60
Cancer in the Older Person: What is Different? Arti Hurria, MD Director, Cancer and Aging Research Program City of Hope Duarte, CA, USA
Cancer in the Older Person:What is Different?
Arti Hurria, MD
Director, Cancer and Aging Research Program
City of Hope
Duarte, CA, USA
Disclosures
Company Role
Celgene PI
Novartis PI
GTx, Inc. Consultant
Boehringer Ingelheim
Pharmaceuticals
Consultant
Carevive (formerly On Q Health) Consultant
Sanofi Consultant

�Demographics of cancer and aging
�Aging and implications for cancer treatment
- What is different?
�Leveraging technology to meld geriatrics &
oncology
�Workforce and educational needs
Outline

The World-Wide Population is Aging2002
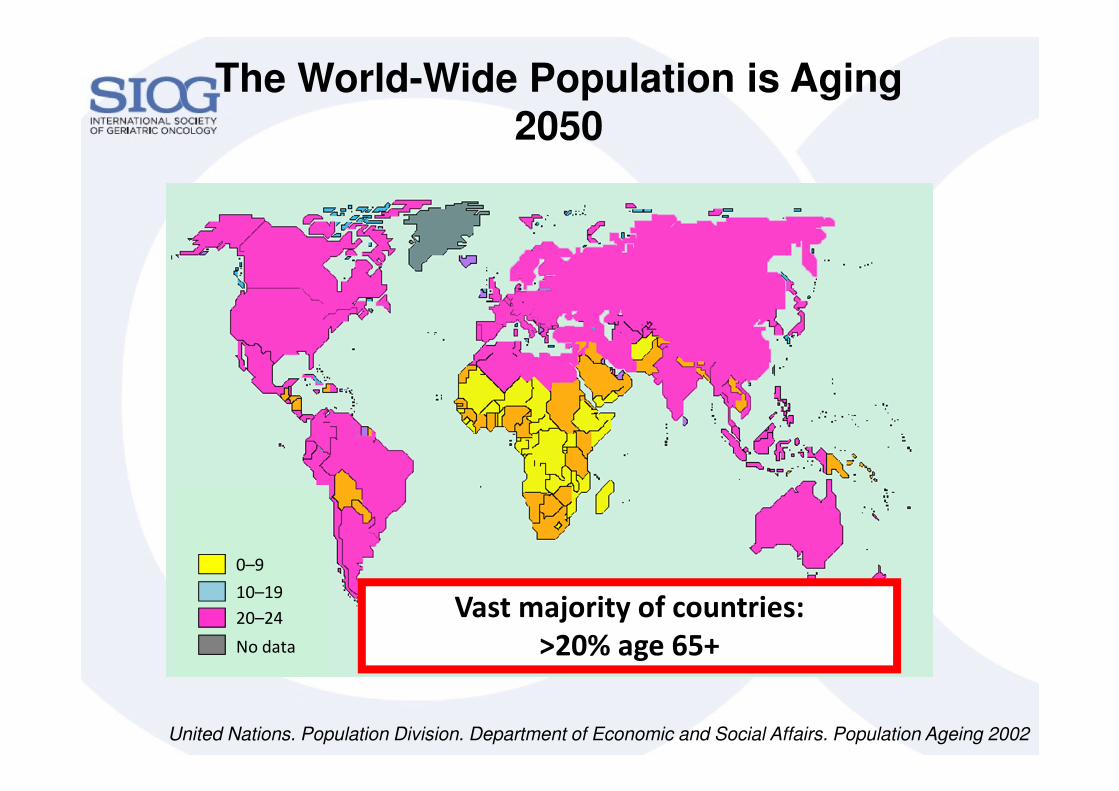
United Nations. Population Division. Department of Economic and Social Affairs. Population Ageing 2002
0–9
10–19
20–24
No data
>20% age 65+
0–9
10–19
20–24
No data
Vast Majority of Countries Age 65+
United Nations. Population Division. Department of Economic and Social Affairs. Population Ageing 2002
0–9
10–19
20–24
No data
Vast majority of countries:
>20% age 65+
The World-Wide Population is Aging2050
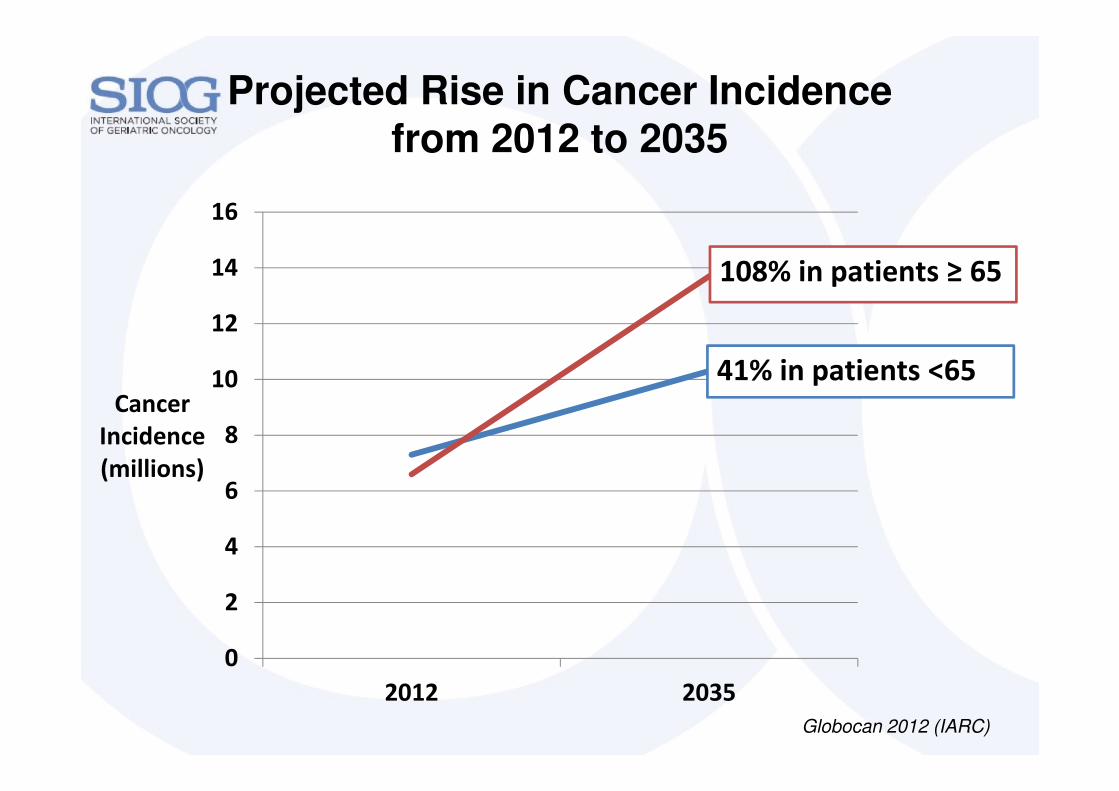
Projected Rise in Cancer Incidence from 2012 to 2035
0
2
4
6
8
10
12
14
16
2012 2035
Cancer
Incidence
(millions)
108% in patients ≥ 65
41% in patients <65
Globocan 2012 (IARC)
Take-Home Message #1: Cancer is a Disease of Aging
What is Different about Older adults?
� The world-wide population is aging
� Majority of cancer diagnosis and death occur
in older adults
� The number of older adults with cancer is
on the rise
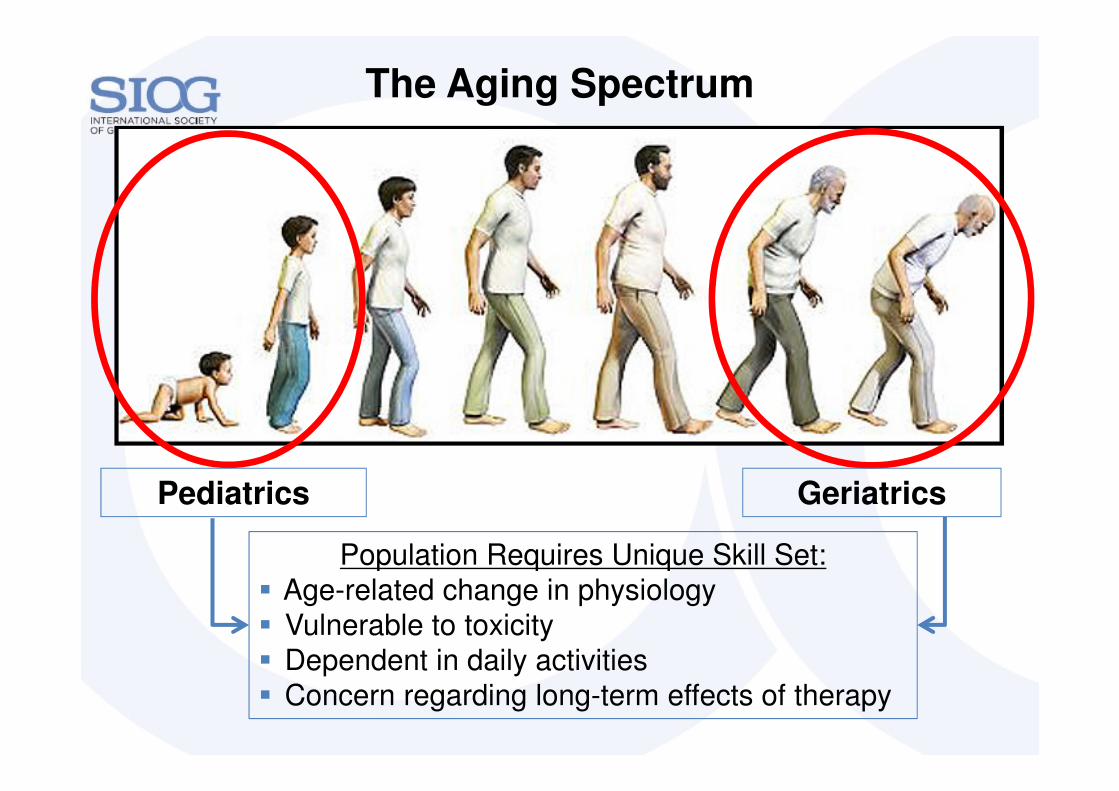
The Aging Spectrum
Pediatrics Geriatrics
Population Requires Unique Skill Set:
� Age-related change in physiology
� Vulnerable to toxicity
� Dependent in daily activities
� Concern regarding long-term effects of therapy

