32
BY Dr.Khaled Helmy Rhinosinusitis & Asthma Al Maamora Chest Hospital
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | roland-thorogood |
| View: | 236 times |
| Download: | 1 times |
BY Dr.Khaled Helmy
BY Dr.Khaled Helmy
Rhinosinusitis &
Asthma
Rhinosinusitis &
Asthma
Al Maamora Chest HospitalAl Maamora Chest Hospital
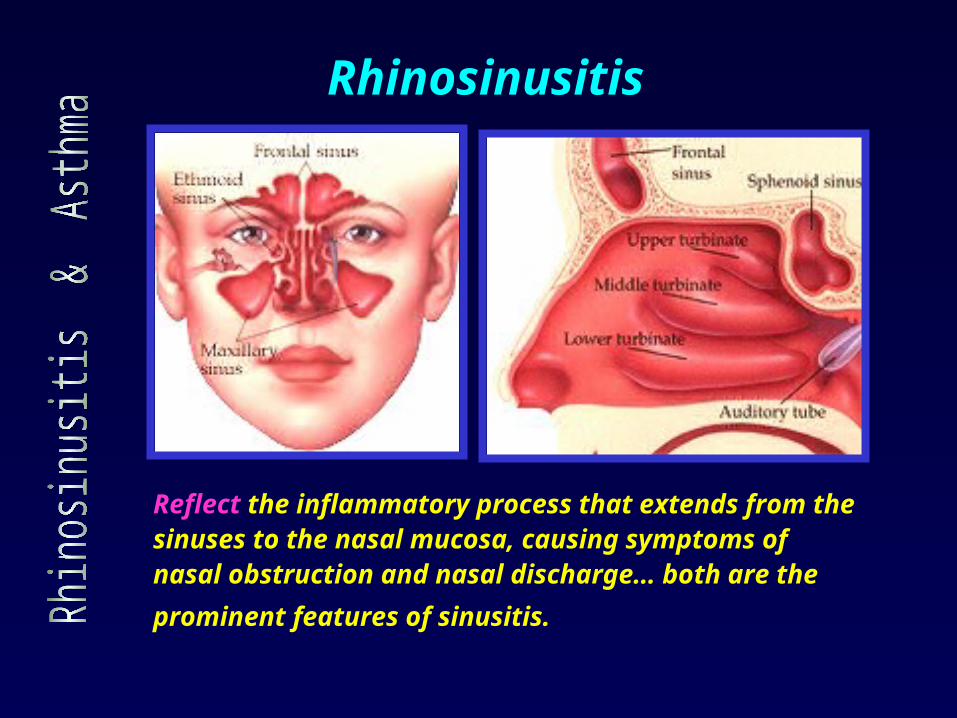
Reflect the inflammatory process that extends from the sinuses to the nasal mucosa, causing symptoms of nasal obstruction and nasal discharge… both are the
prominent features of sinusitis.
Rhinosinusitis
"The nose is the gatekeeper of the lung.“
The link between rhinitis- sinusitis
and asthma has been recognized
since the second century AD, when
Galen drew an association between
the large number of individuals who
suffered from both wheezing and
nasal discharge.
pathophysiologic, and clinical
data confirmed the strong
comorbidity.
Patients with allergic rhinitis and no clinical
evidence of asthma frequently exhibit
bronchial hyperresponsiveness to
bronchoconstrictor agents such as
methacholine or histamine.
Bronchial hyperreactivity may represent an
intermediate phase between nasal allergy and
symptomatic asthma.
Appropriate treatment of allergic rhinitis
results in improvements in asthma symptoms
and lower airway function.
