Referral services Internal Medicine Oncology Diagnostic Imaging Cardiorespiratory Medicine Dermatology Orthopaedic Surgery Spinal Surgery Soft Tissue Surgery Ophthalmology Neurology Anaesthesia and Pain Management Radioiodine Treatment Physiotherapy and Hydrotherapy Call us today on 01332 548911 Pride Veterinary Centre Riverside Road, Pride Park, Derby DE24 8HX As part of the expansion of our referral services, we are delighted to introduce our new referral team members: Referral Newsletter Issue 4 Spring 2014 email: [email protected]Cardiology Tea Time Teaser Answers... Three normal sinus complexes are seen on the tracing with normal morphology, except for a tall R-wave (3.2mV) in lead II (7th, 17th and 18th complexes). Based on consecutively occurring P-waves, the sinus node depolarizes at a rate of 143-167bpm. The ECG tracing shows the occurrence of 2 paroxysms of ventricular tachycardia with variable R-R intervals. The instantaneous rate between the ventricular complexes ranges between 231-353bpm. The morphology of the ventricular ectopic beats suggests conduction with a right bundle branch pattern. The complex following the first sinus complex differs in its morphology from the sinus complexes, as well as the ventricular ectopic complexes. This complex is a fusion beat (8th complex). Fusion beats result from simultaneous depolarisation by the SA node and the VPC. Considering the signalment and ECG findings the puppy most likely has Inherited Ventricular Arrhythmias of German Shepherd Dogs (IVAGSD). Ventricular arrhythmias and the predisposition for sudden death have been identified in German Shepherd Dogs. This arrhythmia is most prevalent in young dogs between 22-26 weeks of age, but can start as early as 8 weeks. ECG findings commonly include rapid, non-sustained, and polymorphic ventricular tachycardia, often preceded by a pause. IVAGSD is bradycardia-dependent and sudden death, secondary to ventricular fibrillation, usually occurs in the early morning hours while asleep or during rest after exercise. Sinus tachycardia usually suppresses the arrhythmia. Ventricular tachycardia is caused by triggered activity; in particular early afterdepolarisations (EADs) are suspected to cause these ventricular arrhythmias. A reduced sympathetic innervation and delayed repolarisation are thought to cause EADs. Over time sympathetic innervation increases and patients grow out of the condition. Diagnosis is complicated by the lack of clinical symptoms (arrhythmias occur at rest) and a Holter monitor is usually necessary to diagnose this disease. A Holter is also recommended in dogs that are related to individuals with IVAGSD. Arrhythmias that might be found during puppy examinations (e.g. vaccinations/pre-neutering checks) warrant further investigation as during episodes of rests an increase in severity and complexity is expected. If untreated, approximately 60% of individuals will experience sudden death. Affected dogs do not show clinical signs and outgrow the condition if they live past 24 months. Once outgrown they can live a normal live and do not require further treatment with antiarrhythmics. This patient was treated with a combination of sotalol and mexiletine until she reached two years of age. The arrhythmia was well controlled with this protocol. Antiarrhythmic drug therapy was discontinued thereafter as she had outgrown her disease. Dr Kinley Smith MA VetMB PhD CertSAS DipECVS MRCVS European Specialist in Veterinary Surgery Kinley graduated from Cambridge Vet School in 2000 and worked in small animal practice prior to undertaking a Residency in Small Animal Surgery at Glasgow Vet School. He gained the European Diploma in Veterinary Surgery in 2014. Kinley’s areas of clinical interest are traumatology and critical care; surgical and medical management of joint disease; wound management and reconstructive surgery. When he is not busy with his three young children, Kinley likes to climb and mountain bike as well as going on long walks with the family pet, Gypsy, a retired Guide Dog. Joshua Steinhaus MS BVMS MRCVS Joshua graduated from Murdoch University in Perth, Australia in 2007. He completed a residency in Small Animal Medicine at Veterinary Referral and Emergency Centre (Norwalk, CT, USA) in 2012. He has worked in small animal practice in both emergency and referral departments in the USA, completing an Internship in 2008. Joshua’s areas of clinical interest are respiratory tracheal collapse management including tracheal stenting, urology including ureteral and urethral obstructions, incontinence, haematuria, and vascular interventions including coil embolisation of intrahepatic shunts and intra-arterial chemotherapy and embolisation. Dr Nick Bexfield BVetMed PhD DSAM DipECVIM(CA) FSBiol MRCVS European Specialist in Small Animal Internal Medicine Clinical Associate Professor in Small Animal Medicine and Oncology, School of Veterinary Medicine and Science, The University of Nottingham Nick graduated in June 1999 from The Royal Veterinary College, University of London. After graduation, Nick spent four years in practice before completing a residency in Small Animal Medicine and Oncology at the University of Cambridge. He gained both the RCVS and European Diplomas in Small Animal Medicine in 2006, and is a European Specialist. He remained at Cambridge as a medicine clinician for a further two years before undertaking a Wellcome Trust funded PhD. He was the Clinical Oncologist at Cambridge for a year, before moving to the University of Nottingham in December 2013 to become Clinical Associate Professor in Small Animal Medicine and Oncology. He is the BSAVA Congress Programme Committee vice-chair and also co-author of the BSAVA Guide to Procedures in Small Animal Practice. Nick’s areas of clinical interest are in internal medicine, especially hepatology, immune-mediated diseases and endocrinology. He also has a special interest in medical