60
Cancer Services Co-ordinating Group Significant Events Audit of Lung Cancer in Primary Care October 2010

Cancer Services Co-ordinating Group Significant Events Audit of Lung Cancer in
Primary Care
October 2010

2
PROJECT TEAM
Dr Richard D Neal Senior Lecturer in General Practice Department of Primary Care and Public Health Cardiff University, North Wales Clinical School, Wrexham Email: [email protected] Dr Iain J Robbé Clinical Senior Lecturer & Honorary Consultant Department of Primary Care & Public Health Cardiff University School of Medicine, Cardiff Email: [email protected] Professor Malcolm Lewis Chairman of COGPED Director Postgraduate Education for General Practice School of Postgraduate Medical and Dental Education Cardiff University, Cardiff Email: [email protected] Dr Ian Williamson Consultant Chest Physician Chair of the Cancer Services Coordinating Group Lung Cancer Advisory Group Cancer Services Co-ordinating Group, Cardiff Email: [email protected] Dr Jane Hanson Director, Cancer Services Coordinating Group Lead Adviser for Cancer and Cancer Services to the Welsh Assembly Government Cancer Services Co-ordinating Group, Cardiff Email: [email protected] 1. The project was funded by the Cancer Services Co-ordinating Group (CSCG) as part of the work
of the all Wales Lung Cancer Advisory Group. The work involved a partnership between the
CSCG, the Deanery, Cardiff University, and the North Wales Clinical School.
2. This is a technical report providing detailed analysis and recommendations for health
professionals, and is not intended as a report for a non-health professional audience.
3. We would like to thank the general practices that participated in this study. In particular we would
like to acknowledge the support from the regional cancer network directors, Damian Heron (North
Wales), Glynis Tranter (South West Wales), Hywel Morgan (South East Wales) and the general
practitioner (GP) leads namely Dr Rhys Davies (North Wales), Dr Bridget Gwynne and Ms Janet
John (South West Wales), and Drs Liam Taylor and Mark Smithies (South East Wales). We would
also like to thank Professor Greg Rubin from the Centre for Integrated Health Research,
University of Durham for advice on the preparation for this project.
3
CONTENTS
PROJECT TEAM .................................................................................................................................... 2
EXECUTIVE SUMMARY ........................................................................................................................ 5
Recommendations .............................................................................................................................. 6
INTRODUCTION ..................................................................................................................................... 7
METHODOLOGY .................................................................................................................................... 8
Ethical Considerations ........................................................................................................................ 8
Data Collection .................................................................................................................................... 8
Definitions, Management of Data, and Analysis ................................................................................. 8
Date of first presentation and duration of symptoms prior to first presentation .............................. 8
Presenting symptoms ...................................................................................................................... 9
Number of consultations prior to referral or investigation ............................................................... 9
Date of request of first GP initiated chest x-ray and date report received ...................................... 9
Referrals and admissions .............................................................................................................. 10
Date of diagnosis .......................................................................................................................... 10
Diagnostic pathways ..................................................................................................................... 10
Time intervals to diagnosis ............................................................................................................ 11
FINDINGS ............................................................................................................................................. 12
Practice characteristics ..................................................................................................................... 13
Age at diagnosis ................................................................................................................................ 13
Symptoms ......................................................................................................................................... 14
Number of consultations prior to referral or admission or investigation ............................................ 14
Chest X-Rays .................................................................................................................................... 16
Routes of referral or admission ......................................................................................................... 16
Diagnostic pathways ......................................................................................................................... 17
Time intervals in diagnostic pathway ................................................................................................ 17
Qualitative analysis of the diagnostic journey ................................................................................... 19
Response of GPs to symptoms ..................................................................................................... 19
Patients‟ responsibility for delaying the diagnostic process .......................................................... 20
Secondary Care responsibility for delaying the diagnostic process .............................................. 20
WHAT WAS LEARNED AND CHANGED BY THE SIGNIFICANT EVENTS AUDIT (SEA) AND WHAT
WAS EFFECTIVE ABOUT IT?.............................................................................................................. 21
What has been learned? ................................................................................................................... 21
Making the diagnosis .................................................................................................................... 21
Process & communication ............................................................................................................. 21
Specific to the ongoing care of an individual patient ..................................................................... 22
What has been changed? ................................................................................................................. 22
Diagnosis ....................................................................................................................................... 22
Process ......................................................................................................................................... 22

4
Prevention ..................................................................................................................................... 22
What was effective about this SEA? ................................................................................................. 23
DISCUSSION ........................................................................................................................................ 24
Methodology ...................................................................................................................................... 24
Summary of main findings and contextualising within the literature ................................................. 24
Sample of patients ........................................................................................................................ 24
Sample of practices ....................................................................................................................... 24
Presenting symptoms .................................................................................................................... 25
Chest x-rays and normal chest x-rays .......................................................................................... 25
Diagnostic pathways and referrals ................................................................................................ 25
Time intervals in the diagnostic pathway ...................................................................................... 25
Qualitative data ............................................................................................................................. 25
REFERENCES ...................................................................................................................................... 27
APPENDIX 1 – GP Invitation Letter ...................................................................................................... 28
APPENDIX 2 – Audit Template ............................................................................................................. 30
APPENDIX 3 – Guidelines for Completion ........................................................................................... 33
APPENDIX 4 – Description of Cases .................................................................................................... 35
APPENDIX 5 – What Was Learned and Changed by the Significant Events Audit and What Was
Effective About It? ................................................................................................................................. 41

5
EXECUTIVE SUMMARY
I. The main objective of this work was to support general practices in a review of their most
recent patient diagnosed with lung cancer from the point of initial presentation to diagnosis
with the outcome of a better understanding of circumstances around diagnosis and referral to
secondary care.
II. All general practices in Wales were contacted and invited to take part in the audit in January
2010. Participating GPs were asked to complete an electronic audit template. The audit
template asked GPs to provide information on the following questions regarding lung cancer
diagnosis: what happened; why did it happen; what has been learned; what has been
changed; and what was effective about this SEA. Audit reports were received for 118
patients.
III. The main findings were:
a. Of the 118 patients audited, 79 [66.9%] had a GP initiated chest x-ray prior to
diagnosis. The longest time from request to report was 24 days. A number of patients
had chest x-rays that did not initially show suspicion of lung cancer: 8 were reported
as normal; 3 reported no change in a pre-existing abnormality; 2 reported other
changes, but with no suspicion of lung cancer; 1 reported a more conspicuous
shadow; 9 reported probable infection and a „treat and repeat x-ray‟.
b. The majority of patients were diagnosed after a GP initiated referral to a chest
physician. In total 10 patients were diagnosed after referral to another specialty, and
25 were diagnosed after a GP initiated acute admission. Of the 87 patients for whom
time from first presentation to referral or admission was measurable, 34 had a
duration of >31 days.
c. For a large number of patients, the response of the GP to the presented symptoms
was exemplary i.e. there was an appropriate response to presented suspicious
symptoms, in line with current NICE guidance. For a smaller number of patients it
was clear that there were opportunities to consider an earlier chest x-ray because of
symptoms. At least 10 atypical presentations were reported that did not lead any of
the clinicians involved to consider lung cancer as a diagnosis. There were a variety of
complex presentations and pathways, with a number of factors relating to the patient,
their symptoms and their pathways.
d. A small number of reports (8) showed that patients either neglected to present
symptoms or failed to attend for diagnostic tests.

6
e. A small number of reports (6) included details of diagnostic delays in secondary care
including: indecision between specialists; non-prioritisation of „urgent‟ GP referrals;
initial misdiagnosis; technical difficulties in the diagnosis; and „bouncing‟ of an urgent
referral.
IV. The SEA process meant that GPs learned much about improving their lung cancer diagnoses,
and about the diagnostic process and communication around this. The process led to
significant changes in the diagnostic process, and was felt to be a very valuable tool, with
many additional benefits.
Recommendations
LHBs and general practitioners need to work towards a focus of reducing the time from first
symptomatic presentation to diagnosis in lung cancer. A further SEA on lung cancer diagnosis should
be undertaken in the future.
LHBs must ensure that:
1. General Practitioners:
a. assiduously adhere to the NICE guidance relating to lung cancer diagnosis;
b. either refer or request further imaging for patients with suspicious symptoms and a
normal chest x-ray;
c. develop a robust process to ensure that all chest x-rays which need repeating are
followed-up.
2. Radiologists rapidly report chest x-rays and direct referrals of abnormal chest x-rays to lung
cancer Multi Disciplinary Teams (MDTs) or for further imaging.
3. Ongoing education for GPs and non-clinical specialists needs to cover awareness of the
significance of both respiratory and non-respiratory symptoms.
4. Respiratory physicians diagnostic processes are as rapid as possible and that findings are
communicated to the patient and their GP.
7
INTRODUCTION
1. In Wales, lung cancer was the second most common cancer in males and females for the 3 year
diagnosis period 2005-2007, with Scotland having the highest incidence rate for both sexes, and
Wales, Northern Ireland and England comparable with the UK average. [Office for National
Statistics, 2010] This statistic demonstrates the seriousness of lung cancer within Wales, and
highlights the benefit to be gained from further understanding of this disease.
2. In 2008-2009, as part of the National Awareness and Early Diagnosis Initiative (NAEDI) in
England, the North of England Cancer Network [NECN] studied cancer in primary care using
significant event methodology. In recognition of the fact that the majority of lung cancer patients
enter the healthcare system through contact with their GP, it was appropriate to undertake a
Significant Events Audit (SEA), a tool already commonly utilised by GPs and described in more
detail in the NAEDI report [Mitchell et al, 2009]. A significant event can be applied to any aspect of
healthcare and can be applied equally to either a good or bad event. In relation to this study the
„significant event‟ was simply a diagnosis of lung cancer.
3. The main objective of this work was to support general practices in a review of their most recent
patient diagnosed with lung cancer from the point of initial presentation to diagnosis with the
outcome of a better understanding of circumstances around diagnosis and referral to secondary
care. A secondary analysis, using the analytical framework described by Mitchell et al [2009] was
undertaken to identify the main findings and make recommendations at an all Wales level. The
project team viewed this as an effective way to support GPs in a learning environment that would
lead to further joint work with local lung cancer MDTs to ensure an effective, prompt referral
process and improved communication if necessary between primary and secondary care.
8
METHODOLOGY
Ethical Considerations
4. In England, the National Research Ethics Service has advised that SEA for cancer is considered
a service audit, providing secondary analysis for GPs and does not require ethical review. This
was also the view of the Post Graduate Dean of Primary Care. All audit forms were handled via
the CSCG central office and coded to ensure anonymity.
Data Collection
5. In January 2010, all 486 general practices in Wales were contacted [Appendix 1] and invited to
take part in the audit, with practices being asked to register their interest by the beginning of
February 2010. The project was set up to manage a maximum SEA of 200. To support a pan
Wales approach, each regional cancer network was invited to support the audit through its GP
leads who were kept informed of the percentage of registrations per Local Health Board (LHB).
6. Participating GPs were asked to complete an electronic audit template regarding the most recent
diagnosis of lung cancer in the practice. The percentage uptake for each individual Health Board,
compared with the places allocated for the Audit, are detailed in Table 1. Midway through the
recruitment process, participating GPs were offered the opportunity to submit a second audit
which resulted in an additional 22 audits being submitted..
7. The audit tool [Appendix 2] was identical to the one used by the NECN [Mitchell et al, 2009]. This
enabled comparisons to be made with similar work undertaken as part of the NAEDI initiative.
The audit tool was based upon the structure for significant event audit recommended by the
National Patient Safety Agency [NPSA 2006]. The audit tool was sent out with guidelines for
completion [Appendix 3]. The audit asked GPs to complete data in the following fields regarding
the lung cancer diagnosis:
What happened?
Why did it happen?
What has been learned?
What has been changed?
What was effective about this SEA?
Definitions, Management of Data, and Analysis
Date of first presentation and duration of symptoms prior to first presentation
8. The first symptom was identified either as verbatim from the text or interpreted from the text by
the researcher. An arbitrary two-year cut off was taken as the maximum duration of symptoms
prior to presentation. When one or more different symptoms with one or more different durations
9
were mentioned, the duration was recorded as the longer value. The durations were recoded into
days from the verbatim entries as shown in Box 1.
Box 1: Calculating duration of symptoms to first presentation
1 week = 7 days [and multiples]
1 month = 30 days [and multiples]
1 year = 365 days [and multiples]
„3-4 months‟ = 3.5 months = 105 days
„Sudden onset‟ = 0 days
„Few‟ = 3 days
„Asymptomatic‟ = 999 [different from missing data]
„Years‟ or „long history‟ coded as „2 years‟ [longest symptom duration reported by GPs]
„Unclear‟ or „not stated‟ = blank
„Short‟ and „relatively short‟ = coded as „ 7 days‟
Presenting symptoms
9. These were recorded as the presenting symptoms as noted by the GP at the time of presentation
and were categorised into either „respiratory‟ or „non-respiratory‟ in the same way as the NECN
audit report [Mitchell et al, 2009]. Some symptoms were not included in their categorisation,
therefore lump in neck, hoarseness, shoulder pain, costal margin pain, and rib pain were also
included as respiratory symptoms. Patients who were asymptomatic were excluded from this as
were patients whose symptoms were unclear or not stated. All of the symptoms were then coded
into categories of single and multiple symptoms, determined by the data.
Number of consultations prior to referral or investigation
10. The number of primary care consultations prior to referral or investigation was counted. This
included all primary care contacts [face to face consultations, nurse consultations, telephone
consultations, Out Of Hours contacts, home visits] prior to initial referral or investigation request
that could reasonably have been expected to lead to a diagnosis. In 3 instances the GP had
simply reported „several‟; these were recoded as „3‟. One had simply recorded „frequent‟; this was
recoded as „12‟ i.e. monthly for a year. Others were either totally unclear [invariably when there
was a complex pathway to diagnosis involving both primary care and secondary care], or were
not stated; these were left blank.
Date of request of first GP initiated chest x-ray and date report received
11. These were recorded verbatim, or calculated from the text e.g. „report received 2 days later‟. The
records were flagged of patients who at some time had either a normal chest x-ray [defined as
one that had no suspicion of lung cancer or that showed no change from previous changes that
were being monitored] or one that required a repeat X-ray after a period of time or treatment.

10
Referrals and admissions
12. A referral was regarded as such where there was clear evidence of a GP referral for one or more
of the presenting symptoms, clinical signs, or investigation results to a specialist. The specialties
referred to were determined by the data, were mutually exclusive, and coded as either „chest
clinic/respiratory physician‟, „ear nose and throat‟, „gastroenterology‟, „neurology‟, „rheumatology‟,
or „not stated‟. Urgency of referral was sometimes mentioned but not in a systematic way; it was
therefore not possible to assess the proportion for example of referrals according to the „urgent
cancer referral guidance‟. Admissions were coded as either „medical admission‟, „surgical
admission‟, or „spinal team admission‟.
Date of diagnosis
13. These were entered as provided by the GP. On reading the audits it became clear that sometimes
the date of diagnosis related to a clinical diagnosis, a Computed Tomography/Positron Emission
Tomography diagnosis, or a tissue diagnosis, a diagnosis after completion of staging. There were
occasional inaccuracies within these dates and a small number were amended e.g. when the GP
stated date of abnormal chest x-ray as the date of diagnosis, but when the patient went on to
have further definitive diagnostic procedures; a „higher level‟ of date of diagnosis was therefore
used when possible.
Diagnostic pathways
14. After reading and re-reading all of the audit reports, each of the patients was then classified into 1
of 11 mutually exclusive pathways. These are shown in Box 2.
Box 2: Classification of diagnostic pathways
1. Symptoms presented to GP – GP admission
2. Symptoms presented to GP – chest x-ray – referral
3. Symptoms presented to GP – chest x-ray – radiology then arranges CT and chest clinic
4. Symptoms presented to GP – chest x-ray - clinical diagnosis only, and no secondary care
involvement
5. Symptoms presented to GP – no chest x-ray - referral
6. Symptoms presented to GP – no chest x-ray - but diagnosis after self referral to A&E
7. Diagnosis made via investigation in a secondary care specialty, but with some primary care
involvement
8. Diagnosis made via investigation in a secondary care specialty, no primary care involvement
9. Most of diagnostic pathway made abroad [came back to UK for CT scan]
10. Via opportunistic chest x-ray taken prior to starting treatment for RA – no primary care
involvement
11. Unclear

11
Time intervals to diagnosis
15. From the data provided, 8 specific time intervals were calculated.. These are shown in Box 3, and
represented in Figure 1. Time intervals were calculated from the first presentation to referral or
investigation, defining a short duration as that of 31 days or less [Mitchell et al, 2009].
Box 3: Time intervals calculated
T1. Time from onset of symptoms to diagnosis [n=48]
T2. Time from onset of symptoms to presentation [n=51]
T3. Time from first presentation to chest x-ray request [n=72]
T4. Time from chest x-ray request to receipt of report [n=58]
T5. Time from x-ray report to referral [n=54]
T6. Time from referral to diagnosis [n=92]
T7. Time from first presentation to referral or admission [n=87]
T8. Time from first presentation to diagnosis [n=106]
Figure 1: Schematic representation of the time intervals from initial presentation to
diagnosis

