Cardiac misconceptions: comparisons among nurses, nursing students and people with heart disease in Taiwan Lin, Y-P. , Furze, G. , Spilsbury, K. and Lewin, R.J.P. Pre-print (submitted version) deposited in CURVE October 2011 Original citation & hyperlink: Lin, Y-P. , Furze, G. , Spilsbury, K. and Lewin, R.J.P. (2008) Cardiac misconceptions: comparisons among nurses, nursing students and people with heart disease in Taiwan. Journal of Advanced Nursing, volume 64 (3): 251-260. http://dx.doi.org/10.1111/j.1365-2648.2008.04802.x Publisher statement: This is the pre-peer reviewed version of the following article: Lin, Y-P. , Furze, G. , Spilsbury, K. and Lewin, R.J.P. (2008) Cardiac misconceptions: comparisons among nurses, nursing students and people with heart disease in Taiwan. Journal of Advanced Nursing, volume 64 (3): 251-260, which has been published in final form at http://dx.doi.org/10.1111/j.1365-2648.2008.04802.x. Copyright © and Moral Rights are retained by the author(s) and/ or other copyright owners. A copy can be downloaded for personal non-commercial research or study, without prior permission or charge. This item cannot be reproduced or quoted extensively from without first obtaining permission in writing from the copyright holder(s). The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the copyright holders. This document is the submitted version of the journal article, as originally submitted to the journal prior to the peer-review process. Some differences between the published version and this version may remain and you are advised to consult the published version if you wish to cite from it.
CURVE is the Institutional Repository for Coventry University http://curve.coventry.ac.uk/open
1
Title: Cardiac misconceptions: comparisons among nurses, nursing students
and people with heart disease in Taiwan.
Abstract
Aim
This paper reports comparison studies of misconceived and potentially maladaptive
beliefs about heart disease (cardiac misconceptions) held by nurses, nursing students
and people with heart disease in Taiwan.
Background
Misconceived and maladaptive beliefs about heart disease have been shown to
influence outcomes in people with heart disease, and eliciting and dispelling
incorrect beliefs decreases disability. However, nurses do not routinely elicit these
maladaptive beliefs, and may reinforce them.
Method
Between October 2005 and March 2006 a survey was conducted using the pilot
[Name] Cardiac Beliefs questionnaire to measure cardiac misconceptions in 64
hospital-based nurses (13 of which were cardiac nurses); 134 nursing students; and
238 people with heart disease.
Results
Nursing students held fewer cardiac misconceptions than nurses (p=0.042). There
were no significant differences in numbers of misconceptions between cardiac and
general nurses, and there were no significant associations between level of
qualification, years of nursing experience and number of misconceptions. Nurses
with higher levels of education were more likely to hold fewer misconceptions
(p=0.24). Patients held significantly more misconceived and maladaptive beliefs
about heart problems than nurses (p< 0.001).
2
Conclusions
Taiwanese nurses require more continuing professional education to develop their
clinical expertise, rather than relying on general nursing knowledge. Nurses who are
involved in care for people with heart disease have a responsibility to assess and
dispel peoples‟ misconceptions about heart disease. Further research should continue
to focus on methods of dispelling cardiac misconceptions in both nursing and patient
education.
Keywords
coronary heart disease, misconceptions, maladaptive beliefs, questionnaire survey,
health professionals, nursing education, Taiwan
3
Summary
What is already known about this topic
Specific misconceptions about heart disease have been shown to influence
patients‟ outcomes and dispelling negative beliefs can decrease disability
Nursing staff have a major role in providing information about recovery for
people with coronary heart disease
Nurses do not routinely ask patients about their beliefs about heart disease and
may inadvertently reinforce misconceptions
What this paper adds
Nurses can hold active misconceptions about heart disease and may pass these
on to patients
Nursing students in Taiwan demonstrate better knowledge about heart disease
than nursing staff; there were no significant differences in numbers of
misconceptions between cardiac and general nurses
More education about heart disease is required in initial nurse education in
Taiwan, and continuing professional education for cardiac specialist nurses
needs to be established
4
Introduction
Coronary heart disease (CHD) is a leading cause of morbidity and disability in
adults in developed countries. Among people with existing CHD, secondary
prevention is aimed at changing behavioural risk factors such as smoking, diet, and
sedentary lifestyles. If people with heart disease hold misconceptions about their
condition and how to cope with it that are different to the advice being given, then
concordance with risk factor reduction and medication adherence may be poor
(Horne, 1997; Byrne et al., 2005). Patients‟ negative perceptions about heart disease
are an important determinant in explaining the relationship between impairment and
disability (Weinman & Petrie, 1997; Lewin, 1999). It is essential therefore that
health professionals are well informed and equipped to elicit commonly held cardiac
misconceptions and dispel them.
Background
Cardiac misconceptions are incorrect beliefs about heart problems, which can lead
people to adopt maladaptive ways of coping. In the 1960s, Wynn (1967) noted that
what people believed about their heart disease could have a profound effect on their
lives after a heart attack. Patients‟ negative perceptions of their heart disease were
related to adopting an unduly careful pattern of life; for example, the false belief that
any work would be harmful to them provoked them to accept premature retirement
(Wynn 1967). People with more misconceptions about living with heart disease were
found to have a slower recovery and reduced rate of return to work (Maeland &
Havik, 1987b; Petrie et al., 1996), reduced autonomy post myocardial infarction
(Havik & Maeland, 1987), more admissions to hospital (Maeland & Havik, 1989),
overprotective behaviours (Petrie & Weinman, 1997) and poor attendance at cardiac
rehabilitation (Broadbent et al., 2006). Therefore, cardiac misconceptions appear to
5
have an effect on recovery from heart disease. Furze et al. (2002, 2003, 2005)
demonstrated that there is a range of commonly held, specific misconceptions about
angina that are implicated in reduced psychological and functional status. These
misconceptions could be elicited by administration of a questionnaire (Furze, et al.,
2003).
Health professionals play an important role in providing information about recovery
for people with CHD, but misconceptions may sometimes be instilled or reinforced
by health professionals (Maeland & Havik, 1987a; Leventhal et al., 1997). Beliefs
and misconceptions about living with heart disease held by health professionals may
influence the beliefs and behaviours of people with CHD. Bassan (1986)
demonstrated that a majority of cardiologists held misconceptions about the effect of
exertion in stable angina, with 58% believing that there was a risk (against the
evidence) of permanent damage to the myocardium.
There are limited numbers of studies (conducted in Western countries) which have
elicited health professionals‟ cardiac knowledge or misconceptions by comparing
them with the knowledge of people suffering with heart problems. Maeland and
Havik (1987a) reported that there were differences in cardiac beliefs held by nurses,
doctors and physiotherapists, with cardiac nurses holding fewer cardiac
misconceptions than doctors.
