919 J. Parasitol., 88(5), 2002, pp. 919–925 q American Society of Parasitologists 2002 CARDIAC MYOCYTE HYPERTROPHY AND PROLIFERATING CELL NUCLEAR ANTIGEN EXPRESSION IN WISTAR RATS INFECTED WITH TRYPANOSOMA CRUZI Marı ´a Rosa Arnaiz, Laura Edith Fichera, and Miriam Postan* Instituto Nacional de Parasitologı ´a ‘‘Dr. Mario Fatala Chaben’’/ANLIS and Consejo Nacional de Investigaciones Cientı ´ficas y Te ´ cnicas (CONICET), Buenos Aires, Argentina. e-mail: [email protected]ABSTRACT: Chagasic cardiomyopathy is a major life-threatening complication of Trypanosoma cruzi infection in human beings. This study focuses on the hypertrophic and hyperplastic mechanisms underlying the structural changes of the heart during experimental infection. Proliferating cell nuclear antigen (PCNA) expression, transversal diameter, nuclear area, and number of nuclei per unit volume were determined in the ventricular myocytes of T. cruzi–infected Wistar rats. PCNA expression was enhanced throughout the inflamed myocardium and in the spared areas of the left ventricular wall and the septum. Myocyte width increased from 26 to 75% at the inflammation-free myocardium (P , 0.0001), whereas it decreased 25% at the inflamed left ventricular wall areas (P , 0.001). Nuclear size increased in the inflammation-free myocardium of the left ventricle and the septum (.10–36%, P , 0.01 and .0.2–32%, P , 0.03, respectively) and decreased at the inflamed areas of the left ventricular wall (10–22%, P , 0.02) with respect to the controls. The number of nuclei per unit volume decreased at the inflamed myocardium regardless of topographical location (36–65%) with respect to the controls (P , 0.0001) and in the inflammation-free myocardium of the right ventricle and the septum (,21–37%, P , 0.002 and ,8–39%, P , 0.002, respectively). These results show that the heart responds to T. cruzi infection with DNA repair and cell multiplication in the inflamed sites and with hypertrophy of the unaffected myocardium. Chagas’ disease is a major life-threatening complication of Trypanosoma cruzi infection in human beings (Morel, 2001). Longitudinal studies indicate that approximately 45% of the infected individuals who become chronic develop progressive heart or digestive disease (or both). Cardiac involvement is characterized by degeneration and loss of cardiac myocytes, mononuclear cell infiltration with cytokine secretion, and fibro- sis of the myocardium. The roles of both the parasite and the host immune system in the outcome of chagasic myocarditis have been extensively studied, but the mechanisms underlying the structural changes of the cardiomyopathy remain unknown. The normal adult heart responds to the loss of myocardial cells and altered hemodynamic conditions by increasing the volume of the remaining myocytes (hypertrophy) or the total number of cells (hyperplasia) (or both) (Olivetti et al., 1991; Anversa and Kajstura, 1998). Myocyte hypertrophy or hyper- plasia in the pathological heart appears to result from the mag- nitude of the hemodynamic stress (Anversa and Kajstura, 1998). Proliferating cell nuclear antigen (PCNA), a nuclear pro- tein expressed in the late G1-phase and during the S-phase of the cell cycle, is used frequently to detect DNA replication and hyperplasia, as well as DNA repair in viable cells (Shivji et al., 1992; Kajstura et al., 1994; Beltrami et al., 1997; Anversa and Kajstura, 1998). In the present study we address the issue whether cardiac myocytes located in T. cruzi–induced inflam- matory lesions and in the spared myocardium undergo hyper- trophy or increase the synthesis of DNA during experimental infection (or both). MATERIALS AND METHODS Infection of animals Four- to six-wk-old male and female Wistar rats (Comisio ´n de Ener- gı ´a Ato ´mica, Buenos Aires, Argentina) and T. cruzi clone Sylvio-X10/ 4 were used. The rats were selected at random and inoculated intraper- itoneally with 10 6 bovine skin and skeletal muscle (BESM) cell culture– derived trypomastigotes, as described previously (Postan et al., 1983). Received 11 January 2002; revised 24 April 2002; accepted 26 April 2002. * To whom correspondence should be addressed. Sham-inoculated rats were used as controls. Infected and control rats were housed separately, with food and water ad libitum. Tissue sampling Infected and control rats were ether anesthetized and bled by intra- cardiac puncture immediately before killing by cervical dislocation. The heart was removed, and samples were obtained from halfway between the base and the apex containing the free right ventricle (RV) and left ventricle (LV) walls and the septum. Tissues were fixed in 10% buffered formalin, processed routinely, and embedded in paraffin. Five-mm sec- tions were cut and stained with hematoxylin and eosin, periodic-acid– Schiff (PAS) counterstained with hematoxylin, and Masson’s trichrome for routine histopathological analysis. Infected rats exhibiting myocar- ditis and controls with normal histology were selected for the study. A total of 39 rats that met the selection criteria were included as follows: 8 infected and 7 controls rats were killed at 30 days postinfection (PI), 8 rats per group were killed at 375 days PI, and 4 rats per group were killed at 515 days PI. Histomorphometric analysis Precoded heart sections underwent double-blind examination under the light microscope, and the code was broken at the end of the exper- iment. Myocardial areas exhibiting obvious inflammation or fibrosis (in- fected inflamed [II]) (or both), and unaffected (infected noninflamed [INI]) myocardium were evaluated separately. Each field was first iden- tified at low-power magnification to