Capacitation-IVM culture of oocytes from small follicles in PCOS patients Johan Smitz & IVM Team Follicle Biology Laboratory Center for Reproductive Medicine Vrije Universiteit Brussel (VUB) Brussels , Belgium
Transcript
Capacitation-IVM culture
of oocytes from small follicles
in PCOS patients
Johan Smitz & IVM Team
Follicle Biology Laboratory
Center for Reproductive Medicine
Vrije Universiteit Brussel (VUB)
Brussels , Belgium
Conflict of interest declaration
Speaker fees from :
BioMérieux,
Besins Female Healthcare,
Ferring Pharmaceuticals,
Merck
LEARNING OBJECTIVES
Acquire knowledge on :
- oocyte development in small human follicles
- oocyte Maturation in-vitro (IVM) :
recent developments
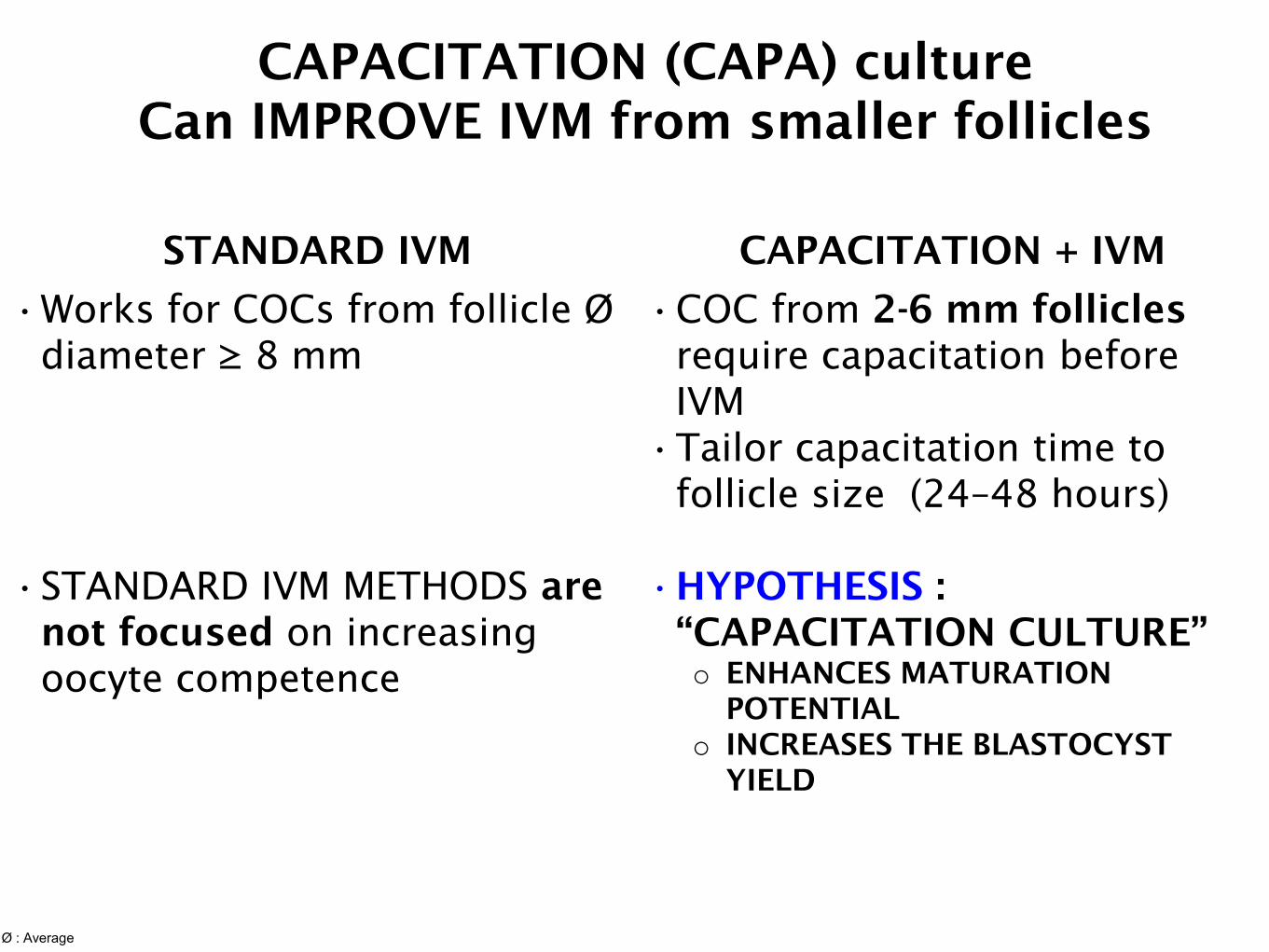
- improved method for clinical IVM :
CAPACITATION – IVM (“CAPA”)
IVM : what is it ?