Newens et al. (1996) investigated differences in knowledge of cardiac-related
symptoms and cardiac misconceptions between patients and nurses. Patients held
more cardiac misconceptions than any health professional group. It was apparent
that there was a significant knowledge gap between nurses and patients, the nurses
were not accurate at assessing patients‟ beliefs, nor did they use opportunities to
correct the misconceptions of patients. In a further study, Newens et al. (1997) found
6
that cardiac nurses held fewer misconceptions than general medical nurses, and that
nurses who had received training to facilitate the Heart Manual - a
cognitive-behavioural rehabilitation programme for post-myocardial infarction
patients (Lewin et al., 1992) - held fewer cardiac misconceptions than any other
group. This viewpoint echoes the observation of Petrie and Weinman (1997), that
health professionals do not routinely ask patients about their beliefs.
However, there is no evidence on cardiac misconceptions among Taiwanese nurses.
It is therefore not known whether nurses in Taiwan hold the same, more or fewer
cardiac misconceptions than their patients.
The Study
Aims
The aims of this study were to compare: (i) the cardiac misconceptions of Taiwanese
nurses and student nurses; (ii) nurses‟ and patients‟ misconceptions and maladaptive
beliefs about heart disease. The research questions were:
To what extent do Taiwanese nurses and nursing students hold misconceived
and maladaptive beliefs about heart disease?
What are the cardiac misconceptions among cardiac and general nurses in
Taiwan? Are there differences between the groups?
Do nurses and student nurses hold similar misconceptions and maladaptive
beliefs about heart disease as people with heart disease?
Design
A cross-sectional survey using a descriptive comparative design was carried out in
Taiwan. The lack of evidence of nurses‟ cardiac misconceptions in Taiwan, meant
that a descriptive design was most the appropriate to address the study questions.
Participants
The Nurses. In Taiwan, there are two routes for training as a nurse. „Registered
7
nurse‟ is used to define nurses who have graduated from an accredited nursing
programme at a technological academy, college or university and therefore hold a
professional license. The term „practical nurse‟ refers to nurses who have received
high school or vocational school nurse training. The roles and responsibilities of
both of these nurses are concerned with the delivery of direct clinical patient care
(Tzeng & Ketefian, 2003). The difference relates to the grade and salary awarded
following the different levels of preparation. Throughout this paper the term „nurse‟
is used and refers to both registered and practical nurses.
A total of 64 nurses were recruited for this study. All nurses (registered and practical)
working on the cardiac or medical wards in three participating hospitals in Northern
and Central Taiwan were eligible for inclusion in the study. Those with less than six
months experience of working as a clinical nurse were excluded. Fifty-one nurses
were recruited from the medical wards (6 nurses from a medical centre; 25 from a
regional hospital; and 20 from a local teaching hospital). Thirteen cardiac nurses
were recruited from one cardiovascular ward at one hospital (patients were also
recruited from this hospital).
The nursing students. In the Taiwanese educational system there are different entry
points into nursing college. Students with a vocational or high school qualification
then enter a 4-year college system to study nursing; whereas those who have studied
at the technological academy where they undertake 2 or 3 years training after
vocational school, then study for a further 2-years at college. A post registration
bachelor of nursing conversion course is designed for registered nurses working in
various clinical settings. Therefore, students were recruited from 4-year and 2-year
nursing degree courses regardless of gender or ethnicity at the Nursing Department.
The students who were currently undertaking a post registration bachelor of nursing
8
conversion course in a 2-year degree were excluded.
A total of 147 nursing students were drawn from a convenience sample of
baccalaureate nursing students enrolled from three classes in one nursing college in
Taipei. One hundred and thirty four questionnaires were completed and returned by
these nursing students, giving a response rate of 91%. No data were collected from
non-responders because the survey was voluntary and anonymous. Therefore, in
total, 198 nurses were included in this study (including registered, practical and
student nurses).
Patients. A total of 238 patients were recruited from a cardiovascular ward and five
outpatient clinics in a hospital in Taipei City. In-patients with a diagnosis of CHD
were identified by case note review undertaken by the first author (YPL). The
selection criteria for patients were adults of all ages with a diagnosis of CHD
regardless of gender or ethnicity. Patients who have had a myocardial infarction
(MI), angina pectoris, mild to moderate congestive heart failure (New York Heart
Association, NYHA Classes 1-3), coronary artery disease (CAD) defined by
angiography, a cardiac revascularisation procedure (coronary artery bypass grafting,
(CABG) or percutaneous transluminal coronary angioplasty (PTCA), were included.
Patients who had undergone heart transplantation, heart valve surgery or who had
severe heart failure (NYHA Class 4) were excluded. Patients who were in the acute
stages of cardiac diseases and/or had unstable conditions were also excluded.
Data collection
Data collection took place for six months from October 2005 to March 2006.
Questionnaires were sent to selected wards (where they were completed by the
nurses and returned to a sealed box in the ward) or distributed to three selected
classes of nursing students (where they were completed by students in the classroom
9
and returned to the researcher, YPL).
Survey instrument: questionnaire
The numbers of common misconceptions and maladaptive beliefs about heart
disease held by the participants were assessed with a pilot version of the [Name]
Cardiac Beliefs Questionnaire (pYCBQ). The pYCBQ is designed to elicit beliefs
about causation and coping in heart disease that are misconceived or potentially
maladaptive. It consists of 24 statements about heart problems with answers scored
at 0 (Disagree) and 1 (Agree). A high score on this questionnaire means that people
held more misconceptions. This questionnaire has been derived from interviews with
English people with heart disease.
Validity and reliability
The pYCBQ has been shown to have good internal reliability (Cronbach‟s alpha
score of 0.81) and stability (r= 0.85) in a study of British people awaiting coronary
artery bypass graft surgery (Furze & Lewin, 2006). For the purpose of the study, the
pYCBQ was translated into Chinese and independently back translated into English
to check for accuracy. The Chinese version of the questionnaire was piloted with 11
Taiwanese at an English University who did not participate in the main study. No
major changes were made to the questionnaire following the pilot study.
Ethical consideration
The study was approved by the Departmental Research Governance Committee at
an English University and the study protocol was reviewed and approved by the
study sites. Permission to conduct the study was also obtained from the directors of
nursing in the participating Taiwanese hospitals, and from the institutional review
board of the nursing department of the Taiwanese college. An information sheet and
10
a consent form were given to people who met the inclusion criteria for the study.
The information sheet provided an explanation of the purpose of study, what would
be requested of the participants and how data generated from the study would be
used. All participants were guaranteed confidentially and anonymity, and were
allowed to refuse or withdraw from the study at any time. Written consent was
gained from all participants. Each participant was given a copy of the information
sheet and consent form.