determine the presence or absence of inflammation; then, they were selected as the initial condition for further study. Only cardiac myocytes with intact cell membrane iden- tified with PAS staining, and centrally located nuclei were analyzed. The morphometric parameters studied were myocyte transversal diam- eter (MTD), nuclear transectional area (NTA), and the number of myo- cyte nuclei per unit volume of myocardium (N(n)v) (Loud et al., 1978; Anversa et al., 1985). MTD and NTA were determined in longitudinally oriented sections at 31,000, using an ocular micrometer disc. Measure- ments were performed in mononucleated myocytes taken at random from inflamed and inflammation-free myocardium at the LV, RV, and septum (50 cells per tissue status per wall). The distance between both sides of the myocytes (MTD) was determined at the plane across the nucleus. Transversal nuclear diameter (TDn) was measured at the nar- rowest site of the nucleus. Nuclear area was calculated with the equation for elliptic cross-section bodies: (longitudinal nuclear diameter/2) 3 (TDn/2) 3p (Liu et al., 1998). An ocular reticle delineating a square area of 0.062 mm 2 in the microscopic field at a magnification of 3400 was used to quantify the number of nuclear profiles per unit area (N(n)A) in transversally oriented myocardial tissue sections. Four of such fields per inflamed and inflammation-free myocardium per wall were analyzed in infected animals (1.488 mm 2 per rat) and on randomly selected areas per wall in the controls (0.744 mm 2 per rat). The equation
Transcript
919
J. Parasitol., 88(5), 2002, pp. 919–925q American Society of Parasitologists 2002
CARDIAC MYOCYTE HYPERTROPHY AND PROLIFERATING CELL NUCLEAR ANTIGENEXPRESSION IN WISTAR RATS INFECTED WITH TRYPANOSOMA CRUZI
Marıa Rosa Arnaiz, Laura Edith Fichera, and Miriam Postan*Instituto Nacional de Parasitologıa ‘‘Dr. Mario Fatala Chaben’’/ANLIS and Consejo Nacional de Investigaciones Cientıficas y Tecnicas(CONICET), Buenos Aires, Argentina. e-mail: [email protected]
ABSTRACT: Chagasic cardiomyopathy is a major life-threatening complication of Trypanosoma cruzi infection in human beings.This study focuses on the hypertrophic and hyperplastic mechanisms underlying the structural changes of the heart duringexperimental infection. Proliferating cell nuclear antigen (PCNA) expression, transversal diameter, nuclear area, and number ofnuclei per unit volume were determined in the ventricular myocytes of T. cruzi–infected Wistar rats. PCNA expression wasenhanced throughout the inflamed myocardium and in the spared areas of the left ventricular wall and the septum. Myocytewidth increased from 26 to 75% at the inflammation-free myocardium (P , 0.0001), whereas it decreased 25% at the inflamedleft ventricular wall areas (P , 0.001). Nuclear size increased in the inflammation-free myocardium of the left ventricle and theseptum (.10–36%, P , 0.01 and .0.2–32%, P , 0.03, respectively) and decreased at the inflamed areas of the left ventricularwall (10–22%, P , 0.02) with respect to the controls. The number of nuclei per unit volume decreased at the inflamed myocardiumregardless of topographical location (36–65%) with respect to the controls (P , 0.0001) and in the inflammation-free myocardiumof the right ventricle and the septum (,21–37%, P , 0.002 and ,8–39%, P , 0.002, respectively). These results show that theheart responds to T. cruzi infection with DNA repair and cell multiplication in the inflamed sites and with hypertrophy of theunaffected myocardium.
Chagas’ disease is a major life-threatening complication ofTrypanosoma cruzi infection in human beings (Morel, 2001).Longitudinal studies indicate that approximately 45% of theinfected individuals who become chronic develop progressiveheart or digestive disease (or both). Cardiac involvement ischaracterized by degeneration and loss of cardiac myocytes,mononuclear cell infiltration with cytokine secretion, and fibro-sis of the myocardium. The roles of both the parasite and thehost immune system in the outcome of chagasic myocarditishave been extensively studied, but the mechanisms underlyingthe structural changes of the cardiomyopathy remain unknown.
The normal adult heart responds to the loss of myocardialcells and altered hemodynamic conditions by increasing thevolume of the remaining myocytes (hypertrophy) or the totalnumber of cells (hyperplasia) (or both) (Olivetti et al., 1991;Anversa and Kajstura, 1998). Myocyte hypertrophy or hyper-plasia in the pathological heart appears to result from the mag-nitude of the hemodynamic stress (Anversa and Kajstura,1998). Proliferating cell nuclear antigen (PCNA), a nuclear pro-tein expressed in the late G1-phase and during the S-phase ofthe cell cycle, is used frequently to detect DNA replication andhyperplasia, as well as DNA repair in viable cells (Shivji et al.,1992; Kajstura et al., 1994; Beltrami et al., 1997; Anversa andKajstura, 1998). In the present study we address the issuewhether cardiac myocytes located in T. cruzi–induced inflam-matory lesions and in the spared myocardium undergo hyper-trophy or increase the synthesis of DNA during experimentalinfection (or both).
MATERIALS AND METHODS
Infection of animals
Four- to six-wk-old male and female Wistar rats (Comision de Ener-gıa Atomica, Buenos Aires, Argentina) and T. cruzi clone Sylvio-X10/4 were used. The rats were selected at random and inoculated intraper-itoneally with 106 bovine skin and skeletal muscle (BESM) cell culture–derived trypomastigotes, as described previously (Postan et al., 1983).
Received 11 January 2002; revised 24 April 2002; accepted 26 April2002.
* To whom correspondence should be addressed.
