97


Carpenters Benefit Funds350 Fordham Road, Wilmington, MA 01887

HEALTH FUNDN E W E N G L A N D C A R P E N T E R SS U M M A R Y P L A N
D E S C R I P T I O N
BENE
FITS GREAT BENEFITS
The New England Carpenters
Health Benefits Fund
FOR LIFE

HEALTH BENE
FITS
FU
ND
GREAT BENEFITS
As a member of the New
England Carpenters Health
Benefits Fund, you and your
family are eligible for a
generous benefits package
that offers you well-being,
security and protection.
FOR LIFE

The New England Carpenters Health Benefits Fund
350 Fordham RoadWilmington, MA 01887Phone: (800) 344-1515Fax: (978) 657-8724
August 2005
Dear Participant:
The Board of Trustees of the New England Carpenters Health Benefits Fund is pleased toissue this revised Summary Plan Description. This handbook has been written to reflectthe changes in the Health Benefits Fund since the last version was printed.
As your Board of Trustees, we continually evaluate the benefits for opportunities forenhancement while maintaining a financially sound Health Benefits Fund. When wedesign our benefit programs and make improvements, we try to do what’s best for theparticipants. This revised Summary Plan Description is a reflection of our efforts.
Note that medical benefits and weekly accident and sickness benefits are provideddirectly by the Fund. Life insurance and accidental death and dismemberment benefitsare underwritten by Hartford Life Insurance Company.
A New ApproachThis book has been designed to be easy to read and understand. “Fast Facts” appear atthe beginning of each section to give you a quick overview of what is contained withinthat section. Also, useful information—such as phone numbers and definitions—appearin the margin as a quick reference.
In addition, this book provides the required information about your rights and protectionunder the law in order to comply with the Employee Retirement Income Security Act of1974 (ERISA). This information is on page 67.
We encourage you and your family to read this Summary Plan Description carefully tomake the best use of the benefits the New England Carpenters Health Benefits Fund offers.
If you have any questions concerning the benefits or your eligibility, please feel free tocontact the Fund Office at (800) 344-1515.
Sincerely,Board of Trustees
1
Health Benefits Fund

Employer Trustees
William J. SullivanSecretary/Treasurer
Stephan A. Adamic Co-Secretary/Treasurer
George M. Bidgood
Theodore H. Brodie
Donald L. Colavecchio
Thomas J. Gunning
Michael Shaughnessy
William Shea
Thomas Steeves
Union Trustees
Thomas J. HarringtonChairman
Mark L. ErlichCo-Chairman
Thomas J. Flynn
Simon R. James
Bruce King
John Murphy
Michael Nelson
David Wallace
Jack Winfield
David A. Woodman
2
Executive Director Harry R. Dow
Director and Field Representative James W. Buckley, Jr.
Legal Counsel O’Reilly, Grosso & Gross
Krakow & Souris, LLC.
Consultants and Actuaries The Segal Company
The Board of Trustees reserves the right to terminate or amend thePlan at any time. This includes the right to amend or terminatebenefits or eligibility for any class of participant, including retirees,when in their sole discretion the Board determines such action is inthe best interest of the Fund and its participants.
Changes to your plan of benefits can happen at any time, so if youhave a question about a particular service or program, contact theFund Office for the most up-to-date information.
BOARD OF TRUSTEES
TABLE OF CONTENTS
Key Contact Phone Numbers and Addresses . . . . . . .4
Your Health Benefits Fund . . . . . . . . . . . . . . . . . . . . .5
Eligibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Maintaining Your Eligibility . . . . . . . . . . . . . . . . . . .7
If You’re Short of Hours . . . . . . . . . . . . . . . . . . . . . .7
Eligible Dependents . . . . . . . . . . . . . . . . . . . . . . . . .8
If Your Child’s Eligibility for Benefits Changes . . . . .9
Extension of Benefits for Totally
Disabled Members . . . . . . . . . . . . . . . . . . . . . . . . .9
When Coverage Ends . . . . . . . . . . . . . . . . . . . . . . . .9
Retiree Health Benefits Plan . . . . . . . . . . . . . . . . . .10
Continuing Your Coverage . . . . . . . . . . . . . . . . . . . . .11
COBRA Continuation Coverage . . . . . . . . . . . . . . .11
Life Events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
If You Move . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
If You Get Married . . . . . . . . . . . . . . . . . . . . . . . . .19
If You Have a Baby . . . . . . . . . . . . . . . . . . . . . . . . .20
If You Adopt a Child . . . . . . . . . . . . . . . . . . . . . . . .21
If You Divorce . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
If You Enter Active Military Service . . . . . . . . . . . .22
If You Become Disabled . . . . . . . . . . . . . . . . . . . . .23
If You Become Eligible for Medicare . . . . . . . . . . . .23
Upon Your Death . . . . . . . . . . . . . . . . . . . . . . . . . .24
Your Medical Plan . . . . . . . . . . . . . . . . . . . . . . . . . . .25
Lifetime Maximum Plan Benefit . . . . . . . . . . . . . . .25
Managed Health Care Program —
Preauthorization . . . . . . . . . . . . . . . . . . . . . . . . .27
Wellness Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . .30
Annual Physical Exams . . . . . . . . . . . . . . . . . . . . .30
Annual Pap Tests and Mammograms . . . . . . . . . . .30
Well-Child Exams . . . . . . . . . . . . . . . . . . . . . . . . .30
Hospitalization and Surgery . . . . . . . . . . . . . . . . . . .31
Hospitalization . . . . . . . . . . . . . . . . . . . . . . . . . . . .31
Surgeon’s Charges . . . . . . . . . . . . . . . . . . . . . . . . . .33
Mental Health and Substance Abuse . . . . . . . . . . . . .35
Preauthorization . . . . . . . . . . . . . . . . . . . . . . . . . . .36
3
Home Health Care . . . . . . . . . . . . . . . . . . . . . . . . . . .37
Hospice Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
Carpenters Assistance Program . . . . . . . . . . . . . . . . .39
Prescription Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Dental Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .43
Vision Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45
Life Insurance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .47
Coverage for Your Spouse . . . . . . . . . . . . . . . . . . . .47
If Your Coverage Ends . . . . . . . . . . . . . . . . . . . . . .48
Accidental Death and Dismemberment . . . . . . . . . . .49
Seatbelt Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . .50
Weekly Accident and Sickness . . . . . . . . . . . . . . . . .51
General Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . .52
Coordination of Benefits . . . . . . . . . . . . . . . . . . . . . .54
Reimbursement and Subrogation . . . . . . . . . . . . . .56
Filing Your Claims . . . . . . . . . . . . . . . . . . . . . . . . . . .58
When Claims Must Be Filed . . . . . . . . . . . . . . . . . .59
When A Claim Is Considered Received By
The Health Benefits Fund . . . . . . . . . . . . . . . . . .59
Urgent, Pre-Service and Concurrent Claims . . . . . .60
Prescription Drug Claims . . . . . . . . . . . . . . . . . . . .60
Claims Communications . . . . . . . . . . . . . . . . . . . .60
Comprehensive Medical Benefits Claims . . . . . . . . .60
Disability Claims (Weekly Accident and
Sickness Benefit) . . . . . . . . . . . . . . . . . . . . . . . . .63
Appeal Process . . . . . . . . . . . . . . . . . . . . . . . . . . . .64
Your ERISA Rights . . . . . . . . . . . . . . . . . . . . . . . . . . .67
Plan Facts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .69
Schedule of Benefits for Plan I . . . . . . . . . . . . . . . . .71
Schedule of Dental Benefits for Plan I . . . . . . . . . . . .74
Schedule of Benefits for Plan II . . . . . . . . . . . . . . . . .75
Schedule of Benefits for the Retiree Plan . . . . . . . . .78
Glossary of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . .80
New England Carpenters Health Benefits
Fund Privacy Notice . . . . . . . . . . . . . . . . . . . . . . . .83
4
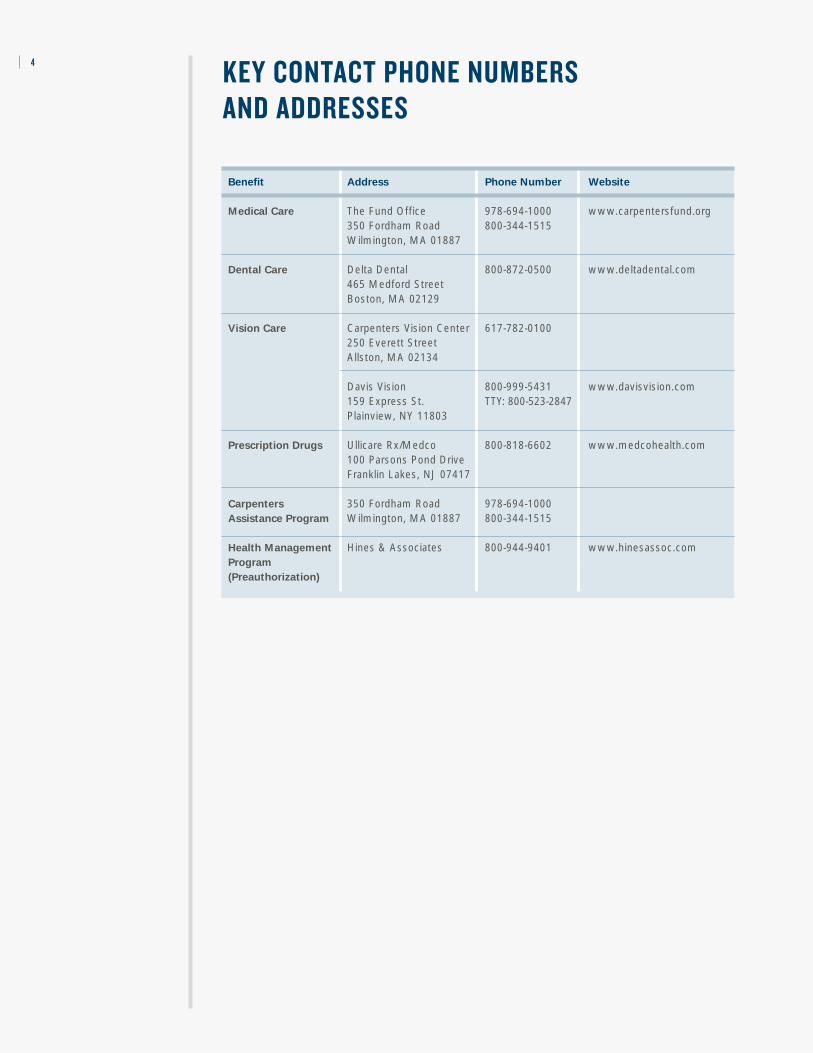
Benefit Address Phone Number Website
Medical Care The Fund Office 978-694-1000 www.carpentersfund.org 350 Fordham Road 800-344-1515 Wilmington, MA 01887
Dental Care Delta Dental 800-872-0500 www.deltadental.com 465 Medford StreetBoston, MA 02129
Vision Care Carpenters Vision Center 617-782-0100250 Everett StreetAllston, MA 02134
Davis Vision 800-999-5431 www.davisvision.com 159 Express St. TTY: 800-523-2847 Plainview, NY 11803
Prescription Drugs Ullicare Rx/Medco 800-818-6602 www.medcohealth.com100 Parsons Pond DriveFranklin Lakes, NJ 07417
Carpenters 350 Fordham Road 978-694-1000Assistance Program Wilmington, MA 01887 800-344-1515
Health Management Hines & Associates 800-944-9401 www.hinesassoc.comProgram
(Preauthorization)
KEY CONTACT PHONE NUMBERS AND ADDRESSES

YOUR HEALTH BENEFITS FUND
The New England Carpenters Health Benefits Fund offers eligiblemembers and their families comprehensive health care coverage.Benefits include office visits, hospitalization and surgery, homehealth care, coverage for prescription drugs, mental health andsubstance abuse treatment, dental and vision care.
You want the comfort of knowing that your family will beprotected if something happens to you. Eligible members qualifyfor a life insurance benefit, accidental death anddismemberment insurance benefits and weekly accident andsickness benefits. The Fund also offers an extension of medicalbenefits for you and your family if you become disabled, or foryour family—at no charge—in the event of your death.
H O W T H E H E A LT H B E N E F I TS F U N D W O R KS
The Health Benefits Fund contains three comprehensive healthcare plans, which offer coverage depending on your eligibility:
• PLAN I, for active members and their dependents;
• PLAN II, for active members and their dependents; and
• THE RETIREE PLAN, for eligible retirees and their dependents.
5

Your eligibility to participate in Plan I or Plan II is based on the number of hours youwork in covered employment and the contribution rate your employer is required tomake to the Fund on your behalf. Plan I offers coverage for members that work 600hours or more in a six-month period. Plan II offers a lower level of coverage for membersthat work at least 350 hours (but fewer than 600) in a six-month period. These rates areoutlined in a Collective Bargaining Agreement between your employer and the NewEngland Carpenters Health Benefits Fund.
Hours Requirements
Your eligibility for benefits—which is different from your eligibility to participate—depends on the number of hours you work in covered employment during a six-month“work period.” If you work the required number of hours—and your employercontributes to the Fund for those hours—you and your eligible dependents will be eligiblefor coverage for six months. The hours requirements for a six-month work period are:
• Plan I—600 hours in one work period or 1,250 hours in two consecutive work periods.
• Plan II—350 hours in one work period
• Local 1996– Plan I— 750 hours in one work period or 1,550 hours in
two consecutive work periods.– Plan II— 425 hours in one work period.
Work Periods and Coverage Periods
There are two work periods per year. The hours you work during the work period areused to determine whether you’re eligible for coverage during the six-month coverageperiod. Coverage periods begin on April 1 or October 1.
6
What is Covered
Employment?
Covered employment iswork you do for whichcontributions are made bya contributing employerunder the terms of a col-lective bargaining agree-ment or signed participa-tion agreement.
What is a Collective
Bargaining Agreement?
A Collective BargainingAgreement is a writtenagreement between aunion and an employerthat requires the employerto make contributions tothe Fund on behalf of itsemployees.
• You must work a specified number of hours in a six-month work period to be able to initially participate in the Plan.
• You must also work a specified number of hours to be eligible to receive benefits for you and /or your eligible dependents.
• When you don’t work enough hours to qualify for benefits, you may be able to purchase Continuation Coverage under the Federal program known as COBRA.
• When you retire, you may be able to purchase coverage under the Retiree Plan if you meet all the requirements.
ELIGIBILITY
FA ST FAC TS :
Review Date If you work the required hours You’ll be eligible for coverage
during the work period... during the coverage period...
April 1 August, September, October, April, May, June, July, August November, December and January and September
October 1 February, March, April, May, October, November, December, June and July January, February and March

7
M A I N TA I N I N G YO U R E L I G I B I L I T Y
Once you gain eligibility, that will continue as long as you work at least 600 hours (Plan I) or 350 hours (Plan II) in the six-month work period prior to the coverage period.
If you do not work the required number of hours, you may be able to maintain yourcoverage, as explained below, by:
• “Buying-In” to the Fund; or• Using the banked hours you’ve accumulated in your Hours Bank for hours
worked before 1989. Banked hours are removed once you retire.
Plan I — Active Members
Plan I members may continue coverage provided they work at least 1,250 hours in theprevious two consecutive six-month work periods preceding the period they werecovered.
Local 51 and Shops in Plan I Only
Shop employers contribute a set dollar amount for hours worked in the current month tobe covered for the following month. Members must work one hour and the employermust make the monthly contribution to be covered. For example, a member who worksone hour in May is entitled to full Plan I coverage for the month of June.
I F YO U ’ R E S H O R T O F H O U R S
If you do not qualify for continued coverage based on your hours worked, coverage maybe continued in two other ways—through the use of a Buy-In or Banked Hours.
Short Hours Buy-In
If you do not work enough hours during a work period to maintain your eligibility, youmay purchase Buy-In coverage if you were short by 30 hours or less. In order to takeadvantage of the buy-in provision, you must have been eligible during the precedingcoverage period under that plan with worked hours only.
You may buy into the plan of coverage you were eligible for in the prior coverage period atthe special buy-in rate per hour. For example, if you are in Plan I and you had worked atleast 570 hours, you could buy the 30 hours you were short (600 required – 570 worked)for the buy-in rate times 30. To buy into Plan II coverage, you must work at least 320hours in a work period. For the most up-to-date buy-in rate, contact the Fund Office.
Payment must be made in one lump sum. You have only until the end of April orOctober to choose this buy-in option. Otherwise, continuation coverage would beavailable under COBRA at COBRA rates. (See page 11 for information on COBRAContinuation Coverage.) If late hours are received and would bring you into 30 hoursshort, you would have 30 days from the date of notification to choose this buy-in option.
Special Rule for New Members
New members may buy into Plan II after working eight hours in the current work period.

An eligibility statement with the monthly cost will be mailed to you in March orSeptember (the end of the insured period) indicating the cost for coverage starting thefollowing month, the next coverage period. Be sure to keep your address current with theFund Office so you can receive this statement.
Banked Hours
Hours that were banked prior to August 1, 1989, may be drawn upon to maintain yourcoverage when you do not work the required number of hours in a work period foractive members. You will be permitted to use hours from your bank to continueeligibility, provided you worked some hours in covered employment during the previousor current work period. You must be eligible to buy into COBRA to exercise this option.
Banked hours are credited at $1.90, which was the actual dollar value of the contributionrate in effect at the time the hours were banked. Therefore, the total banked hours usedto maintain eligibility will reduce the actual cost of the insurance coverage.
✍ To use your banked hours, you must indicate your wishes on a COBRA form(continuation coverage) or send a letter of request to the Fund Office.
E L I G I B L E D E P E N D E N TS
When you become eligible for coverage in the New England Carpenters Health BenefitsFund, your eligible dependents are also eligible for coverage.
Plan’s Definition of Dependent
The term “dependent” means (1) your lawful spouse; (2) your unmarried children(including a legally adopted child) who are under 19 years of age; and your unmarriedchildren who are at least 19 but less than 24 years of age who are enrolled as full-timestudents in an accredited school, college or university, not employed on a full-time basisand dependent upon you for financial support.
If Your Child is Disabled
If an unmarried dependent child is incapable of self-sustaining employment because ofphysical handicap or mental retardation and he or she is dependent upon you forsupport and maintenance, his/her coverage will be continued provided his/her incapabilitycommenced prior to attaining age 19 or age 24 if a full-time student. You must submitproof of your dependent child’s incapability to the Fund Office on the later of 31 daysafter the date he/she attains 19 years of age or age 24 if a full-time student or 31 daysafter you are notified of his/her eligibility. Benefits will continue to be provided for yourchild as long as you remain covered under the Fund.
No person may be eligible for benefits both as a member and as a dependent.
Proof of the continued existence of such incapability shall be furnished to the FundOffice yearly.
The term “child” also includes a stepchild or foster child, provided the child dependsupon you for support and maintenance and has been reported to the Fund Office.
8
Proving Eligibility for
Dependents
You are required to furnishthe following documenta-tion for dependent cover-age if you have not alreadydone so:
• Marriage certificate fromCity Hall or Town Hall;
• Birth certificate documentshowing both parents’names, court document orwritten statement on let-terhead from appropriategovernmental agencyshowing legal guardian-ship and date of birth ofeach child;
• Divorce decree if applicable;
• Proof of a dependentchild’s attendance at anaccredited school or col-lege as a full-time studentupon attainment of age 19must be submitted to theFund Office twice eachyear, as directed by theFund Office, on an originalform which contains theaccredited institution’sseal. He or she must provide a letter from theregistrar.
The letter should include:
– Verification of his or herenrollment;
– The number of coursehours for which he or sheis enrolled; and
– The beginning and endingdates of the term.
9
When Coverage Ends
Your dependents’ eligibility for coverage will end on:
• The date your child or spouse no longer meets the definition of an eligible dependent under the Fund; or
• The date your eligibility ends.
I F YO U R C H I L D ’ S E L I G I B I L I T Y F O R B E N E F I TS C H A N G E S
If your child’s eligibility status changes, you must notify the Fund Office as soon as possible.
Your child may be eligible for COBRA Continuation Coverage for up to 36 months. Seepage 11 for more information.
E X T E N S I O N O F B E N E F I TS F O R TOTA L LY D I S A B L E D M E M B E R S
If you become totally disabled while covered for benefits under this Fund, you may beeligible for an extension of benefits for up to two consecutive coverage periods. Yourcoverage will be under the same Plan you had at the time of your disability, subject toproper documentation. This option is available only once per lifetime. If only one freecoverage period is required, the option for a second coverage period is voided. Contactthe Fund Office for an Extension of Benefits form.
If you are eligible for a Social Security Disability Pension, you may be eligible forcoverage under the Retiree Health Benefits Plan for up to 24 months or until you arecovered by Medicare, whichever comes first.
Widow(er) Extension
If a member is covered by this Fund under worked hours or buying into Plan I at the time of his or her death, the surviving spouse and eligible dependents will be covered by the Fund for a maximum of three additional years under Plan I. Coverage is providedat no premium cost, provided that the spouse and dependents have no other healthinsurance, including Medicare. However, if the member was buying into Plan II at thetime of his or her death, the surviving spouse and eligible dependents are only eligible for coverage under Plan II.
W H E N C OV E R AG E E N D S
Generally, your coverage under the New England Carpenters Health Benefits Fund will end:
• For Shop Employees, the first day of the following month in which you stop working in covered employment;
• The date you do not meet the requirements for eligibility; or• The date the Plan terminates.
What You Need to Do
If you are adopting a child,the following is needed:
• A copy of the birth certifi-cate once it is available;
• A copy of the paperworkfrom the adoption agencyshowing the date the childwas placed in the home.(Coverage for an adoptedchild will begin on the datethe child was placed in thehome.)
If you are the legalguardian, the following isneeded:
• A copy of the birth certificate;
• A copy of the court document stating that the member is the legalguardian of the child.(Coverage will begin onthe date of the legal document.)
If you have not adoptedthe child or do not havelegal guardianship and are only the stepparent by marriage, then the fol-lowing is needed:
• A copy of the birth certificate;
• A copy of the natural par-ent’s divorce decree, themedical insurance section,along with the front pagethat has the name of thedefendant and plaintiff’snames.
• A copy of the tax return.
See page 20 for more information.

