65
CARDIAC PHYSIOLOGY Submitted by: Poonam Negi MPT-II Yr, Cardiopulmonary
| Date post: | 11-Aug-2015 |
| Category: |
Healthcare |
| Upload: | poonam-negi |
| View: | 124 times |
| Download: | 2 times |
CARDIAC PHYSIOLOGY
Submitted by: Poonam Negi
MPT-II Yr, Cardiopulmonary

The Heart is a conical, hollow, muscular pump that lies:
• upon diaphragm• Posterior to sternum• Medial to lungs• Anterior to vertebral column• Base: lies beneath 2nd rib• Apex: at 5th intercostals
space
LOCATION

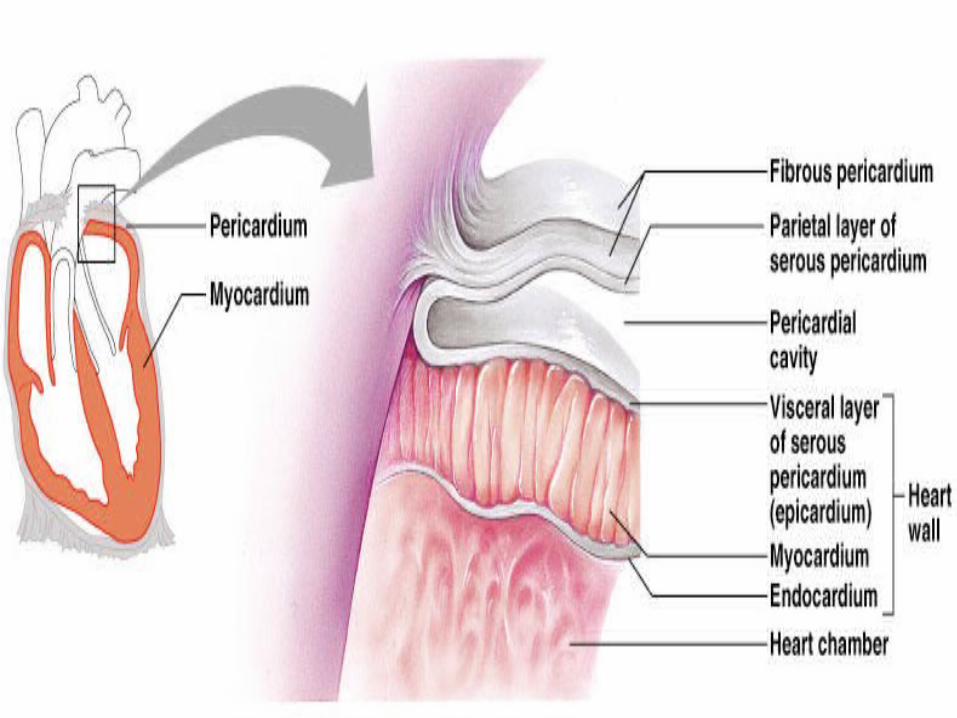
Pericardium – a double-walled sac around the heart that protects, anchors and prevents the overfilling of the heart. It also covers the roots of the great vessels. It is composed of:
1. A superficial fibrous pericardium
2. A deep two-layer serous pericardium The Parietal layer lines the internal surface of the fibrous
pericardium The Visceral layer lines the surface of the heart
3. They are separated by the serous fluid k/a Pericardial fluid which prevents friction as the heart beats
COVERINGS OF HEART
Epicardium – • Protective, outer layer of the heart wall same as the visceral
pericardium• The coronary blood vessels lies in the Epicardium
