56
C4d POSITIVITY IN RENAL REJECTION Dr.Imrana Tanvir
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | imrana-tanvir |
| View: | 362 times |
| Download: | 0 times |
C4d POSITIVITY IN RENAL REJECTION
Dr.Imrana Tanvir
OBJECTIVES
• Introduction of Antibody mediated rejection AMR
• Classification of AMR
• Role of C4d in transplant rejection
• Pros and Cons of C4d marker
• Donor specific antibodies DSA
• Conclusion

Transplant rejection
Cell mediated
(interstitial)
Antibody mediated
(humoral)
Hyperacute
Acute HumoralRejection
Chronic HumoralRejection
Preformed DSA
Preformed/denovo DSA
CHRONIC ALLOGRAFT REJECTION IS DUE TO MANY CAUSES INCLUDING CHRONIC HUMORAL REJECTION
Is one of the causes of chronic allograft rejection
Histological criteria of presumptive diagnosis of AMR
• endothelial injury with swelling
• Acute glomerulitis
• Peri-tubular capillary margination and dilatation
• Fibrin thrombi in vessels/Fibrinoid necrosis
• Interstitial edema/haemmorhage
In minority of cases-Acute tubular necrosis only
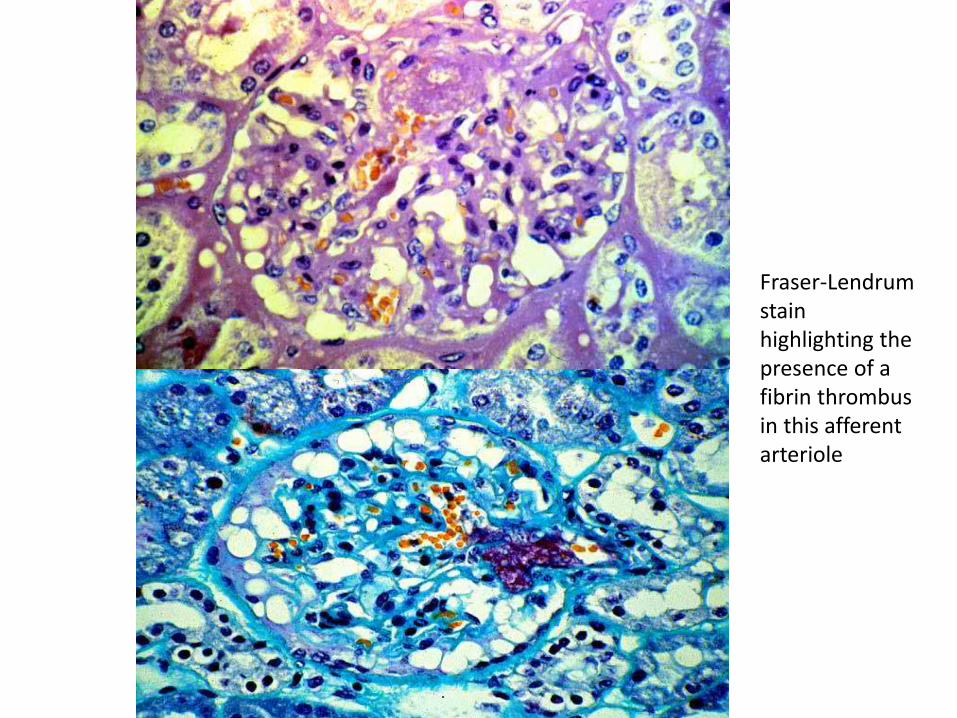
Fraser-Lendrumstain highlighting the presence of a fibrin thrombus in this afferent arteriole

1.Trpkov K, Campbell P, Pazderka F, Cockfield S, Solez K, Halloran PF. Pathologic features of acute renal allograft rejection associated with donor-specific antibody: Analysis using
the Banff grading schema. Transplantation 1996;61(11):1586-92
Fibrinoid necrosis of the glomeruli, focal interstitial hemorrhage and neutrophilic margination