R E T I R E E H E A LT H B E N E F I TS P L A N
If you retire on or after April 1, 1995, with a Service, Normal, Early or Disability Pensionand meet the Plan’s other eligibility requirements, you and your eligible dependents areeligible for the New England Carpenters Retiree Health Benefits Plan. There are fiverequirements:
• You must be eligible for five out of the past ten coverage periods, have 3,000 hours during the five-year period immediately prior to retirement and be covered by the Plan in the period immediately preceding your application for retiree coverage.
• You must have no other group health insurance, including Medicare.• You must share the cost of coverage with the Fund. Your monthly premiums will
increase from time to time.• You must obtain medical services from providers in the Carpenters Preferred Provider
Network unless you do not live within a 20-mile radius of the nearest networkprovider.
• You must obtain pre-certification for all inpatient hospital stays.
Continued Eligibility for Retirees
Eligibility to participate ends on the earlier of:
• The last day of the month when you do not pay the premium when required; • The date your pension benefit is suspended for any reason;• The date you become eligible under another group health plan;• The date you or your eligible dependent become entitled to Medicare; or• The date the Plan terminates.
Local 108 cannot participate in the Retiree Plan.
Eligibility for Widow(ers) and Dependent Children
If you were eligible for a Service, Normal, Early or Disability Pension from the NewEngland Carpenters Pension Fund at the time of your death, your widow(er) and eligibledependent children may continue coverage under the Retiree Health Plan on a self-payment basis. If a dependent child is covered under a member who is purchasing theRetiree Health Plan and the child reaches the age limit, the dependent is eligible to buyinto Plan II under COBRA.
10
What You Need To Do
If your child is no longereligible for coverage underthe Fund, he or she mayelect to continue coverageunder COBRA. You or yourchild must:
• Contact the Fund Officewithin 60 days of losingeligibility; and
• Enroll in COBRAContinuation Coverage.Failure to contact the FundOffice and provide noticeof the “Qualifying Event”(discussed in more detailon page 11) will result in aloss of rights to COBRA.
These same rules apply to a Spouse who losescoverage due to a separa-tion or divorce.
Continuing Your
Coverage Under COBRA
When your coverageunder this Fund ends, you may be eligible to continue some of thesame coverage you hadunder the Health BenefitsFund for a limited timeunder COBRA. For infor-mation about COBRAContinuation Coverage,see page 11.

11
C O B R A C O N T I N U AT I O N C OV E R AG E
If your coverage under the New England Carpenters Health Benefits Fund ends due to a“Qualifying Event” (see below), you and/or your covered dependents may be eligible tocontinue your health care coverage under the Consolidated Omnibus BudgetReconciliation Act of 1985 (COBRA).
By making monthly payments, you and/or your dependents may continue the samemedical, dental, vision and prescription drug coverage that you had before your coverageended. Your coverage can last for up to 18, 29 or 36 months, depending on theQualifying Event that resulted in your loss of coverage.
Qualifying Events
To be eligible to elect COBRA Continuation Coverage, you (as the member) and/or yourdependent(s) must lose coverage due to any one of the Qualifying Events, which arelisted in the first column in the table below. The last column indicates how individualsfind out that they’re eligible for continuation coverage, which are explained below.
• You and your dependents may continue certain medical benefits if your coverage ends due to a“Qualifying Event.”
• Your children are eligible to continue coverage under COBRA when they no longer satisfy theFund’s definition of eligible dependent because of age, marriage or student status.
• To keep your coverage under COBRA, you must make monthly payments to the Fund Office ontime. You are fully responsible for the payment of your benefits through COBRA.
CONTINUING YOUR COVERAGE
FA ST FAC TS :
Qualifying Event Who May Purchase Eligibility Notification Requirements
(Qualified Beneficiary)
Member terminated for Member, spouse and/or 18 months Fund Office will other than gross misconduct dependent children advise eligible participants (including retirement)
Member reduction in hours Member, spouse and/or 18 months Fund Office worked (making Member inel- dependent children igible for coverage or the same coverage under the Plan)
Member becomes Spouse and/or 36 months Fund Office will advise entitled to Medicare dependent children eligible participants when
member reaches 65. If member becomes eligible before 65, he or she must advise Fund Office
Member becomes Member, spouse 11 months in Member must advise eligible for disability through and/or children addition to the Fund Office Social Security 18 months
Death of Member Spouse and/or 36 months minus Family member must dependent children the number of notify Fund Office
months coveredsince the divorce
Member is divorced or legally Spouse and/or 36 months Member or Spouse must separated from spouse dependent children advise Fund Office so
notification can occur
Child ceases to be a Dependent child 36 months Member must advise dependent child under Fund Office so Plan definition notification can occur

Who May Elect COBRA?
Under the law, only “Qualified Beneficiaries” are entitled to elect COBRA ContinuationCoverage. A Qualified Beneficiary is any member, his or her spouse or dependent whowas covered by the New England Carpenters Health Benefits Fund when a QualifyingEvent occurs. A child who becomes a dependent child by birth, adoption or placementfor adoption with the Member during a period of COBRA Continuation Coverage is also a qualified beneficiary. However, a dependent purchasing COBRA who acquires a spouseduring COBRA Continuation Coverage is not a qualified beneficiary.
!! One or more of your family members may elect COBRA even if you do not.Additionally, one member may elect COBRA for all Qualified Beneficiaries. However, in order to elect COBRA Continuation Coverage, the members of the family musthave been covered by the Plan on the date of the Qualifying Event. A parent mayelect or reject COBRA Continuation Coverage on behalf of dependent children livingwith him or her.
How to Elect COBRA Continuation Coverage
✍ In order to elect COBRA Continuation Coverage, the Fund Office must be notifiedwhen you experience a Qualifying Event. You must notify the Fund Office within 60days from the date that the Qualifying Event occurs, or the date that you would losecoverage under the Fund because of the Qualifying Event, whichever is later. See thefollowing Notification Procedures.
✍ When the Fund Administrator receives notice of the Qualifying Event, he or she willmail you an election form, information about COBRA and the date on which yourcoverage will end.
Under the law, you and/or your covered dependents have 60 days from the later of the date:
• You would have lost coverage because of the Qualifying Event; or• You and/or your covered dependents received the election form and COBRA information.
If you and/or any of your covered dependents do not elect COBRA within 60 days of theQualifying Event (or, if later, within 63 days from the mailing date), you and/or yourcovered dependents will not have any group health coverage from this Fund after yourcoverage ends.
COBRA Notification Procedures
As a covered Member or Qualified Beneficiary you are responsible for providing the FundAdministrator with timely notice of certain qualifying events. You must provide the FundAdministrator notice of the following qualifying events:
• The divorce or legal separation of a covered Member from his or her spouse.• A beneficiary ceasing to be covered under the Plan as a dependent child of a member.• The occurrence of a second qualifying event after a Qualified Beneficiary has become
entitled to COBRA with a maximum of 18 (or 29) months. This second qualifyingevent could include a Member’s death, entitlement to Medicare, divorce or legalseparation or child losing dependent status.
12

13
In addition to these qualifying events, there are two other situations when a coveredMember or Qualified Beneficiary is responsible for providing the Fund Administratorwith notice within the timeframe noted in this section:
• When a Qualified Beneficiary entitled to receive COBRA coverage with a maximumof 18 months has been determined by the Social Security Administration to bedisabled. If this determination is made at any time during the first 60 days of COBRAcoverage, the Qualified Beneficiary may be eligible for an 11-month extension of the18 months maximum coverage period, for a total of 29 months of COBRA coverage.
• When the Social Security Administration determines that a Qualified Beneficiary isno longer disabled.
You must make sure that the Fund Administrator is notified of any of these fiveoccurrences listed above. Failure to provide this notice within the form andtimeframes described below may prevent you and/or your dependents from obtainingor extending COBRA coverage.
How Should a Notice Be Provided?
In order to provide the Fund notice of any of these five situations you must complete andsign the Fund’s “COBRA Notice Form for Covered Employees and Qualified Beneficiaries.” You can obtain a copy of the form by calling the Fund Office at (800) 344-1515.
Alternatively, you may send a letter to the Fund containing the following information:your name, for which of the five events listed above you are providing notice, the date ofthe event, the date in which the participant and/or beneficiary will lose coverage.
To Whom Should the Notice Be Sent?
Notice should be sent to the Fund at the following address:
Director and Field RepresentativeThe New England Carpenters Health Benefits FundP.O Box 7075Wilmington, MA 01887Phone: (800) 344-1515Fax: (978) 657-8724
When Should the Notice Be Sent?
If you are providing notice due to a divorce or legal separation, a dependent losingeligibility for coverage or a second qualifying event, you must send the notice no laterthan 60 days after the later of (1) the date upon which coverage would be lost under thePlan as a result of the qualifying event (2) the date of the qualifying event or (3) the dateon which the Qualified Beneficiary is informed through the furnishing of a summaryplan description or initial COBRA notice of the responsibility to provide the notice andthe procedures for providing this notice to the Fund Administrator.
If you are providing notice of a Social Security Administration determination of disability,notice must be sent no later than the end of the first 18 months of continuation coverage.
If you are providing notice of a Social Security Administration determination that you areno longer disabled, notice must be sent no later than 30 days after the later of (1) thedate of the determination by the Social Security Administration that you are no longerdisabled or (2) the date on which the Qualified Beneficiary is informed through thefurnishing of a summary plan description or initial COBRA notice of the responsibility toprovide the notice and the procedures for providing this notice to the FundAdministrator.
Who Can Provide a Notice?
Notice may be provided by the covered Member, Qualified Beneficiary with respect to the qualifying event, or any representative acting on behalf of the covered Member orQualified Beneficiary. Notice from one individual will satisfy the notice requirement forall related qualified beneficiaries affected by the same qualifying event. For example, if amember and his or her spouse and child are all covered by the Plan, and the child ceasesto become a dependent under the Plan, a single notice sent by the spouse would satisfythis requirement.
Where you or your dependents have provided notice to the Fund Administrator ofa divorce or legal separation, beneficiary ceasing to be covered under the Plan as adependent or a second qualifying event, but are not entitled to COBRA, the FundAdministrator will send you a written notice stating the reason why you are not eligiblefor COBRA.
Paying for COBRA Continuation Coverage
You are responsible for the entire cost of COBRA Continuation Coverage. When youand/or your dependents become eligible for this coverage, the Fund Administrator willnotify you of the COBRA premium amounts that you must pay.
Your COBRA premiums may be as high as 102% of the Plan’s cost, except in the case ofSocial Security disability. (See the section below entitled “COBRA Continuation Coveragefor Disabled Participants.”)
You must send the first COBRA payment to the Fund Office within 45 days from the dateon which the Fund Office receives your COBRA election form, as determined by postagecancellation. You must make payments so that coverage is continuous—there can be nolapse in coverage. If you choose COBRA within the election period but after the date onwhich your eligibility ended, you must pay the required COBRA premiums retroactivelyto cover the elapsed period.
Late COBRA Payments
Your monthly payments are due on the 1st day of each month. You will have 30 days in which to pay. Payments should be mailed to the Fund Office. If you do not makepayment by the end of the 30 days, your coverage will be cancelled retroactively to thelast day of the previous month and you will lose your right to continuation coverage.
14
Notify The Fund Office
You or a family membershould notify the FundOffice when anyQualifying Event occurs to avoid confusion overthe status of your healthcare in the event that your Employer does notprovide prompt or correctinformation.
What You Need To Do:
If you lose coverage due to a Qualifying Event:
• Inform the Fund Office of the Qualifying Event and request a COBRAelection form.
• Complete and mail backthe election form within 63 days of the date of the mailing, or 60 days ofthe date the QualifyingEvent occurred, which-ever is later.
• Make your first payment to the Fund Office within45 days from the date theFund Office receives yourCOBRA election form.
15
COBRA Continuation Coverage for Disabled Participants
If you are covered under COBRA for 18 months, and within the first 60 days of coverageyou (or your covered dependent) become disabled, you (and your Qualified Beneficiarieswho elected COBRA) may be eligible to continue your COBRA coverage for an additional11 months for a total of 29 months.
To be eligible, the Social Security Administration must make a formal determination thatyou (or your dependent) were disabled effective within the initial 60-day period of thestart of your COBRA coverage and therefore entitled to Social Security Disability incomebenefits. You (or your dependent) must notify the Fund Office of the Social Securitydetermination of disability by the end of the 18-month initial COBRA period if you wishto continue with the 11-month extension.
If you are eligible for the 11-month extension, your COBRA premiums may be as high as150% of the regular premiums for the additional 11 months of coverage.
This extended period of COBRA coverage will end on the earlier of:
• The last day of the month that occurs 30 days after Social Security has determined that you and/or your dependent(s) are no longer disabled;
• The end of the 29 months’ COBRA Continuation Coverage;• The date the disabled person becomes entitled to Medicare.
If you recover from your disability before the end of the initial 18 months of COBRAContinuation Coverage, you will not have the right to purchase extended coverage. Youmust notify the Fund Office within 30 days of:
• The date that you receive a final Social Security determination that you and/or your dependent(s) are no longer disabled; or
• The date that the disabled person becomes entitled to Medicare.
Multiple Qualifying Events While Covered Under COBRA
The maximum period of coverage under COBRA is 36 months, even if you experienceanother Qualifying Event while you’re already covered under COBRA. If you’re coveredunder COBRA for 18 months because of your termination of employment or reduction inhours, your affected spouse or dependent may extend coverage for another 18 months inthe event of your death or if:
• You get divorced or legally separated;• You become entitled to Medicare; or• Your child is no longer a dependent under the Fund’s definition.
For example, you stop working (the first COBRA-Qualifying Event), and you enroll yourselfand your dependents for COBRA Continuation Coverage for 18 months. Three months afteryour COBRA Continuation Coverage begins, your child turns 19 and no longer qualifies as adependent child under the Fund’s definition. Your child then can continue COBRA coverageseparately for an additional 33 months, for a total of 36 months’ COBRA Continuation Coverage.

You, as the member, are not entitled to COBRA Continuation Coverage for more than atotal of 18 months if your employment is terminated or you have a reduction in hours(unless you are entitled to additional COBRA Continuation Coverage on account ofdisability). Therefore, if you experience a reduction in hours followed by a terminationof employment, the termination of employment is not treated as a second QualifyingEvent and you may not extend your coverage.
Coverage for Your Dependents if You’re Enrolled in Medicare
If you are entitled to or enrolled in Medicare and you have a termination of employmentor reduction in hours, your eligible dependents would be entitled to COBRA for a periodof 18 months (29 months if the 11-month Social Security Disability extension applies)from the date of your termination of employment or reduction in hours or 36 monthsfrom the date you became entitled to Medicare, whichever is longer.
Special COBRA Enrollment Rights
If you marry, have a newborn child, adopt a child or have a child placed with you foradoption while you are enrolled in COBRA, you may enroll that spouse or child forcoverage for the balance of the period of COBRA Continuation Coverage. You mustenroll your new dependent within 31 days of the marriage, birth, adoption or placementfor adoption, with proper documentation.
In addition, if you are enrolled for COBRA Continuation Coverage and your spouse ordependent child loses coverage under another group health plan, you may enroll thatspouse or child for coverage for the balance of the period of COBRA within 31 days afterthe termination of the other coverage.
To be eligible for this special enrollment right, your spouse or dependent child must havebeen eligible for coverage under the terms of the Plan but declined when enrollment waspreviously offered because they had coverage under another group health plan or hadother health insurance coverage, with proper documentation.
Confirmation of Coverage to Health Care Providers
Under certain circumstances, federal rules require the Fund to inform your physician andhealth care providers as to whether you have elected and/or paid for COBRAContinuation Coverage. This rule only applies in certain situations where the physicianor provider is requesting confirmation of coverage and you are eligible for, but have notyet elected, COBRA coverage, or you have elected COBRA coverage but have not yet paidfor it.
Termination of COBRA Continuation Coverage
COBRA Continuation Coverage will terminate on the last day of the maximum period ofcoverage unless it is cut short for any of the following reasons:
• You do not make all required payments on time;
• The person receiving the coverage becomes covered by another group health planthat does not contain any legally applicable exclusion or limitation with respect topre-existing conditions that the covered person may have;
16
17
• The person receiving the coverage becomes entitled to Medicare;
• The Plan terminates its group health plan and no longer provides group healthinsurance coverage to its members; or
• The Employer that employed you prior to the Qualifying Event has stoppedcontributing to the Plan; and
• The Employer establishes one or more group health plans covering a significantnumber of the employer’s employees formerly covered under this Plan; or
• The Employer starts contributing to another multiemployer plan that is a grouphealth plan.
If continuation coverage is terminated before the end of the maximum coverage period,the Fund Administrator will send you a written notice as soon as practicable followingthe Fund Administrator’s determination that continuation coverage will terminate. TheNotice will set out why continuation coverage will be terminated early, the date oftermination, and your rights, if any, to alternative individual or group coverage.
☎ If you have questions about COBRA Continuation Coverage, contact the Fund Officeat (800) 334-1515.
Additional COBRA Election Period and Tax Credit in Cases of
Eligibility for Benefits Under the Trade Act of 1974
If you are certified by the U.S. Department of Labor (DOL) as eligible for benefits underthe Trade Act of 1974, you may be eligible for both a new opportunity to elect COBRAand an individual Health Insurance Act Credit. If you and/or your dependents did notelect COBRA during your election period, but are later certified by the DOL for TradeAct benefits or receive pensions managed by the Pension Benefit Guaranty Corporation(PBGC), you may be entitled to an additional 60-day COBRA election period beginningon the first day of the month in which you were certified. However, in no event wouldthis benefit allow you to elect COBRA later than six months after your coverage endedunder the Plan.
Also under the Trade Act, eligible individuals can either take a tax credit or get advancepayment of 65% of premiums paid for qualified health insurance, including continuationcoverage. If you have questions about these tax provisions, you may call the Health CareTax Credit Customer Contact Center toll-free at 1-866-628-4282. TTD/TTY callers maycall toll-free at 1-866-626-4282. More information about the Trade Act is also available atwww.doleta.gov/tradeact/2002act_index.asp. The Fund Administrator may also be able toassist you with your questions.
Keep the Fund Informed of Address Changes
In order to protect your family’s rights, you should keep the Fund Administratorinformed of any changes in the addresses of your family members. You should also keepa copy, for your records, of any notices that you send to the Fund Administrator.