Myocardium – • Middle layer• Forms the bulk of the heart wall
Endocardium –• Inner layer• Smooth surface that permits blood to move easily• Continuous with lining of blood vessels
PERICARDIAL LAYERS
Vessels returning blood to the heart include:1. Superior and inferior venae cavae2. Right and left pulmonary veins
Vessels conveying blood away from the heart include:1. Pulmonary trunk, which splits into right and left pulmonary
arteries2. Ascending aorta (three branches) –
a. Brachiocephalicb. Left common carotidc. Subclavian arteries
Major Vessels of the Heart
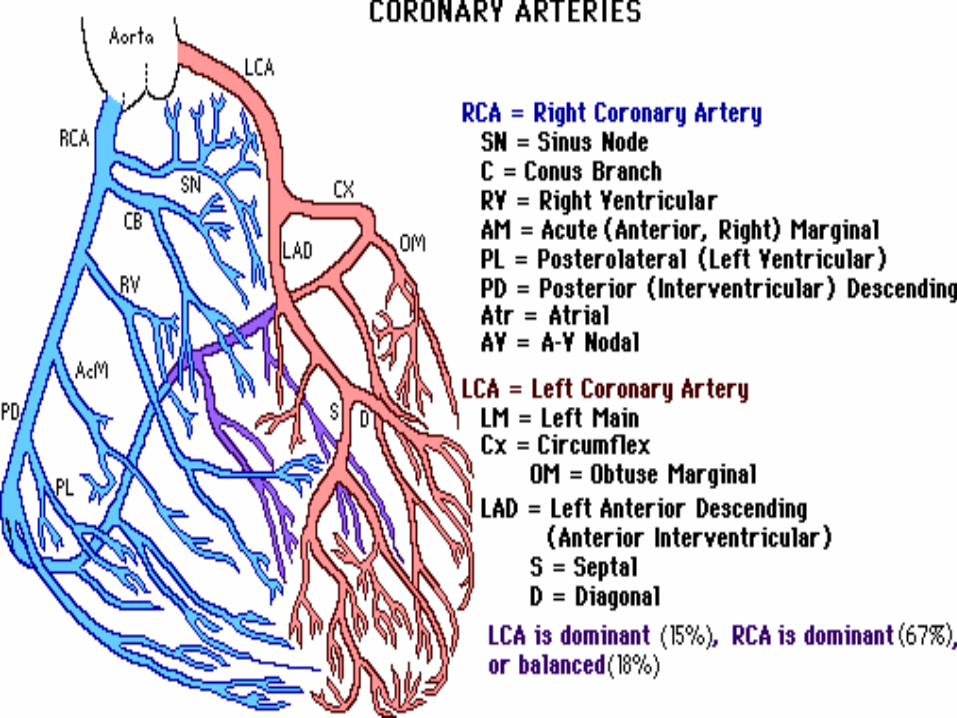
Coronary Arteries: 2 Main • Rt. Coronary Artery- branches into marginal arteries; supplies
RV and posterior of heart.• Lt. Coronary Artery- branches into Lt. Anterior Descending and
circumflex artery; supplies LV.
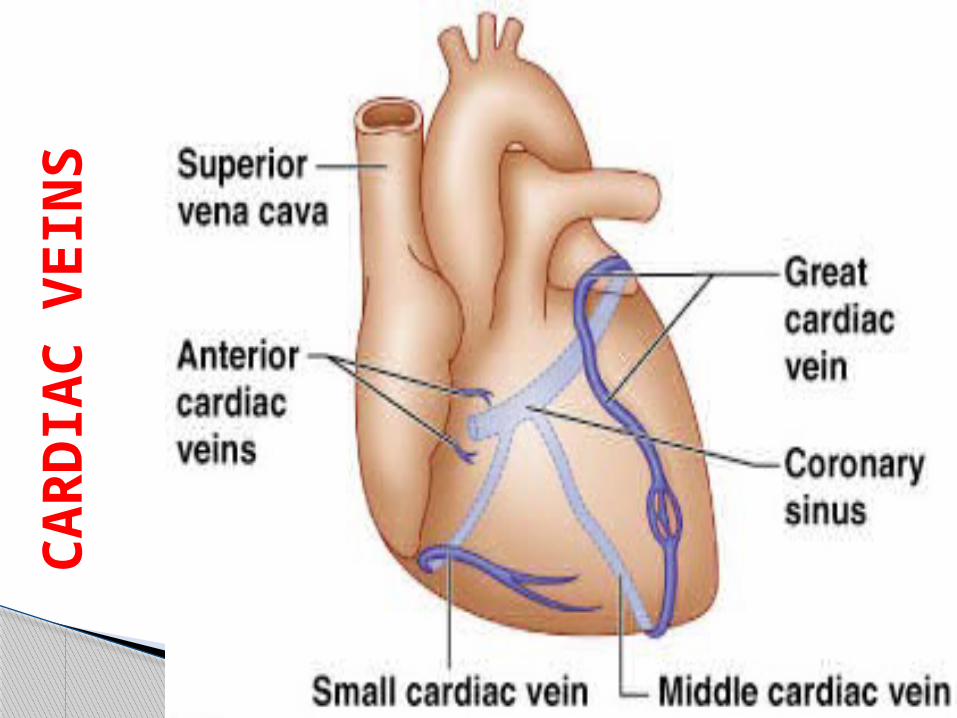
Coronary Veins• Small cardiac & Great cardiac veins, Anterior cardiac, Posterior
cardiac & Middle cardiac veins• Transport deoxygenated blood to coronary sinus• Coronary Sinus drains into RA.
Vessels that Supply/Drain the Heart
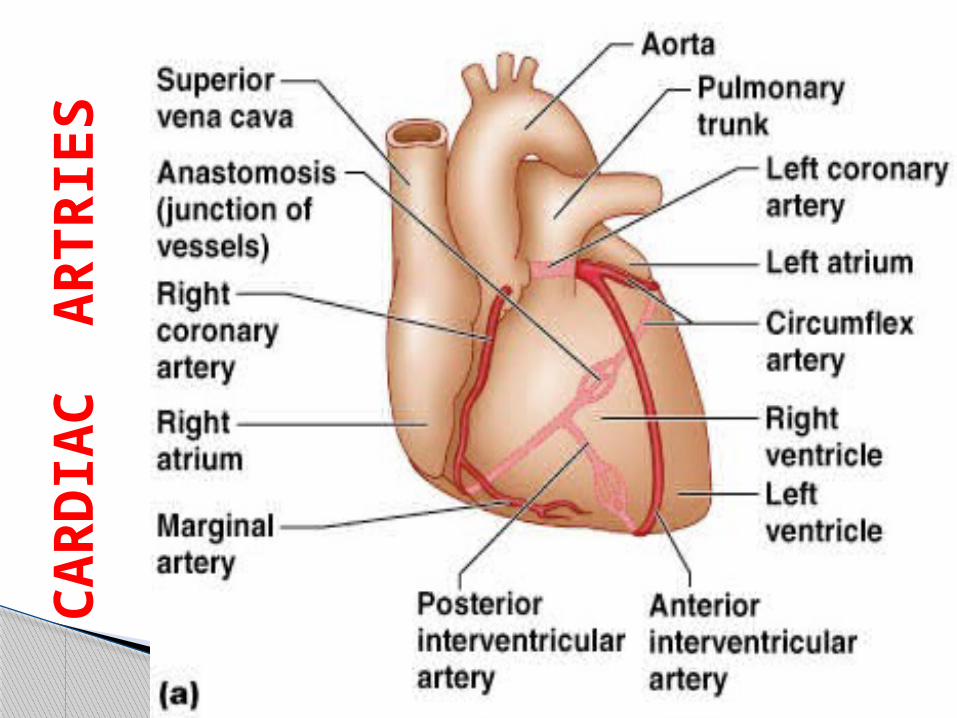
CA
RD
IAC
A
RTR
IES
CA
RD
IAC
VEIN
S