Sham-inoculated rats were used as controls. Infected and control ratswere housed separately, with food and water ad libitum.
Tissue sampling
Infected and control rats were ether anesthetized and bled by intra-cardiac puncture immediately before killing by cervical dislocation. Theheart was removed, and samples were obtained from halfway betweenthe base and the apex containing the free right ventricle (RV) and leftventricle (LV) walls and the septum. Tissues were fixed in 10% bufferedformalin, processed routinely, and embedded in paraffin. Five-mm sec-tions were cut and stained with hematoxylin and eosin, periodic-acid–Schiff (PAS) counterstained with hematoxylin, and Masson’s trichromefor routine histopathological analysis. Infected rats exhibiting myocar-ditis and controls with normal histology were selected for the study. Atotal of 39 rats that met the selection criteria were included as follows:8 infected and 7 controls rats were killed at 30 days postinfection (PI),8 rats per group were killed at 375 days PI, and 4 rats per group werekilled at 515 days PI.
Histomorphometric analysis
Precoded heart sections underwent double-blind examination underthe light microscope, and the code was broken at the end of the exper-iment. Myocardial areas exhibiting obvious inflammation or fibrosis (in-fected inflamed [II]) (or both), and unaffected (infected noninflamed[INI]) myocardium were evaluated separately. Each field was first iden-tified at low-power magnification to determine the presence or absenceof inflammation; then, they were selected as the initial condition forfurther study. Only cardiac myocytes with intact cell membrane iden-tified with PAS staining, and centrally located nuclei were analyzed.The morphometric parameters studied were myocyte transversal diam-eter (MTD), nuclear transectional area (NTA), and the number of myo-cyte nuclei per unit volume of myocardium (N(n)v) (Loud et al., 1978;Anversa et al., 1985). MTD and NTA were determined in longitudinallyoriented sections at 31,000, using an ocular micrometer disc. Measure-ments were performed in mononucleated myocytes taken at randomfrom inflamed and inflammation-free myocardium at the LV, RV, andseptum (50 cells per tissue status per wall). The distance between bothsides of the myocytes (MTD) was determined at the plane across thenucleus. Transversal nuclear diameter (TDn) was measured at the nar-rowest site of the nucleus. Nuclear area was calculated with the equationfor elliptic cross-section bodies: (longitudinal nuclear diameter/2) 3(TDn/2) 3 p (Liu et al., 1998). An ocular reticle delineating a squarearea of 0.062 mm2 in the microscopic field at a magnification of 3400was used to quantify the number of nuclear profiles per unit area(N(n)A) in transversally oriented myocardial tissue sections. Four ofsuch fields per inflamed and inflammation-free myocardium per wallwere analyzed in infected animals (1.488 mm2 per rat) and on randomlyselected areas per wall in the controls (0.744 mm2 per rat). The equation
920 THE JOURNAL OF PARASITOLOGY, VOL. 88, NO. 5, OCTOBER 2002
TA
BL
EI.
His
tom
orph
omet
ric
para
met
ers
ofm
yoca
rdia
lce
lls
from
Wis
tar
rats
infe
cted
wit
hT
rypa
noso
ma
cruz
i.*
Par
am-
eter
RV
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
LV
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
Sep
tum
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
Nuc
lear
tran
sect
iona
lar
ea(m
m2 )
II INI
CO
66.3
16
4.09
74.9
66
4.41
71.2
56
6.69
62.9
56
3.57
†83
.09
66.
5475
.05
63.
09
73.8
76
8.18
†87
.28
64.
9274
.80
65.
96
67.4
96
6.11
†‡82
.44
65.
96§
75.0
06
5.57
63.1
36
2.42
†‡90
.12
65.
06§
80.8
06
3.59
66.2
16
12.0
0‡10
1.10
65.
10§
74.2
26
3.79
69.3
86
3.89
†77
.10
63.
88§
76.9
26
6.04
64.0
26
4.58
†94
.63
66.
62§
71.7
06
4.53
70.6
06
11.5
591
.58
68.
12§
83.6
56
7.07
Myo
cyte
tran
sver
sal
diam
eter
(mm
)
II INI
CO
12.4
46
1.28
†15
.76
61.
02§
10.5
16
0.54
10.9
46
0.36
†17
.32
60.
96§
11.2
26
0.46
15.4
46
2.42
20.2
96
1.06
§11
.60
60.
36
12.6
26
1.20
†15
.51
60.
84§
11.0
36
0.69
10.4
36
0.31
†‡18
.15
60.
69§
13.7
96
1.01
13.8
56
1.84
18.5
06
0.41
§12
.50
60.
30
13.0
06
1.41
†15
.93
60.
55§
11.3
66
0.72
10.8
56
0.82
†18
.84
60.
30§
14.9
46
0.91
15.5
26
2.98
16.7
46
0.65
§12
.67
60.
49
N(n
)v
II INI
CO
3.08
60.
60†‡
4.02
60.
56§
5.07
60.
59
1.46
60.
14†‡
3.16
60.
38§
4.26
60.
20
1.44
60.
20†‡
2.18
60.
31§
3.43
60.
22
2.75
60.
71†‡
3.99
60.
574.
306
0.42
1.58
60.
14†‡
2.44
60.
343.
356
0.38
1.62
60.
34†‡
2.63
60.
213.
576
0.82
3.06
60.
26†‡
4.44
60.
44§
4.83
60.
47
1.86
60.
24†‡
2.52
60.
31§
4.11
60.
26
1.53
60.
37†‡
2.69
60.
48§
3.72
60.