1.Trpkov K, Campbell P, Pazderka F, Cockfield S, Solez K, Halloran PF. Pathologic features of acute renal allograft rejection associated with donor-specific antibody: Analysis using the Banff grading schema. Transplantation 1996;61(11):1586-92
Fibrin thrombus
www.pathologyoutlines.com
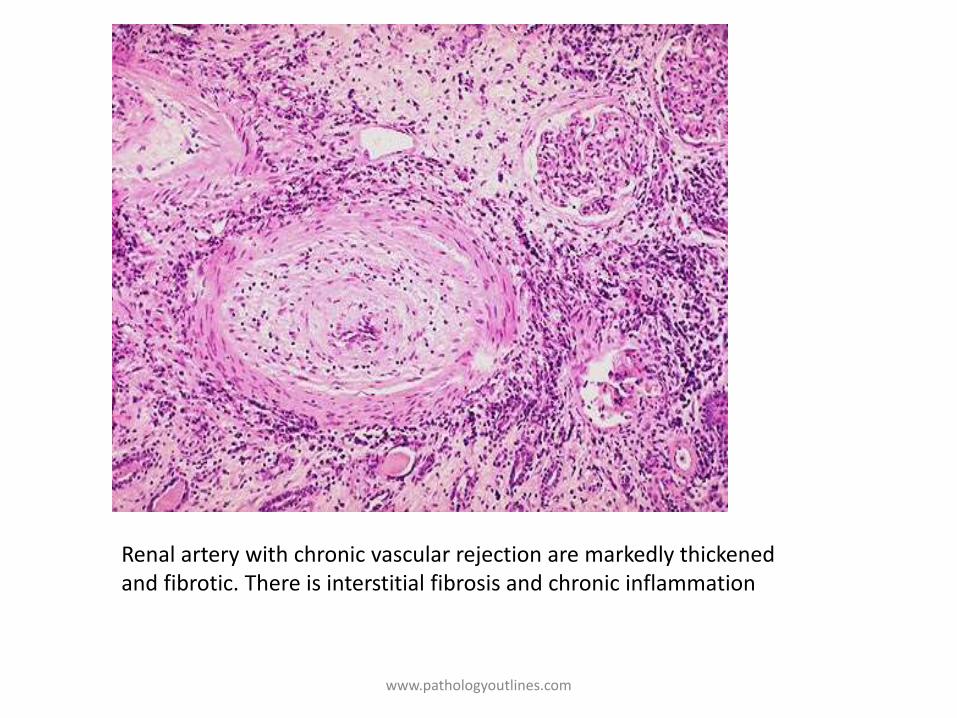
Renal artery with chronic vascular rejection are markedly thickened and fibrotic. There is interstitial fibrosis and chronic inflammation
UPMS-TRANSPLANT PATHOLOGY INTERNET SERVICES
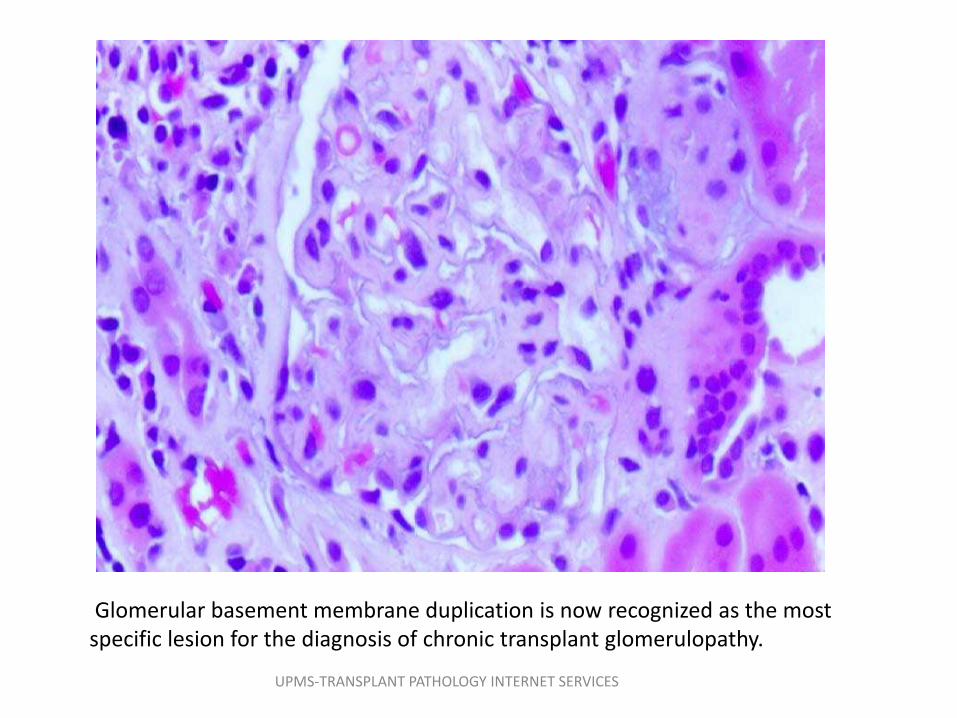
Glomerular basement membrane duplication is now recognized as the most specific lesion for the diagnosis of chronic transplant glomerulopathy.

