Page 34 - VETcpd - Vol 1 - Issue 3 Canine Cruciate Disease – Options for Management In a previous article the authors discussed the aetiology and diagnosis of canine cranial cruciate ligament (CCL) disease. It was explained that the understanding of this disease has evolved in recent years, with a shift from an emphasis on a traumatic to a degenerative aetiology. Management options for cruciate disease in dogs are numerous, and novel surgical techniques, adopted to take account of the paradigm shift in our understanding, are gaining in popularity. Some controversy surrounds the subject of optimal surgical management of this condition in the dog, and the reader should not expect this article to answer all the questions. Key words: canine, orthopaedics, CCL, cruciate disease, management, stifle. Introduction Management of cruciate disease should aim to restore quality of life and to minimise the rate of progression of joint pathology in future. The two primary considerations are: 1. Intra-articular inspection. Injured menisci and possibly inflamed remnants of CCL tissue have been implicated in promoting local inflammatory processes (Fujita and others 2006) and may result in ongoing lameness despite effective joint stabilisation. 2. Stabilisation of the joint. Cranial tibial subluxation during femoro-tibial compression results in abnormal contact forces on articular cartilage and menisci and hinders the stifle joint’s normal weight bearing function. Interventions should aim to minimise cranial tibial subluxation. The previous article emphasised that osteoarthritis is an inevitable consequence of cruciate disease. Management of osteoarthritis should be discussed with the clients prior to any suggestion of intervention. The approach to osteoarthritis is beyond the scope of this article but typically involves weight reduction, exercise modulation and medication (NSAIDs, nutraceuticals, regenerative medicine etc). Conservative management of the cranial cruciate ligament deficient stifle The veterinary literature contains a paucity of comparisons of conservative management and surgical treatment of cruciate disease in dogs. In 1984 Vasseur published a commonly quoted review in Philip Witte BVSc, BSc, CertAVP, MRCVS Philip graduated from the University of Bristol in 2005. Following two years’ work in mixed practice he completed a surgical internship and orthopaedic residency at Southern Counties Veterinary Specialists. He completed the RCVS Certificate in Advanced Veterinary Practice in September 2013 and is due to sit the RCVS Diploma in Small Animal Surgery (Orthopaedics) in 2015. Harry Scott BVSc, CertSAD, CBiol, FSB, DSAS(Orth), FRCVS, CCRP; RCVS Recognised Specialist in Small Animal Surgery (Orthopaedics) Harry graduated from the University of Liverpool. During several years in general small animal practice Harry gained RCVS certificates in dermatology and small animal surgery, became a Fellow of the RCVS in 1992 and gained the RCVS diploma in small animal surgery (orthopaedics) in 1999. He has worked at referral centres in orthopaedics and neurology in the UK and abroad. He is due to sit the European diploma in veterinary neurology in 2015. Southern Counties Veterinary Specialists Forest Corner Farm, Hangersley Ringwood, Hampshire BH24 3JW E: [email protected]Tel: (01425) 485615 www.scvetspecialists.co.uk VET cpd - Orthopaedics For Orthopaedic Referrals in your area visit: vetindex.co.uk/ortho For Orthopaedic Equipment: vetindex.co.uk/orthoequip For Xray equipment: vetindex.co.uk/xray ® 16th Edition 14 The year round guide to veterinary products, supplies and services The year round guide to veterinary products, supplies and services 2014 www.vetindex.co.uk 20th Edition b Partrid Peer Reviewed which 85.7% of dogs <15kg and 19.3% of dogs >15kg were classified as improved or normal at long term follow-up following conservative therapy for cruciate disease. The suggestion was that conservative management of cruciate disease may be more effective in small dogs and less effective in larger dogs. Techniques for conservative management in that report included periods of lead-controlled exercise, weight loss and analgesia. Periods of exercise restriction may result in improvement in clinical function for two reasons: 1) deranged biomechanics associated with cruciate disease causes inflammation, and reducing the forces transmitted through an inflamed joint will improve comfort; and 2) a number of dogs with early cruciate degeneration only show lameness following periods of exercise, so in the absence of exercise, it is to be expected that lameness will not be seen. Intuitively, longer periods of management with an unstable stifle will result in a higher risk of acquiring meniscal injuries and faster progression of articular cartilage loss, although this has not been shown conclusively. Occasionally the authors are presented with dogs with cruciate disease which are not good candidates for surgery, for example, as a result of systemic disease. Stabilisation of the joint may be possible without any surgical intervention, with the use of orthotic braces custom-made for the individual. Braces may be worn during periods of exercise and benefit the dog by 1) permitting longer periods of activity, by supporting the joint during exercise, and 2) reducing the impact of exercise on the joint such that lameness is not worse following exercise. The authors have had
Transcript
Page 34 - VETcpd - Vol 1 - Issue 3
Canine Cruciate Disease – Options for ManagementIn a previous article the authors discussed the aetiology and diagnosis of canine cranial cruciate ligament (CCL) disease. It was explained that the understanding of this disease has evolved in recent years, with a shift from an emphasis on a traumatic to a degenerative aetiology.