12
FINDINGS
16. The number of general practices that registered and subsequently submitted completed audits by
Local Health Board are detailed in Table 1 below. Overall, audit reports were received from 96
general practices on 118 patients.
Table 1: Uptake of GPs in Significant Events Audit
Regional Cancer Networks
Local Health Boards
No. of General Practices per Local Health
Board
No. of General Practices
Registered (% of LHB total)
No. of audits received (% of
registered practices per
LHB)
North Wales Betsi Cadwaladr 121 43 (35.5) 29 (67.4)
South East Wales
Aneurin Bevan 94 27 (28.7) 15 (55.6)
Cardiff & Vale 70 28 (40) 24 (85.7)
Cwm Taf 52 19 (36.5) 10 (52.6)
South West Wales
Abertawe Bro Morgannwg 77 30 (39) 20 (66.7)
Hywel Dda 55 20 (36.4) 14 (70)
Powys 17 8 (47.1) 6 (75)
17. Of the 118 patients diagnosed with lung cancer, the year of diagnosis was as follows;
2010 - 24 patients [20.3%]
2009 - 77 patients [65.3%]
2008 - 12 patients [10.2%]
2007 - 2 patients [1.7%]
2006 - 1 patient [0.8%]
2005 - 1 patient [0.8%]
2004 – 0 patients
2003 – 0 patients
2002 - 1 patient [0.8%]
Audit meetings, where the diagnosis was discussed with primary health team members, were
held at a median of 97 days after diagnosis [SD 334, Inter Quartile Range (IQR) 53-238]. At the
time of the audit 72 [61.0%] patients were alive and 46 [39.0%] were dead. Findings were similar
between regional cancer networks [North Wales 17 alive, 58.6%; South East 31, 63.3%; South
West 24, 60.0%].
18. The diagnoses reported covered the following cancer types: 90 were either stated to be or
presumed to be non-small cell lung cancer [NSCLC] without evidence of metastases [these
included „bronchial‟, „adenocarcinoma‟, „cancer‟, „tumour‟ „non-small cell‟, „squamous‟]; 11 were
presumed NSCLC but with evidence of metastases at diagnosis; 15 were small cell cancers [of
13
whom 3 had evidence of metastases at diagnosis]; 1 was a neuro-endocrine tumour; and 1 was a
mesothelioma.
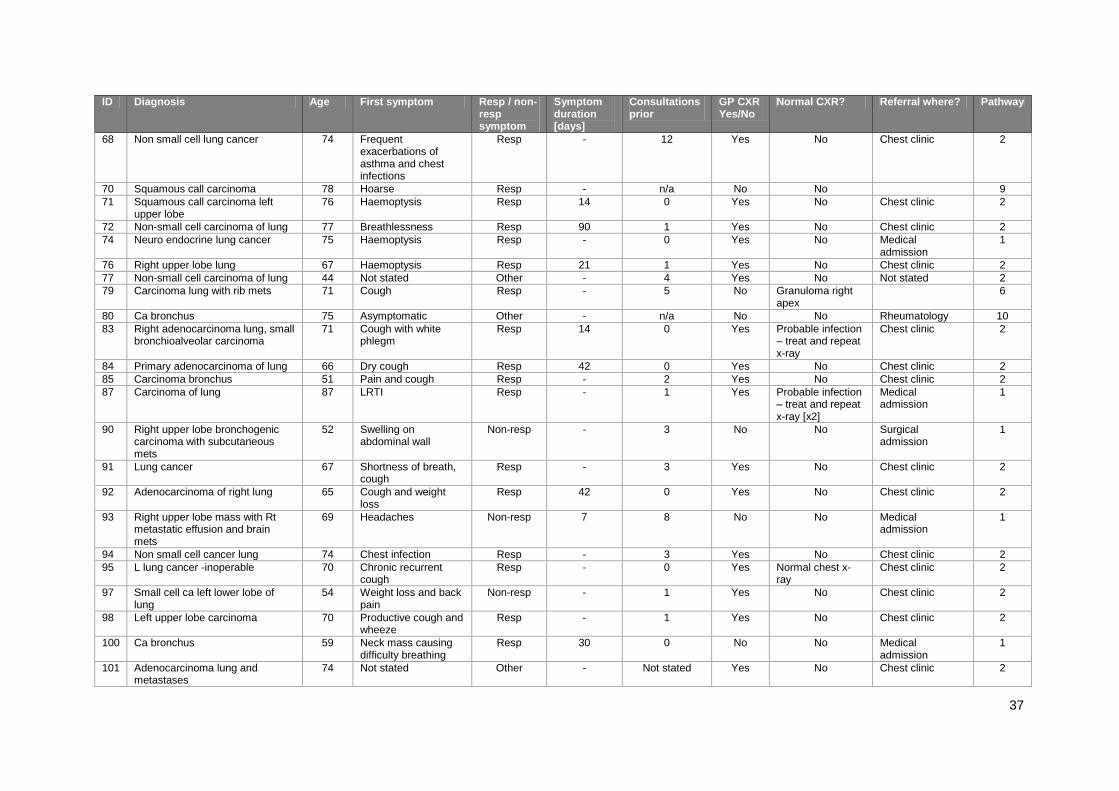
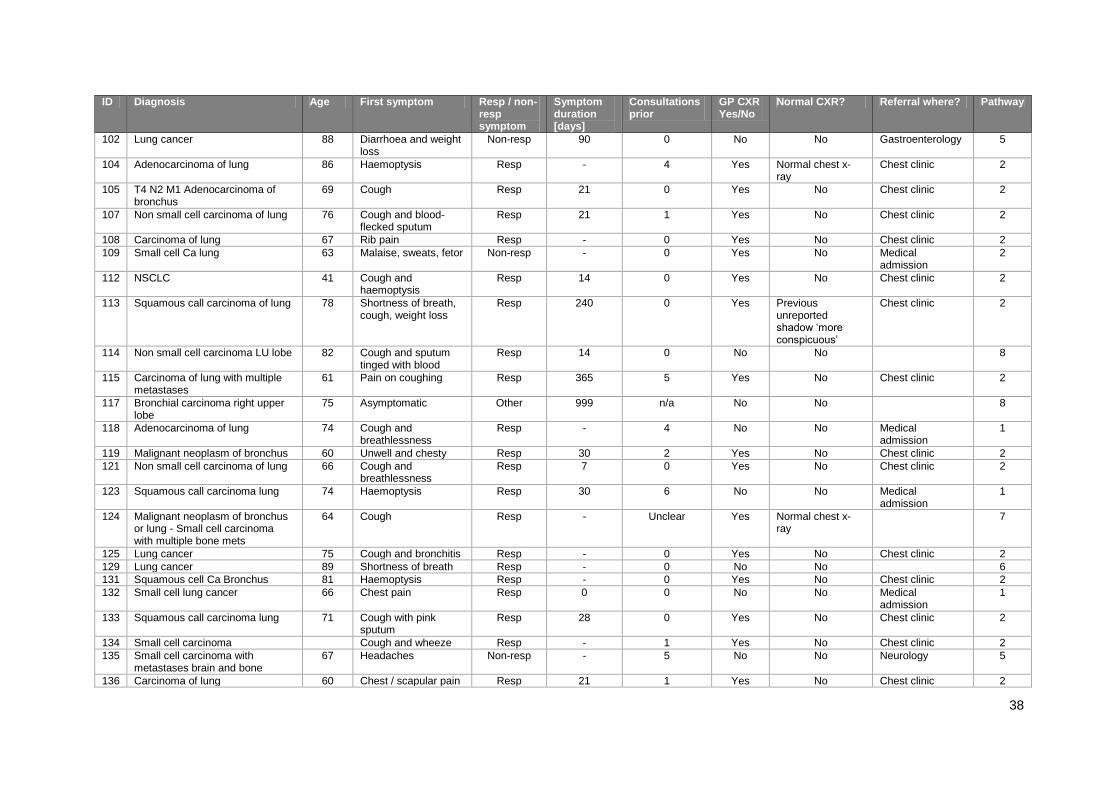
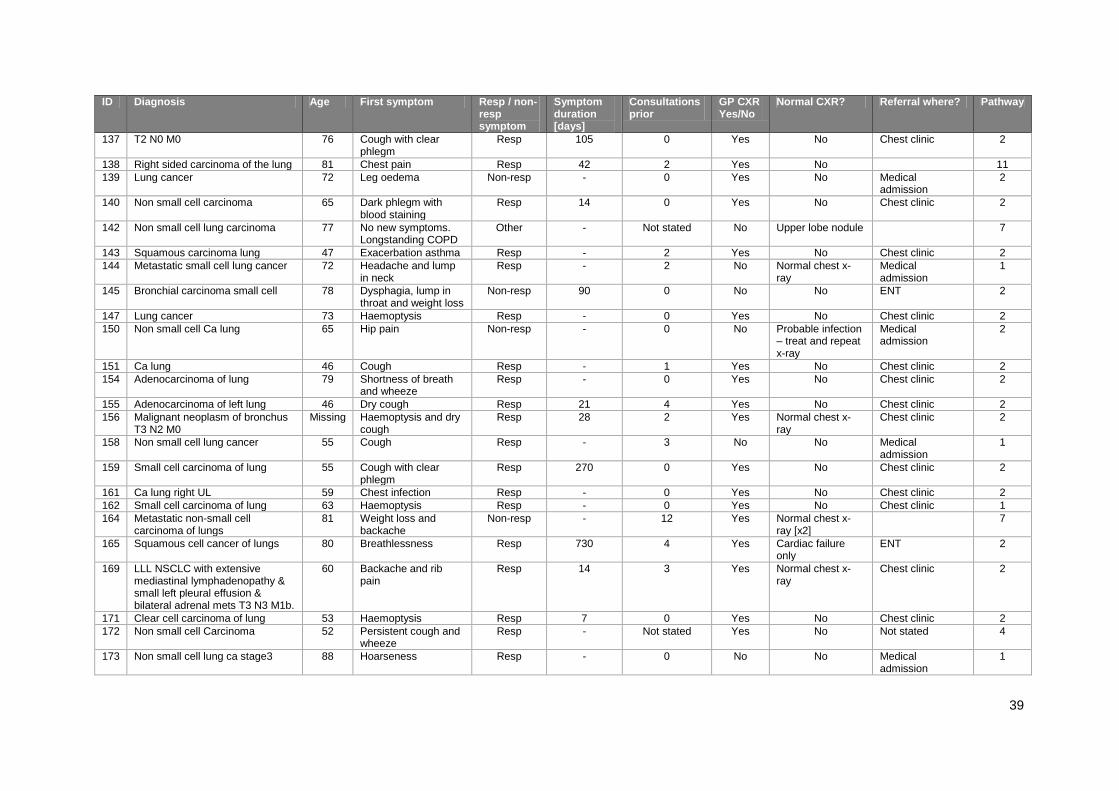
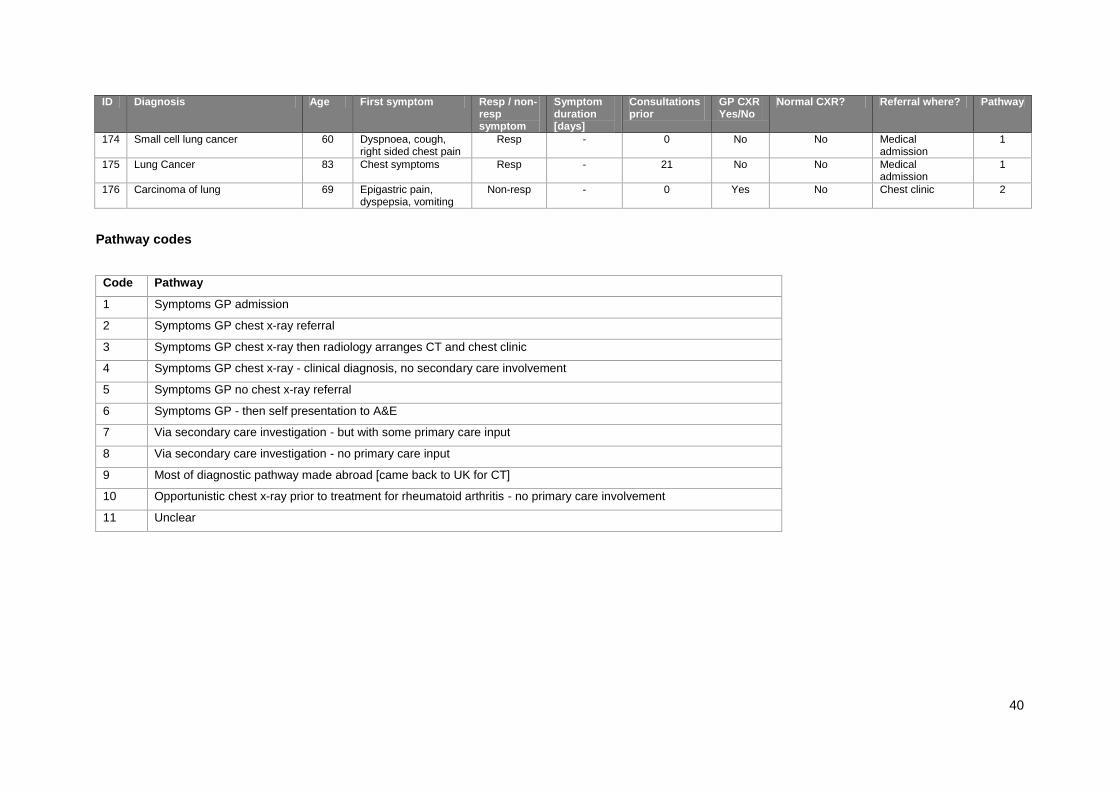
19. A summary of data regarding each audit report is included in Appendix 4.
Practice characteristics
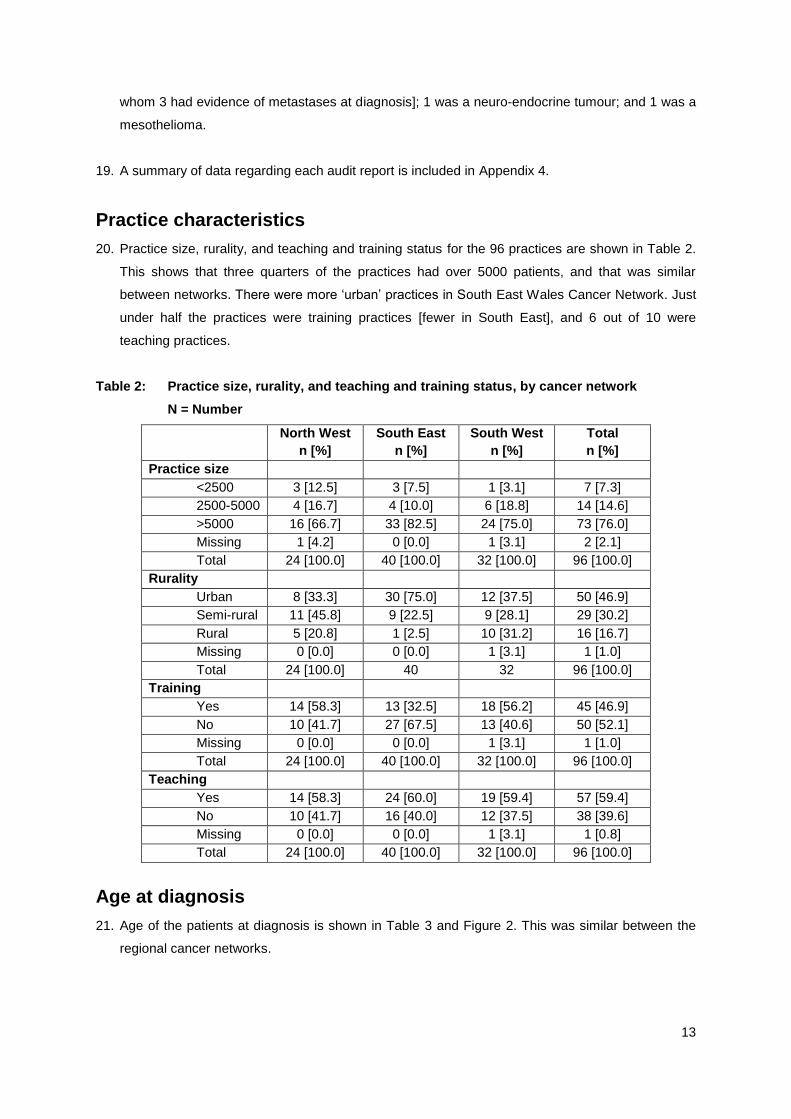
20. Practice size, rurality, and teaching and training status for the 96 practices are shown in Table 2.
This shows that three quarters of the practices had over 5000 patients, and that was similar
between networks. There were more „urban‟ practices in South East Wales Cancer Network. Just
under half the practices were training practices [fewer in South East], and 6 out of 10 were
teaching practices.
Table 2: Practice size, rurality, and teaching and training status, by cancer network
N = Number
North West
n [%]
South East
n [%]
South West
n [%]
Total
n [%]
Practice size
<2500 3 [12.5] 3 [7.5] 1 [3.1] 7 [7.3]
2500-5000 4 [16.7] 4 [10.0] 6 [18.8] 14 [14.6]
>5000 16 [66.7] 33 [82.5] 24 [75.0] 73 [76.0]
Missing 1 [4.2] 0 [0.0] 1 [3.1] 2 [2.1]
Total 24 [100.0] 40 [100.0] 32 [100.0] 96 [100.0]
Rurality
Urban 8 [33.3] 30 [75.0] 12 [37.5] 50 [46.9]
Semi-rural 11 [45.8] 9 [22.5] 9 [28.1] 29 [30.2]
Rural 5 [20.8] 1 [2.5] 10 [31.2] 16 [16.7]
Missing 0 [0.0] 0 [0.0] 1 [3.1] 1 [1.0]
Total 24 [100.0] 40 32 96 [100.0]
Training
Yes 14 [58.3] 13 [32.5] 18 [56.2] 45 [46.9]
No 10 [41.7] 27 [67.5] 13 [40.6] 50 [52.1]
Missing 0 [0.0] 0 [0.0] 1 [3.1] 1 [1.0]
Total 24 [100.0] 40 [100.0] 32 [100.0] 96 [100.0]
Teaching
Yes 14 [58.3] 24 [60.0] 19 [59.4] 57 [59.4]
No 10 [41.7] 16 [40.0] 12 [37.5] 38 [39.6]
Missing 0 [0.0] 0 [0.0] 1 [3.1] 1 [0.8]
Total 24 [100.0] 40 [100.0] 32 [100.0] 96 [100.0]
Age at diagnosis
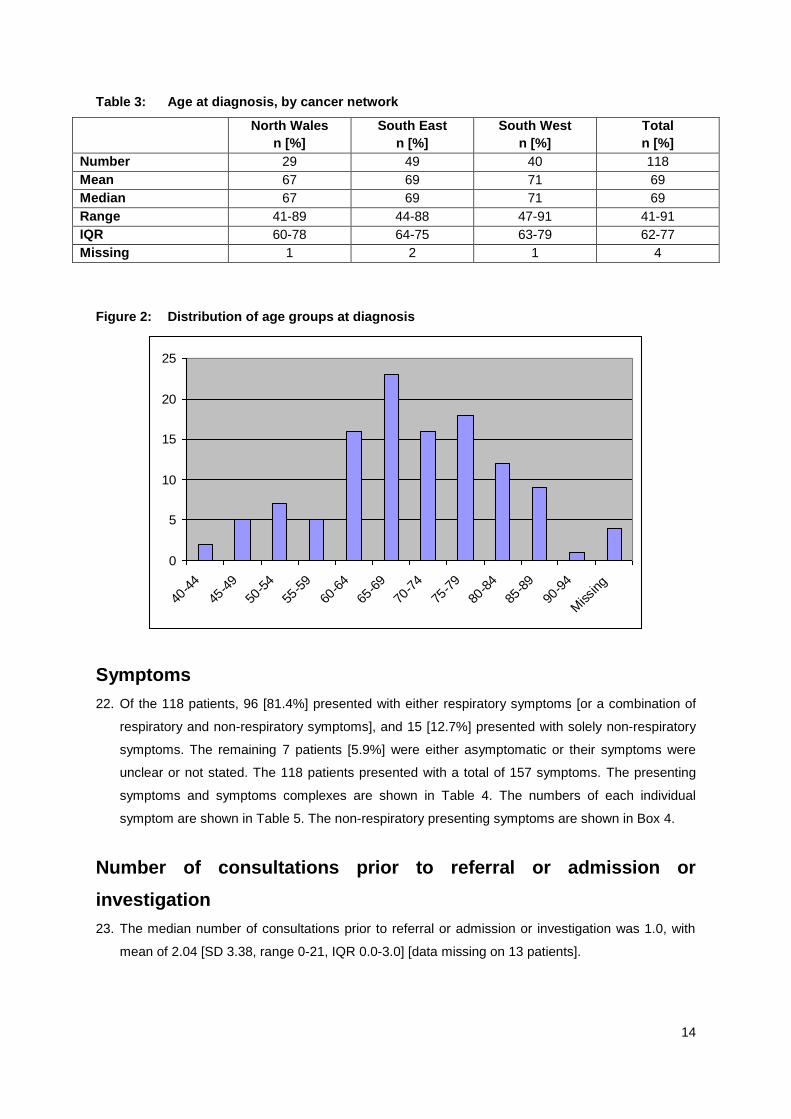
21. Age of the patients at diagnosis is shown in Table 3 and Figure 2. This was similar between the
regional cancer networks.
14
Table 3: Age at diagnosis, by cancer network
North Wales
n [%]
South East
n [%]
South West
n [%]
Total
n [%]
Number 29 49 40 118
Mean 67 69 71 69
Median 67 69 71 69
Range 41-89 44-88 47-91 41-91
IQR 60-78 64-75 63-79 62-77
Missing 1 2 1 4
Figure 2: Distribution of age groups at diagnosis
0
5
10
15
20
25
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85-8
9
90-9
4
Missing
Symptoms
22. Of the 118 patients, 96 [81.4%] presented with either respiratory symptoms [or a combination of
respiratory and non-respiratory symptoms], and 15 [12.7%] presented with solely non-respiratory
symptoms. The remaining 7 patients [5.9%] were either asymptomatic or their symptoms were
unclear or not stated. The 118 patients presented with a total of 157 symptoms. The presenting
symptoms and symptoms complexes are shown in Table 4. The numbers of each individual
symptom are shown in Table 5. The non-respiratory presenting symptoms are shown in Box 4.
Number of consultations prior to referral or admission or
investigation
23. The median number of consultations prior to referral or admission or investigation was 1.0, with
mean of 2.04 [SD 3.38, range 0-21, IQR 0.0-3.0] [data missing on 13 patients].