36
*A
bbre
viat
ions
:R
V,
righ
tve
ntri
cle;
LV
,le
ftve
ntri
cle;
PI,
post
infe
ctio
n;II
,in
fect
ed-i
nflam
edm
yoca
rdiu
m;
INI,
infe
cted
-non
infl
amed
myo
card
ium
;C
O,
myo
card
ium
from
cont
rol
rats
.†
Indi
cate
sst
atis
tica
lsi
gnifi
canc
e(P
,0.
05)
betw
een
INI
vers
usII
.‡
Indi
cate
sst
atis
tica
lsi
gnifi
canc
e(P
,0.
05)
betw
een
IIve
rsus
CO
.§
Indi
cate
sst
atis
tica
lsi
gnifi
canc
e(P
,0.
05)
betw
een
INI
vers
usC
O.
N(n)v 5 (N(n)A)/LDn, described by Anversa et al. (1985), was appliedto determine cell hypertrophy, keeping in mind that the relative pro-portions of mononucleated and multinucleated myocytes remain con-stant both in the aging and in the pathological heart (Olivetti et al.,1996).
Immunohistochemistry
A direct avidin–biotin immunohistochemical technique was used forPCNA localization. Paraffin sections were collected on slides coatedwith 3-amino-propyltrieth-oxy-silane (Sigma Chemical Company, St.Louis, Missouri). Endogenous peroxidase activity was quenched with3% hydrogen peroxide in methanol for 20 min. Sections were immersedin antigen-retrieving solution (Antigen Unmasking Solution, VectorLaboratories, Burlingame, California) and treated twice at 700 W in amicrowave oven for 5 min, with a resting time of 1 min between in-cubations. Nonspecific binding was blocked with phosphate-bufferedsaline (PBS) containing 5% normal goat serum and 1.5% nonfat drymilk for 30 min. Sections were incubated overnight with biotinylatedmouse monoclonal antibody (mAb) anti-human PCNA, clone PC10(Pharmingen, San Diego, California), at 4 C in a humidity chamber,followed by avidin–peroxidase complex (Vectastain Elite ABC, VectorLaboratories). Color was developed with 3,39-diaminobenzidine tetra-hydrochloride and hydrogen peroxide chromogen substrate. PAS andHarris’ hematoxylin were used to counterstain the sections. Heart serialsections obtained from each animal incubated with mouse anti-rat IgGmAb or PBS were used as negative controls. Breast tumor sections wereincluded in each batch of stains as the positive control.
Quantification of PCNA-positive myocytes
The number of PCNA-labeled myocytes was evaluated in four mi-croscopic fields at the inflamed and spared RV, LV, and septal myocar-dium of infected and control rats, using the reticle described above.Intact myocytes were identified morphologically with PAS staining, tak-ing care not to include myocardial cells undergoing necrosis, fibroblasts,pericytes, mononuclear inflammatory cells, and capillary endothelialcells in the analysis.
Statistical analysis
Data were expressed as the mean calculated from the average mea-surement obtained from each rat and wall 6 SD. Statistical analysis wasperformed by analysis of variance and Bonferroni’s methods. Compar-ison of data from infected rats and control rats was performed using acompletely aleatorized design; the data of inflamed compared with non-inflamed myocardium from infected animals were analyzed using com-plete blocks. Values of P , 0.05 were considered significant.
RESULTS
Histopathological analysis of the heart of Wistar rats infectedwith the T. cruzi clone Sylvio-X10/4 showed a small numberof intracellular parasite nests, degenerating and necrotic myo-cardial cells, inflammatory cell infiltration, and fibrosis of var-iable intensity, as described in other animal models (Postan etal., 1987). Multifocal inflammatory infiltrates consisting mainlyof lymphocytes and macrophages, with fewer polymorphonu-clear and mast cells, were more severe during the acute stageof infection. Interstitial thickening and patches of fibrous tissuewere observed throughout the infection, being more extensiveand severe during the chronic stage.
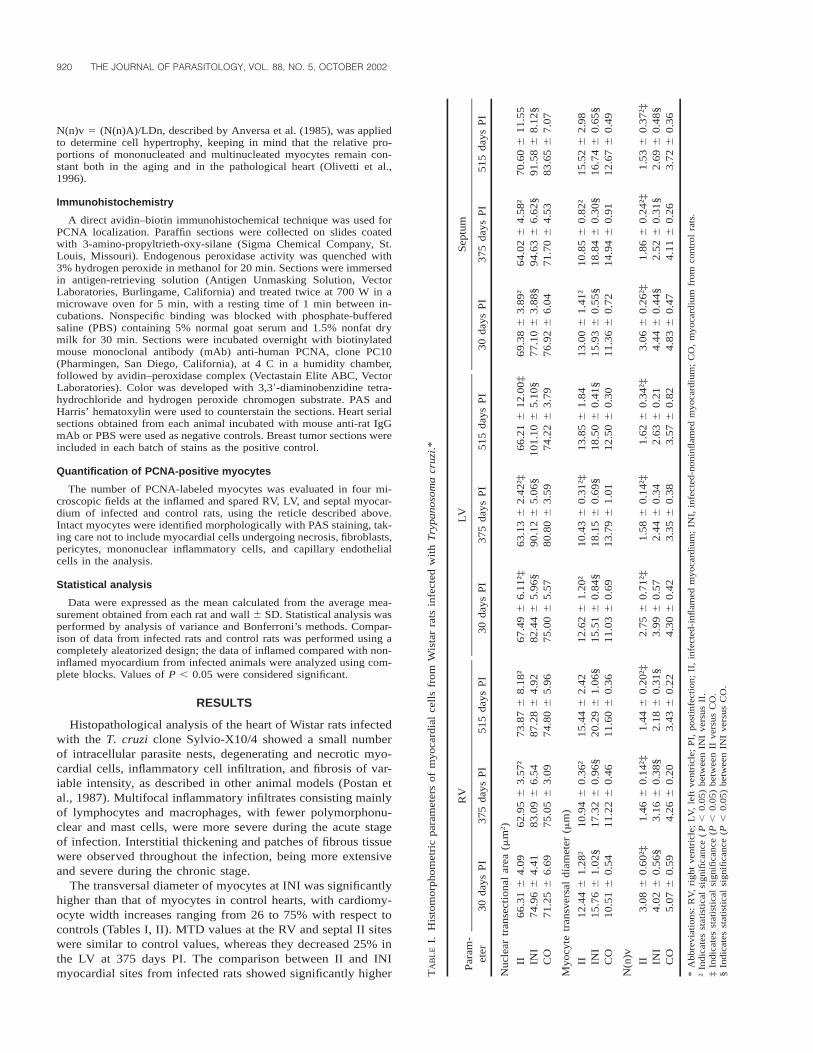