Management options for cruciate disease in dogs are numerous, and novel surgical techniques, adopted to take account of the paradigm shift in our understanding, are gaining in popularity. Some controversy surrounds the subject of optimal surgical management of this condition in the dog, and the reader should not expect this article to answer all the questions.
IntroductionManagement of cruciate disease should aim to restore quality of life and to minimise the rate of progression of joint pathology in future. The two primary considerations are:
1. Intra-articular inspection. Injured menisci and possibly inflamed remnants of CCL tissue have been implicated in promoting local inflammatory processes (Fujita and others 2006) and may result in ongoing lameness despite effective joint stabilisation.
2. Stabilisation of the joint. Cranial tibial subluxation during femoro-tibial compression results in abnormal contact forces on articular cartilage and menisci and hinders the stifle joint’s normal weight bearing function. Interventions should aim to minimise cranial tibial subluxation.
The previous article emphasised that osteoarthritis is an inevitable consequence of cruciate disease. Management of osteoarthritis should be discussed with the clients prior to any suggestion of intervention. The approach to osteoarthritis is beyond the scope of this article but typically involves weight reduction, exercise modulation and medication (NSAIDs, nutraceuticals, regenerative medicine etc).
Conservative management of the cranial cruciate ligament deficient stifleThe veterinary literature contains a paucity of comparisons of conservative management and surgical treatment of cruciate disease in dogs. In 1984 Vasseur published a commonly quoted review in
Philip Witte BVSc, BSc, CertAVP, MRCVS
Philip graduated from the University of Bristol in 2005. Following two years’ work in mixed practice he completed a surgical internship and orthopaedic
residency at Southern Counties Veterinary Specialists. He completed the RCVS Certificate in Advanced Veterinary Practice in September 2013 and is due to sit the RCVS Diploma in Small Animal Surgery (Orthopaedics) in 2015.
Harry Scott BVSc, CertSAD, CBiol, FSB, DSAS(Orth), FRCVS, CCRP; RCVS Recognised Specialist in Small Animal Surgery (Orthopaedics)
Harry graduated from the University of Liverpool. During several years in general small animal practice Harry gained RCVS certificates in dermatology and
small animal surgery, became a Fellow of the RCVS in 1992 and gained the RCVS diploma in small animal surgery (orthopaedics) in 1999. He has worked at referral centres in orthopaedics and neurology in the UK and abroad. He is due to sit the European diploma in veterinary neurology in 2015.
For Orthopaedic Referrals in your area visit: vetindex.co.uk/orthoFor Orthopaedic Equipment:vetindex.co.uk/orthoequipFor Xray equipment: vetindex.co.uk/xray
®
16th Edition
VetIndex 2014 Th
e year
ro
un
d g
uid
e to v
eterin
ar
y pro
du
cts, su
pplies an
d ser
vic
es
The year round guide to veterinary
products, supplies and services
2014
www.vetindex.co.uk
Rossdales equine Hospital & diagnostic centRe
Exning, Newmarketsurgery, medicine, reproduction and clinical diagnostics for local practice and referral services
tel: 01638 577754
Rossdales equine pRacticeBeaufort Cottage Stables, High Street, Newmarket
local practice ambulatory service and out-of-hours telephone servicetel: 01638 663150
BeaufoRt cottage laBoRatoRies
High Street, Newmarket
clinical pathology
tel: 01638 663017
visit our website at www.rossdales.com
20th Edition
®
Plus
The best nutritional supplement, providing antioxidants, probiotics,
Promotes and maintains whole body health including periodontal,
intestinal, cardio-vascular, skin & joint health, immunity & energy
Bob Partridge Dipl. EVDC
European Veterinary Specialist in Dentistry
is pleased to offer dental training, practice seminars,
advice, assistance and referral services for:-
Dental Cases, Facial Trauma, Neoplasia,
Complex Extractions, Orthodontics, Tooth
Fractures, Crowns, Oral Clearance, Imaging.
SpecOakBeck Veterinary Hospital
Harrogate, HG1 3HU
01423 - 561414
Actively Supporting you and
your Client Relationship
Peer Reviewed
which 85.7% of dogs <15kg and 19.3% of dogs >15kg were classified as improved or normal at long term follow-up following conservative therapy for cruciate disease. The suggestion was that conservative management of cruciate disease may be more effective in small dogs and less effective in larger dogs. Techniques for conservative management in that report included periods of lead-controlled exercise, weight loss and analgesia.
