OBSERVATIONAL STUDY Can sadness alter posture? Jose ´ Luı ´s Pimentel do Rosa ´rio, PT, PhD*, Maria Suely Bezerra Dio ´genes, MD, PhD , Rita Mattei, PhD , Jose´ Roberto Leite, PhD Federal University of Sa˜o Paulo, UNIFESP, Department of Psychobiology, Rua Botucatu, 862, 1o. Andar, Vila Clementino, Sa˜o Paulo, SP, CEP 04023062, Brazil Received 3 September 2012; received in revised form 23 November 2012; accepted 30 November 2012 KEYWORDS Posture; Sadness; Emotion; Postural assessment; Analog scales Summary The present study investigated the existence of a relationship between subjective sadness and body posture in 28 women, aged between 20 and 39 years, who had a normal body mass indices (or were underweight) and an absence of neurological, psychiatric or musculo- skeletal disorders. The postural parameter photographed was protraction of the shoulder. The degree of sadness was rated by analog scales representing current and usual sadness. The results indicated that a relationship exists between protraction of the shoulder and usual sadness (p Z 0.05). However, there was no relationship between current sadness and the shoulder position. In conclusion, the usual sadness can lead to shoulder protraction. ª 2012 Elsevier Ltd. All rights reserved. Introduction Posture and emotions, empirically, have a strong connec- tion. However, scientific evidence for a relationship between these two human characteristics has not yet been reported. Emotions affect the muscles in many ways including the following: the effect of anxiety on heart rate and its rhythm generating a tachycardia; the diaphragm and respiratory rate and hyperventilation; and the skeletal muscles in general. Another example is the effect of slow breathing to reduce anxiety (Darwin, 1899; Garbossa et al., 2009). Emotion involves a complex set of interactions mediated by neurohormonal systems, which can give rise to affective experiences, generate cognitive processes, activate wide- spread physiological adjustments to elicit conditions and affect behavior (Kleinginna and Kleinginna, 1981). Emotions affect attention, behavior and responses to events, as well as activating relevant associative networks in memory (Izard, 1991). A painful or traumatic experience is encoded in the central nervous system by the amygdala as a non- verbal memory and stored in patterns of muscle contrac- tions and neurovegetative sensations by the autonomic nervous system, which connects emotions to organic func- tions (Schulz, 1998). It is important to consider that each emotion is the integration of specific neurochemical and * Corresponding author. Rua das Rosas 620, Mirando ´polis, Sa ˜o Paulo, SP, CEP 04048-001, Brazil. Tel.: þ55 42 9992 9992. E-mail address: ze.fi[email protected](J.L.P.doRosa´rio). 1360-8592/$ - see front matter ª 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jbmt.2012.12.001 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/jbmt Journal of Bodywork & Movement Therapies (2013) 17, 328e331
Transcript
Journal of Bodywork & Movement Therapies (2013) 17, 328e331
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/jbmt
OBSERVATIONAL STUDY
Can sadness alter posture?
Jose Luıs Pimentel do Rosario, PT, PhD*,Maria Suely Bezerra Diogenes, MD, PhD ,Rita Mattei, PhD , Jose Roberto Leite, PhD
Federal University of Sao Paulo, UNIFESP, Department of Psychobiology, Rua Botucatu,862, 1o. Andar, Vila Clementino, Sao Paulo, SP, CEP 04023062, Brazil
Received 3 September 2012; received in revised form 23 November 2012; accepted 30 November 2012
1360-8592/$ - see front matter ª 201http://dx.doi.org/10.1016/j.jbmt.201
Summary The present study investigated the existence of a relationship between subjectivesadness and body posture in 28 women, aged between 20 and 39 years, who had a normal bodymass indices (or were underweight) and an absence of neurological, psychiatric or musculo-skeletal disorders. The postural parameter photographed was protraction of the shoulder.The degree of sadness was rated by analog scales representing current and usual sadness.The results indicated that a relationship exists between protraction of the shoulder and usualsadness (p Z 0.05). However, there was no relationship between current sadness and theshoulder position. In conclusion, the usual sadness can lead to shoulder protraction.ª 2012 Elsevier Ltd. All rights reserved.