The fibrous pericardium and the parietal layer of serous pericardium are innervated by Visceral sensory fibers (the branches of Phrenic nerve). These fibers carries the sensation of pain.
Parasympathetic fibers (branch of the Vagus nerve) that are responsible for slowing down of the heart rate, innervate the visceral layer of serous pericardium.
Sympathetic fibers that increase the rate and force of contraction
NERVE SUPPLY TO THE HEART
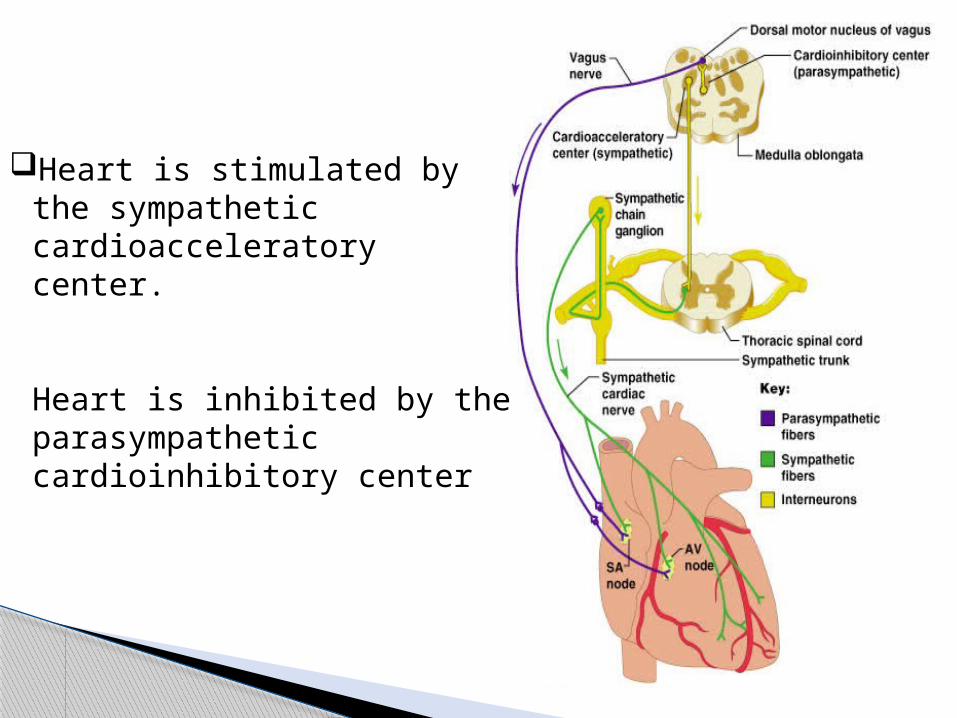
Heart is stimulated by the sympathetic cardioacceleratory center.
Heart is inhibited by the parasympathetic cardioinhibitory center
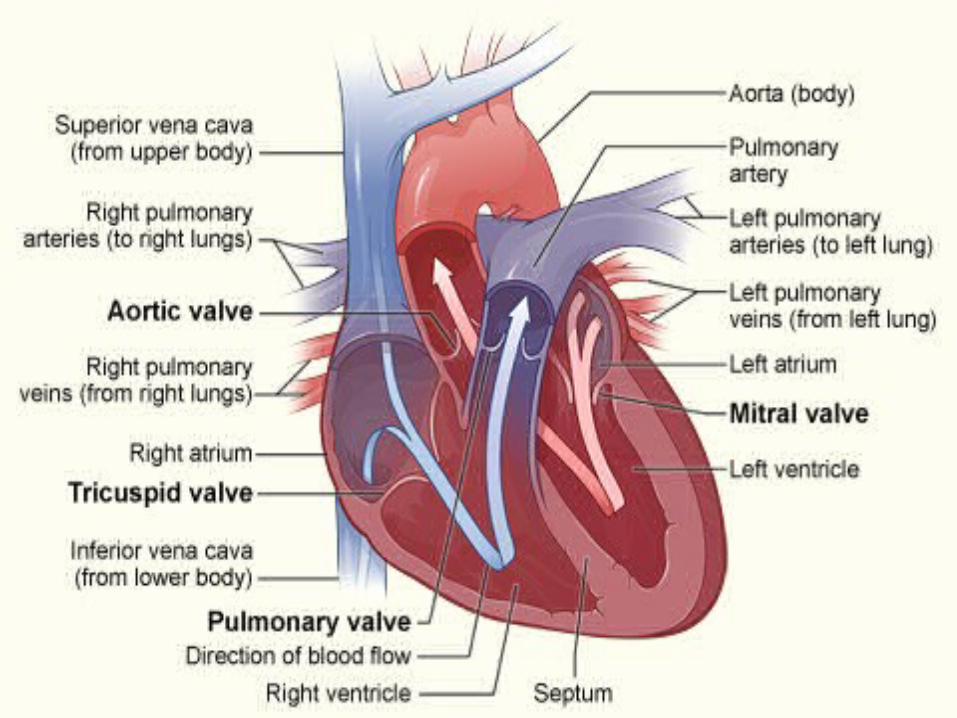
The Heart valves ensure unidirectional blood flow through the heart
Responds to changes in pressure
Two types of valves are present in heart:1. Atrio-ventricular valves (AV)2. Semi-lunar valves
HEART VALVES
1. Atrio-ventricular (AV) valves lie between the atria and the ventricles & prevents backflow into the atria when ventricles contract. Heart contains 2 Atrio-ventricular valves:
• Left AV valve i.e. Mitral valve is bicuspid• Right AV valve i.e. Tricuspid
{Chordae tendineae are tiny collagen cords that anchor cusps of valve to papillary muscles}
2. Semilunar valves lies b/w the great vessels and ventricles and prevent backflow of blood into the ventricles. Heart contains 2 semilunar valves:
• Aortic valve lies between the left ventricle and the aorta
• Pulmonary valve lies between the right ventricle and pulmonary trunk
The Heart contains 2 septum:• Interatrial septum: Muscular division between Rt. & Lt. atria.
Where the Fossa ovalis also presents i.e. a shallow depression; remnants of foramen ovale (opening in fetus)
• Interventricular septum :Thick muscular wall that seperates Rt. & Lt. ventricles.
SEPTUMS OF HEART
Right Atrium: Thinner walls. Receives deoxygenated blood from vena cava. Passes blood through tricuspid valve into right ventricle
Right Ventricle: Thicker wall than atria. Makes most of the anterior surface of heart. Circulates deoxygenated blood to lungs through the pulmonary valve into pulmonary trunk.
PATHWAY OF BLOOD THROUGH HEART
Left Atrium: Receives oxygenated blood from pulmonary vein. Passes blood to left ventricle through mitral valve
Left Ventricle: Thickest myocardial wall. Forms apex of heart. Receives blood from left atrium & sends it to systemic circulation via aorta