Pediatrics: Chronological Age = Functional Age
www.cdc.gov/ActEarly

Chronological Age 80
Geriatrics: Chronological Age ≠ Functional Age
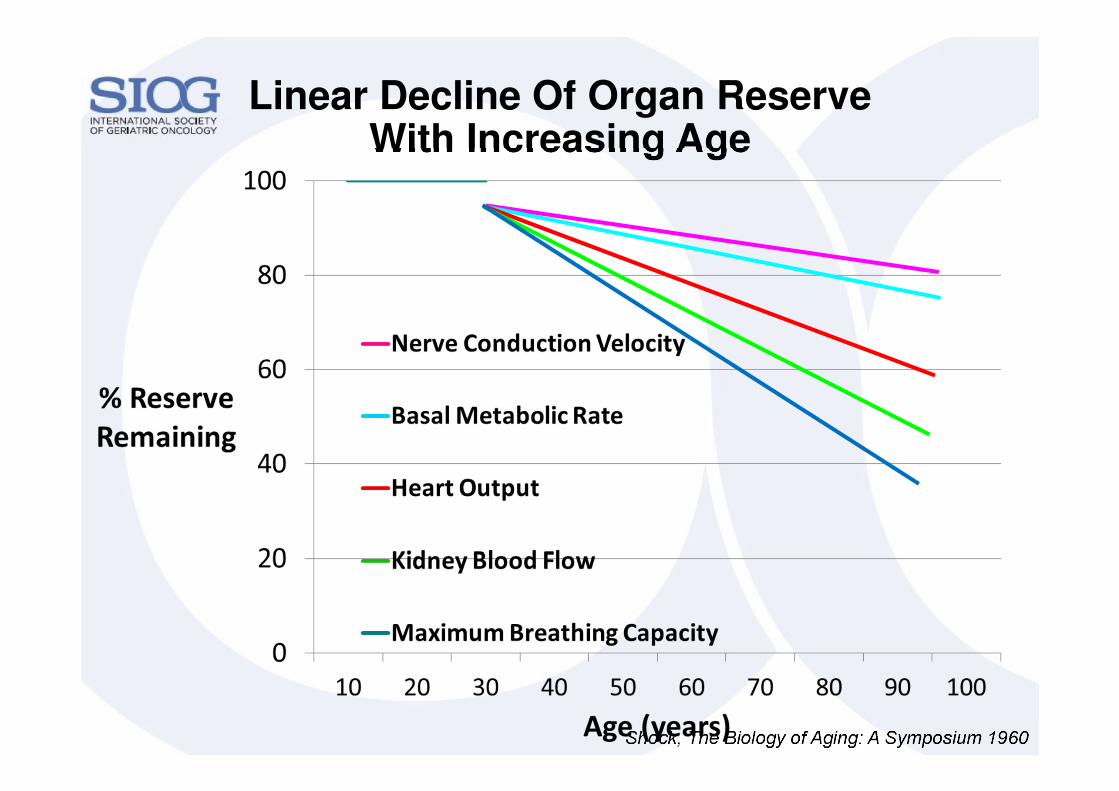
Linear Decline Of Organ Reserve With Increasing Age
Shock, The Biology of Aging: A Symposium 1960
AgeCreatinine
(mg/dL)
CrCl*
(ml/min)
40 1.4
50 1.4
60 1.4
70 1.4
80 1.4
90 1.4
100 1.4
AgeCreatinine
(mg/dL)
CrCl*
(ml/min)
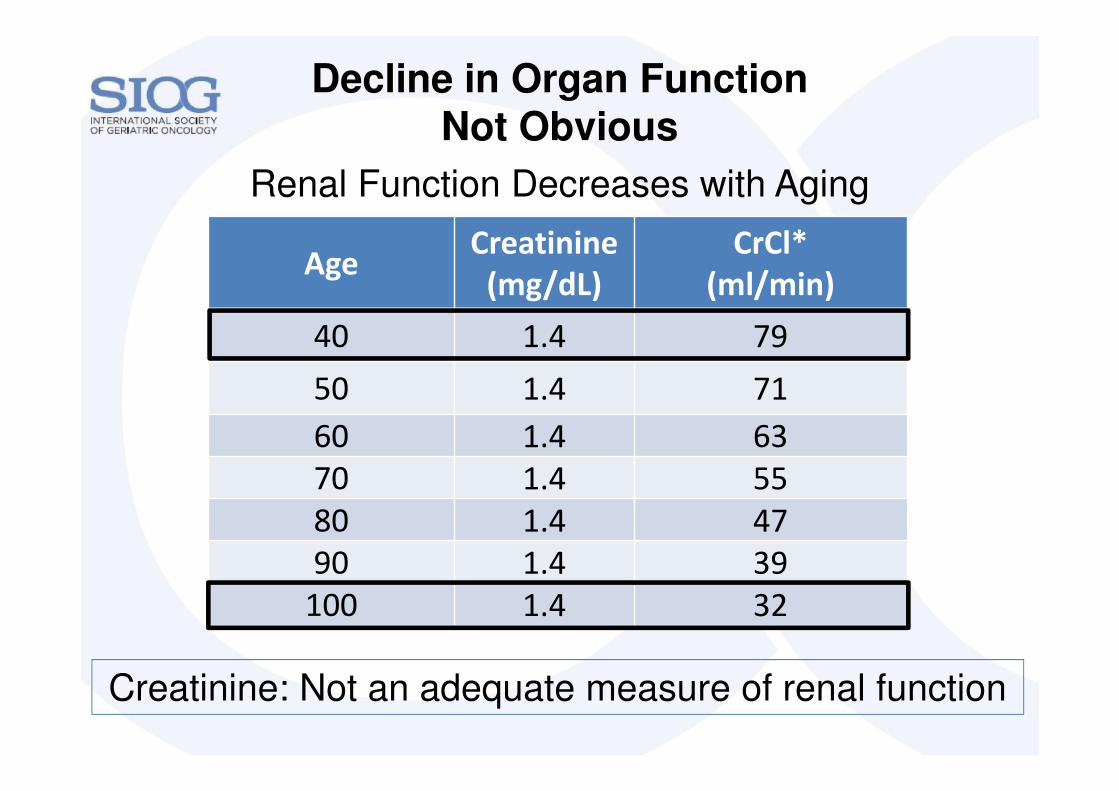
40 1.4 79
50 1.4 71
60 1.4 63
70 1.4 55
80 1.4 47
90 1.4 39
100 1.4 32
Decline in Organ Function Not Obvious
Creatinine: Not an adequate measure of renal function
Renal Function Decreases with Aging
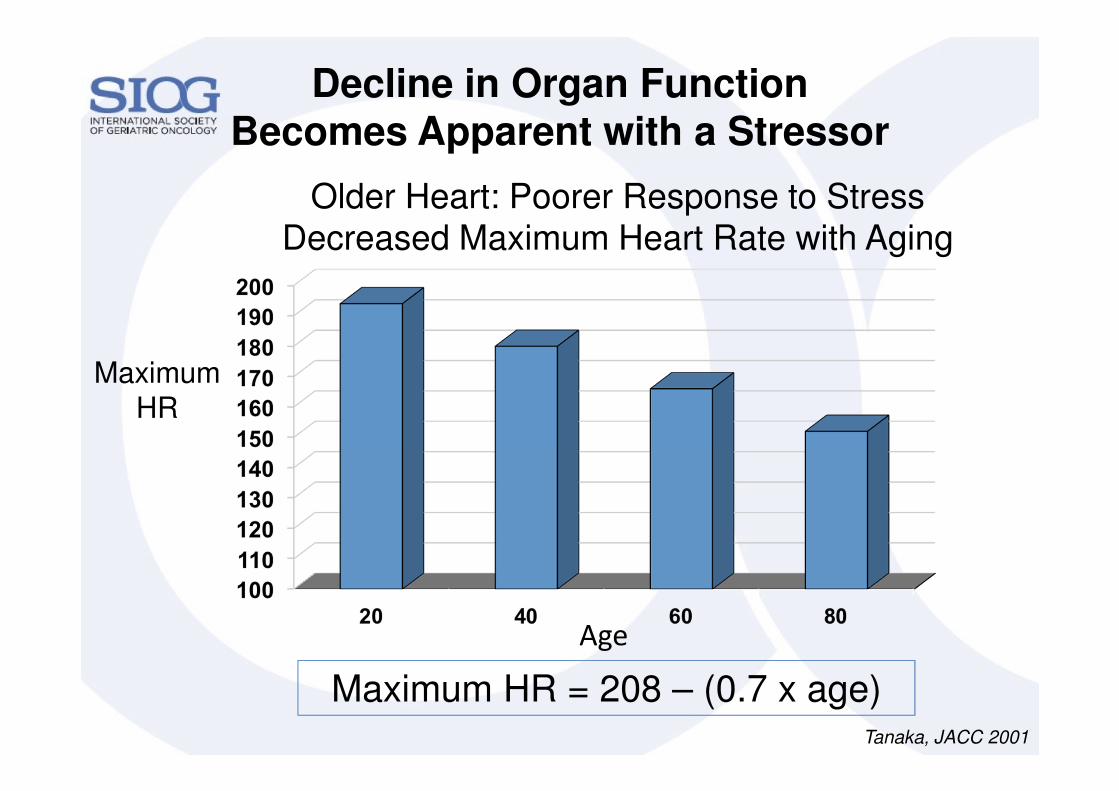
Decline in Organ Function Becomes Apparent with a Stressor
Maximum
HR
Age
Maximum HR = 208 – (0.7 x age)Tanaka, JACC 2001
Older Heart: Poorer Response to Stress Decreased Maximum Heart Rate with Aging
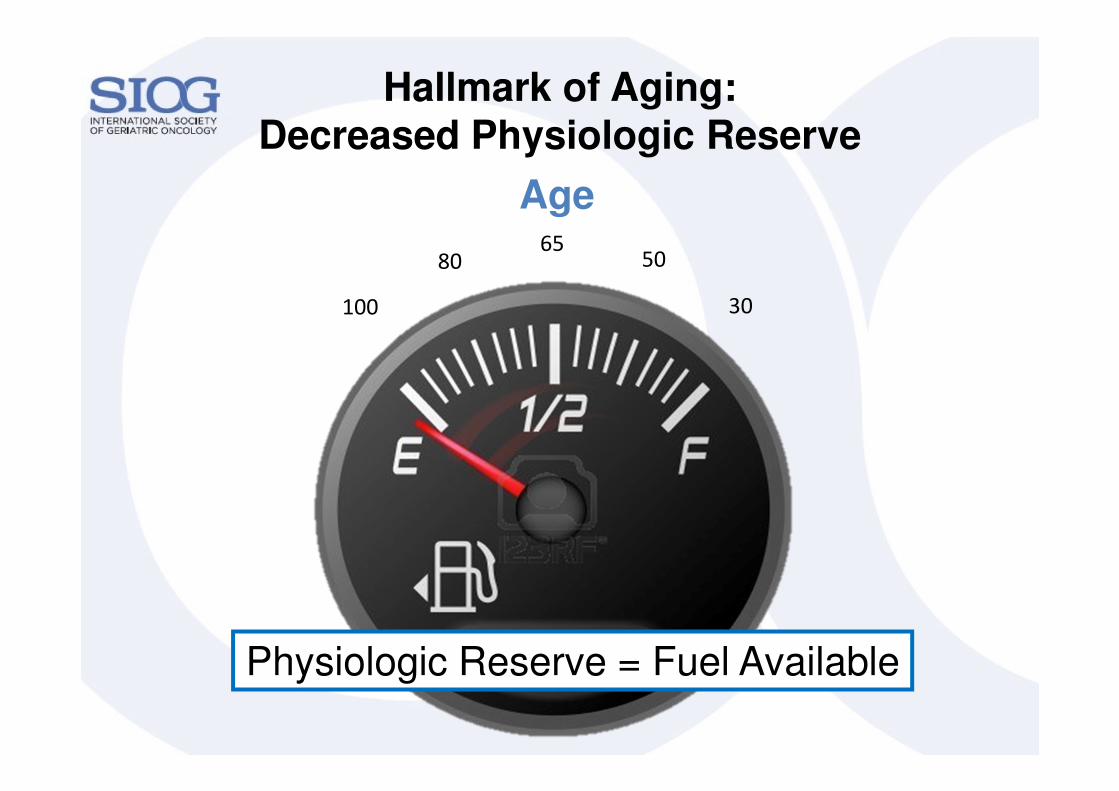
Hallmark of Aging:Decreased Physiologic Reserve
Physiologic Reserve = Fuel Available
Age
30
5065
80
100
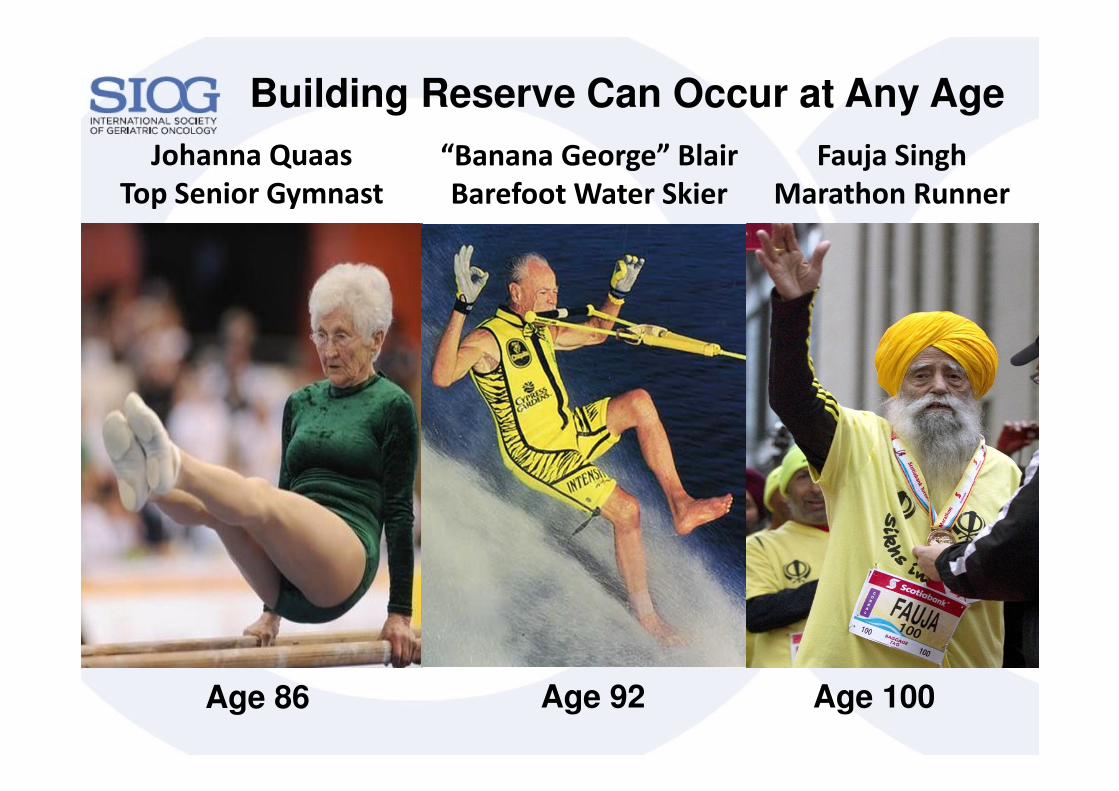
Building Reserve Can Occur at Any Age
“Banana George” Blair
Barefoot Water Skier
Age 92
Fauja Singh
Marathon Runner
Age 100Age 86
Johanna Quaas
Top Senior Gymnast
Take-Home Message #2: Chronological Age ≠ Functional Age
Understanding Physiologic Reserve
� Aging is heterogenous
� The aging trajectory is modifiable
� A hallmark of aging: decline in organ reserve
� May not be obvious at rest
� Becomes apparent with a stressor
Understanding Physiologic Reserve:Integrating Geriatrics into Oncology
� Functional status
� Comorbid medical conditions
� Nutritional status
� Cognition
� Psychological state
� Social support
� Medications (polypharmacy)
Factors other than chronological age that predict
morbidity & mortality in older adults
Geriatric
Assessment
Using Geriatric Assessment in Oncology Practice
to Guide Practical Interventions
Functional Status
Key Questions
� Does my patient need
assistance with daily
activities?
� If my patient gets sick:
� how would they get to the
hospital?
� who will help care for
them at home?
Visiting nurse
Home health aide
Family support
Social work
Family support

