46
CARDIAC MURMURS Dr. saeid Family physician 2014
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | saeid-khezer |
| View: | 161 times |
| Download: | 2 times |

CARDIAC MURMURS
Dr. saeid Family physician 2014

Cardiac Murmurs
Murmurs are audible successive sounds with distinct duration, as opposed to normal heart sounds, which are short transitory events.
MechanismThey are due to turbulence of blood
flow through vessels, valves, & heart chambers or from vibration in valves, vessels or
adjacent
structures…

1. Flow across a partial
obstruction.e.g. aortic stenosis
2. Flow across a valvular or intravascular irregularity without obstruction. e.g. a bicuspid aortic valve without true stenosis.

3. Increased f low through normal structures.
e.g. aortic systolic murmur associated with anemia.
4. Flow into a dilated chamber. e.g. aortic systolic murmur associated with aneurismal dilatation of the ascending aorta.

5. Backward or regurgitation flow across an incompetent valve or defect. e.g. mitral regurgitation.
6. Shunting of blood out of a high pressure chamber or artery through an abnormal passage.
e.g. VSD, PDA
Character of Character of heart murmursheart murmurs

Timing in cardiac cycle:
Duration:
Pitch/Quality: (Range of frequency)
-High frequency: (MR, TR, AR) -Low frequency: (MS, TS)
Intensity (Loudness): Grading from I to VI
Thrill is absent : in grade I II IIIThrill is present: in grade IV V VI

Variation in intensity of Variation in intensity of murmurmurmur
Crescendo versus Crescendo versus DecrescendoDecrescendo
Crescendo-decrescendo --- Crescendo-decrescendo --- PlateauPlateau
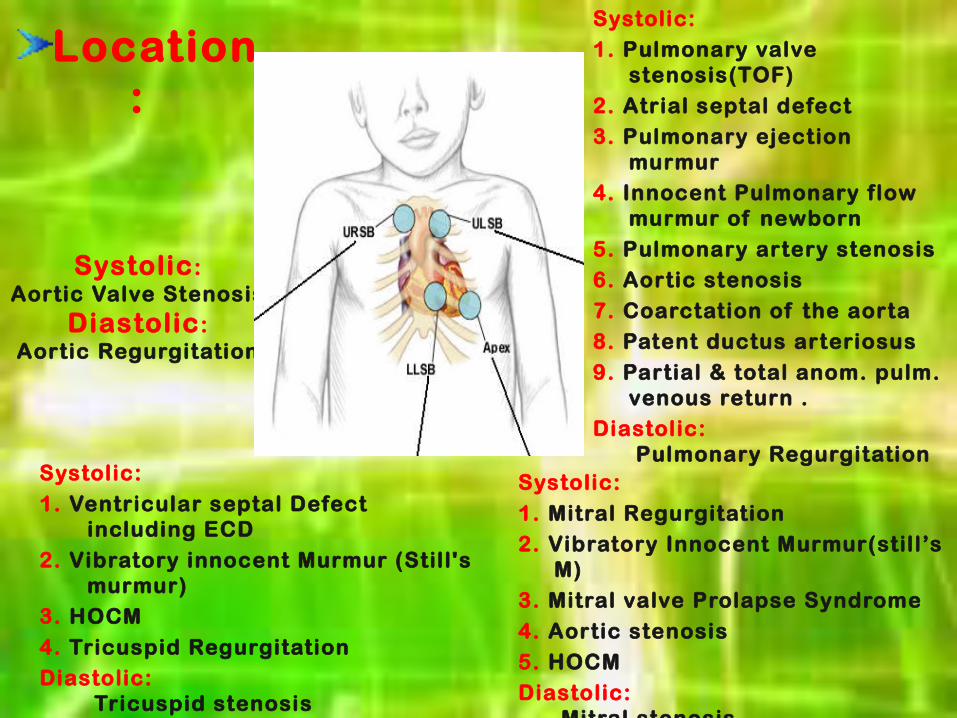
Location:
Systolic :Aortic Valve Stenosis
Diastolic :Aortic Regurgitation
Systolic:1. Pulmonary valve
stenosis(TOF)
2. Atrial septal defect3. Pulmonary ejection
murmur4. Innocent Pulmonary flow
murmur of newborn
5. Pulmonary artery stenosis6. Aortic stenosis
7. Coarctation of the aorta8. Patent ductus arteriosus
9. Partial & total anom. pulm. venous return .
Diastolic: Pulmonary Regurgitation
Systolic:
1. Ventricular septal Defect including ECD
2. Vibratory innocent Murmur (Still's murmur)
3. HOCM
4. Tricuspid RegurgitationDiastolic:
Tricuspid stenosis
Systolic:
1. Mitral Regurgitation2. Vibratory Innocent Murmur(still’s
M)3. Mitral valve Prolapse Syndrome
4. Aortic stenosis
5. HOCMDiastolic:
Mitral stenosis

Cont . Cont .
Point of maximal intensity:
Radiation:
Variation in features:
Classif ication:Classif ication:
1. Innocent 1. Innocent 80%80% 2. Pathological2. Pathological
Innocent murmur:Innocent murmur:Innocent murmurs are heard when blood moves noisily through a normal heart. Blood is f lowing faster than usualAn increased amount of blood
Fever , infection,
anxiety Anaemia ,
hyperthyroidism.