18
Consequences of Failing to Elect COBRA
In considering whether to elect continuation coverage, you should take into account thata failure to continue your group health coverage will affect your future rights underfederal law. First, you can lose the right to avoid having pre-existing exclusions appliedto you by other group plans if you have more than a 63-day gap in health coverage, andelection of continuation coverage may help you prevent such a gap. Second, you will losethe guaranteed right to purchase individual health insurance policies that do not imposethese pre-existing condition exclusions if you do not get continuation coverage for themaximum time available to you. Finally, you should take into account that you havespecial enrollment rights under federal law. You have the right to request specialenrollment in another group health plan for which you are otherwise eligible (such as aplan sponsored by your spouse’s employer) within 30 days after your group healthcoverage ends because of the qualifying events listed above. You will also have the samespecial enrollment right at the end of continuation coverage if you get continuationcoverage for the maximum time available to you.
Certificate of Creditable Coverage
When your coverage ends, the Fund Office will mail you and/or your dependents aCertificate of Creditable Coverage that indicates the period of time that you were coveredunder the New England Carpenters Health Benefits Fund.
If you become eligible for coverage under another group health plan within 62 days ofthe date you lose coverage under the New England Carpenters Health Benefits Fund, thiscertificate may be necessary if your new group health plan has pre-existing conditionlimitations that apply to you.
The Fund Office will mail this certificate to you shortly after they learn that yourcoverage has ended. You may request a certificate from the Fund Office within two yearsfrom the date your coverage ended. To request a Certificate of Creditable Coverage,contact:
Director and Field RepresentativeNew England Carpenters Health Benefits FundP.O. Box 7075Wilmington, MA 01887Phone: (800) 344-1515Fax: (978) 657-8724
LIFE EVENTS
Your benefits are designed to adapt to your needs at different stages of your life. Thissection describes how your coverage is affected when you experience certain “life events”and what you must do to make sure you get the most from your coverage.
19
• You should notify the Fund Office as soon as possible if you experience a life event that may affect your coverage.
• You and/or your dependents may qualify to continue coverage under COBRA in the event of a loss ofeligibility, divorce, or your termination or reduction of your work hours.
• If you become disabled, you may be entitled to receive an extension of coverage for up to 12 months.
The following life events may affect your coverage:
Moving to a new address Entering active military service Getting married Becoming disabled Having a baby RetiringTaking family medical leave Becoming eligible for Medicare Adopting a child Death Getting divorced
If you have a change of address, contact the Fund Office for a change of address form as soon as possible to make sure your records are up to date and to avoid a delay inpayment of claims.
If you legally marry, your spouse is eligible to receive dependent benefits under the NewEngland Carpenters Health Benefits Fund.
What You Need To Do
If you get married, you should provide the Fund Office with the following information:
• A copy of your marriage certificate, available from the town or city hall where you were married;
• Your spouse’s date of birth and Social Security number; and
• A copy of your spouse’s medical insurance information, if he or she is covered under anothergroup insurance plan.
✍ Once you provide the required information, your spouse is eligible for coverageunder the Fund as of the date of your marriage. If you wish to name your spouse asyour beneficiary for your life insurance benefit or accidental death and dismember-ment benefit, contact the Fund Office for “Change of Beneficiary” form.
If your spouse is covered under another group medical plan, you must report this othercoverage to the Fund Office. The amount of benefits payable under this Fund will becoordinated with your spouse’s other coverage. Benefits for your spouse under this Fundwill be paid after any benefits are payable from your spouse’s plan. For more information,see “Coordination of Benefits” on page 54.
FA ST FAC TS :
I F YO U M OV E
I F YO U G E T M A R R I E D

If You Acquire a Child Through Marriage
Notify the Fund Office if you are planning to cover a stepchild under this Fund. Youmust provide certain information in order to cover your stepchild:
1. If the natural parents were married, the following is needed:• The child’s birth certificate;• The child’s Social Security card;• The divorce decree; and• A joint tax return showing that the Member claims the child as a dependent.
2. If the natural parents were never married, the following is needed:• The child’s birth certificate;• The child’s Social Security card;• A joint tax return showing that the Member claims the child as a dependent; and• The court order. If no court order exists, you must provide a written statement
indicating whether the natural mother has insurance for the child(ren) andwhether the natural father has insurance for the child(ren).
3. If one of the natural parents has passed away, the following is needed:• The child’s birth certificate; • The child’s Social Security card; • A joint tax return showing that the Member claims the child as a dependent; and• A copy of the death certificate of the natural parent.
Once your child is born, notify the Fund Office as soon as possible. You will need toprovide certain information in order to have your child covered by this Fund.
What You Need To Do
If you have a baby, you should provide the Fund Office with the following information:
• A copy of the baby’s birth certificate listing both parents;
• A copy of the child’s Social Security card; and
• A copy of your baby’s other medical insurance information if he or she is covered under another group insurance plan.
The Health Benefits Fund covers expenses related to maternity, prenatal care and childwellness exams. For information, see pages 30-34.
20
I F YO U H AV E A B A BY
If you adopt a child, contact the Fund Office. Your child will be covered as of theeffective date of the adoption placement as long as you are responsible for health carecoverage and your child meets the Fund’s definition of a dependent child (see page 8).
What You Need To Do
If you need to add a child to your coverage, you must provide the Fund Office with the following information:
• A copy of the child’s birth certificate, when it becomes available;
• A copy of the child’s Social Security card, when it becomes available;
• A copy of the Adoption Agency paperwork indicating the specific date the child was placed in your home; and
• A copy of the initial adoption paperwork, when it becomes available.
Legal Guardianship
If you become a child’s Legal Guardian, coverage for the child will be effective as of thedate specified on court documents. You must provide the Fund Office with:
• A copy of the child’s birth certificate;• A copy of the child’s Social Security card, when available;• A copy of the court document indicating that you as the
Member are the legal guardian of the child.
Family Medical Leave Act
If you take leave in certain circumstances such as serious illness, birth of a child, orcaring for a seriously ill parent or spouse, your employer may be obligated to continuecontributions on your behalf under the Family Medical Leave Act (FMLA). Talk to youremployer for details.
If you divorce from your spouse, notify the Fund Office as soon as possible. The Planwill cover your ex-spouse as required by the divorce, but under no circumstances will thePlan cover both the ex-spouse and a current spouse.
What You Need To Do
If you get legally divorced, you must provide the Fund Office with the following information:
• A copy of your divorce decree; and
• If you have children and you do not have custody, a copy of any Qualified Medical Child Support Order (QMCSO), if applicable.
If your spouse wants to continue coverage, he or she must:
• Contact the Fund Office; and
• Enroll in COBRA Continuation Coverage.
Your former spouse may continue coverage under COBRA for up to 36 months. He orshe must notify the Fund Office within 60 days of the day that the divorce becomes final.The Fund Office will then send the COBRA Notice and enrollment information to yourformer spouse. For more information, see page 11.
21
I F YO U A D O P T A C H I L D
I F YO U D I VO R C E
Under certain situations, the Fund is required to continue to provide coverage to adivorced spouse of a Member who continues to maintain eligibility and coverage underthe Plan. The Fund will only maintain coverage for a former spouse if presented with acourt separation or alimony agreement stipulating that the Member is required to providehealth coverage for the former spouse. A continuation of benefits under this Plan to aformer spouse shall only be maintained until the termination date set forth in the Orderor the date the Member or spouse remarries, whichever occurs first. Coverage for theformer spouse will terminate when coverage for the Member terminates.
Qualified Medical Child Support Order (QMCSO)
A Qualified Medical Child Support Order (QMCSO) is a court order, judgment or decreethat recognizes that an alternative recipient may be entitled to benefits under this Fund inthe event of a divorce or other family law action. Orders must be submitted to the FundOffice to determine whether the order is a QMCSO under federal law. As required under theEmployee Retirement Income Security Act (ERISA), this Fund will recognize a QMCSO that:
• Provides for health coverage to the child(ren) under state domestic relations law (including a community property law); and
• Relates to benefits under this Fund.
Please notify the Fund Office if your situation involves a QMCSO for information abouthow these orders are handled. Or, you and/or your beneficiary(ies) can obtain, withoutcharge, a copy of the Plan’s QMCSO procedures from the Fund Administrator.
If you are on active duty for 31 days or less, you will continue to receive health carecoverage for up to 31 days, according to the Uniformed Services Employment andReemployment Rights Act of 1994 (USERRA).
If you are on duty for more than 31 days, USERRA permits you to continue medical anddental coverage under COBRA (see page 11) for you and your dependents at your ownexpense for up to 18 months. COBRA will be offered after your active eligibility andcoverage runs out. Your dependent(s) may be eligible for health care coverage underTRICARE. The New England Carpenters Health Benefits Fund will coordinate coveragewith TRICARE, as explained on page 56.
Coverage under this Fund will not be offered for any illness or injury determined by theSecretary of Veterans Affairs to have incurred in, or been aggravated during, performanceof service in the uniformed services. The uniformed services and the Department ofVeterans Affairs will provide care for service-connected disabilities.
When you are discharged (not less than honorably) from “service in the uniformedservices,” your full eligibility will be reinstated on the day you return to the Union Officefor work with a Contributing Employer, provided that you return within:
• Ninety (90) days from the date of discharge if the period of service was more thanone hundred eighty days; or
• Fourteen (14) days from the date of discharge if the period of service was 31 days ormore but less than one hundred eighty days; or
22
I F YO U E N T E R AC T I V EM I L I TA R Y S E R V I C E
• At the beginning of the first full regularly scheduled working period on the firstcalendar day following discharge (plus travel time and an additional eight hours) ifthe period of service was less than thirty-one (31) days.
• You will be granted the same plan of coverage you had when you began active duty.
If you are hospitalized or convalescing from an injury caused by active duty, these timelimits are extended up to two years.
What You Need To Do:
If you are called to military leave, you should:
• Notify your employer and the Fund Office; and
• Make any required self-payments to the Fund Office to continue your coverage.
If you become disabled and cannot work, you may be eligible for a Weekly Accident andSickness Benefit for up to 26 weeks. See page 51 for more information.
Extension of Coverage for Totally Disabled Members
If you are totally disabled due to an injury or illness and your coverage under the HealthBenefits Fund ends, you will be eligible to extend coverage for up to 12 consecutivemonths (two coverage periods) from the date your coverage ends. This is a once-per-lifetime benefit. For more information, see page 9.
If you or your covered spouse become eligible for Social Security Retirement Benefits atage 65, you are also eligible for Medicare. Medicare is the federally sponsored health careprogram consisting of hospital insurance (Part A) and supplementary medical insurance(Part B).
You should enroll in Medicare Parts A and B as soon as you are eligible—three monthsbefore your 65th birthday or in certain cases when you become disabled—in order toavoid a gap in coverage.
To Enroll in Medicare:
• Visit your local Social Security Office;
• Call 1-800-MEDICARE (1-800-633-4227); or
• Go to the Medicare website at www.medicare.gov.
If you remain actively employed beyond age 65, you will continue to receive coverageprovided you work the required number of hours. You (and your spouse) may elect toparticipate on a self-pay basis in the group Medicare supplemental plan, providedthrough the Fund. This supplemental plan is Blue Cross Blue Shield Medex Gold, whichincludes prescription drug coverage.
For information about how your benefits are paid through the New England CarpentersHealth Benefits Fund when you are enrolled in Medicare, see page 55.
23
I F YO U B E C O M E D I S A B L E D
I F YO U B E C O M E E L I G I B L EF O R M E D I C A R E
In the event of your death from any cause while you’re covered under Plan I or Plan II,the Fund may provide an extension of health benefits at no cost to your surviving spouseand children for a period of up to three years. This extended coverage will be available ifthese family members have no other health coverage. Coverage for survivors is providedunder the same Plan that you were covered under at the time of your death. See page 10for more information.
✍ Your designated beneficiary must provide a certified copy of the death certificate inorder to receive a benefit.
What Your Beneficiary Needs To Do:
In the event of your death, your spouse or beneficiary must:
• Notify the Fund Office;
• Provide the Fund Office with an original copy of your death certificate; and
• Apply for your life insurance benefit (and AD&D benefit, if applicable).
24
U P O N YO U R D E AT H
YOUR MEDICAL PLAN
The New England Carpenters Health Benefits Fund provides a comprehensive medicalplan with coverage for office visits, hospitalization and surgery, home health care, mentalhealth and substance abuse treatment.
25
• If you are covered under Plan I or Plan II, as an active member or dependent, you may visit any physician you’d like, including a physician in or out of the PPO.
• If you are in the Retiree Plan, you must use a physician in the PPO to receive benefits, unless you live outside of a 20-mile radius of a PPO provider.
• Before any hospital admission, you must notify the Fund’s managed health care program, for pre-approval.
• Your hours worked determine which Plan you’re eligible for. (Refer to page 6 for more information.)
Plans I and II offer a broad range of medical services. You have the freedom to visit anyprovider you wish, either one that participates in the Plan’s Preferred ProviderOrganization (PPO) network, or an out-of-network provider. Plans I and II offer coverageboth in and out-of-network; however, you’ll save money for you, your family and for theFund if you use a provider in the PPO. For a summary of the benefits offered, refer tothe Schedule of Benefits on pages 71-77.
The Retiree Plan is a self-pay plan for retirees and their dependents. Coverage isprovided when services are obtained only from a network (PPO) provider. For asummary of the benefits offered, refer to the Schedule of Benefits on pages 78-79.
L I F E T I M E M A X I M U M P L A N B E N E F I T
The Lifetime Maximum amount that the Fund will pay toward eligible expenses percovered individual per lifetime is $1,000,000 if the Member or eligible dependent iscovered under Plan I or the Retiree Plan, or $500,000 if covered under Plan II.
Automatic Reinstatement of Lifetime Maximum Plan Benefit
Each year, the amount of expenses that you or your dependents incur during theprevious year is added back to the Lifetime Maximum Plan benefit—up to $50,000 forPlan I and up to $10,000 for Plan II. Note that the total maximum can never exceed$1,000,000 for Plan I or $500,000 for Plan II. Automatic reinstatement can apply if thereis a minimum of one benefit cent remaining at the end of the calendar year.
The Lifetime Maximum Plan Benefit is separate among all three plan options per coveredindividual. For example, if a covered individual switches between Plan II and Plan I andthen to the Retiree Plan, each Plan has a separate maximum benefit.
Preferred Provider Organization
The Fund contracts with CCN, and pays a monthly fee for access to its network ofdoctors, hospitals and other health care providers that contract with the CCN PPO.
FA ST FAC TS :
Using the PPO provides savings and convenience to you, your family and the Fund.When you use a PPO:
• The provider bills the Fund directly; and• Just one claim form is required each calendar year for each family member.
Your Share of the Cost
To help cover health care expenses, you are responsible for sharing some of the cost forservices. You are responsible for:
• Copayments;• The calendar year deductible;• Your coinsurance; and• Charges (if any) above the Reasonable and Customary amount
if you obtain services outside of the PPO network.
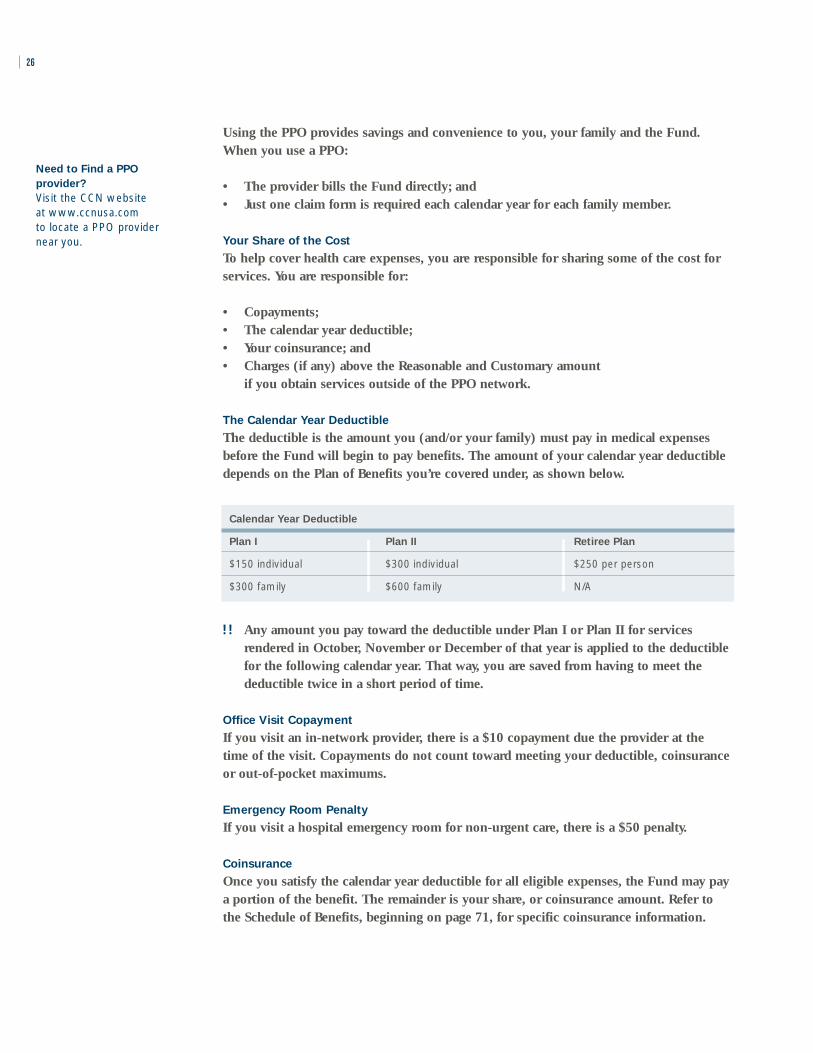
The Calendar Year Deductible
The deductible is the amount you (and/or your family) must pay in medical expensesbefore the Fund will begin to pay benefits. The amount of your calendar year deductibledepends on the Plan of Benefits you’re covered under, as shown below.
Calendar Year Deductible
Plan I Plan II Retiree Plan
$150 individual $300 individual $250 per person
$300 family $600 family N/A
!! Any amount you pay toward the deductible under Plan I or Plan II for servicesrendered in October, November or December of that year is applied to the deductiblefor the following calendar year. That way, you are saved from having to meet thedeductible twice in a short period of time.
Office Visit Copayment
If you visit an in-network provider, there is a $10 copayment due the provider at thetime of the visit. Copayments do not count toward meeting your deductible, coinsuranceor out-of-pocket maximums.
Emergency Room Penalty
If you visit a hospital emergency room for non-urgent care, there is a $50 penalty.
Coinsurance
Once you satisfy the calendar year deductible for all eligible expenses, the Fund may paya portion of the benefit. The remainder is your share, or coinsurance amount. Refer tothe Schedule of Benefits, beginning on page 71, for specific coinsurance information.
26
Need to Find a PPO
provider?
Visit the CCN website at www.ccnusa.com to locate a PPO providernear you.

Reasonable and Customary Charges
A Reasonable and Customary (R&C) charge is the “going rate,” as determined by thePlan based on published guidelines, for a particular medical service or supply in aspecific geographic area. If your health care provider charges more than the R&C rate fora particular service, you will be responsible for paying that additional amount. Forexample, if your doctor charges $500 for a service, but the R&C charge is $475, you willbe responsible for paying $25 in addition to your coinsurance.
Out-of-Pocket Maximums
The Fund has limits on the amount that you must pay out of your own pocket foreligible medical expenses (your coinsurance and deductibles) each year. After you’vereached that limit, the Fund will pay 100% of your eligible medical expenses for theremainder of the calendar year, up to the Lifetime Maximum.
Out-of-Pocket Maximum
Plan I Plan II Retiree Plan
$1,500 per person $3,000 per person $3,000 per person
Coinsurance for mental health or alcohol/substance abuse inpatient and outpatientservices does not apply toward the out-of-pocket maximum per calendar year.
M A N AG E D H E A LT H C A R E P R O G R A M — P R E A U T H O R I Z AT I O N
You or your medical provider must contact Hines & Associates in advance if you aregoing to be admitted to the hospital for any reason or will receive home health careservices or hospice care upon discharge from an inpatient stay. The Hines & Associatesprovider will contact your doctor and evaluate your proposed treatment needs andmedical care standards in your community.
What Services Require Preauthorization?
Contact Hines & Associates at 1-800-944-9401 for authorization before you receive any of the following treatments or services:
• Inpatient hospitalization;• Certain out-patient surgeries;• Home health care services; or• Hospice care.
27

Preauthorization for Hospitalization
The managed health care program helps the Health Benefits Fund keep down the cost ofa hospital admission and helps you to make better decisions when you need care. Thisprogram is mandatory for all eligible Members and dependents under all Plans ofBenefits. It is your responsibility to contact Hines & Associates before any inpatienthospitalization. If you do not receive prior authorization for any hospital admission, yourhospitalization benefit will be reduced by $500.
Precertification Requirement for Outpatient Surgical Procedures
Hines & Associates must be contacted to Pre-certify the Outpatient Surgical Procedureslisted below:
• EVLT (Endovenous Laser Therapy) for Varicose Veins• Septoplasty• Blepharoplasty• Breast Reduction• Abdominoplasty (Panniculectomy)• Biopsy• LeForte Osteotomy• UPPP (Uvulopalatopharyngoplasty)
The following is an example of the medical information Hines & Associates may request:
• Clinical History• Office Notes• Photos
This is only a partial list of procedures that need precertification and medical informationHines & Associates may require. Please contact the Fund office for more information.
What You Need To Do:
Contact Hines & Associates by calling 1-800-944-9401 for authorization prior to yourinpatient Hospitalization.
Make sure you have the following information available:
• Name and Social Security number of the patient;• Name and Social Security number of the covered Member if different
from the patient;• Date of proposed admission;• Name, address and telephone number of the attending physician; and• Name, address and telephone number of the hospital.
You will be notified in writing of the authorization. If you have not received a writtenauthorization by the day of your admission, call Hines & Associates.
28