oncology. By Maxie Krueger MedVet DipACVIM (Cardiology) MRCVS American Specialist in Veterinary Cardiology Jessica Adamany BSc, DVM, MRCVS ECVIM Small Animal Internal Medicine Resident Jessica graduated from the University of Maryland, College Park in 2007, and completed a Small Animal Medicine and Surgical Internship at the University of Saskatchewan. After spending a year travelling, Jessica completed an internship then joined the referral service at Pride Veterinary Centre as a Resident in Internal Medicine. Jessica’s areas of clinical interest are small animal internal medicine - specifically endocrine diseases, haematology, and infectious disease. Annette graduated in Hanover, Germany in 2000 followed by completion in 2002 of a doctoral thesis in ‘Hereditary Ataxia in the Jack Russell Terrier’. Annette moved to the UK shortly afterwards and undertook a residency at the Royal Veterinary College in veterinary neurology, and has since been awarded the European Diploma in Veterinary Neurology. She then worked as a small animal neurologist at a referral centre, and as a senior lecturer in veterinary neurology at the University of Glasgow Veterinary School. Annette joined the referral team at Pride Veterinary Centre in March 2013. Annette regularly presents at the Annual Symposium of the European College of Veterinary Neurology and gave CPD presentations at the Scottish BSAVA. Annette’s areas of clinical interest are neurosurgery, rehabilitation in small animals following spinal cord injury, and the quality of life aspect in epileptic dogs and their owners caring for a dog with epilepsy. Annette Wessmann DrMedVet DipECVN PGCertAcPrac FHEA MRCVS European Specialist in Veterinary Neurology 1: Gutierrez-Quintana R, Hammond G, Wessmann A. Ventral occipito-atlanto-axial fluid-filled lesion causing dynamic spinal cord compression in a cat. J Feline Med Surg. 2013 Oct 7. 2: Wessmann A, Hennessey A, Goncalves R, Benigni L, Hammond G, Volk HA. The association of middle ear effusion with trigeminal nerve mass lesions in dogs. Vet Rec. 2013 Nov 9;173(18):449. 3: Gutierrez-Quintana R, Carrera I, Dobromylskyj M, Patterson-Kane J, Ortega M, Wessmann A. Pituitary metastasis of pancreatic origin in a dog presenting with acute-onset blindness. J Am Anim Hosp Assoc. 2013 Nov-Dec;49(6):403-6. Recent work published by our clinicans CPD Evening "From Pacemaker to Stents. An Introduction to the Interventional Radiology and Cardiology Services available at Pride." Wednesday 30th April 2014 7.00pm for 7.30pm start The Priest House Hotel, Castle Donnington Sponsored by Dextronix Hot food provided To book your place at our CPD evening, please contact us on 01332 548911 or email [email protected]providing your name, practice name and address, telephone number and the best email address to use for correspondence. If you have any dietary requirements, please advise us in advance.
Transcript
ReferralservicesInternal Medicine
Oncology
Diagnostic Imaging
CardiorespiratoryMedicine
Dermatology
Orthopaedic Surgery
Spinal Surgery
Soft Tissue Surgery
Ophthalmology
Neurology
Anaesthesia and PainManagement
RadioiodineTreatment
Physiotherapy andHydrotherapy
Call us today on
01332 548911Pride Veterinary CentreRiverside Road, Pride Park,Derby DE24 8HX
As part of the expansion of our referral services, we are delighted to introduce our new referral team members:
Cardiology Tea Time TeaserAnswers...Three normal sinus complexes are seen onthe tracing with normal morphology, exceptfor a tall R-wave (3.2mV) in lead II (7th, 17thand 18th complexes). Based on consecutivelyoccurring P-waves, the sinus node depolarizes at a rate of 143-167bpm. The ECGtracing shows the occurrence of 2 paroxysmsof ventricular tachycardia with variable R-Rintervals. The instantaneous rate between the ventricular complexes ranges between231-353bpm. The morphology of the ventricular ectopic beats suggests conduction with a right bundle branch pattern.The complex following the first sinus complexdiffers in its morphology from the sinus complexes, as well as the ventricular ectopiccomplexes. This complex is a fusion beat (8th complex). Fusion beats result from simultaneous depolarisation by the SA nodeand the VPC.
Considering the signalment and ECG findingsthe puppy most likely has Inherited VentricularArrhythmias of German Shepherd Dogs
(IVAGSD). Ventricular arrhythmias and thepredisposition for sudden death have beenidentified in German Shepherd Dogs. Thisarrhythmia is most prevalent in young dogsbetween 22-26 weeks of age, but can start as early as 8 weeks. ECG findings commonlyinclude rapid, non-sustained, and polymorphic ventricular tachycardia, oftenpreceded by a pause. IVAGSD is bradycardia-dependent and sudden death,secondary to ventricular fibrillation, usuallyoccurs in the early morning hours whileasleep or during rest after exercise. Sinustachycardia usually suppresses the arrhythmia. Ventricular tachycardia is causedby triggered activity; in particular early afterdepolarisations (EADs) are suspected to cause these ventricular arrhythmias. A reduced sympathetic innervation anddelayed repolarisation are thought to causeEADs. Over time sympathetic innervationincreases and patients grow out of the condition. Diagnosis is complicated by thelack of clinical symptoms (arrhythmias
occur at rest) and a Holter monitor is usuallynecessary to diagnose this disease. A Holteris also recommended in dogs that are relatedto individuals with IVAGSD. Arrhythmias thatmight be found during puppy examinations(e.g. vaccinations/pre-neutering checks) warrant further investigation as duringepisodes of rests an increase in severity and complexity is expected.
If untreated, approximately 60% of individualswill experience sudden death. Affected dogsdo not show clinical signs and outgrow thecondition if they live past 24 months. Onceoutgrown they can live a normal live and do not require further treatment with antiarrhythmics.