Statistical analyses
Analysis was performed with SPSS version 13.0 for Windows [Statistical Package
for the Social Sciences (SPSS Inc, Chicago, IL. USA) 2004]. Demographic data,
such as type of ward, level of qualification, length of time on current ward, age, and
education, were analysed by descriptive analysis. Mean differences in pYCBQ
scores between groups were analysed by student t-test and mean scores on pYCBQ
across length time on current ward, education, years of nursing experience using
analysis of variance or student t-test. Chi-square test of independence was used to
compare responses to individual items of the pYCBQ. A p value of less than 0.05
was considered significant. Bonferroni adjustment was used when undertaking
multiple comparisons of the data (the acceptance of a more stringent level of
significance can help to guard against Type I errors).
Additionally, standard multiple regression analysis was conducted to assess the
value of nurses‟ baseline demographic variables (type of ward, age, the length time
on current ward, level of qualification, education, cardiac specialist qualification,
total years working in nursing) as the independent variables in predicting the scores
on the pYCBQ. Prior to performing regression analyses, initial assumptions
checking were undertaken of the independent variables for multicollinearity and
11
singularity, outliers, normality, linearity, homoscedasticity and independence of
residuals (Field, 2000; Pallant, 2005), applying SPSS Explore and SPSS Regression.
Results
Characteristics of nurse participants
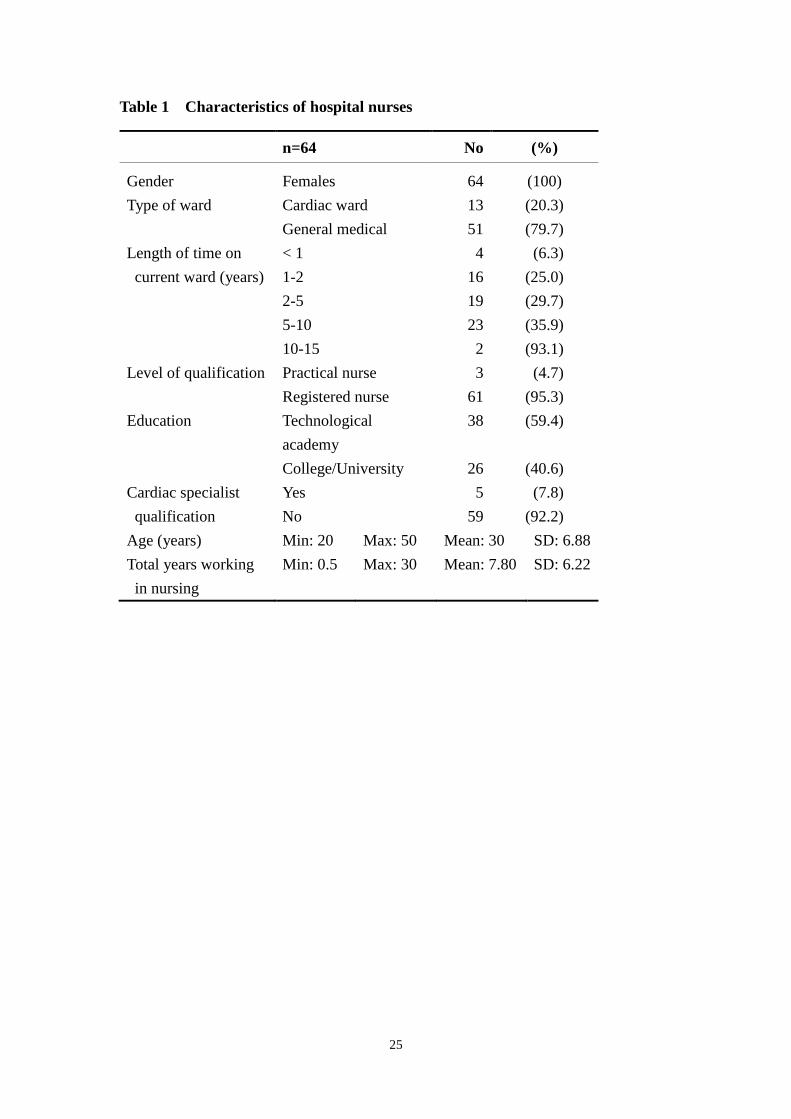
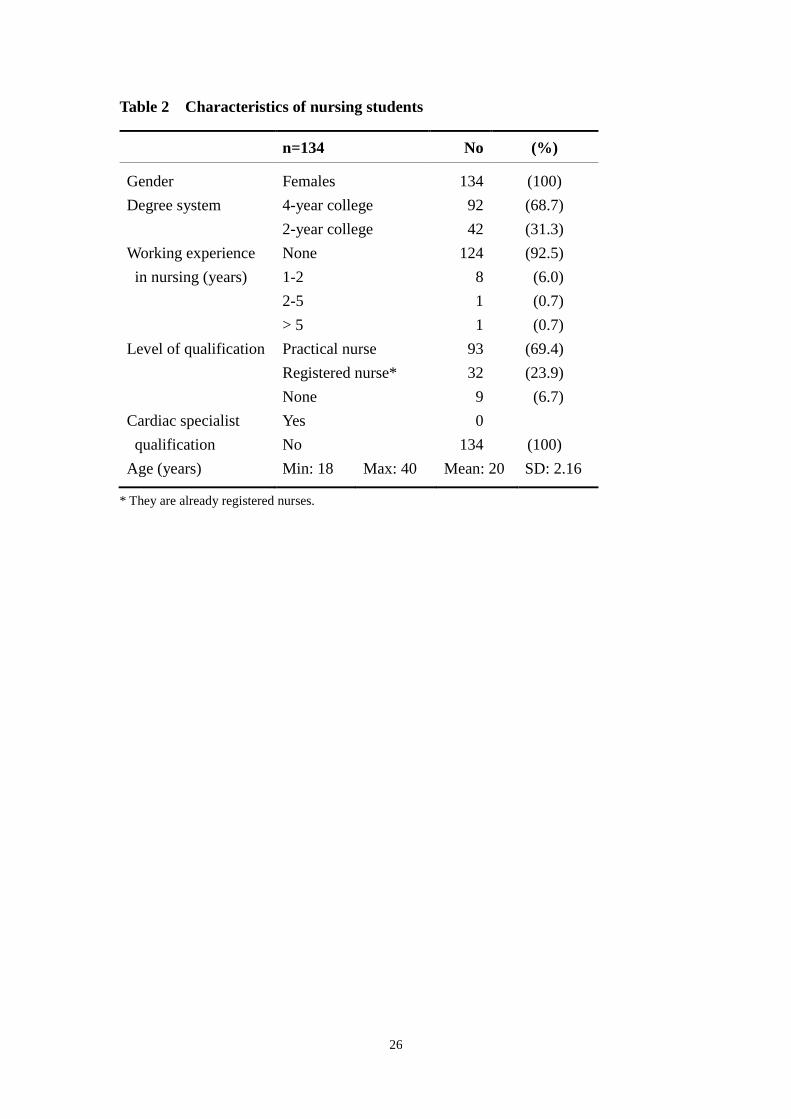
All nurses in this study were female; the characteristics of nurses and nursing
students are shown in Tables 1 and 2. Hospital nurses‟ age ranged from 20-50 years,
with a mean age of 30 years (SD = 6.88). The majority of the nurses were registered
nurses (95.3%) and had been nursing for a mean 7.8 years. 69.4% of the nursing
students were practical nurses and 92.5% of those had not previously worked in the
nursing field.
