22
Business and disparities in South Carolina SC Business Coalition on Health Board meeting June 16, 2015
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | charlotte-cooper |
| View: | 215 times |
| Download: | 0 times |

Business and disparities in South Carolina
SC Business Coalition on Health Board meetingJune 16, 2015

The SC Health Coordinating Council is now the…
*Formal announcement will be made on June 23, 2015
Some definitions
• Population health
• Health Disparities
Population Health
Health outcomes of the population. Inclusive of the distribution of the outcomes inside the population.

Health Disparities
• Inequalities that exist when members of certain population groups do not benefit from the same health status as other groups.
• Health disparities are caused by a complex interaction of multiple factors including individual, genetic and environmental risk factors, pervasive structural inequities and social determinants of health.
Data
• Disparities among the employed in South Carolina
• Disparities among the insured in South Carolina
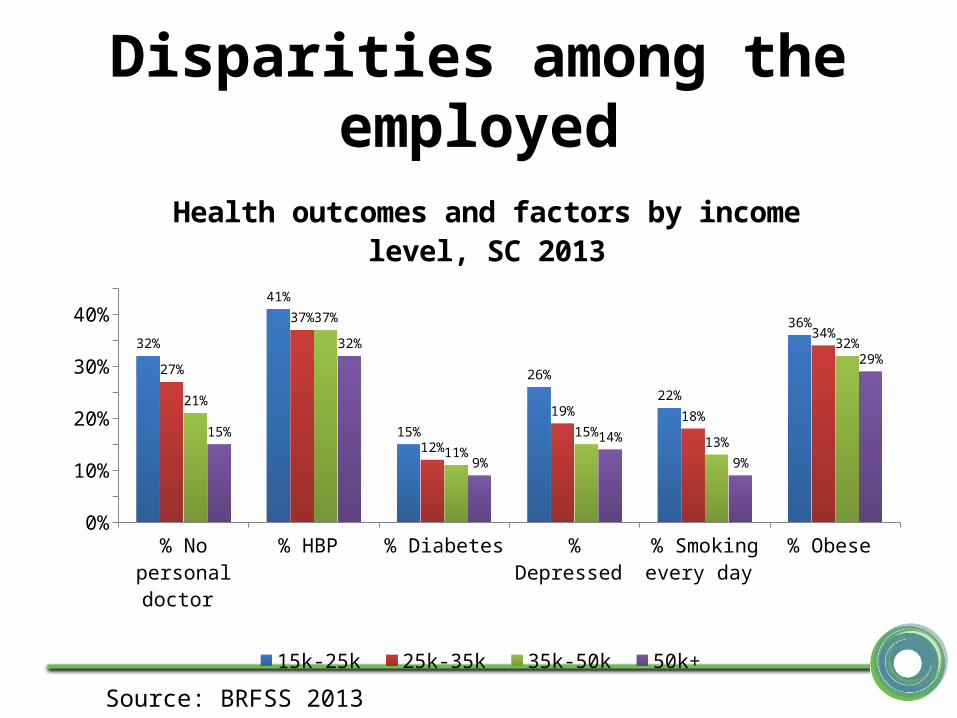
Disparities among the employed
% N
o pe
rson
al d
octo
r
% H
BP
% D
iabe
tes
% D
epre
ssed
% S
mok
ing
ever
y da
y
% O
bese
0%
10%
20%
30%
40%32%
41%
15%
26%22%
36%
27%
37%
12%
19% 18%
34%
21%
37%
11%15% 13%
32%
15%
32%
9%14%
9%
29%
Health outcomes and factors by income level, SC 2013
15k-25k 25k-35k 35k-50k 50k+
Source: BRFSS 2013

Disparities among the insured
Estimated cost of Prematurity/LBW: $15,000 hospital stay vs $600 for normal birth
$51,000 over life time
LBW and prematurity CAN be prevented!
Overall White Black0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
7.9%6.7%
12.6%
10.4% 9.8%
13.1%
Prematurity and Low birth-weight. Insured population.
SC 2009-2013
LBW Prematurity
Source: Vital statistics
Why should employers care?
• National data indicate that over the 10-year period from 2009-2018, the total cost of
health disparities will be approximately $337 billion dollars, with $117 billion incurred
by private insurers*.
• Racial and ethnic minorities now comprise roughly one-third of the U.S. population,
and are expected to represent a 54% majority by 2050.
• Employers shoulder the lion’s share of health care costs to cover their employees
and families, yet not every enrollee is able to receive the optimal level of health care.
• Health disparities associated with race and ethnicity persist even minorities have
adequate health benefits coverage, equivalent socioeconomic status and comparable
co-morbidities.

Key stakeholders to solve the problem
Peers Employers
Communities

Peer support: a powerful tool
• decreases morbidity and mortality rates• increases life expectancy• increases knowledge of a disease• improves self-efficacy• improves self-reported health status and self-
care skills, including medication adherence• reduces use of emergency services• Additionally, providers of social support report
less depression, heightened self-esteem and self-efficacy, and improved quality of life.
Scope of influence of the employers
• Inside the organization– Employees spend 8-10 hours a day at
their job– Policy and environmental changes– Incentives• Wellness programs• Benefit design

Scope of influence of the employers
• In the community/geographic area of influence
– The current and future workforce come from these areas
– Business leaders are influential in policymaking, and with their peers


Relevance for Wellness Programs
A “one size fits all” approach to health and wellness programs does not
work because different groups of the population (minorities, lower income
jobs, etc) experience stark differences in health conditions and
outcomes as well as preventive, diagnostic and treatment services
provided.

Relevance for Wellness Programs
• Good health outcomes are a set of products/services you sell, so you can cut your costs – Worksite wellness programs– Chronic disease management programs– Benefit packages
• You identify your target population (Collect, stratify, and use data!!!)
• You focus group your populations (Learn from your target population what matters and moves them)
• You develop products/publicity that resonate with your populations, and often are promoted by people of influence in your target population

SC Health Coordinating Council Call to Action for Health Equity
For improving health for ALL in South Carolina

Health Equity starts in our organization
A. Data driven interventions– Identify the groups of the population that require additional support
(Checklist section II)
B. Cultural competence and responsiveness:– Tailored communication strategies, trust building, empathy (Checklist
section IV)– Culturally competent care provision
C. Inclusive decision making:– Wellness teams composed of peers of the diverse individuals that
you have prioritized– Filling the pipeline!!
D. Community engagement:– Identify hot-spots in your area and partner with organizations that
can help improve the social determinants in those areas– Leverage business leader influence to improve the health of those
areas supplying your workforce
The ask
• Launching partner – SCBCH and members– Pioneer organizations making the commitment to make
improvement in the four building blocks of the call to action
– Organizations that will advocate for the adoption of the call to action by other organizations
– Organizations that commit to share best practices, good contacts, successes and lessons learned to accelerate improvement in health equity in South Carolina.
– Confirm by July 31
• Peer coaches– Volunteer to be a resource for organizations joining the call
to action for one or more of the building blocks

Launching partners (6/15/15)
Tools for business (National Business Group on Health)
• Health Disparities Cost Impact Tool• Getting started• Checklist• Case studies• Marketing techniques to reach diverse empl
oyees• Toolkit to reduce health disparities in the wo
rkplace• Complete disparity resources by the Nationa
l Business Group on Health

Tools to get to know the community
• http://www.communitycommons.org/maps-data/
• Census, BRFSS, Vital Statistics, etc
• Local community meetings
• Email [email protected] to brainstorm

















