07.08.2014 1 Lung Cancer in Older Adults….. 2 Cases Dr Christopher Steer Border Medical Oncology Albury-Wodonga Inaugural Chair Geriatric Oncology Interest Group (COSA) Cancer in the Older Person Individualised management Cancer in the Older Person Individualised management ? + Individualised Oncologic and Geriatric Care Plan Lung Cancer – Case 1 Lung Cancer – Case 1 Mr JN aged 85 years November 2013 Married, supportive wife Retired truck driver Social – in process of selling large family home Moving into retirement village in centre of town. Ex smoker – ceased 25 years ago. Mr JN aged 85 years November 2013 Married, supportive wife Retired truck driver Social – in process of selling large family home Moving into retirement village in centre of town. Ex smoker – ceased 25 years ago. Lung Cancer – Case 1 Lung Cancer – Case 1 Mr JN aged 85 years Comorbidities Hypertension - on candesartan Gout Mild osteoarthritis - Operation for diverticular disease in 2001 Performance Status = 1 Mr JN aged 85 years Comorbidities Hypertension - on candesartan Gout Mild osteoarthritis - Operation for diverticular disease in 2001 Performance Status = 1
Transcript
07.08.2014
1
Lung Cancer in Older
Adults…..
2 Cases
Dr Christopher SteerBorder Medical Oncology
Albury-WodongaInaugural Chair Geriatric Oncology Interest Group (COSA)
Cancer in the Older Person