"The nose is the gatekeeper of the lung.“
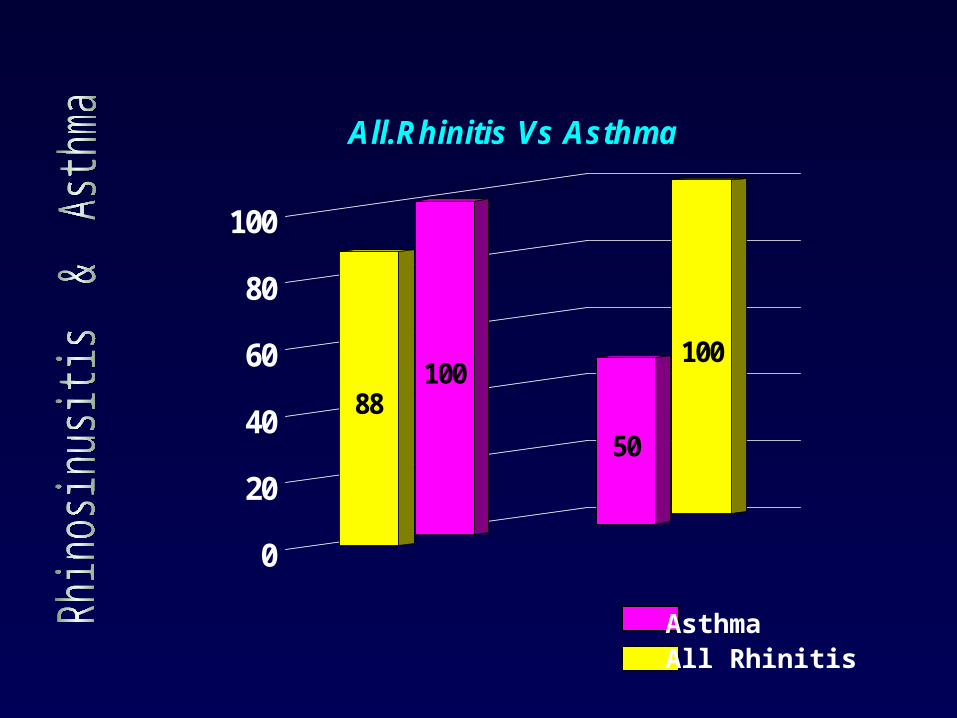
100
50
10088
0
20
40
60
80
100
All.Rhinitis Vs Asthma
AsthmaAll Rhinitis
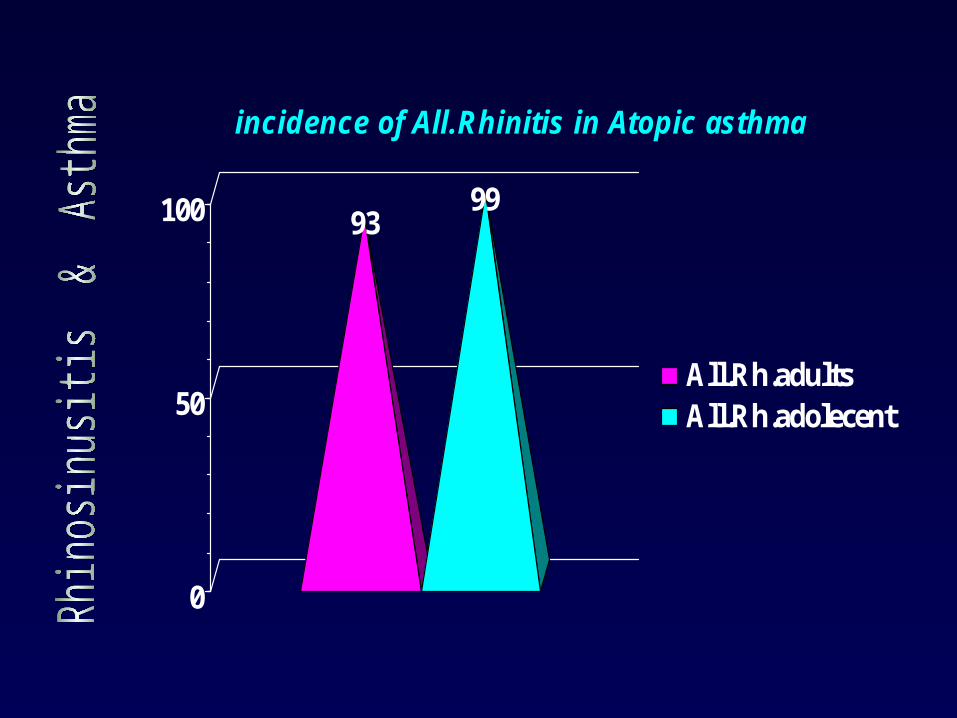
9399
0
50
100
incidence of All.Rhinitis in Atopic asthma
All.Rh.adultsAll.Rh.adolecent
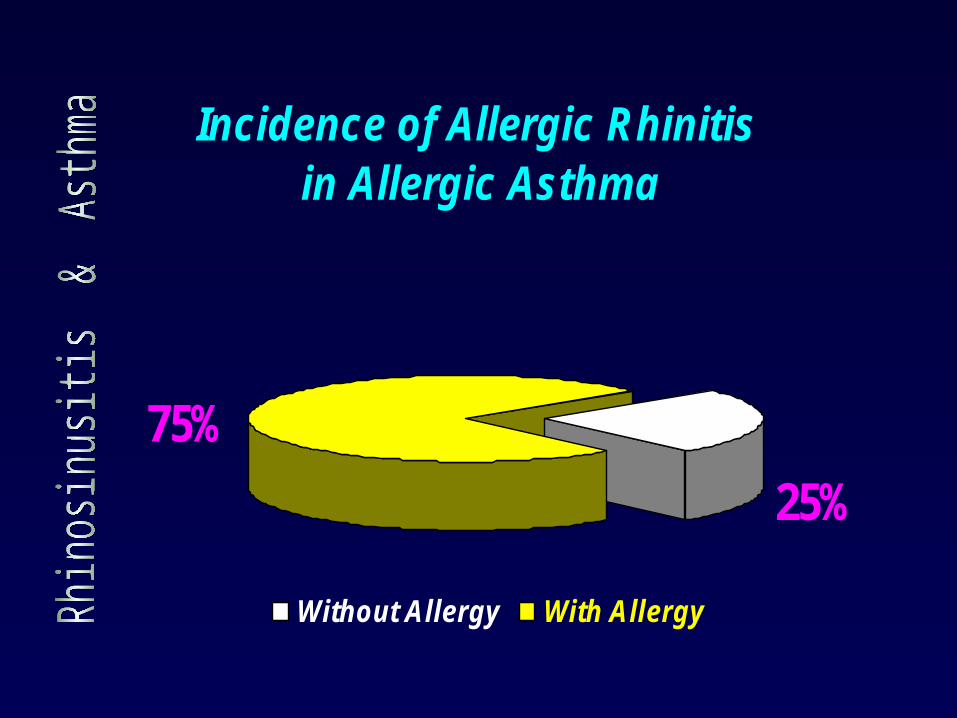
Incidence of Allergic Rhinitis in Allergic Asthma
25%
75%
Without Allergy With Allergy
1.cetirizine
1.e
What is interrelationship of Rhinosinusitis and asthma?
