Cardiac Risk Factor Management in the Older South Asian Female Dr. Aashish Contractor Head of Dept: Preventive Cardiology and Rehabilitation Asian Heart Institute, Mumbai, India e-mail: [email protected]
Transcript
Cardiac Risk Factor Management in
the Older South Asian Female
Dr. Aashish Contractor
Head of Dept: Preventive Cardiology and Rehabilitation
• Factors affecting risk factor reduction in S. Asians
• Conclusions
Leading Causes of Death in India
Year 2000 2010
Total death
(in millions)
9.4 10.2
CVD
(only IHD)
3
1.6
3.75
2
Infectious
Diseases
2.4 2.2
Burden of CHD in the U.K.
• Coronary heart disease (CHD) remains the leading cause of death in the United Kingdom (UK) accounting for around 300,000 deaths per year.
• South Asians have a 40–50% greater mortality from CHD compared to the indigenous white European population
Coronary heart disease statistics 2004: British Heart Foundation Statistics: website www.heartstats.org
Why do South Asians have premature CHD mortality?
• Several hypotheses, which include:
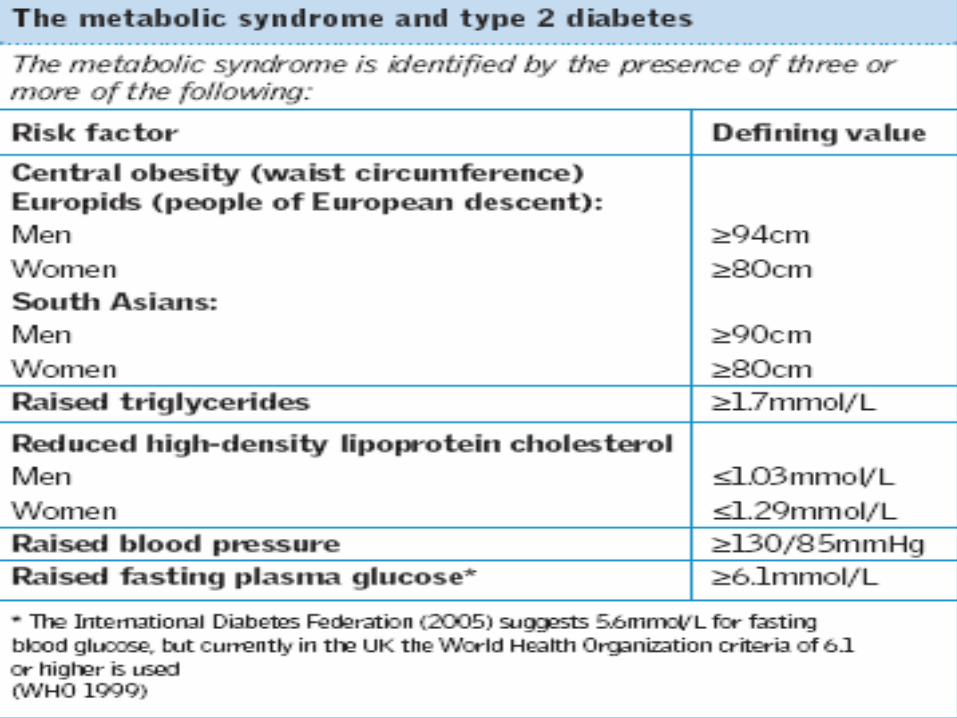
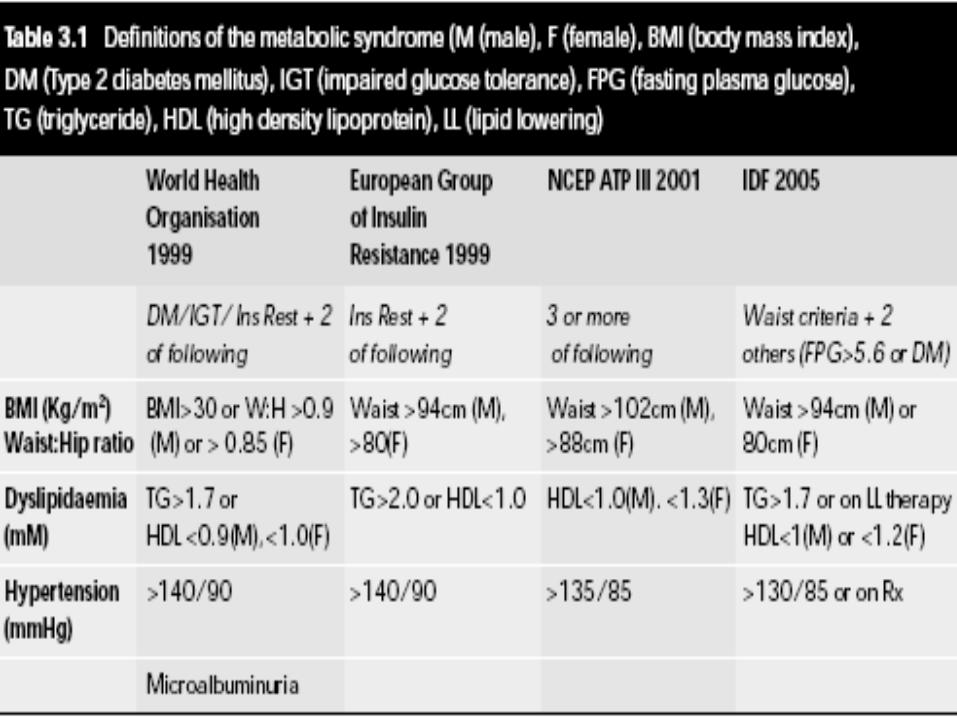
• Higher prevalence of the metabolic syndrome and diabetes mellitus
• Pro-atherogenic diet
• Lack of physical activity
• High levels of homocysteine and Lp(a)
Presentation of CHD
• South Asians, especially women are more likely to present with ‘atypical’ symptoms and more likely to be diagnosed as ‘non-cardiac’
Barakat K,Wells Z, Ramdhany S,Mills P,Timmis A. Bangladeshi patients present with non-classic features of acute myocardial infarction and are treated less aggressively in east London, UK.Heart 2003; 89: 276–9.
Estimation of CHD risk
• CHD risk estimation tool validated in this ethnic group is currently non-existent.
• The available scales such as the Framingham, FINRISK and the SCORE systems (derived from cohort studies of American and European white populations) have been shown to underestimate CHD risk in South Asians
• Bhopal R, Fischbacher C,Vartiainen E,Unwin N,White M, Alberti G. Predicted and observed cardiovascular disease in South Asians: application of FINRISK, Framingham and SCORE models to Newcastle Heart Project data. Journal of Public Health. 2005;27: 93–100.
Outline
• Reasons for higher CHD prevalence in S. Asians
• Significance of CHD risk factors in S. Asians
• Factors affecting risk factor reduction in S. Asians