The heart is composed of three major types of cardiac muscle:
• Atrial muscle, • Ventricular muscle and • Specialized excitatory & Conductive muscle fibers.
CARDIAC MUSCLES
1. Atrial and ventricular muscle fibers: contracts for longer duration (like skeletal muscle).
2. Specialized excitatory & conductive fibers: contracts very weakly because of few contractile fibrils. Function:
• Generates the automatic electrical discharge in the form of action potentials and
• Conduction of the action potentials through Heart that causes rhythmic beating.

MICROSCOPIC ANATOMY OF HEART MUSCLES
Cardiac muscle is striated, arranged in latticework, branched, and interconnected.
They contain Actin and Myosin filaments that slides over one another during contraction.
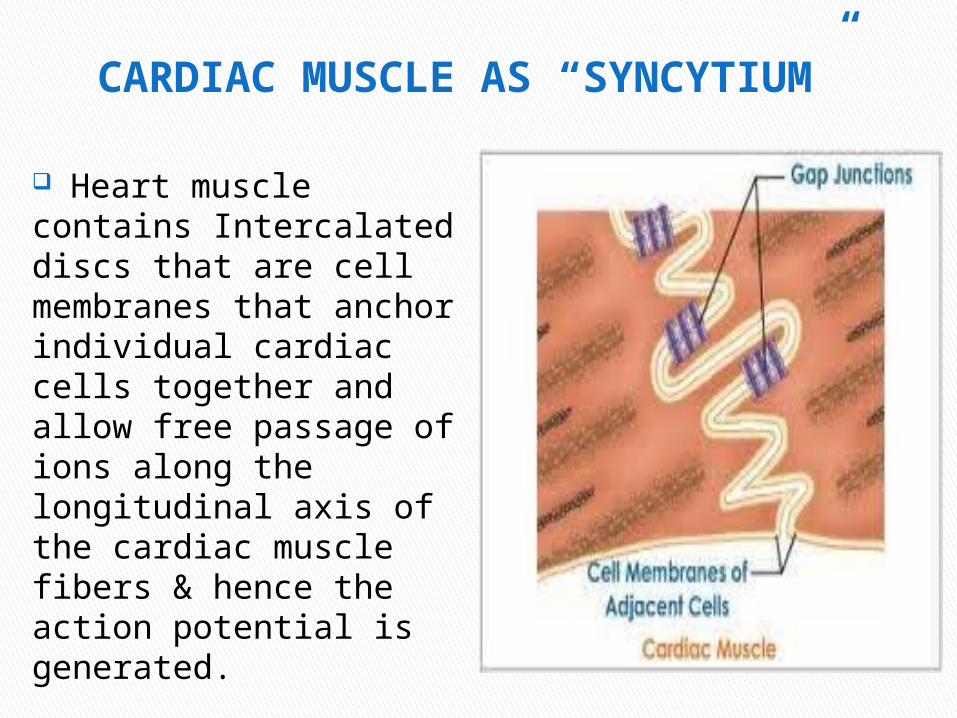
CARDIAC MUSCLE AS “SYNCYTIUM”
Heart muscle contains Intercalated discs that are cell membranes that anchor individual cardiac cells together and allow free passage of ions along the longitudinal axis of the cardiac muscle fibers & hence the action potential is generated.
Thus, cardiac muscle behaves as a functional Syncytium of many heart muscle cells in which the cardiac cells are interconnected & when one cells get excited, the action potential spreads to all of them through the latticework interconnections.
Two Syncytiums are present: • Atrial syncytium: that constitutes the walls of the two atria, and • Ventricular syncytium: that constitutes the walls of the two
ventricles.
This division of heart muscle into two functional Syncytiums allows the atria to contract for shorter duration & before ventricular contraction, which is important for heart pumping.
AUTOMACITY: Capability of stimulated by nerves as well as self-excitable
RHYTHMICITY: Heart beats are extremely regular
CONTRACTIBILITY: Cardiac muscle contracts in response to stimulus
EXCITABILITY: Ability of cardiac muscles to respond to different stimuli
PROPERTIES OF CARDIAC MUSCLE

CONDUCTIVITY: Impulses produced in the SA nodes are conducted by specialized conducting pathway
DISTENSIBILITY: Occurs due to compliance of cardiac muscle
FUNCTIONAL SYNCYTIUM: allows the atria to contract for shorter duration & before ventricular contraction
In cardiac muscle, the action potential is caused by opening of two types of channels:
(1) the fast sodium channels and (2) the slow calcium channels (also k/a calcium-sodium channels)
Calcium channels are slower to open and remain open for several tenths of a second. During this time, a large quantity of both calcium and sodium ions flows through the cardiac muscle fiber and maintains a prolonged period of depolarization, causing the plateau in the action potential.
ACTION POTENTIAL IN CARDIAC MUSCLE
The calcium ions that enter during this plateau phase activates the muscle contractile process.
After the onset of the action potential, the permeability of potassium ions decreases about fivefold due to excess calcium influx
The decreased potassium permeability decreases the out flux of positively charged potassium ions during the action potential plateau and thereby prevents early return of the action potential voltage to its resting level.