The Questions ??
What are the mechanisms of this interrelationship ?
What are the suggestions for optimal treatment of both?
Objectives
To identify the indicators of rhinosinusitis and asthma.
To understand the various pathophysiologic mechanisms responsible for the concomitant occurrence of rhinosinusitis and asthma.
To recognize the importance of identification and treatment of upper airway disease in management of chronic asthma .
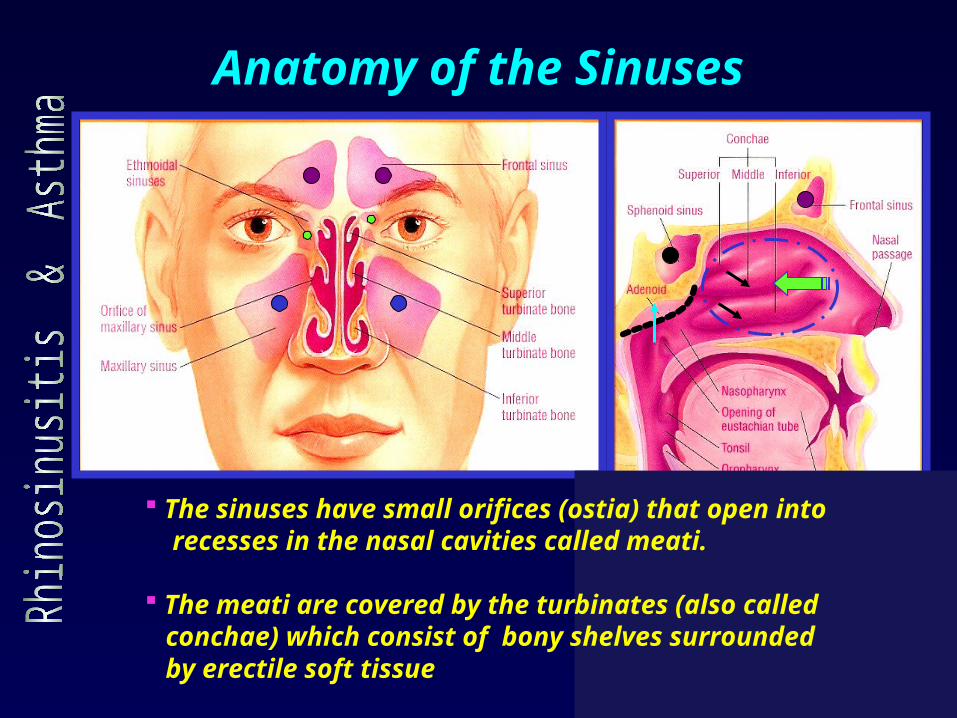
Anatomy of the Sinuses
The sinuses have small orifices (ostia) that open into recesses in the nasal cavities called meati. The meati are covered by the turbinates (also called conchae) which consist of bony shelves surrounded by erectile soft tissue
Functions of the paranasal sinuses
Air conditioning.
Pressure damping.
Reduction of skull weight.
Heat insulatio .
Flotation of skull in water.
Increasing the olfactory area.
Vocal resonance and diminution
of auditory feedback. Nitric Oxide
Nitric Oxide secretion.