• Conclusions
Age
• The INTERHEART study revealed that the median age for presentation with a cardiac event was 50 years for men of South Asian origin vs 59 years for European men
• The median age for South Asian women was 60 vs 68 for European women
• Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study Lancet 2004; 364: 937–52
Diabetes
• Diabetes is 3-5 times more common in people of South Asian origin living in the UK
• Mortality rates in South Asians with diabetes are two fold higher compared to Europeans with diabetes
• Cappuccio FP,Cook DG,Atkinson RW, Strazzullo P. Prevalence, detection and management of cardiovascular risk factors in different ethnic groups in South London. Heart 1997; 78: 555–63.
Diabetes
• Premature death, especially in South Asian females, is reportedly linked with the earlier onset of diabetes
Sverdlow AJ, Laing SP, Dos Santos Silva I et al. Mortality of South Asian patients with insulin-treated diabetes mellitus in the United Kingdom: a cohort study. Diabetic Medicine 2004; 21 (8): 845-51
Diabetes
• Figures suggest that 20 per cent of the South Asian community living in the UK have Type 2 diabetes in contrast to three per cent of the general population.
• Diabetes and the disadvantaged: reducing health inequalities in the UK World Diabetes Day 14 November 2006. A report by the All Parliamentary Group for Diabetes and Diabetes UK
Attitudes towards diabetes
• South Asians with diabetes in the U.K. have been shown to have accepted their diagnosis with resignation and expressed the view that the condition had been “sent by God” .
• Most people have family members and friends with the disease, and accept it as inevitable, and are therefore less motivated to attempt to control it.
• Stone M et al. Empowering patients with diabetes: a qualitative primary care study focusing on South Asians in Leicester, UK. Family Practice 2005;22:647-52
Hypertension
• The prevalence of hypertension appears to be significantly higher in some studies of South Asian immigrants in the UK compared to Europeans
• This contrasts with some reports both in the UK and in the South Asian groups living in Tanzania
• (Cappuccio FP,Cook DG,Atkinson RW, Strazzullo P. Prevalence, detection and management of cardiovascular risk factors in different ethnic groups in South London. Heart 1997; 78: 555–63.)
