasciotomy
Vit K may be required to correct bleeding and clotting abnormalities
Tetanus toxoid administered and abx recommended to prevent secondary infection


Insect Stings
Group includes the honey bee, bumblebee, wasp, hornets and fire ants
Venom is just as potent a that of snakes Sxs consist of
*Localized pain *Petechial hemorrhages
*Swelling of skin and mucus membrane
*Generalized erythema *Abdominal cramps
*H/A *Pulmonary and cerebral edema
*Blurred vision *Vascular collapse

Insect Stings
Death results from combination of shock, respiratory failure and CNS changes
Most death from insect sting occur within 15 to 30 minutes
Early application of a tourniquet may prevent rapid spread of venom
Emergency kit containing epinephrine commercially available

Black Widow Spider

Spider Bites:Black Widow Spider The most biting spider in US is the black widow
(latrodetus mataus) Its venom is neurotoxic Generalized muscle spasm is the most prominent
physical finding Other sxs are nausea/vomiting, headache Priapism and ejaculation (have been reported) Tx:
Narcotics for pain Muscle relaxant for spasm Calcium gluconate relieves most sxs
Most pts recover within 24 hrs

Brown Recluse Spider

Spider Bites:Brown Recluse Spider Severe bite results in necrosis and sloughing of
skin with residual ulcer formation Pathophysiology of bite: intravascular
coagulation →formation of micro thrombi → capillary occlusion → hemorrhage → necrosis
Sxs include fever, nausea, vomiting, weakness, arthralgia, malaise, petechiae
Hemolysis and thrombocytopenia responsible for death


Brown Recluse Spider
Tx: Early excision Corticosteroids Heparin Dapsone (reduces inflammation at site of
venom injection)


Scorpion Stings
Only the bark scorpion (centraroides exilicanda) medically important
Found mainly in the desert of Southwest Venom is neurotoxic Diagnosis reinforced by the “tap test” Sxs include anxiety, blurred vision, or
temporary blindness, dyspnea, wheezing, involuntary urination and defecation, SVT, SZ

Scorpion Stings
Tx: Airway management Treat arrhythmias and HTN if indicated Calcium gluconate for muscle spasms No narcotics (aggravate neurotoxic effects) Goat-derived antivenin available only in
Arizona

Burns-Classification

Burns-Classification

Rule of Nines

Rule of Nines
Topical Treatment of Burns
Silver Nitrate Causes electrolyte imbalances (Na+, Ca+, Po4-, Cl-) No Pseudomonas sp. coverage Limited eschar penetration
Silvadene (Silver Sulfadiazine)
Can cause neutropenia and thrombocytopenia Limited eschar penetration and ineffective against Pseudomonas sp Sulfa allergy
Sulfamylon (Mafenide Sodium) Carbonic anhydrase inhibitor Coverage against Pseudomonas sp Painful For burns over cartilage
Parkland Formula
Measure of adequate resuscitation
Escharotomy –(indication, timings)
Indications for Intubation
Complications after Burns (ulcer types)

Parkland Formula
For burns > 20% 4cc/kg x % body burn x 24 hrs Give half in 8 hrs
Parkland Formula
Measure of adequate resuscitation Urine Output
1cc/kg in adult and 2-4 cc/kg in peds Escharotomy –(indication, timings)
Circumferential burns Problem with ventilation with chest burns
Indications for Intubation Upper airway stridor or obstruction, hypoxemia,
Complications after Burns (ulcer types) Curling’s Marjolin’s








![Common Bites and Stings Final - Handout.ppt Bites... · Microsoft PowerPoint - Common Bites and Stings Final - Handout.ppt [Compatibility Mode] Author: free42 Created Date: 1/23/2020](https://static.documents.pub/doc/80x56/5f5cd628d13de6545a286646/common-bites-and-stings-final-bites-microsoft-powerpoint-common-bites-and.jpg)