15
Table 4: Presenting symptoms and symptom complexes
Presenting symptoms N [%]
Haemoptysis 10 [8.5]
Haemoptysis and non-respiratory 1[0.8]
Haemoptysis and cough 7 [5.9]
Cough 16 [13.6]
Cough and non-respiratory 1 [0.8]
Cough and pain in chest or rib or costal margin or shoulder 5 [4.2]
Cough and weight loss or loss of appetite 2 [1.7]
Cough and breathless or wheeze 9 [7.6]
Cough and chest infection or exacerbation asthma or Chronic Obstructive Pulmonary Disease
or chesty 1 [0.8]
Cough, breathless or wheeze, and pain in chest or rib or costal margin or shoulder 1 [0.8]
Cough, breathless or wheeze, hoarseness and non-respiratory 1 [0.8]
Pain in chest or rib or costal margin or shoulder 11 [9.3]
Chest infection or exacerbation asthma or Chronic Obstructive Pulmonary Disease or chesty 11 [9.3]
Weight loss or loss of appetite and chest infection or exacerbation asthma or Chronic
Obstructive Pulmonary Disease or chesty 1 [0.8]
Breathless or wheeze 6 [5.1]
Breathless and weight loss or loss of appetite 1 [0.8]
Lump in neck 3 [2.5]
Hoarseness 2 [1.7]
Weight loss or loss of appetite 2 [1.7]
Weight loss or loss of appetite and non-respiratory 4 [3.4]
Weight loss or loss of appetite, cough and breathless or wheeze 1 [0.8]
Non-respiratory 15 [12.7]
Asymptomatic 2 [1.7]
Longstanding Chronic Obstructive Pulmonary Disease, no new symptoms 1 [0.8]
Unclear or not stated 4 [3.4]
Total 118 [100.0]
Table 5: Presenting symptoms
Presenting symptoms n [%]
Cough 44 [28.0]
Non-respiratory 22 [14.0]
Breathless or wheeze 19 [12.1]
Haemoptysis 18 [11.5]
Pain in chest or rib or costal margin or shoulder 17 [10.8]
Chest infection or exacerbation asthma or Chronic Obstructive Pulmonary Disease or chesty 13 [8.3]
Weight loss or loss of appetite 11 [7.0]
Unclear or not stated 4 [2.5]
Hoarseness 3 [1.9]
Lump in neck 3 [1.9]
Asymptomatic or longstanding Chronic Obstructive Pulmonary Disease with no new
symptoms 3 [1.9]
Total 157 [100.0]

16
Box 4: Non-respiratory presenting symptoms
Back pain or slipped disc
Collapse with no prior symptoms
Confusion, falls, bed bound
Epigastric pain, dyspepsia, vomiting
Headaches [2 patients]
Hip pain
Leg oedema
Lump on thigh
Malaise, sweats, fetor
Mechanical back pain
Sore throat
Right side pain
RUQ pain
Swelling on abdominal wall
Chest X-Rays
24. Of the 118 patients 79 [66.9%] patients had a GP initiated chest x-ray prior to diagnosis and 39
[33.1%] did not. For patients for whom date of receipt of chest x-ray report was available, the
median time from request to report was 5 days [Standard Deviation 6.7], but with a range up to 24
days [see Table 8]. A number of patients had chest x-rays that did not initially show suspicion of
lung cancer. Of these:
8 were reported as normal [including 1 patient who had 3 normal chest x-rays, the last a
month before bronchoscopic diagnosis, and another had 2 normal chest x-rays within 2
months of diagnosis]
3 reported no change in a pre-existing abnormality [granuloma right apex, upper lobe nodule,
costophrenic angle blunting]
2 reported other changes [Chronic Obstructive Pulmonary Disease, cardiac failure], but with
no suspicion of lung cancer
1 patient had an x-ray in August of 2009 that reported „a shadow that was more conspicuous
than the previous chest x-ray in November 2008‟, but this had not been mentioned on the
November 2008 report
9 reported probable infection „treat and repeat x-ray‟ [including 4 patients who had the same
probable diagnosis and management recommended twice].
Routes of referral or admission
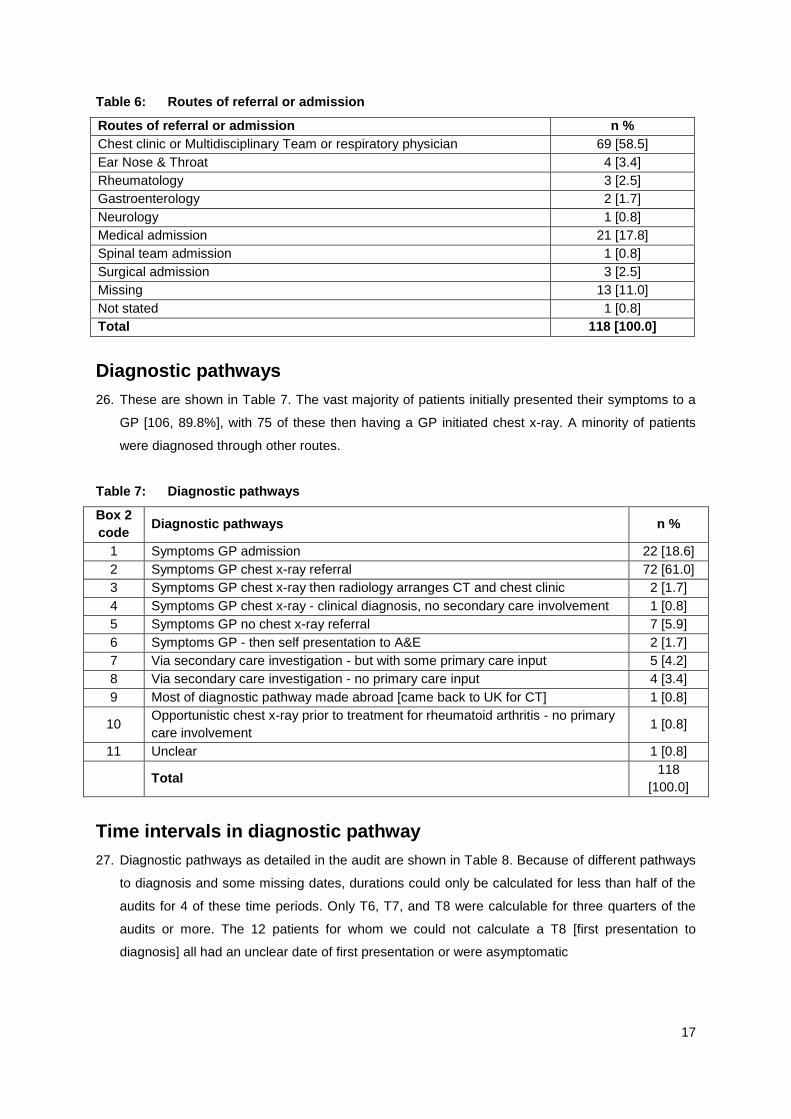
25. Routes of referral or admission are shown in Table 6. The majority of patients were diagnosed
after a GP initiated referral to a chest physician, however 10 patients were diagnosed after
referral to another specialty, and 25 [21.2%] were diagnosed after a GP initiated acute admission.
17
Table 6: Routes of referral or admission
Routes of referral or admission n %
Chest clinic or Multidisciplinary Team or respiratory physician 69 [58.5]
Ear Nose & Throat 4 [3.4]
Rheumatology 3 [2.5]
Gastroenterology 2 [1.7]
Neurology 1 [0.8]
Medical admission 21 [17.8]
Spinal team admission 1 [0.8]
Surgical admission 3 [2.5]
Missing 13 [11.0]
Not stated 1 [0.8]
Total 118 [100.0]
Diagnostic pathways
26. These are shown in Table 7. The vast majority of patients initially presented their symptoms to a
GP [106, 89.8%], with 75 of these then having a GP initiated chest x-ray. A minority of patients
were diagnosed through other routes.
Table 7: Diagnostic pathways
Box 2
code Diagnostic pathways n %
1 Symptoms GP admission 22 [18.6]
2 Symptoms GP chest x-ray referral 72 [61.0]
3 Symptoms GP chest x-ray then radiology arranges CT and chest clinic 2 [1.7]
4 Symptoms GP chest x-ray - clinical diagnosis, no secondary care involvement 1 [0.8]
5 Symptoms GP no chest x-ray referral 7 [5.9]
6 Symptoms GP - then self presentation to A&E 2 [1.7]
7 Via secondary care investigation - but with some primary care input 5 [4.2]
8 Via secondary care investigation - no primary care input 4 [3.4]
9 Most of diagnostic pathway made abroad [came back to UK for CT] 1 [0.8]
10 Opportunistic chest x-ray prior to treatment for rheumatoid arthritis - no primary
care involvement 1 [0.8]
11 Unclear 1 [0.8]
Total 118
[100.0]
Time intervals in diagnostic pathway
27. Diagnostic pathways as detailed in the audit are shown in Table 8. Because of different pathways
to diagnosis and some missing dates, durations could only be calculated for less than half of the
audits for 4 of these time periods. Only T6, T7, and T8 were calculable for three quarters of the
audits or more. The 12 patients for whom we could not calculate a T8 [first presentation to
diagnosis] all had an unclear date of first presentation or were asymptomatic

18
28. Of the 87 patients for whom time from first presentation to referral or admission was measurable [
coded T7 Table 8/Box 3], 34 [39.1%] had a duration of >31 days.
Table 8: Time intervals in diagnostic pathway [days]
N = Number and SD = Standard Deviation
Time intervals to diagnosis n Mean Median SD Range
T1. Time from onset of symptoms to diagnosis 48 204.5 101.5 264.9 28 - 1072
T2. Time from onset of symptoms to presentation 51 107.4 28.0 196.5 0-730
T3. Time from first presentation to chest x-ray
request 72 19.1 0.0 33.1 0 - 152
T4. Time from chest x-ray request to receipt of
report 58 7.1 5.0 6.7 0 - 24
T5. Time from chest x-ray report to referral 54 7.8 1.0 16.2 -2 - 79
T6. Time from referral to diagnosis 92 37.1 17.5 70.5 -5 - 520
T7. Time from first presentation to referral or
admission 87 50.4 21.0 73.4 0 - 365
T8. Time from first presentation to diagnosis 106 93.4 48.5 121.8 0 - 689
Note: time intervals were calculated from the verbatim information given (Box 1) and in a small number of cases,
this resulted in paradoxically negative values; this reflects the reporting by the GPs, and the definitions of date of
diagnosis used. Because they are small and infrequent we have left these in.
29. The mean and median for each interval categorised by whether first presentation was for
respiratory or non-respiratory symptoms is presented in Table 9. These numbers are too small to
draw meaningful conclusions and do not provide robust evidence as to whether patients
presenting with non-respiratory symptoms have a slower diagnostic journey than those that
presenting with respiratory symptoms.
Table 9: Time intervals in diagnostic pathway [days] by respiratory or non-respiratory
symptoms
N = Number SD = Standard Deviation Med = Median
Time intervals to diagnosis Respiratory symptoms Non-respiratory
symptoms
n Mean Med n Mean Med
T1. Time from onset of symptoms to diagnosis 44 194.9 94.50 4 310.8 195.5
T2. Time from onset of symptoms to presentation 46 100.6 28.00 5 169.6 21.0
T3. Time from first presentation to chest x-ray
request 68 19.7 0.00 3 0.0 0.0
T4. Time from chest x-ray request to receipt of
report 56 7.3 5.50 2 1.5 1.5
T5. Time from x-ray report to referral 50 8.1 1.00 2 2.5 2.5
T6. Time from referral to diagnosis 75 38.3 16.00 14 30.5 18.5
T7. Time from first presentation to
referral/admission 73 51.3 21.00 14 45.8 19.0
T8. Time from first presentation to diagnosis 90 97.4 48.50 14 76.3 68.5
Note: a small number of patients who were asymptomatic or whose symptoms were not stated or unclear were
excluded from this analysis, hence n not the same as previous table

19
Qualitative analysis of the diagnostic journey
30. The data were analysed as described by Mitchell et al [2009]. These are reported as major and
sub-themes.
Response of GPs to symptoms
Exemplary practice
31. For a large number of patients, the response of the GP to the presented symptoms, working from
the data provided on the audit forms, can only be described as exemplary. That is that there was
an appropriate response (chest x-ray request, admission, or urgent referral) to presented
suspicious symptoms, in line with current National Institute for Heath and Clinical Excellence
(NICE) guidance. There were at least 46 examples of these, and for many of the other patients
the GP referral pathway was complex due to secondary care and/or asymptomatic and atypical
presentations. A small number of patients had almost exemplary primary care behaviour [e.g.
referral for chest x-ray investigation or opinion within a few weeks of symptoms, but technically
outside of current NICE guidance] [e.g. 9, 10, 23, 38, Appendix 4].
Opportunities for earlier diagnosis
32. For a small number of patients it was clear that there were opportunities to consider a chest x-ray
earlier because of symptoms, although in retrospect it was difficult to know how easy it could have
been to have done this at the time [e.g. 32, 47, 50, 64, 91, 158, Appendix 4]. In 1 report the GP
suspected that an abnormal chest x-ray report could have been acted upon earlier [156, Appendix
5]]. In 1 report haemoptysis was considered „viral‟, and was only acted upon when represented 3
weeks later [76, Appendix 5].
Atypical and complex presentations
33. At least 10 atypical presentations were reported that did not lead any of the clinicians involved to
consider lung cancer as a diagnosis [e.g. 14, 18, 22, 34, 90, 93, 102, 124, 135, 169, Appendix 5].
There were a variety of complex presentations and pathways, with a number of factors relating to
the patient, their symptoms and their pathways [e.g. 79, 142, 164, Appendix 5]; one example of
this was trying to make sense of the symptoms presented by a man with schizophrenia [77,
Appendix 5].
Determining onset of symptoms that were due to lung cancer
34. In several cases, it was impossible for the GPs to know at the time of presentation whether the
„presenting symptoms‟ were due to lung cancer or not. These included, for example, ongoing
chest symptoms [175, 118, Appendix 5] and shoulder pain [39, Appendix 5].

20
Patients’ responsibility for delaying the diagnostic process
35. GPs reported that these occurred at various points in the diagnostic process, including late
presentation [e.g. 98, 159, Appendix 5], failure to attend chest clinic following exacerbations of
COPD [e.g. 147, Appendix 5], and refusal of investigations after initial referral [e.g. 7, 28, 100,
Appendix 5]. In 1 instance a patient failed to re-attend for invited review in primary care after initial
symptoms [165, Appendix 5], and 1 patient failed to accept admission, due to a „hedonistic
lifestyle‟ [11, Appendix 5].
Secondary Care responsibility for delaying the diagnostic process
36. Several GP reports included details of their perception of significant delays in secondary care,
with pointers as to the likely causes of these, which included indecision between locum
consultants and various other specialties and non-prioritisation of „urgent‟ GP referrals [113,
Appendix 5], initial misdiagnosis [62, Appendix 5], technical difficulties in the diagnosis [e.g. 63,
137, Appendix 5], and „bouncing‟ of an urgent referral as suggested by a radiologist followed by
non-communication to the GP [reported to Medical Director and disciplinary action taken] [112,
Appendix 5]. Only 1 GP report bemoaned the delay in reporting, apparently due to lack of
radiologists [a complaint to the Chief Executive of the Health Board ensued] [131, Appendix 5].
37. On the other hand 1 GP report demonstrated the ability of non-respiratory secondary care clinics
to deal with symptoms such as cough and sputum tinged with blood [114, Appendix 5]. Only 1
patient was lost to follow-up after initially being seen in the chest clinic [95, Appendix 5].