This patient was treated with a combination of sotalol and mexiletineuntil she reached two years of age. The arrhythmia was well controlledwith this protocol. Antiarrhythmic drugtherapy was discontinued thereafter as she had outgrown her disease.
Dr Kinley SmithMA VetMB PhD CertSAS DipECVS MRCVS
European Specialist in VeterinarySurgery
Kinley graduated from CambridgeVet School in 2000 and worked insmall animal practice prior toundertaking a Residency in SmallAnimal Surgery at Glasgow VetSchool. He gained the EuropeanDiploma in Veterinary Surgery
in 2014. Kinley’s areas of clinical interest are traumatology and critical care; surgical and medicalmanagement of joint disease; wound managementand reconstructive surgery.
When he is not busy with his three young children,Kinley likes to climb and mountain bike as well asgoing on long walks with the family pet, Gypsy, aretired Guide Dog.
Joshua Steinhaus MS BVMS MRCVS
Joshua graduated from MurdochUniversity in Perth, Australia in2007. He completed a residency in Small Animal Medicine atVeterinary Referral andEmergency Centre (Norwalk, CT, USA) in 2012. He has worked
in small animal practice in both emergency and referral departments in the USA, completing anInternship in 2008.
Joshua’s areas of clinical interest are respiratory tracheal collapse management including trachealstenting, urology including ureteral and urethralobstructions, incontinence, haematuria, and vascular interventions including coil embolisation ofintrahepatic shunts and intra-arterial chemotherapyand embolisation.
Dr Nick Bexfield BVetMed PhD DSAM DipECVIM(CA) FSBiol MRCVS
European Specialist in Small AnimalInternal Medicine
Clinical Associate Professor in SmallAnimal Medicine and Oncology, Schoolof Veterinary Medicine and Science, The University of Nottingham
Nick graduated in June 1999 from The Royal Veterinary College, University of London.After graduation, Nick spent four years in practice before completing a residency in SmallAnimal Medicine and Oncology
at the University of Cambridge. He gained both theRCVS and European Diplomas in Small AnimalMedicine in 2006, and is a European Specialist. Heremained at Cambridge as a medicine clinician for a further two years before undertaking a WellcomeTrust funded PhD. He was the Clinical Oncologist at Cambridge for a year, before moving to the University of Nottingham in December 2013 tobecome Clinical Associate Professor in Small Animal Medicine and Oncology. He is the BSAVACongress Programme Committee vice-chair and also co-author of the BSAVA Guide to Procedures in Small Animal Practice.
Nick’s areas of clinical interest are in internal medicine, especially hepatology, immune-mediateddiseases and endocrinology. He also has a specialinterest in medical oncology.
By Maxie Krueger MedVet DipACVIM (Cardiology) MRCVSAmerican Specialist in Veterinary Cardiology
Jessica Adamany BSc, DVM, MRCVS
ECVIM Small Animal InternalMedicine Resident
Jessica graduated from theUniversity of Maryland, CollegePark in 2007, and completed aSmall Animal Medicine andSurgical Internship at theUniversity of Saskatchewan. After spending a year travelling,
Jessica completed an internship then joined the referral service at Pride Veterinary Centre as aResident in Internal Medicine.
Jessica’s areas of clinical interest are small animalinternal medicine - specifically endocrine diseases,haematology, and infectious disease.
Annette graduated inHanover, Germany in 2000followed by completion in2002 of a doctoral thesis in ‘Hereditary Ataxia in the Jack Russell Terrier’.Annette moved to the UK
shortly afterwards and undertook a residencyat the Royal Veterinary College in veterinaryneurology, and has since been awarded theEuropean Diploma in Veterinary Neurology.She then worked as a small animal neurologistat a referral centre, and as a senior lecturer inveterinary neurology at the University ofGlasgow Veterinary School. Annette joinedthe referral team at Pride Veterinary Centre inMarch 2013. Annette regularly presents at theAnnual Symposium of the European Collegeof Veterinary Neurology and gave CPD presentations at the Scottish BSAVA.Annette’s areas of clinical interest are neurosurgery, rehabilitation in small animalsfollowing spinal cord injury, and the quality oflife aspect in epileptic dogs and their ownerscaring for a dog with epilepsy.
1: Gutierrez-Quintana R, Hammond G,Wessmann A. Ventral occipito-atlanto-axial fluid-filled lesion causing dynamic spinal cordcompression in a cat. J Feline
Med Surg. 2013 Oct 7.
2: Wessmann A, Hennessey A, Goncalves R,Benigni L, Hammond G, Volk HA. The association of middle ear effusion with trigeminalnerve mass lesions in dogs.
Vet Rec. 2013 Nov 9;173(18):449.
3: Gutierrez-Quintana R, Carrera I, DobromylskyjM, Patterson-Kane J, Ortega M, Wessmann A.Pituitary metastasis of pancreatic origin in a dogpresenting with acute-onset blindness. J AmAnim Hosp Assoc. 2013 Nov-Dec;49(6):403-6.
Recent work published by our clinicans CPD Evening
"From Pacemaker to Stents.An Introduction to the
Interventional Radiology and Cardiology Services
available at Pride."
Wednesday 30th April 2014
7.00pm for 7.30pm start
The Priest House Hotel,Castle Donnington
Sponsored by DextronixHot food provided
To book your place at our CPD evening,please contact us on 01332 548911 or [email protected] your name, practice name andaddress, telephone number and the bestemail address to use for correspondence. If you have any dietary requirements,please advise us in advance.
