126
ONCOLOGY BOARD REVIEW Calvin Thigpen, M.D. July 18, 2014
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | horace-booth |
| View: | 215 times |
| Download: | 0 times |

ONCOLOGY BOARD REVIEW
Calvin Thigpen, M.D.
July 18, 2014
If you could only…
Study 5 things in oncology, they should be:
1. Breast Cancer
2. Lung Cancer
3. Colon Cancer
4. Prostate Cancer
5. Complications (of these diseases and their therapy)

As you study…
Pay close attention to:1. Interventions that lead to a cure
2. Emergent situations
3. Inherited conditions
4. Atypical approaches to cancer care
These are the kinds of things practicing general internists need to know.
Breast Cancer
It will DEFINITELY be on the exam.

What they will ask Risk factors Locoregional disease therapy Hormone/endocrine therapy
Indications Side effects
Recurrent disease

What they won’t ask
Exactly when to start, or how often to get, mammograms
Specific combinations of chemotherapy
Look for this in the stem Age and family history Menopausal status Exposure to estrogen Hormone receptor status Previous cancer therapy Site of metastasis Drugs

We Are YoungA nulliparous 29-year-old Ashkenazi Jewish woman has a palpable left breast mass present for 6 months. Her mother was adopted; her father is 72 years old and has a history of prostate cancer. Her paternal aunt was diagnosed with ovarian cancer at age 48 years. Another paternal aunt was diagnosed with breast cancer at age 49 years. Her paternal grandmother died of complications from breast cancer at age 60 years.
On exam, there is a 4-cm mass in the left breast affixed to the chest wall and a 1-cm, freely movable left axillary lymph node. Biopsy reveals moderately differentiated ER+, PR+, H2N- invasive ductal carcinoma. CT and bone scan show no metastatic disease. She will receive preoperative chemotherapy followed by surgery.
Which of the following will be most helpful in determining the best surgical approach?
A. Counseling and genetic testing
B. Genomic profile assay
C. PET scan
D. Tumor marker testing

Key Point
For women who have breast cancer and are at high risk for BRCA1 or
BRCA2 mutations, genetic testing and counseling may inform surgical
options.
BRCA1 and BRCA2 risk 2 1st degree relatives with
breast cancer (one at <50 years of age)
3 or more 1st or 2nd degree relatives with breast cancer regardless of age;
Both breast and ovarian cancer among 1st and 2nd degree relatives;
1st degree relative with
bilateral breast cancer; 2 or more 1st or 2nd degree
relatives with ovarian cancer regardless of age;
1st or 2nd degree relative with both breast and ovarian cancer at any age; or
Breast cancer in a male relative.

Why genetic testing? The history suggests genetic cancer Test results either:
Establish the diagnosis Influence the management of family
members at risk
Test those already with cancer if at all possible

I Can’t Go For ThatA 65-year-old woman is evaluated for a 2-cm right breast mass discovered on routine mammography.
Vital signs and physical exam are unremarkable, and there is no palpable breast mass or lymphadenopathy.
Ultrasound-guided needle biopsy reveals a well-differentiated, ER+, PR+, H2N- invasive ductal carcinoma.
Which of the following is the most appropriate next step in management?
A. Right breast lumpectomy
B. Right breast lumpectomy, sentinel lymph node biopsy, and radiation
C. Right breast mastectomy
D. Right breast mastectomy, sentinel lymph node biopsy, and radiation

Key Point
Breast conservation therapy, which consists of excision of the primary
tumor and radiation therapy, is equivalent to mastectomy in long-term
survival.

Primary therapy All breast cancer patients need surgery
at some point. Breast-conserving therapy is
equivalent to mastectomy. Sentinel lymph node biopsy:
For clinically lymph node negative disease Fewer side effects (far less lymphedema)
Adjuvant radiation reduces local recurrence.