21
WHAT WAS LEARNED AND CHANGED BY THE
SIGNIFICANT EVENTS AUDIT (SEA) AND WHAT
WAS EFFECTIVE ABOUT IT?
38. A summary table showing what was learned and changed by the SEA and what was effective
about it is presented in Appendix 5. These data were edited slightly for clarity and for reasons of
space, but are otherwise verbatim. As can be seen, much has been learned and changed, and
much was regarded as effective about the process. These are presented as a series of bullet
points under each heading and sub-themes.
What has been learned?
Making the diagnosis
GPs recognised that they needed to:
Think widely in terms of diagnosis, moving beyond initial impressions and labels, thinking
laterally, with a lower threshold of suspicion for lung cancer than previously held
Be more aware of the possibility of some atypical symptoms such as back pain, shoulder
pain, sub-cutaneous lumps and non-resolving symptoms e.g. chesty cough, being caused by
malignancy
Identify and have suspicion roused by relevant history of risk factors e.g. smoking and
asbestos exposure
Be more aware of NICE guidance and exactly what it recommends in terms of lung cancer
diagnosis
Be more aware that NICE guidance is not always applicable within the context of atypical or
complex presentations
Process & communication
GPs recognised that they needed to:
Monitor processes e.g. timeliness of x-ray reporting
Be aware of their lack of knowledge about specific cancer treatments e.g. chemotherapy
Be aware that „normal‟ chest x-rays need to be repeated or patients referred if they have
ongoing symptoms
„Push the system‟ where necessary, if the diagnostic process is not working properly e.g.
ringing consultants, chasing appointments, checking that patients have appointments
Be aware of the issues about patient autonomy and choice about management of symptoms
or disease
Be aware of the need to prepare families for death

22
Specific to the ongoing care of an individual patient
Need for GP to undertake a review phone call with the patient, in the light of identified poor
communication from the hospital
What has been changed?
Diagnosis
GPs reported that as a consequence of the SEA process they had:
Reinforced and/or implemented National Institute for Health and Clinical Excellence (NICE)
guidelines within the practice team
Increased general awareness to reduce risks from „cognitive biases and omissions‟
Increased awareness of lung cancer as possible diagnosis in the face of symptoms, even in
the light of a „normal‟ recent chest x-ray
Lowered the threshold for chest x-ray, and pushing for „next-day‟ x-rays
Improved systems for chasing up abnormal chest x-ray results
Process
GPs reported that as a consequence of the SEA process, they had:
Improved systems for sending urgent referrals, ensuring their arrival, ensuring patients have
appointments, and following up hospital discharges
Developed a template to ensure all areas covered
Complained to the Local Health Board with subsequent action
Contacted consultants more frequently by phone and email
Improved systems for chronic disease management (CDM) for patients in residential settings
Increased training and involvement of CDM nurses in the practice
Asked for communication to be addressed within the South West Wales cancer group
Undertaken/requested more cancer Significant Events Audits in the future
Prevention
GPs reported that as a consequence of the SEA process, they had:
Focused on smokers who do not attend on a regular basis
Suggested improving smoking cessation services and access to smoking cessation services

23
What was effective about this SEA?
GPs reported that as a consequence of the SEA process, they had:
Made improvements in clinical practice and administrative systems
Made improvements in team building, morale, and improved communication within the
practice
Provided a focus on lung cancer, its symptoms, and the application of NICE guidelines
Re-affirmations that their clinical actions were appropriate
Many examples of learning about different types of tumours and their presentation
Made changes in a consultant‟s modus operandi
New opportunities to review the ongoing care of patients
24
DISCUSSION
Methodology
39. The methodology and analysis was as described by Mitchell et al [2009]. These data were
dependent upon reporting by the GP, hence the data can only be reported as such. There is the
potential of bias in the data reporting, although the text in the audit reports does suggest that
there was much „honest‟ reporting of the referral process. There is also the potential for some
post-hoc rationalisation, after a significant diagnosis. There are several issues worthy of
discussion:
a. Difficulty in the definition of date of diagnosis. The date of diagnosis was asked of GPs
exactly as such. The data supplied could have referred to either a „clinical‟ diagnosis, that
based upon CT [or other imaging], a tissue diagnosis or a full staging diagnosis. We were
unable to distinguish in many cases exactly how the date of diagnosis was defined.
b. Difficulty of interpreting first symptom. This is sometimes difficult to judge, from the
perspective of the patient, the physician and the researcher. However there is often no right
answer and assumptions made about this must be taken with some caution.
c. The „narrative‟ nature of the data sought, meant that for many patients there were missing
data, especially relating to key dates in the diagnostic process.
d. The diagnoses in the audit were made over a long time period with different policies and
practice at the time of diagnosis.
Summary of main findings and contextualising within the literature
Sample of patients
40. Our sample of patients in the audit was both similar to the NECN audit and to the age at diagnosis
national data [WCISU 2006] . The average age [69 years] was similar to the NECN audit [68
years] and is in keeping with national data [WCISU 2006]. The proportion of small cell cancers
[13%] was similar to national data [15-20%] [WCISU 2006]. In comparison to the NECN audit,
slightly fewer Welsh patients were alive at the time of diagnosis [61% compared with 64%].
Sample of practices
41. In comparison with the NECN audit the Welsh practices were very similar in terms of:
Size of the practices [NECN: 11.9% <2500, 17.4% 2500-5000, and 67.4% >5000]
Rurality [NECN: 50.4% urban, 32.6% semi-urban, and 9.8% rural]

25
Proportion of training practices [NECN: 43.5%]
Proportion of teaching practices [NECN: 55.4%]
Presenting symptoms
42. Slightly more Welsh patients presented with respiratory symptoms [81%] compared with 74% in
the NECN audit.
Chest x-rays and normal chest x-rays
43. A similar proportion of patients had a GP-initiated x-ray prior to diagnosis in this Welsh audit
[67%] compared with a series reported in Devon [66%] [Stapley et al 2006]. Fourteen x-rays
[11.8%] were reported as essentially normal, compared with 12.8% in Devon.
Diagnostic pathways and referrals
44. The diagnostic pathways reported here [Table 7] are very similar to those reported by Barrett and
Hamilton in their cohort from Devon [Barrett and Hamilton, 2008]. They reported the proportion of
diagnoses made after outpatient referral as 61%, emergency referral 23% and asymptomatic
11%.
Time intervals in the diagnostic pathway
45. The NECN audit reported time from relevant symptom presentation to referral or acute admission
as a mean of 59 days [Welsh audit mean of 50 days] and a median of 21 days [Welsh median 21
days], with [59%] of 31 days or less [Welsh data 61%]. The figure from a Scottish audit [Baughan
et al, 2009], was a median of 11 days. The findings reported from secondary analysis of data from
the national survey of cancer patients [Allgar & Neal, 2005] are also similar to the data presented
here; a median time from referral to diagnosis of 21 days [Welsh data 16 days]. In comparison
with the Scottish audit data [based on 981 patients, exact method of asking the questions not
stated], the time from first symptom to presentation was longer in Wales [median 28 days] than
Scotland [median 9.5 days].
Qualitative data
46. Analysis of these data showed that for many patients, and not simply those that had „straight-
forward‟ symptoms, the response of the GP in getting the patient into a diagnostic system was
exemplary. For a smaller number, there had been opportunities for the GP in retrospect to have
investigated or referred earlier, however the analysis of the data relating to changes suggests that
many practices have updated their knowledge and application of NICE guidance. Atypical and
complex presentations have different challenges, and in some cases it remains impossible to
know when the symptoms associated with ongoing lung disease become those of a lung cancer.
Other factors that are difficult to legislate about in the diagnostic process are patients delaying for
a variety of reasons. The GPs believed that in some instances there were secondary care issues

26
that delayed the diagnosis. Technical diagnostic difficulties may be improved after publication of
the updated NICE guidelines on the diagnosis and management of lung cancer in late 2010.
Specific concerns were raised in a small number of cases and these were dealt with through the
Health Board. Much was learned through the SEA process by the GPs, in the fields of diagnosis
and the process of working with secondary care and the patient. Much of this resulted in
significant changes in practices, and significant benefit from participation in the SEA process.

27
REFERENCES
i. Allgar VL, Neal RD. Delays in the diagnosis of six cancers: analysis of data from the National
Survey of NHS Patients: Cancer. Br J Cancer 2005;92:1959-1970.
ii. Barrett J, Hamilton W. Pathways to the diagnosis of lung cancer in the UK: a cohort study.
BMC Fam Pract 2008;9:31.
iii. Baughan P, O‟Neill B, Fletcher E. Auditing the diagnosis of cancer in primary care: the
experience in Scotland. Br J Cancer 2009;101:S87-S91.
iv. Mitchell E, Macleod U, Rubin G. Cancer in primary care. An analysis of significant event
audits [SEA] for diagnosis of lung cancer and cancers in teenagers and young adults 2008-9.
Universities of Dundee, Glasgow and Durham, 2009.
v. National Patient Safety Agency. Seven steps to patient safety for primary care. NPSA:
London, 2006. [available from http://www.npsa.nhs.uk]
vi. Office for National Statistics. Cancer and Mortality in the United Kingdom 2005-2007. August
2010. [available at http://www.statistics.gov.uk/pdfdir/canuk0810.pdf]
vii. Stapley S, Sharp D, Hamilton W. Negative chest x-rays in primary care patients with lung
cancer. Br J Gen Pract 2006;56:570-573.
viii. Welsh Cancer Intelligence and Surveillance Unit. Trachea, Bronchus and Lung Cancer in
Wales. Welsh Cancer Intelligence and Surveillance Unit, 2006

28
APPENDIX 1 – GP Invitation Letter
Page 1

29
Page 2

30
APPENDIX 2 – Audit Template
Page 1

31
Page 2
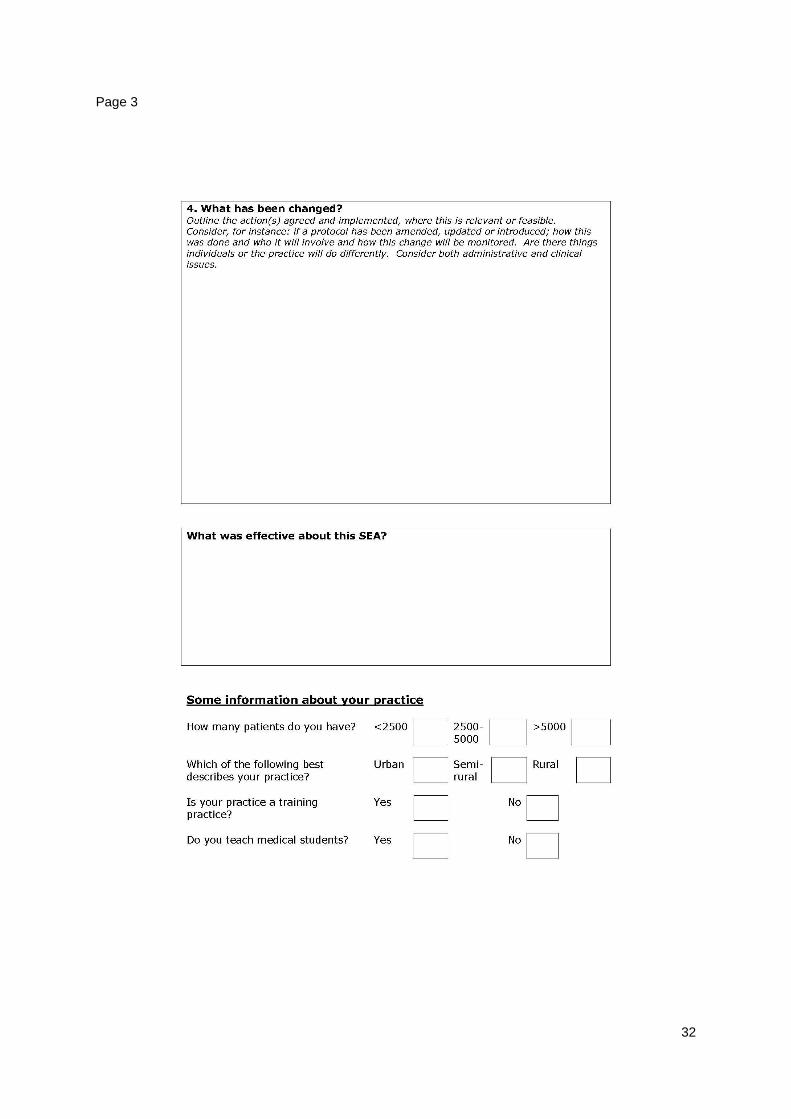
32
Page 3

33
APPENDIX 3 – Guidelines for Completion
Page 1

34
Page 2
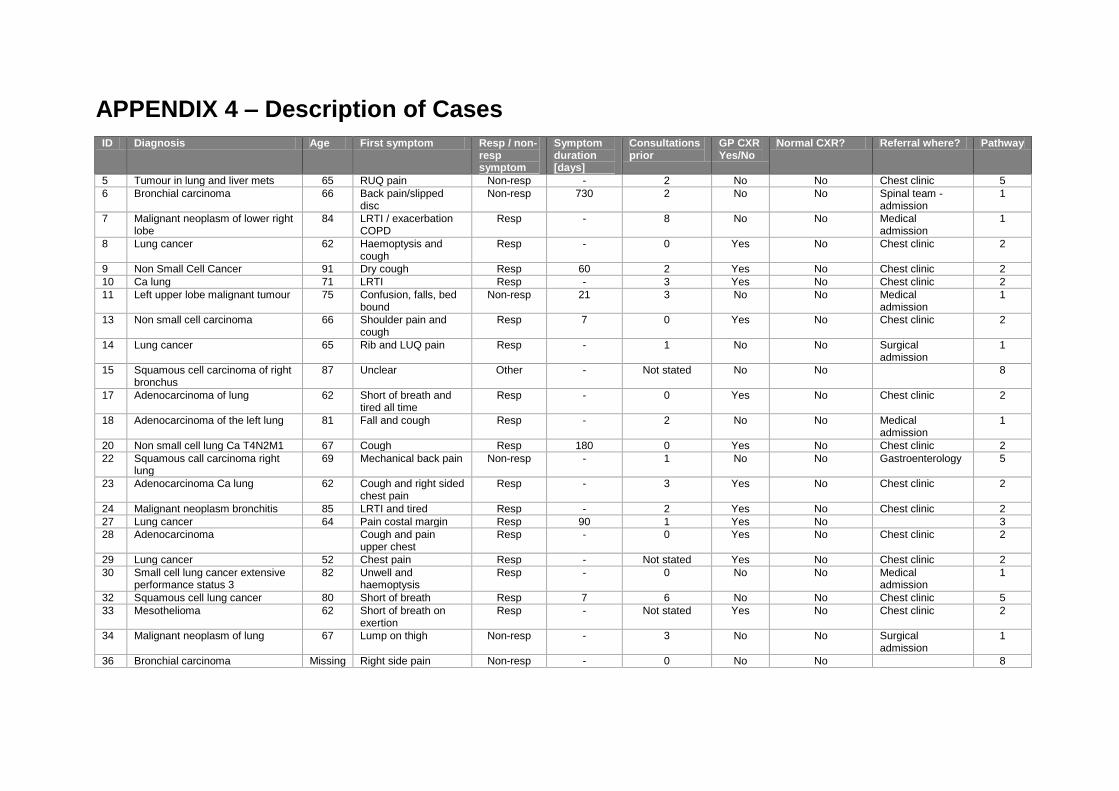
APPENDIX 4 – Description of Cases
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
5 Tumour in lung and liver mets 65 RUQ pain Non-resp - 2 No No Chest clinic 5
6 Bronchial carcinoma 66 Back pain/slipped disc
Non-resp 730 2 No No Spinal team - admission
1
7 Malignant neoplasm of lower right lobe
84 LRTI / exacerbation COPD
Resp - 8 No No Medical admission
1
8 Lung cancer 62 Haemoptysis and cough
Resp - 0 Yes No Chest clinic 2
9 Non Small Cell Cancer 91 Dry cough Resp 60 2 Yes No Chest clinic 2
10 Ca lung 71 LRTI Resp - 3 Yes No Chest clinic 2
11 Left upper lobe malignant tumour 75 Confusion, falls, bed bound
Non-resp 21 3 No No Medical admission
1
13 Non small cell carcinoma 66 Shoulder pain and cough
Resp 7 0 Yes No Chest clinic 2
14 Lung cancer 65 Rib and LUQ pain Resp - 1 No No Surgical admission
1
15 Squamous cell carcinoma of right bronchus
87 Unclear Other - Not stated No No 8
17 Adenocarcinoma of lung 62 Short of breath and tired all time
Resp - 0 Yes No Chest clinic 2
18 Adenocarcinoma of the left lung 81 Fall and cough Resp - 2 No No Medical admission
1
20 Non small cell lung Ca T4N2M1 67 Cough Resp 180 0 Yes No Chest clinic 2
22 Squamous call carcinoma right lung
69 Mechanical back pain Non-resp - 1 No No Gastroenterology 5
23 Adenocarcinoma Ca lung 62 Cough and right sided chest pain
Resp - 3 Yes No Chest clinic 2
24 Malignant neoplasm bronchitis 85 LRTI and tired Resp - 2 Yes No Chest clinic 2
27 Lung cancer 64 Pain costal margin Resp 90 1 Yes No 3
28 Adenocarcinoma Cough and pain upper chest
Resp - 0 Yes No Chest clinic 2
29 Lung cancer 52 Chest pain Resp - Not stated Yes No Chest clinic 2
30 Small cell lung cancer extensive performance status 3
82 Unwell and haemoptysis
Resp - 0 No No Medical admission
1
32 Squamous cell lung cancer 80 Short of breath Resp 7 6 No No Chest clinic 5
33 Mesothelioma 62 Short of breath on exertion
Resp - Not stated Yes No Chest clinic 2
34 Malignant neoplasm of lung 67 Lump on thigh Non-resp - 3 No No Surgical admission
1
36 Bronchial carcinoma Missing Right side pain Non-resp - 0 No No 8