Characteristics of patient participants
The characteristics of patients are shown in Table 3.
Cardiac misconceptions
Descriptive scores of the pYCBQ
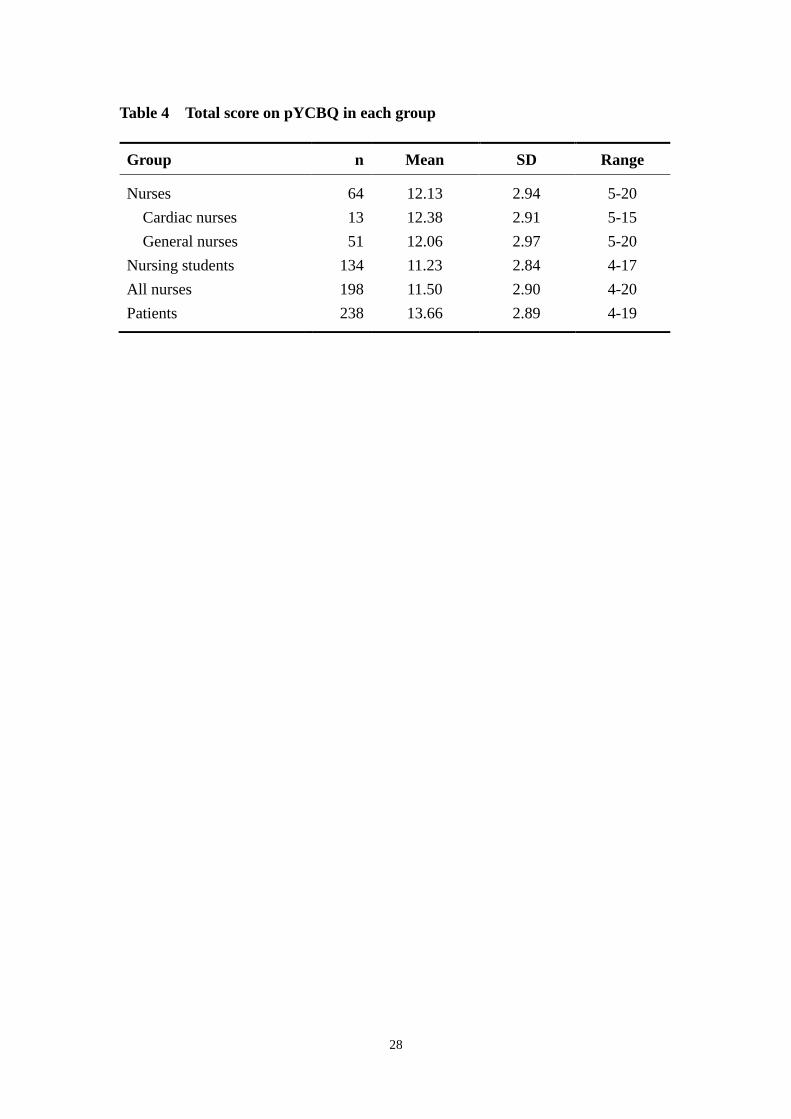
Mean score, standard deviation and range for pYCBQ total score for each group are
shown in Table 4. Nursing students held the lowest mean score of pYCBQ than any
other group.
Nurses and nursing students
There was a significant difference between nurses and nursing students in the total
score on the pYCBQ (nurses mean score, 12.1 [SD=2.9]; nursing students, 11.2
[SD=2.8]; t = 2.05, p= 0.042; 95% CI= 0.03 - 1.75). Nursing students held fewer
misconceptions and maladaptive beliefs about heart disease than the nurses.
Analysis of nurses‟ and nursing students‟ responses to the individual items showed
12
four items with differences in responses (an alpha value of less than 0.05), however,
with a bonferroni correction (p=0.002) these items were not significantly different.
Cardiac nurses and general nurses
The overall scale score across all 24 items of the pYCBQ for cardiac nurses ranged
from 5 to 15; the range for general nurses was from 5 to 20. A surprising finding was
that there were no significant differences on scores on the pYCBQ between nurses
working on the cardiac ward and those working on other general wards (cardiac
nurses: mean = 12.4, SD=2.9; general wards nurses: mean = 12.1, SD=2.9; t = 0.36,
p= 0.724).
Scores were not related to the level of qualification (t = 0.13, p= 0.901), cardiac
specialist nurse qualification (t = - 2.56, p = 0.799) or the length of years since
qualifying (F = 0.76, p = 0.555), while there was a small difference in mean scores
of the years on the current ward (F = 2.59, p =0.046). Post hoc tests revealed that
nurses who had worked on their current ward for between 1 and 2 years had higher
mean scores (13.8, SD = 3.12) than those who had worked there for 5 to10 years
(10.9, SD = 2.94, p= 0.019), that is, nurses with less experience on their current
wards held more misconceptions. There was also a slight difference on the mean
scores on the pYCBQ related to education degree (t =2.26, P = 0.027); nurses who
graduated from college or university held fewer misconceptions about heart disease
(mean 11.1, SD = 3.13) than those with a technological academy degree (mean 12.8,
SD = 2.63).