29
Emergency Admission Review Procedure
If you have a medical emergency, you (or a family member) must notify Hines &Associates within 24 hours of your admission. Show your insurance identification card toyour doctor and the admissions office of the hospital. For your convenience, Hines &Associates phone number is printed on your card. Failure to notify Hines & Associateswill result in a $500 penalty.
What’s Covered
The New England Carpenters Health Benefits Fund provides eligible Members and their dependents with a comprehensive plan of benefits. Coverage includes office visits,hospitalization and surgery, wellness benefits, substance abuse and mental healthtreatment, coverage for prescription drugs, dental care (Plan I only) and vision care. The benefits are described in more detail on the following pages of this book.
For more information about what’s covered under your Plan of Benefits, refer to theSchedule of Benefits on pages 71-79.
What’s Not Covered
A comprehensive listing of the Fund’s general exclusions are listed on page 52 and 53.
30 WELLNESS BENEFITS
A N N U A L P H YS I C A L E X A M S
You and your spouse are entitled to one physical exam per calendar year, up to amaximum of $150 for Plan I, $75 for Plan II and $100 for the Retiree Plan.
Flu shots can be considered under this benefit if the available dollars are not exhausted.Any additional charges such as laboratory and/or x-ray charges that exceed the maximumamount the Plan will pay will be your financial responsibility.
A N N U A L PA P T E STS A N D M A M M O G R A M S
Annual Pap tests and mammograms are covered as a sickness benefit and are not subjectto the maximum for the routine physical exam.
W E L L- C H I L D E X A M S
Plan I
Your children are covered for routine well-child exams at 100% of charges after a $10copayment from birth up through age five. Your children age six and older are covered at100% for annual physical exams to a maximum of $70 per calendar year until they turn19 (or through age 23 if a full-time student).
Plan II
Your children through age five only are covered at 100% with a $10 copayment forannual physical exams when network providers are used. Well-child exams for childrenaged six or older are not covered under Plan II.
Retiree Plan
Your children in the Retiree Plan are not covered for well-child exams.
Refer to the Schedule of Benefits on pages 71-79 for more information.
31HOSPITALIZATION AND SURGERY
The New England Carpenters Health Benefits Fund provides hospitalization and surgerycoverage for you and your eligible family members. Your specific coverage depends onyour Plan of Benefits and whether you use a hospital and/or a surgeon in the PPO network.
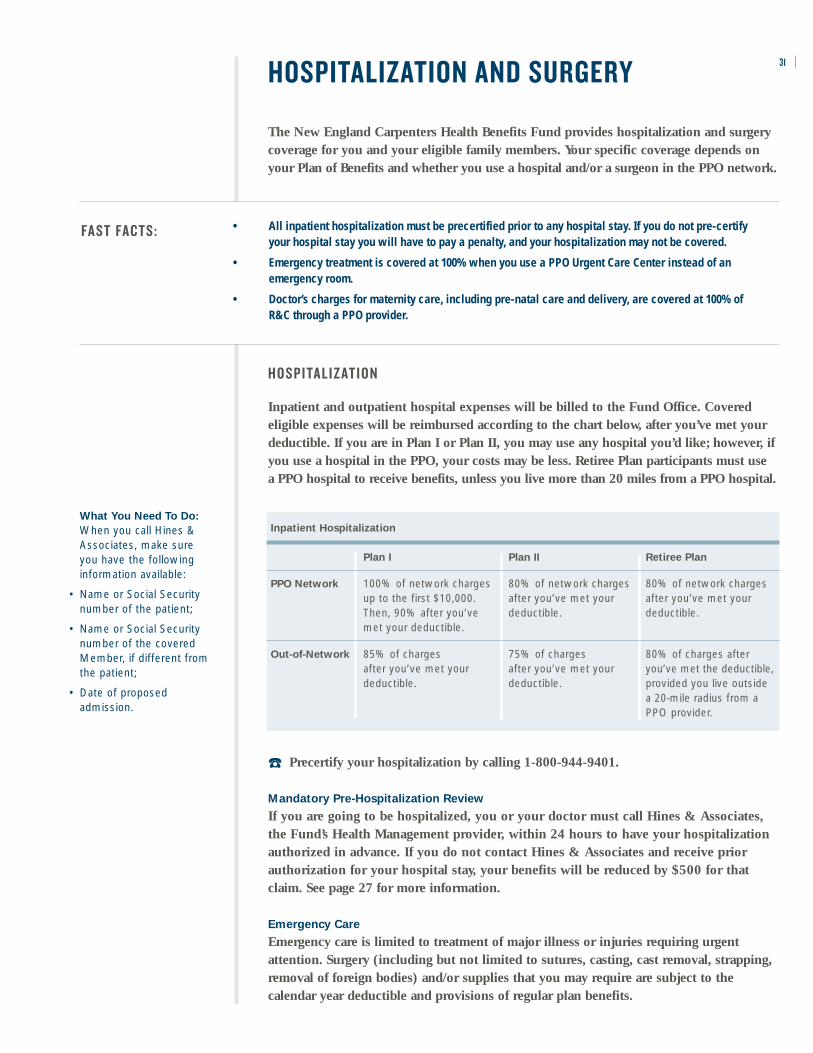
H O S P I TA L I Z AT I O N
Inpatient and outpatient hospital expenses will be billed to the Fund Office. Coveredeligible expenses will be reimbursed according to the chart below, after you’ve met yourdeductible. If you are in Plan I or Plan II, you may use any hospital you’d like; however, ifyou use a hospital in the PPO, your costs may be less. Retiree Plan participants must use a PPO hospital to receive benefits, unless you live more than 20 miles from a PPO hospital.
• All inpatient hospitalization must be precertified prior to any hospital stay. If you do not pre-certify your hospital stay you will have to pay a penalty, and your hospitalization may not be covered.
• Emergency treatment is covered at 100% when you use a PPO Urgent Care Center instead of anemergency room.
• Doctor’s charges for maternity care, including pre-natal care and delivery, are covered at 100% of R&C through a PPO provider.
FA ST FAC TS :
Inpatient Hospitalization
Plan I Plan II Retiree Plan
PPO Network 100% of network charges 80% of network charges 80% of network charges up to the first $10,000. after you’ve met your after you’ve met your Then, 90% after you’ve deductible. deductible. met your deductible.
Out-of-Network 85% of charges 75% of charges 80% of charges after after you’ve met your after you’ve met your you’ve met the deductible, deductible. deductible. provided you live outside
a 20-mile radius from a PPO provider.
☎ Precertify your hospitalization by calling 1-800-944-9401.
Mandatory Pre-Hospitalization Review
If you are going to be hospitalized, you or your doctor must call Hines & Associates, the Fund’s Health Management provider, within 24 hours to have your hospitalizationauthorized in advance. If you do not contact Hines & Associates and receive priorauthorization for your hospital stay, your benefits will be reduced by $500 for that claim. See page 27 for more information.
Emergency Care
Emergency care is limited to treatment of major illness or injuries requiring urgentattention. Surgery (including but not limited to sutures, casting, cast removal, strapping,removal of foreign bodies) and/or supplies that you may require are subject to thecalendar year deductible and provisions of regular plan benefits.
What You Need To Do:
When you call Hines & Associates, make sure you have the followinginformation available:
• Name or Social Securitynumber of the patient;
• Name or Social Securitynumber of the coveredMember, if different fromthe patient;
• Date of proposed admission.
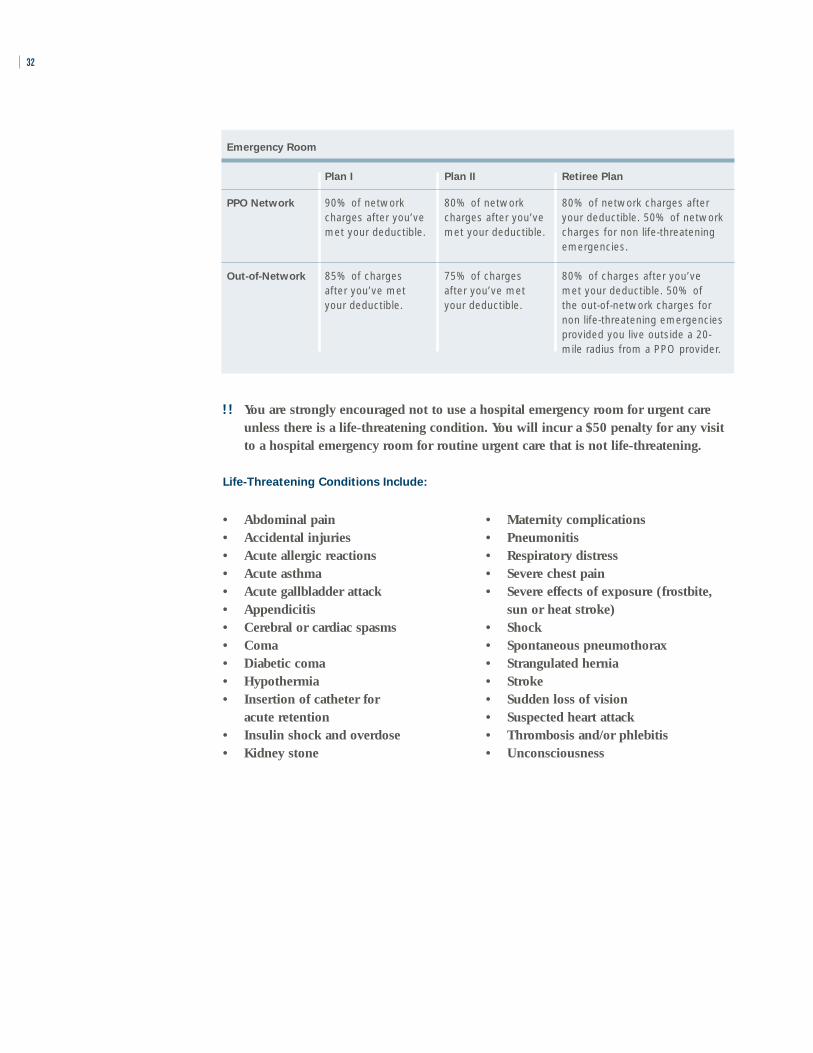
!! You are strongly encouraged not to use a hospital emergency room for urgent careunless there is a life-threatening condition. You will incur a $50 penalty for any visitto a hospital emergency room for routine urgent care that is not life-threatening.
Life-Threatening Conditions Include:
32
Emergency Room
Plan I Plan II Retiree Plan
PPO Network 90% of network 80% of network 80% of network charges after charges after you’ve charges after you’ve your deductible. 50% of network met your deductible. met your deductible. charges for non life-threatening
emergencies.
Out-of-Network 85% of charges 75% of charges 80% of charges after you’ve after you’ve met after you’ve met met your deductible. 50% of your deductible. your deductible. the out-of-network charges for
non life-threatening emergencies provided you live outside a 20-mile radius from a PPO provider.
• Abdominal pain• Accidental injuries• Acute allergic reactions• Acute asthma• Acute gallbladder attack• Appendicitis• Cerebral or cardiac spasms• Coma• Diabetic coma• Hypothermia• Insertion of catheter for
acute retention• Insulin shock and overdose• Kidney stone
• Maternity complications• Pneumonitis• Respiratory distress• Severe chest pain• Severe effects of exposure (frostbite,
sun or heat stroke)• Shock• Spontaneous pneumothorax• Strangulated hernia• Stroke• Sudden loss of vision• Suspected heart attack• Thrombosis and/or phlebitis• Unconsciousness
33
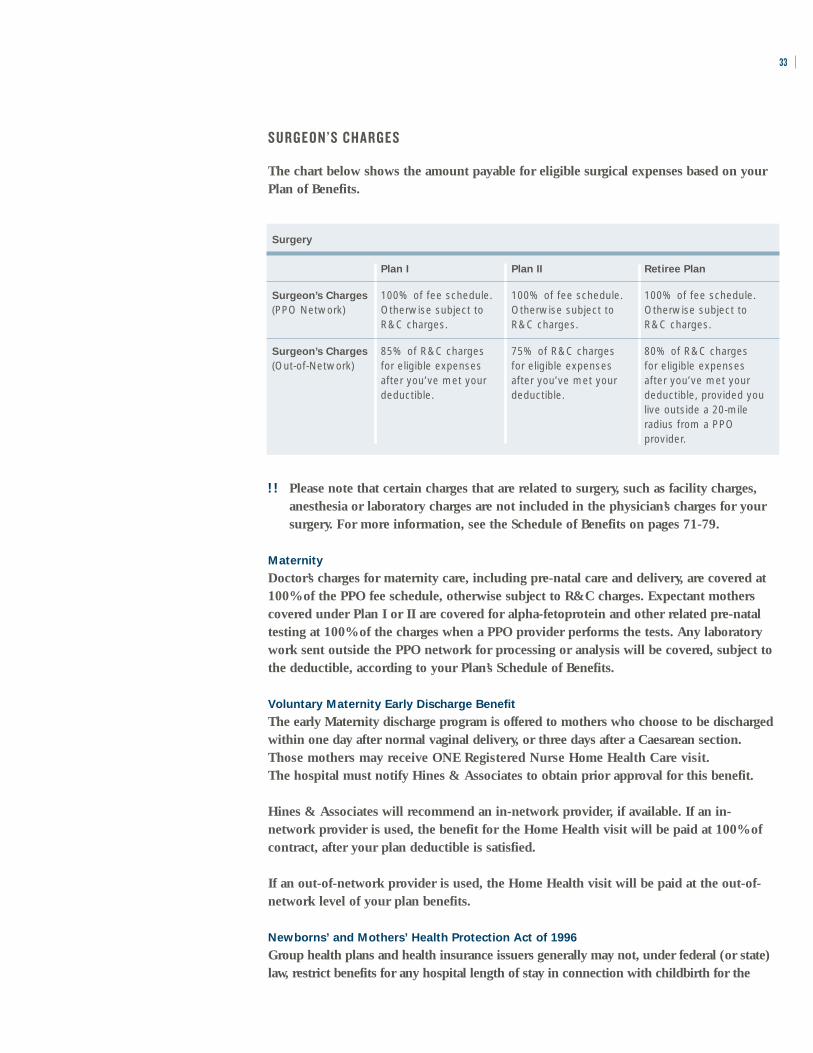
S U R G E O N ’ S C H A R G E S
The chart below shows the amount payable for eligible surgical expenses based on yourPlan of Benefits.
!! Please note that certain charges that are related to surgery, such as facility charges,anesthesia or laboratory charges are not included in the physician’s charges for yoursurgery. For more information, see the Schedule of Benefits on pages 71-79.
Maternity
Doctor’s charges for maternity care, including pre-natal care and delivery, are covered at100% of the PPO fee schedule, otherwise subject to R&C charges. Expectant motherscovered under Plan I or II are covered for alpha-fetoprotein and other related pre-nataltesting at 100% of the charges when a PPO provider performs the tests. Any laboratorywork sent outside the PPO network for processing or analysis will be covered, subject tothe deductible, according to your Plan’s Schedule of Benefits.
Voluntary Maternity Early Discharge Benefit
The early Maternity discharge program is offered to mothers who choose to be dischargedwithin one day after normal vaginal delivery, or three days after a Caesarean section. Those mothers may receive ONE Registered Nurse Home Health Care visit. The hospital must notify Hines & Associates to obtain prior approval for this benefit.
Hines & Associates will recommend an in-network provider, if available. If an in-network provider is used, the benefit for the Home Health visit will be paid at 100% ofcontract, after your plan deductible is satisfied.
If an out-of-network provider is used, the Home Health visit will be paid at the out-of-network level of your plan benefits.
Newborns’ and Mothers’ Health Protection Act of 1996
Group health plans and health insurance issuers generally may not, under federal (or state)law, restrict benefits for any hospital length of stay in connection with childbirth for the
Surgery
Plan I Plan II Retiree Plan
Surgeon’s Charges 100% of fee schedule. 100% of fee schedule. 100% of fee schedule.(PPO Network) Otherwise subject to Otherwise subject to Otherwise subject to
R&C charges. R&C charges. R&C charges.
Surgeon’s Charges 85% of R&C charges 75% of R&C charges 80% of R&C charges (Out-of-Network) for eligible expenses for eligible expenses for eligible expenses
after you’ve met your after you’ve met your after you’ve met your deductible. deductible. deductible, provided you
live outside a 20-mile radius from a PPO provider.
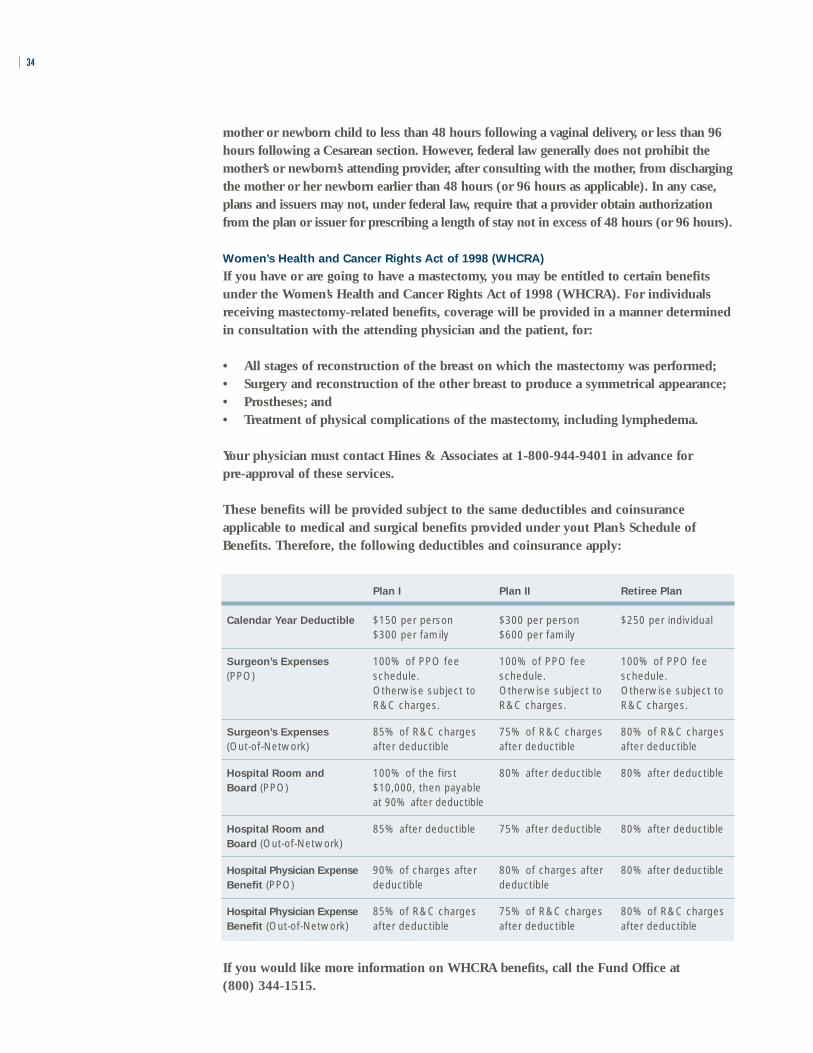
Plan I Plan II Retiree Plan
Calendar Year Deductible $150 per person $300 per person $250 per individual $300 per family $600 per family
Surgeon’s Expenses 100% of PPO fee 100% of PPO fee 100% of PPO fee (PPO) schedule. schedule. schedule.
Otherwise subject to Otherwise subject to Otherwise subject toR&C charges. R&C charges. R&C charges.
Surgeon’s Expenses 85% of R&C charges 75% of R&C charges 80% of R&C charges (Out-of-Network) after deductible after deductible after deductible
Hospital Room and 100% of the first 80% after deductible 80% after deductible Board (PPO) $10,000, then payable
at 90% after deductible
Hospital Room and 85% after deductible 75% after deductible 80% after deductible Board (Out-of-Network)
Hospital Physician Expense 90% of charges after 80% of charges after 80% after deductible Benefit (PPO) deductible deductible
Hospital Physician Expense 85% of R&C charges 75% of R&C charges 80% of R&C charges Benefit (Out-of-Network) after deductible after deductible after deductible
mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96hours following a Cesarean section. However, federal law generally does not prohibit themother’s or newborn’s attending provider, after consulting with the mother, from dischargingthe mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case,plans and issuers may not, under federal law, require that a provider obtain authorizationfrom the plan or issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
Women’s Health and Cancer Rights Act of 1998 (WHCRA)
If you have or are going to have a mastectomy, you may be entitled to certain benefitsunder the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individualsreceiving mastectomy-related benefits, coverage will be provided in a manner determinedin consultation with the attending physician and the patient, for:
• All stages of reconstruction of the breast on which the mastectomy was performed;• Surgery and reconstruction of the other breast to produce a symmetrical appearance; • Prostheses; and• Treatment of physical complications of the mastectomy, including lymphedema.
Your physician must contact Hines & Associates at 1-800-944-9401 in advance for pre-approval of these services.
These benefits will be provided subject to the same deductibles and coinsuranceapplicable to medical and surgical benefits provided under yout Plan’s Schedule ofBenefits. Therefore, the following deductibles and coinsurance apply:
34
If you would like more information on WHCRA benefits, call the Fund Office at (800) 344-1515.