Endocrine therapy ER+/PR+
Premenopausal Tamoxifen for 5 years If tumor large, chemotherapy + Tamoxifen
Postmenopausal Aromatase inhibitor (anastrazole, letrozole,
exemestane) for 5 years +/- Tamoxifen for 5 years prior to AI If tumor large, chemotherapy + AI
H2N+ One year of Trastuzumab
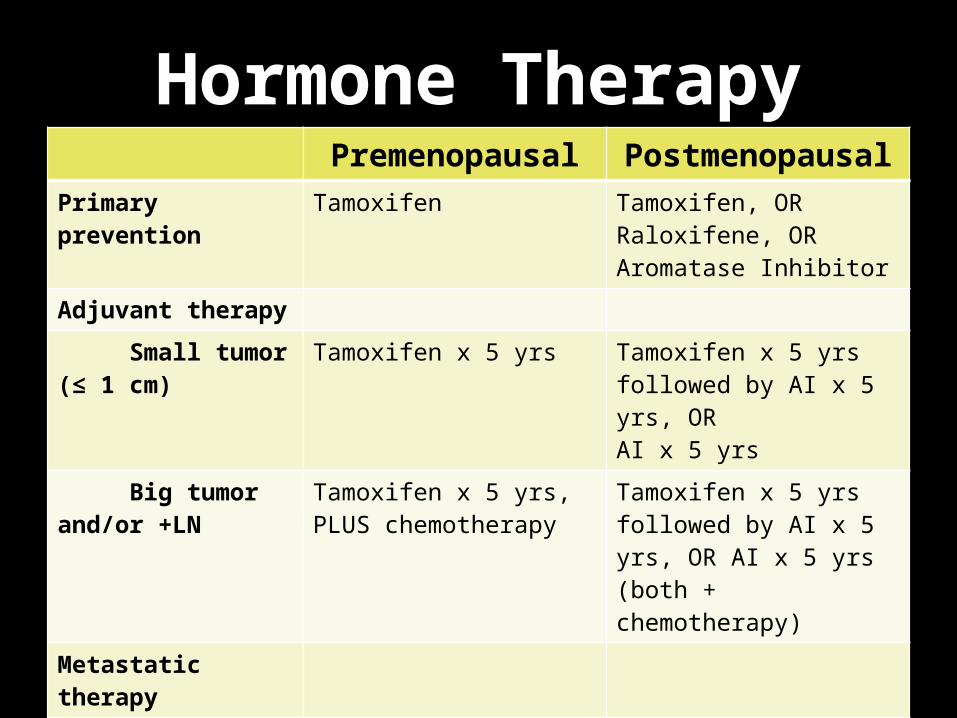
Hormone TherapyPremenopausal Postmenopausal
Primary prevention Tamoxifen Tamoxifen, OR Raloxifene, OR Aromatase Inhibitor
Adjuvant therapy
Small tumor (≤ 1 cm)
Tamoxifen x 5 yrs Tamoxifen x 5 yrs followed by AI x 5 yrs, ORAI x 5 yrs
Big tumor and/or +LN
Tamoxifen x 5 yrs, PLUS chemotherapy
Tamoxifen x 5 yrs followed by AI x 5 yrs, OR AI x 5 yrs(both + chemotherapy)
Metastatic therapy
Non-visceral disease
Tamoxifen +/- chemotherapy
AI +/- chemotherapy
Visceral disease Tamoxifen + chemotherapy
AI + chemotherapy

Systemic therapy
For those with the two most important prognostic factors:
Positive lymph nodesLarger tumors (>1 cm)

Metastatic therapy Endocrine therapy + chemotherapy
Endocrine therapy Premenopausal – Tamoxifen Postmenopausal – Aromatase inhibitor
Chemotherapy Sequential single agents equivalent to combination Anthracyclines, Taxanes, Methotrexate, Cytoxan, 5-FU
H2N Trastuzumab In combination with chemotherapy or not
Zoledronic acid or denosumab for bony disease

She’s Always a WomanA 45-year-old woman undergoes evaluation after a recent diagnosis of stage II ER+, PR+, H2N- breast cancer. She is premenopausal. She was treated with modified radical mastectomy and just completed adjuvant chemotherapy. She had a DVT associated with oral contraceptive pill use 20 years ago. She is a nonsmoker and is very physically active.
Physical exam and labs are unremarkable.
Which of the following is the most appropriate next step in management?
A. Adjuvant aromatase inhibitor therapy
B. Adjuvant trastuzumab therapy
C. Baseline imaging with whole-body CT scan or PET scan
D. Ovarian ablation
Key Point
Tamoxifen can increase the risk for thromboembolic complications.

Hello AgainA 60-year-old woman is evaluated for 6 weeks of worsening left hip and right arm pain. She had stage III ER+, PR+, HER2- breast cancer diagnosed 5 years ago and treated with modified radical mastectomy, chemotherapy, and radiation. She declined adjuvant hormonal therapy.
Physical exam reveals tenderness over the left sacroiliac joint and the right humerus.
Bone scan shows uptake in the bilateral femurs, lumbar spine, and right humerus consistent with metastases. CT shows no abnormalities in the lungs or liver, but bony lesions are evident and are consistent with the bone scan findings. No pathologic fractures are present.
Which of the following is the most appropriate intervention?
A. Aromatase inhibitor
B. Bone biopsy
C. Chemotherapy
D. Radiation therapy
E. Trastuzumab therapy

Key Point
A lesion due to a first recurrence of breast cancer should be biopsied to confirm malignancy and hormone
receptor and HER2 status, which then guides treatment.

Tamoxifen Originally, the only FDA approved drug for
primary breast cancer prevention (5 years) Used in adjuvant treatment for ER+ tumors
to reduce the risk of recurrence (5 years) Used in treatment of ER+ metastatic breast
cancer Side effects:
Thromboembolism Endometrial cancer Serotonin syndrome (when given with SSRIs)

Aromatase inhibitors Anastrazole, letrozole, exemestane Adjuvant therapy for postmenopausal
women with ER+ tumors to prevent recurrence
Therapy for postmenopausal women with metastatic ER+ tumors
Side effects: Hot flashes Arthralgias Osteoporosis

Anthracyclines Doxorubicin, epirubicin,
daunorubicin Reduce dose for hepatic
dysfunction Cardiac toxicity
Determined by cumulative dose of drugCardiomyopathy largely irreversible,
difficult to treat
Trastuzumab (Herceptin) For women with Her-2-neu + tumors To be given for 52 weeks as adjuvant therapy
Reduces recurrence by 50% Reduces mortality by up to 30%
Given in metastatic disease MAJOR side effect – can induce heart failure
Especially when given with an anthracycline (so don’t do it)
Monitor LV EF before, during, and after treatment