When the slow calcium-sodium channels closes at the end of 0.2 to 0.3 second and the influx of calcium and sodium ions stops, the membrane permeability for potassium ions increases rapidly; this rapid loss of potassium from the fiber immediately returns the membrane potential to its resting level, thus ending the action potential.
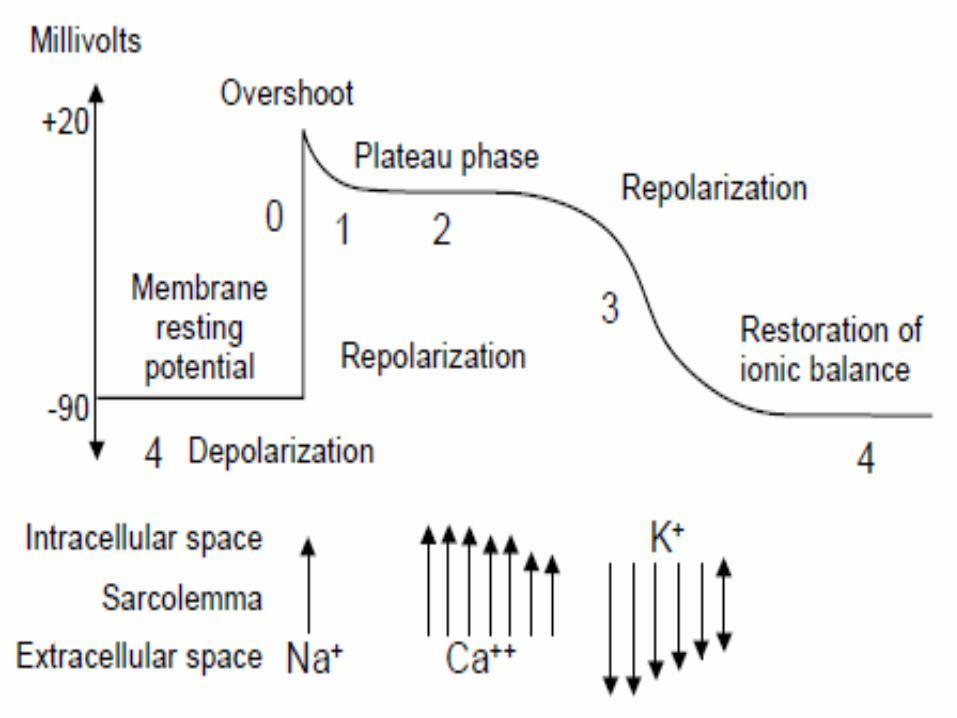
In ventricular muscle fiber, during each beat the intracellular potential rises from -85 millivolts towards a positive value of about +20 millivolts to averages about 105 millivolts. This causes initial spike.
Plateau causes ventricular contraction to last for longer duration.
After which the membrane remains depolarized for about 0.2 second leading to a plateau followed by an abrupt repolarization at the end.
WHAT HAPPENS DURING EXCHANGE OF IONS???
REFRACTORY PERIOD OF CARDIAC MUSCLE
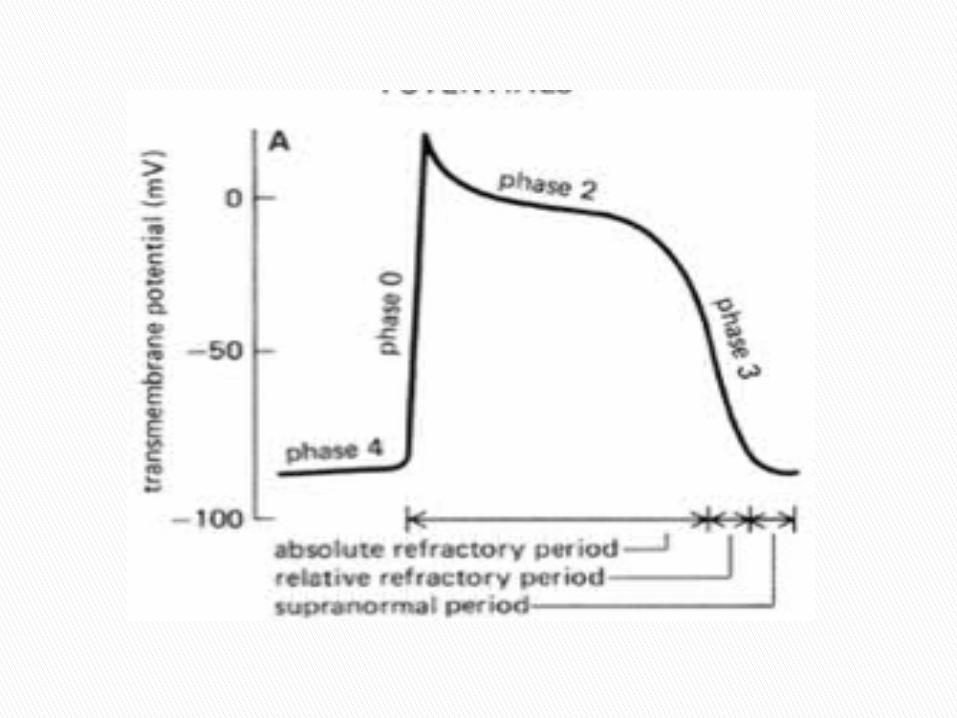
Refractory period is the time period during which a normal cardiac impulse cannot re-excite an already excited area of cardiac muscle. The normal refractory period of the ventricle is 0.25 to 0.30 sec (=plateau period in action potential.)
There is an additional relative refractory period of about 0.05 sec during which the muscle is more difficult than normal to excite but nevertheless can be excited by a very strong excitatory signal.
Sinoatrial (SA) node generates impulses of about 75 times/minute
Atrioventricular (AV) node delays the impulse approximately 0.1 second
Impulse passes from atria to ventricles via AV bundle(bundle of His)
AV bundle splits into two pathways i.e. Rt. & Lt. bundle branch in the interventricular septum & carries the impulse toward the apex of the heart.
Purkinje fibers carry the impulse to the heart apex and ventricular walls.
SEQUENCE OF EXCITATION