Geriatric Assessment: Functional Status
Instrumental Activities of Daily Living
Required to maintain independence in the
community
Shopping
Housekeeping
Transportation
Laundry
Telephone
Finances
Medications
Preservation of functional status is key

Loss of Physical Function Predicts Distress in Older Adults with Cancer
� 250 older adults with cancer completed a geriatric assessment
Hurria et al, JCO 2009
Greatest predictor of distress is impaired physical function
P value = 0.015
Assistance Needed

Assistance with IADLs ���� Worse Survival in Patients with Lung Cancer
Maione et al, J Clin Oncol 2005
Categories of IADLs:
� Better:
Score of 100%
� Intermediate:
Score of 51-99%
� Worse:
Score of 0-50%
Better
Intermediate
Worse
ComorbidityKey Questions
� Will other medical problems impact the ability to
tolerate cancer treatments?
� Can these conditions be optimized prior to
treatment?
� How do these other medical conditions impact life
expectancy?
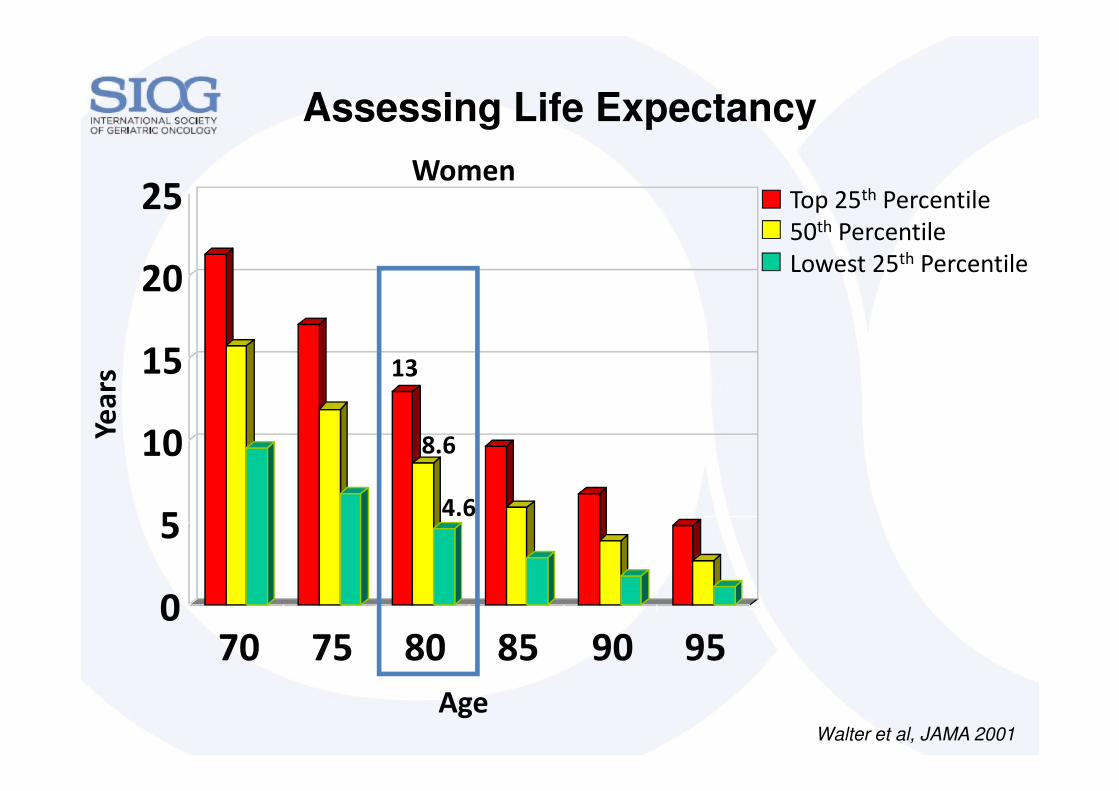
0
5
10
15
20
25
70 75 80 85 90 95
Assessing Life Expectancy
Walter et al, JAMA 2001
Age
Yea
rs
WomenTop 25th Percentile
50th Percentile
Lowest 25th Percentile
13
8.6
4.6
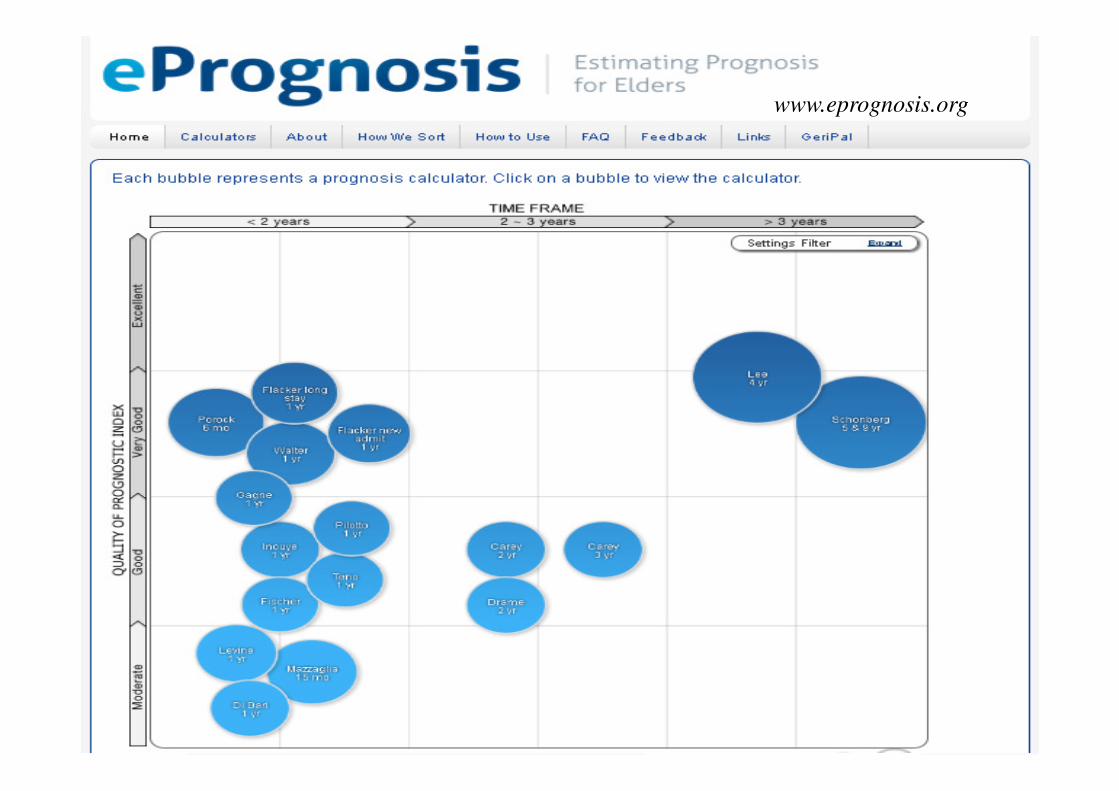
www.eprognosis.org
Nutritional StatusKey Questions
� Does my patient have:
� BMI < 22kg/m2
� unintentional weight loss > 5%
� If my patient gets sick,
� do they have access to food?
Nutritional
consultation
Social work
Family support
Meal on
Wheels