I Gotta FeelingA 45-year-old woman is evaluated for severe hot flushes that significantly limit her quality of life as well as vaginal dryness that is controlled with local lubricants. She had stage II ER+, PR+, HER2- invasive breast cancer diagnosed 1 year ago and treated with lumpectomy, chemotherapy, and radiation therapy. She has not had a menstrual cycle since her 4th cycle of chemotherapy. She began taking tamoxifen 3 months ago after completing radiation therapy. Nonpharmacologic interventions for hot flushes have brought no improvement.
Physical exam is normal other than evidence of surgery on the left breast and radiation changes on her skin.
Which of the following is the most appropriate therapy for this patient?
A. Fluoxetine
B. Low-dose estrogen-progesterone
C. Red clover
D. Venlafaxine

Key Point
Selective serotonin reuptake inhibitors that are potent CYP2D6 inhibitors
(such as fluoxetine and paroxetine) should be avoided in patients with menopausal symptoms caused by
tamoxifen.
50 Ways to Say GoodbyeA 65-year-old woman is evaluated during a routine examination. She is asymptomatic. She had stage I ER-, PR-, HER2- breast cancer diagnosed 3 years ago treated with modified radical mastectomy followed by chemotherapy with docetaxel and cyclophosphamide.On physical exam, the left chest wall is well healed with no nodularity. No right breast masses, axillary lymphadenopathy, or supraclavicular lymphadenopathy are present. The patient will undergo periodic mammography and routine health maintenance.
Which of the following would be the most appropriate additional evaluation in this patient?A. Bone scan yearlyB. CT scan yearlyC. PET scan yearlyD. Tumor marker measurement, complete blood count, and comprehensive metabolic panel yearlyE. No additional studies
Key Point
The use of screening blood tests (including tumor markers) and imaging is not recommended for routine breast
cancer follow-up in an otherwise asymptomatic patient with no specific
findings on clinical examination.

Lung Cancer
The most common and the biggest
killer

What they may ask Knowing when to search for it – smoker
with symptoms Non-small cell
Early stage therapy – surgery or radiation Metastatic therapy – platinum-based
chemotherapy Isolated recurrent therapy – resection, then
chemotherapy

What they may ask Small cell
Limited stage therapy – concurrent chemoradiation, then prophylactic brain irradiation
Extended stage therapy – platinum-based chemotherapy
What they won’t ask
Specifics of staging in non small cell Use of gamma knife radiation in
brain metastases Specific combinations of
chemotherapy
A few definitions… Non small cell
Early stage – I or II Tumor confined to one lobe No mediastinal nodes
Advanced stage – III Another nodule in the same lung Mediastinal nodes
Metastatic disease Nodule in opposite lung Pleural effusion Disease in other organs
A few definitions… Small cell
Limited stage Disease confined to one hemithorax or radiation
port Includes mediastinal and ipsilateral supraclavicular
nodes
Extensive stage Any spread outside of the above 1/3 of the time, this is in the brain

…and generalities… Non-small cell
Slower growing Not very chemo- or radiosensitive Resect disease confined to one lobe and
nodes on one side
Small cell Faster growing Very chemo- and radiosensitive Surgery only accidentally

…and paraneoplasias Hypercalcemia – PTHrP – squamous cell Hyponatremia – ectopic ADH – small cell Cushing’s syndrome – from ectopic
ACTH – small cell Hypertrophic pulmonary osteoarthropathy Lambert-Eaton Syndrome Cerebellar degeneration

Non-small cell lung cancer
More serious than the common cold
Keep the FaithA 56-year-old woman is evaluated for a persistent cough of 2.5 months' duration. She also notes a 10-lb weight loss. The patient has no history of pulmonary disease and has never smoked cigarettes.
Physical exam is unremarkable.
Right hilar and subcarinal lymphadenopathy, as well as several hepatic hypodensities consistent with metastatic disease, are identified on CT of the chest and abdomen. MRI brain is normal. Bone scan notes uptake in several ribs. Lung biopsy demonstrates adenocarcinoma.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. CT-guided biopsy of the liver
B. Epidermal growth factor receptor mutation tumor analysis
C. Mediastinoscopy with biopsy
D. Serum chromogranin measurement

Key Point
Patients with epidermal growth factor receptor (EGFR) gene tumor mutations—
most commonly women with adenocarcinoma who are never smokers or
have a very limited smoking history and women of East Asian descent—often
benefit dramatically from therapy targeting this receptor.

Who gets the knife? Patients with no evidence of nodal disease,
or with nodal disease only in the ipsilateral lung (and hilum) on PET, PET/CT, or medastinoscopy
Patients with a single lesion recurrence in the liver or brain
Patients with cord compression Patients with a good performance status
Remember this is in non-small cell only!