Cohen, R. B. Colvin, M. R. Daha et al., “Pros and cons for C4d as a biomarker,” Kidney International, vol. 81, no. 7, pp. 628–639, 2012
CLASS I Presence of acute tubular necrosis (ATN) only, with minimal inflammation
CLASS II glomerulitis, peritubular capillaritis, and microthrombosis
CLASS III Arteritis
HISTOLOGICAL EVIDENCE
DONOR SPECIFIC
ANTIBODIES (DSA)
BANFF
2003
C4d STAINING

Introduction to C4d

Complement system

• C4d has a thioester moiety that enables strong covalent bonding with the endothelial cells and basement membrane.
• C4d has been called 'a footprint' of antibody-mediated tissue injury
C4d

Expression of C4d
• C4d is normally expressed in the mesangium and the vascular pole.
• It also involves glomerular capillaries in cases of immune-mediated glomerulopathies .
• In transplant kidney (AMR) peritubular C4d may be noted.
• There have been rare reports of C4d presence in PTC of donor kidneys
Chethan Puttarajappa, Ron Shapiro and Henkie P. Tan . Antibody-Mediated Rejection in Kidney Transplantation: A Review

Methods of detection
1.Immunofluorescence (IF) on frozen tissue (monovalent antibody against C4d )
2. Immunohistochemistry (IHC) on paraffin-embedded tissue (polyvalent antibody).
– Diffuse C4d implies >50% of PTC staining for C4d
– Focal staining implies 10–50%
– Minimal staining implies <10%
Note:IHC is less sensitive than IF for C4d detection.
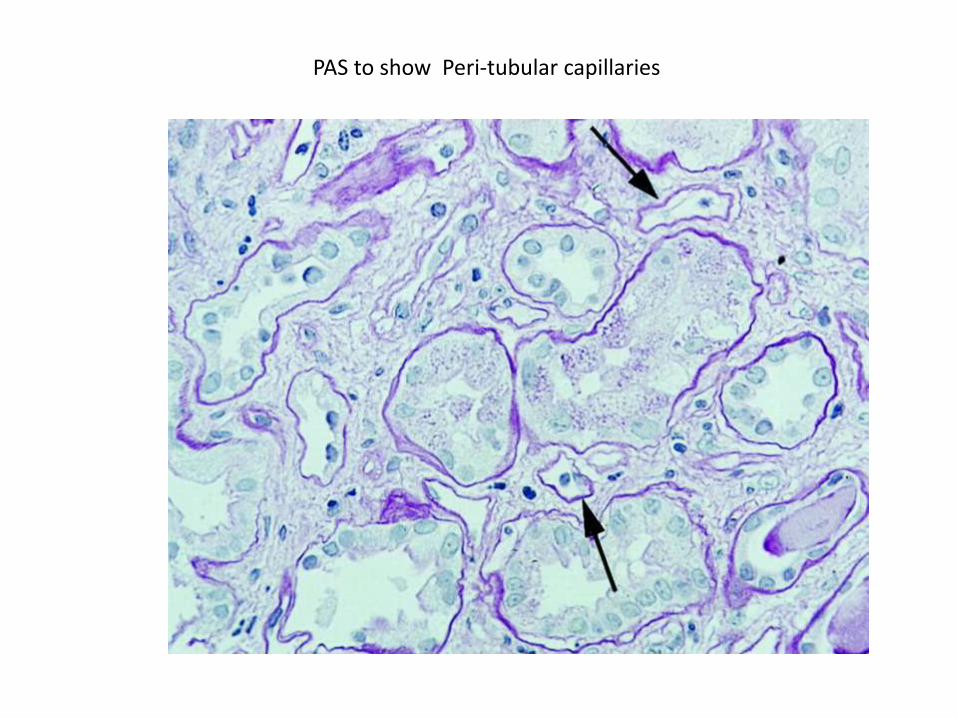
PAS to show Peri-tubular capillaries

IF showing C4d staining in peri-tubular capillaries (AMR)

IHC-C4d in Peritubular capillaries (tubular membranes are unstained)in AMR

Strong , linear staining along entire circumference of PTCs

C4d
• Feucht et al- C4d in PTCs
Associated with poor graft survival
• Collin et al- close correlation of PTC C4d staining with
– concurrent circulating DSA
– Neutrophils in cappilaries(peritubular,gloomerular)
– Vascular arterial fibrinoid necrosis

C4d positive AMR
• Feucht et al. - 1991
Significant association of C4d with preformed anti HLA antibodies in patients with acute rejection .
Confirmed in a study of 16 biopsies with DSA and histopathological evidence of AMR (neutrophiliccapillaritis).
Diffuse C4d-staining with trace or no staining in the biopsies with acute cellular rejection and 5 of the 6 biopsies with cyclosporine toxicity.