DEFINITION
- is NOT a truncated IVF
- is NOT ‘rest’ material from IVF
DeVos et al. Human
Reproduction, 2016
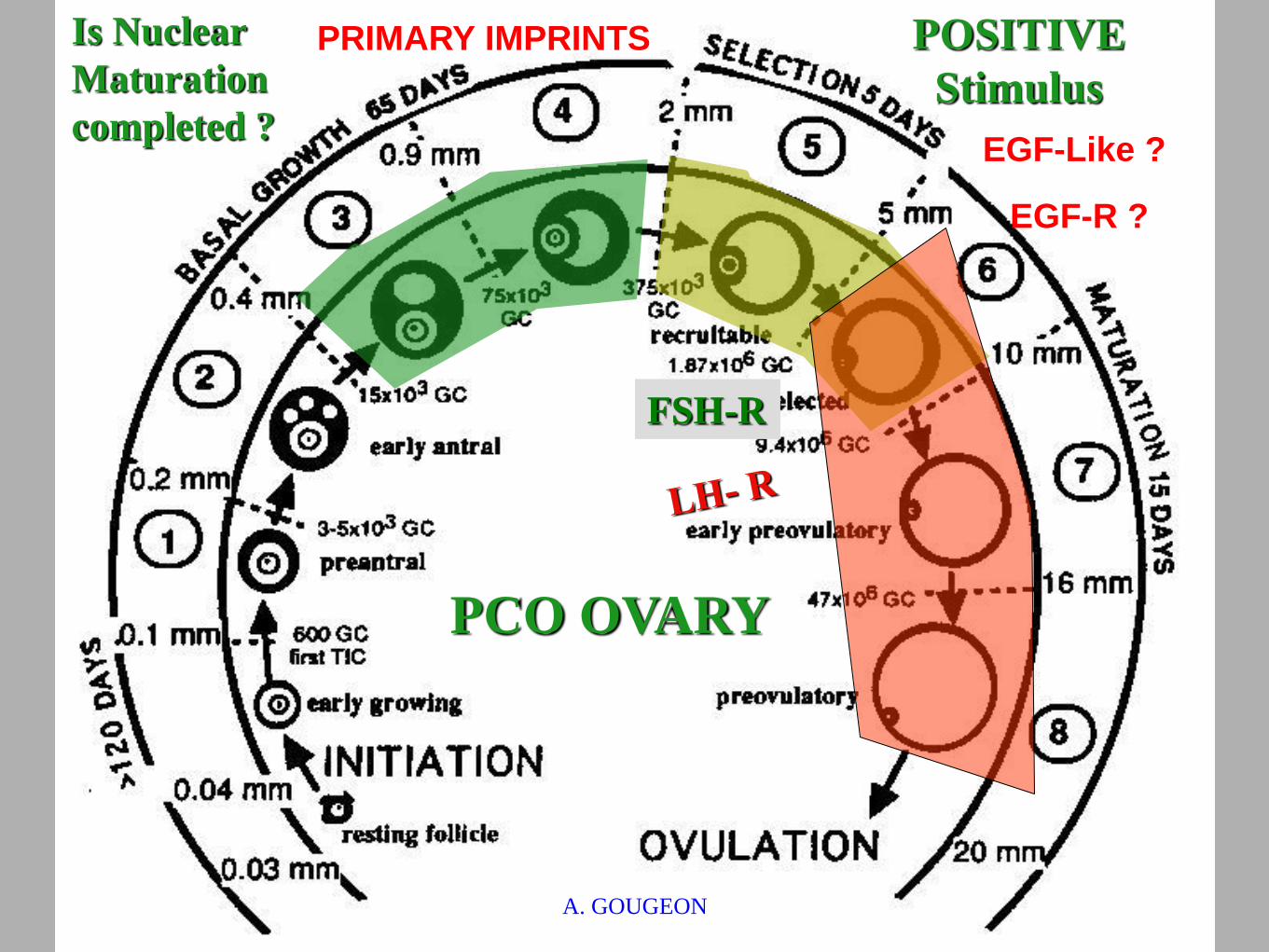
SELECTION
PROCESS
Gougeon A. Human Reproduction 1986;2:81 - 87.