Who gets chemo?
Anyone with positive lymph nodes or
metastatic disease

Who gets radiation? Any patient who was a candidate for
surgery, but for their functional status Patients with localized pain from
their tumor Patients with brain metastases Patients with cord compression
where surgery was not performed

I’m Coming OutA 52-year-old man is evaluated for a 5-week history of hemoptysis, a 6-month history of cough, and a 10-lb weight loss. He has a 60-pack-year smoking history.
On physical exam, he has expiratory wheezing localized to the left upper pulmonary lobe.
CT of the thorax and abdomen reveals a 7-cm pulmonary mass in the left upper lobe and small mediastinal lymph node enlargement. Biopsy of the lung lesion shows squamous cell carcinoma. A PET/CT shows extensive uptake in the mass but a low level of uptake in the mediastinal nodes. An MRI brain is normal. Mediastinoscopy and lymph node sampling reveal no evidence of cancer. Stage II disease is confirmed.
Which of the following is the most appropriate treatment of this patient?
A. Combination radiation and chemotherapy
B. Surgical resection
C. Surgical resection followed by chemotherapy
D. Systemic chemotherapy
Key Point
Stage II non-small cell lung cancer is potentially curable with surgical
resection and adjuvant postoperative chemotherapy to reduce the
recurrence risk.

TroublemakerA 54-year-old woman is evaluated for shortness of breath of 3 months' duration and a 10-lb weight loss. She has a 35-pack-year smoking history.
On physical exam, O2 sat is 92% on room air. The patient has clubbing of the fingertips. The lung fields are clear on the left, with diminished breath sounds and dullness to percussion over the lower half of the right lung.
CXR reveals a large right pleural effusion. A thoracentesis demonstrates an exudate, with cytologic analysis indicating adenocarcinoma. A chest tube is placed, and talc pleurodesis is performed. A CT scan reveals a 4-cm right peripheral lung mass with no obvious lymphadenopathy. A bone scan and brain MRI are normal.
Which of the following is the most appropriate treatment?
A. Combination chemotherapy and radiation
B. Radiation
C. Surgical resection of the lung mass
D. Systemic chemotherapy
Key Point
Patients with non-small cell lung cancer and a malignant pleural
effusion have, by definition, metastatic disease, and the most appropriate
therapy is palliative systemic chemotherapy.

Small Cell Lung Cancer
Not a small deal

Always on My MindA 65-year-old man is evaluated for a 3-week history of hemoptysis and a recent 10-lb weight loss. He has a 90-pack-year smoking history.
On physical exam, vital signs are normal. The pulmonary exam reveals occasional crackles at the posterior right midlung field.
CT of the chest shows a 5-cm right hilar mass with bulky mediastinal lymphadenopathy. Bronchoscopy reveals small cell lung cancer. MRI brain and bone scan are negative.
The patient receives 6 cycles of cisplatin and etoposide chemotherapy with radiation to the lung mass and regional disease concurrent with the first cycle of chemotherapy. A follow-up CT chest shows a residual 1.5-cm right hilar abnormality.
Which of the following is the most appropriate next step in this patient's management?
A. Biopsy of the residual mass
B. Three additional cycles of chemotherapy
C. Whole-brain radiation
D. Observation

Key Point
Patients with limited-stage small cell lung cancer who respond to
chemotherapy and radiation should receive prophylactic brain irradiation to
decrease central nervous system relapses and prolong median survival.

Who gets chemo?
In small cell, they all do!

Who gets the knife?
In small cell, no one does! (at least for the board exam)
Who gets radiation? Patients with limited stage disease – to the
chest Patients with limited stage disease and
good response to chest therapy – to the brain prophylactically
Patients with extensive stage disease (and no brain mets) who respond to therapy
Patients with brain mets
Remember that we’re talking about small cell here!

Whip ItA 63-year-old man is evaluated for fatigue and a persistent cough of 7 weeks' duration. He has a 60-pack-year smoking history.
Physical exam is unremarkable.
CT of the thorax shows a right perihilar mass and enlarged hilar and mediastinal lymph nodes.
An endobronchial mass is identified by bronchoscopy; brushings and biopsy reveal small cell lung cancer. CT of the abdomen and pelvis is negative. A bone scan and MRI brain are negative.
Which of the following is the most appropriate next step in the management of this patient?
A. Chemotherapy with adjunctive radiation therapy
B. Mediastinoscopy
C. Radiation therapy
D. Resection for cure
Key Point
Patients with limited-stage small cell lung cancer are treated with
combination chemotherapy and radiation therapy.

Colorectal Cancer
The 4th most common malignancy, the 2nd
leading cause of death
What they may ask Screening measures Colon cancer
Treatment for node negative disease – surgery Treatment for node positive disease – surgery,
then adjuvant chemotherapy Treatment for metastatic disease – surgery, then
chemotherapy (with bevacizumab) Treatment for isolated recurrence in the liver –
resection Treatment for localized rectal cancer –
surgery, then adjuvant chemoradiation

Common ground
All patients with colorectal cancer
need surgery! All of them!
What they won’t ask Hair-splitting questions about high-risk
Stage II disease The use of monoclonal antibodies other
than bevacizumab Chemotherapy combinations for
metastatic rectal cancer 2nd line chemotherapy
At risk groups FAP – Familial Adenomatous Polyposis
Mutation in the APC gene HNPCC – Hereditary Non-Polyposis Colorectal
Cancer Mutation in the MSH2, PMS1, or PMS2 genes At risk for ovarian and endometrial cancer
Or any of the following Personal history of adenomatous, villous, or tubulovillous
polyps Family history of the same Inflammatory bowel disease Diabetes, obesity, tobacco, alcohol
Screening – When? Average risk – age 50 1st degree relative affected (by cancer or
with adenomatous polyp) Age 40, OR 10 years younger than the family member
was diagnosed