The transversal diameter of myocytes at INI was significantlyhigher than that of myocytes in control hearts, with cardiomy-ocyte width increases ranging from 26 to 75% with respect tocontrols (Tables I, II). MTD values at the RV and septal II siteswere similar to control values, whereas they decreased 25% inthe LV at 375 days PI. The comparison between II and INImyocardial sites from infected rats showed significantly higher
ARNAIZ ET AL.—CARDIAC REMODELING IN T. CRUZI INFECTION 921
TABLE II. Percentage of change in histomorphometric measurements from Wistar rats infected with Trypanosoma cruzi with respect to controls.*
Days PI
INI
NTA MTD N(n)v
II
NTA MTD N(n)v
RV 30375515
NSNSNS
149.96154.37174.91
220.71225.82236.45
NSNSNS
NSNSNS
239.26265.73258.02
Septum 30375515
10.23131.9819.48
140.23126.10132.12
28.07238.67227.69
NSNSNS
NSNSNS
236.65254.74242.74
LV 30375515
19.92111.53136.22
140.61131.62148.00
NSNSNS
210.00221.87210.79
NS224.76
NS
236.05252.83254.62
* Abbreviations: RV, right ventricle; LV, left ventricle; PI, postinfection; INI, infected-noninflamed myocardium; II, infected-inflamed myocardium; NTA, nucleartransectional area; MTD, myocyte transversal diameter; N(n)v, number of nuclei per unit volume of myocardium; NS, non-significant.
FIGURE 1. Photomicrograph showing PCNA-labeled nuclei in mononucleated and binucleated myocytes (arrows) in inflammatory foci 30days PI with Trypanosoma cruzi. PCNA labeling is also present in cellular infiltrates and interstitial cells. Bar in the lower right cornerrepresents 100 mm.
MTD values in the latter at 30 and 375 days PI. In addition,age-related MTD increases occurred at the INI myocardium ofinfected rats and the controls.
The transectional area of the nucleus at INI sites of the freeLV wall and the septum was significantly higher than in thecontrols, regardless of time of infection (Tables I, II). In con-trast, NTA at II sites of the LV was significantly smaller thanin the respective controls. Significant NTA differences werealso observed between II and INI sites of infected rat hearts,depending on the wall of the heart and the time of infection.
A 36–66% decrease in N(n)v values was found at II sitesfrom T. cruzi–infected rats with reference to the controls, de-
pending on both the topographic location within the heart andthe time of infection. N(n)v values at the RV and septum INIsites from infected rats were also smaller (21–36% and 8–39%,respectively) than those in the controls (Tables I, II). The de-crease in N(n)v values at II sites was more pronounced than atINI sites, regardless of time of infection.
Labeling of PCNA protein was detected in mononucleatedand binucleated cardiac myocytes, interstitial cells, and inflam-matory mononuclear cells infiltrating the myocardium of T. cru-zi–infected rats (Fig. 1). A low level of PCNA nuclear stainingwas detected also in myocytes and interstitial cells from non-infected control rats, as reported by other authors (Marino et
922 THE JOURNAL OF PARASITOLOGY, VOL. 88, NO. 5, OCTOBER 2002
FIGURE 2. Photomicrograph showing a binucleated myocyte positively stained for PCNA. Note the presence of PCNA-positive interstitial andinflammatory cells. Bar in the lower right corner represents 30 mm.
al., 1996). The frequency of PCNA-positive myocytes at II sitesof infected animals was significantly higher than in the controls,regardless of the topographical location within the heart and thetime of infection (Fig. 2; Table III). Myocyte PCNA labelingwas more frequent also at INI sites of the LV wall and theseptum with respect to the controls, in all periods of the infec-tion analyzed (Figs. 3, 4). Comparison between PCNA labelingin II and INI sites of infected animals showed a higher fre-quency of PCNA-positive myocytes at II myocardium of theRV during the 3 periods of infection and of the LV wall andthe septum at 375 days PI.