• (Agyemang C,.Bhopal RS. Is the blood pressure of South Asian adults in the UK higher or lower than that in European white adults? A review of cross-sectional data. J Hum Hypert 2002; 16: 739–51.)
Hypertension
• Further, the risk of hypertension going undetected is highest among South Asians (odds ratio 2.34, 95% CI) when compared with Caucasians and people of African descent living in the UK
• Cappuccio F, Oakeshott P, Strazzullo P, Kerry S. Application of Framingham risk estimated in ethnic minorities in United Kingdom ad implications for primary prevention of heart disease in general practice: cross-sectional population based study. BMJ 2002; 325:1271
Hypertension: beliefs
• To address the cardiovascular disparities in South Asians in the U.S., an understanding of the community’s health care seeking patterns need to be considered.
• A series of 8 focus groups with South Asian community members in the New York Metropolitan Area were conducted to evaluate their hypertension beliefs, knowledge, and screening and treatment practices, and their experiences in accessing the health care system
Hypertension: beliefs• While some participants did acknowledge that people in
home countries may also have hypertension/stress, others associated high blood pressure to moving to the US
• Additionally, stress/fear felt specifically by Muslim community in the United States as a result of 9/11 (and the "war on terror"), in the community were cited as causes for disease, heart attacks.
• Also, for some participants, loneliness, isolation, etc. contributes to stress and disease. They identified stress being a result of not being able to speak about personal, family issues, especially immigration.
Smoking
• Smoking rates are generally significantly lower in South Asian females than in Whites
Prevalence of Tobacco Smoked by American Adults age 20 and above by Race/Ethnicity and Sex
White Black Mexican Asian/Pac. S. Asian
Male 25.8% 26.1% 24.1% 24.3% 26.8%
Female 21.6% 20.8% 12.3% 7.1% 1.8%
Percentage of South Asians Chewing Tobacco (info.cancerresearchuk.org/.../oral/riskfactors/ )
Cholesterol
• High triglycerides and low HDL are the most common dyslipidemias seen in this population
• It is interesting to note that although total plasma cholesterol may actually be lower in UK South Asians than white Europeans, it is still significantly higher than that seen in South Asians in India.
• South Asian women are much more likely to have low levels of protective HDL cholesterol
Classification BMI(kg/m²)
Principal cut-off points Additional cut-off points
Underweight <18.50 <18.50
Severe thinness <16.00 <16.00
Moderate thinness 16.00 - 16.99 16.00 - 16.99
Mild thinness 17.00 - 18.49 17.00 - 18.49
Normal range 18.50 - 24.9918.50 - 22.99
23.00 - 24.99
Overweight ≥25.00 ≥25.00
Pre-obese 25.00 - 29.9925.00 - 27.49
27.50 - 29.99
Obese ≥30.00 ≥30.00
Obese class I 30.00 - 34-9930.00 - 32.49
32.50 - 34.99
Obese class II 35.00 - 39.9935.00 - 37.49
37.50 - 39.99
Obese class III ≥40.00 ≥40.00
Source: Adapted from WHO, 1995, WHO, 2000 and WHO 2004.
Lancet 2004; 363: 157–63
Threshold for BMI cut-offs
• Conventional cut points were derived primarily in European populations to correspond to risk thresholds for a wide range of chronic diseases and mortality.
• Emerging evidence suggests that South Asians (people who originate from the Indian subcontinent) and Chinese suffer from an elevated risk of type 2 diabetes, hypertension, and dyslipidemia even if their BMI is low (ie, 25.0 kg/m2).
• Possible explanations include that non-Europeans have a relative excess of adipose tissue or deficit of lean body mass compared with Europeans for a given BMI.
• The study demonstrated that South Asians, Chinese, and Aboriginal people have similar distributions of glucose and lipid factors at significantly lower BMI values compared with Europeans
Circulation. 2007;115:2111-2118.)