Introduction
Posture and emotions, empirically, have a strong connec-tion. However, scientific evidence for a relationshipbetween these two human characteristics has not yet beenreported. Emotions affect the muscles in many waysincluding the following: the effect of anxiety on heart rateand its rhythm generating a tachycardia; the diaphragm andrespiratory rate and hyperventilation; and the skeletalmuscles in general. Another example is the effect of slow
osas 620, Mirandopolis, Sao: þ55 42 9992 9992.(J.L.P. do Rosario).
2 Elsevier Ltd. All rights reserved2.12.001
breathing to reduce anxiety (Darwin, 1899; Garbossa et al.,2009).
Emotion involves a complex set of interactions mediatedby neurohormonal systems, which can give rise to affectiveexperiences, generate cognitive processes, activate wide-spread physiological adjustments to elicit conditions andaffect behavior (Kleinginna and Kleinginna, 1981). Emotionsaffect attention, behavior and responses to events, as wellas activating relevant associative networks in memory(Izard, 1991). A painful or traumatic experience is encodedin the central nervous system by the amygdala as a non-verbal memory and stored in patterns of muscle contrac-tions and neurovegetative sensations by the autonomicnervous system, which connects emotions to organic func-tions (Schulz, 1998). It is important to consider that eachemotion is the integration of specific neurochemical and
Figure 1 Lateral photograph with tracings of the angle ofprotrusion of the shoulder.
Posture and emotion 329
motor processes, and it can be considered as the primarymotivational system in humans (Izard, 1991). The emotionof sadness can be seen as a reaction to the failure to ach-ieve or maintain a goal (Stein and Trabasso, 1992).
A differentiation seems to exist between males andfemales in terms of the embodiment of emotions. Femalesare better at showing some emotions, as well as the asso-ciated postures and facial expressions. Among fourcommonly studied emotions (love, happiness, anger andsadness) females obtained higher scores than males in testsof all emotions except anger (Kevrekidis et al., 2008).
The study of human posture is relatively new comparedto other areas of medical science, and refers to the align-ment and maintenance of body segments in certain posi-tions (Rosario et al., 2004). Some postural deviations mayadversely affect muscular efficiency, predispose individualsto pain and pathological musculoskeletal conditions andprovoke unaesthetic alterations (Rosario et al., 2004;Liebenson, 2008; James et al., 2009; Wallden, 2009). Thespecific focus on posture is very important since it is relatedto quality of life, a fact that has stimulated interest indifferent areas.
Wilhelm Reich was a pioneer in correlating body postureand muscle contraction (muscular armoring), which in turnis related to emotional aspects (Reich, 1942). A programcould exist in humans, at the level of the nervous system,which establishes a connection between specific emotionsand certain muscle movements. This correspondence wouldbe invariable (Ekman et al., 1983).
Based on a literature review, emotional changes can,with proper stimulation, affect any human being and causemuscle changes coherent with the emotional state. In thiscontext, posture can be an important tool in terms of thediagnosis and treatment of emotional problems. However,there are still very few studies in the literature that haveinvestigated this correlation. The aim of the present studywas to investigate the existence of a relationship betweenthe posture represented by protraction of the shoulder andthe sadness emotion.
Methods
Twenty-eight women, aged between 20 and 39 years, whohad a normal body mass indices between 16 and 24.9 kg/m2were assessed (WHO, 1998). The women could not be intheir menstrual period at the time of the assessment. Theexclusion criteria included any psychiatric, neurological ormusculoskeletal disorders. The present study receivedapproval from the Human Research Ethics Committee of theUNIFESP under protocol number 1391/05 and the partici-pants signed a statement of informed consent.
The volunteers were subjected to the same assessmentprotocol which included demographic data (age, weight inkilograms and height in meters). A digital camera (CanonPower Shot A400) was used for the documentation of thesubject’s standing right lateral view. The image wastransferred to an Intel Core 2 Duo computer and the angleof protraction of the shoulder was examined by Corel Draw(Fig. 1), as described by Munhoz et al. (2005). The first stepwas to draw a parallel line to the ground. Then, anotherline was drawn perpendicular to the first line, which had
the same function as a plumb line. This line was positionedin the photo, at the very back of the heel of the subject.Another line was drawn from this heel point to the mostanterior part of the shoulder. The angle between these twolines, with the heel as the fulcrum, revealed the shoulder’sprotrusion angle. The temperature in the assessment roomwas kept at a constant 25 �C to avoid possible influences onposture.