HUMAN FOLLICLE DEVELOPMENT
A. GOUGEON
IVF
Why IVM systems stay under-utilised
1- FOLLICLE HETEROGENEITY
the HCG injection on 6-12 mm follicles
causes asynchronous maturation of oocytes
2 - INAPPROPRIATE SIGNALLING is
induced “spontaneous” vs “induced” meiosis
re-initiation
Effect of hCG triggering in IVM
( Son et al., RBM Online 2008 )
compact cumulus
expanded
cumulus
GV
GV
MI
MII
PR 23,3%
PR 40%
Post HCG = In vivo + in vitro
maturation
Type of cumulus-oocytes obtained and OUTCOME
NOTE :
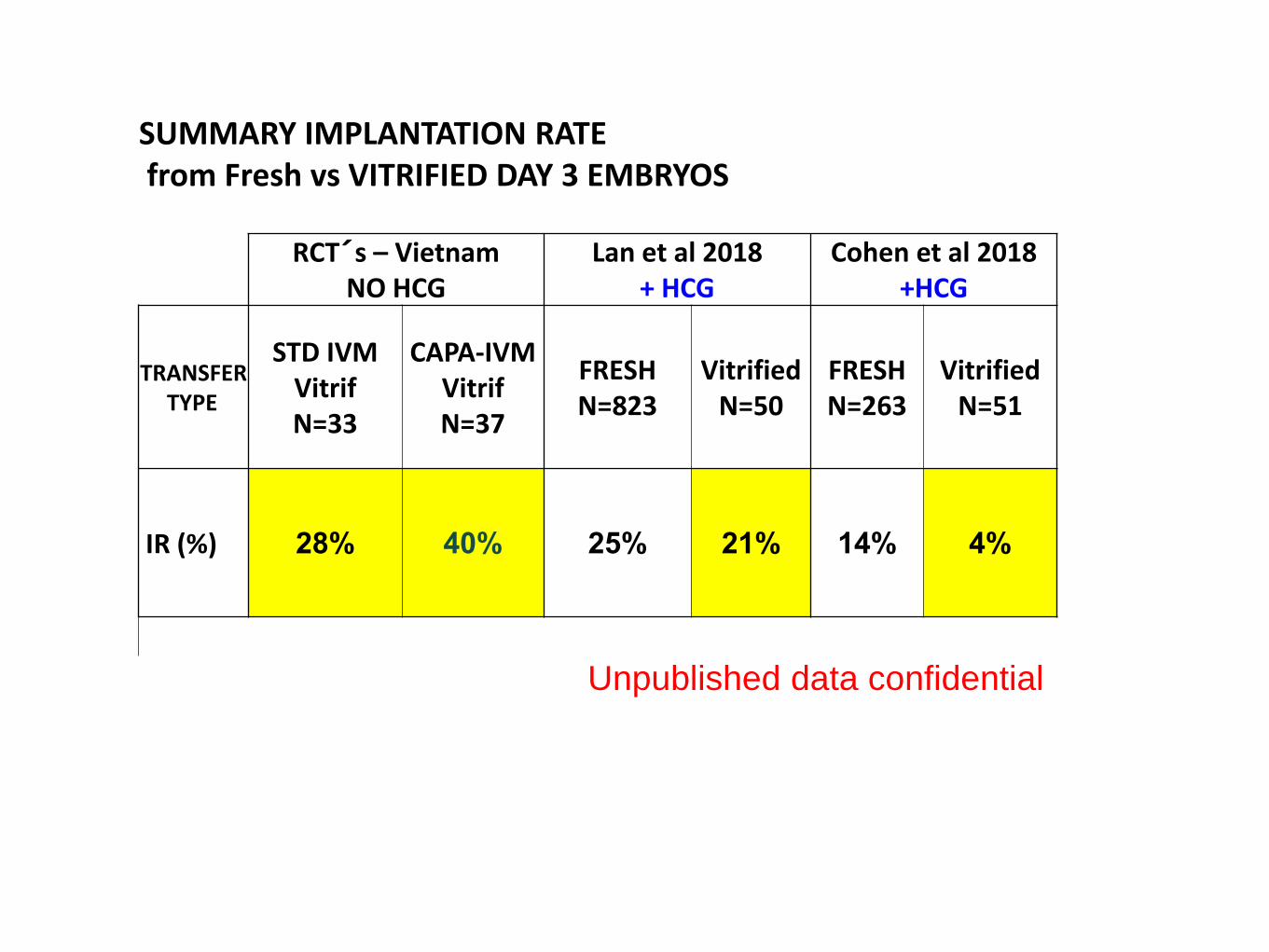
What the data show on “+hCG” - IVM
Generally low implantation rates
Increased early pregnancy loss
Need for multiple ET(2-4 Embryos)
Results: hesitant adoption by clinics
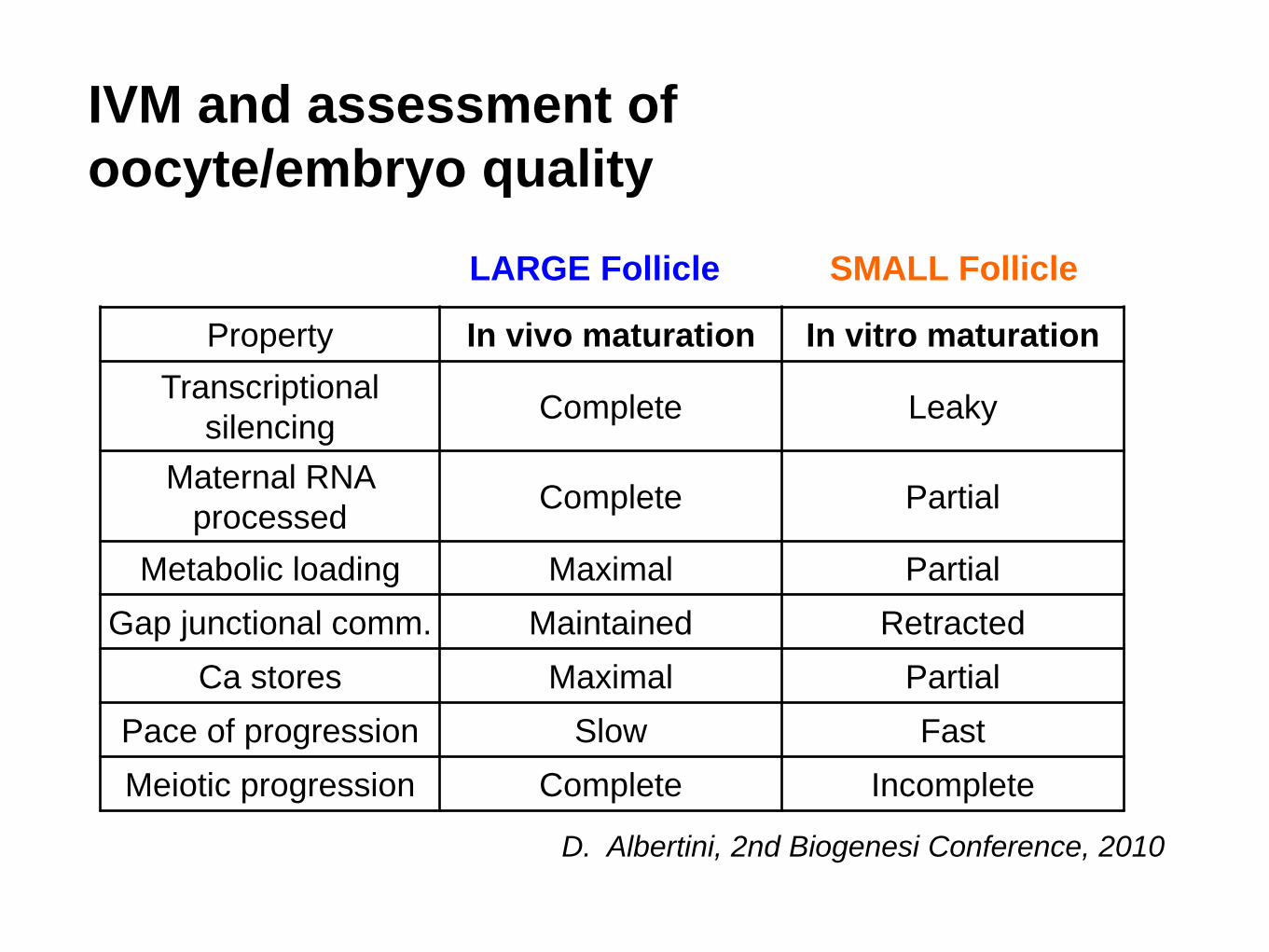
IVM and assessment of
oocyte/embryo quality
Property In vivo maturation In vitro maturation
Transcriptional
silencing Complete Leaky
Maternal RNA