36
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
37 SCC left lower lobe bronchus infiltrating squamous cell carcinoma
63 Cough with blood streaked sputum
Resp 28 0 Yes Probable infection – treat and repeat x-ray [x2]
Chest clinic 2
38 Non small cell carcinoma lung 82 Cough Resp 10 2 Yes No Chest clinic 2
39 Primary Adenocarcinoma of lung 77 Shoulder pain Resp 730 3 No No Rheumatology 7
43 Squamous CC Lung 82 Dry cough Resp 730 1 Yes Probable infection – treat and repeat x-ray [x2]
Chest clinic 2
44 Pancoast syndrome 58 Right upper anterior chest and right shoulder pain
Resp 28 16 Yes Normal chest x-ray
Rheumatology 7
45 Lung cancer T1N0M0 86 Collapse with no prior symptoms
Non-resp 0 0 No No Medical admission
1
47 Right upper lobe bronchogenic carcinoma
75 Exacerbations COPD Resp - 10 Yes Probable infection – treat and repeat x-ray
3
48 Lung cancer 87 Weakness and weight loss
Non-resp - Not stated Yes No Chest clinic 2
49 Tumour L main Bronchus 67 Exacerbation COPD Resp - 2 No COPD only ENT 5
50 Non small cell carinoma of lung 72 Loss of weight Non-resp 90 2 Yes No Chest clinic 2
53 Adenocarcinoma lung 62 URTI , headache, hoarseness, dry cough
Resp 28 1 Yes No Chest clinic 2
54 Carcinoma of lung 62 Weight loss nausea, poor appetite, cough, noisy breathing
Resp 90 0 Yes No Chest clinic 2
55 Small call bronchial carcinoma 66 Dyspnoea and cough Resp 14 0 Yes No Chest clinic 2
56 Carcinoma of lung 72 Cough and breathlessness
Resp 21 0 Yes Probable infection – treat and repeat x-ray
Chest clinic 2
59 Non small cell carcinoma 79 Blood-stained cough Resp 60 0 Yes No Chest clinic 2
62 Cancer of lung (small cell) 48 Chesty cough and wheeze
Resp - 3 Yes No Chest clinic 2
63 Lung cancer 69 Chest pain Resp - Not stated No Probable infection – treat and repeat x-ray [x2]
Medical admission
1
64 Malignant neoplasm of lung 49 Sore throat Non-resp 90 3 No No ENT 5
65 Small cell carcinoma lung 54 Occipital lymph node Resp - 2 Yes Probable infection – treat and repeat x-ray
Chest clinic 2
67 Stage IV squamous carcinoma left upper lobe
75 Not stated Other Not stated Yes Costophrenic angle blunting
Chest clinic 2
37
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
68 Non small cell lung cancer 74 Frequent exacerbations of asthma and chest infections
Resp - 12 Yes No Chest clinic 2
70 Squamous call carcinoma 78 Hoarse Resp - n/a No No 9
71 Squamous call carcinoma left upper lobe
76 Haemoptysis Resp 14 0 Yes No Chest clinic 2
72 Non-small cell carcinoma of lung 77 Breathlessness Resp 90 1 Yes No Chest clinic 2
74 Neuro endocrine lung cancer 75 Haemoptysis Resp - 0 Yes No Medical admission
1
76 Right upper lobe lung 67 Haemoptysis Resp 21 1 Yes No Chest clinic 2
77 Non-small cell carcinoma of lung 44 Not stated Other - 4 Yes No Not stated 2
79 Carcinoma lung with rib mets 71 Cough Resp - 5 No Granuloma right apex
6
80 Ca bronchus 75 Asymptomatic Other - n/a No No Rheumatology 10
83 Right adenocarcinoma lung, small bronchioalveolar carcinoma
71 Cough with white phlegm
Resp 14 0 Yes Probable infection – treat and repeat x-ray
Chest clinic 2
84 Primary adenocarcinoma of lung 66 Dry cough Resp 42 0 Yes No Chest clinic 2
85 Carcinoma bronchus 51 Pain and cough Resp - 2 Yes No Chest clinic 2
87 Carcinoma of lung 87 LRTI Resp - 1 Yes Probable infection – treat and repeat x-ray [x2]
Medical admission
1
90 Right upper lobe bronchogenic carcinoma with subcutaneous mets
52 Swelling on abdominal wall
Non-resp - 3 No No Surgical admission
1
91 Lung cancer 67 Shortness of breath, cough
Resp - 3 Yes No Chest clinic 2
92 Adenocarcinoma of right lung 65 Cough and weight loss
Resp 42 0 Yes No Chest clinic 2
93 Right upper lobe mass with Rt metastatic effusion and brain mets
69 Headaches Non-resp 7 8 No No Medical admission
1
94 Non small cell cancer lung 74 Chest infection Resp - 3 Yes No Chest clinic 2
95 L lung cancer -inoperable 70 Chronic recurrent cough
Resp - 0 Yes Normal chest x-ray
Chest clinic 2
97 Small cell ca left lower lobe of lung
54 Weight loss and back pain
Non-resp - 1 Yes No Chest clinic 2
98 Left upper lobe carcinoma 70 Productive cough and wheeze
Resp - 1 Yes No Chest clinic 2
100 Ca bronchus 59 Neck mass causing difficulty breathing
Resp 30 0 No No Medical admission
1
101 Adenocarcinoma lung and metastases
74 Not stated Other - Not stated Yes No Chest clinic 2
38
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
102 Lung cancer 88 Diarrhoea and weight loss
Non-resp 90 0 No No Gastroenterology 5
104 Adenocarcinoma of lung 86 Haemoptysis Resp - 4 Yes Normal chest x-ray
Chest clinic 2
105 T4 N2 M1 Adenocarcinoma of bronchus
69 Cough Resp 21 0 Yes No Chest clinic 2
107 Non small cell carcinoma of lung 76 Cough and blood-flecked sputum
Resp 21 1 Yes No Chest clinic 2
108 Carcinoma of lung 67 Rib pain Resp - 0 Yes No Chest clinic 2
109 Small cell Ca lung 63 Malaise, sweats, fetor Non-resp - 0 Yes No Medical admission
2
112 NSCLC 41 Cough and haemoptysis
Resp 14 0 Yes No Chest clinic 2
113 Squamous call carcinoma of lung 78 Shortness of breath, cough, weight loss
Resp 240 0 Yes Previous unreported shadow „more conspicuous‟
Chest clinic 2
114 Non small cell carcinoma LU lobe 82 Cough and sputum tinged with blood
Resp 14 0 No No 8
115 Carcinoma of lung with multiple metastases
61 Pain on coughing Resp 365 5 Yes No Chest clinic 2
117 Bronchial carcinoma right upper lobe
75 Asymptomatic Other 999 n/a No No 8
118 Adenocarcinoma of lung 74 Cough and breathlessness
Resp - 4 No No Medical admission
1
119 Malignant neoplasm of bronchus 60 Unwell and chesty Resp 30 2 Yes No Chest clinic 2
121 Non small cell carcinoma of lung 66 Cough and breathlessness
Resp 7 0 Yes No Chest clinic 2
123 Squamous call carcinoma lung 74 Haemoptysis Resp 30 6 No No Medical admission
1
124 Malignant neoplasm of bronchus or lung - Small cell carcinoma with multiple bone mets
64 Cough Resp - Unclear Yes Normal chest x-ray
7
125 Lung cancer 75 Cough and bronchitis Resp - 0 Yes No Chest clinic 2
129 Lung cancer 89 Shortness of breath Resp - 0 No No 6
131 Squamous cell Ca Bronchus 81 Haemoptysis Resp - 0 Yes No Chest clinic 2
132 Small cell lung cancer 66 Chest pain Resp 0 0 No No Medical admission
1
133 Squamous call carcinoma lung 71 Cough with pink sputum
Resp 28 0 Yes No Chest clinic 2
134 Small cell carcinoma Cough and wheeze Resp - 1 Yes No Chest clinic 2
135 Small cell carcinoma with metastases brain and bone
67 Headaches Non-resp - 5 No No Neurology 5
136 Carcinoma of lung 60 Chest / scapular pain Resp 21 1 Yes No Chest clinic 2
39
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
137 T2 N0 M0 76 Cough with clear phlegm
Resp 105 0 Yes No Chest clinic 2
138 Right sided carcinoma of the lung 81 Chest pain Resp 42 2 Yes No 11
139 Lung cancer 72 Leg oedema Non-resp - 0 Yes No Medical admission
2
140 Non small cell carcinoma 65 Dark phlegm with blood staining
Resp 14 0 Yes No Chest clinic 2
142 Non small cell lung carcinoma 77 No new symptoms. Longstanding COPD
Other - Not stated No Upper lobe nodule 7
143 Squamous carcinoma lung 47 Exacerbation asthma Resp - 2 Yes No Chest clinic 2
144 Metastatic small cell lung cancer 72 Headache and lump in neck
Resp - 2 No Normal chest x-ray
Medical admission
1
145 Bronchial carcinoma small cell 78 Dysphagia, lump in throat and weight loss
Non-resp 90 0 No No ENT 2
147 Lung cancer 73 Haemoptysis Resp - 0 Yes No Chest clinic 2
150 Non small cell Ca lung 65 Hip pain Non-resp - 0 No Probable infection – treat and repeat x-ray
Medical admission
2
151 Ca lung 46 Cough Resp - 1 Yes No Chest clinic 2
154 Adenocarcinoma of lung 79 Shortness of breath and wheeze
Resp - 0 Yes No Chest clinic 2
155 Adenocarcinoma of left lung 46 Dry cough Resp 21 4 Yes No Chest clinic 2
156 Malignant neoplasm of bronchus T3 N2 M0
Missing Haemoptysis and dry cough
Resp 28 2 Yes Normal chest x-ray
Chest clinic 2
158 Non small cell lung cancer 55 Cough Resp - 3 No No Medical admission
1
159 Small cell carcinoma of lung 55 Cough with clear phlegm
Resp 270 0 Yes No Chest clinic 2
161 Ca lung right UL 59 Chest infection Resp - 0 Yes No Chest clinic 2
162 Small cell carcinoma of lung 63 Haemoptysis Resp - 0 Yes No Chest clinic 1
164 Metastatic non-small cell carcinoma of lungs
81 Weight loss and backache
Non-resp - 12 Yes Normal chest x-ray [x2]
7
165 Squamous cell cancer of lungs 80 Breathlessness Resp 730 4 Yes Cardiac failure only
ENT 2
169 LLL NSCLC with extensive mediastinal lymphadenopathy & small left pleural effusion & bilateral adrenal mets T3 N3 M1b.
60 Backache and rib pain
Resp 14 3 Yes Normal chest x-ray
Chest clinic 2
171 Clear cell carcinoma of lung 53 Haemoptysis Resp 7 0 Yes No Chest clinic 2
172 Non small cell Carcinoma 52 Persistent cough and wheeze
Resp - Not stated Yes No Not stated 4
173 Non small cell lung ca stage3 88 Hoarseness Resp - 0 No No Medical admission
1
40
ID Diagnosis Age First symptom Resp / non-resp symptom
Symptom duration [days]
Consultations prior
GP CXR Yes/No
Normal CXR? Referral where? Pathway
174 Small cell lung cancer 60 Dyspnoea, cough, right sided chest pain
Resp - 0 No No Medical admission
1
175 Lung Cancer 83 Chest symptoms Resp - 21 No No Medical admission
1
176 Carcinoma of lung 69 Epigastric pain, dyspepsia, vomiting
Non-resp - 0 Yes No Chest clinic 2
Pathway codes
Code Pathway
1 Symptoms GP admission
2 Symptoms GP chest x-ray referral
3 Symptoms GP chest x-ray then radiology arranges CT and chest clinic
4 Symptoms GP chest x-ray - clinical diagnosis, no secondary care involvement
5 Symptoms GP no chest x-ray referral
6 Symptoms GP - then self presentation to A&E
7 Via secondary care investigation - but with some primary care input
8 Via secondary care investigation - no primary care input
9 Most of diagnostic pathway made abroad [came back to UK for CT]
10 Opportunistic chest x-ray prior to treatment for rheumatoid arthritis - no primary care involvement
11 Unclear

41
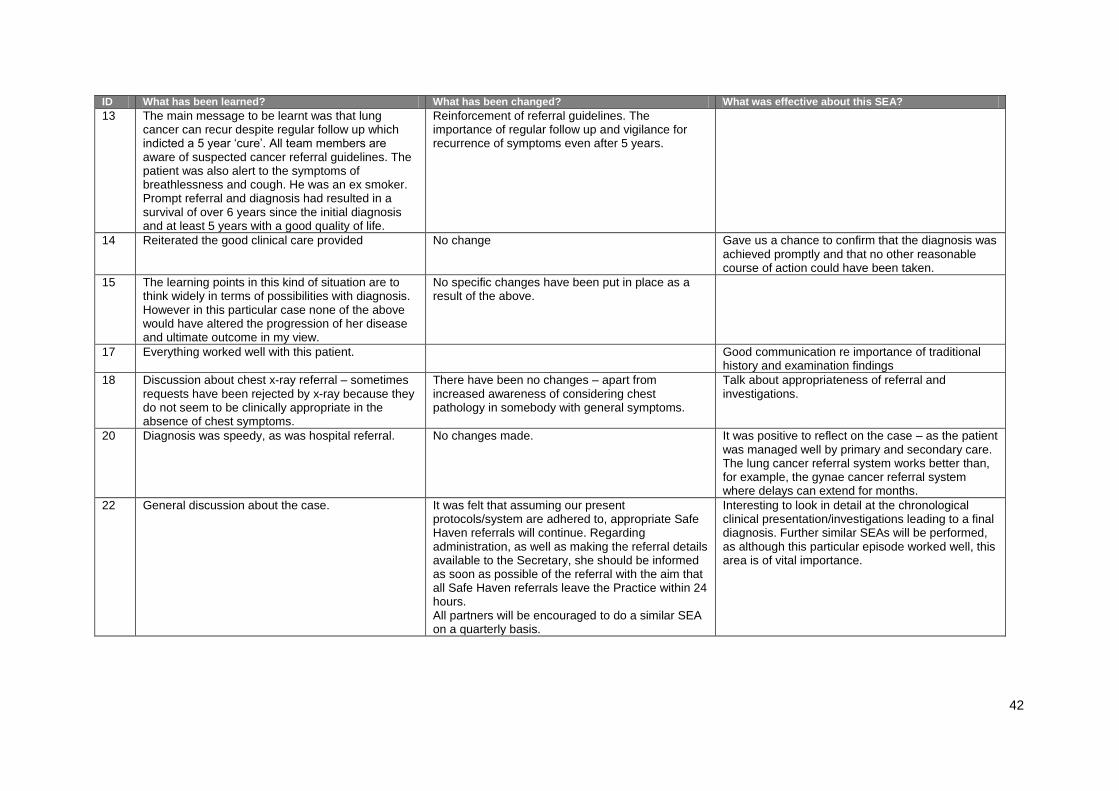
APPENDIX 5 – What Was Learned and Changed by the Significant Events Audit
and What Was Effective About It?
ID What has been learned? What has been changed? What was effective about this SEA?
5 Poor communication between secondary and primary care
The issue of communication will be addressed through the South West Wales cancer group
Reflection on the need for seamless care along the primary secondary care interface
6 The main conclusion was that he had been seen by 3 different doctors including a locum which may have affected how quickly he was referred. We all agreed that we needed to be more aware of the possibility of bony metastases in patients with unexplained back pain.
No changes were made to any practice protocols. It relieved me that colleagues felt my actions appropriate.
7 The NICE Guidelines (2007) on referral for suspected cancer outline key recommendations for this process.
A further clinical practice meeting was held to discuss the implementation of the NICE (2005) guidelines on referral for suspected cancer into the practice protocols. These will be written up and copied given to all clinicians. In this case, the GP was to discuss diagnosis further with the family, mainly the daughter and try to convince her of the need to disclose to the patient.
It was also useful to reflect on the process and assess how the NICE guidelines can and should be utilized for such cases.
8 We have noted a number of patients with lung cancer recently (i.e. over the last 8 years or so) and we have discussed early chest x-ray in patients with prolonged cough, un-resolving chest infection or haemoptysis.
We have discussed chest x ray as an investigation for respiratory symptoms, but also for “malaise”
A good team discussion with good team building, and a recognition that we have high rates of lung cancer because of our „deprived‟ practice population, and heavy smoking habits.
9 No lessons learned Not aware of any need to change protocols Useful to reflect on processes
10 We agreed that a high index of suspicion should be maintained in patients with unresolving symptoms, especially smokers. We agreed that communication between primary and secondary care in this instance was excellent. Likewise, in-house communication between administrative and clinical staff was equally effective.
No changes It highlighted the ever-present possibility of new pathology in patients with established chronic disease.
11 Discussion around patient autonomy In this case, nothing Highlighted the difficulty we have with patients not actually wanting to access appropriate care for their problems and the ethical dilemmas it poses.
42
ID What has been learned? What has been changed? What was effective about this SEA?
13 The main message to be learnt was that lung cancer can recur despite regular follow up which indicted a 5 year „cure‟. All team members are aware of suspected cancer referral guidelines. The patient was also alert to the symptoms of breathlessness and cough. He was an ex smoker. Prompt referral and diagnosis had resulted in a survival of over 6 years since the initial diagnosis and at least 5 years with a good quality of life.
Reinforcement of referral guidelines. The importance of regular follow up and vigilance for recurrence of symptoms even after 5 years.
14 Reiterated the good clinical care provided No change Gave us a chance to confirm that the diagnosis was achieved promptly and that no other reasonable course of action could have been taken.
15 The learning points in this kind of situation are to think widely in terms of possibilities with diagnosis. However in this particular case none of the above would have altered the progression of her disease and ultimate outcome in my view.
No specific changes have been put in place as a result of the above.
17 Everything worked well with this patient. Good communication re importance of traditional history and examination findings
18 Discussion about chest x-ray referral – sometimes requests have been rejected by x-ray because they do not seem to be clinically appropriate in the absence of chest symptoms.
There have been no changes – apart from increased awareness of considering chest pathology in somebody with general symptoms.
Talk about appropriateness of referral and investigations.
20 Diagnosis was speedy, as was hospital referral. No changes made. It was positive to reflect on the case – as the patient was managed well by primary and secondary care. The lung cancer referral system works better than, for example, the gynae cancer referral system where delays can extend for months.
22 General discussion about the case. It was felt that assuming our present protocols/system are adhered to, appropriate Safe Haven referrals will continue. Regarding administration, as well as making the referral details available to the Secretary, she should be informed as soon as possible of the referral with the aim that all Safe Haven referrals leave the Practice within 24 hours. All partners will be encouraged to do a similar SEA on a quarterly basis.
Interesting to look in detail at the chronological clinical presentation/investigations leading to a final diagnosis. Further similar SEAs will be performed, as although this particular episode worked well, this area is of vital importance.

43
ID What has been learned? What has been changed? What was effective about this SEA?
23 Importance of safety netting discussed. Discussion took place on help available for stopping smoking. Follow up appointment at second consultation could have been made for 10 days to check on response to repeated course antibiotics. Discussion about referrals to different hospitals.
All agreed that Wrexham provides a better service for suspected lung cancer and that an appointment will be offered there for patients prepared to travel. We did not feel there were any administrative issues that needed to be addressed. The practice reviewed the NICE guidelines. The referrer will consider immediate X-ray in smokers in any cough persisting more than 3 weeks. The practice will monitor presentations of lung cancer as significant events at clinical meetings. Looking at the 2 other cases of lung cancer diagnosed in the last year the times from presentation to x-ray were considered acceptable. One other problem is how to direct letters to the referring doctor. Ideally letters would be addressed to the referring doctor but in this case this did not happen.
Chance to review guidelines and critically examine each others‟ practice. Share experience of management of patients in different secondary care settings.
24 No lessons identified at the meetings. Not applicable. Practice reassured that action had been taken quickly and promptly.
27 The learning that has taken place is primarily the importance of considering the patient‟s occupational history, particularly in our area the possibility of exposure to asbestos.
No changes identified after discussion. N/A
28 Whether somehow she could have been persuaded by primary, secondary, tertiary care or family to change her mind sooner. May not have had significant effect as she was still able to have primary resection.
No change required. Nil specific
29 Lung cancer guidelines from NICE and SW Cancer Network have been compared with our current practice and discussed.
We have updated and agreed on the threshold for urgent CXR investigation, based on the current guidelines and patient symptoms and signs. All urgent CXRs will be made by phone. Safer follow-up arrangements and patient ECR Alerts will be used. We will discuss these and other guidelines three monthly at clinical meetings in future.
It has been used to improve clinical and administrative practice. He is hoped that this will lead to improved patient diagnosis and safety.
30 Further discussion about case. No new protocol has been amended / updated since reflecting on this case. No new things individuals would do differently.
Further discussion about case.
32 General discussion about the case within the context of the February 2005 NICE guidelines – Lung Cancer.
All doctors and nurses to be familiar with referral guidelines.
Revisited area already highlighted in previous reviews.