There were no significant correlations between type of ward, age, level of
qualification, cardiac specialist qualification, and total years working in nursing and
score on the pYCBQ. Therefore, it was not possible to undertake multiple regression
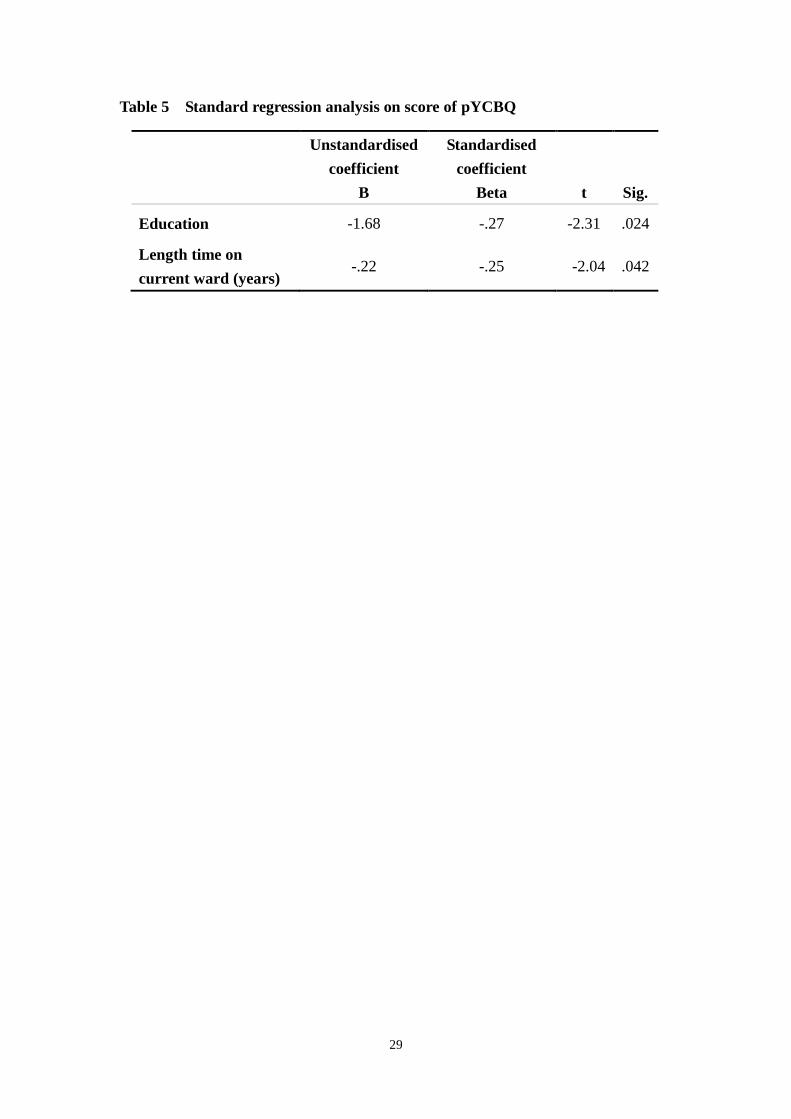
using these variables. Only education (r= -0.28, p= 0.014) and the length time on
13
current ward (r= -0.25, p= 0.024) showed a relationship to the scores of pYCBQ.
Therefore, standard multiple regression was performed to measure which is the best
predictor of scores of pYCBQ. Following assumptions checking, there were no other
violations. Results of the analysis are presented in Table 5. The model was
significant (F[2, 61]= 4.84, p= 0.011) and explained 13.7% of the variance (adjusted
R2). Of these two variables, education made the largest unique contribution in scores
of pYCBQ (beta = -0.274), although the length time on current ward also made a
near statistically significant contribution (beta = -0.247). The negative correlation
between education and score of pYCBQ shows that nurses with higher education
were more likely to hold fewer misconceptions.
Compared to Patients
The mean score on the pYCBQ for all nurses was 11.5 (SD=2.9) which was
significantly lower than the patients‟ mean of 13.7 (SD=2.9; t = 7.71, p<0.001). The
patients held significantly more misconceived and maladaptive beliefs about living
with heart disease than the nurses. There were no significant differences between the
nurses working in the cardiac ward and people with heart disease (cardiac nurses:
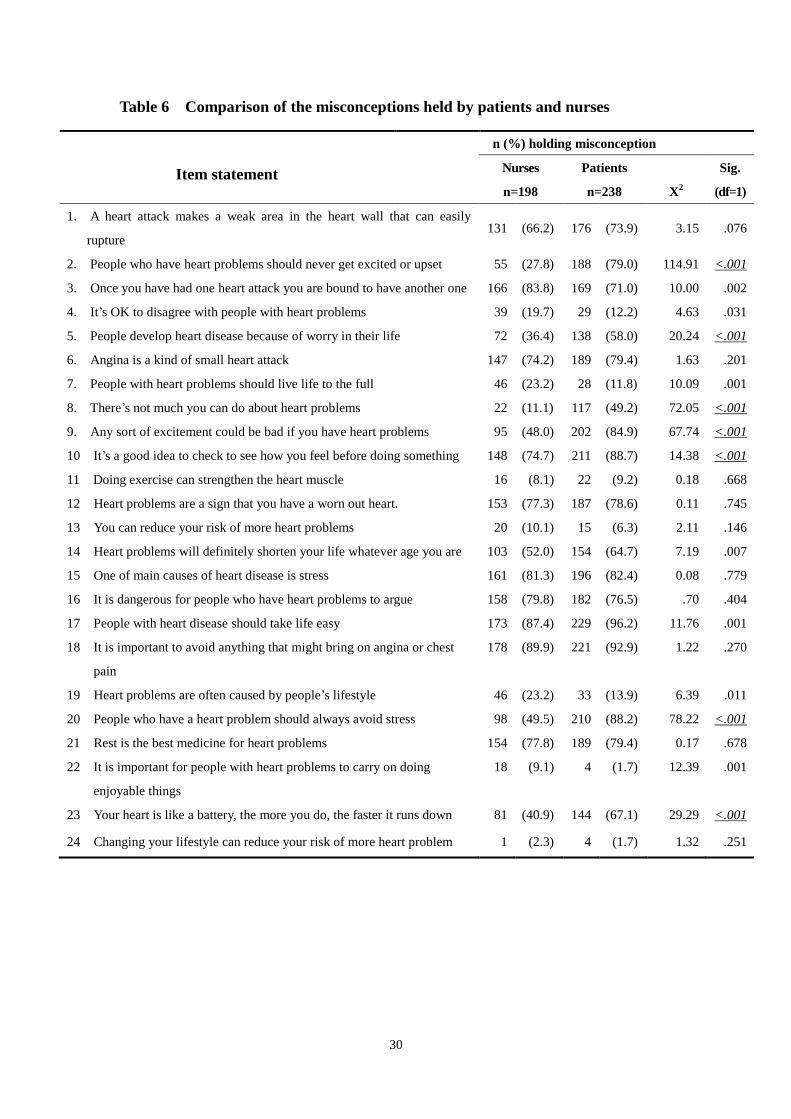
mean = 12.4, SD=2.9; patients mean: 13.7, SD = 2.89; t = -1.56, p = 0.121). Table 6
shows the percent responses to individual pYCBQ items of nurses and patients.
When patients‟ and nurses‟ responses to each item of the questionnaire were
compared, there were significant differences on 7 items (2, 5, 8, 9, 10, 20 and 23; p<
0.001) between the two groups.
Discussion
Nurses and nursing students
14
It may be expected that the level of cardiac misconceptions depends on nurses‟
qualifications and working experiences, and that nurses may be better informed and
hold fewer cardiac misconceptions than nursing students. However, data from this
study revealed a slightly different picture, the findings showed that nursing students
held slightly fewer misconceptions and maladaptive beliefs about heart disease than
did nurses. Despite the majority of nursing students having little experience of
nursing work, the students had received at least 3-5 years of formal nursing training
courses and qualified as practice or registered nurses, and they were undertaking
nursing college courses designed to convert their diploma certificate to a Bachelor of
Nursing. In this study, all nursing students were undertaking college courses, while
only 40% of qualified nurses had graduated from college or university. It suggests
that a programme of continuing professional education may be required in order to
enhance nurses‟ knowledge.