Analog scales were used to assess the degree ofsubjective sadness (Williams et al., 2010), which facilitatedan assessment of usual sadness (a chronic feeling) andcurrent sadness (momentary feeling present at the time ofassessment). The scales were characterized by a 10 cmline, with the words: “no sadness at all” to the extreme leftand “Utter despair” to the extreme right, numbered from0 to 10 (Fig. 2). The volunteers were instructed to makea dash at the place of the line that best described theiremotional state. The usual sadness scale sheet, designed tohelp the subjects to understand, said “you always feel”right above the numbers. The current sadness scale sheetreads “How you are feeling at this exact moment”.
The linear regression technique and the effect of samplesize were calculated using the ‘Statistical Package for theSocial Sciences’ (SPSS) software. The level of significancefor the linear regression was set at p < 0.05. The power of
Usual sadness (you always feel)
0 1 2 3 4 5 6 7 8 9 10
No sadness at all Utter despair
Figure 2 Example of the analog scales used in the presentstudy e a value of 0 signifies an absence of the emotion studiedwhereas a value of 10 would be the strongest possible feelingrelated to that emotion.
Figure 4 Scatter graph showing the distribution of the usualsadness values and the resulting line.
330 J.L.P. Rosario et al.
the sample had a small effect if r Z 0.10 (explained 1% ofthe total variance), a medium effect if r Z 0.30 (explained9% of the total variance) and a large effect if r Z 0.50(explained 25% of the total variance).
For a better understanding of the results, Fig. 3 showsa scatter graph of the variable current sadness. Fig. 4 showsthe same graph for usual sadness, which is closer thancurrent sadness to the protrusion shoulder line as seen inFig. 5.
Results
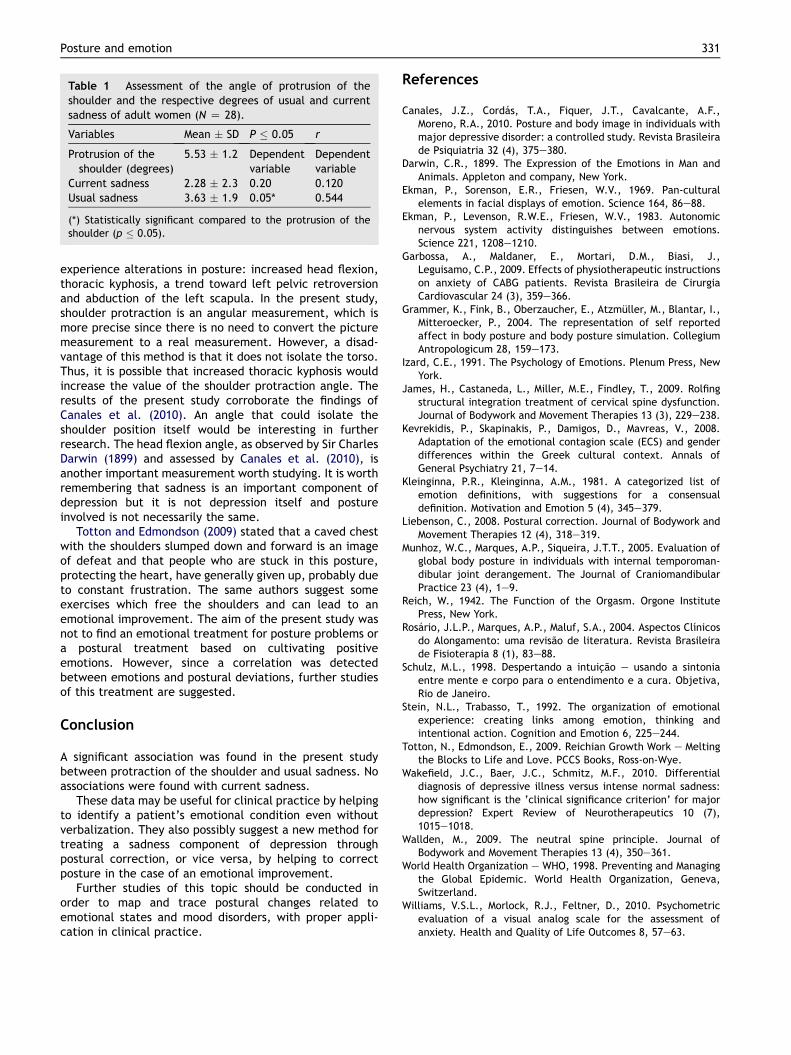
Table 1 displays the data obtained from the calculation ofthe linear regression between the postural and emotionalvariables. It is possible to notice a clear correlationbetween Usual Sadness (p Z 0.05) and protrusion of theshoulders. The power of the sample value was r Z 0.544,which indicated a large sample size effect. For the corre-lation between protrusion of the shoulders and CurrentSadness (p Z 0.20), the hypothesis of equality could not berejected, and a small sample size was obtained (rZ 0.120).