� Can my patient:
� Follow complex directions
� Take medications on schedule
� Recognize toxicity and seek help
Cognitive FunctionKey Questions
Visiting nurse
Family/
Caregiver
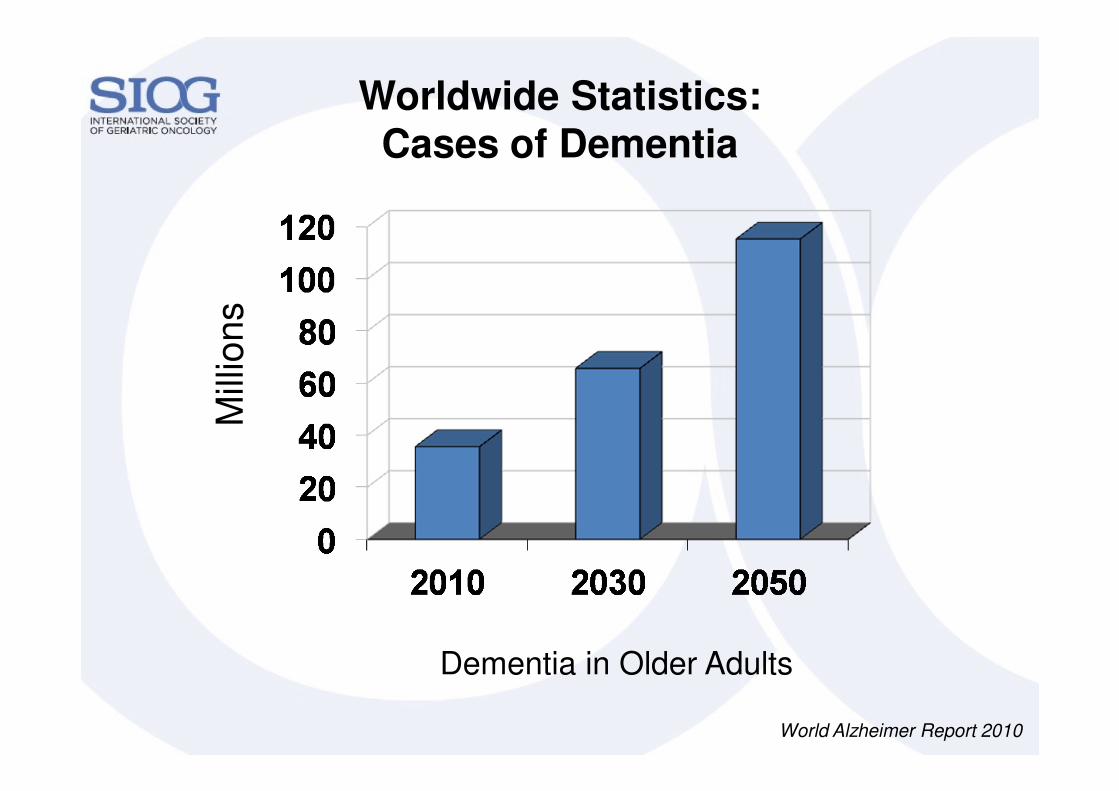
Worldwide Statistics: Cases of Dementia
Mill
ion
s
World Alzheimer Report 2010
Dementia in Older Adults
Four Components to Assessing Capacity
1. Understands the relevant information
2. Appreciate their situation
3. Uses reason to make a decision
4. Communicates their choice
Does the Patient Have Decision Making Capacity?
Sessums et al. JAMA 2011

Psychological Status & Social SupportKey Questions
� Is my patient depressed, anxious,
or distressed?
� Does my patient have a caregiver?
� Is my patient the caregiver for
someone else?
Psychiatry
Social work
Social work
Family

Correlation Between
Social Support & Psychological State
Kornblith et al, Cancer 2001

Who Provides Care for Older Adults with Cancer?
Informal Caregivers(family and friends)
Formal Caregivers(paid)
Family Caregiving Alliance, 2008
80%20%
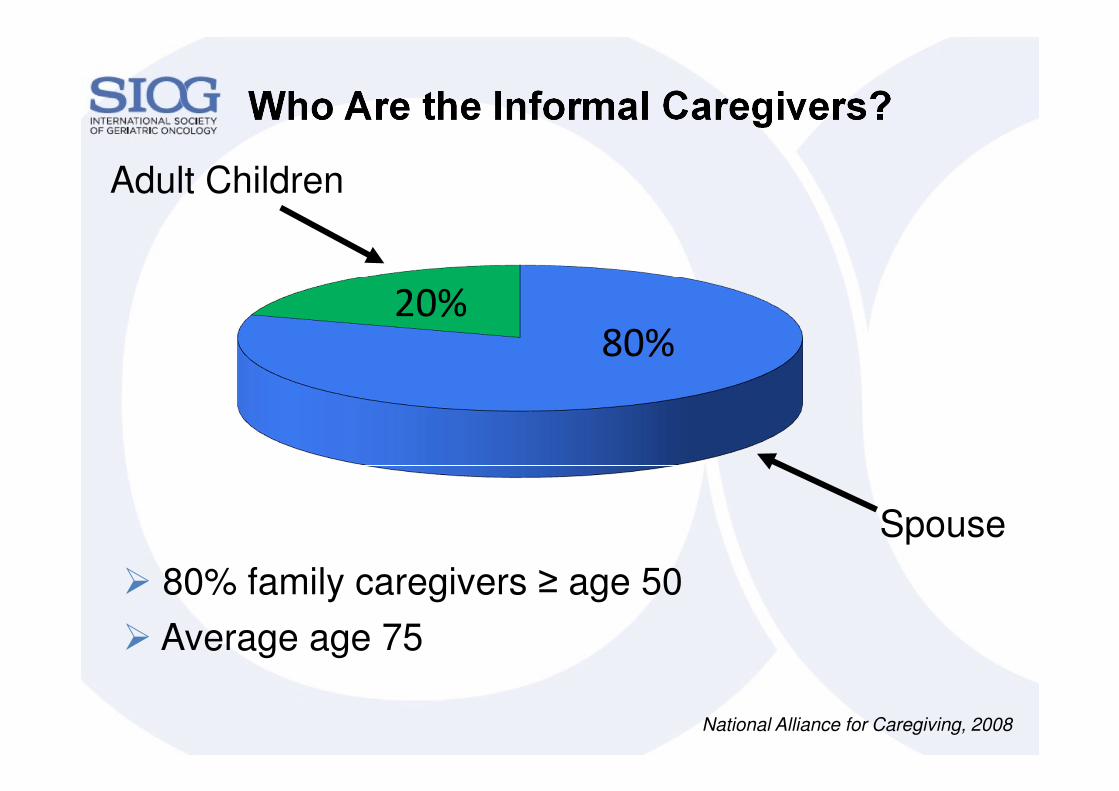
Who Are the Informal Caregivers?
Spouse
Adult Children
� 80% family caregivers ≥ age 50
� Average age 75
National Alliance for Caregiving, 2008
20%80%
� Does my patient take medications
that:
� will interact with the cancer-
directed therapy?
� duplicative or not needed?
� potentially “inappropriate”:
risk of side effects
PolypharmacyKey Questions
Medication
reconciliation
Pharmacist
review
Take-Home Message #3: A Geriatric Assessment Can Identify
Older Adults At Risk
Is it feasible to incorporate these tools into
oncology practice?
� Uncover problems not detected by routine H&P
� Leads to practical interventions
� Predict risk of chemotherapy toxicity
(to be discussed on July 2nd in the Supportive Care session)
� Predict survival of older patients with cancer

Too little time…Too much to do
Development of a Short Geriatric
Assessment Tool for Oncologists