44
ID What has been learned? What has been changed? What was effective about this SEA?
33 General discussion about the case On this occasion am happy all was done quickly and straightforwardly. Reminds me of importance listening to patient and doing a thorough examination. There can sometimes be the problem of delayed discharge letters or clinic reviews which has impacted communication in the past, although not in this instance.
It is always useful to review presenting symptoms and signs of patients with new cancers – this lady was a non smoker and not typically at high risk lung ca. Useful to know we have not had any other similar diagnoses since this time.
34 General discussion about the case No protocols amended. We discussed the diagnosis of lung cancer prior to this in the practice – chest x-ray done the day symptoms presented, reviewed by GP that day who spoke to consultant who saw her the next day and gave diagnosis then. GPs‟ agreed that lumps in muscle need prompt USS to investigate possible sarcoma or less commonly metastatic deposit.
Discussion about a very quick patient journey from symptoms to diagnosis and a slow process. Due to very unusual nature of symptoms and lack of symptoms of lung cancer at diagnosis.
36 We discussed the usefulness of following patients up who are reluctant to come to surgery. Also the importance of cancer care questions within 6 months of diagnosis and discussion 3 monthly at palliative care meetings, together with the difficulties of a multi disciplinary approach when patient declines help from District Nurses and staff from the St David‟s Foundation.
Ensure that similar patients are discussed at Multi Disciplinary palliative care meetings even if not on the St David‟s list and then offer regular follow up with GP if patient declines District Nurse and St David‟s Nurse reviews.
It was useful to review our approach following cancer diagnosis of a patient and how to go about following up a patient who declines usual care.
37 General discussion about the case The responsibility for referring the patient to secondary care rests with the GP concerned. An abnormal CXR in a smoker is lung cancer, unless proved otherwise. I do not consider there is a need for protocol, but certainly there are lessons to be learned all round.
It gave me the chance to experience the journey made by this patient from presentation to treatment. This is undoubtedly going to improve the way abnormal radiological findings are dealt with.
38 NICE guidelines state that if the cough was present for 3 weeks, then an urgent chest x-ray should have been requested at that time. Guidelines discussed at PHCT meeting. Unsure as to how useful these are in primary care as if we referred everyone who had a cough present for more than 3 weeks – would inundate the system.
Administratively – no change is necessary. Urgent faxed information will continue to be presented to the doctor on call for immediate attention. Continued use of urgent suspected cancer proformas – faxed appropriately. Clinically – common practice is to request a chest x-ray if symptoms are persisting despite 2 courses of antibiotics. Should we now make all these referrals urgent? What do you think about the 3 week symptom guidelines as recommended by NICE?
Discussion ensued regarding actual NICE guidelines re: urgent chest x-ray requests. Should chest x-ray have been requested at 2nd visit when cough had persisted for more than 3 weeks? Relevance to primary care discussed and limitations within our system for adherence to guidelines. Positive feedback regarding quick and appropriate referral to respiratory physician. Decision made to e-mail clinical director in radiology to ask their opinion on urgent chest x-ray requests as per NICE guidelines and will feed back to PHCT.

45
ID What has been learned? What has been changed? What was effective about this SEA?
39 Consider referred pain in patients presenting with shoulder pain. Always consider possibility of dual diagnosis – do not assume could not be synchronous tumours.
Increased awareness of referred pain in cancer. Useful reminder of referred pain.
43 General discussion about the case None. When patient complained about delay from diagnosis (On CT) to treatment we were unaware that it had been so long.
44 1. Persistent shoulder pain can be a symptom of carcinoma of lung 2. A drooping eyelid can be a part of Horner's syndrome which can be part of Pancoast Ca lung 3. Not to be reluctant to expediate patient follow up with specialists if feel this is clinically necessary 4. Not to rely totally on a plain CXR to exclude Ca lung if there are other clinical suspicions 5. Apical Ca lung can cause local nerve compression and bone erosion effects before it causes a cough.
The case has been discussed by the partners and also used as a teaching example by myself (clinical tutor/trainer) my registrar and my 5th year medical student.
1. Learning about Pancoast syndrome i.e. partners, registrar, medical student, and nurses 2. Observing the involvement of the local hospice on a domiciliary basis (patient refused hospital admission) 3. It highlighted the patient's right to plan to die where they desire i.e. at home in this case 4. It highlighted how the early stages of this type of Ca lung (apical), a CXR may be negative and a cough absent
45 Some cancers present late at an untreatable stage particularly in the elderly who due to co-morbidity and frailty may not be fit for treatment.
No changes suggested No changes needed
47 It was agreed we need to maintain a high level of vigilance in high risk candidates. It was also agreed to involve the respiratory nurse re whether spirometry is in keeping with known diagnoses. There was some doubt about whether NICE guidelines have much impact on decisions.
Increased involvement of respiratory nurse has been agreed. Also increased use of spirometry to aid exclusion of diagnoses. Agreed to always do repeat chest X-rays where indicated post infection.
Heightened awareness of the limitations of chest X-rays.
48 General discussion about the case Nil specific To discuss at MDT meeting. It emphasizes the importance of full appropriate examination. It made us look at our use of referral pathways, and involved clinicians and administration staff.

46
ID What has been learned? What has been changed? What was effective about this SEA?
49 General discussion about the case The main lessons learned were to retain a high index of suspicion and not to allow “normal” chest x-rays to reduce this. There have been at least 2 cases in the last 12 months where “normal” chest x-rays have been reported in patients in whom lung cancers diagnosed within a few months. Secondly we, as a practice, will be much more proactive in pushing secondary care for patients to be seen more promptly. Particularly in this case with a delay of >4weeks between initial review in the ENT clinic & subsequent chest clinic appointment. However we are dependent upon the patients letting us know of any delays.
Good frank discussion with another other case in which there was an apparently normal chest x-ray being reviewed again. As a practice we tend to have a high index of suspicion and this case confirmed that this is necessary.
50 Despite no chest symptoms any weight loss does warrant CXR. Obviously radiologist and Chest Physician work closely together. Access via secretary using fax made referral quick and easy.
Recently implemented Urgent Cancer Suspected referral templates with dedicated fax that does not go to local hospital. New protocols would involve no discussion with secretary. To date I have not used this system but would hope it would be as efficient as the system that previously existed.
All were impressed with the speed of arranging first appointment and bronchoscopy all within 1 week. Delay in initiating chemotherapy was disappointing and feel this may be an issue the Trust should look into.
53 On reviewing the NICE guidelines it is evident that this lady should have ideally been referred on presentation since she had cough, headache and hoarse voice for > 3 weeks, however the referral was only delayed 1 week which we don‟t think would have significantly affected prognosis.
Make all aware of NICE guidelines for referral in suspected cancer. Consider the need for CXRs on diagnosis of COPD and following exacerbations.
Showed that there was good record keeping, appropriate referral. NICE guidelines weren‟t adhered to fully, but now everyone is aware.
54 If suspect Ca Lung, need urgent CXR, urgent result, urgent CT scan and urgent scan result to prompt urgent referral.
Discussion with other partners in Palliative Care Team meetings, urgency of investigations and referral if suspect Ca Lung.
It made us all think about when to refer smokers or ex smokers, with significant and suspicious symptoms, but also those with non specific symptoms. Low threshold for both really, and if the CXR is suspicious, then even lower threshold for referral to clinic or for CT scan. Interesting discussion, and well worthwhile.
55 Main concern in this case was delay in receiving x-ray report. Patients are advised to phone surgery to ensure that results have been received by the practice, as occurred in this case. Good clinical skills considered important in facilitating diagnosis.
No change to current practice has been made. We believe that the system for referral is robust, and “safety net” of informing patients to contact surgery in 2 weeks of an x-ray and also if no appointment received within 2/52 of a rapid access referral being made is useful.
Focused the mind on the importance if robust safety net to prevent missed/delayed diagnosis.

47
ID What has been learned? What has been changed? What was effective about this SEA?
56 It was agreed to continue to maintain a high index of suspicion in smokers who present with a new onset of chest symptoms and to reinforce the smoking cessation advise. It was also mentioned that the appropriate referral form should continue to be used for suspected lung cancer
There was no change in the Practice. We were please that the correct procedure was followed. The Doctor who saw him on the last occasion, who has now retired, should have checked his smoking status and given advise.
It gave the opportunity to reflect our activity and to carry out an audit to see whether we are doing things correctly.
59 General discussion about the case. Referrals were prompt and administration dealt with them appropriately as a priority as per our internal systems.
Supported good practice and improved team spirit and morale – job well done. Encouraged reflection about the need to be alert to the odd amongst the common and to be vigilant.
62 General discussion about the case All missed/delayed diagnosis are discussed in our practice multi-disciplinary meetings on a regular basis.
Missed and delayed diagnoses are treated as significant events and are discussed openly at our monthly practice meetings.
63 Main issue for the practice and focus of discussion was distress caused to family of uncertain diagnosis.
Difficult to identify any learning points about the path to diagnosis for the family but we benefited from sharing the experience of dealing with the distressed family as several doctors had been involved and this was first opportunity to compare notes formally. One feels we would deal with a case of diagnostic uncertainty more effectively next time but it is hard to say exactly how.
This case would have been discussed by the practice but the path to diagnosis would not have been discussed so thoroughly. We felt this gave the discussions a more rounded feel compared to the post diagnostic problems being discussed in isolation which is how the practice would have identified the case.
64 Chest x-ray in smokers presenting with respiratory symptoms lasting more than 4 weeks.
Change of practice protocol: Chest x-ray in smokers and non smokers presenting with respiratory symptoms of more than 4 weeks.
Learning from this event and change of clinical practice.
65 Individual and team focused on how communication of important results are given to patients and how this can be improved.
Clinical - Try to get more patients for CXR on a “next day” basis now. Administrative - Ensure that we have up to date contact numbers for all patients who are having further investigations, not assume that telephone numbers are correct. Admin staff upon receipt of results to be “actioned” (as in this case) to confirm with GP who is taking action and when. PM or secretary to take on this role, to assist the GP.
We learnt that we could have communicated the result of ongoing tests better with the patient.
67 We have learnt to be vigilant especially in those with risk factors. NICE guidelines are helpful but as this case demonstrates each patient is different and the doctor uses his own judgment and experience. Perhaps researchers should be looking at screening?
No change as appropriate management. It was a reminder not to be overly reassured by test results.
68 This case proves that a CXR is a valuable investigation and should be used in pts with abnormal symptoms or signs.
Agreed that CXR should be used for abnormal signs or symptoms. CXR should be performed in new diagnoses of COPD or late onset asthma
Reinforces the value of CXRs in investigating a patient with symptoms.
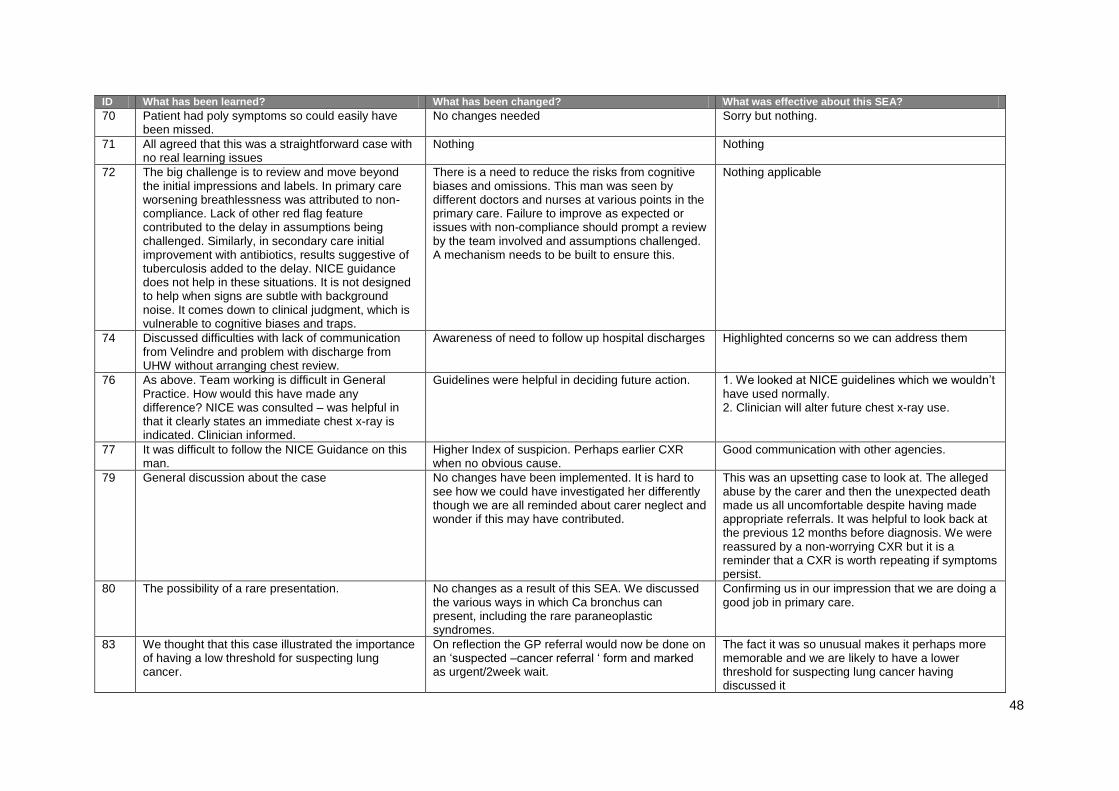
48
ID What has been learned? What has been changed? What was effective about this SEA?
70 Patient had poly symptoms so could easily have been missed.
No changes needed Sorry but nothing.
71 All agreed that this was a straightforward case with no real learning issues
Nothing Nothing
72 The big challenge is to review and move beyond the initial impressions and labels. In primary care worsening breathlessness was attributed to non-compliance. Lack of other red flag feature contributed to the delay in assumptions being challenged. Similarly, in secondary care initial improvement with antibiotics, results suggestive of tuberculosis added to the delay. NICE guidance does not help in these situations. It is not designed to help when signs are subtle with background noise. It comes down to clinical judgment, which is vulnerable to cognitive biases and traps.
There is a need to reduce the risks from cognitive biases and omissions. This man was seen by different doctors and nurses at various points in the primary care. Failure to improve as expected or issues with non-compliance should prompt a review by the team involved and assumptions challenged. A mechanism needs to be built to ensure this.
Nothing applicable
74 Discussed difficulties with lack of communication from Velindre and problem with discharge from UHW without arranging chest review.
Awareness of need to follow up hospital discharges Highlighted concerns so we can address them
76 As above. Team working is difficult in General Practice. How would this have made any difference? NICE was consulted – was helpful in that it clearly states an immediate chest x-ray is indicated. Clinician informed.
Guidelines were helpful in deciding future action. 1. We looked at NICE guidelines which we wouldn‟t have used normally. 2. Clinician will alter future chest x-ray use.
77 It was difficult to follow the NICE Guidance on this man.
Higher Index of suspicion. Perhaps earlier CXR when no obvious cause.
Good communication with other agencies.
79 General discussion about the case No changes have been implemented. It is hard to see how we could have investigated her differently though we are all reminded about carer neglect and wonder if this may have contributed.
This was an upsetting case to look at. The alleged abuse by the carer and then the unexpected death made us all uncomfortable despite having made appropriate referrals. It was helpful to look back at the previous 12 months before diagnosis. We were reassured by a non-worrying CXR but it is a reminder that a CXR is worth repeating if symptoms persist.
80 The possibility of a rare presentation. No changes as a result of this SEA. We discussed the various ways in which Ca bronchus can present, including the rare paraneoplastic syndromes.
Confirming us in our impression that we are doing a good job in primary care.
83 We thought that this case illustrated the importance of having a low threshold for suspecting lung cancer.
On reflection the GP referral would now be done on an „suspected –cancer referral „ form and marked as urgent/2week wait.
The fact it was so unusual makes it perhaps more memorable and we are likely to have a lower threshold for suspecting lung cancer having discussed it
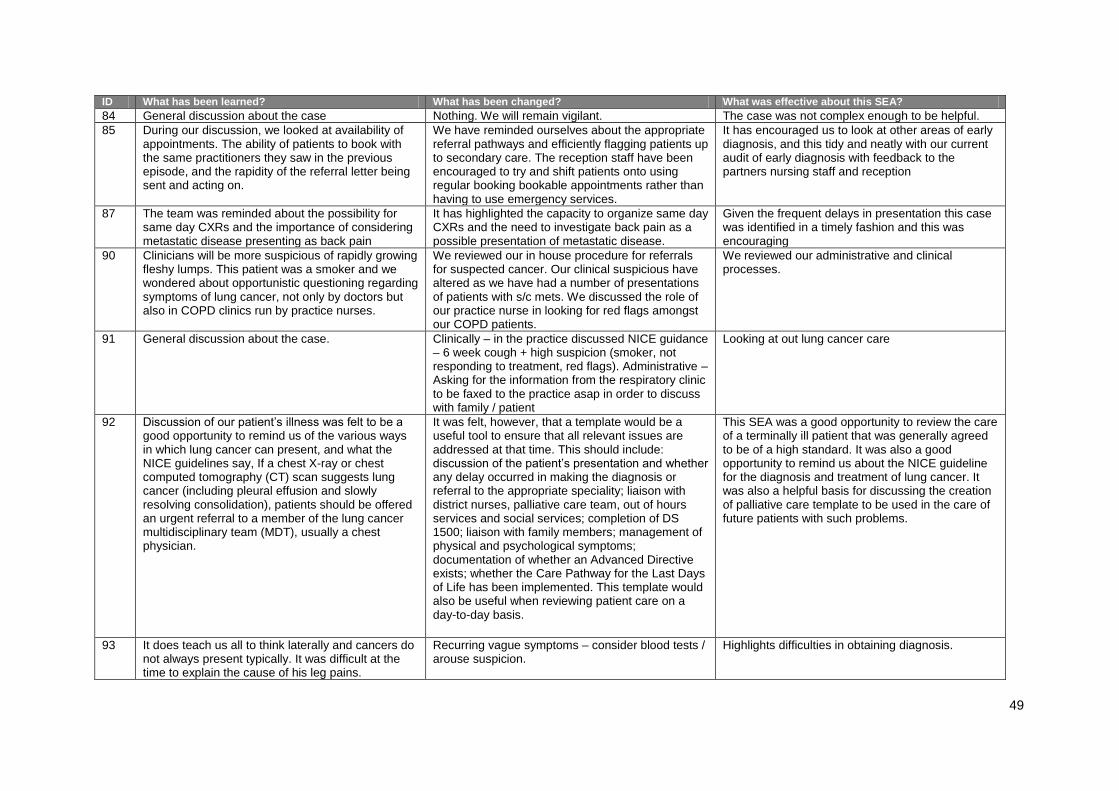
49
ID What has been learned? What has been changed? What was effective about this SEA?
84 General discussion about the case Nothing. We will remain vigilant. The case was not complex enough to be helpful.
85 During our discussion, we looked at availability of appointments. The ability of patients to book with the same practitioners they saw in the previous episode, and the rapidity of the referral letter being sent and acting on.
We have reminded ourselves about the appropriate referral pathways and efficiently flagging patients up to secondary care. The reception staff have been encouraged to try and shift patients onto using regular booking bookable appointments rather than having to use emergency services.
It has encouraged us to look at other areas of early diagnosis, and this tidy and neatly with our current audit of early diagnosis with feedback to the partners nursing staff and reception
87 The team was reminded about the possibility for same day CXRs and the importance of considering metastatic disease presenting as back pain
It has highlighted the capacity to organize same day CXRs and the need to investigate back pain as a possible presentation of metastatic disease.
Given the frequent delays in presentation this case was identified in a timely fashion and this was encouraging
90 Clinicians will be more suspicious of rapidly growing fleshy lumps. This patient was a smoker and we wondered about opportunistic questioning regarding symptoms of lung cancer, not only by doctors but also in COPD clinics run by practice nurses.
We reviewed our in house procedure for referrals for suspected cancer. Our clinical suspicious have altered as we have had a number of presentations of patients with s/c mets. We discussed the role of our practice nurse in looking for red flags amongst our COPD patients.
We reviewed our administrative and clinical processes.
91 General discussion about the case. Clinically – in the practice discussed NICE guidance – 6 week cough + high suspicion (smoker, not responding to treatment, red flags). Administrative – Asking for the information from the respiratory clinic to be faxed to the practice asap in order to discuss with family / patient
Looking at out lung cancer care
92 Discussion of our patient‟s illness was felt to be a good opportunity to remind us of the various ways in which lung cancer can present, and what the NICE guidelines say, If a chest X-ray or chest computed tomography (CT) scan suggests lung cancer (including pleural effusion and slowly resolving consolidation), patients should be offered an urgent referral to a member of the lung cancer multidisciplinary team (MDT), usually a chest physician.
It was felt, however, that a template would be a useful tool to ensure that all relevant issues are addressed at that time. This should include: discussion of the patient‟s presentation and whether any delay occurred in making the diagnosis or referral to the appropriate speciality; liaison with district nurses, palliative care team, out of hours services and social services; completion of DS 1500; liaison with family members; management of physical and psychological symptoms; documentation of whether an Advanced Directive exists; whether the Care Pathway for the Last Days of Life has been implemented. This template would also be useful when reviewing patient care on a day-to-day basis.
This SEA was a good opportunity to review the care of a terminally ill patient that was generally agreed to be of a high standard. It was also a good opportunity to remind us about the NICE guideline for the diagnosis and treatment of lung cancer. It was also a helpful basis for discussing the creation of palliative care template to be used in the care of future patients with such problems.
93 It does teach us all to think laterally and cancers do not always present typically. It was difficult at the time to explain the cause of his leg pains.
Recurring vague symptoms – consider blood tests / arouse suspicion.
Highlights difficulties in obtaining diagnosis.