Discussion
It was possible to confirm a statistically significant associ-ation between protrusion of the shoulder and usualsubjective sadness. These results are similar to those ofother authors who have stated that emotions are related topatterns of contraction of the facial muscles (Ekman et al.,1969, 1983) and body posture (Grammer et al., 2004).These results demonstrated that there are postures takenby the body in response to the experience of a specific
Figure 3 Scatter graph showing the distribution of thecurrent sadness values and the resulting line.
emotion. There were no statistically significant associationsbetween protrusion of the shoulder and current subjectivesadness at the time of testing.
The absence of associations between current sadnessand protrusion of the shoulder may have occurred becauseof the environment where the assessments took place. Ina neutral situation, an event that causes transient sadnessto the subject may not have as strong an influence at thetime of assessment. If this sadness was not experiencedwith the relevant intensity when the photo was taken, thiscould explain why the shoulders do not protrude signifi-cantly in response. On the other hand, chronic sadnessfeelings have an influence on the postural muscles forlengthy periods, sometimes for years, and may leave tracesthat are not easily hidden because of resulting muscleshortening.
Darwin wrote about posture and depression in his book‘The Expression of Emotion in Man and Animals’ (1899).According to the author, individuals fall into a depressivestate after suffering a problem or sorrow when its causeremains. The same occurs with prolonged pain. There is nodesire for action in this state and as a result, the circulationbecomes weaker and slower, the muscles become flabby,the eyelids fall, the head is hung on the contracted chest,and the lips and chin slide down with their own weight. If‘contracted chest’ can also be described as protraction ofthe shoulders, this is similar to the findings of the presentstudy, since sadness is one of the symptoms of depression(Wakefield et al., 2010).
Canales et al. (2010) found that, during episodes ofdepression, individuals with major depressive disorder
Figure 5 Scatter graph showing the distribution of theprotrusion of the shoulder values and the resulting line.
Table 1 Assessment of the angle of protrusion of theshoulder and the respective degrees of usual and currentsadness of adult women (N Z 28).
(*) Statistically significant compared to the protrusion of theshoulder (p � 0.05).
Posture and emotion 331
experience alterations in posture: increased head flexion,thoracic kyphosis, a trend toward left pelvic retroversionand abduction of the left scapula. In the present study,shoulder protraction is an angular measurement, which ismore precise since there is no need to convert the picturemeasurement to a real measurement. However, a disad-vantage of this method is that it does not isolate the torso.Thus, it is possible that increased thoracic kyphosis wouldincrease the value of the shoulder protraction angle. Theresults of the present study corroborate the findings ofCanales et al. (2010). An angle that could isolate theshoulder position itself would be interesting in furtherresearch. The head flexion angle, as observed by Sir CharlesDarwin (1899) and assessed by Canales et al. (2010), isanother important measurement worth studying. It is worthremembering that sadness is an important component ofdepression but it is not depression itself and postureinvolved is not necessarily the same.
Totton and Edmondson (2009) stated that a caved chestwith the shoulders slumped down and forward is an imageof defeat and that people who are stuck in this posture,protecting the heart, have generally given up, probably dueto constant frustration. The same authors suggest someexercises which free the shoulders and can lead to anemotional improvement. The aim of the present study wasnot to find an emotional treatment for posture problems ora postural treatment based on cultivating positiveemotions. However, since a correlation was detectedbetween emotions and postural deviations, further studiesof this treatment are suggested.