Individualised managementCancer in the Older Person
Individualised management
?
+
Individualised Oncologic and Geriatric Care Plan
Lung Cancer – Case 1Lung Cancer – Case 1
Mr JN aged 85 years
November 2013
Married, supportive wife
Retired truck driver
Social – in process of selling large family home
Moving into retirement village in centre of town.
Ex smoker – ceased 25 years ago.
Mr JN aged 85 years
November 2013
Married, supportive wife
Retired truck driver
Social – in process of selling large family home
Moving into retirement village in centre of town.
Ex smoker – ceased 25 years ago.
Lung Cancer – Case 1Lung Cancer – Case 1
Mr JN aged 85 years
Comorbidities
Hypertension - on candesartan
Gout
Mild osteoarthritis -
Operation for diverticular disease in 2001
Performance Status = 1
Mr JN aged 85 years
Comorbidities
Hypertension - on candesartan
Gout
Mild osteoarthritis -
Operation for diverticular disease in 2001
Performance Status = 1
07.08.2014
2
Lung Cancer – Case 1Lung Cancer – Case 1
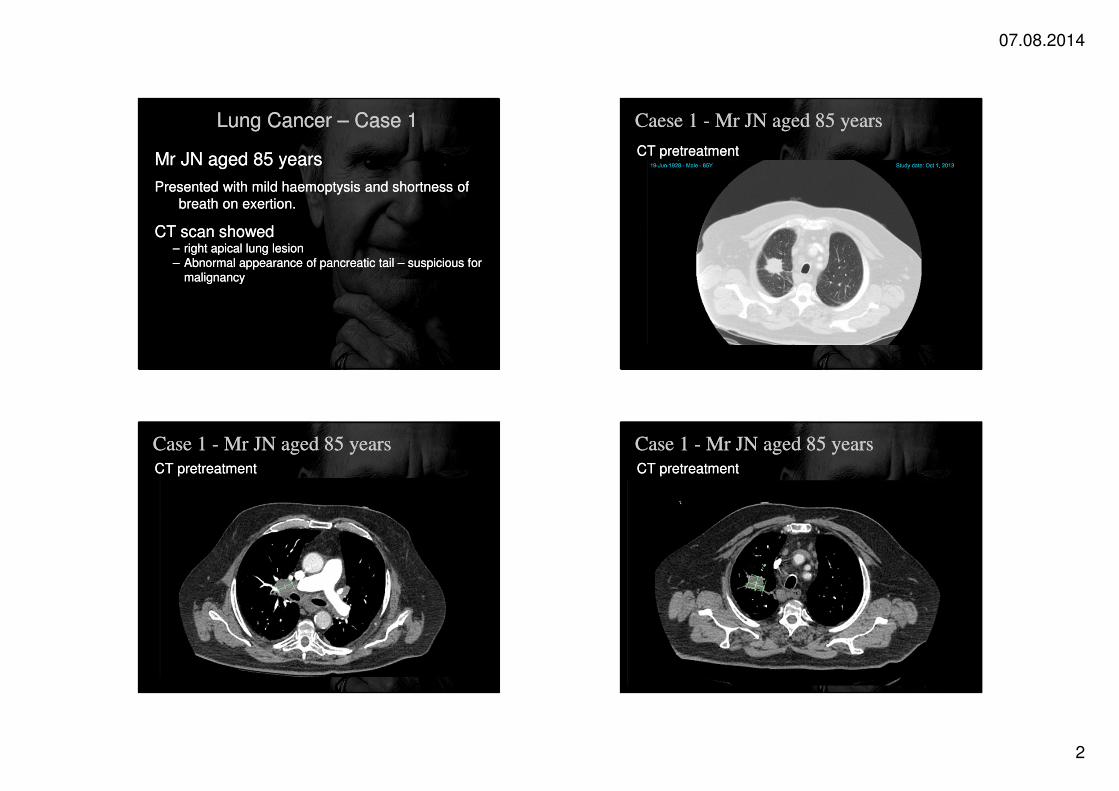
Mr JN aged 85 years
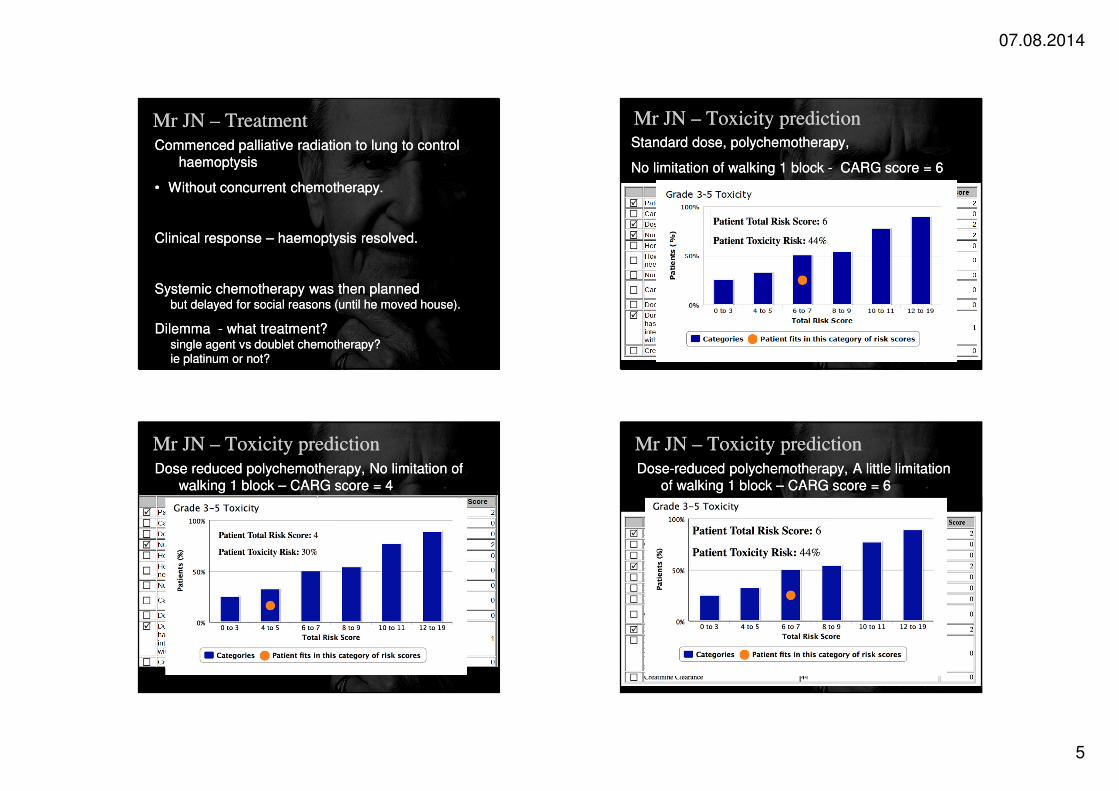
Presented with mild haemoptysis and shortness of
breath on exertion.
CT scan showed – right apical lung lesion– Abnormal appearance of pancreatic tail – suspicious for
malignancy
Mr JN aged 85 years
Presented with mild haemoptysis and shortness of
breath on exertion.