Bonnie made a very good recovery and was eating well the evening following the procedure.She was immediately fed with food that wasgiven as a wet mash. We advised feeding her in a standing position to ease the oesophagealtransit. Ideally that could be done with a foodbowl placed on a stand or by feeding her on thestairs. She was discharged from the hospital 2 days after the procedure. Apart from a self-resolving subcutaneous seroma, recoverywas straight forward, and no lameness nor discomfort were observed on the left hinddespite the ligation of the left subclavian artery.
Eleven months after the surgery, Bonnie is doingextremely well. She is a very active and fit dogand despite eating very well, the owners arestruggling to make her gain weight as she isexercising all the time. As is common in PRAAshe still needs to be fed from a height but she isnow eating medium size kibbles without anyhelp. Regurgitation is no longer observed. At thetime of writing, the owner reported that theweek-end before, Bonnie even managed to eat awhole bird which was due to be put on the tablefor the family's Sunday roast!
Referral Service at Pride Veterinary Centre email: [email protected]
Soft Tissue Surgery CaseStudy‘Bonnie’ (a very lively female Cocker Spaniel puppy) was only 5 months old when she was referred to the Pride VeterinaryCentre's surgery department, weighing only 6.5kg. Bonnie wasreferred because of frequent regurgitation when eating, herobvious stunted growth and her very poor body condition.
The referring veterinary surgeon took radiographs of the chest with contrast in theoesophagus which showed cranial oesophagealdilation, potentially consistent with oesophagealconstriction/ stricture (Figure 1).
Clinical examination was unremarkable.However Bonnie appeared very thin and underdeveloped for a 5 month old puppy. The ownersreported that feeding mashed food by hand(with a spoon) markedly reduced the regurgitation. According to them, regurgitationwas observed as soon as Bonnie started to be fed with solid food.
Based on the history, examination and initial RVS radiographs, oesophageal stricture by an aberrant aortic arch was suspected. CTexamination of the chest was performed. Thisshowed a right sided aortic cross (situs inversus)with a remaining left ligamentum arteriosumwhich was compressing the oesophagus againstthe heart base. These features are most commonly associated with a persistent rightaortic arch (PRAA). The examination also
showed an aberrant left subclavian artery whichwas compressing the oesophagus at the level ofthe thoracic inlet from dorsal to ventral (Figure 2).
Surgical exploration was performed the day following imaging . A left 4th intercostal spacethoracotomy was performed. A large bore Foleycatheter was placed orally into the stomach, theballoon was inflated and the tube was retrieved to show the stricture point. The persistent left ligamentum arteriosum was identified, isolatedand ligated (Figure 3). The fibrous tissue preventing oesophageal distention was also dissected. The tube was then retrieved furtherorally and showed partial stricture by the aberrantdorsal left subclavian artery. Full occlusion of thisvessel showed initial complete arrest of the pedalpulse in the left fore then after a minute re-ignitionof the pulse was detected by the Doppler probe.This was possible by collateral circulation provided by the vertebral artery above the aberrant vessel. Vessel ligature and sectionallowed free dilation of the oesophagus at thelevel of the thoracic inlet without any restriction.