Age was not associated with pYCBQ score, and there was also no association found
between work experience and the level of misconceptions among nurses in this study.
However education was associated with scores on the pYCBQ; the higher educated
the nurse was, the fewer misconceptions they held.
In Taiwan, nurses graduate from an official nursing education programme and hold a
professional license as Registered Nurse or Practical Nurse. There is no difference in
the responsibilities of Registered and Practice Nurses because their main
responsibility is to provide direct clinical patient care (Tzeng & Ketefian, 2003) and
also the certification is a permanent license without further assessment compared to
western countries. In the USA and the UK, nurses need to undertake regular
re-examination or to report that they have updated their professional knowledge in
order to re-license. This may reflect that the health care system in Taiwan placed
15
more emphasis on basic clinical skills in nurses rather than in-service training; it is
therefore suggested that continuing educational programmes are fundamental needs
for clinical nurses.
Cardiac nurses and general nurses
A surprising finding of this study was that the cardiac nurses did not hold more
cardiac knowledge than general nurses, and the level of qualification and years of
nursing experiences were also not associated with number of misconceptions. The
findings differ from previous studies that compared the responses between groups of
nurses (Newens et al., 1996; 1997). However, it must be noted that findings from
research among nurses in different countries may not be generalisable to the
Taiwanese health system. Newens et al. (1997) found that nurses working in
specialist wards were significantly better informed about cardiac care and held fewer
misconceptions than did nurses on general medical wards. The reasons were not
explored; however, the possible explanations may be that nursing policy in Taiwan
has not emphasized the need for specialist training in cardiac care and has focused
on basic clinical skills (Tzeng & Ketefian, 2003), which is demonstrated by the fact
that only 7.8% of nurses in this study held a specialist license. This lack of
encouragement to undertake specialist training may have created a barrier to
continuing education in nurses with a heavy workload in clinical care. Moreover, the
study by Newens et al. (1997) demonstrated that nurses who had undertaken the
Heart Manual training programme, held fewer misconceptions than those did not.
This may provide evidence that nurses who are continuing to care for people with
heart disease should undertake specialist training rather than relying on general
medical knowledge. Another explanation is that the cardiac nurses in this study were
recruited from only one unit and were a small sample, so the results could not be
16
generalized to other institutions or hospitals.
Nurses and cardiac patients
As might be expected, the patients held significantly more misconceived and
maladaptive beliefs about heart problems than nurses and are consistent with the
findings of Newens et al. (1996). It indicates that there were significant
discrepancies in beliefs of heart problems between nurses and patients; this suggests
that even when nurses are knowledgeable they may not convey the information to
patients. It is most noteworthy that there may be nurses with a number of
misconceptions that they may then pass on to the patients.
Both nurses and patients had a poor understanding of the disease process and
physiology of CHD (items 1, 3, and 6). More than 70 percent of both groups believed
that “the heart wall can easily rupture”, “bound to another one [heart attack]” and
“angina is a small heart attack”. These strongly indicates that nurses did not have the
correct knowledge of cardiac anatomy and physiology, and these misconceptions may
be passed on to patients, with the result that they may cause patients to have an
unnecessarily frightening image of living with heart disease. The consequence of
holding such catastrophic misconceptions is that the patient may then adopt
profoundly sedentary and avoidant lifestyles which would increase their risk of future
cardiac events (Thompson et al., 1976; Maeland & Havik, 1987a).
Moreover, the majority of nurses and patients believed that people should avoid
anything that might bring on chest pain (item 18), take life easy (item 17) and rest is
the best medicine (item 19). These findings are similar to those of Bassan (1986) who
found that a majority of cardiologist believed that the symptom of angina must be
avoided because there was a high risk of myocardial damage (which is contrary to the
definition of stable angina – that any changes to the myocardium are reversed at the
17
end of the self-limiting episode) (Task Force of the European Society of Cardiology,
1997). However, these misconceptions can cause excessive anxiety among patients
and may leads to patients restricting activities. These views of professionals may
cause patients to adopt an inactive lifestyle at all costs and/or may lead to emotional
distress about the consequences of undertaking activities, with the consequence of
reduced physical fitness which means an increase in cardiac risk. All of the guidelines
for secondary prevention in heart disease (for example: American College of
Cardiology - American Heart Association, 2004; Scottish Intercollegiate Guidelines
Network, 2007) emphasise the importance of maintaining and improving physical
fitness through exercise, as lack of fitness is a risk factor for further events. In
addition, nurses beliefs may also inform patients that they must never get excited or
upset (item 2) and any kind of excitement could be bad (item 9). This may lead to a
contraction of social life and a reduction in quality of life.
A common belief held by both nurses and patients was that stress is one main causes
of developing heart disease. However the role of everyday life stress in atherogenesis
is still under debate. The confusing results which feed this debate can be illustrated by
two similar studies: (i) Macleod et al. (2002) found no link between perceived stress
and objective indices of CHD in a prospective, 21-year follow-up of 5606 men in
Scotland, and (ii) Rosengren et al. (1991), who found that people with higher
perceived stress were more likely to suffer from cardiovascular disease in a
prospective 11-year study of 6935 men in Sweden. What is known is that people who
perceive stress to be the main cause of their heart disease (rather than the accepted
behavioural risk factors) are less likely to engage with behavioural risk factor
reduction (Petrie & Weinman, 1997; Weinman et al., 2000). This suggests that, while
believing that stress causes heart disease may not be a true misconception (as the
18
evidence is equivocal), it is a maladaptive belief because it encourages behavioural
avoidance. Avoidance coping includes strategies such as denial and withdrawal
(Roesch & Weiner, 2001). Although denial has been associated with a rapid recovery
in the early phase of an illness, if patients continue to deny the severity of their
condition then lifestyle change does not occur and mortality can increase (Havik &
Maeland, 1988; Steptoe & Wardle, 1994). Nurses were less likely to believe that
people with a heart problem should avoid stress, which, when taking their other belief
that stress causes heart disease into account, may suggest that whilst nurses may
hold strong views on links between everyday life stress and heart disease, they may
also believe that a life without stress could not be achieved.
Study limitations
A few limitations of this study should be noted when considering and interpreting
the findings. The small number of nurses were recruited from one cardiac ward,
three hospitals and one participating nursing college; therefore, the results could not
be generalised to all nurse populations across Taiwan. Convenience samples were
used in the study which may also result in an unrepresentative or biased study
population. Further, a cross-sectional and descriptive comparative design was used,
thus, the findings cannot be taken to imply a causal relationship of the knowledge
gap between nurses and patients. Third, the questionnaire instrument was derived
from belief statements held by English people with heart disease; it may not cover
other aspects of misconceptions that were influenced by Taiwanese culture or social
norm factors.