World-Wide Workforce Shortage
� There is a shortage of 7.2 million health-care workers world-
wide today
� In 2035, there will be a shortage of 12.9 million health-care
workers
� Shortages of 2 million across all EU countries by 2020
� <80% healthcare coverage for the population: 57 countries
� Compounding the problem: The health workforce is aging
“A Universal Truth: No Health Without a Workforce”, Global Health Workforce Alliance ReportWorld Health Organization
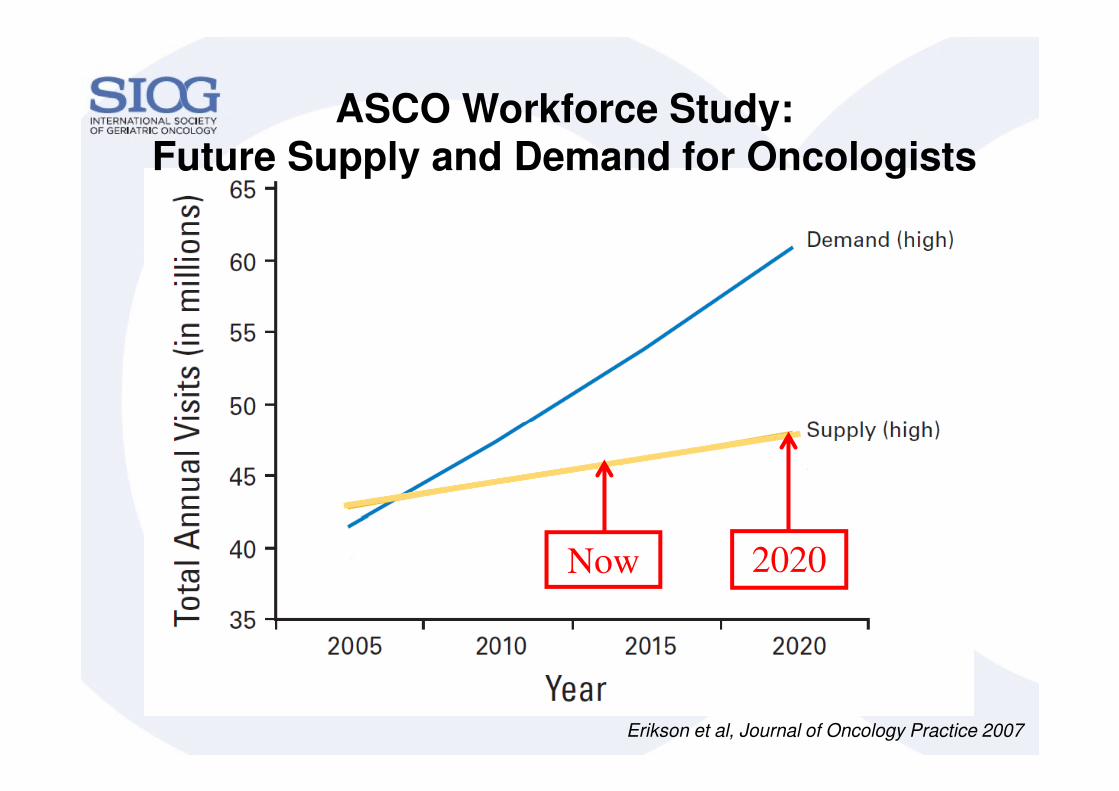
Erikson et al, Journal of Oncology Practice 2007
Now 2020
ASCO Workforce Study:Future Supply and Demand for Oncologists

Year
Anticipated Decline in Geriatricians
American Geriatrics Society:
Geriatrics Workforce Policy Studies Center
2030 Projection:1 Geriatrician : 3,798 Patients


http://www.siog.org/content/comprehensive-geriatric-assessment-cga-older-patient-cancer

Developing a Geriatric Assessment for Oncologists
• Functional Status:Activities of Daily Living (subscale of MOS Physical Health)
Instrumental Activities of Daily Living (subscale of the OARS)
Karnofsky Performance Rating Scale
Timed Up & Go
Number of Falls in Last 6 Months
• Comorbidity: Physical Health Section (subscale of the OARS)
• Cognition: Blessed Orientation-Memory-Concentration Test
• Psychological: Hospital Anxiety and Depression Scale
• Social Functioning: MOS Social Activity Limitations Measure
• Social Support:MOS Social Support Survey: Emotional and Tangible Subscales
Seeman and Berkman Social Ties
• Nutrition:Body Mass Index
% Unintentional Weight Loss in the Last 6 Months
- Validity
- Reliability
- Length
- Time to complete
- Ability to self-
administer
- Multidisciplinary
input
- Alliance Cancer in
Elderly Committee
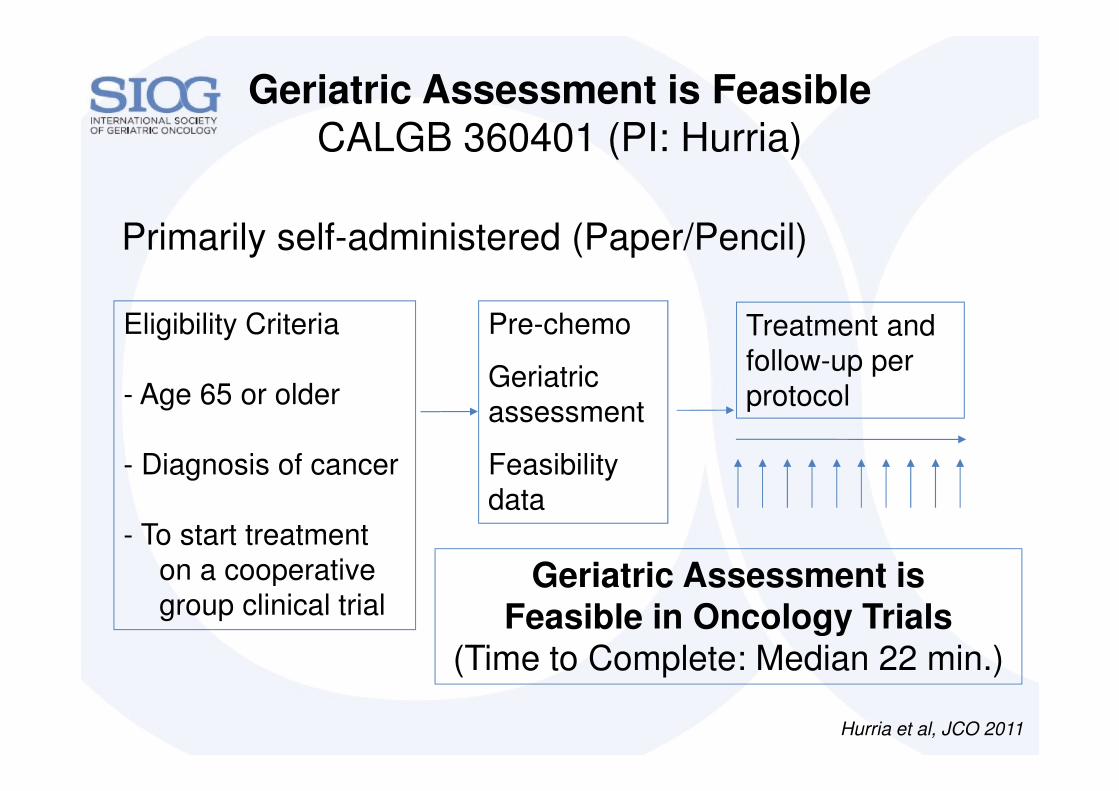
Geriatric Assessment is Feasible CALGB 360401 (PI: Hurria)
Pre-chemo
Geriatric
assessment
Feasibility
data
Eligibility Criteria
- Age 65 or older
- Diagnosis of cancer
- To start treatment
on a cooperative
group clinical trial
Treatment and
follow-up per
protocol
Geriatric Assessment is Feasible in Oncology Trials
(Time to Complete: Median 22 min.)
Hurria et al, JCO 2011
Primarily self-administered (Paper/Pencil)