Screening – What? Guaiac FOBT – annual Fecal Immunochemical Testing (FIT) –
annual Sigmoidoscopy – every 5 years (with
FOBT every 3 years) Colonoscopy – every 10 years (or every
3-5 for those with relatives diagnosed at <60)
Surveillance Colon cancer
Perioperative colonoscopy Colonoscopy at 1 year, repeat in 3 years, then repeat
in 5 years (assuming all were normal) CEA every 3 months for 2 years, every 6 months for
3 more years CT Chest/Abdomen/Pelvis annually for 3 years
Rectal cancer Same as above, PLUS Proctosigmoidoscopy every 3 to 6 months for 3
years

Colon vs. Rectal Colon
Above the peritoneal reflection Tends to metastasize to the liver first NO ROLE WHATSOEVER FOR RADIATION
Rectal Below the peritoneal reflection Can spread to the lungs before the liver Radiation used to reduce local recurrence

What chemotherapy? Colon
Oxaliplatin based (often with 5-FU) With bevacizumab for metastatic disease
Rectal 5-FU based for localized disease Metastatic depends on squamous vs.
adenocarcinoma (highly unlikely to be tested)
Alive and KickingA 51-year-old man is evaluated for 6 months of increased fatigue and decreased exercise tolerance. He is otherwise well with no significant medical history.
Physical exam is unremarkable. FOBT discloses brown, guaiac-positive stool.
Labs: Hgb 8.4; MCV 80.
Colonoscopy reveals a 5-cm mass in the cecum. Biopsy shows moderately differentiated adenocarcinoma. CT of the chest, abdomen, and pelvis demonstrates the cecal mass and no evidence of metastatic disease. Final pathology from right hemicolectomy reveals a tumor penetrating into the pericolonic fat with clear margins, and 3 of 28 lymph nodes have cancer (T3N1M0; stage III).
Which of the following is the most appropriate management?
A. 5-Fluorouracil and leucovorin
B. 5-Fluorouracil, leucovorin, and oxaliplatin (FOLFOX)
C. Radiation therapy
D. Radiation therapy plus 5-fluorouracil followed by FOLFOX

Key Point
An adjuvant chemotherapy regimen of 5-fluorouracil, leucovorin, and
oxaliplatin (FOLFOX) has been shown to improve disease-free survival in patients with stage III colon cancer.
C’est La VieA 68-year-old woman underwent right hemicolectomy 2 years ago for stage III colon cancer. She received 6 months of chemotherapy with 5-fluorouracil, leucovorin, and oxaliplatin (FOLFOX) after surgery. On a recent follow-up visit, CEA was 43 ng/mL (upper limit of normal, 5 ng/mL). She has no comorbidities and takes no medications. She works full time and is fully functional.
Physical exam reveals a palpable liver edge just below the right costal margin.
Labs: Hgb 13.5, WBC 9000, platelets 288,000.
CT of the chest, abdomen, and pelvis shows 3 hypodense lesions on the right lobe of the liver ranging from 1.5 to 4.0 cm.
Which of the following is the most appropriate management?
A. CT-guided fine-needle aspiration of liver lesion
B. Hepatic arterial embolization
C. Palliative systemic chemotherapy
D. Radiation therapy to the liver
E. Right hepatectomy
Key Point
Surgical resection of a few isolated metastatic lesions may be curative for
patients with colorectal cancer.
Prostate Cancer
The most common cancer in men

What they may ask Making a decision on whether or not
to treat – risk categories Treatment for disease confined to
prostate Side effects of therapy Cord compression

What they won’t ask
Screening recommendations Differentiating between types of
radiation Chemotherapy other than docetaxel

Risk categoriesRisk Tumor Gleason PSA
LowNot
palpable or visible
2-6 <10
Intermediate Confined to prostate 7 10-20
High Extends outside prostate
8-10 >20

Treatment
Risk Life Expectancy Treatment Options
Low
<10 years
10-20 years
>20 years
Observe
Observe, or XRT, or prostatectomy
XRT, or prostatectomy
Intermediate
<10 years
≥10 years
Observe, or XRT, or prostatectomy
XRT, or prostatectomy
High
<5 years
≥5 years
Observe with hormone therapy
XRT with hormone therapy, or XRT alone, or prostatectomy
I Will WaitAn 80-year-old man undergoes an annual physical exam. He has had mild stable nocturia for many years. He reports no bone pain, weight loss, fever, chest pain, or shortness of breath. Medical history is notable for HTN and type 2 DM for which he takes antihypertensive and diabetic medications.
Rectal exam reveals an enlarged prostate gland with a nodule on the right side.
PSA 6.4 ng/mL.
Prostate biopsy reveals several small foci of adenocarcinoma in 2 of 12 cores on the right side, with a Gleason score of 6.
Which of the following is the most appropriate management?
A. Androgen deprivation therapy
B. Radiation with androgen deprivation therapy
C. Radical prostatectomy
D. Observation

Key Point
Patients with low-risk prostate cancer and a short life expectancy are
optimally managed with observation.