Conclusions
There have been no previous studies conducted in Taiwan with nurses related to
misconceptions about heart disease. The findings of this study provide information
19
for nursing practice and education. The results suggest that damaging
misconceptions are common in both patients and nurses and that as a result patients
may become more distressed and disabled than is necessary (Furze et al., 2005). It
seems that training programmes need to be organised for nurses to educate them
about these misconceptions, the effect these can have on patients and how best to
dispel them. Nursing educators may incorporate the findings of this study into the
cardiovascular nursing course for both nurses and nursing students, to assist them to
a better understanding about heart disease and to also ensure that nurses‟
maladaptive beliefs will not reinforce those of the patients. Finally, further research
should be conducted to ascertain any cultural differences between British and
Taiwanese people beliefs about cardiac illness and misconceptions.
20
References
American College of Cardiology - American Heart Association. (2004). ACC/AHA
guidelines for the management of patients with ST-elevation myocardial
infarction. ACC/AHA: Washington DC.
Bassan, M. (1986). Who's afraid of angina pectoris? Separating the symptom from
the marker. The Lancet, 328, 1442-1443.
Broadbent, E., Petrie, K. J., Main, J., & Weinman, J. (2006). The brief illness
perception questionnaire. Journal of Psychosomatic Research, 60(6),
631-637.
Byrne, M., Walsh, J., & Murphy, A. W. (2005). Secondary prevention of coronary
heart disease: Patients beliefs and health-related behaviour. Journal of
Psychosomatic Research, 58, 403-415.
Field, A. (2000). Discovering statistics using SPSS for windows. London: Sage.
Furze, G., Bull, P., Lewin, R. J. P., & Thompson D.R. (2003). Development of the
York angina beliefs questionnaire. Journal of Health Psychology, 8(3),
307-315.
Furze, G., & Lewin, R. J. P. (2006). Prehabilitation for surgery patients. Paper
presented at the The 6th York Cardiac Care Conference, University of York,
May 2006.
Furze, G., Lewin, R. J. P., Murberg, T., Bull, P., & Thompson, D. R. (2005). Does it
matter what patients think? The relationship between changes in patients'
beliefs about angina and their psychological and functional status. Journal of
Psychosomatic Research, 59, 323-329.
21
Furze, G., Roebuck, A., Bull, P., Lewin, R. J. P., & Thompson, D. R. (2002). A
comparison of the illness beliefs of people with angina and their peers: A
questionnaire study. BMC Cardiovascular Disorders, 2:4,
http://www.biomedcentral.com/1471-2261/2/4.
Havik, O. E., & Maeland, J. G. (1987). Knowledge and expectations: Perceived
illness in myocardial infarction patients. Scandinavian Journal of Psychology,
28, 281-292.
Havik, O. E., & Maeland, J. G. (1988). Verbal denial and outcomes in myocardial
infarction patients. Journal of Psychosomatic Research, 32(2), 145-157.
Horne, R. (1997). Representations of medication and treatment: Advanced in theory
and measurement. In K. Petrie & J. Weinman (Eds.), Perceptions of illness
and health (pp. 155-187). Amsterdam; The Netherlands: Harwood Academic
Publishers.
Leventhal, H., Benyamini, Y., Brownlee, S., Diefenbach, M., Leventhal, E. A., &
Patrick-Miller, L., et al. (1997). Chapter 1: Illness representations:
Theoretical foundations. In K. J. Petrie & J. A. Weinman (Eds.), Perceptions
of health and illness (pp. 19-45). Amsterdam; The Netherlands: Harwood
Academic Publishers.
Lewin, B., Robertson, I., Cay, E. L., Irving, J., & Campbell, M. A. (1992). Effects of
self-help post myocardial infarction rehabilitation on psychological
adjustment and use of health services. Lancet, 339, 1036-1040.
Lewin, R. J. P. (1999). Improving quality of life in patients with angina. Heart, 82,
654-655.
Macleod, J., Davey Smith, G., Heslop, P., Metcalfe, C., Carroll, D., Hart, C., et al.
22
(2002). Psychological stress and cardiovascular disease: Empirical
demonstration of bias in a prospective observational study of Scottish men.
British Medical Journal, 324, 1247-1253.
Maeland, J. G., & Havik, O. E. (1987a). Measuring cardiac health knowledge.
Scandinavian Journal of Caring Sciences, 7, 23-31.
Maeland, J. G., & Havik, O. E. (1987b). Psychological predictors for return to work
after a myocardial infarction. Journal of Psychosomatic Research, 31(4),
471-481.
Maeland, J. G., & Havik, O. E. (1989). Use of health services after a myocardial
infarction. Scandinavian Journal of Social Medicine, 17, 93-102.
Newens, A. J., Mccoll, E., Bond, S., & Priest, J. F. (1996). Patients' and nurses'
knowledge of cardiac-related symptoms and cardiac misconceptions. Heart
Lung, 25(3), 190-199.
Newens, A. J., McColl, E., Lewin, B., & Bond, S. (1997). Cardiac misconceptions
and knowledge in nurses caring for myocardial infarction patients. Coronary
Health Care, 1, 83-89.
Pallant, J. (2005). SPSS survival manual. A step by step guide to data analysis using
SPSS for windows (version 12) (Second ed.): Open University Press.
Petrie, K. J., Weinman, J., Sharp, N., & Buckley, J. (1996). Role of patients' view of
their illness in predicting return to work and functioning after myocardial
infarction: Longitudinal study. British Medical Journal, 312, 1191-1194.
Petrie, K. J., & Weinman, J. A. (1997). Chapter 15: Illness representations and
recovery from myocardial infarction. In K. J. Petrie & J. A. Weinman (Eds.),
Perceptions of health and illness (pp. 441-461). Amsterdam; The
23
Netherlands: Harwood Academic Publishers.
Roesch, S. C., & Weiner, B. (2001). A meta-analytic review of coping with illness.
Do causal attributions matter? Journal of Psychosomatic Research, 50,
205-219.
Rosengren, A., Tibblin, G., & Wilhelmsen, L. (1991). Self perceived psychological
stress and incidence of coronary artery: Disease in middle aged men. The
American Journal of Cardiology, 68, 1171-1175.
Scottish Intercollegiate Guidelines Network. (2007). Risk estimation and the
prevention of cardiovascular disease: A national clinical guideline - no. 97.
SIGN, Edinburgh.
Steptoe, A., & Wardle, J. (1994). Coping with illness and disability. In A. Steptoe &
J. Wardle (Eds.), Psychosocial processes and health. Cambridge University
Press.