35MENTAL HEALTH AND SUBSTANCE ABUSE
The Fund provides certain coverage under Plan I, Plan II and the Retiree Plan fortreatment of Mental Health and Substance Abuse for you and your eligible dependents.
Mental Health and Substance Abuse Treatment
Plan I Plan II Retiree Plan
Outpatient 100% of network charges 100% of network charges 100% of network charges Mental Health to a calendar year to a calendar year to a calendar year PPO Network; maximum of 25 visits per maximum of 10 visits per maximum of 25 visits per requires a $10 person per calendar year. person per calendar year. person per calendar year. copay
Outpatient 50% of R&C charges to 50% of R&C charges to 50% of R&C charges up to Mental Health a calendar year maximum a calendar year maximum a calendar year maximum Out-of-Network of 25 visits per person per of 10 visits per person per of 25 visits per person,
calendar year, after you’ve calendar year, after you’ve after you’ve met your met your deductible. met your deductible. deductible, if you live
outside a 20-mile radius from a PPO provider.
Inpatient 90% of network charges 80% of network charges 80% of network charges Mental Health to a calendar year to a calendar year to a calendar year PPO Network maximum of 30 days maximum of 30 days maximum of 15 days
per person, after you’ve per person, after you’ve per person, after you’ve met your deductible. met your deductible. met your deductible.
Inpatient 85% of charges to a 75% of charges to a 80% of charges to a Mental Health calendar year maximum calendar year maximum calendar year maximum Out-of-Network of 30 days per person, of 30 days per person, of 15 days per person,
after you’ve met your after you’ve met your after you’ve met your deductible. deductible. deductible.
Outpatient 100% of network charges 100% of network charges 100% of network charges Substance Abuse to a calendar year to a calendar year to a calendar year PPO Network; maximum benefit of maximum benefit of maximum benefit of requires a $10 $500 per calendar year $500 per calendar year $500 per calendar year copay per person. per person. per person.
Outpatient 85% of R&C charges to a 75% of R&C charges to a 80% of R&C charges to a Substance Abuse calendar year maximum calendar year maximum calendar year maximum Out-of-Network benefit of $500 per benefit of $500 per benefit of $500 per
calendar year per person, calendar year per person, calendar year per person, after you’ve met your after you’ve met your after you’ve met your deductible. deductible. deductible.
Inpatient 90% of network charges, 80% of network charges, 80% of network charges, Substance Abuse after you’ve met your after you’ve met your after you’ve met your (Drug & Alcohol) deductible deductible deductiblePPO Network Maximum of 30 Inpatient Maximum of 30 Inpatient Maximum of 15 Inpatient
Days Per Calendar Year Days Per Calendar Year Days Per Calendar Year Per Person Per Person Per Person Maximum of Two (2) Maximum of Two (2) Maximum of Two (2) LIFETIME Occurrences LIFETIME Occurrences LIFETIME Occurrences Per Person Per Person Per Person
Inpatient 85% of charges after 75% of charges after 80% of charges after Substance Abuse you’ve met your deductible you’ve met your deductible you’ve met your deductible(Drug & Alcohol) Maximum of 30 Inpatient Maximum of 30 Inpatient Maximum of 15 Inpatient Out-Of-Network Days Per Calendar Year Days Per Calendar Year Days Per Calendar Year
Per Person Per Person Per Person Maximum of Two (2) Maximum of Two (2) Maximum of Two (2) LIFETIME Occurrences LIFETIME Occurrences LIFETIME Occurrences Per Person Per Person Per Person
36
P R E A U T H O R I Z AT I O N
If your doctor recommends inpatient care for the treatment of Mental Health orSubstance Abuse, you must obtain pre-approval through the Fund’s Health Managementprovider, Hines & Associates, by calling 1-800-944-9401 for authorization before youradmission. You will be notified in writing of the authorization. If you have not received awritten authorization by the day of your admission, call Hines & Associates.
A person who does not complete the prescribed treatment plan that is established atthe beginning of his/her treatment will be responsible for paying the full cost of thetreatment.
Payment for the treatment of inpatient substance abuse, whether alcohol or drugs, willbe limited to two occurrences in a lifetime.
The Health Fund’s utilization review firm, Hines & Associates, along with the CarpentersAssistance Program, will assist the Fund in assuring that our Members receive thehighest level of care in the appropriate facilities.

HOME HEALTH CARE
Home Health Care helps the Fund to keep down hospital expenses by providing analternative to inpatient hospital care. Home Health Care can not only decrease the lengthof a hospital admission but can also, in some cases, eliminate a hospital admissionaltogether. This service can save the Fund 50% or more on the cost of inpatient care. Inaddition, Home Health Care provides a sense of security during a time of illness. You or afamily member can receive many services at home in familiar surroundings and close tofamily and friends.
37
• A Home Health Care Agency is a licensed organization that provides skilled nursing and other therapeuticservices for participants that are recovering from an injury or illness in the comfort of their own home.
• Home Health Care through a PPO provider is covered at 100% after you meet the deductible.
• Help with daily living (custodial care) is covered if provided in your home at the direction of a hospice organization.
The Fund’s Managed Health Care provider will arrange for medically necessary homehealth care through the PPO. To be covered, your doctor must submit a letter of medicalnecessity to the Fund Office. Benefits for Home Health Care are shown in the chart below.
FA ST FAC TS :
Home Health Care
Plan I Plan II Retiree Plan
PPO Network 100% of network charges, 90% of network charges, 100% of network charges, after you’ve met your after you’ve met your after you’ve met your calendar year deductible calendar year deductible calendar year deductible if care begins within if care begins within if care begins within 7 days of discharge from 7 days of discharge from 7 days of discharge froman inpatient stay; an inpatient stay; an inpatient stay; otherwise, 90% after otherwise, 80% after otherwise, 80% afterdeductible. deductible. deductible.
Out-of-Network 90% of R&C charges, 80% of R&C charges, 80% of R&C charges after you’ve met your after you’ve met your if you’ve met your calendar year deductible calendar year deductible deductible and you live if care begins within if care begins within outside a 20-mile radius 7 days of discharge from 7 days of discharge from from a PPO provider an inpatient stay; an inpatient stay; if care begins within otherwise, 85% after otherwise, 75% after 7 days of discharge fromdeductible. deductible. an inpatient stay.
To be covered, charges by a Home Health Care Agency for care at home must start withinseven days of a prior hospital confinement for the same or for a related condition OR inorder to prevent a proposed hospital confinement.

What’s Covered
Note that only medically necessary services that are prescribed by the attending physicianand under the supervision of the attending physician are covered. The following is apartial list of health services available through a Home Health Care Agency:
• Part-time or intermittent nursing care by a registered nurse or by a licensed practicalnurse under the supervision of a registered nurse, if services of a registered nurse areunavailable;
• Part-time or intermittent home health aide services, consisting primarily of patientcare of a medical or therapeutic nature by other than a registered or licensed practicalnurse;
• Physical therapy, speech therapy, medical social work and nutritional consultationsprovided by the Home Health Care Agency; and
• Medical supplies, medications prescribed by a physician and laboratory services by oron behalf of the Home Health Care Agency to the extent such items would have beencovered if the insured had remained in the hospital. Visits must be medically necessary.
H O S P I C E C A R E
Hospice Care is covered at 100% through the PPO for Plans I and II only. A hospice is afacility that provides care and services for the terminally ill and that:
• Provides 24-hour a day nursing care for the terminally ill person with necessaryphysical, psychological and spiritual needs, with acute inpatient and outpatient care,home care, bereavement counseling directly or indirectly;
• Has a medical director who is a physician;
• Has an interdisciplinary team that coordinates the care and services it provides and that includes at least one physician, one registered professional nurse and onesocial worker;
• Maintains central clinical records on all patients; and
• Is licensed or accredited as a hospice if required.
38
What is a Home
Health Aide?
A home health aide is a person who providescare of a medical or therapeutic nature andreports to and is underthe direct supervision of a Home Health CareAgency.
! NOTE: Custodial care is covered as part of yourhospice care benefits if provided in your home at the direction of a hospice organization.

CARPENTERS ASSISTANCE PROGRAM
The Carpenters Assistance Program (CAP) provides free, confidential assistance for youand your family members when confronting stress, depression, alcoholism, drug abuse,and job or family problems.
39
How to Contact the CAP
Call 1-800-344-1515 extension 1160 to speakconfidentially with a counselor or to make anappointment.
☎ CAP, in association with the Employee Assistance Program (EAP) service of theMount Auburn Hospital, provides assistance through a network of facilitiesthroughout the area. Professionals determine an appropriate treatment plan for you and/or your covered dependents. To contact Mount Auburn (EAP), call 617-661-0090 or 1-800-888-5105.
You and your family are eligible for the following benefits:
• Assessment for drug, alcohol, marital, emotional or legal difficulties and/or careerproblems;
• Referral to the appropriate facility for the treatment of drug or alcohol dependency(see Mental Health and Substance Abuse on page 35);
• Diagnostic evaluation and referral to inpatient and/or residential treatment facilities;
• Full coverage for short-term counseling provided by the EAP services of MountAuburn Hospital for up to eight one-hour visits per incident;
• Case management and follow-up services for one year; and
• Educational seminars, outreach activities and consultation.
☎ If you are admitted to a hospital or other facility for emergency care for a mentaldisorder or for substance abuse treatment, you, a member of your family, your doctor,or the hospital must call Hines & Associates at 1-800-944-9401 within 24 hours ofyour admission.
!! Note: Court-ordered or random drug testing is not covered under the Carpenters Assistance Program.
• The Carpenters Assistance Program is available to participants and eligible dependents in Plan I, Plan IIand the Retiree Plan.
• When you call, a CAP counselor will assess your situation and set up an appointment for short-termcounseling or refer you to the appropriate provider for treatment.
• Treatment you receive through the Carpenters Assistance Program is strictly confidential.
• If you receive a referral for inpatient treatment of mental health or substance abuse, you must contactHines & Associates, the Fund’s Health Management provider, at 1-800-944-9401 for pre-admissioncertification within 24 hours of your admission.
FA ST FAC TS :

PRESCRIPTION DRUGS
The prescription drug benefit offers you and your family a convenient and cost-effectiveway to receive your prescription medication. You may have your prescriptions filled bymail or at a pharmacy. If you use generic drugs, you will save money for yourself and forthe Health Benefits Fund.
40
• Present your Ullicare Rx/Medco card at a participating pharmacy and make the applicable copayment toreceive your prescription drugs.
• You can save time and money by using the mail order program. You can order a 90-day supply of genericprescription drugs for just $20.
• For retirees, a $15,000 per individual per calendar year maximum applies.
The chart below shows your copayments for prescription drugs based on whether youreceive your prescription medication from a retail pharmacy or through the mail.
FA ST FAC TS :
Prescription Drugs*
Generic Brand Preferred Brand Non-Preferred
Retail (34-day supply) $10.00 $20.00 $30.00
Mail (90-day supply) $20.00 $40.00 $60.00
Generic Drugs
The Health Benefits Fund encourages the use of generic drugs. Generic drugs are a lessexpensive alternative to brand name drugs. The generic version of any drug containsidentical active chemical ingredients and must meet the same manufacturing standardsand federal requirements for safety and effectiveness as a brand name drug. Yourcopayments for generic drugs are lower whether you use a retail pharmacy or order yourprescription drugs by mail.
Brand Preferred
This category of medications consists of brand name and generic medications that are themost commonly used, the most cost efficient and the most therapeutically beneficial inthe treatment of common health conditions.
Brand Non-Preferred
All brand name and generic medications not falling into the above categories.
How to Get Your Prescription Drugs
When you fill a prescription at a pharmacy, you simply present your Ullicare Rx/Medcocard when you request your medication and pay the applicable copayment.
Mail Order Program
The mail order program is a convenient way for you to receive any medication—especially “maintenance drugs” that you need to take on a regular basis. Because you
* The calendar year maximum is $15,000 per individual in the Retiree Plan.

know in advance that you will need this medication, it’s easy to establish a routine offilling such prescriptions by mail. Through the mail order program, you are eligible toreceive medication for up to a 90-day supply. Contact the Fund Office for a mail orderform.
What’s Covered
Coverage for prescription drugs is provided for the following non-hospital items:
• Legend drugs;
• Injectable insulin and supplies, including hypodermic needles, syringes and testmaterial;
• Compounded medication of which at least one ingredient is a prescription legenddrug; or any other drug which, under state law, may only be dispensed upon thewritten prescription of a physician;
• Oral contraceptives;
• Viagra (6 tablets every 30 days).
What’s Not Covered
No benefits are payable for:
• The difference in charges between a generic drug and brand name drug unless“Dispensed as Written” appears on the prescription;
• Drugs or medicines lawfully obtainable without a prescription order of a physician ordentist except insulin;
• Birth control devices (other than oral contraceptives);
• Levonorgestrel (Norplant);
• Therapeutic devices or appliances and support garments;
• Immunization agents, biological sera, blood or blood plasma;
• Drugs labeled “Caution—limited by federal law to investigational use” or withsimilar language or experiment drugs even though a charge is made to the person;
• Any charge for the administration of prescription legend drugs or insulin;
• Any medication, legend or not, which is consumed or administered at the placewhere it is dispensed;
• Medication which is to be taken by or administered to the person in whole or in partwhile he or she is a patient in a licensed hospital, rest home, sanitarium, extendedcare facility, convalescent hospital, nursing home or similar institution whichoperates on its premises, a facility for dispensing pharmaceuticals;
• Refilling of a prescription in excess of the number specified by the physician ordentist or any other refill dispensed after one year from the order of a physician ordentist;
• Prescription drugs that may be properly received without charge under local, state orfederal programs, including Workers’ Compensation or similar law;
41
How to Fill a
Mail Order Prescription
Obtain a written prescrip-tion from your doctor for a90-day supply of medica-tion. The prescription mustinclude:
• The patient’s full name
• The doctor’s name, phonenumber and address
• Exact strength, quantityand dosage; and
• Diagnosis, if required forthat drug.
• Call the Fund Office torequest a mail order form.
What are
Maintenance Drugs?
Maintenance drugs arethose that you require onan ongoing basis such asmedication for high bloodpressure, heart conditionsor diabetes.

• The following drugs:– Aero Chamber (covered under the Medical Plan with a letter of medical
necessity);– Hepatitis A or B (covered under the Medical Plan with a letter of medical
necessity); – Rogaine (Minoxidil or Loniten) when prescribed for hair restoration;– Retin-A (Tretinoin Cream, Gel, Liquid) except when prescribed by a physician for
acne or a skin disorder for an eligible dependent child before age 24 (coveredunder the medical plan for adults with letter of medical necessity);
– Smoking deterrent medications;– Fertility drugs* such as, but not limited to:
– Pergonal (menotropins);– Profasi HP (HCG-Human Chorionic Gonadotropin);– Pro-Ception;– Serophene (Clomiphene Citrate);– Clomid (Dienestrol);– Lupron;
– Ephinephrine – primatine mist;– Ephedrine sulfate – absolute decongestant;– Ferrous sulfate – iron supplement;– Elixir terpin hydrate – expectorant; – Over the counter vitamins with or without fluoride; and– Growth hormones.
*Certain fertility drugs are covered under the Medical Plan.
42

DENTAL CARE
Healthy teeth and gums are an important part of your overall health. That’s why the HealthBenefits Fund offers comprehensive dental benefits through Delta Dental, the nation’slargest dental network. Dental benefits are provided for participants in Plan I only.
43
• You do not have to meet a deductible to receive dental care.
• You may visit any dentist you’d like, but you’ll save money if you use a provider in the Delta Dentalnetwork— “Delta Preferred Option USA Plus.”
• There are no claim forms to file if you use a Delta Dental Network provider.
• Dental benefits are available to Plan I participants and their eligible dependents.
• The Plan covers orthodontia, even for adults.
FA ST FAC TS :
If you are covered for benefits under Plan I, you and your dependents are eligible fordental benefits through Delta Dental. Dentists that participate in the Delta Dental networkhave agreed to provide services at a pre-negotiated discounted rate. When you visit aDelta Dental provider, show your Delta Dental ID card to receive the discounted rates.
The chart below shows the amount the Plan pays for Dental Care through the DeltaDental network.
Dental Benefits (Plan I only) Plan Pays
Diagnostic and Preventive (includes cleanings and x-rays) 100% of network charges
Restorative, Oral Surgery, Periodontics, Endodontics, Prosthetic 80% of network charges Maintenance and Emergency Dental Care
Prosthodontics (dentures) and Major Restorative 50% of network charges
Orthodontics 100% of network, up to $2,000 per person per lifetime
Out-of-Network Benefits
If you do not use a Delta Dental provider, you will be billed for any amount that yourout-of-network dentist charges that is more than the pre-negotiated Delta Dental networkcharge.
Maximum Benefits
A $1,500 calendar year maximum dental benefit applies to each covered person fordental services per calendar year. The lifetime maximum benefit for orthodontia is$2,000 per covered person. There’s no age limit for orthodontia.
Covered Dental Surgical Services
The following surgical procedures are covered under the New England Carpenters HealthBenefits Fund:
• Surgical removal of unerupted teeth or impacted teeth when imbedded in the bone or soft tissue– Soft tissue impaction– Partial bony impaction– Complete bony impaction
• Extraction of seven or more permanent teeth• The excision of a benign or cancerous growth other than a radicular cyst• Radicular cysts involving the roots of three or more teeth• Gingivectomies involving two or more gum quadrants• Gingival flap• Mucogingival surgery• Osseous surgery• Osseous graft• Soft tissue graft• Apicoectomy
44
Questions about
What’s Covered?
Contact Delta DentalCustomer Service at 1-800-872-0500 for information about limitations or exclusionsthat may apply to a particular procedure.

Routine vision examinations are essential for maintaining healthy eyes and good vision.Vision benefits are provided under Plans I, II and the Retiree Plan and for Members andtheir spouses who are retired and are collecting a pension from the Carpenters Unionand are current in their monthly dues. Also eligible are spouses of deceased pensionedMembers who continue to collect the Member’s pension after their death provided theMember was current with dues at the time of his or her death.
The Plan provides:
• For adults – routine eye exam and glasses once every two years; and
• For children – (up to age 19 or 24 if full-time students) routine eye exam and glassesonce every year.
“Glasses” means one pair of bifocals or two pairs of single-vision glasses, one for distanceand one for close-up. Special lens materials and coatings that are not covered under thevision benefit are available for a reasonable copayment through the Vision Center andDavis Network.
!! Note: When using the Davis Network, you must obtain your examination and glasses at the same timeand from one provider.
*You also have the option of choosing contact lenses instead of eyeglasses at the VisionCenter or through a Davis Vision Network Provider, with a copayment. The contact lensbenefit guidelines are as follows:
• New wearers, either new to the doctor or first-time obtaining contacts — routine eyeexamination, a comprehensive fitting and two standard lenses or two boxes of eitherdisposable lenses or planned replacement lenses; and
• Existing wearers — routine eye examination, a reassessment fitting and two standardlenses or two boxes of planned replacement lenses or four boxes of disposable lenses.
45
FA ST FAC TS :
VISION CARE
• You and your spouse may receive an eye exam and a pair of glasses or contacts* once every 24 monthsfrom the Carpenters Vision Center or from a Davis Vision provider. Your dependent children areeligible for an eye exam and a pair of glasses or contacts once every 12 months.
• The Optional Vision Benefit may also be available to you, allowing you to visit a vision care specialistof your choice and receive partial reimbursement for examinations and glasses.

The contact lens benefit is not available through the Optional Vision Benefit explained below.
You have three alternatives for receiving vision benefits:
• Carpenter Vision Center — owned and operated under the New England CarpentersHealth Benefits Fund. It offers complete eye examinations and the largest selection offrames available under the Plan. Optical services that aren’t provided under the Planare available at a discounted rate through the Vision Center. The Vision Center is at250 Everett St., Allston, MA, and offers afternoon, evening and Saturdayappointments. Call (617) 782-0100 for an appointment.
• Davis Vision Program—a network of private doctors under contract to provideroutine eye exams and eyeglasses or contact lenses. There is a select group of framesavailable under the Davis Vision Plan. Network doctors are located throughout NewEngland. To find a convenient doctor, call 1-800-999-5431or visit their website atwww.davisvision.com.
Be sure to choose a full-service doctor who can provide both the exam and eyeglassesor contact lenses. When you make your appointment and at the time of your visit,tell the staff you are in the Davis Vision program. If you are retired, you must contactthe Carpenter Vision Center (617-782-0100) before contacting Davis Vision.
• Optional Vision Benefit — allows you to see any eye doctor you choose and receive apartial reimbursement. This option is available only to members of Plan I or Plan IIor members of Local 1996 who live in Maine, Vermont or Northern New Hampshire.
Reimbursement is as follows, regardless of the fee the provider charges:
– Eye exam (routine) — $50– Frames (one pair only) — $40– Eyeglass lenses (one pair only) — $60– Contact lenses — no reimbursement
The following Plan participants must use either the Carpenters Vision Center or a DavisVision Network Provider:
• Retirees covered under the Retiree Plan.
• Retired members (and their spouses) who are collecting a pension from the Carpenters Pension Plan and are current in their dues.*
• A surviving spouse who is receiving the Pension of a retired Member who was current in his or her dues at the time of his or her death.*
*Members in these categories must contact the Vision Center at 617-782-0100 beforeutilizing their vision benefit.
!! The PPO Network ophthalmologists are not part of the vision care benefit.
46
Questions about
Vision Coverage
Call the Carpenter VisionCenter (617) 782-0100 or the Carpenters Health Benefits FundOffice if you have ques-tions (1-800-344-1515).