Up All NightA 73-year-old man is evaluated for a 6-month history of progressive nocturia.Rectal exam reveals a hard, irregular, and markedly enlarged prostate gland. PSA is 22.5 ng/mL. Bone scan is negative. CT scan reveals a markedly enlarged prostate gland and extension into the seminal vesicles. No lymphadenopathy or evidence of metastatic disease is present. Prostate biopsy reveals adenocarcinoma in all 12 cores with a Gleason score of 8. He has high-risk T3 stage III prostate cancer.
Which of the following is the most appropriate treatment?A. Androgen deprivation therapy (ADT)B. ADT and radiation therapyC. BrachytherapyD. Radiation therapyE. Radical prostatectomy

Key Point
Patients with high-risk prostate cancer are optimally managed with a
combination of androgen deprivation therapy and radiation.

Order of therapy Surgery and radiation equally effective for early
stages Check PSA q6-12 months x 5 years after
primary treatment Goal with recurrence: achieve castrate levels of
testosterone Orchiectomy or androgen deprivation therapy (ADT) Surgical and hormonal (ADT) castration equivalent
Docetaxel based chemotherapy for those who are hormone refractory
Hormone therapy? Potential side effects:
Impotence Hot flashes Weight gain Fatigue Gynecomastia Osteopenia Diarrhea Hepatotoxicity Diabetes Cardiovascular disease
Observation doesn’t sound so bad

Or other therapy? Radiation side effects:
Proctitis Cystitis Erectile dysfunction
Prostatectomy side effects: Erectile dysfunction Urinary incontinence
Back in TimeA 55-year-old man is evaluated in the ER for gradually increasing midback pain for 3 weeks. Metastatic prostate cancer was diagnosed 18 months ago and progressed on antiandrogen therapy. He is now taking bicalutamide, zoledronic acid, docetaxel, and prednisone.
On physical exam, the lower extremities are diffusely weak. He has diminished pinprick sensation from the nipples downward. Reflexes are 2+ in the biceps and triceps and 3+ in the knees and ankles. An extensor plantar response is present bilaterally. Anal sphincter tone is diminished.
IV dexamethasone is administered.
MRI confirms spinal cord compression at the 4th thoracic vertebra.
Which of the following is the most appropriate next step in treatment?
A. Addition of leuprolide
B. Anterior surgical decompression
C. Radiation therapy
D. Substitution of paclitaxel for docetaxel
Key Point
Clinical outcomes in solid tumors are better with surgical decompression of spinal cord compression than they are
with radiation or chemotherapy.

Cord Compression Breast, Lung, Prostate (blastic only),
Renal, Lymphoma, and Myeloma (lytic only)
MRI of the entire spine IV Decadron to reduce vasogenic edema,
relieve pain Neurosurgical consultation for surgical
decompression and spine stabilization
Don’t Know What You GotA 63-year-old woman presents with abrupt onset left upper-extremity weakness and no other symptoms. Until today, she has been active and fully functional. She had stage IIB non-small cell lung cancer diagnosed 1 year ago and underwent right upper lobectomy followed by adjuvant cisplatin and vinorelbine chemotherapy. Mediastinoscopy at the time was negative, and PET showed no metastatic disease. Neurologic exam shows weakness of the left arm with hyperreflexia of the brachioradialis reflex. MRI brain demonstrates a right parietal lesion measuring 1.5 cm, with evidence of significant edema. She has no evidence of extracranial disease. Dexamethasone is initiated.
Which of the following is the most appropriate next step in management?A. Best supportive careB. Initiation of erlotinibC. Initiation of temozolomide followed by radiation therapyD. Surgical resection of metastasis
Key Point
Resect isolated brain (or liver) metastases when there is no other
evidence of cancer.
RememberBrain mets are life-limiting; they
must always be addressed immediately when found.
Decadron immediately Surgery Radiation Chemotherapy

Head GamesA 46-year-old woman is evaluated for the recent onset of headaches that are most intense on waking in the morning and are not relieved by analgesics. She has no nausea or vomiting but notes some difficulty with fine motor skills when using her right hand. The patient has a 2-year history of stage II breast cancer last treated with chemotherapy 2 years ago.
Funduscopic exam reveals papilledema. She has reduced strength (4/5+) in her right hand.
A CT of the head reveals 2 separate masses in the left temporal lobe with associated edema, as well as blastic lesions involving the skull.
Which of the following is the most appropriate management?
A. Chemotherapy
B. Intravenous dexamethasone and radiation therapy
C. Lumbar puncture
D. Resection of the masses

Key Point
Immediate corticosteroid administration and early initiation of
radiation therapy are indicated to treat brain metastasis and increased
intracranial pressure.