Periods of exercise restriction may result in improvement in clinical function for two reasons: 1) deranged biomechanics associated with cruciate disease causes inflammation, and reducing the forces transmitted through an inflamed joint will improve comfort; and 2) a number of dogs with early cruciate degeneration only show lameness following periods of exercise, so in the absence of exercise, it is to be expected that lameness will not be seen. Intuitively, longer periods of management with an unstable stifle will result in a higher risk of acquiring meniscal injuries and faster progression of articular cartilage loss, although this has not been shown conclusively.
Occasionally the authors are presented with dogs with cruciate disease which are not good candidates for surgery, for example, as a result of systemic disease. Stabilisation of the joint may be possible without any surgical intervention, with the use of orthotic braces custom-made for the individual. Braces may be worn during periods of exercise and benefit the dog by 1) permitting longer periods of activity, by supporting the joint during exercise, and 2) reducing the impact of exercise on the joint such that lameness is not worse following exercise. The authors have had
Full article available for purchase at www.vetcpd.co.uk/modules/ VETcpd - Vol 1 - Issue 3 - Page 35
some success managing cases which were not good candidates for surgical intervention using custom-made trans-stifle braces produced by OrthoPets.
Surgical management of the cranial cruciate ligament deficient stifleSurgical management allows us to inspect the joint and address stifle instability. Stifle stabilisation may be performed with passive mechanisms, the aim of which is to tether the femur and tibia together using man-made or autologous tissues to resist cranial tibial subluxation; or may rely on alteration of biomechanics such that a CCL is no longer required to stabilise the joint during weight bearing.
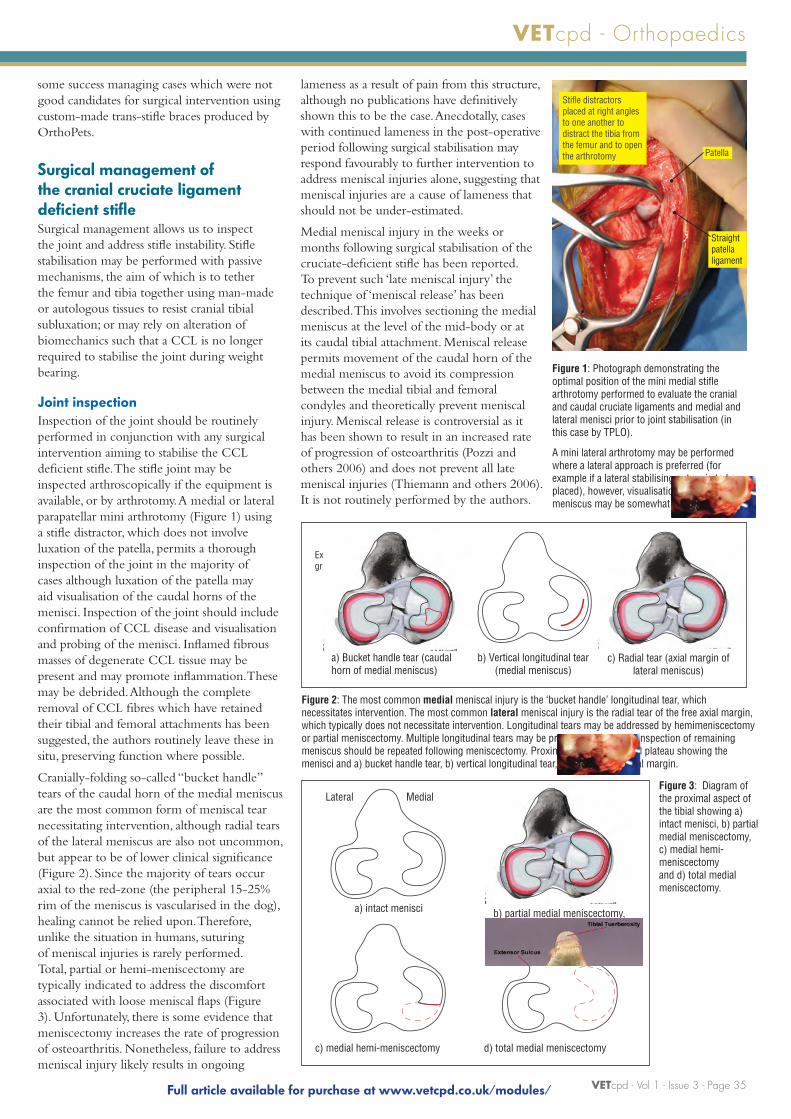
Joint inspectionInspection of the joint should be routinely performed in conjunction with any surgical intervention aiming to stabilise the CCL deficient stifle. The stifle joint may be inspected arthroscopically if the equipment is available, or by arthrotomy. A medial or lateral parapatellar mini arthrotomy (Figure 1) using a stifle distractor, which does not involve luxation of the patella, permits a thorough inspection of the joint in the majority of cases although luxation of the patella may aid visualisation of the caudal horns of the menisci. Inspection of the joint should include confirmation of CCL disease and visualisation and probing of the menisci. Inflamed fibrous masses of degenerate CCL tissue may be present and may promote inflammation.These may be debrided. Although the complete removal of CCL fibres which have retained their tibial and femoral attachments has been suggested, the authors routinely leave these in situ, preserving function where possible.