processed Complete Partial
Metabolic loading Maximal Partial
Gap junctional comm. Maintained Retracted
Ca stores Maximal Partial
Pace of progression Slow Fast
Meiotic progression Complete Incomplete
D. Albertini, 2nd Biogenesi Conference, 2010
SMALL Follicle LARGE Follicle
How to IMPROVE
1- FOLLICLE HETEROGENEITY
the HCG injection on 6-12 mm follicles
causes asynchronous maturation of oocytes
2 - INAPPROPRIATE SIGNALLING is
induced “spontaneous” vs “induced” meiosis
re-initiation
Positive stimulus
HOW TO IMPROVE ?
Use a system inspired from animal production
Better exploit the small (2-8 mm) follicles ? Learn about
Gamete competences
Receptors expression
Signalling cascades
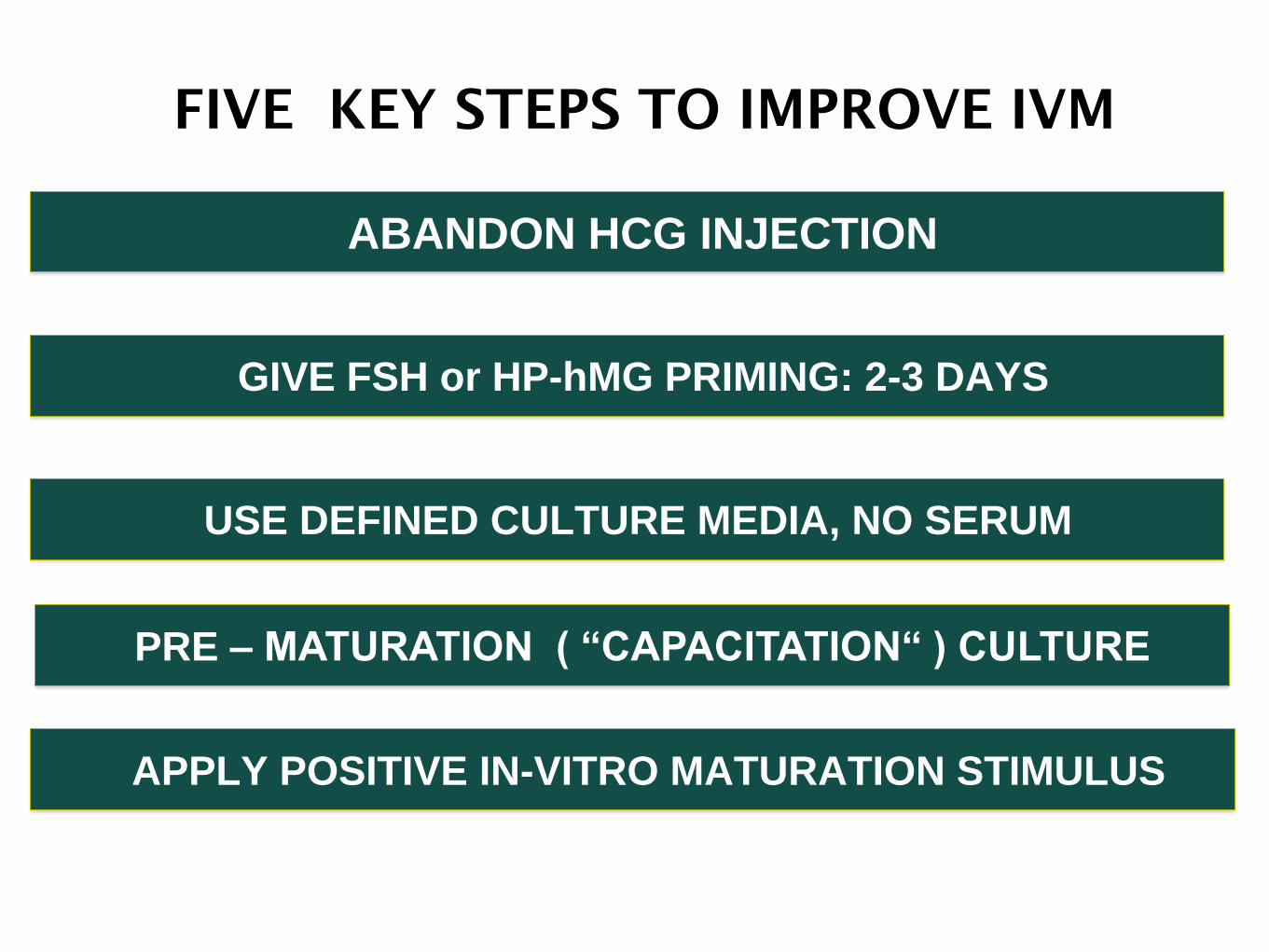
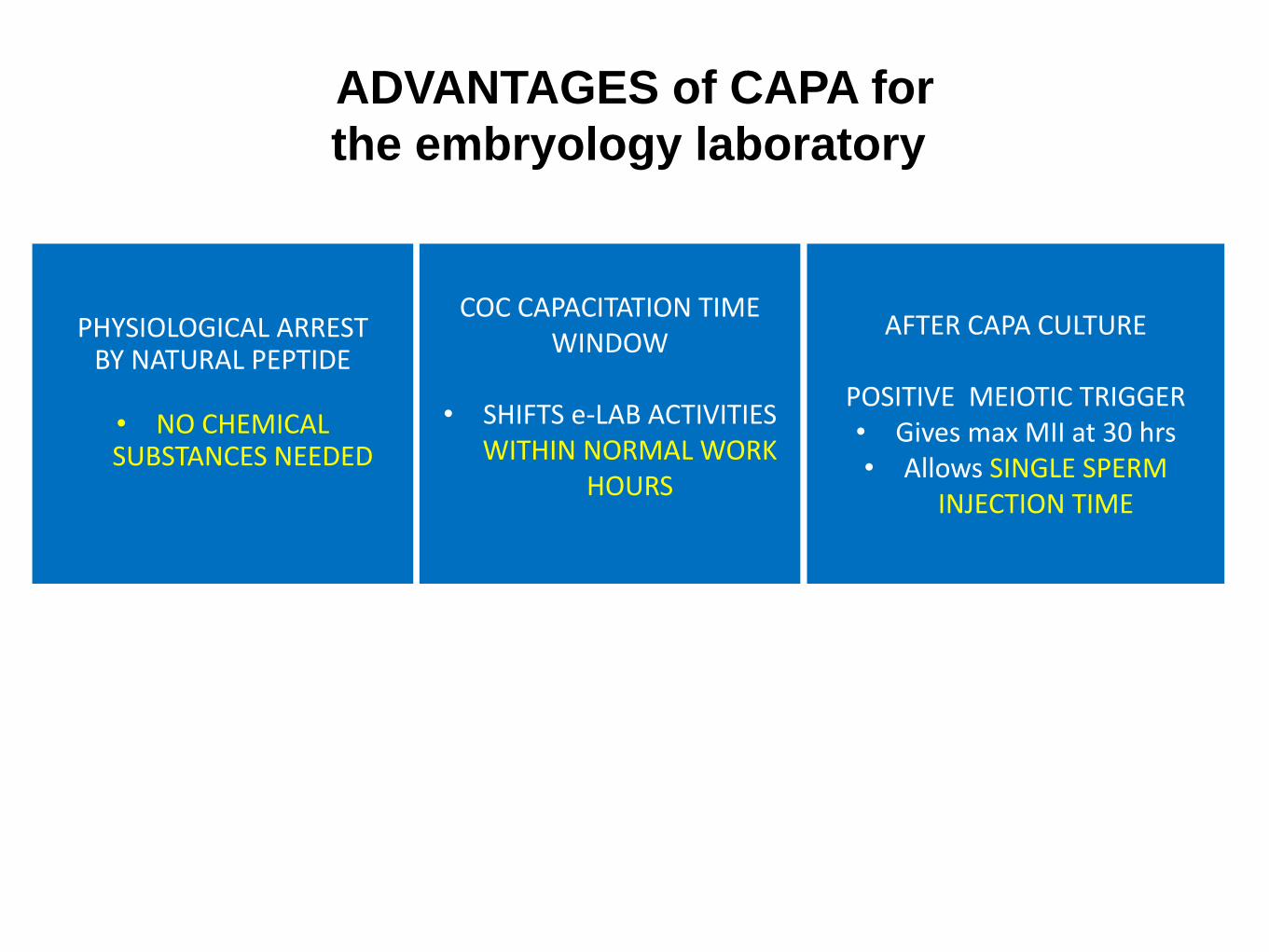
FIVE KEY STEPS TO IMPROVE IVM
ABANDON HCG INJECTION
GIVE FSH or HP-hMG PRIMING: 2-3 DAYS
USE DEFINED CULTURE MEDIA, NO SERUM