Classical vibratory (still s) ̓murmur:
Peak age: 3 to 6 years Quality: Vibratory or
musical & medium - pitched
Intensity: Il or IIl / VI Timing: Ejection systolic Location: Between apex &
LLSB Radiation: Well-localized Maneuvers: Increase in Exercise &
Supine Decrease in Sitting &
standing

Pulmonic ejection murmur (Pulmonic
outflow murmur) Peak age: 8 to 14 years Quality: Rough & high
pitch Intensity: I or llI / VI Timing: Ejection systolic Location: Right base
(ULSB) Radiation: Well-localized Maneuvers: Increase in Exercise,
Supine, Valsalva maneuver, thin chest; pectus excavetum

Pulmonary flow murmur of newborn:
Quality: Harsh, high frequency
Intensity: l or ll / VI
Timing: systolic ejection murmur
Location: upper left sternal border
Radiation: back and in both axilla
Maneuvers: decrease or disappear with the valsalva

Carotid or brachiocephalic arterial
bruit:Peak age: 2 to 10 years Quality: HarshIntensity: ll or lll / VITiming: Early ejection
systolic Location: Supraclavicular
fossaRadiation: NeckManeuvers: -Increase in exercise -Decrease in Shoulders
back & chin forward
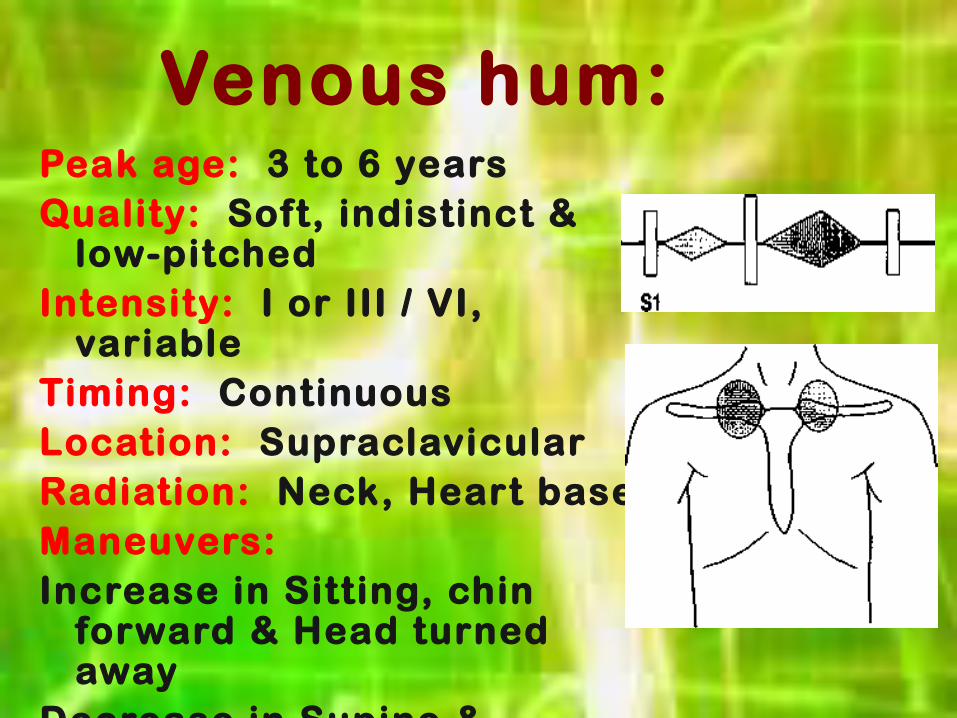
Venous hum: Peak age: 3 to 6 years Quality: Soft, indistinct &
low-pitchedIntensity: I or III / VI,
variable Timing: ContinuousLocation: SupraclavicularRadiation: Neck, Heart baseManeuvers: Increase in Sitting, chin
forward & Head turned away
Decrease in Supine & Pressure over neck ( jugular vein)
WHEN TO REGARD WHEN TO REGARD MURMUR PATHOLOGICAL MURMUR PATHOLOGICAL
ONE?ONE?Type of Type of Pathological Pathological
MurmursMurmurs