CT scan showed – right apical lung lesion– Abnormal appearance of pancreatic tail – suspicious for
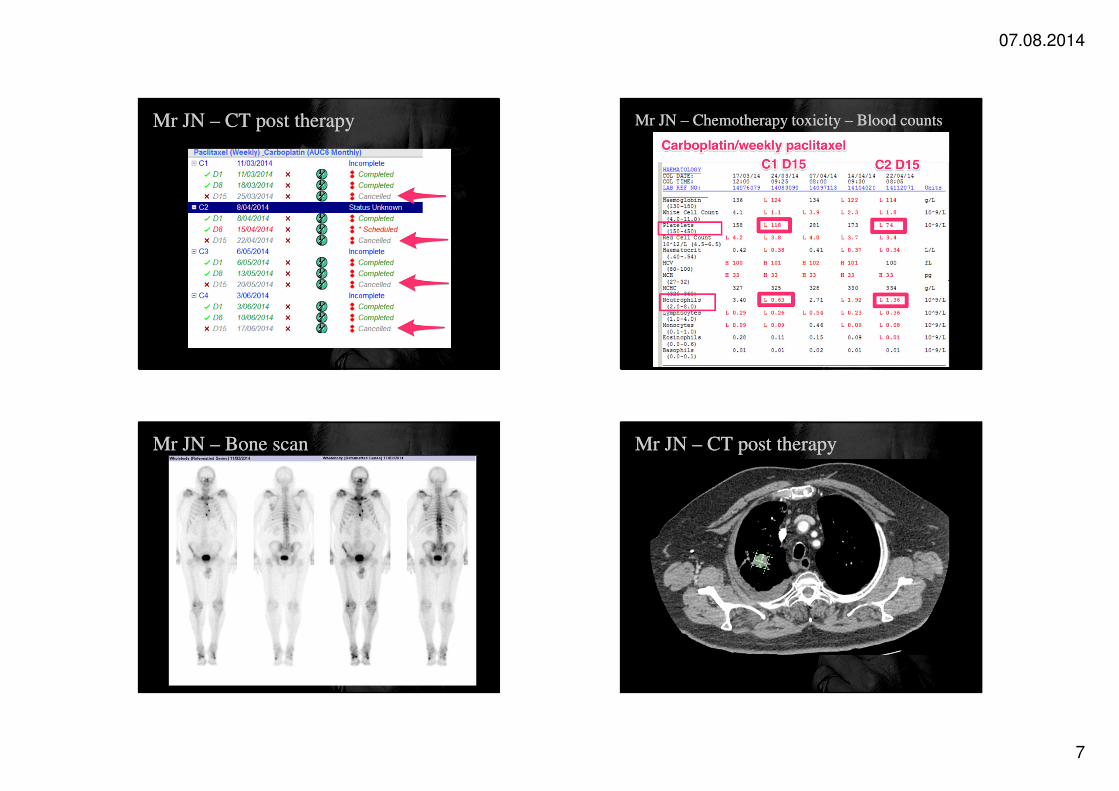
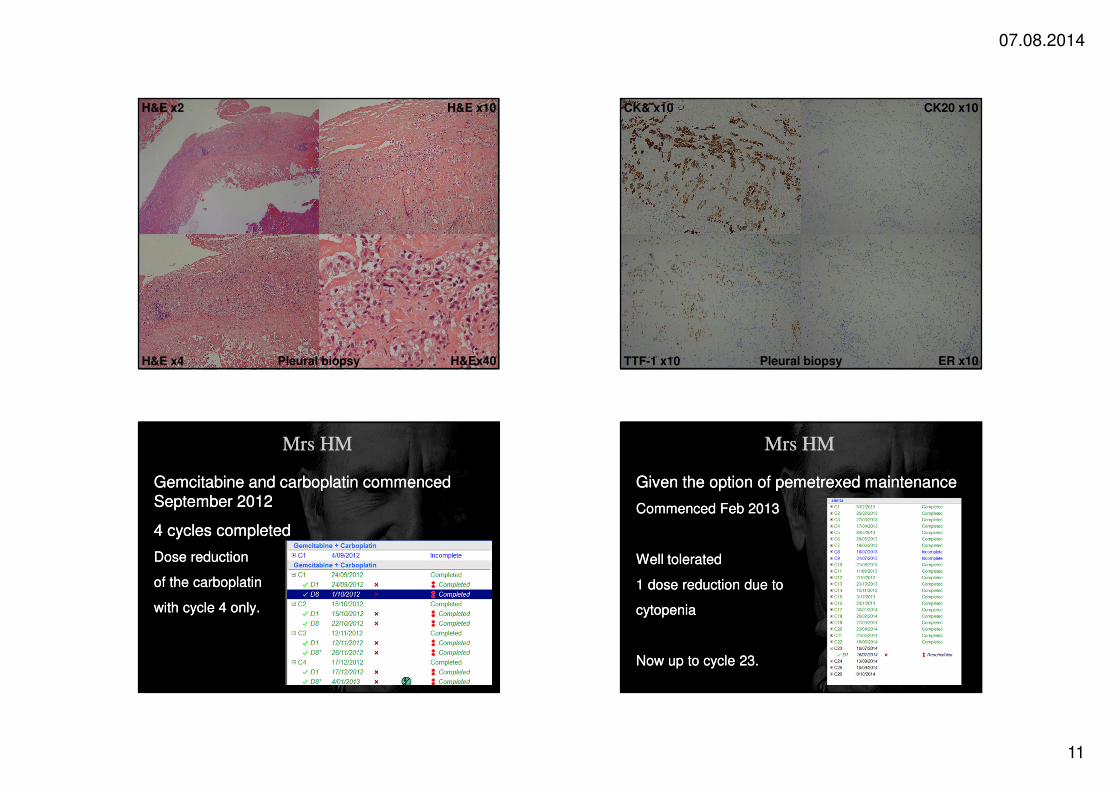
Gemcitabine and carboplatin commenced September 2012
4 cycles completed
Dose reduction
of the carboplatin
with cycle 4 only.