Cranially-folding so-called “bucket handle” tears of the caudal horn of the medial meniscus are the most common form of meniscal tear necessitating intervention, although radial tears of the lateral meniscus are also not uncommon, but appear to be of lower clinical significance (Figure 2). Since the majority of tears occur axial to the red-zone (the peripheral 15-25% rim of the meniscus is vascularised in the dog), healing cannot be relied upon. Therefore, unlike the situation in humans, suturing of meniscal injuries is rarely performed. Total, partial or hemi-meniscectomy are typically indicated to address the discomfort associated with loose meniscal flaps (Figure 3). Unfortunately, there is some evidence that meniscectomy increases the rate of progression of osteoarthritis. Nonetheless, failure to address meniscal injury likely results in ongoing
Figure 1: Photograph demonstrating the optimal position of the mini medial stifle arthrotomy performed to evaluate the cranial and caudal cruciate ligaments and medial and lateral menisci prior to joint stabilisation (in this case by TPLO).
A mini lateral arthrotomy may be performed where a lateral approach is preferred (for example if a lateral stabilising suture is to be placed), however, visualisation of the medial meniscus may be somewhat more difficult.
Figure 2: The most common medial meniscal injury is the ‘bucket handle’ longitudinal tear, which necessitates intervention. The most common lateral meniscal injury is the radial tear of the free axial margin, which typically does not necessitate intervention. Longitudinal tears may be addressed by hemimeniscectomy or partial meniscectomy. Multiple longitudinal tears may be present, so thorough inspection of remaining meniscus should be repeated following meniscectomy. Proximal views of the tibial plateau showing the menisci and a) bucket handle tear, b) vertical longitudinal tear, c) radial tear of axial margin.
Figure 3: Diagram of the proximal aspect of the tibial showing a) intact menisci, b) partial medial meniscectomy, c) medial hemi-meniscectomy and d) total medial meniscectomy.
VETcpd - Orthopaedics
Patella
Stifle distractors placed at right angles to one another to distract the tibia from the femur and to open the arthrotomy
Straight patella ligament
a) intact menisci b) partial medial meniscectomy,
d) total medial meniscectomyc) medial hemi-meniscectomy
MedialLateral
a) Bucket handle tear (caudal horn of medial meniscus)
MedialLateralExtensor groove
b) Vertical longitudinal tear (medial meniscus)
c) Radial tear (axial margin of lateral meniscus)
lameness as a result of pain from this structure, although no publications have definitively shown this to be the case. Anecdotally, cases with continued lameness in the post-operative period following surgical stabilisation may respond favourably to further intervention to address meniscal injuries alone, suggesting that meniscal injuries are a cause of lameness that should not be under-estimated.
Medial meniscal injury in the weeks or months following surgical stabilisation of the cruciate-deficient stifle has been reported. To prevent such ‘late meniscal injury’ the technique of ‘meniscal release’ has been described. This involves sectioning the medial meniscus at the level of the mid-body or at its caudal tibial attachment. Meniscal release permits movement of the caudal horn of the medial meniscus to avoid its compression between the medial tibial and femoral condyles and theoretically prevent meniscal injury. Meniscal release is controversial as it has been shown to result in an increased rate of progression of osteoarthritis (Pozzi and others 2006) and does not prevent all late meniscal injuries (Thiemann and others 2006). It is not routinely performed by the authors.















![CAN CONTRACEPTION CONTROL DEER … · A review article by Peter Green BVSc Cert EO MRCVS for the Deer Initiative 1] Introduction and history ... [Rudolph, Porter & Underwood 2000;](https://static.documents.pub/doc/80x56/5ace92357f8b9aca598b6daf/can-contraception-control-deer-review-article-by-peter-green-bvsc-cert-eo-mrcvs.jpg)