1.Systolic Murmur
Ejection murmurs:
1. PS, AS, ASD 2. others: e.g.:
HOCM, Coarctation of aorta
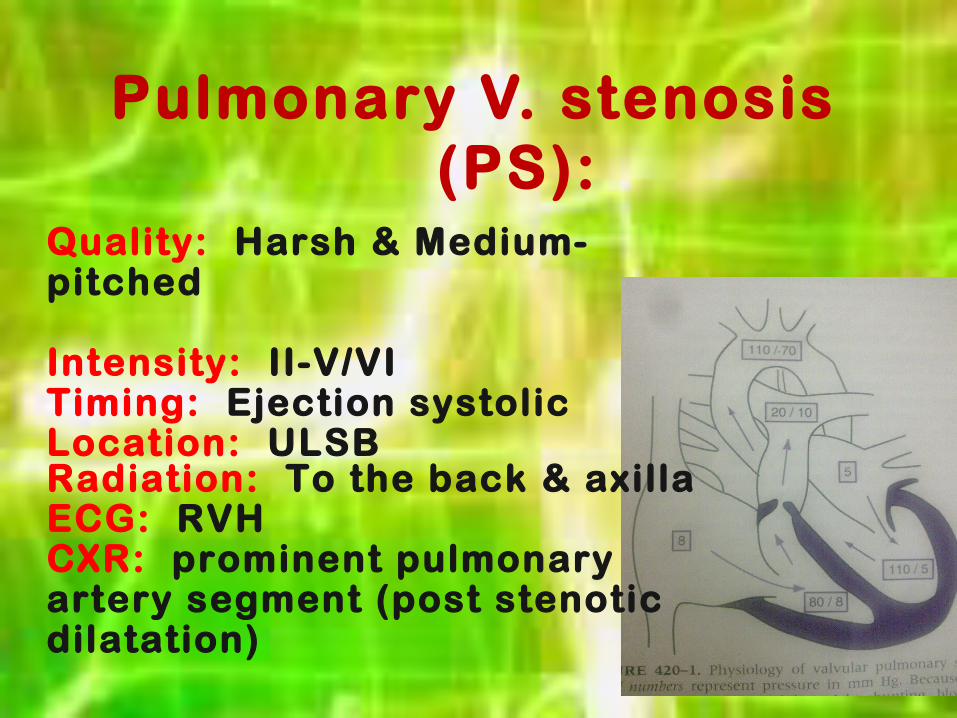
Pulmonary V. stenosis (PS):
Quality: Harsh & Medium- pitched Intensity: II-V/VITiming: Ejection systolic Location: ULSBRadiation: To the back & axillaECG: RVH CXR: prominent pulmonary artery segment (post stenotic dilatation)

Aortic V. Stenosis (AS):
Quality: Harsh & Medium-pitched
Intensity: II-V / VI
Timing: Ejection systolic
Location: URSB
Radiation: Neck
ECG: LVH
CXR: Post stenotic dilatation
Maneuvers: Heard best with the
patient sitting and
leaning forward


Atrial Septal Defect
Quality: Soft ejection systolic
Intensity: ll-lll / Vl
Location: ULSB
Radiation: ASD primum may radiate to left axilla
CXR: Mild cardiomegaly & increase pulmonary vascular marking

Hypertrophic cardiomyopathy:
Quality: Harsh & Medium-Pitched Intensity: II-IV / VI Timing: Ejection systolic Location: LLSB Radiation: left sternal border, apex,
possibly to the base, but not to the neck. CXR: cardiomegaly ECG: LVH +- RVH Maneuvers: Decreases with squatting,
increases with standing & valsalva.


Coarctation of the Aorta:
Timing: Short Systolic ejection
Location: LSB at 3 R D-4 T H ICS
Radiation: Left interscapular area of the back & neck
CXR: Cardiac enlargement & rib notching
ECG: LVH
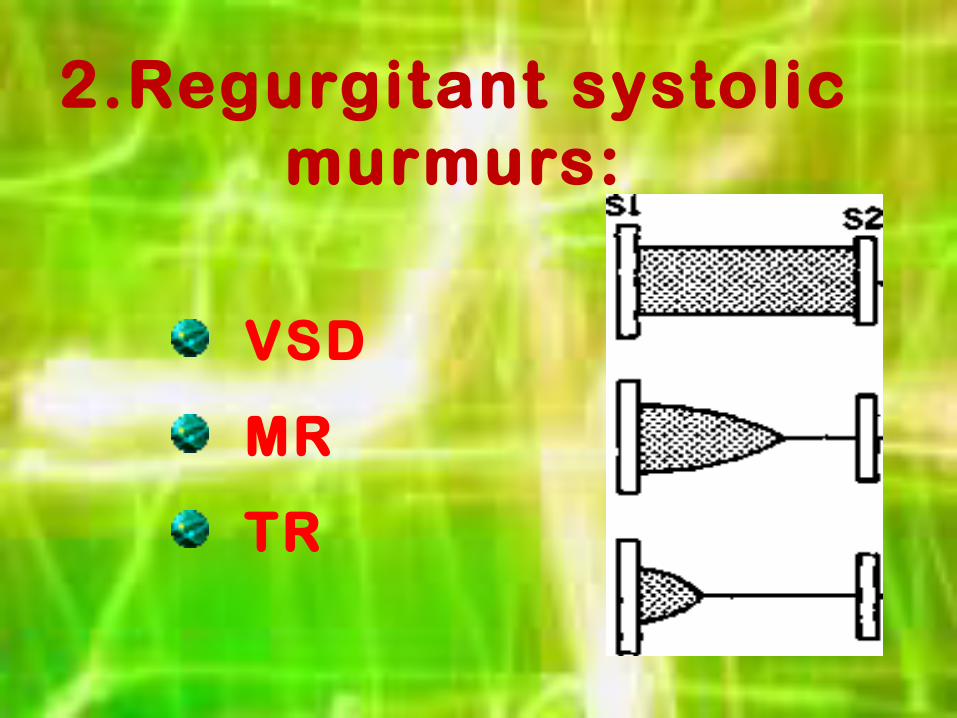
2.Regurgitant systolic murmurs:
VSD
MR
TR