DISCUSSION
The major finding of the present study is the distinctive adap-tive response of the Wistar rat ventricular myocardium to T.cruzi–induced injury, depending on the region of the heart, thetime of infection, and the presence of inflammatory cells. Inthis animal model, myofibers tend to retain their normal widthat inflammation sites but enlarge significantly in the sparedmyocardium. Nuclei followed inconsistent patterns in relationto the dimension of myocytes. For example, myocytes with ex-panded cytoplasm had enlarged nuclei at the LV- and septal-spared myocardium but not at the RV wall. Paradoxically, thesize of nuclei at the RV-spared myocardium remained withinthe same range as that of the normal controls, in spite of beingat the level at which the highest myocyte width increases wereregistered. The values of N(n)v decreased throughout the myo-cardium of T. cruzi–infected rats, a change indicative of myo-cyte hypertrophy. But the equation N(n)v was designed pri-
marily to detect myocyte enlargement in pure hypertrophicheart conditions. The presence of a strong inflammatory com-ponent may make the equation unsuitable for estimation of thecell volume per nucleus in the inflamed myocardium. The de-creased cell volume per nucleus found at the inflammation siteprobably results from the expansion of the interstitial space byedema, inflammatory cells, and fibrosis rather than from an in-crease in myocyte size (Baandrup and Olsen, 1981). The in-dependent analyses of the number of nuclear profiles per unitarea and the mean nuclear length indicate that the cell volumeper nucleus changes at these sites were related to modificationsin nuclear density, whereas the length of myocyte nuclei tendsto remain constant (data not shown). Changes in nuclear densitywere described also in hypertensive Wistar rats, although nu-clear polymorphism also occurred (Mandarim-de-Lacerda andPereira, 2001).
The pattern of myocyte growth exhibited at the level of non-inflamed myocardium from T. cruzi–infected rats is similar tothe hypertrophic response described in the spared myocardiumduring infarction (Anversa et al., 1985). Myocyte hypertrophyin the spared myocardium of T. cruzi–infected rats developsearly after infection and persists throughout the chronic stage.On the other hand, the cells remaining viable within inflam-matory and fibrotic foci appear to be unable to undergo hyper-trophy. The behavior of individual myocytes during T. cruziinfection might be related to the altered atrial natriuretic factorplasma levels described previously (Scaglione et al., 2001).
Aging and pathological hearts respond to the loss of myo-cardial cells with myocellular hypertrophy, DNA synthesis, and
ARNAIZ ET AL.—CARDIAC REMODELING IN T. CRUZI INFECTION 923
FIGURE 3. Photomicrograph showing a PCNA-labeled myocyte in the margin of a fibrotic scar 375 days PI. Bar in the lower right cornerrepresents 30 mm.
FIGURE 4. Myocyte PCNA labeling in an unaffected ventricular site from a rat 375 days PI with Trypanosoma cruzi. Bar in the lower rightcorner represents 30 mm.
924 THE JOURNAL OF PARASITOLOGY, VOL. 88, NO. 5, OCTOBER 2002
TA
BL
EII
I.P
CN
Ala
beli
ngin
card
iac
myo
cyte
sfr
omW
ista
rra
tsin
fect
edw
ith
Try
pano
som
acr
uzi.
*
RV
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
LV
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
Sep
tum
30da
ysP
I37
5da
ysP
I51
5da
ysP
I
II INI
CO
2.13
60.
50†‡
0.72
60.
220.
106
0.03
2.59
60.
49†‡
0.94
60.
320.
366
0.09
2.69
60.
54†‡
0.88
60.
380.
526
0.20
1.72
60.
49†
1.06
60.
61§
0.16
60.
06
3.44
60.
70†‡
2.18
60.
78§
0.43
60.
18
1.88
60.
79†
0.94
60.
54§
0.41
60.
13
1.31
60.
39†
0.63
60.
15§
0.13
60.
05
3.22
60.
55†‡
1.94
60.
51§
0.71
60.
23
2.44
61.
01†
0.75
60.
18§
0.25
60.
05
*T
heva
lues
repr
esen
tth
em
ean
6S
Dof
PC
NA
1m
yocy
tes/
0,06
2m
m2 .
Abb
revi
atio
ns:
PC
NA
,pr
olif
erat
ing
cell
nucl
ear
anti
gen;
RV
,ri
ght
vent
ricl
e;L
V,
left
vent
ricl
e;P
I,po
stin
fect
ion;
II,
infe
cted
-infl
amed
myo
card
ium
;IN
I,in
fect
ed-n
onin
flam
edm
yoca
rdiu
m;
CO
,m
yoca
rdiu
mfr
omco
ntro
lra
ts.
†In
dica
tes
stat
isti
cal
sign
ifica
nce
(P,
0.05
)be
twee
nII
vers
usC
O.
‡In
dica
tes
stat
isti
cal
sign
ifica
nce
(P,
0.05
)be
twee
nIN
Ive
rsus
II.
§In
dica
tes
stat
isti
cal
sign
ifica
nce
(P,
0.05
)be
twee
nIN
Ive
rsus
CO
.
nuclear mitotic division (Olivetti et al., 1991; Quaini et al.,1994; Beltrami et al., 1997, 2001; Anversa and Kajstura, 1998;Kanoh et al., 1999; Petrovic et al., 2000). Necrosis in chagasicmyocarditis is characteristically associated with inflammationand fibrosis. The enhanced expression of PCNA protein foundat these sites probably reflects both DNA damage repair andreentry into the cell cycle (Shivji et al., 1992; Quaini et al.,1994; Soonpaa and Field, 1998). Although mitotic figures wererarely observed in the rats studied, the presence of binucleatedmyocytes positively labeled for PCNA in inflamed tissues sug-gests nuclear division. Mononucleated and binucleated myo-cytes expressing PCNA protein were observed previously inadult patients and also in animal models of other myocardialdiseases and after cardiac transplantation (Arbustini et al., 1993;Quaini et al., 1994; Liu et al., 1995; Beltrami et al., 1997).Whether the abnormal expression of PCNA protein representsa beneficial or detrimental effect in the development of chagasiccardiomyopathy remains to be determined.