Figure 1:Lateral view of the chest after barium swallow. There is a marked barium accumulation in theproximal thoracic oesophagus (green arrowheads) with a narrowing just after the thoracicinlet consistent with a compression (later identified as the imprint of the aberrant subclavianartery). The accumulation of barium stops acutely just before the heart base.
Hervé Brissot graduatedfrom the VeterinarySchool of Toulouse inFrance in 1994. Since then he has pursued hisinterest in small animalsurgery.
Hervé has been a Diplomate of the European College of Veterinary Surgeonssince 2005 and as such he is a EuropeanRecognised Specialist in Small AnimalSurgery. He has been working in the UKsince 2006, joining the team at PrideVeterinary Centre in 2013.
Hervé is mainly interested in soft tissue surgery and especially oncosurgery, lung surgery and mini-invasive surgery. He hasalready published original papers in peerreviewed international veterinary journals and textbooks, and has spoken and lecturedin UK and European congresses.
Hervé BrissotDV DipECVS MRCVS
European Specialist in Small Animal Surgery
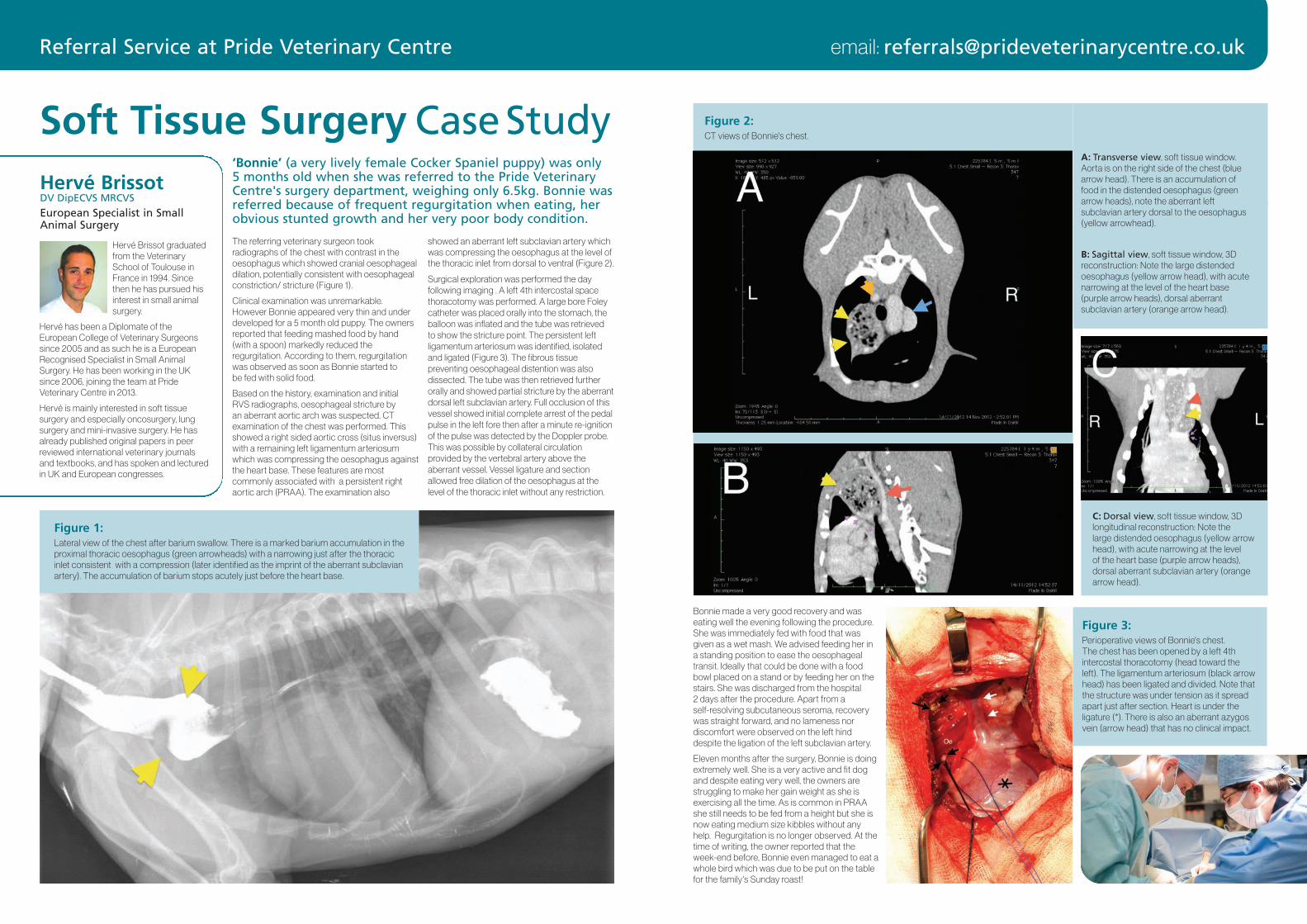
Figure 2:CT views of Bonnie's chest.
B: Sagittal view, soft tissue window, 3Dreconstruction: Note the large distendedoesophagus (yellow arrow head), with acutenarrowing at the level of the heart base (purple arrow heads), dorsal aberrant subclavian artery (orange arrow head).
C: Dorsal view, soft tissue window, 3Dlongitudinal reconstruction: Note the large distended oesophagus (yellow arrowhead), with acute narrowing at the level of the heart base (purple arrow heads),dorsal aberrant subclavian artery (orangearrow head).
A: Transverse view, soft tissue window.Aorta is on the right side of the chest (bluearrow head). There is an accumulation offood in the distended oesophagus (greenarrow heads), note the aberrant left subclavian artery dorsal to the oesophagus(yellow arrowhead).
Figure 3:Perioperative views of Bonnie's chest. The chest has been opened by a left 4thintercostal thoracotomy (head toward theleft). The ligamentum arteriosum (black arrowhead) has been ligated and divided. Note thatthe structure was under tension as it spreadapart just after section. Heart is under the ligature (*). There is also an aberrant azygosvein (arrow head) that has no clinical impact.
Joshua SteinhausMS BVMS MRCVS
Joshua graduated fromMurdoch University inPerth, Australia in 2007.He completed a residency in Small Animal Medicineat Veterinary Referral andEmergency Centre
(Norwalk, CT, USA) in 2012. He has worked insmall animal practice in both emergency and referral departments in the USA, completingan Internship in 2008.
Joshua’s areas of clinical interest are respiratory tracheal collapse managementincluding tracheal stenting, urology includingureteral and urethral obstructions, incontinence, haematuria, and vascular interventions including coil embolisation ofintrahepatic shunts and intra-arterialchemotherapy and embolisation.
Referral Service at Pride Veterinary Centre email: [email protected]
Figure 1:Lateral radiograph showing A SUB devicewith a locking loop catheter in the kidneyand another catheter in the bladder connecting to a vascular access port.
Figure 2:Lateral radiograph of a patient with a prostatic adenocarcinoma following urethral stent placement. There is contrast in the bladder and urethral stent demonstrating patency.
We listen to you! As a referral practice we arekeen to continue to build our relationships withthe local practices we listen to what you say, andidentified the following;