Geriatric Assessment Questions are Acceptable to Patients
87% Completed patientquestionnaire w/o assistance
95% Easy to comprehend96% Not upsetting
92% Length is ““““Just Right””””
94% Completed healthcare provider portion
Hurria et al, JCO 2011
94%
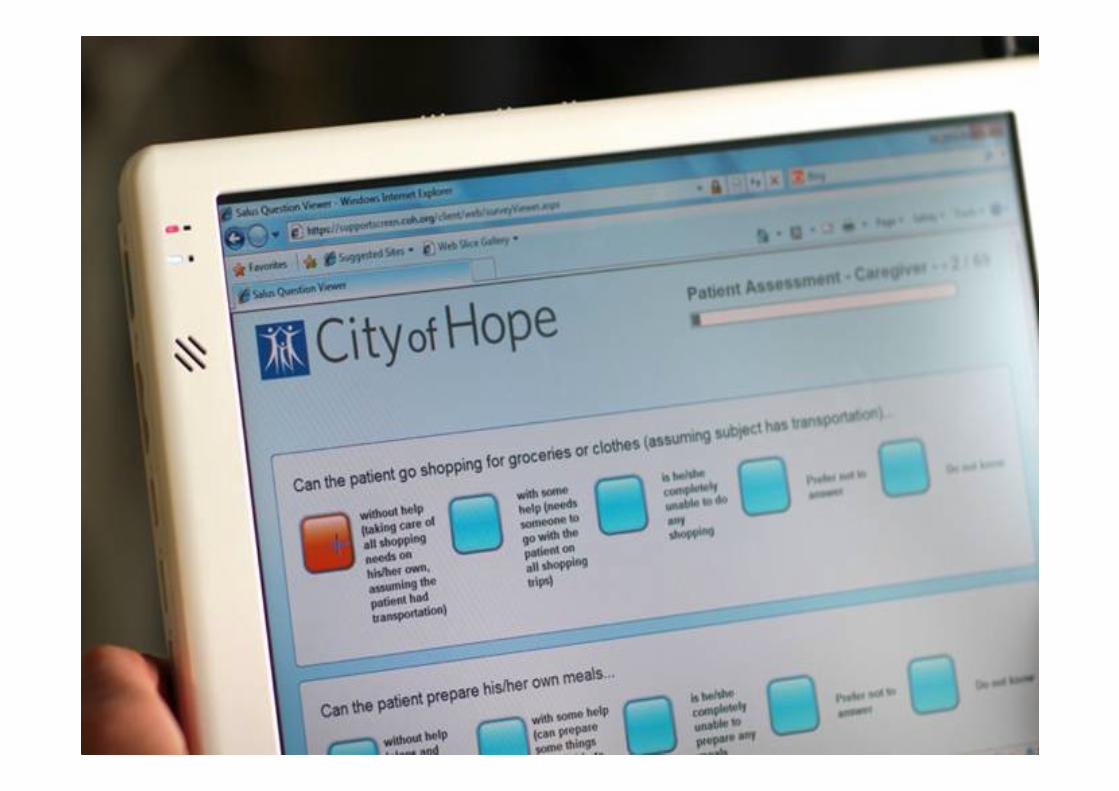
Utilizing Technology to Capture Geriatric Assessment
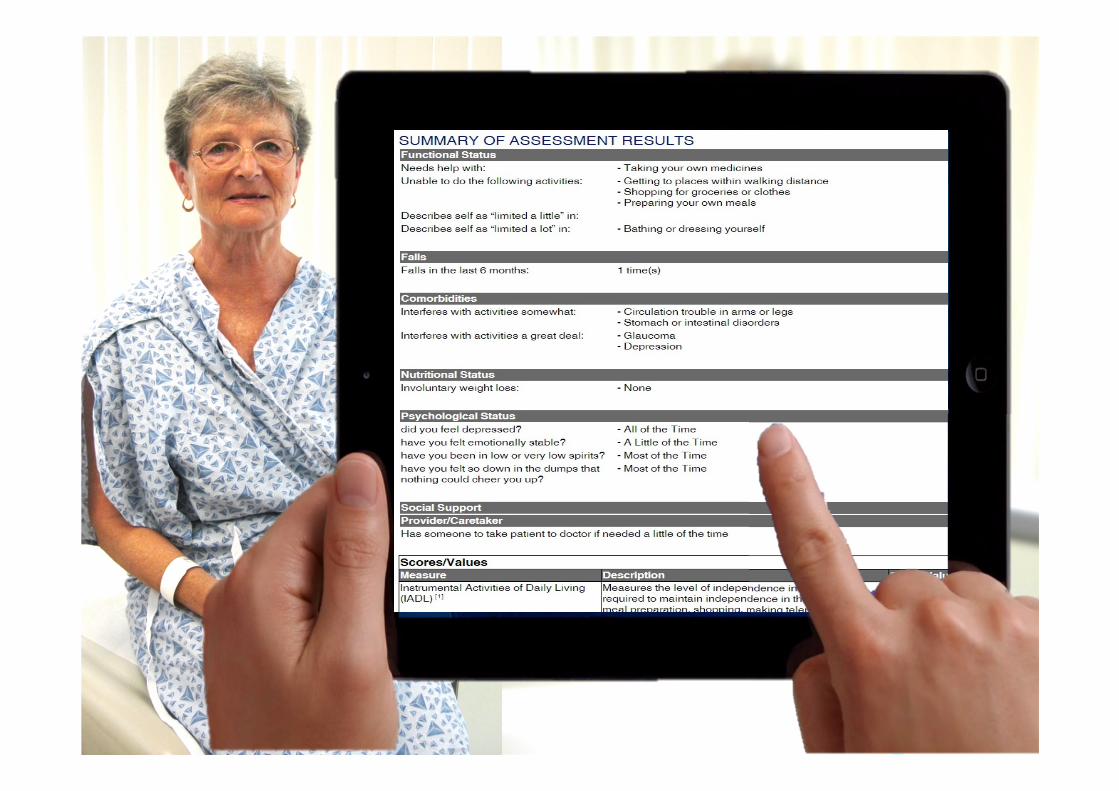

Where to get a CGA?
Geriatric Assessment Tool available in English, Spanish, & Mandarin
• Geriatric Assessment (Patient)
• Geriatric Assessment(Healthcare Team )
Cancer and Aging Research Group
www.MyCARG.org

Take-Home Message #4: Technology can be Utilized to
Integrate Geriatrics & Oncology Care
� Geriatric assessment is feasible in oncology
� Utilize technology to:
� Capture the geriatric assessment
� Pinpoint areas of vulnerability and intervene

“…to meet the healthcare needs of thenext generation of older adults,
the geriatric competence of the entire workforce needs to be enhanced…
innovative models need to be developed and implemented…”
Retooling for an Aging America:Institute of Medicine Report