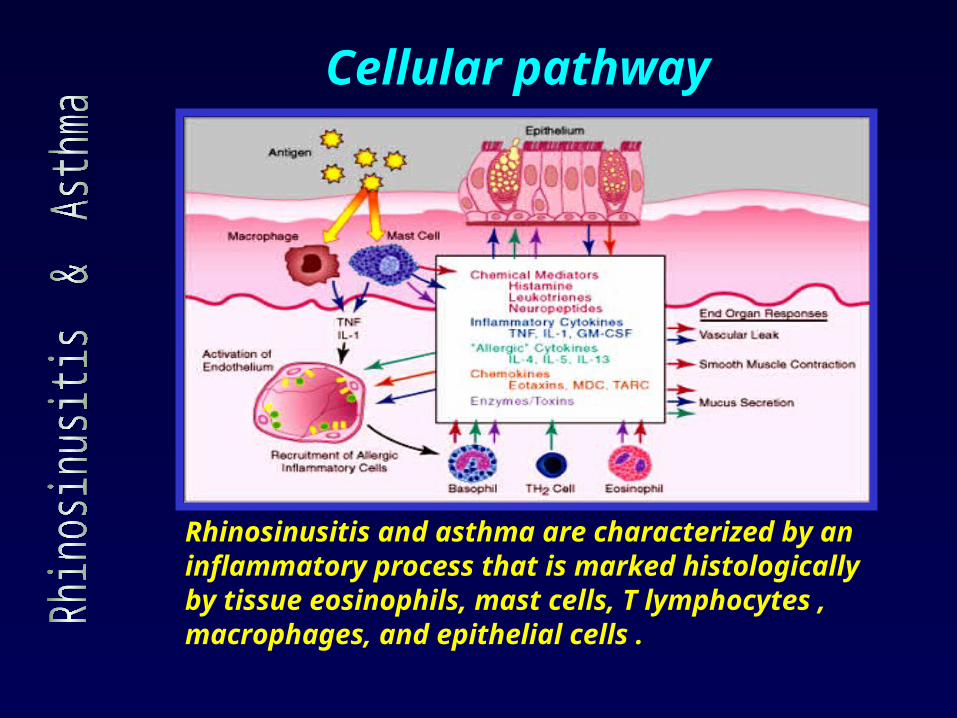
Rhinosinusitis and asthma are characterized by an inflammatory process that is marked histologicallyby tissue eosinophils, mast cells, T lymphocytes ,macrophages, and epithelial cells .
Cellular pathway
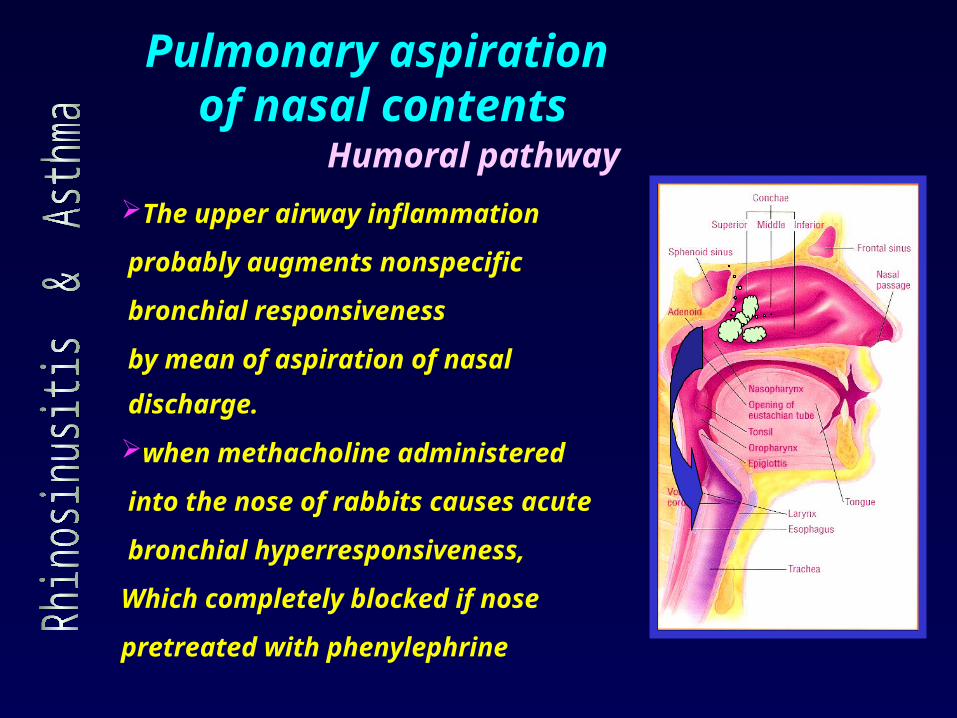
Pulmonary aspiration of nasal contents
Humoral pathway
when methacholine administered
into the nose of rabbits causes acute
bronchial hyperresponsiveness,
Which completely blocked if nose
pretreated with phenylephrine
The upper airway inflammation
probably augments nonspecific
bronchial responsiveness
by mean of aspiration of nasal
discharge.
Same airway = Same disease
Rhinitis and asthma are two manifestations of allergic respiratory disease.
Pathogenic events are triggered by exposure to aeroallergens.
The histology of these diseases shows chronic, eosinophilic inflammation .
Rhinitis and asthma represent global allergic involvement of the airways.