1. You want set prices to quote your clientsand so we have set the following e.g.
l TTA £2200
l Lateral Suture £1000
l Patella luxation £1400
l Healthy dog fracture repair
l Simple pin £1200+ implants
l Simple plate £1500+implants
l Complex fractures £2,000-£4,000
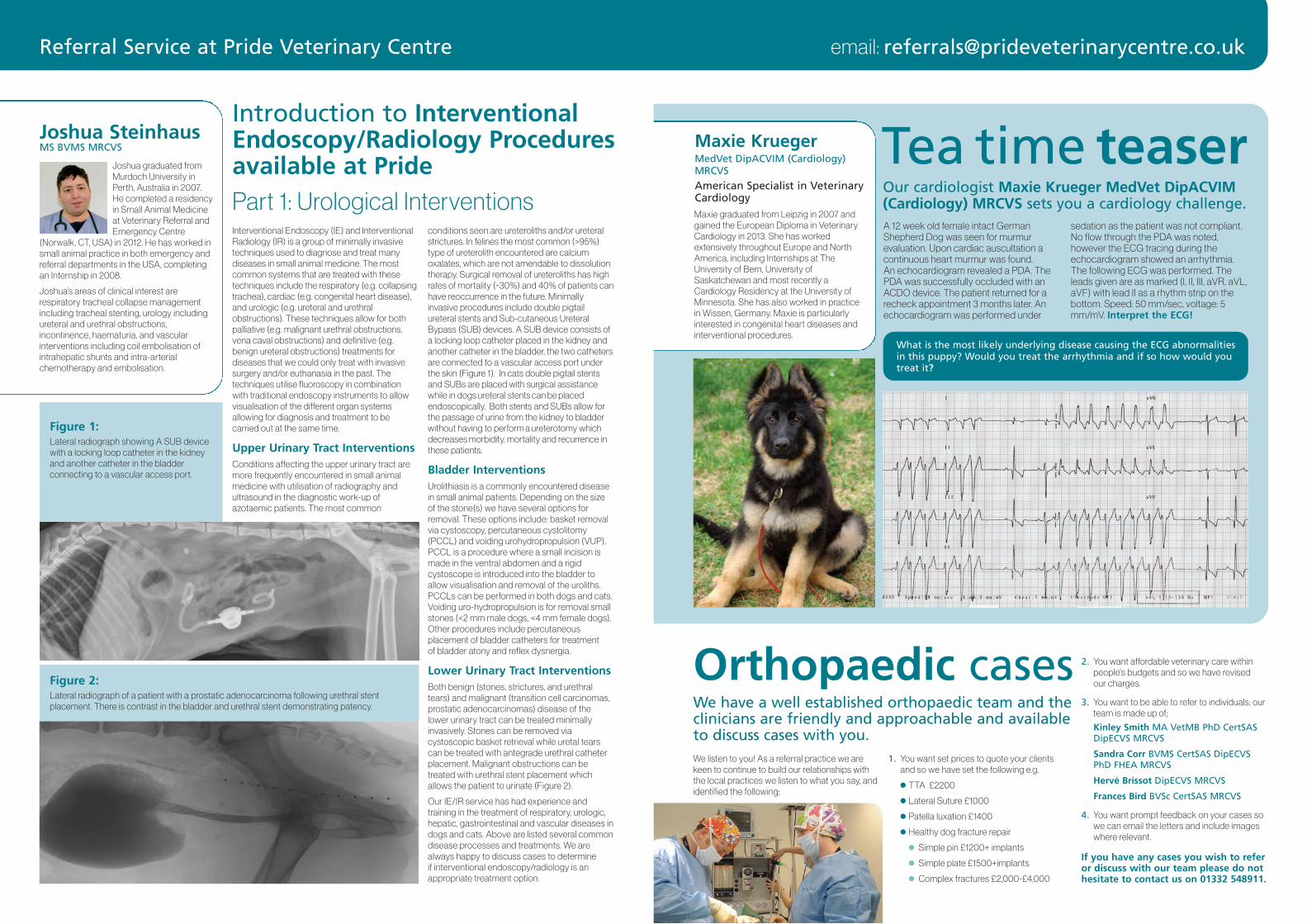
Tea time teaserOur cardiologist Maxie Krueger MedVet DipACVIM(Cardiology) MRCVS sets you a cardiology challenge.A 12 week old female intact GermanShepherd Dog was seen for murmur evaluation. Upon cardiac auscultation acontinuous heart murmur was found. An echocardiogram revealed a PDA. ThePDA was successfully occluded with anACDO device. The patient returned for arecheck appointment 3 months later. Anechocardiogram was performed under
sedation as the patient was not compliant.No flow through the PDA was noted, however the ECG tracing during theechocardiogram showed an arrhythmia.The following ECG was performed. Theleads given are as marked (I, II, III, aVR, aVL,aVF) with lead II as a rhythm strip on thebottom. Speed: 50 mm/sec, voltage: 5mm/mV. Interpret the ECG!
Maxie graduated from Leipzig in 2007 andgained the European Diploma in VeterinaryCardiology in 2013. She has worked extensively throughout Europe and NorthAmerica, including Internships at TheUniversity of Bern, University ofSaskatchewan and most recently aCardiology Residency at the University ofMinnesota. She has also worked in practicein Wissen, Germany. Maxie is particularlyinterested in congenital heart diseases andinterventional procedures.
Maxie KruegerMedVet DipACVIM (Cardiology) MRCVS
American Specialist in VeterinaryCardiology
What is the most likely underlying disease causing the ECG abnormalitiesin this puppy? Would you treat the arrhythmia and if so how would youtreat it?
Interventional Endoscopy (IE) and InterventionalRadiology (IR) is a group of minimally invasivetechniques used to diagnose and treat many diseases in small animal medicine. The mostcommon systems that are treated with thesetechniques include the respiratory (e.g. collapsingtrachea), cardiac (e.g. congenital heart disease),and urologic (e.g. ureteral and urethral obstructions). These techniques allow for bothpalliative (e.g. malignant urethral obstructions,vena caval obstructions) and definitive (e.g.benign ureteral obstructions) treatments for diseases that we could only treat with invasivesurgery and/or euthanasia in the past. The techniques utilise fluoroscopy in combination with traditional endoscopy instruments to allowvisualisation of the different organ systems allowing for diagnosis and treatment to be carried out at the same time.