• Crespo et al.
evaluated DSA and C4d in steroid-resistant rejections and found positive DSA in 37% of the cases. Among these, 95% had positive PTC C4d-staining.
Association with Chronic AMR
• Mauiyyedi et al. reported presence of C4d in 23 of 38 biopsies with features of chronic AMR but no C4d in the control group without features of chronic AMR .
• However, some studies found no correlation between presence of TG and diffuse C4d, with many TG patients showing no C4d positivity .
TG(transplant glomerulopathy)
• In 2007, a retrospective study of biopsies from 1320 transplanted patients showed that more than 40% of cases with transplant glomerulopathy—were C4d negative, despite the fact that anti-HLA antibodies were detected in 73% of patients*
33.Sis B, Campbell PM, Mueller T et al. Transplant glomerulopathy, late antibody-mediated rejection and the ABCD tetrad in kidney allograft biopsies for cause. Am J
Transplant 2007; 7: 1743–1752
C4d negative AMR
• In chronic AMR
• as common, if not more than the C4d-positive AMR and has similar poor prognosis in terms of graft survival
• Loupy et al. [38,39] showed that C4d or capillaritis in 3-month protocol biopsies were risk factors for later transplant glomerulopathy, and capillaritis was predictive even in the absence of C4d*
Loupy et al. [38,39] showed that C4d or capillaritis in 3-month protocol biopsies were risk factors for later transplant glomerulopathy, and
capillaritis was predictive even in the absence of C4d
• Haas &Mirocha,who investigated patients with DSAs who had a biopsy during the first 3 months after transplantation. Patients with a C4d-negative biopsy who were not treated for AMR had a higher rate of progression to transplant glomerulopathy than those who were treated for AMR post-biopsy
.Haas M, Mirocha J. Early ultrastructural changes in renal allografts: correlation with antibody-mediated rejection and transplant glomerulopathy. Am J Transplant 2011.
• complement independent• Experimental studies“allo-antibodies themselves can alter the state of the endothelium in the absence of complement or other inflammatory cells”
• Endothelial transcripts combined with DSA show excellent sensitivities for AMR (although less specificity than C4d)

• Variability of staining over time suggesting a constant flux between states of positive to negative C4d .
• In a significant number of these biopsies, there was presence of microvascularinflammation (PTC and glomerular capillaritis) in spite of negative C4d-staining .*
. Loupy, G. S. Hill, C. Suberbielle et al., “Significance of C4d Banff scores in early protocol biopsies of kidney transplant recipients with preformed donor-specific antibodies (DSA),” The American Journal of Transplantation, vol. 11, no. 1, pp. 56–65, 2011.
Results
cases
• Biopsies-132
• Acute rejection-59
• ATN-10
• CAN-41
• Normal-18
• BK nephropathy-4 (morphology)
• Miscellaneous-8
C4d staining•Overall prevelance 45%•P-AbAR-81%•ACR-20%•CAN-30%

ADVANTAGES OF C4D
• C4d is now one of the core diagnostic tools to identify AMR
• ‘A magic marker‘:because of its stability, its strong association with antibody-mediated rejection (AMR), and finally, its major impact on graft survival and patient treatment*

• Emergence of new therapeutics that block complement activation makes C4d a marker with potential to identify patients who may possibly benefit from these drugs
LIMITATIONS OF C4D

1. In ABO-incompatible transplantations ,C4d is present in the majority of grafts but this seems to point at 'graft accommodation' rather than antibody-mediated rejection*
2. Potential biomarker in other fields where antibodies can cause tissue damage, such as systemic autoimmune diseases
C4d deposition in native kidneys, mainly in the setting of autoimmunity