APPLY POSITIVE IN-VITRO MATURATION STIMULUS
PRE – MATURATION ( “CAPACITATION“ ) CULTURE
AVOID HCG to FOSTER CUMULUS- OOCYTE COMMUNICATION
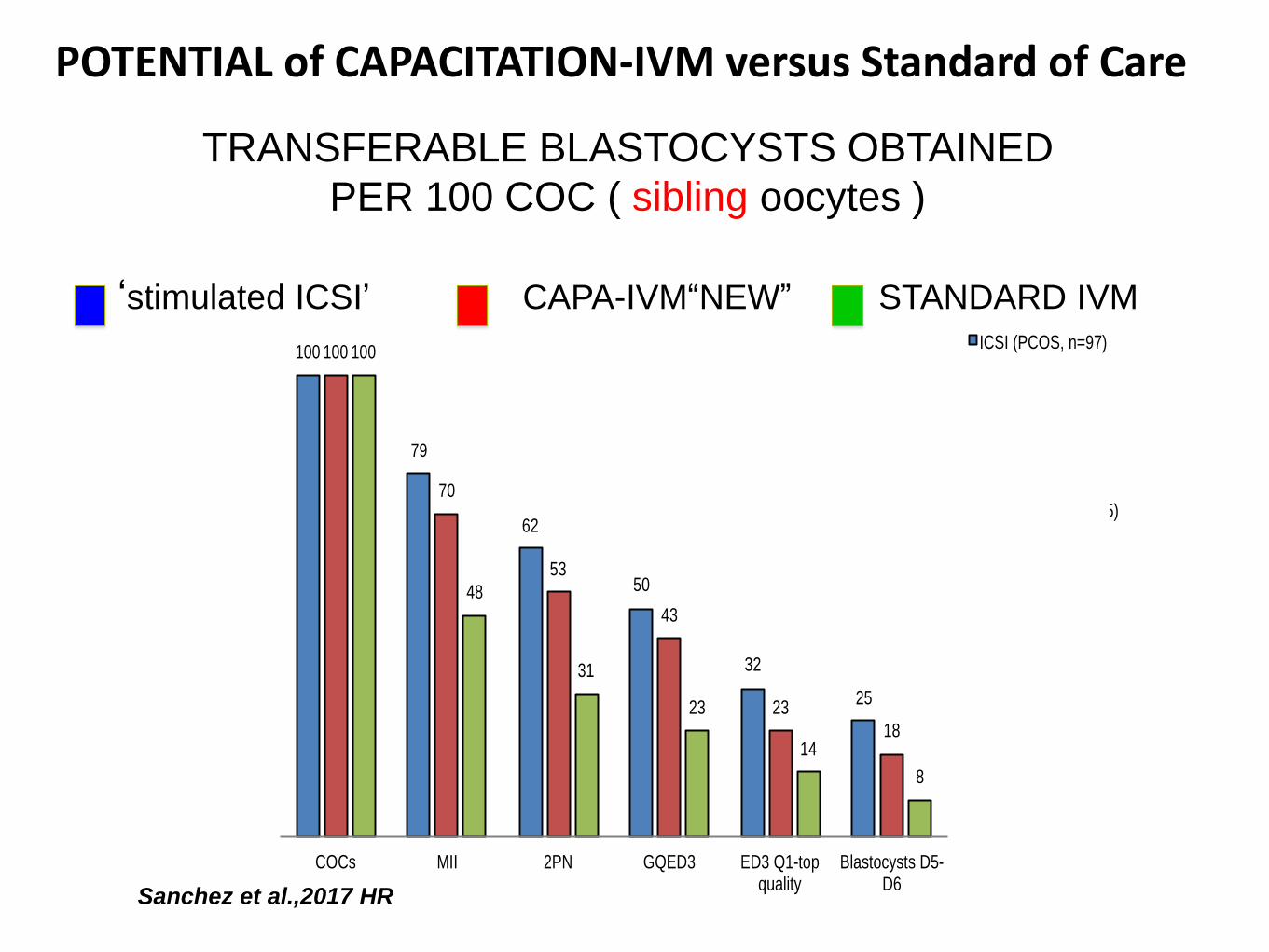
POTENTIAL of CAPACITATION-IVM versus Standard of Care
Sanchez et al.,2017 HR
100
79
62
50
32
25
100
70
53
43
23
18
100
48
31
23
14
8
COCs MII 2PN GQED3 ED3 Q1-top quality
Blastocysts D5-D6
ICSI (PCOS, n=97)
CAPA (n=15)
Standard IVM (n=15)
TRANSFERABLE BLASTOCYSTS OBTAINED
PER 100 COC ( sibling oocytes )
‘stimulated ICSI’ CAPA-IVM“NEW” STANDARD IVM
OOCYTE PHYSIOLOGY : ‘flash’ REVIEW
1- In the small antral follicle (2-8 mm) the
oocyte is actively kept under meiotic arrest
what are the main mechanisms ?
2- By LH rise: meiosis reinitiation and
cumulus expansion ?
what are the prerequisite conditions ?
MEIOTIC ARREST
Regulation
cAMP
ATP
AC
5’AMP
ATP
AC
5’AMP
cAMP
LH ACTIVATES THE EGF- LIKE SYSTEM ESSENTIAL TO OOCYTE MATURATION