50
ID What has been learned? What has been changed? What was effective about this SEA?
94 Reinforcement of Lung cancer guidelines which several doctors had not read.
All partners to refresh knowledge of lung cancer diagnosis via NICE guidelines. Practice already has partner monitoring those patients with cancer diagnosis. Continue to aim to fulfill and exceed cancer quality guideline. Nurse practitioner received further education in breaking bad news.
Encouraged reading of NICE guidelines on lung cancer-common problem so patients seen regularly with it. Refreshed and clarified diagnosis of cancer in high risk individuals. Congratulate team with regard to rapid identification of lung cancer in this instance.
95 After discussion it was felt that this lady was particularly in need of support and possibly a regular telephone review call from the GP was suggested. The breakdown in communication between the hospital and patient is quite concerning and a safety net would be to say to the patient to contact the surgery if they have not heard from the hospital within 2 weeks. Personally, I will be keeping a list of all cancer referrals and doing a telephonic follow-up after 2 weeks to confirm that they have received an appointment
A discussion with the patient in terms of support structures should take place and if family/friend support is lacking, the practice staff should offer support in the way of regular telephone calls or offer the availability of follow-up consultations. As mentioned before, it would be seen as a safety net to contact this group of patients 2 weeks after referral to verify that they have had correspondence from the hospital.
This discussion emphasized again the vulnerability of this group of patients. It also made us think about consultation skills and how we break bad news and how important it is to offer a follow-up service. As this lady has an inoperable carcinoma her name will be added to the palliative care list and be discussed at our next 3 monthly PHCT palliative meeting.
97 It was felt that this had been an useful exercise in understanding the background and relevant history regarding diagnosis and treatment of this patient. The NICE guidelines were discussed, it was felt that they were useful information regarding which symptoms should alert you for sending patients for chest x-rays. There was a lack of knowledge regarding the type of chemotherapy that the patient has had. It was felt that a more detailed letter from the oncologist regarding specific potential side effects would be useful.
The potential respiratory problems at the end of life were discussed and the possibility of using the occupational health team and a respiratory specialist nurse. Acute medication to help with symptom relief was discussed with the GPs and DNs. Individual GPs have been directed to the BMJ learning modules to do with chemotherapy side effects to improve knowledge in this area. Also hand-outs regarding respiratory problems at the end of life.
Opportunity to discuss in depth about the process of diagnosis and subsequent treatment of this lung cancer patients. Would be useful to follow this approach for many of our patients. All members of the team felt they had a more in depth knowledge of the patient and potential problems which hopefully would improve the quality of his care.
98 General discussion about the case. Nothing changed as access and diagnosis proceeded well and support in place.
Useful to highlight case management and probable End of Life Care issues Good communication in Practice essential in order to facilitate best care
100 Following his death and the family attempting resuscitation I will be reviewing the way I prepare families for the expected death of patients. I know the patient would not have chosen to be resuscitated. I will discuss this at our next quarterly SEA meeting.
As the patient refused practically all interventions – he did not conform to any protocol!
Useful to discuss such late presentation, informed choice, our discomfort with his decision and how to manage that.

51
ID What has been learned? What has been changed? What was effective about this SEA?
101 We need to check at an early stage of involvement on how much the patient knows of his condition and prognosis, and what he understands from what he has been told. We also need to liaise with the oncologist‟s regarding deterioration of the patient. We need to avoid this group of patients being on General Medical intake (with advice and agreement of all parties).
The doctors attending the meeting decided to take more care with the detail of communication at an early stage with a palliative care patient and to check their understanding of the condition. It was thought that home care may be more appropriate with the patient‟s and relatives consent and consistency was required and with drug regimes. Patient and relative consent was needed regarding place of care and therapy. Services of the voluntary sector (e.g. Marie Curie) and other supportive organizations e.g. SPICE need to be involved at an earlier stage.
We were able to demonstrate the importance of good communication in palliative care.
102 General discussion about the case. None Relevance of atypical chest pain
104 Discussed our management of haemoptysis – if seen again to organize URGENT CXR. Urgent respiratory referral through safe haven pathway if lesion is found on CXR. To refer every slight streak of blood may swamp the system was noted by some GPs. We felt that a quicker pathway once lesion has been identified on initially X-ray would be useful - direct referral from radiology to the appropriate speciality?
Copies of brief summary of NICE guidance for suspected lung cancer distributed to GPs so that they can read these and place on their notice boards. GP involved is due to retire soon and other GP is a locum so not with practice in long term. No issues with communication in our practice. GPs aware early referral to chest physician and for CXR necessary for haemoptysis in future. Could do a haemoptysis/ lung cancer follow up audit next year. Limitations to this are haemoptysis may not be Read coded in the notes.
Raised awareness of difficulties our patients face in getting an early diagnosis with cancer.
105 It sharpened awareness of lung cancer – in this patient presenting with a short history of cough and a very small amount of haemoptysis, in an ex-smoker of more than 10 years
No protocols were changed. The important points in the process were safety netting, awareness of red flag symptoms, prompt CXR referral, prompt chest clinic referral and double checking follow up.
Opportunity to discuss a case in detail as a team. Confirmation that current systems seem to be effective. Raising awareness of lung cancer.
107 General discussion about the case. The Nurse Practitioner was refreshed her knowledge of „red flag‟/‟alarm‟ symptoms and signs
It was reassuring to see that in this case a speedy diagnosis was made despite the fact that the long term prognosis for the individual concerned is not good. Certain local procedures could be tightened up e.g. radiologists forwarding „red flag‟ chest X-ray results directly to the appropriate consultant.
108 I don‟ know who our „Cancer network lead GP‟ is! Nothing has changed yet. Hopefully my reflections will generate discussion and develop a pathway to address referral times.
It seems to demonstrate that there is little dialogue between primary and secondary care – except the sending of outpatient letters!

52
ID What has been learned? What has been changed? What was effective about this SEA?
109 Discussion in clinical practice meetings-awareness of spectrum of severity of clinical symptoms and signs. Awareness of impact of recent psychosocial stressors e.g. job loss ?low mood as being contributory to presentation Relevance of shoulder tip pain with elevated inflammatory markers.
No change in protocols. Change in my personal practice and to trust intuition/gut feelings despite possible red herrings To persevere with requesting appropriate investigations in the face of rapid discharges from secondary care
Involved multidisciplinary team working with district nursing teams, GP and Macmillan nursing input It did highlight the central role of the GP in diagnosis and palliative management. It highlighted the benefits of a strong doctor patient relationship and joint decision making re final pathways
112 This case was felt to be particularly worrying [along with a few others] where the chest consultant was disputing the radiologist‟s findings and then being found to be incorrect. I believe the Royal College of Radiologists arranged a review of his cases and some disciplinary action was taken. I do not work in the hospital and have no details. I know that he was off work for a time but is back at work now.
Continue to listen to patients and have a high index of suspicion for serious disease even if age makes it less likely. Use quick access routes for investigations when appropriate. Only use the word „urgent‟ when it truly is. USC for urgent suspected cancer and chase patients if there is no feedback after 2 weeks. I don‟t believe that we needed to change anything at our end but filling in SEA forms can bring about [unexpectedly] major effects.
It resulted in a change in a consultant‟s defective modus operandi.

53
ID What has been learned? What has been changed? What was effective about this SEA?
113 1.All letters are coded into the patients problems page in the electronic records but the gastroenterology OPD letter hadn‟t been coded into the records and indeed investigations planned by the Gastroenterologists weren‟t performed. 2.CKD4 was known before but wasn‟t coded but this was because until recent years CKD hasn‟t been classified as it is now 3.Highlight abnormal x-rays more clearly when expediting 4. The referral to secondary care seemed quick and efficient once it was made but there seemed to be a lack of urgency and leadership at times. The Locum Consultant assessment seemed to put off scoping/biopsying the area of concern because of the close proximity to the aorta. Perhaps if the specialist felt it wasn‟t within their comfort zone that they should have sought further help 5. Radiology reports show some discrepancies?
Misinterpretation as when the definitive report was
issued in 8/2009 the nodule was reported as been
on the 11/2008 film but this had not been reported
then.
1. Reminder to Partners in the Practice to continue to code ALL significant diseases and operations and consultations in secondary care. i.e. OGD/FOS-if seen in clinic for assessment and no tests are ordered then a clinical entry should be made e.g. "seen by gastroenterology” and free text a short resume of the OPD attendance. ACTION BY THE PARTNERS 2. Reminder to look for and code CKD patients and manage according to NICE guidelines. ACTION BY PARTNERS 3. Abnormal results after referral-need to send letter and results to relevant secretary-fax through to the secretary-ring to confirm received and also obtain evidence that an appointment had been made. ACTION BY PARTNERS AND SECRETARIES IN THE PRACTICE. 4. Issues 4 and 5 are more difficult to influence-Consistent Leadership and Decision making needed particularly when the Lead Consultant is absent? CANCER NETWORK COULD BE INVOLVED HERE.
1.Systems are in place in the Practice but we need to monitor them 2. Diagnosis when made led to rapid MDT/Decision making and sadly in this case even if it had been made quicker the patient‟s general condition would have contraindicated invasive/aggressive treatment.
114 General discussion about the case. All team members are alert to the necessity of early referral for haemoptysis. We are also in a different LHB from our nearest DGH, which makes access to reports and results a little difficult. We are working on gaining access to their CWS.
I will work on access to results at the DGH personally
115 General discussion about the case. Need to be vigilant for symptoms suggestive of carcinoma of the lung
Reflection on diagnosis but also on future management.
117 This diagnosis was discovered opportunistically. The patient had no previous symptoms or early signs that may have been picked up.
We have considered this case and feel that there is very little change that can be put into place.
There was very little to learn from this SEA.

54
ID What has been learned? What has been changed? What was effective about this SEA?
118 We should continue to have a high index of suspicion in any smoker or ex smoker presenting with respiratory symptoms, and emphasize the importance of follow up if any symptoms fail to resolve. Any patient with persisting symptoms should have a CXR even if, clinically the chest is clear. Every new COPD patient should have a routine CXR.
No change to current practice as a result of this case.
Useful discussion about lung cancer referrals.
119 Most of or discussion focused on our failure to engage this patient and his wife in our palliative care role and the resulting piecemeal care that he had in his last weeks. This was not for want of trying and fell outside our control.
This case has stimulated reflection but no substantial change in practice has resulted.
Thought and reflection in the team. Why so few cases of lung cancer? Only 5 in last two years. Practice population 8,500.
121 The need to remain vigilant during “routine” reviews of patients and also to encourage patients with chronic disease to report any unexpected and / or persistent symptoms was also discussed. The NICE guidelines on referral were discussed briefly but in this case they were largely bypassed as the investigations were promptly arranged so that by the time the patient was seen in clinic the diagnosis had been made.
No specific changes have been implemented following this case but we will continue to review cancer diagnoses as significant events.
Reinforcing the communication channels between members of the clinical team
123 The main point of learning was to have a higher index of suspicion when physical condition not so good – had also been seeing gastroenterology for ulcerative colitis increased urgency for investigation of haemoptysis as NICE guidelines suggest.
Practice will continue SEA for diagnosis of lung tumours. All clinicians are updating knowledge of NICE guidelines as time had lapsed since some had read them. Maintain a high index of suspicion in at risk patients.
Highlighted importance of prompt investigation of haemoptysis. Reinforced considering multifactorial problems causing symptoms.
124 General discussion about the case. As already said as we are a small practice it is easier to have good communication. One improvement that could have been made was if the patient had told us about the cancellation of the MRI, especially as he was attending surgery regularly for INR. If we had known this our secretary could have chased up the appointment. It is normal practice here for nurses and HCA to ask patients when attending if they are feeling well.
Looking back over the patient‟s notes it showed us that really there were only a few months between patient showing symptoms and diagnosis. Unfortunately, while the patient is not too bad, there has been significant spread of the disease.
125 This patient was managed in the primary care as per her wishes and we realized the importance of team work for the benefit of the patients
Following the meeting we amended the protocol for rapid access referral to chest clinic
Knowing the patient and past history were important to investigate early. In this case she was a heavy smoker.
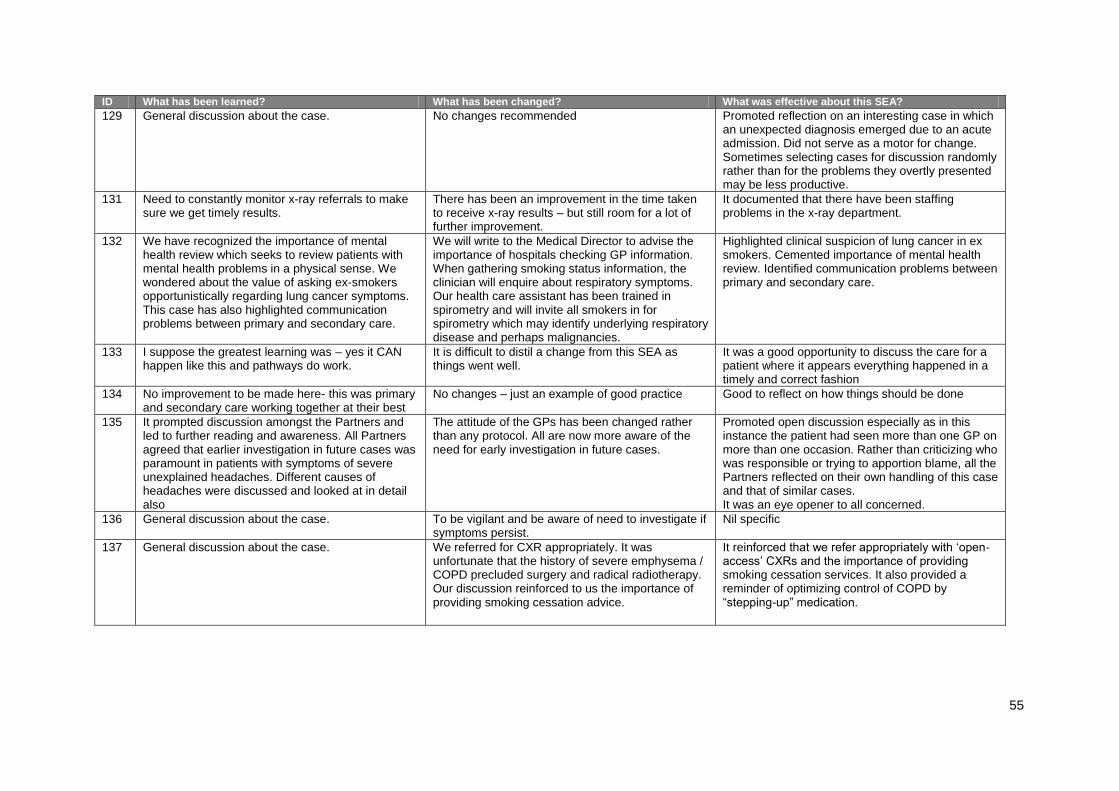
55
ID What has been learned? What has been changed? What was effective about this SEA?
129 General discussion about the case. No changes recommended Promoted reflection on an interesting case in which an unexpected diagnosis emerged due to an acute admission. Did not serve as a motor for change. Sometimes selecting cases for discussion randomly rather than for the problems they overtly presented may be less productive.
131 Need to constantly monitor x-ray referrals to make sure we get timely results.
There has been an improvement in the time taken to receive x-ray results – but still room for a lot of further improvement.
It documented that there have been staffing problems in the x-ray department.
132 We have recognized the importance of mental health review which seeks to review patients with mental health problems in a physical sense. We wondered about the value of asking ex-smokers opportunistically regarding lung cancer symptoms. This case has also highlighted communication problems between primary and secondary care.
We will write to the Medical Director to advise the importance of hospitals checking GP information. When gathering smoking status information, the clinician will enquire about respiratory symptoms. Our health care assistant has been trained in spirometry and will invite all smokers in for spirometry which may identify underlying respiratory disease and perhaps malignancies.
Highlighted clinical suspicion of lung cancer in ex smokers. Cemented importance of mental health review. Identified communication problems between primary and secondary care.
133 I suppose the greatest learning was – yes it CAN happen like this and pathways do work.
It is difficult to distil a change from this SEA as things went well.
It was a good opportunity to discuss the care for a patient where it appears everything happened in a timely and correct fashion
134 No improvement to be made here- this was primary and secondary care working together at their best
No changes – just an example of good practice Good to reflect on how things should be done
135 It prompted discussion amongst the Partners and led to further reading and awareness. All Partners agreed that earlier investigation in future cases was paramount in patients with symptoms of severe unexplained headaches. Different causes of headaches were discussed and looked at in detail also
The attitude of the GPs has been changed rather than any protocol. All are now more aware of the need for early investigation in future cases.
Promoted open discussion especially as in this instance the patient had seen more than one GP on more than one occasion. Rather than criticizing who was responsible or trying to apportion blame, all the Partners reflected on their own handling of this case and that of similar cases. It was an eye opener to all concerned.
136 General discussion about the case. To be vigilant and be aware of need to investigate if symptoms persist.
Nil specific
137 General discussion about the case. We referred for CXR appropriately. It was unfortunate that the history of severe emphysema / COPD precluded surgery and radical radiotherapy. Our discussion reinforced to us the importance of providing smoking cessation advice.
It reinforced that we refer appropriately with „open-access‟ CXRs and the importance of providing smoking cessation services. It also provided a reminder of optimizing control of COPD by “stepping-up” medication.