SEQUENCE OF EXCITATION
Due to this special arrangement of the conducting system, there is a delay of >0.1sec during passage of the cardiac impulse from the atria to the ventricles. This allows atria to contract before ventricular contraction begins. Thus, the atria act as Primer Pumps for the Ventricles, & the ventricles in turn provide the major source of power for moving blood to the body’s vascular system.
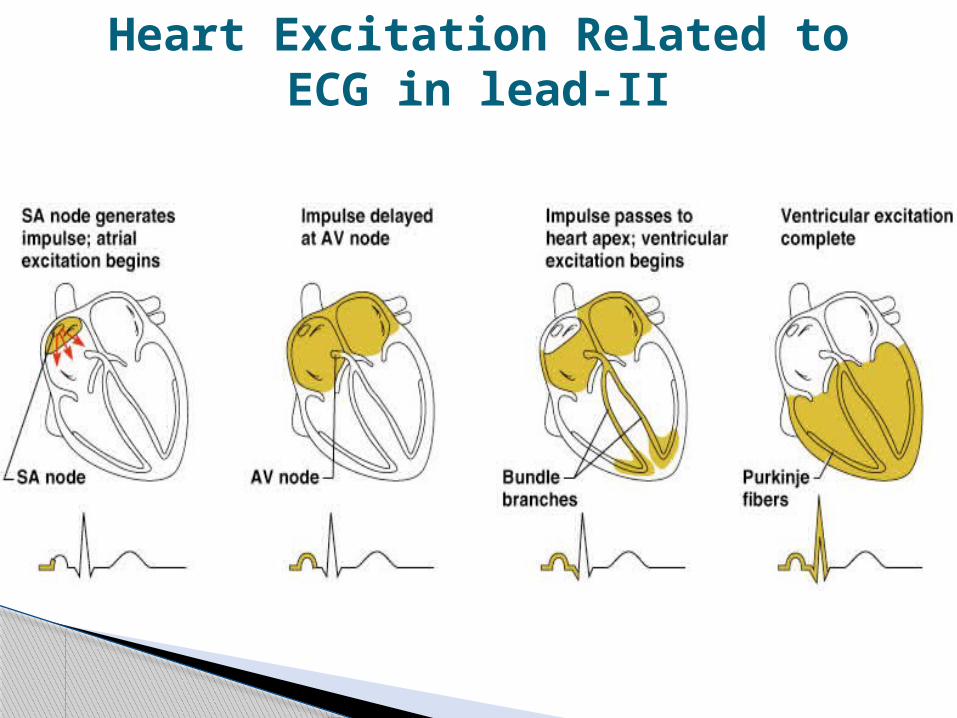
Heart Excitation Related to ECG in lead-II

The velocity of conduction of the excitatory action potential signal along both atrial and ventricular muscle fibers is about 0.3 to 0.5 m/sec.
The velocity of conduction in the Purkinje fibers is 4 m/sec, which allows reasonably rapid conduction of the excitatory signal to the different parts of the heart
Velocity of Signal Conduction in Cardiac Muscle
The impulse, after traveling through the internodal pathways, reaches the A-V node about 0.03 second after its origin in the sinus node. Then there is a delay of another 0.09 second in the A-V node itself before the impulse enters the penetrating portion of the A-V bundle, where it passes into the ventricles. A final delay of another 0.04 second occurs mainly in this penetrating A-V bundle, which is composed of multiple small fascicles passing through the fibrous tissue separating the atria from the ventricles.
Thus, the total delay in the A-V nodal and A-V bundle system is about 0.13 second. This, in addition to the initial conduction delay of 0.03 second from the sinus node to the A-V node, makes a total delay of 0.16 second before the excitatory signal finally reaches the contracting muscle of the ventricles.
Atrioventricular Node, and Delayof Impulse Conduction from the Atria
to the Ventricles
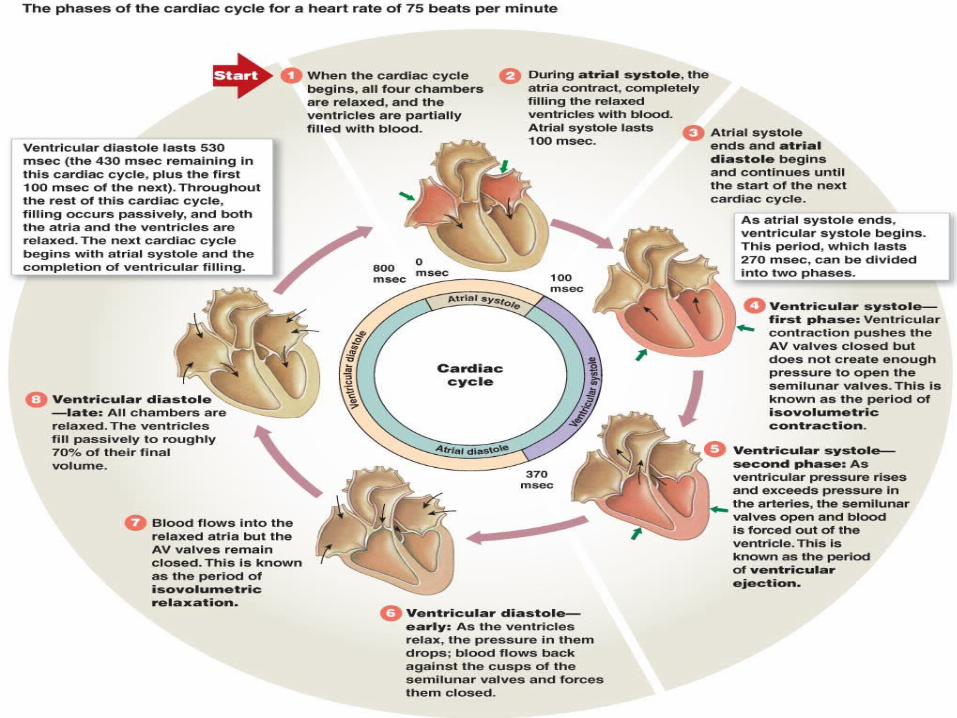
The cardiac events that occur from the beginning of one heartbeat to the beginning of the next are called the cardiac cycle.
Each cycle is initiated by spontaneous generation of an action potential in the sinus node
The cardiac cycle consists of:• Diastole- period of relaxation during which the heart fills with
blood • Systole- period of contraction
CARDIAC CYCLE