Ventricular Septal Defect
Quality: Harsh & High-pitched
Intensity: II-V / VI
Timing: Pan systolic
Location: LLSB
Radiation: Well localized
ECG: variable, RVH, BiVH,
CXR: cardiomegaly & increase pulmonary vascular marking.

Mitral Regurgitation (MR):
Quality: Harsh & Medium to high-pitched
Intensity: II-III/VI Timing: Regurgitant systolic Location: Apex Radiation: Left axilla ECG: Bif id P-wave(P- mitrale) &
LVH,, CXR: confirm the LVH.
Tricuspid regurgitation (TR):
Quality: Harsh & Medium-pitched Intensity: II-III/VITiming: Regurgitant systolic Location: LLSB(4TH ICS) Radiation: right of the sternum, xiphoid area, left midclavicular line, Maneuvers: the intensity may increase slightly with inspiration (carvallo`s sign)

2. Dias to l i c Murmurs2. Dias to l i c MurmursAR
PR
PDA
TS
MS

Early Early diastolicdiastolic murmurs murmurs
caused by incompetence of the aortic or pulmonary valve.
AR murmurs are high pitched and blowing in quality, may be mistaken with breath sound, best heard with the diaphragm of a stethoscope at the 2 n d-4 t h right intercostal space.
It radiates well to the apex Bounding peripheral pulses may be present if the AR is significant.

Cont.
This murmur is heard best with the patient sitting, lining forward & breath held in exhalation. Is grade 1-3, with out thrill.. CXR & ECG shows LVH.
PR They are usually medium pitched but may be high pitched if pulmonary hypertension is present. They are best heard at the third left ICS and radiate along the left sternal border. ECG shows RVH, CXR confirm it also with dilated pulmonary vessels
Mid-diastolic murmurs :
These murmurs are caused by turbulence in the mitral or tricuspid valve secondary to stenosis.

Cont. Mitral mid-diastolic murmurs are best
heard at the apex. Associated with mitral stenosis (MS) or a large L-R shunt, VSD or PDA, which produces relative MS secondary to a large flow across the normal-sized mitral valve.
Tricuspid mid-diastolic murmurs are best heard along the LLSB. Associated with ASD, PAPVR, TAPVR, and ECD, because they all result in relative tricuspid stenosis (TS).

Presystolic murmurs:
They result from active atrial contraction that ejects blood into the ventricle, rather than a passive pressure dif ference between the atrium and ventricle.
These low frequency murmurs occur late in diastole or just before the onset of systole and are found with anatomic stenosis of the mitral or tricuspid valve.

3.Continuous Murmurs:
1. Aortopulmonary or arteriovenous
connection. e.g., PDA, arteriovenous fistula, after
systemic-to-PA shunt surgery, persistent truncus arteriosus (rarely)
2. Disturbance of f low pattern in arteries (e.g., COA, PA stenosis)

Cont.
The murmur of PDA has a machinery-like quality, maximally heard in the left infraclavicular area or ULSB. With pulmonary hypertension, only the systolic portion can be heard, but it is crescendic during systole.


Evaluation of murmur:Evaluation of murmur:
History:Clinically:
Eight keys to efficient and adequate cardiac auscultation:

INVESTIGATION:
1. Chest X-ray
2. ECG
3. Echocardiography
4. Cardiac catheterization
5. MRI

How Are Heart Murmurs Treated?
Innocent Murmurs:In anaemia,
hyperthyroidism, or fever, the murmur will go away once the illness or condition is treated.
Pathological Murmurs: Varies depending on the specific heart problem. Either medicine or surgery.

THANK YOUTHANK YOU

