Ovarian Cancer
Risk and Screening The most significant risk factor for ovarian cancer,
especially in premenopausal women, is the presence of BRCA1/BRCA2 gene mutations; hereditary nonpolyposis colorectal cancer syndrome also confers a significantly increased risk.
Use of oral contraceptive agents decreases the risk of ovarian cancer by as much as 50% with the protective effect lasting up to 20 years after oral contraception cessation.
Screening for ovarian cancer is not recommended for average-risk women.
In women at high risk for developing ovarian cancer, prophylactic bilateral salpingo-oophorectomy before age 40 years reduces the risk of developing cancer by 95%.
Diagnosis and Staging Most patients with ovarian cancer have
advanced disease at initial evaluation. Findings on ultrasonography suggestive of
ovarian cancer include a solid mass, a cyst with thick septations, and ascites.
The diagnosis of advanced ovarian cancer is usually made by CT or ultrasound-guided biopsy of a suspicious mass or cytologic examination of ascitic fluid.
Surgical Role Optimal tumor debulking (no residual tumor
mass >1 cm) is associated with increased survival in patients with ovarian cancer.
Surgical resection is appropriate for patients with a recurrent solitary ovarian tumor or with limited relapse of cancer at sites favorable for surgical removal.

Chemotherapy Adjuvant chemotherapy is indicated for patients
with high-risk, early-stage ovarian cancer and those with advanced disease.
Use of hematopoietic growth factors to maintain adequate blood counts has helped improve the quality of life and decrease complication rates in patients with ovarian cancer who are receiving chemotherapy.

Follow-up Patients who have completed initial treatment
for ovarian cancer require routine follow-up clinical evaluations, including history, physical examination, and serum CA-125 measurement.

Gastrointestinal Cancer
Pancreatic Cancer Patients with metastatic pancreatic cancer
have a median survival ranging from 4 to 6 months; those with locally unresectable disease have a median survival of about 1 year.
Surgery is the only potentially curative intervention for patients with pancreatic cancer who have an apparent technically resectable tumor without evidence of metastases.
Gastric Cancer Helicobacter pylori infection is a major risk factor for
development of gastric cancer. In patients who undergo surgery as initial therapy for
gastric cancer, postoperative 5-fluorouracil and leucovorin plus radiation therapy have been shown to confer a survival benefit compared with postoperative observation alone.
Patients with gastric and gastroesophageal junction adenocarcinoma whose tumors expressed HER2 experienced statistically significantly improved median survival when trastuzumab was added to cisplatin plus 5-fluorouracil or capecitabine.

Esophageal Cancer Gastroesophageal reflux disease, Barrett
esophagus, and obesity are risk factors for esophageal cancer.
The diagnosis of esophageal cancer is established by upper endoscopy and biopsy.
Local and locoregional esophageal cancers are usually treated surgically; perioperative treatment with chemotherapy or chemotherapy plus radiation therapy may improve survival.

Anal Cancer Anal cancer is treated initially with combined
radiation therapy and chemotherapy. Mitomycin plus 5-fluorouracil is the standard
chemotherapy regimen used in conjunction with radiation therapy in the treatment of anal cancer.

Urgencies & Emergencies
Structural Superior vena cava syndrome is most often caused
by lung cancer; other causes are lymphoblastic and diffuse large B-cell lymphoma, Hodgkin lymphoma, and germ cell tumors.
Primary therapy for the underlying malignancy is usually associated with rapid and complete resolution of symptoms and physical findings of superior vena cava syndrome.
Lumbar puncture is contraindicated when increased intracranial pressure is due to mass effect because the procedure may precipitate catastrophic brainstem herniation.
Structural Corticosteroids such as dexamethasone are
initially used to treat patients with increased intracranial pressure.
Patients with breast, lung, and prostate cancer are most likely to develop spinal cord compression.
Patients with suspected spinal cord compression require prompt diagnosis (MRI of the spine), usually before any motor deficit is detected, and immediate administration of corticosteroids.

Structural A malignant pleural effusion is most often caused
by lung cancer, breast cancer, and lymphoma, and less frequently by cancer of unknown primary site.
Thoracentesis is required for immediate palliation of a symptomatic malignant pleural effusion.
Excessive drainage in patients with malignant pleural effusion should be avoided to prevent pulmonary edema following lung re-expansion.
Echocardiography is essential to establish the diagnosis of malignant pericardial effusion.
Metabolic Prevention and treatment of tumor lysis
syndrome require hydration with normal saline as well as allopurinol or rasburicase in high-risk patients to limit the degree of hyperuricemia.
Symptoms of hypercalcemia include nausea and vomiting, constipation, polyuria and polydipsia, weakness, and confusion.
The mainstays of treatment of hypercalcemia are aggressive hydration with normal saline for short-term control and parenteral bisphosphonates for longer-term control.
Effects of Cancer Therapy

Chemotherapy The risk of life-threatening infection in patients
receiving cancer treatment significantly increases with absolute neutrophil counts lower than 500/µL (0.5 × 109/L) and as the duration of neutropenia increases.
Recombinant granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor are effective in preventing neutropenia and neutropenic fever and maintaining the dose intensity of chemotherapy.
Myelodysplasia and leukemia can be caused by chemotherapy and, to a lesser extent, radiation therapy.
Other Involved-field radiation therapy may cause acute
and chronic cardiac disorders. Patients with breast cancer who are treated with
combined chemotherapy or radiation have an increased lifetime risk for developing myelodysplasia, leukemia, endometrial cancer, and rarely, soft tissue sarcoma.
Long-term administration of aromatase inhibitors in women with breast cancer has significantly increased the incidence of osteopenia and risk for late pathologic fractures.
Head & Neck Cancer

Risk and Presentation The major risk factors for development of head
and neck cancer are alcohol and tobacco use. Epstein-Barr virus and human papillomavirus
infection may be responsible for development of head and neck cancer in a subset of patients without a history of tobacco use.
Diagnosis and Staging Presenting signs and symptoms of head and
neck cancer depend on the location of the primary tumor.
Patients with cervical lymphadenopathy require expert evaluation of the upper aerodigestive tract to identify a primary lesion; fine-needle aspiration of a palpable lymph node is performed, followed by a lymph node biopsy if the aspirate is nondiagnostic.