C4d positivity along the glomerular basement membrane
Hui M, Uppin MS, Prayaga AK, Raju SB, Rajasekhar L. C4d immunohistochemistry in membranous nephropathy. J Lab Physicians [serial online] 2014 [cited 2014 Nov 12];6:76-9
Granular peritubularcapillary PTC staining has been rarely described in lupus nephritis
• C4d staining was investigated in many forms of glomerulonephritiswhere peritubularcapillary C4d staining was virtually never observed*
• Glomerular C4d deposition on the other hand is a relatively common finding
*Chen M, Daha MR, Kallenberg CG. The complement system in systemic autoimmune disease. J Autoimmun 2010; 34: J276–J286.*Cohen D, Koopmans M, Kremer Hovinga I et al. Potential for glomerular C4d as an indicator of thrombotic microangiopathy in lupus
nephritis. Arthritis Rheum 2008; 58: 2460–2469.*Kusunoki Y, Itami N, Tochimaru H et al. Glomerular deposition of C4 cleavage fragment (C4d) and C4-binding protein in idiopathic
membranous glomerulonephritis. Nephron 1989; 51: 17–19..*Xing GQ, Chen M, Liu G et al. Differential deposition of C4d and MBL in glomeruli of patients with ANCA-negative pauci-immune
crescentic glomerulonephritis. J Clin Immunol 2010; 30: 144–156
DEVELOPMENTS
Certain endothelial transcripts EDNAT appear to be expressed more often in patients with histological features of AMR even in the absence of C4d-staining.
Sis et al. (ENDAT) in kidney transplants
• ENDAT expression was higher in all types of rejection but more so in AMR.
• 40% of patients with ENDAT and chronic AMR features demonstrated no C4d-staining.
• strong correlation between elevated ENDAT and presence of anti-HLA antibodies, particularly HLA Class II antibodies
• Biology: endothelial cell activation, repair, and angiogenesis which are well known mechanisms of AMR .

• it is not inconceivable that this or a simpler derivative method will partly or fully replace C4d in future

DONOR SPECIFIC ANTIBODIES
DSA
DSA
• Anti-HLA antibodies generated against donor cells
• Positivity for DSA before transplantation is a contraindication
HISTORY
• P.A.Gorer 1938- first to introduce role of antibodies in transplantation
• Terasaki & Ozawa 2004-monitor DSA as predictor of transplantation outcome.
(DSA presence indicated higher risk for AMR ,both acute and chronic)

DETECTION OF DSA
• CDC :complement dependent cytotoxicity test
Golden standard to detect the presence of non HLA molecules that could be target for anti-HLA antibodies.
Based on complement fixation,Specific IgG not fixing complement-false negatives
Solid phase assays
• ELISA – detect complement and non complement fixing antibodies
• Pei et all 1998-microbeads coated with purified HLA antigens,detected by flow cytometry
• Luminex assay-HLA attached to bead-most applied
• Extremely sensitive,no accepted standard cutoff value
• False negatives-IgM antibodies mask

Acute Humoral Rejection
• DSA (donor specific antibodies)
– PRA levels (panel reactive antibody)
– Flow cytometry cross match
– Flow PRA bead assays
Do not correlate with morphological as well as immunopathological evidence

False negatives
• IgM antibodies mask
• Prozone phenomenum-C1 cometitivelydisplaces antibodies
Clinical evidence
• 1/3rd patients are sensitized
• Antibody mediated rejection
• Monitoring of DSA to predict allograft outcome-non invasive surrogate method compared to graft biopsy
• Not only correlation of pre transplantation but also post transplantation DSA
Desensitization approaches
1. Remove circulating DSA by plasmapheresis
2. Block their effect with proteasome inhibitors
3. Reduce production with anti-CD20
• Significant survival benefit
• Considered a risk factor more than a contraindication
• Methodology to detect and therapy to remove is evolving

ALTERNATIVES TO C4D

• •Alternatives for C4d are emerging (genomics, molecular diagnostics, and endothelial transcripts) and if proven useful, effort will be made to transform these techniques or their progeny to practical tests

REFERENCES
1. Chethan Puttarajappa, Ron Shapiro and Henkie P. Tan . Antibody-Mediated Rejection in Kidney Transplantation: A Review
2. Danielle Cohen, Robert B Colvin, Mohamed R Daha, Cinthia B Drachenberg, Mark Haas, Volker Nickeleit, Jane E Salmon, Banu Sis, Ming-Hui Zhao, Jan A Bruijn, Ingeborg M Bajema .Pros and Cons for C4d as a Biomarker. Kidney Int. 2012;81(7):628-639

REFERENCES
• V. Pietroni, A. Toscano, F. Citterio. Donor-Specific Antibody in Solid Organ Transplantation: Where are We?

Queries???

