Task Force of the European Society of Cardiology. (1997). Management of stable
angina pectoris. European Heart Journal, 18, 394-413.
Thompson, P. L., Wark, J., & Garland, S. (1976). The heart attack and doctor/patient
communication. The Medical Journal of Australia, 1, 166-167.
Tzeng, H. M., & Ketefian, S. (2003). Demand for nursing competencies: An
exploratory study in Taiwan's hospital system. Journal of Clinical Nursing,
12(4), 509-518.
Weinman, J., & Petrie, K. J. (1997). Illness perceptions: A new paradigm for
psychosomatics? Journal of Psychosomatic Research, 42(2), 113-116.
Weinman, J., Petrie, K. J., Sharpe, N., & Walker, S. (2000). Causal attributions in
patients and spouses following first-time myocardial infarction and
24
subsequent lifestyle changes. British Journal of Health Psychology, 5,
263-273.
Wynn, A. (1967). Unwarranted emotional distress in men with ischaemic heart
disease. The Medical Journal of Australia, 2, 847-851.
25
Table 1 Characteristics of hospital nurses
n=64 No (%)
Gender Females 64 (100)
Type of ward Cardiac ward 13 (20.3)
General medical 51 (79.7)
Length of time on
current ward (years)
< 1 4 (6.3)
1-2 16 (25.0)
2-5 19 (29.7)
5-10 23 (35.9)
10-15 2 (93.1)
Level of qualification Practical nurse 3 (4.7)
Registered nurse 61 (95.3)
Education Technological
academy
38 (59.4)
College/University 26 (40.6)
Cardiac specialist
qualification
Yes 5 (7.8)
No 59 (92.2)
Age (years) Min: 20 Max: 50 Mean: 30 SD: 6.88
Total years working
in nursing
Min: 0.5 Max: 30 Mean: 7.80 SD: 6.22
26
Table 2 Characteristics of nursing students
n=134 No (%)
Gender Females 134 (100)
Degree system 4-year college 92 (68.7)
2-year college 42 (31.3)
Working experience
in nursing (years)
None 124 (92.5)
1-2 8 (6.0)
2-5 1 (0.7)
> 5 1 (0.7)
Level of qualification Practical nurse 93 (69.4)
Registered nurse* 32 (23.9)
None 9 (6.7)
Cardiac specialist
qualification
Yes 0
No 134 (100)
Age (years) Min: 18 Max: 40 Mean: 20 SD: 2.16
* They are already registered nurses.
27
Table 3 Characteristics of patients
n=238 No (%)
Age mean (SD) 71 0(10.63)
Gender Male 139 (58.4)
Female 99 (41.6)
Marital status Unmarried 8 0(3.4)
Married 192 (80.7)
Divorced 8 0(3.4)
Widowed 30 (12.6)
Work status Working 47 (19.7)
Retired 156 (65.5)
Unemployed 2 0(0.8)
Off sick 1 0(0.4)
Other(housewife) 32 (13.4)
Education None/Never 22 0(9.2)
Primary 60 (25.2)
Secondary 35 (14.7)
High 62 (26.1)
College/University 54 (22.7)
Graduate 5 0(2.1)
Comorbidity None 45 (18.9)
Diabetes 11 0(4.6)
Hypertension 126 (52.9)
Diabetes & hypertension 46 (19.3)
Others 10 0(4.2)
Years since
diagnosis
mean(SD) 5.6 00(4.73)
28
Table 4 Total score on pYCBQ in each group
Group n Mean SD Range
Nurses 64 12.13 2.94 5-20
Cardiac nurses 13 12.38 2.91 5-15
General nurses 51 12.06 2.97 5-20
Nursing students 134 11.23 2.84 4-17
All nurses 198 11.50 2.90 4-20
Patients 238 13.66 2.89 4-19
29
Table 5 Standard regression analysis on score of pYCBQ
Unstandardised
coefficient
B
Standardised
coefficient
Beta t Sig.
Education -1.68 -.27 -2.31 .024
Length time on
current ward (years) -.22 -.25 -2.04 .042
30
Table 6 Comparison of the misconceptions held by patients and nurses
Item statement
n (%) holding misconception
Nurses
n=198
Patients
n=238
X2
Sig.
(df=1)
1. A heart attack makes a weak area in the heart wall that can easily
rupture 131 (66.2) 176 (73.9) 3.15 .076
2. People who have heart problems should never get excited or upset 55 (27.8) 188 (79.0) 114.91 <.001
3. Once you have had one heart attack you are bound to have another one 166 (83.8) 169 (71.0) 10.00 .002
4. It‟s OK to disagree with people with heart problems 39 (19.7) 29 (12.2) 4.63 .031
5. People develop heart disease because of worry in their life 72 (36.4) 138 (58.0) 20.24 <.001
6. Angina is a kind of small heart attack 147 (74.2) 189 (79.4) 1.63 .201
7. People with heart problems should live life to the full 46 (23.2) 28 (11.8) 10.09 .001
8. There‟s not much you can do about heart problems 22 (11.1) 117 (49.2) 72.05 <.001
9. Any sort of excitement could be bad if you have heart problems 95 (48.0) 202 (84.9) 67.74 <.001
10 It‟s a good idea to check to see how you feel before doing something 148 (74.7) 211 (88.7) 14.38 <.001
11 Doing exercise can strengthen the heart muscle 16 (8.1) 22 0(9.2) 0.18 .668
12 Heart problems are a sign that you have a worn out heart. 153 (77.3) 187 (78.6) 0.11 .745
13 You can reduce your risk of more heart problems 20 (10.1) 15 0(6.3) 2.11 .146
14 Heart problems will definitely shorten your life whatever age you are 103 (52.0) 154 (64.7) 7.19 .007
15 One of main causes of heart disease is stress 161 (81.3) 196 (82.4) 0.08 .779
16 It is dangerous for people who have heart problems to argue 158 (79.8) 182 (76.5) .70 .404
17 People with heart disease should take life easy 173 (87.4) 229 (96.2) 11.76 .001
18 It is important to avoid anything that might bring on angina or chest
pain
178 (89.9) 221 (92.9) 1.22 .270
19 Heart problems are often caused by people‟s lifestyle 46 (23.2) 33 (13.9) 6.39 .011
20 People who have a heart problem should always avoid stress 98 (49.5) 210 (88.2) 78.22 <.001
21 Rest is the best medicine for heart problems 154 (77.8) 189 (79.4) 0.17 .678
22 It is important for people with heart problems to carry on doing
enjoyable things
18 (9.1) 4 0(1.7) 12.39 .001
23 Your heart is like a battery, the more you do, the faster it runs down 81 (40.9) 144 (67.1) 29.29 <.001
24 Changing your lifestyle can reduce your risk of more heart problem 1 0(2.3) 4 0(1.7) 1.32 .251