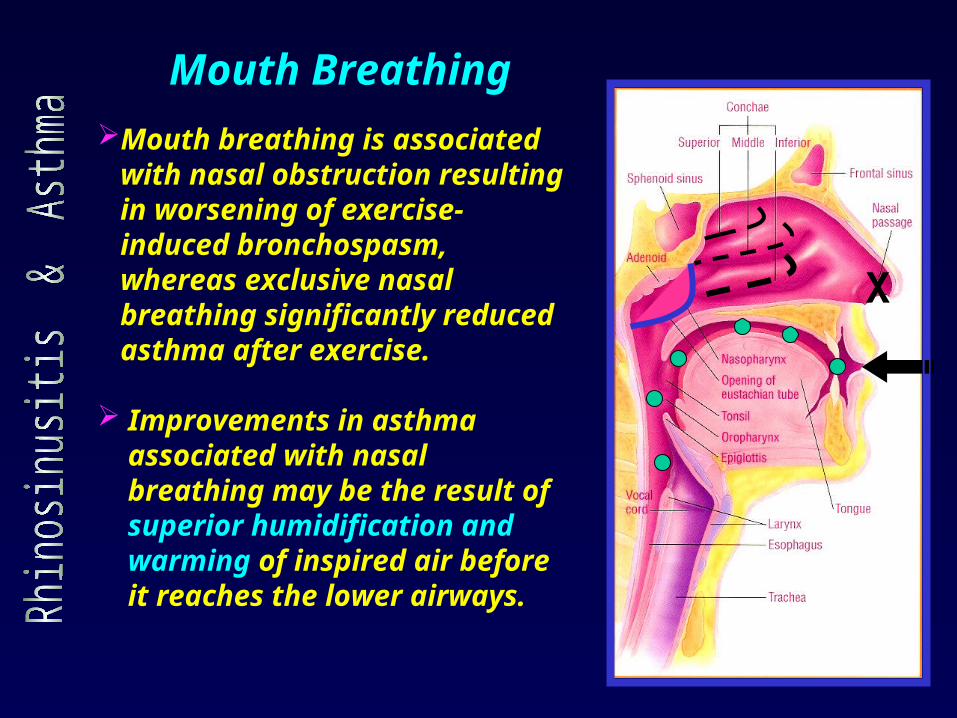
Mouth breathing is associated with nasal obstruction resulting in worsening of exercise- induced bronchospasm, whereas exclusive nasal breathing significantly reduced asthma after exercise.
Improvements in asthma associated with nasal breathing may be the result of superior humidification and warming of inspired air before it reaches the lower airways.
Mouth Breathing
X
Since the second century AD Galen was observed that purging nasal secretions offered relief to persons with pulmonary disease.
In 1919, Sluder hypothesized the existence of a sinopulmonary reflex thought to be responsible for that phenomenon.
In 1928, the French physiologist Kratchmer used noxious agents to stimulate nasal mucosa in animals, and acute bronchial hyperresponsiveness resulted.
Nasal - bronchial reflexSinopulmonary reflex
In 1969, Kaufman and Wright applied
silica particles onto the nasal mucosa
of individuals without lower airway
disease and noted significant,
immediate increases in lower airway
resistance.
This bronchospasm induced by
nasal silica was blocked by both
resection of the trigeminal nerve and
systemic administration of atropine.
Nasal - bronchial reflexSinopulmonary reflex
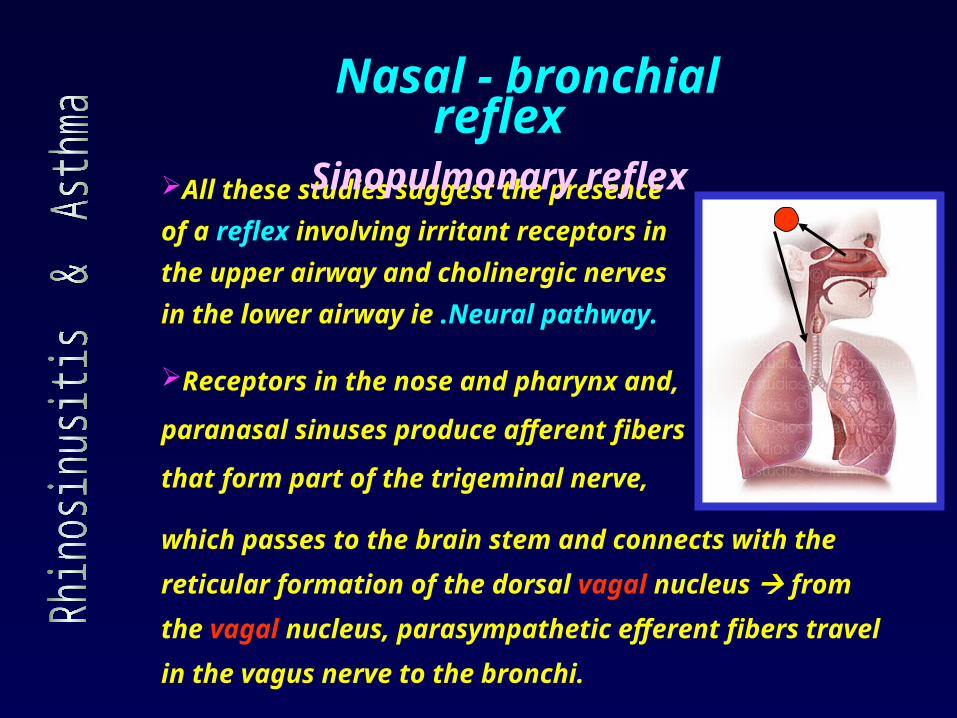
All these studies suggest the presence
of a reflex involving irritant receptors in
the upper airway and cholinergic nerves
in the lower airway ie .Neural pathway.