56
ID What has been learned? What has been changed? What was effective about this SEA?
138 General discussion about the case. One of the issues that came out of this audit was knowing when to refer for chest x-ray, according to NICE guidelines. The inclusion criterion for this referral was reiterated by all clinicians. This means in future patients with significant history will be referred for x-ray when they meet these criteria. The GPs will have to refer to the guidelines if a patient falls within these criteria.
It was useful to understand the need for proper communication between professionals and the need to respect patient choice. This case was managed as well as it could have been in the circumstances, especially as the patient was refusing any further treatment.
139 General discussion about the case. The Practice discussed how we could develop a system to try and deal with patients who are smokers and do not attend surgery on a regular basis. The development of the process will be added to the Practice‟s Strategic Plan which is the responsibility of the Business Manager, who will address this matter during the next few months.
Although this was an unusual case due to the rapidity of death from diagnosis, the SEA focused the Practice team on looking inwardly on our own Practices even though, in this case, we could not have done anything further to prevent the death of the patient. The Practice could have written off the need to do anything due to the circumstances, but the SEA has focused our thoughts into what we may be able to do to identify the onset of this disease at an earlier stage.
140 General discussion about the case. Clinical issues arising - none. Admin issues - none Discussion of this diagnosis support the effectiveness of team working and helped to feedback good practice in following administrative protocols to our admin staff and help them to see the real benefits to good patient care that their contributions and patients have even though they are not face to face
142 The main topic of discussion in this area was around the need to be vigilant when assessing new or changing symptoms in patients with chronic conditions. Although not strictly relevant in this case, we discussed the need to remain aware that new chest symptoms may not simply be related to their diagnosis to COPD. We also discussed false negative Chest X-ray results and the need to pursue further investigation if there is doubt over the diagnosis, particularly in the presence of red flag symptoms. We also discussed the difficulty in remaining objective when dealing with “difficult” patients. The pitfalls of over-investigating or overlooking symptoms in patients with communication or relationship difficulties were mentioned.
No specific changes have been made to practice policy.
The main outcome of the SEA was an increase in awareness of managing new symptoms in patients with chronic illness

57
ID What has been learned? What has been changed? What was effective about this SEA?
143 I am not sure that the referral guide was much helpful in this circumstances
No changes clearly arose. The effectiveness of team working between practice staff and also secondary care.
144 The overwhelming message of this case was how hard lung cancer can be to spot – this man proved to have widespread disseminated disease only three months after a clear CXR.
This case is a reminder to always consider alternative causes of a headache but there was a feeling at the meeting that this presentation was going to be very hard to spot early on. We speculated ion whether the gentleman had withheld reports of chest symptoms.
This patient would not have been routinely discussed and the practice found it a useful case to review. We were pleased to have noted the excellent record keeping of our HCA when the patient refused her advice to see a doctor.
145 The practice has noticed a number of diabetics with apparently very well controlled diabetes have had cancer, and it is something that we now consider if there is an improving HBA1c in the absence of an obvious explanation
We do not believe that any change in process could have improved the outcome in this case, and more effective treatment of small cell carcinoma of the lung is required
This was a complicated presentation due to the disease being advanced at diagnosis – it reinforces the need to urgently investigate dysphagia at any level.
147 Not to rely on other disciplines to have extended pathology. In this case Walton ITU when being treated for chest infection complicating disectomy
Nothing applicable. Enhances the fact that we dealt with presentation correctly.
150 With regard to individual team members‟ reflections: - Doctor 1 realises that ongoing bony pain in presence of raised ARP‟s in a long term smoker could have been looked at more closely even in the presence of a normal hip x-ray. - Doctor 2 realises CXR could have been done earlier irrespective of perceived failings in secondary care - Doctor 3 recognises that effective communication between team members may have led to a more joined up plan for investigations/treatment.
Plans to change - Acknowledgement that weekly meetings have fallen by the wayside and acceptance that we have no real forum to discuss clinical matters on a regular basis. Plans to reinstate these to be discussed more fully at next Practice Meeting. Actions agreed – Acceptance that we need to have a lower threshold for investigation in smokers and also that we should not necessarily be reassured by an unremarkable hospital admission/discharge. This has in fact been a theme recognised from previous SEAs and we still have to learn from this.
Opportunity to discuss the case together and possibly ventilate some background unease concerning the delay in diagnosis. Agreement to learn form the case and possibly taking forward a weekly clinical meeting, where such cases can be discussed.
151 Certainly did NOT meet NICE Guidelines because there was no appointment. We could not influence that.
Nil specific Review on “breaking bad news”. - Served to highlight shortcomings of current
Lung Cancer Services. - To encourage team members to investigate
appropriate Ix during waiting phase.
154 We learned that CXR is recommended in patients with chest or shoulder pain if not resolved within 3 weeks, and in patients with hoarseness, even if they are not smokers. We also noted that referral is advised whilst CXR result is awaited in smokers with haemoptysis.
We are now aware of NICE recommendations and indications for CXR. This will change our practice, and we will review this at our next SEA meeting.
Very useful discussion around NICE guidelines. They would not have changed the outcome in this case, but may reduce time to diagnosis in future cases.

58
ID What has been learned? What has been changed? What was effective about this SEA?
155 The importance of communication and picking up the telephone. Also , thinking beyond the obvious – the „cellulitis‟ was in reality flitting superficial thrombophlebitis with secondary infection. Always being aware of the potential for a serious diagnosis even when the presentation seems simple (although there was clear safety netting here). Being willing to push the system when necessary (this would have taken much longer if we had waited for an X-ray report and referred on a form rather than a phone call)
We have been more likely to directly contact consultants – either by phone or by email. We have discussed this as being a useful tool. We are pushing to have access to X-ray images via the link with the hospital.
It was overall a case that had gone well, but there were still useful issues to look at from it
156 Reminder to all clinicians. Consider referring if red flags are present (haemoptysis in a smoker), possibly prior to any further investigations being done/results received.
Discussion of case and reminder to refer early. Flag up Record e.g. “REVIEW RE: XYZ”
Served as a powerful reminder to pay attention to Red Flags and not to wait for patient to return.
158 We discussed the NICE guidelines when we talked about this as a SE. We all needed to revise the recommendations regarding an urgent chest x-ray when a patient presents with unexplained cough for more than 3 weeks. We felt that this is sometimes difficult as many smokers cough all the time anyway, and they tend to be a group who do not attend the surgery for things such as spirometry as they are worried about being told to stop smoking.
We have not changed any protocols but the clinicians in the team have re read the NICE guidelines and are now more aware of the clinical guidelines regarding diagnosis of lung cancer.
We thought we knew what was in the NICE guidelines Regarding diagnosis and treatment of lung cancer, but when we all discussed this we realized that we needed to revise the recommendations.
159 General discussion about the case. Local and NICE guidelines have been reviewed and discussed. Consideration was given to a practice protocol for these referrals but it was decided that this was not necessary as we have local guidelines which work well and of which all practitioners are aware.
Reflection on this case raised awareness for our GP Registrars and showed them how this kind of problem should be handled. It also provided assurance that on the practical side our practice team dealt with this case very well indeed.
161 Nil Nothing This is not exactly a SEA for the surgery
162 Sometimes diagnosis can proceed smoothly with minimal delay and still be of an inoperable tumour. Could have brought forward GP review once CXR report received which would have shortened time to diagnosis. This would have been our usual practice but was not done as CT scan had already been booked.
Re-emphasised that all haemoptysis should be investigated with CXR Re-iterated practice policy not to refer under 2w rules until patient has been seen, but that this appt may need to be brought forward.
It demonstrates that when all systems work well rapid diagnosis can be made whilst still leaving a poor prognosis.
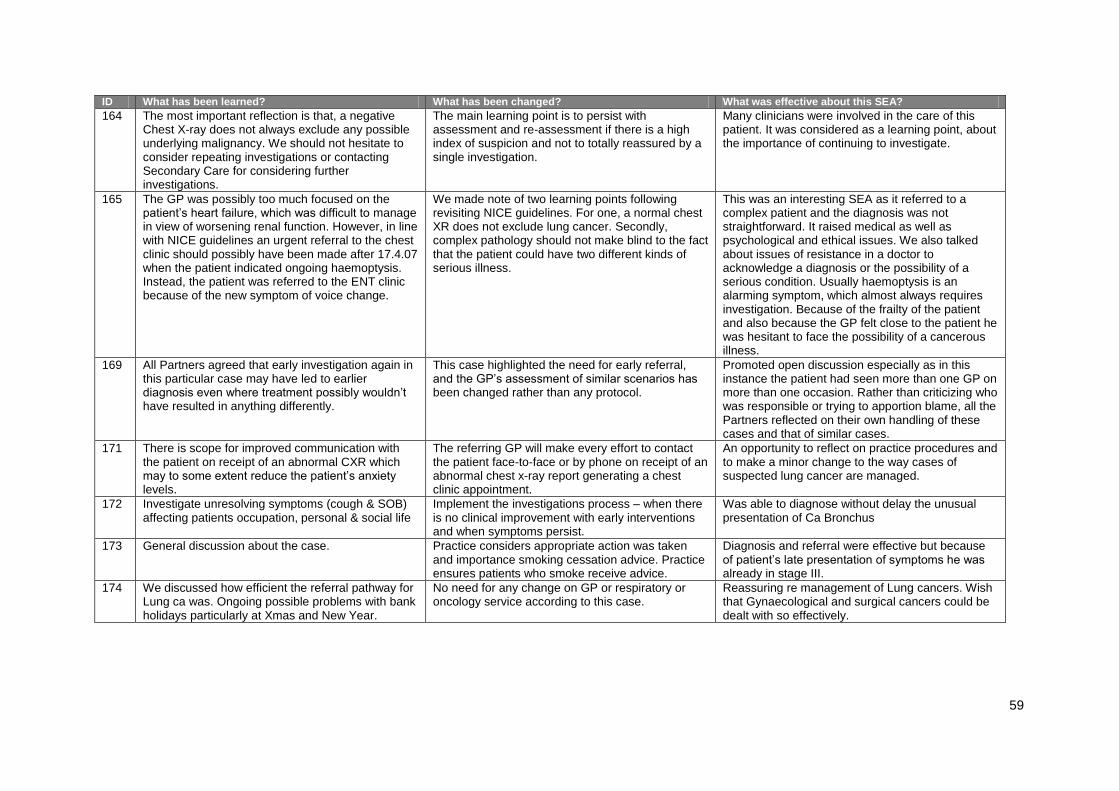
59
ID What has been learned? What has been changed? What was effective about this SEA?
164 The most important reflection is that, a negative Chest X-ray does not always exclude any possible underlying malignancy. We should not hesitate to consider repeating investigations or contacting Secondary Care for considering further investigations.
The main learning point is to persist with assessment and re-assessment if there is a high index of suspicion and not to totally reassured by a single investigation.
Many clinicians were involved in the care of this patient. It was considered as a learning point, about the importance of continuing to investigate.
165 The GP was possibly too much focused on the patient‟s heart failure, which was difficult to manage in view of worsening renal function. However, in line with NICE guidelines an urgent referral to the chest clinic should possibly have been made after 17.4.07 when the patient indicated ongoing haemoptysis. Instead, the patient was referred to the ENT clinic because of the new symptom of voice change.
We made note of two learning points following revisiting NICE guidelines. For one, a normal chest XR does not exclude lung cancer. Secondly, complex pathology should not make blind to the fact that the patient could have two different kinds of serious illness.
This was an interesting SEA as it referred to a complex patient and the diagnosis was not straightforward. It raised medical as well as psychological and ethical issues. We also talked about issues of resistance in a doctor to acknowledge a diagnosis or the possibility of a serious condition. Usually haemoptysis is an alarming symptom, which almost always requires investigation. Because of the frailty of the patient and also because the GP felt close to the patient he was hesitant to face the possibility of a cancerous illness.
169 All Partners agreed that early investigation again in this particular case may have led to earlier diagnosis even where treatment possibly wouldn‟t have resulted in anything differently.
This case highlighted the need for early referral, and the GP‟s assessment of similar scenarios has been changed rather than any protocol.
Promoted open discussion especially as in this instance the patient had seen more than one GP on more than one occasion. Rather than criticizing who was responsible or trying to apportion blame, all the Partners reflected on their own handling of these cases and that of similar cases.
171 There is scope for improved communication with the patient on receipt of an abnormal CXR which may to some extent reduce the patient‟s anxiety levels.
The referring GP will make every effort to contact the patient face-to-face or by phone on receipt of an abnormal chest x-ray report generating a chest clinic appointment.
An opportunity to reflect on practice procedures and to make a minor change to the way cases of suspected lung cancer are managed.
172 Investigate unresolving symptoms (cough & SOB) affecting patients occupation, personal & social life
Implement the investigations process – when there is no clinical improvement with early interventions and when symptoms persist.
Was able to diagnose without delay the unusual presentation of Ca Bronchus
173 General discussion about the case. Practice considers appropriate action was taken and importance smoking cessation advice. Practice ensures patients who smoke receive advice.
Diagnosis and referral were effective but because of patient‟s late presentation of symptoms he was already in stage III.
174 We discussed how efficient the referral pathway for Lung ca was. Ongoing possible problems with bank holidays particularly at Xmas and New Year.
No need for any change on GP or respiratory or oncology service according to this case.
Reassuring re management of Lung cancers. Wish that Gynaecological and surgical cancers could be dealt with so effectively.
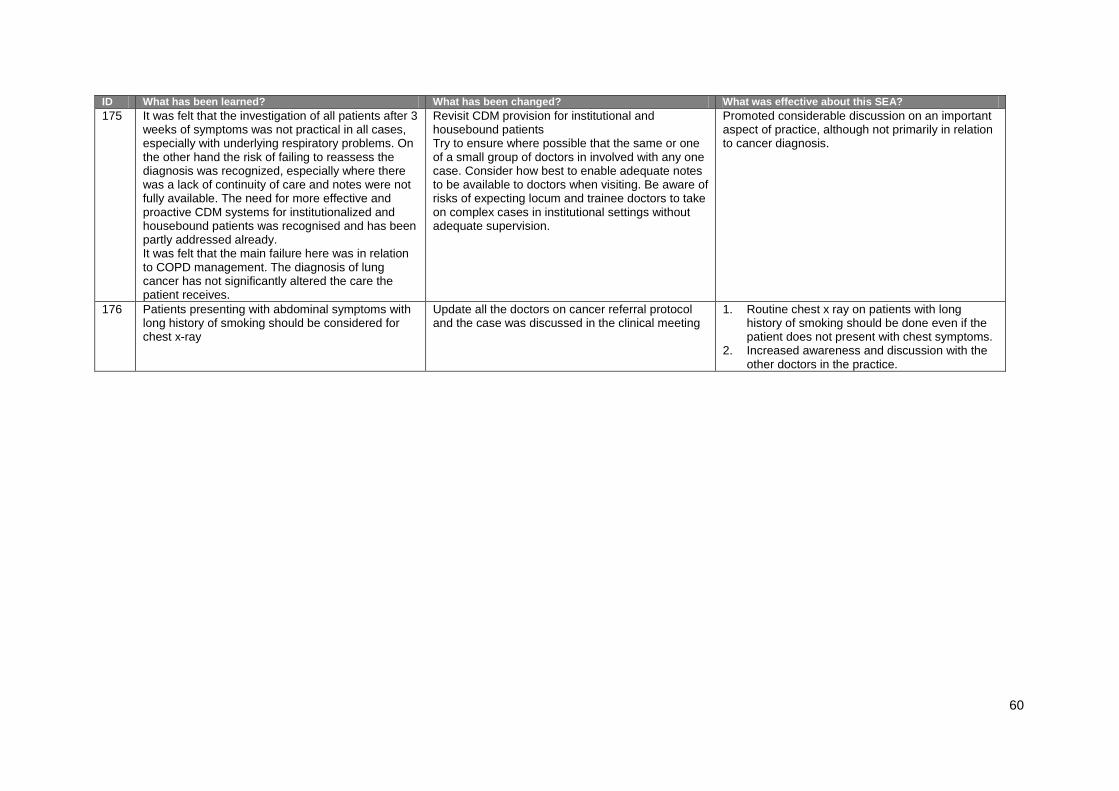
60
ID What has been learned? What has been changed? What was effective about this SEA?
175 It was felt that the investigation of all patients after 3 weeks of symptoms was not practical in all cases, especially with underlying respiratory problems. On the other hand the risk of failing to reassess the diagnosis was recognized, especially where there was a lack of continuity of care and notes were not fully available. The need for more effective and proactive CDM systems for institutionalized and housebound patients was recognised and has been partly addressed already. It was felt that the main failure here was in relation to COPD management. The diagnosis of lung cancer has not significantly altered the care the patient receives.
Revisit CDM provision for institutional and housebound patients Try to ensure where possible that the same or one of a small group of doctors in involved with any one case. Consider how best to enable adequate notes to be available to doctors when visiting. Be aware of risks of expecting locum and trainee doctors to take on complex cases in institutional settings without adequate supervision.
Promoted considerable discussion on an important aspect of practice, although not primarily in relation to cancer diagnosis.
176 Patients presenting with abdominal symptoms with long history of smoking should be considered for chest x-ray
Update all the doctors on cancer referral protocol and the case was discussed in the clinical meeting
1. Routine chest x ray on patients with long history of smoking should be done even if the patient does not present with chest symptoms.
2. Increased awareness and discussion with the other doctors in the practice.

