Conclusion
A significant association was found in the present studybetween protraction of the shoulder and usual sadness. Noassociations were found with current sadness.
These data may be useful for clinical practice by helpingto identify a patient’s emotional condition even withoutverbalization. They also possibly suggest a new method fortreating a sadness component of depression throughpostural correction, or vice versa, by helping to correctposture in the case of an emotional improvement.
Further studies of this topic should be conducted inorder to map and trace postural changes related toemotional states and mood disorders, with proper appli-cation in clinical practice.
References
Canales, J.Z., Cordas, T.A., Fiquer, J.T., Cavalcante, A.F.,Moreno, R.A., 2010. Posture and body image in individuals withmajor depressive disorder: a controlled study. Revista Brasileirade Psiquiatria 32 (4), 375e380.
Darwin, C.R., 1899. The Expression of the Emotions in Man andAnimals. Appleton and company, New York.
Ekman, P., Sorenson, E.R., Friesen, W.V., 1969. Pan-culturalelements in facial displays of emotion. Science 164, 86e88.
Ekman, P., Levenson, R.W.E., Friesen, W.V., 1983. Autonomicnervous system activity distinguishes between emotions.Science 221, 1208e1210.
Garbossa, A., Maldaner, E., Mortari, D.M., Biasi, J.,Leguisamo, C.P., 2009. Effects of physiotherapeutic instructionson anxiety of CABG patients. Revista Brasileira de CirurgiaCardiovascular 24 (3), 359e366.
Grammer, K., Fink, B., Oberzaucher, E., Atzmuller, M., Blantar, I.,Mitteroecker, P., 2004. The representation of self reportedaffect in body posture and body posture simulation. CollegiumAntropologicum 28, 159e173.
Izard, C.E., 1991. The Psychology of Emotions. Plenum Press, NewYork.
James, H., Castaneda, L., Miller, M.E., Findley, T., 2009. Rolfingstructural integration treatment of cervical spine dysfunction.Journal of Bodywork and Movement Therapies 13 (3), 229e238.
Kevrekidis, P., Skapinakis, P., Damigos, D., Mavreas, V., 2008.Adaptation of the emotional contagion scale (ECS) and genderdifferences within the Greek cultural context. Annals ofGeneral Psychiatry 21, 7e14.
Kleinginna, P.R., Kleinginna, A.M., 1981. A categorized list ofemotion definitions, with suggestions for a consensualdefinition. Motivation and Emotion 5 (4), 345e379.
Munhoz, W.C., Marques, A.P., Siqueira, J.T.T., 2005. Evaluation ofglobal body posture in individuals with internal temporoman-dibular joint derangement. The Journal of CraniomandibularPractice 23 (4), 1e9.
Reich, W., 1942. The Function of the Orgasm. Orgone InstitutePress, New York.
Rosario, J.L.P., Marques, A.P., Maluf, S.A., 2004. Aspectos Clınicosdo Alongamento: uma revisao de literatura. Revista Brasileirade Fisioterapia 8 (1), 83e88.
Schulz, M.L., 1998. Despertando a intuicao e usando a sintoniaentre mente e corpo para o entendimento e a cura. Objetiva,Rio de Janeiro.
Stein, N.L., Trabasso, T., 1992. The organization of emotionalexperience: creating links among emotion, thinking andintentional action. Cognition and Emotion 6, 225e244.
Totton, N., Edmondson, E., 2009. Reichian Growth Work e Meltingthe Blocks to Life and Love. PCCS Books, Ross-on-Wye.
Wakefield, J.C., Baer, J.C., Schmitz, M.F., 2010. Differentialdiagnosis of depressive illness versus intense normal sadness:how significant is the ‘clinical significance criterion’ for majordepression? Expert Review of Neurotherapeutics 10 (7),1015e1018.
Wallden, M., 2009. The neutral spine principle. Journal ofBodywork and Movement Therapies 13 (4), 350e361.
World Health Organization e WHO, 1998. Preventing and Managingthe Global Epidemic. World Health Organization, Geneva,Switzerland.
Williams, V.S.L., Morlock, R.J., Feltner, D., 2010. Psychometricevaluation of a visual analog scale for the assessment ofanxiety. Health and Quality of Life Outcomes 8, 57e63.