LIFE INSURANCE
Your designated beneficiary will be eligible for a life insurance benefit from this Fund ifyou die from any cause while you’re an active member and you’re covered by the NewEngland Carpenters Health Benefits Fund.
47
• Your designated beneficiary will receive a lump sum benefit if you die while you are an activemember covered by this Fund.
• Your beneficiary must provide the Fund Office with a certified copy of your death certificate in orderto receive a benefit.
• If your current legal spouse dies while you are an active member covered by this Fund, you will beeligible for a lump sum benefit of $2,000.
The chart below shows the lump sum that is payable to your designated beneficiary uponyour death.
Life Insurance
Plan I Plan II Retiree Plan
Benefit $20,000 $10,000 No Benefit
Naming a Beneficiary
✍ You may name anyone you wish to be your beneficiary and you may change thisdesignation at any time. To change your beneficiary, call the Fund Office for theappropriate form. You do not need to get your beneficiary’s consent to make thischange. Your change will be effective when the Fund Office receives your completedform.
!! Your beneficiary designation must be on file at the Fund Office at the time of yourdeath to be valid.
If you do not have a designated beneficiary form on file at the Fund Office at the time ofyour death, or if your designated beneficiary does not survive you, your life insurancebenefit will be paid to your estate.
C OV E R AG E F O R YO U R S P O U S E
The Fund also provides a life insurance benefit for your spouse. If your current legalspouse dies from any cause while covered under the New England Carpenters HealthBenefits Fund, you, as the Member, will be eligible for a lump sum benefit of $2,000.Note that ex-spouses are not eligible for this benefit.
Keep Your Beneficiary
Information Up-To-Date
Contact the Fund Office if you’d like to change your beneficiary if you getmarried, have a child or get divorced.
FA ST FAC TS :

Continuing Coverage If You Become Disabled
✍ If you become totally and permanently disabled while you're covered under theHealth Benefits Fund, your life insurance benefit will be continued at no cost to youunless you recover from your disability or attain age 65. You must complete and filean application for total and permanent disability with the Fund Office within oneyear of the date you become disabled and prior to your 60th birthday. The FundOffice will require proof of your continued disability to keep your life insurance inforce. Contact the Fund Office to request an application.
I F YO U R C OV E R AG E E N D S
Extended Benefits
If you die within 31 days from the date your coverage under the New EnglandCarpenters Health Benefits Fund ends, the full amount of life insurance will be payableto your beneficiary.
Converting Your Coverage
✍ You may convert your life insurance to an individual policy if your coverage underthe Health Benefits Fund ends. To apply, contact the Fund Office for an applicationfor conversion through the Hartford Life Insurance Company within 31 days of thedate your coverage ends.
48
What is Total and
Permanent Disability?
The Health Benefits Fundconsiders you totally andpermanently disabled ifyou are not working at anyjob for wage or profit, andyou are unable to work inany job that is reasonablysuited to you by your edu-cation, training or experi-ence due to an illness orinjury.
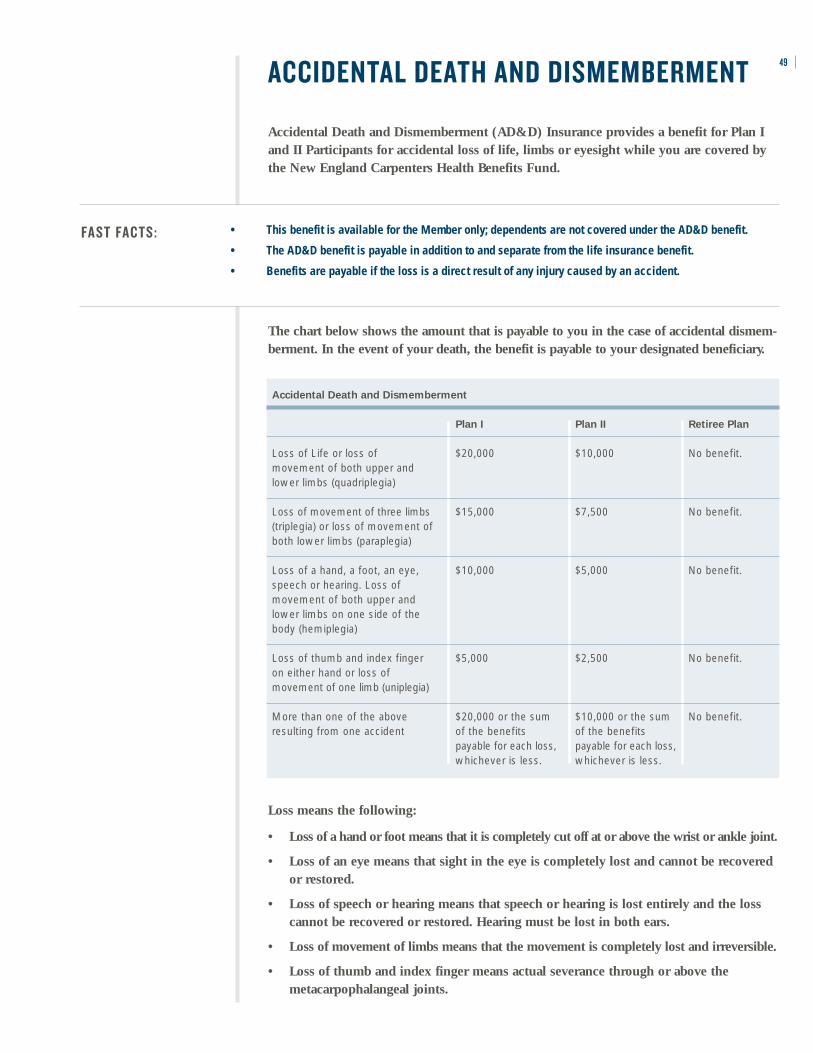
ACCIDENTAL DEATH AND DISMEMBERMENT
Accidental Death and Dismemberment (AD&D) Insurance provides a benefit for Plan Iand II Participants for accidental loss of life, limbs or eyesight while you are covered bythe New England Carpenters Health Benefits Fund.
49
• This benefit is available for the Member only; dependents are not covered under the AD&D benefit.
• The AD&D benefit is payable in addition to and separate from the life insurance benefit.
• Benefits are payable if the loss is a direct result of any injury caused by an accident.
FA ST FAC TS :
The chart below shows the amount that is payable to you in the case of accidental dismem-berment. In the event of your death, the benefit is payable to your designated beneficiary.
Accidental Death and Dismemberment
Plan I Plan II Retiree Plan
Loss of Life or loss of $20,000 $10,000 No benefit. movement of both upper and lower limbs (quadriplegia)
Loss of movement of three limbs $15,000 $7,500 No benefit. (triplegia) or loss of movement of both lower limbs (paraplegia)
Loss of a hand, a foot, an eye, $10,000 $5,000 No benefit. speech or hearing. Loss of movement of both upper and lower limbs on one side of the body (hemiplegia)
Loss of thumb and index finger $5,000 $2,500 No benefit. on either hand or loss of movement of one limb (uniplegia)
More than one of the above $20,000 or the sum $10,000 or the sum No benefit. resulting from one accident of the benefits of the benefits
payable for each loss, payable for each loss, whichever is less. whichever is less.
Loss means the following:
• Loss of a hand or foot means that it is completely cut off at or above the wrist or ankle joint.
• Loss of an eye means that sight in the eye is completely lost and cannot be recoveredor restored.
• Loss of speech or hearing means that speech or hearing is lost entirely and the losscannot be recovered or restored. Hearing must be lost in both ears.
• Loss of movement of limbs means that the movement is completely lost and irreversible.
• Loss of thumb and index finger means actual severance through or above themetacarpophalangeal joints.

50
S E AT B E LT B E N E F I T
If you are properly wearing a seatbelt (as verified on the police report) at the time of anautomobile accident and you suffer a loss that is payable under the AD&D benefit, youmay be eligible for a “seatbelt benefit.” To be eligible, you must be a passenger riding inan automobile or the licensed operator of the automobile that is involved in the accident. For Plan I, the seatbelt benefit is $2,000. For Plan II, the seatbelt benefit is $1,000. Thereis no seatbelt benefit for members in the Retiree Plan.
What’s Not Covered
The Fund will not pay an AD&D benefit for death or any loss resulting from or causeddirectly, wholly or partly by:
• Sickness;
• Disease;
• Medical treatment for sickness or disease;
• Any infection, except a pus-forming infection of an accidental cut or wound;
• War or any act of war, whether war is declared or not;
• Any injury received while in any armed service of a country that is at war or engagedin armed conflict;
• Any intentionally self-inflected injury, suicide, or suicide attempts, whether sane or insane;
• The injured person’s intoxication. Intoxication means that blood alcohol content or theresults of other means of testing blood alcohol level meet or exceed the legalpresumption of intoxication under the law of the state where the accident took place;
• Participation in the commission of a felony; or
• Taking drugs, sedatives, narcotics, barbituates, amphetamines, or hallucinogensunless prescribed for or administered by a licensed physician.
FA ST FAC TS :
WEEKLY ACCIDENT AND SICKNESS
If you become totally disabled and cannot work due to a non-work related injury orillness, you are eligible for a weekly accident and sickness benefit through the NewEngland Carpenters Health Benefits Fund. This benefit is only available to Members inPlan I with worked hours.
51
• If you are an eligible Plan I Member and you become disabled while covered under Plan I, you mayreceive a weekly benefit of $250 from the Health Benefits Fund for up to 26 weeks.
• The Weekly Accident and Sickness benefit is only available to you while you are under the care of aphysician.
• If you are receiving a benefit under Workers’ Compensation or unemployment benefit, OccupationalDisease Law or similar legislation, you are not eligible for the Weekly Accident and Sickness benefit.
Payment of Benefits
Your benefit of $250 per week will begin on the first day of the disability if it is due to anaccident or the eighth day of the disability if it is due to an illness. Payment willcontinue during your disability for a maximum of 26 weeks for any one continuousperiod of disability due to the same or related cause or causes.
When Benefits Begin Day 1 (Accident) Day 8 (Illness)
Maximum Benefit 26 Weeks 26 weeks
Successive periods of disability that are separated by less than two weeks of continuousactive covered employment are considered one period of disability. If you suffer anotherdisability due to a different and unrelated cause, you must return to active work for aperiod of more than two weeks to receive a benefit for another period of disability.
!! It is not necessary for you to be confined to your home in order to collect a weeklyaccident and sickness benefit, but you must be under the care of a legally qualifiedphysician licensed to practice medicine.
Pregnancy-Related Disability
If you are totally disabled and medically unable to work because of pregnancy, childbirthor miscarriage, your weekly accident and sickness benefit is payable from the eighth dayof disability on the same basis as any other illness.
Please Note
• Payments you receivefrom the weekly accidentand sickness benefit areconsidered taxable incomeand must be reported onyour federal income taxreturn. The Fund Officewill withhold state andfederal income taxes.
• No Social Security (FICA)tax is deducted from yourpayment. The Fund paysthis tax for you.
• You are not eligible for thisbenefit if you are usingBanked Hours to maintainyour eligibility.
• For information about filingweekly accident and sick-ness claims, see page 63.
• If your disability is relatedto a motor vehicle acci-dent, the Fund does notpay until the benefit fromthe automobile insurancehas been exhausted.
• If your disability is due toan injury but you do notstop working at the timeof the injury, the disabilityis considered an illnessand the waiting periodapplies.
• It is your responsibility toprovide updates of yourcondition to the FundOffice.
If You’re Injured on the Job
If you become disabled due to a work-related illness or injury, you may be eligible for aWorkers’ Compensation benefit. Contact your employer or Local for information on how toapply for benefits.

52 GENERAL EXCLUSIONS
The following is a partial list of plan exclusions for Plan I, II and the Retiree Plan. Youmay call the Fund Office to request specific information as to whether or not a service orsupply is a covered expense. The Plan excludes expenses or charges:
• For services or supplies not recommended by a physician or surgeon or notmedically necessary in treating the injury or illness;
• That are in excess of Reasonable and Customary (R&C) charges;
• For medical care or treatment and services or supplies for charges that are made by anursing home, rest home, convalescent home or similar establishment;
• For services or supplies that are:– Not provided in accordance with generally accepted professional medical
standards; or– For experimental or investigational treatment;
• Custodial care, when not provided in your home at the direction of a hospice care organization;
• That result from cosmetic or reconstructive surgery except:– When surgery is performed on an eligible dependent child because of a
congenital disease or anomaly that has resulted in a functional defect asdetermined by his or her attending physician or surgeon; or
– In the case of an accidental bodily injury;
• In connection with dental work, x-rays or surgery (unless part of the dental benefitsfor Plan I participants), except expenses for services that are required for correctionof damage caused by an accidental injury to a sound and natural tooth sustained byan eligible person, or for tumors or cysts of an eligible person;
• Under Plan I and Plan II Temporomandibular Joint Disorders (TMJ) are excluded forappliances and services, supplies or procedures to increase the height of teeth(increase vertical dimension or restore occlusion) except for (1) disorders caused byor result in a specific medical condition, such as degenerative arthritis and jawfractures or dislocations. The medical condition must be proven to exist by means ofdiagnostic x-ray tests or other generally accepted diagnostic procedures; and amandibular orthopedic repositioning appliance (MORA);
• Temporomandibular Joint Disorders (TMJ) for Retirees;
• Early Intervention Services;
• Made by a Veterans’ Administration Hospital or by a physician employed by aVeterans’ Administration Hospital if the disability is service related, except asmandated by law;
• That the member is not legally required to pay or that is for medical care furnishedwithout charge, paid for or reimbursable by or through a government agency orcounty, except where specifically prohibited by applicable statute;
• For special home construction to accommodate a disabled person;
• For medical or surgical treatment of obesity, including but not limited to, gastricrestrictive procedures, intestinal bypass and reversal procedures, weight lossprograms, dietary instructions, and any complications thereof;
• For medical or surgical treatment of severe underweight, including, but not limitedto high calorie and/or high protein food supplements, other food or nutritionalsupplements, or nutritional counseling, except in conjunction with medicallynecessary treatment of anorexia, bulimia or acute starvation. Severe underweightmeans a weight more than 25 percent under normal body weight for the patient’s age,sex, height and body frame based on weight tables generally used by physicians todetermine normal body weight;
• For memberships in or visits to health clubs, exercise programs, gymnasiums, and/orany other facility for physical fitness programs;
• For sterilization reversals;
• For failure to appear for an appointment as scheduled, for completion of claim forms,attorneys’ reports or late stay charges;
• For injury, illness or dental treatment for which an eligible person has received or isentitled to receive benefits under a Workers’ Compensation or Occupational DiseaseLaw or that arises out of or in the course of any occupation or employment;
• For any loss, expense or charge resulting from an eligible person’s participation in thecommission of a felony;
• For any loss, expense or charge resulting from an act of declared or undeclared war,armed aggression or act of terrorism;
• For any loss, expense or charge incurred while an eligible person is on active duty orin training in the Armed Forces, National Guard or Reserves of any state or country;
• For supplies or equipment for personal hygiene, comfort or convenience such as airconditioning, humidifier, physical fitness and exercise equipment, tanning bed orwater bed;
• For court-ordered or random drug testing;
• For Infertility Treatment under the Retiree Plan;
• For acupuncture unless rendered by an M.D. (Medical Doctor);
• For services rendered when not an eligible participant; and
• Claims not received in the Fund Office within 12 months from date of service.
☎ Contact the Fund Office at (800) 344-1515 for specific information about whether ornot a service or supply is a covered expense.
53
54 COORDINATION OF BENEFITS
Members of a family are often covered under more than one group health plan, whichcould result in duplication of health coverage. To avoid this, the health care benefitsprovided by this Fund are coordinated with similar benefits payable under other plans.
• You must report any duplicate group health coverage for yourself and/or your dependents on any claim you submit to the Fund Office.
• Benefits under this Fund are coordinated with HMO, PPO, Medicare or other group health care coverage.
FA ST FAC TS :
Under the Coordination of Benefits provision, if you are covered under any other grouphealth plan, the total payment you receive from all programs may not be more than 100%of the “allowable expenses.” Allowable expenses are the necessary and reasonable expensesfor treatment or supplies covered by the primary plan that you are covered under.
Methods of Coordination
The plan under which benefits are payable first is the primary plan. All other plans arecalled secondary plans. The following rules determine which plan’s benefits are payablefirst and follow the National Association of Insurance Commissioner’s Model Rules:
• A plan that does not contain a Coordination of Benefits provision is always primary.
• A plan that covers you as a Member is primary.
• If you are covered as a Member under two plans, the plan that has covered you for a longer period is primary.
• A plan that covers you as an active Member pays before a plan which covers you as a laid-off Member or retiree.
Rule 2: Dependent Child Covered Under More Than One Plan
A. If the parents of a child are married or are living together, then the plan that coversthe parent whose Birthday falls earlier in the calendar year pays first; and the planthat covers the parent whose Birthday falls later in the calendar year pays second. Ifthe parents are not living together but a court decree awards joint custody to bothparents without specifying that one parent has the responsibility to provide healthcare coverage for the child, this rule also applies.
B. If both parents have the same Birthday, the plan that has covered one of the parentsfor a longer period of time pays first; and the plan that has covered the other parentfor the shorter period of time pays second.
C. The word “Birthday” refers only to the month and day in a calendar year; not theyear in which the person was born.
D. If the specific terms of a court decree state that one parent is responsible for thechild’s health care expenses or health care coverage, and the plan of that parent hasactual knowledge of the terms of that court decree, that plan pays first. If the parentwith financial responsibility has no coverage for the child’s health care services orexpenses, but that parent’s current spouse does, the plan of the spouse of the parentwith financial responsibility pays first. However, this provision does not apply during