Gemcitabine and carboplatin commenced September 2012
4 cycles completed
Dose reduction
of the carboplatin
with cycle 4 only.
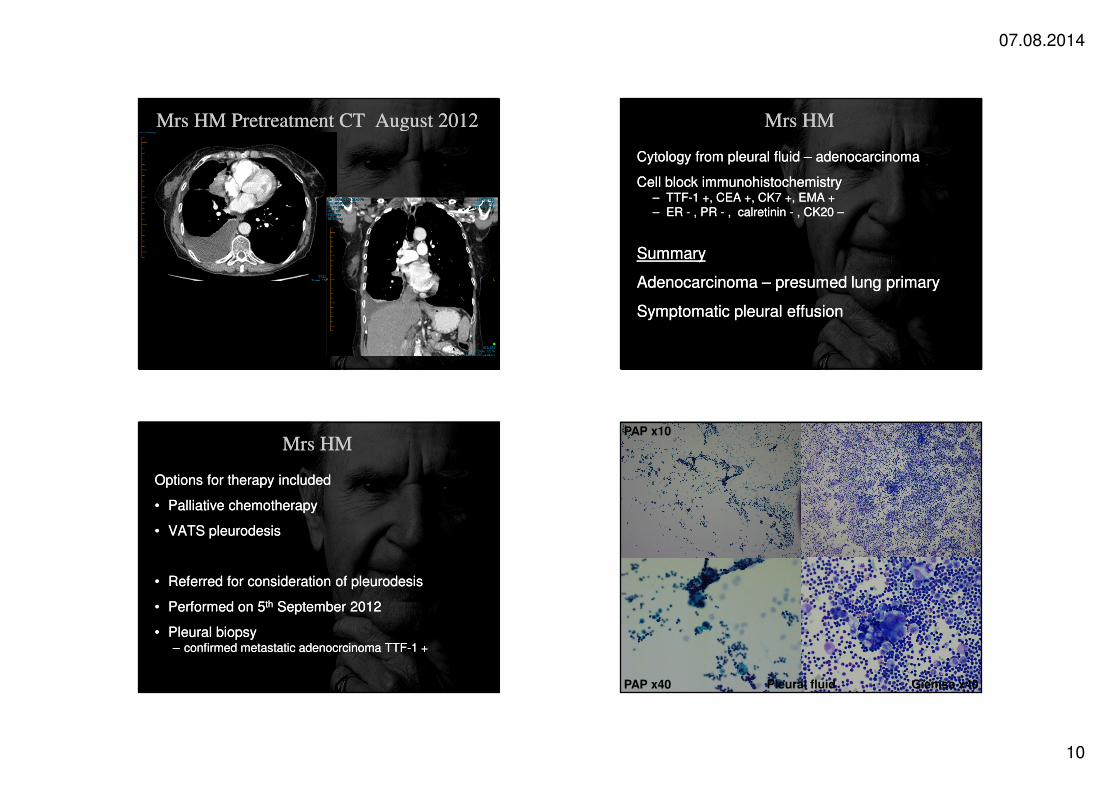
Mrs HMMrs HM
Given the option of pemetrexed maintenance
Commenced Feb 2013
Well tolerated
1 dose reduction due to
cytopenia
Now up to cycle 23.
Given the option of pemetrexed maintenance
Commenced Feb 2013
Well tolerated
1 dose reduction due to
cytopenia
Now up to cycle 23.
07.08.2014
12
Mrs HM - CT June 2014Mrs HM - CT June 2014 Mrs HM - CT June 2014
Assessing patients using the “Rule of Thumb”Assessing patients using the “Rule of Thumb” Assessing patients using the CGA.Assessing patients using the CGA.