Treatment Goals of treatment of head and neck cancer focus on
improving survival while preserving organ function and minimizing complications.
Early-stage (stage I and II) head and neck cancer is highly curable with surgical resection or radiation therapy.
Locally advanced stage III and IV head and neck cancer is treated with a combination of surgical resection, radiation therapy, and chemotherapy.
Complications following treatment of head and neck cancer include damage to cranial and sensory nerves, xerostomia, swallowing dysfunction, voice changes, altered taste sensation, fibrosis, dental problems, and esophageal strictures.

Genitourinary Cancer

Germ Cell Tumor Testicular cancer is the most common solid
tumor in young men and is one of the most highly curable of all malignancies.
The primary risk factors for development of testicular cancer are the presence of Klinefelter syndrome, cryptorchidism, and a family history of testicular cancer.
Patients with testicular cancer usually present with a unilateral mass or testicular swelling.

Germ Cell Tumor Initial urologic evaluation of a patient with suspected
testicular cancer includes a chest radiograph, CT scan of the abdomen and pelvis, and determination of serum tumor marker levels.
All patients with testicular cancer (either seminoma or nonseminoma) require radical orchiectomy as initial treatment.
Patients with nonseminoma have a poorer prognosis than those with seminoma and require more aggressive treatment, but even with widespread metastases, may be cured with additional surgery and combination chemotherapy.
Bladder Cancer Most bladder cancers occur in men, who are
typically over 60 years of age. Cigarette smoking is the major risk factor for
development of bladder cancer. Patients with bladder cancer most often
present with painless hematuria. All components of the urinary tract must be
evaluated in patients with hematuria to identify a potential malignant source (or sources) of bleeding.

Bladder Cancer Approximately 60% of patients with bladder cancer are
found to have noninvasive disease at the time of initial TNM staging.
Patients with noninvasive bladder cancer are usually treated with transurethral resection of the bladder tumor and have an excellent prognosis.
Patients with bladder cancer that invades muscle usually require radical cystectomy, including removal of the bladder, adjacent pelvic organs, and regional lymph nodes.
Metastatic bladder cancer is incurable, and palliative platinum-based chemotherapy is often used in this setting.

Renal Cell Cancer Most patients with renal cell cancer present with a mass
found incidentally on a radiographic study performed for other reasons.
Large solid tumors seen on ultrasound imaging are so likely to be renal cell carcinoma that needle biopsy is not needed before definitive surgical resection is planned.
Partial nephrectomy is appropriate for patients with renal cell tumors measuring less than 4 cm that are not adjacent to the renal pelvis.
Molecularly targeted agents such as sunitinib, sorafenib, bevacizumab, temsirolimus, and everolimus have been shown to be effective in treating patients with resected renal cell cancer who develop metastatic disease.

Cancer of Unknown Primary

Diagnosis Before more specialized studies are done in patients
with cancer of unknown primary site, biopsy samples of tumor from the most accessible location should be obtained for immunohistochemical marker determinations.
An exhaustive search for a primary tumor should not be done in patients with cancer of unknown primary site because finding an asymptomatic and occult primary tumor has not been shown to improve outcome.
Evaluation of patients with cancer of unknown primary (CUP) site should focus on whether findings are consistent with a treatable primary tumor or a treatable subtype of CUP.
Treatment & Prognosis Women with cancer of unknown primary site
associated with isolated malignant axillary lymphadenopathy should be assumed to have locoregional breast cancer until proved otherwise.
Women with cancer of unknown primary site presenting as abdominal carcinomatosis and ascites should be assumed to have ovarian cancer until proved otherwise.
Patients with cancer of unknown primary site that is not included in a favorable subgroup generally have a poor prognosis and typically receive empiric therapy.

Melanoma
Risk & Treatment Risk factors for melanoma include sun
exposure, a history of multiple sunburns, fair complexion, the presence of multiple cutaneous nevi, and a personal or family history of melanoma or dysplastic nevi.
The primary treatment of local and locoregional melanoma is surgical resection.
Resection is indicated for patients with limited metastatic melanoma that is surgically resectable.
Final Advice If you get stuck, remember these
generalities: The only way to “cure” cancer includes surgery. Cancer that has spread to lymph nodes or beyond
requires systemic treatment (i.e., chemotherapy). If you’re going to act, make it definitive (e.g.,
obtain a diagnosis, prefer curative treatments). You stand a good chance of guessing correctly.

Good Luck!
If you prepare well, you won’t need it.

