There is increasing evidence that cytokines released locallyby both cardiac myocytes and myocardial inflammatory cellsplay an important role in the development of cardiovasculardisease (Matsumori, 1996; Meldrum, 1998). Tumor necrosisfactor alpha (TNF-a) and interleukin 1 beta (IL-1b) have a neg-ative effect on the contractility of cardiac myocytes throughinduction of nitric oxide (NO) synthase and NO release (Bal-ligand et al., 1993). NO is also a mediator for myocyte cellnecrosis (Pinsky et al., 1995; Meldrum 1998). Furthermore, itis known that IL-1b induces cardiac myocyte hypertrophy andreinitiates DNA synthesis (Palmer et al., 1995). TNF-a, IL-1b,IL-6, interferon-g, and transformation growth factor beta aresome of the cytokines known to be produced by inflammatorycells in the heart of chagasic patients and experimentally in-fected animals (Zhang and Tarleton, 1996; Reis et al., 1997;Huang et al., 1999). The enhanced expression of PCNA in theheart of T. cruzi–infected rats suggests that some of these cy-tokines may play an important role in cardiac remodeling dur-ing Chagas’ disease.
In summary, our study documents that ventricular myocytehypertrophy and hyperplasia participate in the cardiac remod-eling process during T. cruzi–induced myocarditis. Myocyte hy-pertrophy is the hallmark of the noninflamed myocardium. Onthe other hand, myocellular nuclear division and DNA repairprevail at inflammation sites. Both myocyte hypertrophy andhyperplasia can be considered as growth reserve mechanismsderived by the viable myocardial fraction to compensate for theloss of myocytes in the chagasic heart.
LITERATURE CITED
ANVERSA, P., C. BEGHI, Y. KIKKAWA, AND G. OLIVETTI. 1985. Myocardialresponse to infarction in the rat. Morphometric measurement ofinfarct size and myocyte cellular hypertrophy. American Journal ofPathology 118: 484–492.
———, AND J. KAJSTURA. 1998. Ventricular myocytes are not termi-nally differentiated in the adult mammalian heart. Circulation Re-search 83: 1–14.
ARBUSTINI, E., M. DIEGOLI, M. GRASSO, R. FASANI, A. D’ARMINI, L.MARTINELLI, C. GOGGI, C. CAMPANA, A. GAVAZZI, AND M. VIGANO.1993. Expression of proliferating cell markers in normal and dis-eased human hearts. American Journal of Cardiology 72: 608–614.
BAANDRUP, U., AND E. G. J. OLSEN. 1981. Critical analysis of endo-myocardial biopsies from patients suspected of having cardiomy-
ARNAIZ ET AL.—CARDIAC REMODELING IN T. CRUZI INFECTION 925
opathy. I: Morphological and morphometric aspects. British HeartJournal 45: 475–486.
BALLIGAND, J. L., D. UNGUREANU, R. A. KELLY, L. KOBZIK, D. PIMEN-TAL, T. MICHEL, AND T. W. SMITH. 1993. Abnormal contractile func-tion due to induction of nitric oxide synthesis in rat cardiac myo-cytes follows exposure to activated macrophage-conditioned me-dium. Journal of Clinical Investigation 91: 2314–2319.
BELTRAMI, A. P., C. DI LORETO, N. FINATO, M. ROCCO, D. ARTICO, E.CIGOLA, S. R. GAMBERT, G. OLIVETTI, J. KAJSTURA, AND P. ANVERSA.1997. Proliferating cell nuclear antigen (PCNA), DNA synthesisand mitosis in myocytes following cardiac transplantation in man.Journal of Molecular and Cellular Cardiology 29: 2789–2802.
———, K. URBANEK, J. KAJSTURA, S. M. YAN, N. FINATO, R. BUSSANI,B. NADAL-GINARD, F. SILVESTRI, A. LERI, C. A. BELTRAMI, AND P.ANVERSA. 2001. Evidence that human cardiac myocytes divide aftermyocardial infarction. New England Journal of Medicine 344:1750–1757.
HUANG, H., J. CHAN, M. WITTNER, L. A. JELICKS, S. A. MORRIS, S. M.FACTOR, L. M. WEISS, V. L. BRAUNSTEIN, C. J. BACCHI, N. YARLETT,M. CHANDRA, J. SHIRANI, AND H. B. TANOWITZ. 1999. Expressionof cardiac cytokines and inducible form of nitric oxide synthase(NOS2) in Trypanosoma cruzi-infected mice. Journal of Molecularand Cellular Cardiology 31: 75–88.
KAJSTURA, J., X. ZHANG, K. REISS, E. SZOKE, P. LI, C. LAGRASTA, W.CHENG, Z. DARZYNKIEWICZ, G. OLIVETTI, AND P. ANVERSA. 1994.Myocyte cellular hyperplasia and myocyte cellular hypertrophycontribute to chronic ventricular remodeling in coronary artery nar-rowing-induced cardiomyopathy in rats. Circulation Research 74:383–400.
KANOH, M., G. TAKEMURA, J. MISAO, Y. HAYAKAWA, T. AOYAMA, K.NISHIGAKI, T. NODA, T. FUJIWARA, K. FUKUDA, S. MINATOGUCHI, AND
H. FUJIWARA. 1999. Significance of myocytes with positive DNAin situ nick end-labeling (TUNEL) in hearts with dilated cardio-myopathy: Not apoptosis but DNA repair. Circulation 101: 2757–2764.