Normally about 80% of the blood directly flows through the atria into the ventricles even before the atria contract.
Then, atria contracts causing an additional 20% filling of the ventricles. Therefore, atria function as primer pumps that increase the ventricular pumping effectiveness by 20%.
Without this extra 20%the heart can work effectively because ventricles has the capability of pumping 300 to 400% of more blood than is required by the resting body.
Therefore, when the atria fail to function, there is less/no symptoms until unless a person exercises; then shortness of breath develops.
ATRIA AS A PRIMER PUMP
The a wave: Occurs due to atrial contraction. When:• The right atrial pressure increases 4 to 6 mm Hg and • the left atrial pressure increases about 7 to 8mmHg.
The c wave: when ventricles begin to contract; it is caused partly by backflow of blood into the atria but mainly by bulging of the A-V valves backward because of increasing pressure in the ventricles.
Pressure Changes in the Atria—The a, c, and v Waves
The v wave: end of ventricular contraction; it results from slow blood flow into the atria from the veins when the A-V valves are closed during ventricular contraction.
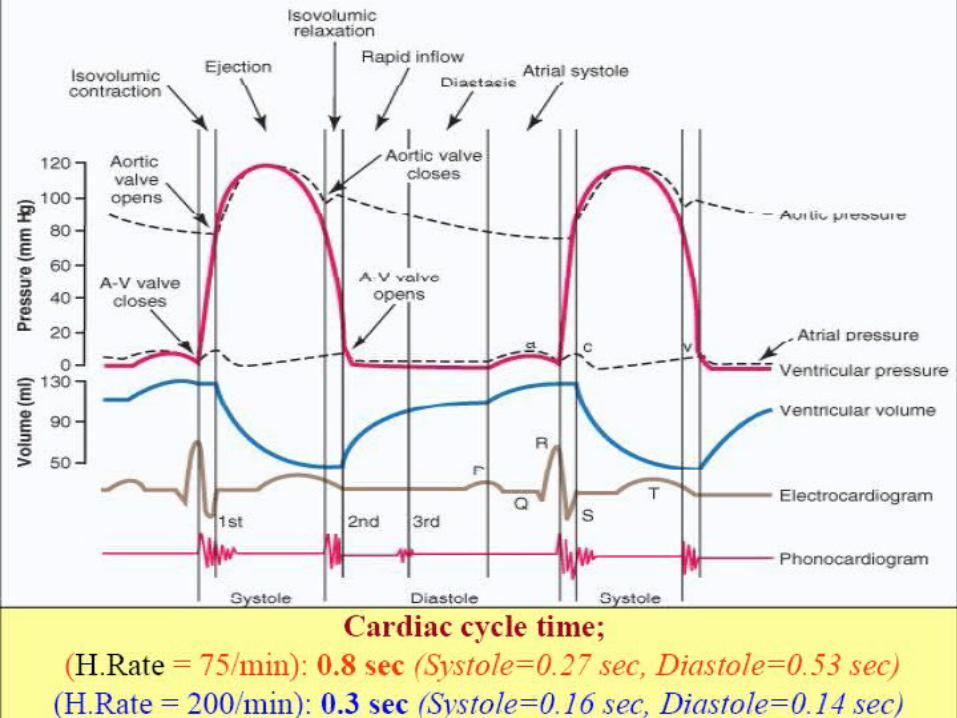

During diastole, normal filling of the ventricles increases the volume of each ventricle to about 110 to 120 milliliters. This volume is called the end-diastolic volume.
Then, as the ventricles empty during systole, the volume decreases about 70 milliliters, which is called the stroke volume output.
END-DIASTOLIC VOLUME, STROKE VOLUME OUTPUT AND END-SYSTOLIC
VOLUME.
The remaining volume in each ventricle, about 40 to 50 milliliters, is called the end-systolic volume.
The fraction of the end-diastolic volume that is ejected is called the ejection fraction— usually equal to about 60 per cent.
When the heart contracts strongly, the end-systolic volume can be decreased to as little as 10 to 20 milliliters.
Conversely, when large amounts of blood flow into the ventricles during diastole, the ventricular end diastolic volumes can become as great as 150 to 180 milliliters in the healthy heart.
By both increasing the end-diastolic volume and decreasing the end-systolic volume, the stroke volume output can be increased to more than double normal.
Atrioventricular Valves (tricuspid and mitral valves) prevent backflow of blood from the ventricles to the atria during systole, and
Semilunar valves (aortic and pulmonary valves) prevent backflow from the aorta and pulmonary arteries into the ventricles during diastole.
Valves get closed when a backward pressure gradient pushes blood backward, and they open when a forward pressure gradient forces blood in the forward direction.
For anatomical reasons, the thin, filmy A-V valves require almost no backflow to cause closure, whereas the much heavier semilunar valves require rather rapid backflow for a few milliseconds.
FUNCTIONS OF VALVES