any Plan Year during which any benefits were actually paid or provided before theplan had actual knowledge of the specific terms of that court decree.
E. If the parents are divorced, separated or not living together (regardless of whetherthey were ever married), and there is no court decree allocating responsibility for thechild’s health care services or expenses, the order of benefit determination among theplans of the parents and their spouses (if any) is:
1. The plan of the custodial parent pays first; and 2. The plan of the spouse of the custodial parent pays second; and 3. The plan of the non-custodial parent pays third; and 4. The plan of the spouse of the non-custodial parent pays last.
Coordination of Benefits with Health Maintenance Organizations (HMOs),
Preferred Provider Organizations (PPOs) and Similar Organizations
If you or your dependents are covered by an HMO, a PPO, or a similar health care organ-ization and that group health plan is primary, you must utilize all health care alternativesavailable to you through the other provider(s) before this Fund will honor any claim for benefits. Also, if a member or his/her dependents violates the provisions of the HMO,such as neglecting to use that plan’s facilities or following managed care or precertifica-tion provisions, no benefits will be payable under this Plan.
Coordination of Benefits with Medicare
When you reach age 65 or if you become disabled, you are eligible for hospital insurancebenefits (“Part A”) and supplementary medical insurance (“Part B”) under Medicare. Thechart below illustrates how your benefits are paid at that time.
55
Type of Plan Participant Primary Plan Secondary Plan
Retiree or dependent who is Medicare eligible Medicare This Fund (and unemployed) unless you are covered under work hours, then it is reversed
Retiree who is not Medicare eligible This Fund N/A
Active Member and/or dependent who is This Fund Medicare Medicare eligible
Disabled Active Member This Fund Medicare
Coverage for Disabled Members or Members’ Disabled Dependents with
End-Stage Renal Disease (ESRD)
If you are actively employed and you or any of your covered dependents become entitledto Medicare because of end-stage renal disease (ESRD), this Plan pays first and Medicarepays second for 30 months starting the earlier of:
• The month in which Medicare ESRD coverage begins; or• The first month in which the individual receives a kidney transplant.
Then, starting with the 31st month, Medicare pays first and this Plan pays second.
Any covered charges incurred by such disabled individual should be submitted to thisPlan for payment. Afterward, any unpaid balance should be submitted to Medicare, fortheir consideration.
To Enroll in Medicare...
• Visit your local SocialSecurity Office,
• Call 1-800-MEDICARE (1-800-633-4227), or
• Log on towww.medicare.gov.
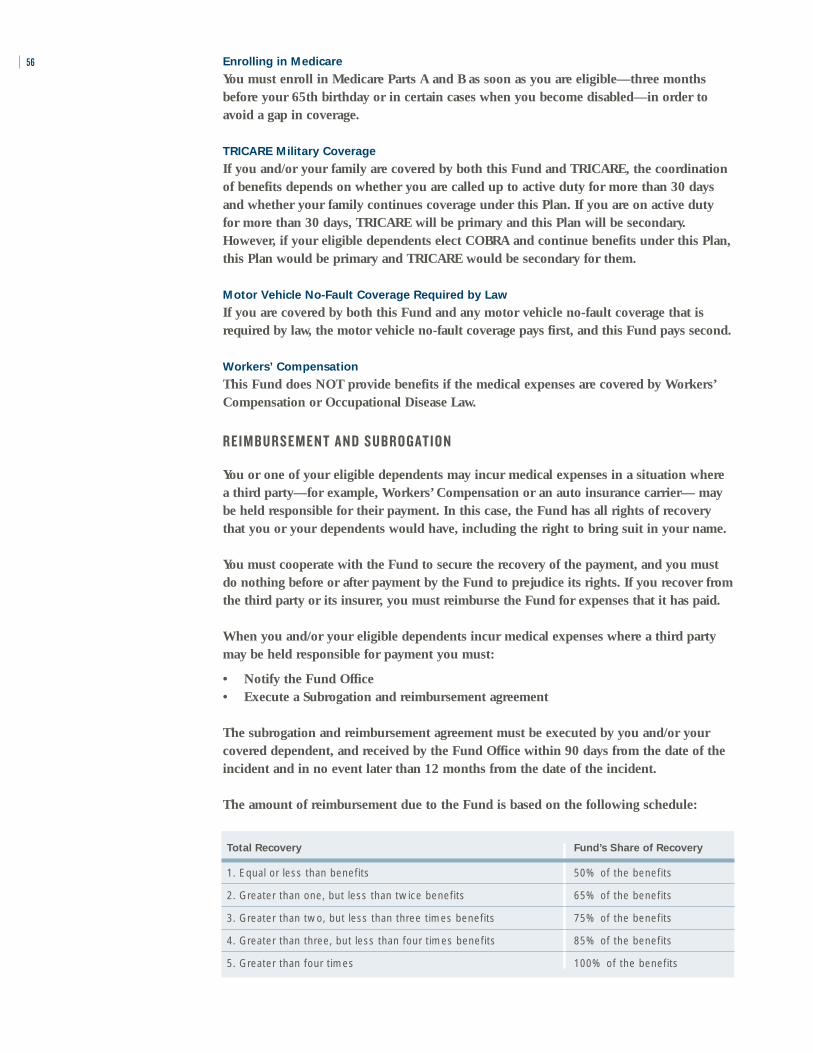
56 Enrolling in Medicare
You must enroll in Medicare Parts A and B as soon as you are eligible—three monthsbefore your 65th birthday or in certain cases when you become disabled—in order toavoid a gap in coverage.
TRICARE Military Coverage
If you and/or your family are covered by both this Fund and TRICARE, the coordinationof benefits depends on whether you are called up to active duty for more than 30 daysand whether your family continues coverage under this Plan. If you are on active dutyfor more than 30 days, TRICARE will be primary and this Plan will be secondary.However, if your eligible dependents elect COBRA and continue benefits under this Plan,this Plan would be primary and TRICARE would be secondary for them.
Motor Vehicle No-Fault Coverage Required by Law
If you are covered by both this Fund and any motor vehicle no-fault coverage that isrequired by law, the motor vehicle no-fault coverage pays first, and this Fund pays second.
Workers’ Compensation
This Fund does NOT provide benefits if the medical expenses are covered by Workers’Compensation or Occupational Disease Law.
R E I M B U R S E M E N T A N D S U B R O G AT I O N
You or one of your eligible dependents may incur medical expenses in a situation wherea third party—for example, Workers’ Compensation or an auto insurance carrier— maybe held responsible for their payment. In this case, the Fund has all rights of recoverythat you or your dependents would have, including the right to bring suit in your name.
You must cooperate with the Fund to secure the recovery of the payment, and you mustdo nothing before or after payment by the Fund to prejudice its rights. If you recover fromthe third party or its insurer, you must reimburse the Fund for expenses that it has paid.
When you and/or your eligible dependents incur medical expenses where a third partymay be held responsible for payment you must:
• Notify the Fund Office• Execute a Subrogation and reimbursement agreement
The subrogation and reimbursement agreement must be executed by you and/or yourcovered dependent, and received by the Fund Office within 90 days from the date of theincident and in no event later than 12 months from the date of the incident.
The amount of reimbursement due to the Fund is based on the following schedule:
Total Recovery Fund’s Share of Recovery
1. Equal or less than benefits 50% of the benefits
2. Greater than one, but less than twice benefits 65% of the benefits
3. Greater than two, but less than three times benefits 75% of the benefits
4. Greater than three, but less than four times benefits 85% of the benefits
5. Greater than four times 100% of the benefits
In no event shall the Fund’s share of recovery be greater than 50% of the total recovery following the deduction of the participant’s reasonable attorney’s fees (not to exceed 33% of the total recovery).
Before paying benefits for expenses that may be the responsibility of a third party, you and/or yourdependents will be required to sign an agreement affirming the obligation of you and your depend-ents to reimburse the Fund from the proceeds of any recovery. The Fund may withhold payments onany claim until a reimbursement agreement is executed. Your obligation to reimburse the Fund, how-ever, is not dependent on whether you sign a reimbursement agreement. By accepting the payment ofbenefits, you and your dependents agree to the Fund’s subrogation and reimbursement policies.
You and/or your eligible dependent must execute the reimbursement agreement and submit itfor receipt by the Fund Office within 90 days of the date of the accident or injury. If it is notreasonably possible to submit the executed reimbursement agreement within 90 days, it mustbe received by the Fund Office as soon as reasonably possible but in no event later than oneyear from the date of the accident or injury. If you fail to comply with this obligation to signand submit the reimbursement agreement within the deadline, the Fund will deny claims relat-ing to the accident or injury.
If you receive payment from a third party under any circumstances, you must reimburse theFund in accordance with the schedule above from the proceeds. Reimbursement is mandatoryregardless of whether:
• a claim was ever asserted for the amount received.
• the proceeds were paid by way of settlement, judgment, arbitration award or otherwise.
• you feel that you were “made whole” for your losses by recovery.
• the amount received is characterized as attributable to medical expenses, lost income, painand suffering, loss of consortium or otherwise.
• part of the recovery is received by family members other than the primary injured partysuch as on a loss of consortium.
The Fund has an equitable interest and lien in the amount that you receive, and you, yourdependents, and those acting on your behalf are under obligation to keep the amount receivedin a separate segregated account until your obligations to the Fund are satisfied and all dis-putes concerning those obligations are settled. The Fund may enforce this obligation by seek-ing equitable relief in court.
In the event that the participant or dependent submits additional claims for benefits followingsettlement of a liability claim and reimbursement to the Fund, the Fund will withhold futurebenefits, but only to the extent that the additional benefits would have been reimbursableunder the formula had the settlement occurred later.
If you or your dependents do not reimburse the Fund after receiving payment from a thirdparty, the Fund may institute legal and/or equitable action in court. In such event, you will beresponsible for all the costs and attorney’s fees associated with that court proceeding, and willbe obligated to pay all interest on all amounts owed from the date they were due. If you or adependent fails to reimburse the Fund, the Fund may withhold payment of future benefitsfrom you as well as all of your dependents up to the amount due plus interest.
57

58 FILING YOUR CLAIMS
A claim for benefits is a request for Plan benefits made in accordance with the Plan’sreasonable claims procedures. In order to file a claim for benefits offered under this Plan,you must submit a completed claim form unless your hospital, doctor or other healthcare provider uses a standard billing form, such as a UB 92 or HCFA 1500, and files itdirectly with the Fund on your behalf.
General inquiries about the Plan’s provisions that are unrelated to any specific benefitclaim or requests to add or improve the Plan’s benefits will not be treated as a claim forbenefits. In addition, a request for pre-approval of a benefit that does not require priorapproval by the Plan is not a claim for benefits.
All of the following information must be completed on the claim form that you get fromyour provider(s) in order for your request for benefits to be a claim, and for the FundOffice to be able to decide your claim.
• Member’s name and Social Securitynumber
• Member’s address• Member’s date of birth • Member’s marital status• Coordination of benefits information• Spouse’s name and Social Security
number (if applicable)• Spouse’s date of birth and
employment status (if applicable)• Name, address and telephone number
for spouse’s employer• Patient name and address (if different
from Member)• Patient’s relationship to insured• Patient date of birth• Patient’s sex• Patient’s student status• Was condition related to patient’s
employment, or accident• Date(s) of service• Date patient able to return to work
• Date of total/partial disability• Name of referring physician • Hospitalization dates, if applicable• CPT-4 (the code for physician
services and other health care servicesfound in the Current ProceduralTerminology, Fourth Edition or later, as maintained and distributedby the American Medical Association)
• ICD-9 (the diagnosis code found inthe International Classification of Diseases, 9th Edition or later, ClinicalModification as maintained anddistributed by the U.S. Department of Health and Human Services)
• Billed charge, amount paid andbalance due
• Signature of service provider• Federal taxpayer identification
number (TIN) of the provider• Provider billing name and address
Most accepted standard claim forms contain an assignment of benefits agreement, in theevent you wish to assign your hospital or surgical benefits directly to the hospital ordoctor. Upon receipt of the assignment agreement, the Fund Office will directly pay thesebenefits to your health care provider. Please remember that any CCN provider will bepaid directly by the Fund. You are only responsible for the copayment amount at thetime of the service and any coinsurance and deductible, depending on the benefit.
W H E N C L A I M S M U ST B E F I L E D
Claims should be filed within 90 days from the date the charges were incurred.
Failure to file claims within the time required shall not invalidate or reduce any claim ifit was not reasonably possible to file the claim within such time. However, in that case,the claim must be submitted as soon as reasonably possible and in no event later thanone year from the date the charges were incurred.
When you and/or your eligible dependents incur charges in circumstances where a thirdparty may be liable, you and/or your eligible dependent must:
• Notify the Fund Office.
• Execute and return a reimbursement agreement within 90 days of the accident orinjury. (See section of this book on Reimbursement and Subrogation).
W H E N A C L A I M I S C O N S I D E R E D R E C E I V E D BY T H E H E A LT H B E N E F I TS F U N D
Post-Service Claims
A post-service claim for benefits (as defined on page 62) is considered received by theFund as follows:
For Medical, Hospital, and Accident and Sickness (Disability) Claims
• On the first business day when the claim is received by U.S. mail or hand- deliveredto the Fund Office at the following address:
New England Carpenters Health Benefits Fund 350 Fordham RoadWilmington, MA 01887Phone: (800) 344-1515Fax: (978) 657-8724
• It is submitted electronically by your provider and received by the Health and WelfareFund.
For Dental Claims
• On the first business day when the claim is received by U.S. mail by Delta Dental atthe following address:
Delta Dental Plan of MassachusettsP.O. Box 9695Boston, MA 02114
• The claim is submitted electronically by your provider and received by Delta Dental.
For Vision Claims
• On the first business day when the claim is received by U.S. mail by Davis Vision atthe following address:
Davis Vision 159 Express St.Plainview, NY 11803
• The claim is submitted electronically by your provider and received by Davis Vision.
59

60
U R G E N T, P R E-S E R V I C E A N D C O N C U R R E N T C L A I M S
Urgent, pre-service and concurrent claims (as defined on pages 60-62) are generallyrequests for preauthorization or precertification of a treatment or hospital stay. Anurgent, pre-service or concurrent claim is considered received when a telephone call ismade by you or your provider to Hines & Associates at 1-800-944-9401, or yourprovider electronically contacts the Hines & Associates requesting precertification.
P R E S C R I P T I O N D R U G C L A I M S
Ullicare Rx/Medco provides drug preauthorizations for specified drugs. For a completelisting of these drugs, call (800) 818-6602.
When you present a prescription to a pharmacy to be filled under the terms of this Plan,that request is not a “claim” under these procedures. However, if your request for aprescription is denied, in whole or in part, you may file a claim and appeal regarding thedenial by using these procedures.
C L A I M S C O M M U N I C AT I O N S
All claims communications will be addressed to and sent to the Member unless the patientmakes a written request to the Health Benefits Fund Office specifically requesting that anyclaims communications be sent under the patient’s name and/or to a different address.
Authorized Representatives
An authorized representative, such as your spouse, may complete the claim form for youif you are unable to complete the form yourself and have designated an individual to acton your behalf. A form can be obtained from the Fund Office to designate an authorizedrepresentative. The Plan may request additional information to verify that this person isauthorized to act on your behalf. A health care professional with knowledge of your medicalcondition may act as an authorized representative in connection with an Urgent CareClaim (defined below) without you having to complete the special authorization form.
C O M P R E H E N S I V E M E D I C A L B E N E F I TS C L A I M S
The claims procedures for comprehensive medical benefits will vary depending onwhether your claim is for a Pre-Service Claim, an Urgent Care Claim, a ConcurrentCare Claim, a Post-Service Claim, or a Disability Claim. Read each section carefully todetermine which procedure is applicable to your request for benefits:
Pre-Service and Urgent Care Claims
A Pre-Service Claim is a claim for a benefit for which the Plan requires approval of thebenefit (in whole or in part) before medical care is obtained. Under this Plan, priorapproval of services is required for all hospital admissions, complementary medicine,home health care, hospice care, certain prescription drugs, inpatient and partial daymental/nervous disorders and alcohol/substance abuse disorders.

Important: Failure To Comply Could Result In A Minimum Penalty Of $500 ToComplete Denial Of The Claim.
The Fund has a contract with Hines & Associates to administer Pre-Service, Urgent andConcurrent Care Claims.
For properly filed Pre-Service Claims, you and/or your doctor will be notified of a deci-sion within 15 days from receipt of the claim unless additional time is needed. The timefor response may be extended up to an additional 15 days if necessary due to mattersbeyond the control of Hines & Associates. You will be notified of the circumstances requir-ing the extension of time and the date by which a decision is expected to be rendered.
If an extension is needed because Hines & Associates needs additional information fromyou, the extension notice will specify the information needed. In that case you and/oryour doctor will have 45 days from receipt of the notification to supply the additionalinformation. If the information is not provided within that time, your claim will bedenied. During the period in which you are allowed to supply additional information,the normal period for making a decision on the claim will be suspended. The deadline issuspended from the date of the extension notice until either 45 days or the date yourespond to the request (whichever is earlier). Hines & Associates then has 15 days tomake a decision on the Pre-Service Claim and notify you of the determination.
If you or your doctor improperly file a Pre-Service Claim, Hines & Associates will notifyyou as soon as possible but not later than 5 days after receipt of the claim, of the properprocedures to be followed in filing a claim. You will only receive notice of an improperlyfiled Pre-Service Claim if the claim includes (i) your name, (ii) your specific medicalcondition or symptom, and (iii) a specific treatment, service or product for whichapproval is requested. Unless the claim is re-filed properly, it will not constitute a claim.
An Urgent Care Claim is any claim for medical care or treatment with respect to whichthe application of the time periods for making Pre-Service claim determinations:
1. could seriously jeopardize the life or health of the claimant or the ability of theclaimant to regain maximum function, or
2. in the opinion of a physician with knowledge of the claimant’s medical condition,would subject the claimant to severe pain that cannot be adequately managedwithout the care or treatment that is the subject of the claim.
Any claim that a physician with knowledge of your medical condition determines is anUrgent Care Claim within the meaning described above, will be treated as an UrgentCare Claim. Absent a determination by that physician, whether your claim is an UrgentCare Claim will be determined by Hines & Associates applying the judgment of aprudent layperson who possesses an average knowledge of health and medicine.
If you are requesting precertification of an Urgent Care Claim, the time deadlines aredifferent than those that apply to Pre-Service Claims. Hines & Associates will respond toyou and/or your doctor with a determination by telephone as soon as possible takinginto account the medical condition, but not later than 72 hours after receipt of the claimby Hines & Associates. The determination will also be confirmed in writing.
61

62
If an Urgent Care Claim is received without sufficient information to determine whetheror to what extent benefits are covered or payable, Hines & Associates will notify youand/or your doctor as soon as possible, but not later than 24 hours after receipt of theclaim, of the specific information necessary to complete the claim. You and/or yourdoctor must provide the specified information within 48 hours of receiving notice. If theinformation is not provided within that time, your claim will be denied. Unless the claimis re-filed properly, it will not constitute a claim.
Notice of the decision will be provided no later than 48 hours after Hines & Associatesreceives the specified information or the end of the period given for you to provide thisinformation, whichever is earlier.
Concurrent Claims
A concurrent claim is a claim for additional treatment or hospital days or a claim that isreconsidered after an initial approval was made and results in a reduction, termination orextension of a benefit. (An example of this type of claim would be an inpatient hospitalstay originally approved for five days that is reviewed at three days to determine if thefull five days is appropriate.) In this situation a decision to reduce, terminate or extendtreatment is made at the same time or “concurrently” with the provision of treatment.
A reconsideration of a benefit with respect to a concurrent claim that involves the termina-tion or reduction of a previously approved benefit (other than by plan amendment or termi-nation) will be made by Hines & Associates as soon as possible, but in any event earlyenough to allow you to have an appeal decided before the benefit is reduced or terminated.
Any request by a claimant to extend approved urgent care treatment will be acted uponby Hines & Associates within 24 hours of receipt of the claim, provided the claim isreceived at least 24 hours prior to the expiration of the approved treatment. A request toextend approved treatment that does not involve urgent care will be decided according topre-service or post-service timeframes, whichever applies.
Post-Service Claim
The following procedure applies to Post-Service Claims. A Post-Service Claim is a claimthat is not a Pre-Service, Urgent Care, or Concurrent Claim (for example, a claimsubmitted for payment after health services and treatment have been obtained).
Your provider should submit all claims on your behalf to the Fund Office or to CCN. If you experience a problem submitting a claim, call the Fund Office.
You do not have to submit an additional claim form with your bills or statements, if youhave filed the annual health claim during the calendar year. Mail any further bills orstatements for any medical or hospital services covered by the Plan to the address shownon your I.D. Card as soon as you receive them. Your provider may also submit bills onyour behalf.
Ordinarily, you will be notified of the decision on your Post-Service Claim within 30days from the Plan’s receipt of the claim. This period may be extended once by the Planfor up to 15 days if the extension is necessary due to matters beyond the control of the

Plan. If an extension is necessary, you will be notified before the end of the initial 30-dayperiod of the circumstances requiring the extension of time and the date by which thePlan expects to render a decision.
If an extension is needed because the Plan needs additional information from you, theextension notice will specify the information needed. In that case you will have 45 daysfrom receipt of the notification to supply the additional information. If the information isnot provided within that time, your claim is deemed denied. During the period in whichyou are allowed to supply additional information, the normal period for making adecision on the claim will be suspended. The deadline is suspended from the date of theextension notice until either 45 days or until the date you respond to the request(whichever is earlier). The Plan then has 15 days to make a decision on a Post-ServiceClaim and notify you of the determination.
D I S A B I L I T Y C L A I M S ( W E E K LY AC C I D E N T A N D S I C K N E S S B E N E F I T )
You must file a claim for Weekly Accident and Sickness Benefits with the Fund Office nolater than 90 days after the date your disability began.
For Disability Claims, the Plan will make a decision on the claim and notify you of thedecision within 45 days. If the Plan requires an extension of time due to matters beyondthe control of the Plan, the Plan will notify you of the reason for the delay and when thedecision will be made. This notification will occur before the expiration of the 45-dayperiod. A decision will be made within 30 days of the time the Plan notifies you of thedelay. The period for making a decision may be delayed an additional 30 days, providedthe Plan administrator notifies you, prior to the expiration of the first 30-day extensionperiod, of the circumstances requiring the extension and the date as of which the Planexpects to render a decision.
If an extension is needed because the Plan needs additional information from you, theextension notice will specify the information needed. In that case you will have 45 daysfrom receipt of the notification to supply the additional information. If the information isnot provided within that time, your claim will be denied. During the period in which youare allowed to supply additional information, the normal period for making a decision onthe claim will be suspended. The deadline is suspended from the date of the extensionnotice until either 45 days or until the date you respond to the request (whichever isearlier). Once you respond to the Plan’s request for the information, you will be notifiedof the Plan’s decision on the claim, or the need for an extension, within 30 days.
Notice Of A Denied Claim
You will be provided with written notice of a denial of a claim (whether denied in wholeor in part). This notice will state:
• The specific reason(s) for the determination.
• Reference to the specific Plan provision(s) on which the determination is based.
• A description of any additional material or information necessary to perfect theclaim, and an explanation of why the material or information is necessary.
63

64
• A description of the appeal procedures (including voluntary appeals, if any) andapplicable time limits.
• A statement of your right to bring a civil action under ERISA Section 502(a) followingan adverse benefit determination on review.
• If an internal rule, guideline or protocol was relied upon in deciding your claim, you willreceive either a copy of the rule or a statement that it is available upon request at no charge.
• If the determination was based on the absence of medical necessity, or because the treat-ment was experimental or investigational, or other similar exclusion, you will receive anexplanation of the scientific or clinical judgment for the determination applying the termsof the Plan to your claim, or a statement that it is available upon request at no charge.
Appeal Process for Denied Claims
If your claim is denied in whole or in part, or if you disagree with the decision made on a claim,you may ask for a review. Your request for review must be made in writing to the Fund Officeand must be received within 180 days after you receive a notice of denial. Appeals involvingUrgent Care Claims may be made orally by calling the Fund Administrator at (800) 344-1515for urgent and concurrent claim appeals only. There is a second level of appeal for Post-Service and Disability claims, and appeals to the second level concerning those claims must bereceived by the Fund Office within 60 days of the date of the decision at the first level of appeal.
A P P E A L P R O C E S S
The appeal process works as follows:
Urgent, Pre-Service and Concurrent Claim Appeals
For Urgent, Pre-Service and Concurrent Claim Appeals, there is one level of appeal.Appeals should be made in writing to the Fund Office. A subcommittee of the Board ofTrustees will review Urgent, Pre-Service and Concurrent Claim appeals. In certaincircumstances such as Urgent Claim appeals where medical conditions exist that require anexpedited review process, appeals may be made orally via telephone.
Post-Service and Disability Claim Appeals
For Post-Service and Disability claims appeals, there is a two-level appeal process. Appeals atboth levels must be in writing and must be submitted to the Fund Office. The first level ofappeal will consist of a review by the Fund Administrator. First level appeals must bereceived by the Fund Office within 180 days after you receive the Fund’s notice of its denialof your claim. If the Fund Administrator denies your first level appeal, you have the right to asecond level appeal to the full Board of Trustees. Second level appeals must be received by theFund Office within 60 days of the date of the Fund Administrator’s decision at the first level.
Information To Which You Are Entitled
You have the right to review documents relevant to your claim. A document, record orother information is relevant if it was relied upon by the Plan in making the decision; it wassubmitted, considered or generated (regardless of whether it was relied upon in making thedecision); it demonstrates compliance with the Plan’s administrative processes for ensuringconsistent decision making; or it constitutes a statement of Plan policy regarding the deniedtreatment or service.