Upper Urinary Tract InterventionsConditions affecting the upper urinary tract aremore frequently encountered in small animalmedicine with utilisation of radiography andultrasound in the diagnostic work-up of azotaemic patients. The most common
conditions seen are ureteroliths and/or ureteralstrictures. In felines the most common (>95%)type of ureterolith encountered are calciumoxalates, which are not amendable to dissolutiontherapy. Surgical removal of ureteroliths has highrates of mortality (~30%) and 40% of patients canhave reoccurrence in the future. Minimally invasive procedures include double pigtail ureteral stents and Sub-cutaneous UreteralBypass (SUB) devices. A SUB device consists ofa locking loop catheter placed in the kidney andanother catheter in the bladder, the two cathetersare connected to a vascular access port underthe skin (Figure 1). In cats double pigtail stentsand SUBs are placed with surgical assistancewhile in dogs ureteral stents can be placedendoscopically. Both stents and SUBs allow forthe passage of urine from the kidney to bladderwithout having to perform a ureterotomy whichdecreases morbidity, mortality and recurrence inthese patients.
Bladder InterventionsUrolithiasis is a commonly encountered diseasein small animal patients. Depending on the sizeof the stone(s) we have several options forremoval. These options include: basket removalvia cystoscopy, percutaneous cystolitomy(PCCL) and voiding urohydropropulsion (VUP).PCCL is a procedure where a small incision ismade in the ventral abdomen and a rigid cystoscope is introduced into the bladder toallow visualisation and removal of the uroliths.PCCLs can be performed in both dogs and cats.Voiding uro-hydropropulsion is for removal smallstones (<2 mm male dogs, <4 mm female dogs).Other procedures include percutaneous placement of bladder catheters for treatment of bladder atony and reflex dysnergia.
Lower Urinary Tract InterventionsBoth benign (stones, strictures, and urethraltears) and malignant (transition cell carcinomas,prostatic adenocarcinomas) disease of the lower urinary tract can be treated minimally invasively. Stones can be removed via cystoscopic basket retrieval while uretal tearscan be treated with antegrade urethral catheterplacement. Malignant obstructions can be treated with urethral stent placement whichallows the patient to urinate (Figure 2).
Our IE/IR service has had experience and training in the treatment of respiratory, urologic,hepatic, gastrointestinal and vascular diseases indogs and cats. Above are listed several commondisease processes and treatments. We arealways happy to discuss cases to determine if interventional endoscopy/radiology is anappropriate treatment option.
Introduction to InterventionalEndoscopy/Radiology Procedures available at PridePart 1: Urological Interventions
Orthopaedic casesWe have a well established orthopaedic team and theclinicians are friendly and approachable and availableto discuss cases with you.
2. You want affordable veterinary care withinpeople's budgets and so we have revisedour charges.
3. You want to be able to refer to individuals; ourteam is made up of;
Kinley Smith MA VetMB PhD CertSASDipECVS MRCVS
Sandra Corr BVMS CertSAS DipECVSPhD FHEA MRCVS
Hervé Brissot DipECVS MRCVS
Frances Bird BVSc CertSAS MRCVS
4. You want prompt feedback on your cases sowe can email the letters and include imageswhere relevant.
If you have any cases you wish to refer or discuss with our team please do nothesitate to contact us on 01332 548911.
Referral Service at Pride Veterinary Centre email: [email protected]
Specialist visit to Cuba
The WSAVA brings together veterinary organisations from all over the world, with theaim of encouraging ‘exchange of scientific information between individual veterinarians and veterinary organisations.’
During 14th-18th November, Sandra met witharound 120 Cuban vets, who attended a one-daycourse (in Havana) or a two-day course (in Pinardel Rio). Sandra lectured on subjects such as basic fracture treatment and bandaging techniques, and how to perform common
abdominal surgical procedures. Despite the language barrier - and with the help of an interpreter - the lectures and discussions werevery interactive, with the Cuban vets very keen to discuss cases and learn about new treatments. As is traditional, such meetings endwith a social event; the music, dancing and cocktails were as amazing as you might imagine!
Later this year, Sandra will be lecturing inUkraine, Albania and Romania on behalf ofWSAVA - watch this space!
At the end of last year, Dr Sandra Corr, who is one ofour surgical Specialists visited Cuba to provide teachingto local vets, on behalf of the World Small AnimalVeterinary Association (WSAVA).
Dr Sandra CorrBVMS CertSAS DipECVS FHEA PhDMRCVS
European Specialist in SmallAnimal Surgery
Associate Professor in SmallAnimal Surgery - University ofNottingham
Sandra Corr graduatedfrom Glasgow Universityfollowed by a residency in Small Animal Surgery.Sandra worked extensivelywithin small animal andequine practice in Surrey
and Essex. She travelled to work at theUniversity of Zimbabwe for 2 years, thenundertook several University positions including a PhD. Sandra became a SeniorLecturer and Head of Orthopaedics at theRoyal Veterinary College, London before joining the University of Nottingham team as a Reader and Associate Professor in SmallAnimal Surgery. Sandra is on the NottinghamUniversity teaching team based at PrideVeterinary Centre. Her areas of clinical interest are orthopaedic surgery, animal locomotion and biomechanics. Sandra is dedicated to animal welfare and ethics relating to companion animals and is currently co-authoring a book on Companion AnimalEthics. In addition, she regularly presents atCPD courses, meetings and conferencesworldwide.
What are the goals of breedheart testing?It has been shown that some heart diseases aremore common in certain breeds and lines. Inorder to determine whether a dog or cat suffersfrom acquired (e.g. chronic degenerative valvedisease (CDVD), dilated cardiomyopathy (DCM),hypertrophic cardiomyopathy (HCM)) or congenital heart disease we offer a range ofdiagnostic tests. Identifying dogs and cats thatare free from cardiac abnormalities is especiallyimportant in pets that are used for breeding andbreed clubs will encourage screening of theseanimals. If there is a murmur or arrhythmia present it is advisable to further investigate the cause. Once diagnosed we will be able to discuss further tests, whether treatment is indicated and the implication of the condition for the patient. Last but not least, collating dataabout heart diseases will help improve ourknowledge of genetically determined heart diseases in a given breed.