Outline
• Reasons for higher CHD prevalence in S. Asians
• Significance of CHD risk factors in S. Asians
• Factors affecting risk factor reduction in S. Asians
• Conclusions
Challenges in risk factor reduction
• Barriers in communication
• Cultural issues
• Dietary practices
• Low levels of physical activity
• Its important to bear in mind, that South Asian women do not share a homogeneous culture or identity
Barriers in communication
• Inability to speak or read English
• This impairs comprehension of education
• The availability of multilingual literature would be very helpful
Cultural issues
• Fatalistic approach to health and illness
• Often believe that illness is ‘God’s will’ or that ‘what is written in my destiny no one can change’ (Karma)
• Such an approach often results in patients being less proactive in the recovery process
Cultural issues
• In addition to Western medicine, traditional healers and healing practices are valued by South Asian women
• Often patients are not told about their diagnosis, for fear of ‘frightening’ them
Diet-composition
• Fat intake is higher in South Asians. Clarified butter, known as ‘ghee’ is used frequently in cooking, and is very high in saturated fat
• They tend to have a low level of fish consumption (other than Bangladeshis)
• Indian snacks tend to be usually deep-fried
• Diet tends to high in full fat milk (buffalo milk)
Diet- cultural issues
• Diet: The cultural significance of food for South Asians is enormous. People are offered fatty, sweet food at social gatherings, religious festivals, weddings and celebrations. To refuse the food would mean social isolation, and South Asian patients in the U.K. with diabetes have been reported as being reluctant to do so
• Hill J. Management of diabetes in South Asian communities in the UK. Nursing Standard 2006; 20(25): 57-64.
Diet- excess sugar consumption
• In the U.K., one in three Asian Indian diabetics have been reported as consuming Asian sweets, high in sugar content, at least once a week. Approximately 80% consumed tea with high sugar content, and 75% ate snacks cooked in fats/oils daily
• Samantha A, Campbell JE, Spalding DL, Panja KK, Neogi SK, Burden AC. Eating habits in Asian diabetics. Diabet Med 2002; 3(3):283-4
Diet- fasting
• Related to the dietary practices are fasts and feasts. Muslim patients who observe Ramadan face additional challenges to maintain a steady blood glucose level during this month.
• In Hindus, there are several periods of fasting throughout the year from one to nine days. These fasts are usually preceded and followed by feasts, and present a challenge for self-care in the South Asian diabetic.
Results
• Indian, Pakistani and Bangladeshi men were 14, 30, and 45% less likely than the general population to meet current guidelines for physical activity
• Levels of physical activity were lower in all South Asian groups than the general population
Results
• The Health Survey for England reported that only 1 % of Bangladeshi women, and 2 % of Indian women above 55 years, reported a high level of physical activity
• The corresponding figure in the general population was 11 %
• Very unlikely to take part in any type of sporting activity
Attitude of healthcare professionals
• Any tendency of health promotion strategies to overemphasize barriers of cultural difference, which may promote defeatist attitudes among professionals, needs to be avoided
Barriers to exercise
• Low awareness and uncertainty
• Low priority
• Over protective attitude of family
• Worried about activity being harmful
• Mixed sex exercise facilities
Low priority
• Low priority to physical activity as a leisure activity to be pursued in limited spare time when set against family and other obligations
• They felt they were being active from care-giving, housekeeping and workday activities
• Attending the gym may be difficult for South Asian women unless single-sex facilities are available, as certain religions require that the women keep their bodies covered.
• Hill J. Management of diabetes in South Asian communities in the UK. Nursing Standard 2006; 20(25): 57-64.
Perception of exercise
• Study was conducted at AHI with 40 female participants to reveal perception of benefit and barrier to exercise using a questionnaire.
• The participants were divided in 3 groups.
• Group A- Participants attending Cardiac rehabilitation (age 50-60 yrs).
• Group B- Relatives accompanying participants (age 50-60 yrs).
• Group C- Students at AHI (age 20-25 yrs).
143.1
130.4134.8
A B C
Groups
Exercise Benefits / Barriers Scale
46.2636.6
0
20
40
60
% of patients in Cardiac Rehabilitation (March- July 07)
Males
Females
Males 46.26
Females 36.6
% Joined
Relatives Accompanying patients
61%
86%
0%
20%
40%
60%
80%
100%
Male Female
% of female patients in rehab
Male82%
Female18%
Male
Female
Outline
• Reasons for higher CHD prevalence in S. Asians
• Significance of CHD risk factors in S. Asians
• Factors affecting risk factor reduction in S. Asians
• Conclusions
Conclusions
• South Asians are at much higher risk for CHD than the general population
• Their risk factor profile is different, especially in relation to the metabolic syndrome
• Physical activity and healthful dietary habits need to be promoted, keeping in mind certain cultural differences (however, these should not be over-emphasized)