Nasal - bronchial reflexSinopulmonary reflex
Receptors in the nose and pharynx and,
paranasal sinuses produce afferent fibers
that form part of the trigeminal nerve,
which passes to the brain stem and connects with the
reticular formation of the dorsal vagal nucleus from the
vagal nucleus, parasympathetic efferent fibers travel in
the vagus nerve to the bronchi.
The Treatment Link
The link between rhinosinusitis and asthma ,
suggesting that when one condition is
effectively treated, the other may improve
as well.
Administering the intranasal corticosteroid
beclomethasone dipropionate to patients
with allergic rhinitis and asthma significantly
decreased bronchial hyperreactivity and
improved asthma symptoms leading to
conclude that ignoring inflammation in
the upper airway is likely to lead to
suboptimal results in asthma treatment
A reduction in nitric oxide, which is a potent
modulator of bronchial tone, may precipitate acute
bronchial hyperresponsiveness .
GERD has a role in inducing the nasal mucosal
edema and inflammation that cause obstruction of the
sinus ostia, which in turn stimulates the autonomic
nervous system. The amount of pharyngeal reflux of
gastric acid is greater in patients with chronic sinusitis
that does not respond to initial antireflux therapy.
Other associated processes
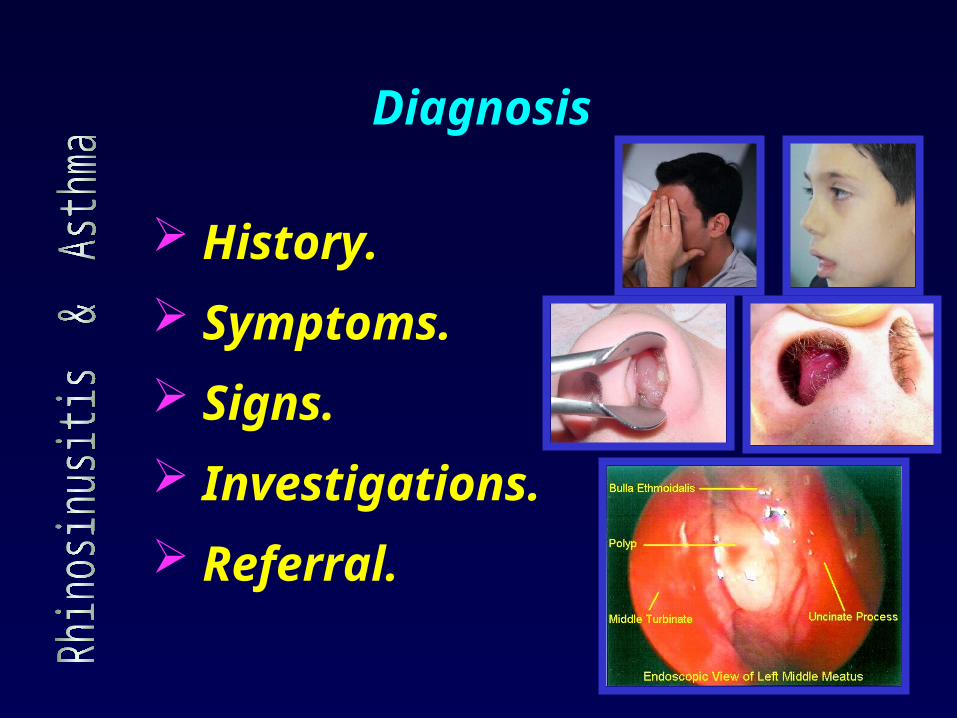
Diagnosis
History.
Symptoms.
Signs.
Investigations.
Referral.
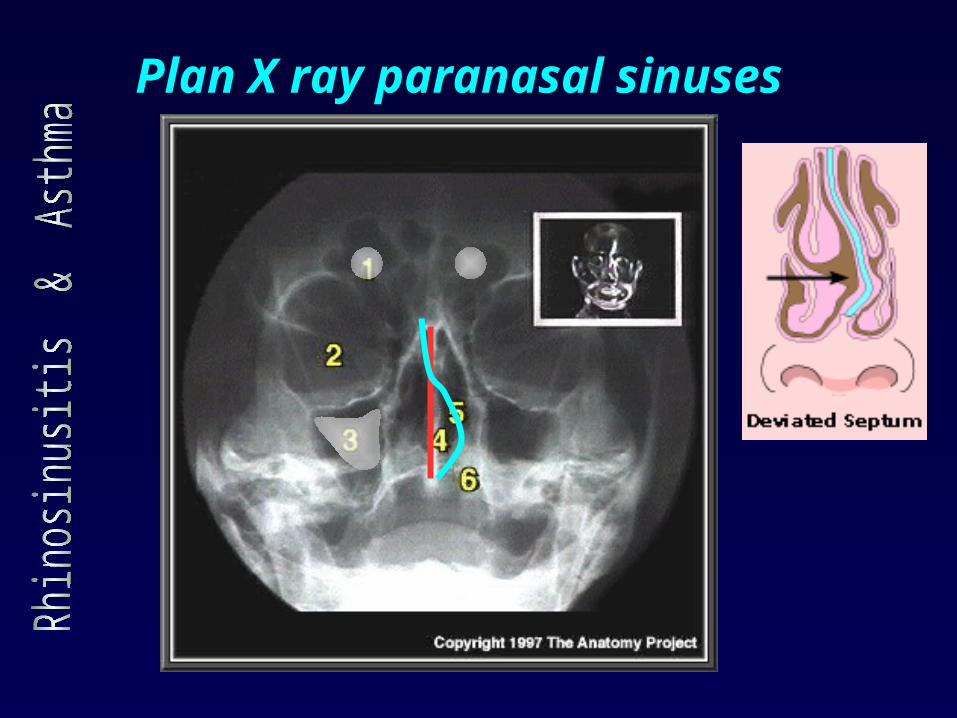
Plan X ray paranasal sinuses
Asthma diminishes when coexistent rhinosinusitis is maximally treated by medical or surgical intervention.