What methods are availablefor heart testing?Auscultation:
Heart murmurs and arrhythmias are commonclinical findings in dogs and cats with congenitalor acquired heart disease. If present, the murmurwill be graded based on timing, location, andintensity. However, there is a limitation to the diagnostic yield of auscultation. Not all significant
heart diseases, including DCM and HCM, willpresent with a murmur and auscultation might be within normal limits. Some factors can influence auscultatory findings, e.g. nervous, ordeep-chested patients can be a challenge.
Electrocardiogram (ECG):
An ECG is indicated if an abnormal heart rhythm is detected. It allows us to diagnose thearrhythmia and evaluate the heart’s electricalconduction system.
Echocardiogram (with Doppler):
Echocardiography and Doppler technologyallow us to critically evaluate the heart, includingquantification of wall thickness, chamber size,valve function, blood flow, and contractility.Structural changes of the heart that occur withcongenital heart diseases, CDVD, DCM, or HCMand severity of disease can be diagnosed withthis technique.
ConclusionsHeart testing can help breeders and breed clubsto identify heart disease in potential breedinganimals, in an effort to reduce the prevalence ofhereditary heart disease. It also shows theprevalence of congenital or acquired heart diseases in their breed. However, acquired heartdiseases can be challenging. Even if we find thata patient is free of a heart condition at the time of examination, this patient may develop cardiacdisease later in life. It is therefore recommendedto repeat the heart testing on a regular basis.
The Pride Veterinary Centre Cardiology Service is pleased tooffer breed screenings for dogs and cats. Our board certifiedcardiologist Maxie Krueger, MedVet DipACVIM (Cardiology)MRCVS is eligible to test for heart diseases in accordancewith the Veterinary Cardiovascular Society (VCS).
Heart testing in dogs and cats
We are lucky enough at Pride VeterinaryCentre to work with a large team of highly skilled nurses. All our nurses’ workwith both the first opinion and referralcases ensuring the highest standard ofcare is given to all our patients.
We have specialised nurses that work in medicine, theatre, anaesthesia, imaging, wards,ICU, neurology, ophthalmology, surgery, clinicsand out of hours critical care. We also have nurses that split their time betweendepartments. All of our nurses are registeredand fully qualified. Within these teams we havethree diploma holders, one emergency and critical care certificate holder and two moreworking towards the certificate. We also havethree nurses working toward their VTS qualifications in anaesthesia, surgery and criticalcare. The VTS is a specialised American qualification designed for nurses who specialisein one area. We also have nurses with qualifications in bereavement counselling, dogtraining and behaviour.
Our neurology, ophthalmology, and surgerynurses organise the referral clinicians in theirarea, helping them with their day patient list,checking their inpatients and liaising with theward nurses regarding their care. Our ward nurses look after all the inpatients and daypatients ensuring care plans are carried out,medications given, pain and comfort assessedand addressed and appropriate people are keptinformed of progress. One nurse also looks afterour isolation ward for anything infectious. For our very sick patients that require intensive monitoring we have a dedicated ICU nurse. Ourmedicine nurses organise the day cases for themedicine clinicians and assist with proceduressuch as endoscopy and ultrasound. They also coordinate the care of medical cases, for example blood transfusions. The out of hoursnurse is responsible for looking after the patientsovernight along with a veterinary surgeon andintern. The imaging nurse will monitor anaesthesia for advanced imaging and alsoposition animals for radiographs. Our theatreand anaesthesia nurses monitor anaesthesia
for surgical cases, they also set up for the specialised procedures such as laparoscopy,phacoemulsification, fluoroscopy and stenting.Our anaesthesia nurses alongside the anaesthesia clinicians to place jugular and arterial catheters for advanced monitoring as wellas using local techniques for pain management.
This diverse mix of skills means our patients canbe nursed by the appropriate team based on itsindividual needs. As always with nurses this alsocomes with masses of cuddles, a nursing skillwhich should never be overlooked!
Pride nursing team
Maxie KruegerMedVet DipACVIM (Cardiology) MRCVS
American Specialist in VeterinaryCardiology
Maxie graduated fromLeipzig in 2007 and gainedthe European Diploma in Veterinary Cardiology in 2013. She has workedextensively throughoutEurope and North
America, including Internships at TheUniversity of Bern, University of Saskatchewanand most recently a Cardiology Residency at the University of Minnesota. She has alsoworked in practice in Wissen, Germany. Maxieis particularly interested in congenital heartdiseases and interventional procedures.
Tuesday 8th April 2014
Medicine
The aim is to provide an informal evening(with pizza and beer) run by one of our referral veterinary surgeons discussing a hottopic and their approach. They will showsome of their cases and ideas and then discuss any cases that you may have thatcould be of interest. It is also the ideal opportunity to bring along any radiographs or bloods for discussion even if they do not fit with the topic.
To book your place at a clinical club event, please register by email [email protected] your name, practice name andaddress, telephone number and the bestemail address to use for correspondence.Please also state which clinical club you wishto attend as the email heading. If you haveany dietary requirements, please advise
us in advance.
We host a monthly clinical club and we would like to invite you to come along.
Clinical Club Dates at Pride Veterinary CentreTuesday 6th May 2014
Cardiology
Tuesday 3rd June 2014
Medicine
Tuesday 1st July 2014
Orthopaedics
Tuesday 5th August 2014
MedicineThey are held at Pride VeterinaryCentre, starting at 7.30pm.