Workforce Shortage:
Evolving Models of Care
Patient
Physician
Pharmacist
Home Care
Aides
Social Work
Principles of Geriatrics: Multidisciplinary Care
Physician
Assistants
Rehab
Family/
Caregivers
Nurses
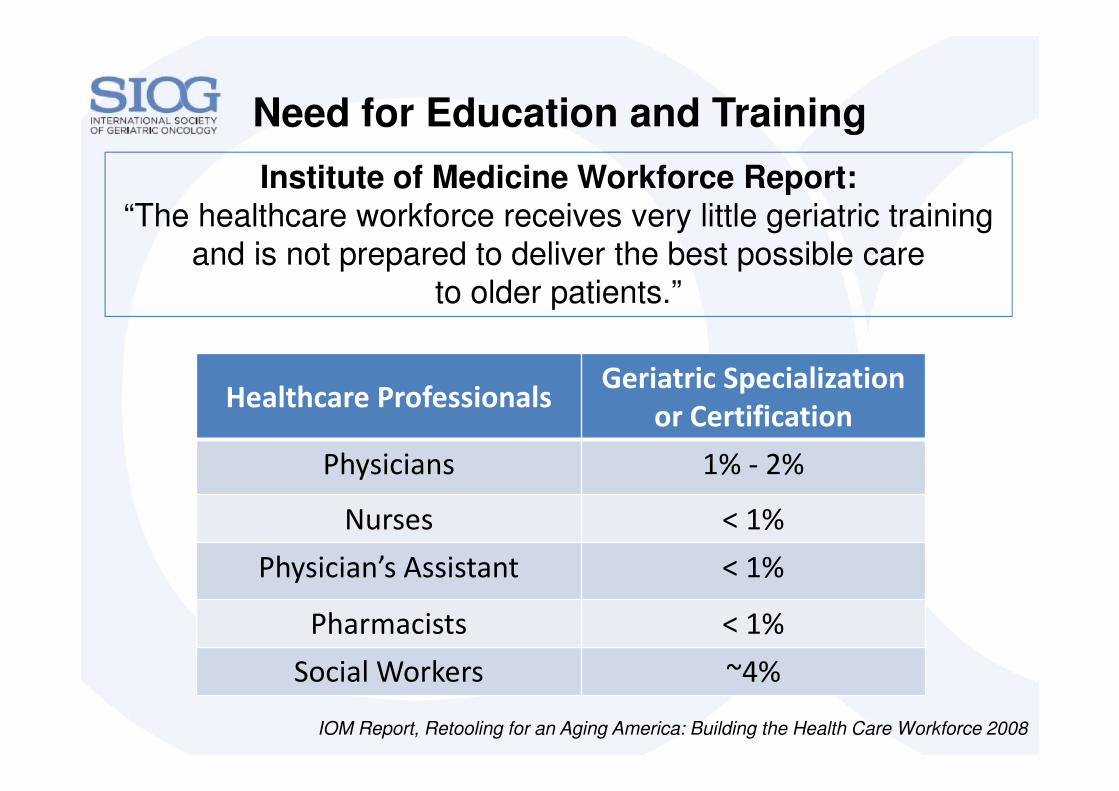
Institute of Medicine Workforce Report:“The healthcare workforce receives very little geriatric training
and is not prepared to deliver the best possible care
to older patients.”
Need for Education and Training
Healthcare ProfessionalsGeriatric Specialization
or Certification
Physicians 1% - 2%
Nurses < 1%
Physician’s Assistant < 1%
Pharmacists < 1%
Social Workers ~4%
IOM Report, Retooling for an Aging America: Building the Health Care Workforce 2008
The IOM report calls for a
“substantial focus” in our
healthcare infrastructure to provide
skilled care to this vulnerable population
Who sets the bar for
education and training?
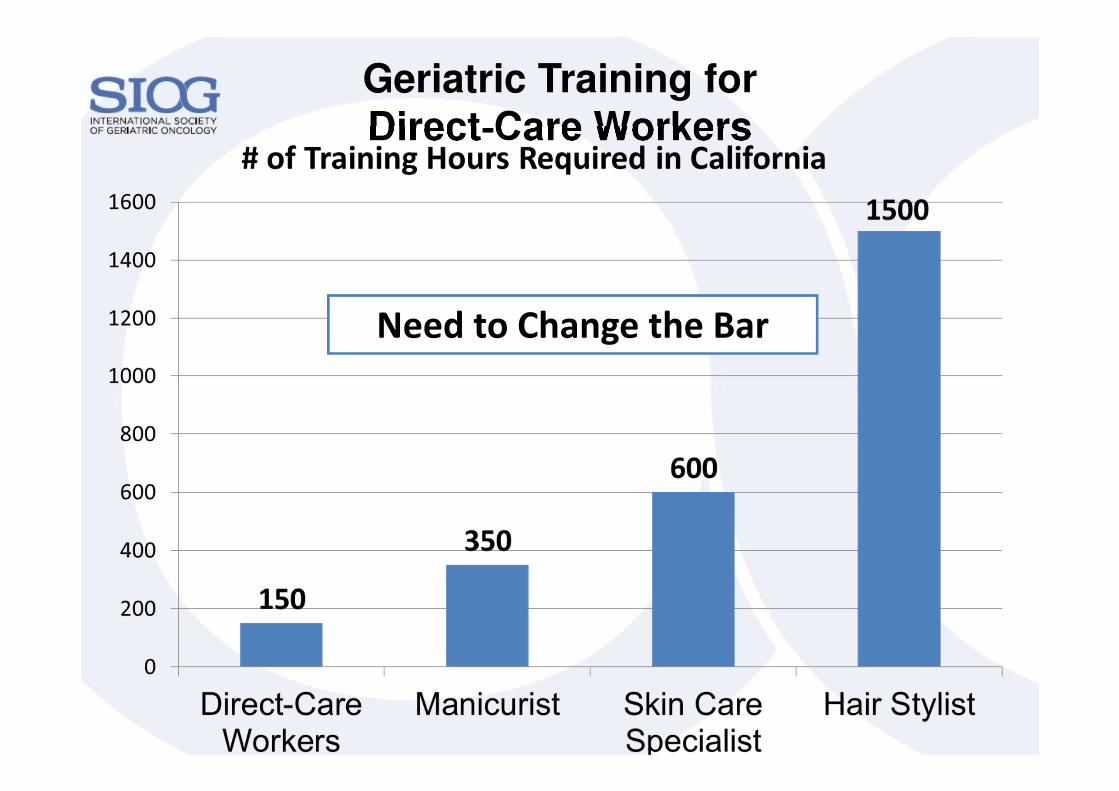
Geriatric Training for Direct-Care Workers
Need to Change the Bar

Educating Nurses in Geriatric Oncology to Improve Quality Care
� Educate 400 nurses from across the nation in caring for
older adults with cancer
� “Train the trainer”
� Geriatric oncology initiatives at their own institution
� Follow-up with participants 6, 12, and 18 months post-
course
� Monthly conference calls
Delivering High-Quality Cancer Care:Institute of Medicine Report
“A system that provides competent, trusted,
interprofessional cancer care teams that are
aligned with patients’ needs, values, and
preferences, as well as coordinated with the
patients’ noncancer care teams and their
caregivers”
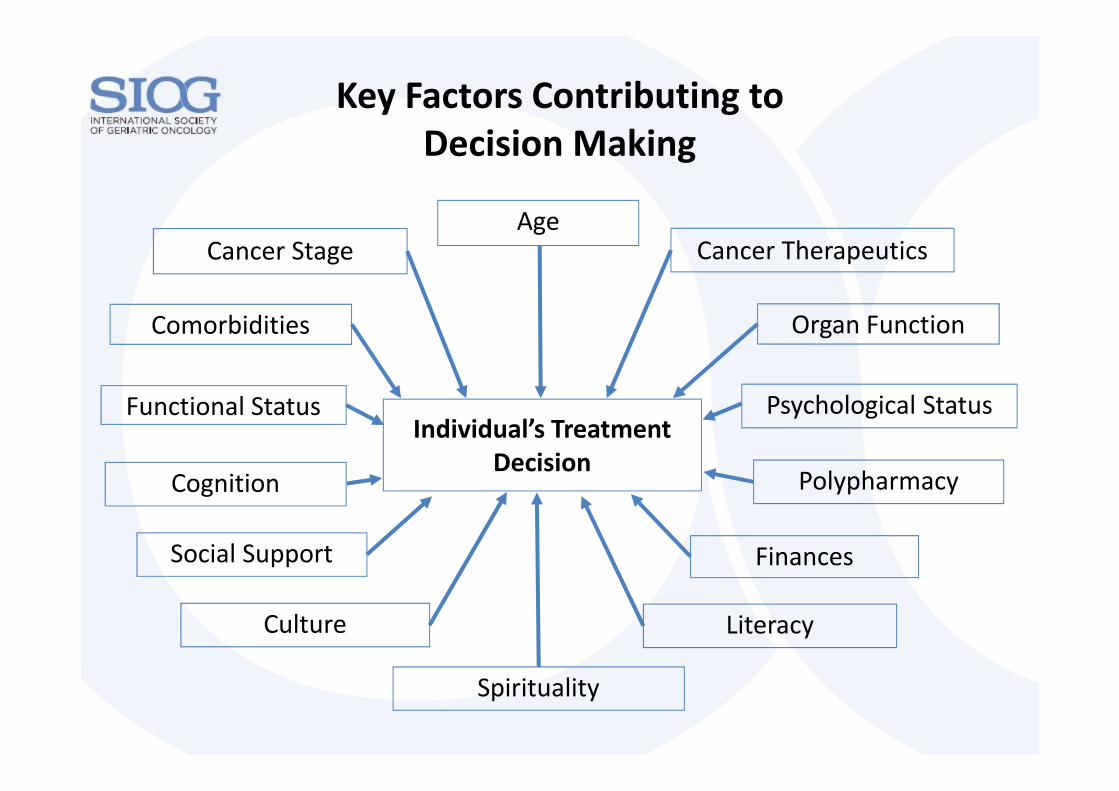
Functional Status
Comorbidities
Key Factors Contributing to
Decision Making
Finances
Age
Individual’s Treatment
Decision
Cancer Stage
Psychological Status
Cancer Therapeutics
Organ Function
Cognition
Spirituality
Polypharmacy
Social Support
Culture Literacy
Take-Home Messages
� Cancer is a disease of aging
� The number of older adults with cancer is on the rise
� Several unique considerations in caring for older adults
� Decline in organ function
� Chronological age ≠ Functional age
� A geriatric assessment can identify older adults at risk
� Treatment must be individualized
� There is a workforce shortage
� Evolving models of care
� Education in geriatrics is needed
� Utilize technology to integrate geriatrics & oncology

Aging begins from the minute we are born.
Geriatrics
Oncology
Geriatric Oncology
Thank you!

