Medical treatment include…. antihistamines ,topical intranasal corticosteroids , decongestants, sinopulmonary lavage and broad-spectrum antibiotic therapy (when indicated).
The role of medication in treatment is to reduce chronic inflammation associated with asthma and coexisting nose& paranasal sinus disease.
Treatment strategies
Antihistamines effectively block H1 receptors
and function as anti-inflammatory agents.
Decongestants can significantly affect ostial
blockage .
Topical intranasal corticosteroids has a
profound effect on reducing tissue edema and
inflammation in the sinuses.
Antibiotic should be used only ifthere is
infection.
Medical Treatment
Functional endoscopic sinus surgery (FESS)
FESS on 125 rhinosinusitis –asthmatic patients monitored for an average of 6.5years after FESS was performed.
About 90% of patients improved asthma symptoms.
Benefit was demonstrated by
* Less frequent use of a beta-agonist inhaler in 50% of patients.
* Fewer need of oral corticosteroid to control acute asthma exacerbations in 66% of patients.
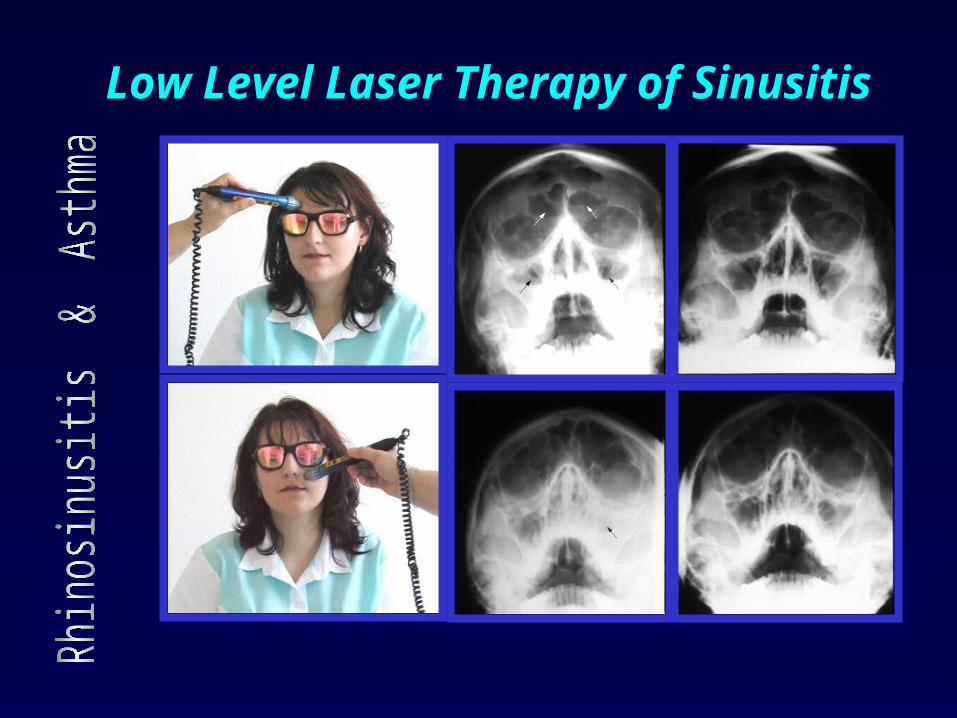
Low Level Laser Therapy of Sinusitis
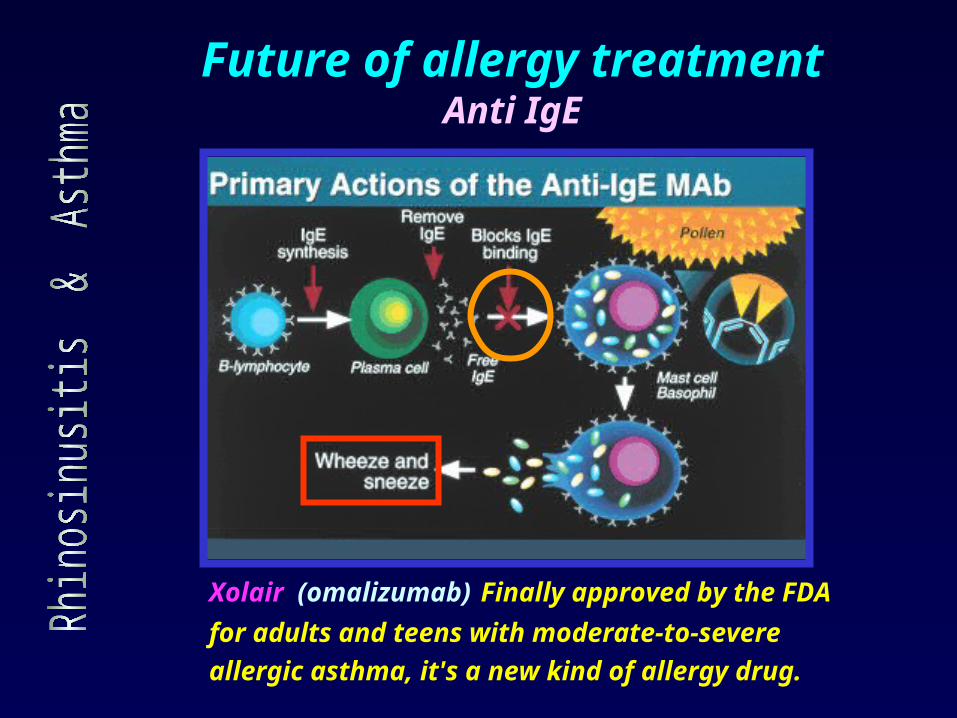
Future of allergy treatmentAnti IgE
Xolair (omalizumab) Finally approved by the FDA
for adults and teens with moderate-to-severe
allergic asthma, it's a new kind of allergy drug.