LIU, Y., E. CIGOLA, W. CHENG, J. KAJSTURA, G. OLIVETTI, T. H. HINTZE,AND P. ANVERSA. 1995. Myocyte nuclear mitotic division and pro-grammed myocyte cell death characterize the cardiac myopathyinduced by rapid ventricular pacing in dogs. Laboratory Investi-gation 73: 771–787.
———, A. LERI, B. LI, X. WUANG, W. CHENG, J. KAJSTURA, AND P.ANVERSA. 1998. Angiotensin II stimulation in vitro induces hyper-trophy of normal and postinfarcted ventricular myocytes. Circula-tion Research 82: 1145–1159.
LOUD, A. V., P. ANVERSA, F. GIACOMELLI, AND J. WIENER. 1978. Absolutemorphometric study of myocardial hypertrophy in experimental hy-pertension. I. Determination of myocyte size. Laboratory Investi-gation 38: 586–596.
MANDARIM-DE-LACERDA, C. A., AND L. M. MEIRELLES PEREIRA. 2001.Volume-weighted mean nuclear volume and numerical nuclear den-sity in the cardiomyocyte following enalapril and verapamil treat-ment. Virchows Archives 438: 92–95.
MARINO, T. A., W. CAO, J. LEE, AND R. COURTNEY. 1996. Localizationof proliferating cell nuclear antigen in the developing and maturerat heart cell. Anatomical Record 245: 677–684.
MATSUMORI, A. 1996. Cytokines in myocarditis and cardiomyopathies.Current Opinion in Cardiology 11: 302–309.
MELDRUM, D. R. 1998. Tumor necrosis factor in the heart. AmericanJournal of Physiology 274: R577–R595.
MOREL, C. M. 2001. Snippets of achievement. Vector control for Cha-gas’ disease. UNDP/World Bank/WHO, Special Programme forResearch and Training in Tropical Diseases. TDR/GEN/01.1.
OLIVETTI, G., E. CIGOLA, R. MAESTRI, D. CORRADI, C. LAGRASTA, S. R.GAMBERT, AND P. ANVERSA. 1996. Aging, cardiac hypertrophy andischemic cardiomyopathy do not affect the proportion of mono-nucleated and multinucleated myocytes in the human heart. Journalof Molecular and Cellular Cardiology 28: 1463–1477.
———, M. MELISSARI, J. M. CAPASSO, AND P. ANVERSA. 1991. Cardio-myopathy of the aging human heart. Circulation Research 68:1560–1568.
PALMER, J. N., W. E. HARTOGENSIS, M. PATTEN, F. D. FORTUIN, AND C.S. LONG. 1995. Interleukin-1b induces cardiac myocyte growth butinhibits cardiac fibroblast proliferation in culture. Journal of Clin-ical Investigation 95: 2555–2564.
PETROVIC, D., R. ZORC-PLESKOVIC, AND M. ZORC. 2000. Apoptosis andproliferation of cardiomyocytes in heart failure of different etiolo-gies. Cardiovascular Pathology 9: 149–152.
PINSKY, D. J., B. CAI, X. YANG, C. RODRIGUEZ, R. R. SCIACCA, AND P.J. CANNON. 1995. The lethal effects of cytokine-induced nitric ox-ide on cardiac myocytes are blocked by nitric oxide synthase an-tagonism or transforming growth factor-b. Journal of Clinical In-vestigation 95: 667–685.
POSTAN, M., J. A. DVORAK, AND J. P. MCDANIEL. 1983. Studies of Try-panosoma cruzi clones in inbred mice. I. A comparison of thecourse of infection of C3H/HeN-mice with two clones isolatedfrom a common source. American Journal of Tropical Medicineand Hygiene 32: 497–506.
———, J. P. MCDANIEL, AND J. A. DVORAK. 1987. Comparative studiesof infection of Lewis rats with 4 Trypanosoma cruzi clones. Trans-actions of the Royal Society of Tropical Medicine and Hygiene 81:415–419.
QUAINI, F., E. CIGOLA, C. LAGRASTA, G. SACCANI, E. QUAINI, C. ROSSI,G. OLIVETTI, AND P. ANVERSA. 1994. End-stage cardiac failure inhumans is coupled with the induction of proliferating cell nuclearantigen and nuclear mitotic division in ventricular myocytes. Cir-culation Research 75: 1050–1063.
REIS, M. M., M. L. HIGUCHI, L. A. BENVENUTI, V. DEMARCHI AIELLO, P.SAMPAIO GUTIERREZ, G. BELLOTTI, AND F. PILEGGI. 1997. An in situquantitative immunohistochemical study of cytokines and IL-2R1in chronic human chagasic myocardits: Correlation with the pres-ence of myocardial Trypanosoma cruzi antigens. Clinics in Im-munology and Immunopathology 83: 165–172.
SCAGLIONE, J., A. M. PUYO, H. A. DUPUY, M. POSTAN, AND B. E. FER-NANDEZ. 2001. Behaviour of atrial natriuretic factor in an experi-mental model of Trypanosoma cruzi infection in rats. Journal ofParasitology 87: 923–926.
SHIVJI, K. K., M. K. KENNY, AND R. D. WOOD. 1992. Proliferating cellnuclear antigen is required for DNA excision repair. Cell 69: 367–374.
SOONPAA, M. H., AND L. J. FIELD. 1998. Survey of studies examiningmammalian cardiomyocyte DNA synthesis. Circulation Research83: 15–26.
ZHANG, L., AND R. L. TARLETON. 1996. Persistent production of inflam-matory and anti-inflammatory cytokines and associated MHC andadhesion molecule expression at the site of infection and diseasein experimental Trypanosoma cruzi infection. Experimental Para-sitology 84: 203–213.