The semilunar valves function differently from the A-V valves in two manner:
1. The high pressures in the arteries at the end of systole cause the semilunar valves to snap to the closed position, as compared to the much softer closure of the A-V valves.
2. Due to smaller openings, the velocity of blood ejection through the aortic and pulmonary valves is far greater than that through the much larger A-V valves.
Also, because of the rapid closure and rapid ejection, the edges of the aortic and pulmonary valves are subjected to much greater mechanical abrasion than are the A-V valves. Finally, the A-V valves are supported by the chordae tendineae, which is not true for the semilunar valves.
The papillary muscles contract when the ventricular walls contract but they do not help the valves to close
They pull the valves inward toward the ventricles to prevent their bulging too far backward toward the atria during ventricular contraction.
If a chorda tendinea becomes ruptured or if one of the papillary muscles becomes paralyzed, the valve bulges far backward during ventricular contraction, causing severe leakage which may result in lethal cardiac incapacity.
FUNCTION OF PAPILLARY MUSCLES
When the valves close, the vanes of the valves and the surrounding fluids vibrate under the influence of sudden pressure changes, giving off sound that travels in all directions through the chest.
When the ventricles contract, one first hears a sound caused by closure of the A-V valves. The vibration is low in pitch and relatively long-lasting and is known as the first heart sound.
When the aortic and pulmonary valves close, a rapid snap can be heard because these valves close rapidly, and the surroundings vibrate for a short period. This sound is called the second heart sound.
HEART SOUND DURING PUMPING

Phase I: Period of filling- It begins at a ventricular volume of about 45 milliliters(end-systolic volume) and a diastolic pressure near 0 mm Hg.
As venous blood flows into the ventricle from the left atrium, the end-diastolic volume of lt. ventricle becomes115milliliters. Therefore, the volume-pressure diagram during phase I extends along the line labeled “I,” with the volume increasing to 115 milliliters and the diastolic pressure rising to about 5 mm Hg.
VOLUME PRESSURE DIAGRAM

Phase II: Period of isovolumic contraction- During this phase, the volume of the ventricle does not change because all valves are closed but the pressure inside the ventricle increases to equal the pressure in the aorta (80 mm Hg).
Phase III: Period of ejection- During ejection, the systolic pressure rises and volume of ventricles decreases. The aortic valve has now opened and blood flows out of the ventricle into the aorta.
Phase IV: Period of isovolumic relaxation- At the end of the period of ejection, the aortic valve closes, and the ventricular pressure falls back. The line labeled “IV” traces this decrease in intraventricular pressure without any change in volume. Thus, the ventricle returns to its starting point, with about 45 milliliters of blood left in the ventricle and at an atrial pressure near 0 mmHg.
Preload is usually considered to be the end-diastolic pressure when the ventricle has become filled.
Afterload of the ventricle is the pressure in the artery leading from the ventricle. This corresponds to the systolic pressure described by the phase III curve of the volume-pressure diagram
PRELOAD & AFTERLOAD
Heart muscles uses chemical energy that is derived from oxidative metabolism of fatty acids and other nutrients like lactate & glucose
This chemical energy is converted in heat & work output.
The ratio of work output and chemical energy expenditure is known as efficiency of cardiac contraction. Maximum efficiency of the normal heart is between 20 and 25%. In heart failure, this can decrease to as low as 5 to 10 per cent.
Chemical Energy Required for Cardiac Contraction: Oxygen Utilization by the Heart
When a person is at rest, the heart pumps only 4 to 6 liters of blood each minute. During severe exercise, the heart may be required to pump four to seven times this amount.
The basic means by which the volume pumped by the heart is regulated are
(1) Change in volume by Intrinsic cardiac regulators and (2) control of heart rate and strength of heart pumping by the
autonomic nervous system.
Regulation of Heart Pumping

The amount of blood pumped by the heart each minute is determined venous return. The heart, in turn, automatically pumps this incoming blood into the arteries, so that it can flow around the circuit again.
This intrinsic ability of the heart to adapt to increasing volumes of inflowing blood is called the Frank- Starling mechanism of the heart.
The Frank-Starling mechanism means that the greater the heart muscle is stretched during filling, the greater is the force of contraction and the greater the quantity of blood pumped into the aorta
Intrinsic Regulation of Heart Pumping—The Frank-Starling Mechanism
The pumping effectiveness of the heart also is controlled by the sympathetic and parasympathetic nerves, which abundantly supply the heart.
The amount of blood pumped each minute (cardiac output) can be increased more than 100% by sympathetic stimulation.
AND The output can be decreased to as low as zero or almost zero
by parasympathetic stimulation (vagal).
Control of the Heart by the Autonomic nervous system (Sympathetic and Parasympathetic Nerves)
Effect of Potassium Ions Excess potassium in the extracellular fluids causes the heart to
become dilated and flaccid and also slows the heart rate.
Elevation of potassium concentration to only 8 to 12 mEq/L (two to three times the normal value) can cause weakness of the heart and abnormal rhythm that this can cause death.
This is because high potassium concentration in the extracellular fluids decreases the resting membrane potential which causes the intensity of the action potential to decreases, which further makes contraction of the heart progressively weaker.
EFECT OF POTASSIUM AND CALCIUM IONS ON HEART FUNCTION
Effect of Calcium Ions An excess of calcium ions causes effects almost exactly
opposite to those of potassium ions, causing the heart to go toward spastic contraction. This is caused by a direct effect of calcium ions to initiate the cardiac contractile process,
Conversely, deficiency of calcium ions causes cardiac flaccidity, similar to the effect of high potassium.
Fortunately, calcium ion levels in the blood normally are regulated within a very narrow range. Therefore, cardiac effects of abnormal calcium concentrations are seldom of clinical concern.
Increased body temperature, as occurs when one has fever, causes a greatly increased heart rate, sometimes to as fast as double normal.
Decreased temperature causes a greatly decreased heart rate, falling to as low as a few beats per minute
This is because heat increases the permeability of the cardiac muscle membrane to ions that control heart rate, resulting in acceleration of the self-excitation process.
If there is prolonged elevation of temperature, it exhausts the metabolic systems of the heart and eventually causes weakness.
Effect of Temperature onHeart Function



