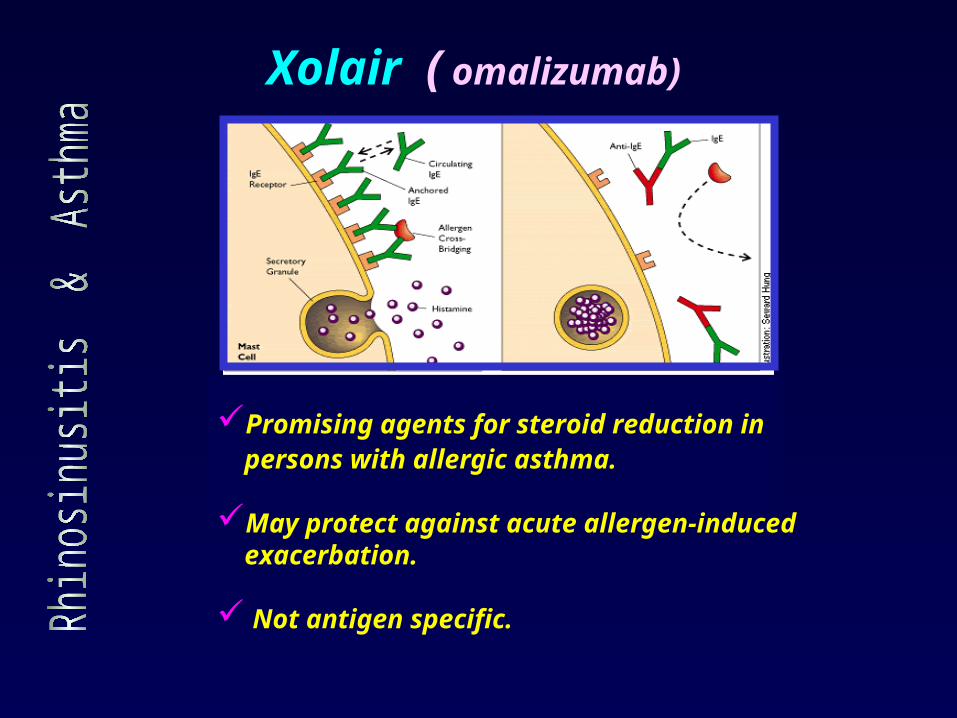
Promising agents for steroid reduction in persons with allergic asthma.
May protect against acute allergen-induced exacerbation.
Not antigen specific.
Xolair ( omalizumab)
May have uses in other allergic diseases.
Not every case of asthma is triggered by an
allergic reaction.. Exercise, cold outdoor
temperatures and other factors may be the
seminal event in susceptible individuals. While
those cases, too, are characterized by
inflammation and narrowing of the airways.
Tanox is developing a similar drug, known as
TNX-901.
Xolair ( omalizumab)
Considerable clinical and research evidence substantiates the interrelationship between
rhinosinusitis and asthma.
Optimal treatment of asthma depends on aggressive management of associated rhinosinusitis.
Rhinosinusitis is best managed by the use of antihistamines, intranasal corticosteroids, decongestants, sinus lavage to maintain adequate mucociliary clearance
Antibiotics should be used only if needed.
Anti IgE is a promising treatment for allergic diseases.
Conclusions

Given by injection once or twice a
month, it lets many patients cut
back on other asthma drugs.
A genetically engineered
antibody(Anti IgE) that blocks the
cascade of events in the body that
triggers allergic asthma .

