Upon request, you will be provided with the identification of medical or vocationalexperts, if any, who gave advice to the Plan on your claim, without regard to whethertheir advice was relied upon in deciding your claim.
A different person will review your claim than the one who originally denied the claim orthe previous appeal. The reviewer will not give deference to the previous adverse benefitdeterminations. The decision will be made on the basis of the record, including suchadditional documents and comments that may be submitted by you.
If your claim was denied on the basis of a medical judgment (such as a determinationthat the treatment or service was not medically necessary, or was investigational orexperimental), a health care professional who has appropriate training and experience ina relevant field of medicine will be consulted.
Timing of Notice of Decision on Appeal
• Pre-Service Claims: You will be sent a notice of decision on review within 30 days ofreceipt of the appeal by the Fund Office.
• Urgent Care Claims: You will be notified of a decision on your appeal, either orallyor in writing (or both) within 72 hours of receipt of the appeal by the Fund Office.
• Post-Service Claims: For first level appeals, a decision will be made on the appealwithin 30 days of receipt of the appeal by the Fund Administrator. For second levelappeals, decisions will be made at the next regularly scheduled meeting of the Boardof Trustees following receipt of your request for review. However, if your request forreview is received within 30 days of the next regularly scheduled meeting, yourrequest for review will be considered at the second regularly scheduled meetingfollowing receipt of your request. In special circumstances, a delay until the thirdregularly scheduled meeting following receipt of your request for review may benecessary. You will be advised in writing in advance if this extension will benecessary. Once a decision on review of your claim has been reached, the Fund Officewill give you written notice of the decision as soon as possible, but no later than 5days after the decision has been reached.
• Disability Claims: For first level disability claim appeals a decision will be made bythe Fund Administrator within 45 days of receipt of the appeal at the Fund Office. Ifthe Fund Administrator determines that special circumstances require an extensionof time, then you will receive a written notice of the extension before the end of the45-day period. The notice will include the reasons required for the extension and theapproximate date the Plan expects to make a decision.
For second level appeals, decisions will be made at the next regularly scheduledmeeting of the Board of Trustees following receipt of your request for review.However, if your request for review is received within 30 days of the next regularlyscheduled meeting, your request for review will be considered at the second regularlyscheduled meeting following receipt of your request. In special circumstances, a delayuntil the third regularly scheduled meeting following receipt of your request forreview may be necessary. You will be advised in writing in advance if this extension
65

66
will be necessary. Once a decision on review of your claim has been reached, the FundOffice will give you written notice of the decision as soon as possible, but no later than 5days after the decision has been reached.
• Concurrent Claims: Appeals of concurrent claims involving a termination or reductionof benefits of previously approved care shall be completed before the termination orreduction. The claimant shall be given notice sufficiently in advance of the terminationor reduction to allow the claimant to appeal before the benefit is terminated or reduced.Appeals of concurrent claims involving an extension of care shall be conducted withinthe timeframe for urgent, pre-service or post-service appeals described above, dependingon which category applies to the appeal.
Notice of Decision on Review
The decision on any review of your claim will be given to you in writing. The notice of adenial of a claim on review will state:
• The specific reason(s) for the determination.
• Reference to the specific Plan provision(s) on which the determination is based.
• A statement that you are entitled to receive reasonable access to and copies of alldocuments relevant to your claim, upon request and free of charge.
• A statement of your right to bring a civil action under ERISA Section 502(a) followingan adverse benefit determination on review.
• If an internal rule, guideline or protocol was relied upon by the Plan, you will receiveeither a copy of the rule or a statement that it is available upon request at no charge.
• If the determination was based on medical necessity, or because the treatment was experi-mental or investigational, or other similar exclusion, you will receive an explanation ofthe scientific or clinical judgment for the determination applying the terms of the Planto your claim, or a statement that it is available upon request at no charge.
Limitation on When a Lawsuit May Be Started
You may not start a lawsuit to obtain benefits until after you have exhausted all levels ofappeal and final decisions have been reached on those appeals, or until the appropriate timeframe described above has elapsed since you filed a request for review and you have receiveda final decision or notice that an extension will be necessary to reach a final decision. Thelaw also permits you to pursue your remedies under section 502(a) of the EmployeeRetirement Income Security Act without exhausting these appeal procedures if the Plan hasfailed to follow them. No lawsuit to recover Plan benefits may be started more than 15months after the date of loss (that is, the date you incurred the expense you are seeking tohave the Plan pay) upon which the lawsuit is based. Because the Plan grants its fiduciariesdiscretionary authority to determine eligibility for benefits and to construe the terms of thePlan, the issue in a lawsuit will be limited to whether or not the Board of Trustees (or itsdelegates, including the subcommittee for Urgent Care, Pre-service and Concurrent Claims)acted arbitrarily or capriciously in making its determination. No lawsuit to recover Planbenefits may be started more than 12 months after the date the Board of Trustees makes itsfinal decision on an appeal, or after the date the Fund was required but failed to act inaccordance with its appeal procedures.

YOUR ERISA RIGHTS
As a participant in the New England Carpenters Health Benefits Fund, you are entitled tocertain rights and protections under the Employee Retirement Income Security Act of1974 (ERISA). ERISA provides that all Plan participants are entitled to:
Receive Information About Your Plan and Benefits
• Examine, without charge, at the Fund Administrator’s office and at other specifiedlocations, such as worksites and union halls, all documents governing the Plan,including insurance contracts and Collective Bargaining Agreements, and a copy ofthe latest annual report (Form 5500 Series) filed by the Fund with the U.S.Department of Labor and available at the Public Disclosure Room of the EmployeeBenefits Security Administration.
• Obtain, upon written request to the Fund Administrator, copies of documentsgoverning the operation of the Plan, including insurance contracts and CollectiveBargaining Agreements, and copies of the latest annual report (Form 5500 Series)and updated Summary Plan Description. The Administrator may make a reasonablecharge for the copies.
• Receive a summary of the Fund’s annual financial report. The Fund Administrator isrequired by law to furnish each participant with a copy of this summary annual report.
• Continue health care coverage for yourself, spouse or dependents if there is a loss ofcoverage under the Plan as a result of a qualifying event. You or your dependentsmay have to pay for such coverage. Review this Summary Plan Description and thedocuments governing the Plan on the rules governing your COBRA ContinuationCoverage rights.
• Reduce or eliminate exclusionary periods of coverage for pre-existing conditionsunder your group health plan, if you have creditable coverage from another plan.When you lose coverage under the New England Carpenters Health Benefits Fund,your group health plan or health insurance issuer should provide you with acertificate of creditable coverage, free of charge when: – You become entitled to elect COBRA Continuation Coverage, – Your COBRA coverage ceases, if you request it before losing coverage, or if you
request it up to 24 months after losing coverage.
Prudent Actions By Plan Fiduciaries
In addition to creating rights for Fund participants, ERISA imposes duties upon thepeople who are responsible for the operation of the employee benefit plan. The peoplewho operate your Fund, called “fiduciaries” of the Fund, have a duty to do so prudentlyand in the interest of you and other Fund participants and beneficiaries. No one,including your employer, your union, or any other person, may fire you or otherwisediscriminate against you in any way to prevent you from obtaining a welfare benefit orexercising your rights under ERISA.
Enforce Your Rights
If your claim is denied or ignored, in whole or in part, you have a right to know why thiswas done, to obtain copies of documents relating to the decision without charge, and toappeal any denial, all within certain time schedules.
67

Under ERISA, there are steps you can take to enforce the above rights. For instance, ifyou request a copy of the Plan documents or the latest annual report from the Fund anddo not receive them within 30 days, you may file suit in a federal court. In such a case,the court may require the Fund Administrator to provide the materials and pay you up to$110 a day until you receive the materials, unless the materials were not sent because ofreasons beyond the control of the Administrator.
If you have a claim for benefits that is denied or ignored, in whole or in part, you mayfile suit in a state or federal court. In addition, if you disagree with the Fund’s decision orlack thereof concerning the qualified status of a domestic relations order or a medicalchild support order, you may file suit in federal court. If it should happen that Fundfiduciaries misuse the Fund’s money, or if you are discriminated against for assertingyour rights, you may seek assistance from the U.S. Department of Labor, or you may filesuit in a federal court. The court will decide who should pay court costs and legal fees. Ifyou are successful the court may order the person you have sued to pay these costs andfees. If you lose, the court may order you to pay these costs and fees, for example if itfinds your claim is frivolous.
Assistance with Your Questions
If you have any questions about your Plan, you should contact the Fund Administrator.If you have any questions about this statement or about your rights under ERISA, or ifyou need assistance in obtaining documents from the Fund Administrator, you shouldcontact the nearest office of the Employee Benefits Security Administration, U.S.Department of Labor, listed in your telephone directory or the Division of TechnicalAssistance and Inquiries, Pension and Welfare Benefits Administration, U.S. Departmentof Labor, 200 Constitution Avenue, N.W., Washington D.C. 20210. You may also obtaincertain publications about your rights and responsibilities under ERISA by calling thepublications hotline at the Employee Benefits Security Administration.
68

69
Name of Plan The New England Carpenters Health Benefits Fund
Type of Plan A self-funded Employee Health and Welfare Benefit Plan thatprovides coverage for medical care, prescription drugs, dental care,vision care, weekly accident and sickness benefits, life insurance andaccidental death and dismemberment benefits to eligible membersand their qualified dependents.
Name of Plan Sponsor Board of TrusteesNew England Carpenters Health Benefits Fund
Fund Office Address 350 Fordham Road, Wilmington, MA 01887
Agent for Service of Service of legal process may be made upon any Fund Trustee. Legal Process
Plan Administrator Board of TrusteesNew England Carpenters Health Benefits Fund
Type of Administration Collectively Bargained, jointly trusteed labor management trust of the Plan
Plan Number 501
IRS Employer 04-2191579 Identification Number
Plan Fiscal Year January 1—December 31
Sources of Financing Payments made to the trust by individual employers under theprovisions of the Collective Bargaining or Participation Agreements,employee contributions, and any income earned from investment ofemployer and employee contributions.
The Fund Office will provide you, upon written request, withinformation as to whether a particular employer is contributing to thisPlan on behalf of Participants working under the Collective BargainingAgreement and, if so, with that employer’s address.
All monies are used exclusively for providing benefits to eligibleemployees, early retirees, and their dependents, and the paying of allexpenses incurred with respect to the operation of the Plan. TheTrustees shall review annually the funding status of the Plan.
Organizations Through Which Plan Benefits
are Provided or Administered
PPO Network Access Only Medical CareCCN
PPO Network Access Only Substance Abuse and Mental Health CCN
Utilization Review Vendor Hines & Associates
Self-funded Prescription Drugs Ullicare Rx/Medco
Self-funded, Network Dental Care access and dental claims Delta Dental administration
Self-funded benefit, Vision CareNetwork access and vision Davis Vision claims administration
Insurance Policies Life Insurance and Accidental Death and Dismemberment Insurance–Hartford Life Insurance Company
PLAN FACTS
The Board of Trustees
The Board of Trustees is made up of an equal number of Representatives and UnionRepresentatives who serve without compensation. Under a Trust Agreement, the Boardhas full authority and discretion to operate and administer this Plan.
Discretionary Authority of the Board of Trustees and its Designees
In carrying out their respective responsibilities under the Plan, the Board of Trustees, theFund Administrator and other individuals with delegated responsibility for theadministration of the Plan will have discretionary authority to interpret the terms of thePlan and to determine eligibility and entitlement to Plan benefits in accordance with theterms of the Plan. Any interpretation or determination will be given full force and effect,unless it can be shown that the interpretation or determination was arbitrary andcapricious.
Collective Bargaining Agreement
A collective bargaining agreement is a written agreement between a union and anemployer that requires the employer to make contributions to the Fund on behalf of itsemployees. To inquire about whether a particular employer contributes to this Fund, orto request a copy of the collective bargaining agreement, contact the Fund Office.
Plan Amendment and Termination
The Board of Trustees reserves the right to terminate or amend the Plan including theright to amend or terminate benefits or eligibility for any class of participant, includingretirees, when in their sole discretion they determine such action is in the best interest ofthe Fund and its participants. Eligibility requirements are reviewed regularly by theTrustees.
In addition, the Plan may be terminated by the Trustees if there is no longer anagreement in effect between the Employers and the Union requiring contributions to theHealth Benefits Fund.
Should the Plan terminate, the Trustees will apply remaining assets of the Fund tocontinue benefits beyond the date of termination. The Trustees reserve the right toamend the eligibility rules at the time of termination. Retiree benefits are funded fromcurrent contributions and are not guaranteed or vested. In any case, the Trustees will useany remaining assets of the Fund to provide benefits and pay administration expenses orotherwise to carry out the purpose of the Plan in accordance with the Plan Documentand Trustee Agreement until the entire remainder of the Fund has been disbursed.
70

SCHEDULE OF BENEFITS FOR PLAN I
The chart that follows highlights the benefits of the New England Carpenters HealthBenefits Fund. For more detailed information, contact the Fund Office.
Your Calendar Year Deductible $150 per person$300 per family
Your Calendar Year Out-of-Pocket Maximum $1,500 per person
Maximum Benefit the Plan Will Pay Per Person Per Lifetime $1,000,000
The Life Insurance benefit is available to members and spouses. Accidental Death and Dismemberment and Weekly Accident and Sickness benefits are available toMembers only.
Life Insurance $20,000 for Member; $2,000 for spouse
Accidental Death and Dismemberment Refer to page 49
Weekly Accident and Sickness $250 per week for up to 26 weeks per period of disability
The following schedule shows the percentage of charges that the Fund pays under Plan I,whether medical services are obtained in the PPO network or out-of-network. Note:Charges for benefits provided by PPO network providers are based on a negotiatedcontract. Charges for benefits provided by out-of-network providers are based onreasonable and customary rates as described on page 27. You are responsible for anyprovider charges in excess of reasonable and customary rates.
Plan Pays Plan Pays
PPO Network Out-of-Network
Ambulance Service 90% after deductible. 85% after deductible.Air Ambulance service payable Air Ambulance service payable at 90% after deductible to a at 85% after deductible to a maximum of $2,000 per maximum of $2,000 per life-threatening emergency life-threatening emergency
Cardiac Rehabilitation 90% after deductible when 85% after deductible when medically necessary following medically necessary following heart attack or stroke, upon heart attack or stroke, upon recommendation of and with recommendation of and with supervision of attending physician, supervision of attending physician, to a lifetime maximum of $3,000 to a lifetime maximum of $3,000
Chiropractic Care 100% after $10 copay per visit 85% after deductible to a to a calendar year maximum of calendar year maximum of 20 visits per person 20 visits per person
71
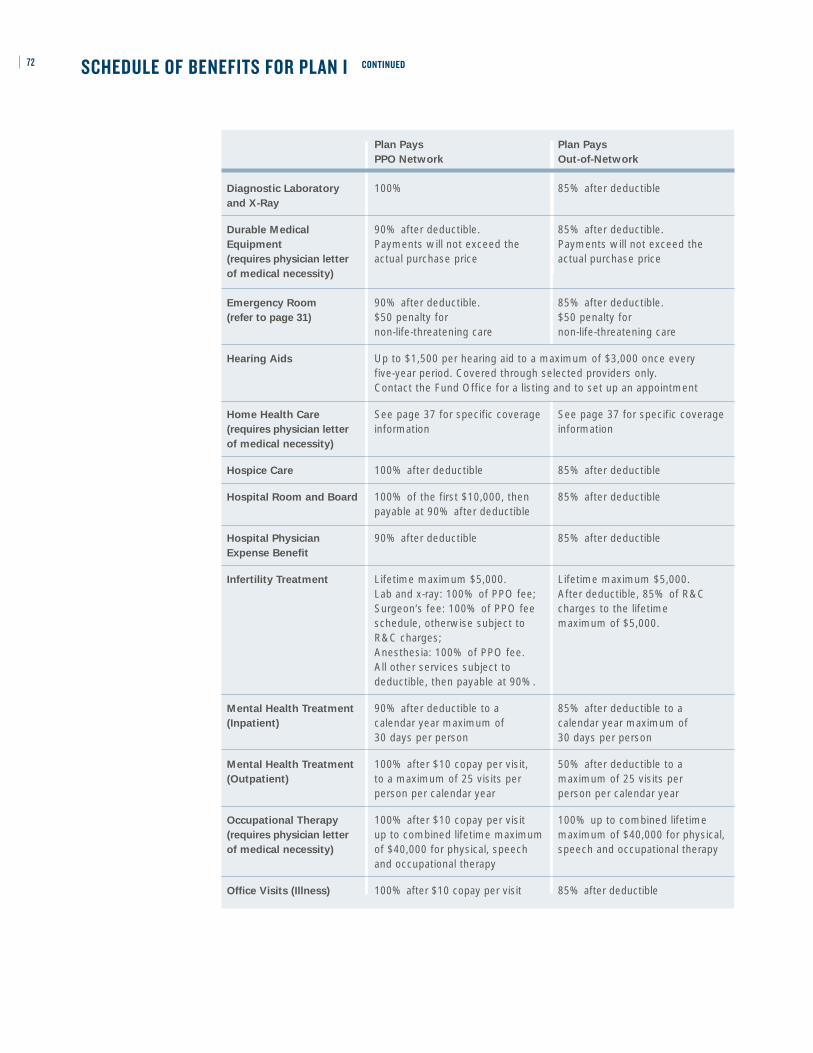
72
Plan Pays Plan Pays
PPO Network Out-of-Network
Diagnostic Laboratory 100% 85% after deductible and X-Ray
Durable Medical 90% after deductible. 85% after deductible.Equipment Payments will not exceed the Payments will not exceed the (requires physician letter actual purchase price actual purchase price of medical necessity)
Emergency Room 90% after deductible. 85% after deductible. (refer to page 31) $50 penalty for $50 penalty for
non-life-threatening care non-life-threatening care
Hearing Aids Up to $1,500 per hearing aid to a maximum of $3,000 once every five-year period. Covered through selected providers only. Contact the Fund Office for a listing and to set up an appointment
Home Health Care See page 37 for specific coverage See page 37 for specific coverage (requires physician letter information informationof medical necessity)
Hospice Care 100% after deductible 85% after deductible
Hospital Room and Board 100% of the first $10,000, then 85% after deductible payable at 90% after deductible
Hospital Physician 90% after deductible 85% after deductible Expense Benefit
Infertility Treatment Lifetime maximum $5,000. Lifetime maximum $5,000. Lab and x-ray: 100% of PPO fee; After deductible, 85% of R&C Surgeon’s fee: 100% of PPO fee charges to the lifetime schedule, otherwise subject to maximum of $5,000. R&C charges;Anesthesia: 100% of PPO fee. All other services subject to deductible, then payable at 90%.
Mental Health Treatment 90% after deductible to a 85% after deductible to a (Inpatient) calendar year maximum of calendar year maximum of
30 days per person 30 days per person
Mental Health Treatment 100% after $10 copay per visit, 50% after deductible to a (Outpatient) to a maximum of 25 visits per maximum of 25 visits per
person per calendar year person per calendar year
Occupational Therapy 100% after $10 copay per visit 100% up to combined lifetime (requires physician letter up to combined lifetime maximum maximum of $40,000 for physical, of medical necessity) of $40,000 for physical, speech speech and occupational therapy
and occupational therapy
Office Visits (Illness) 100% after $10 copay per visit 85% after deductible
SCHEDULE OF BENEFITS FOR PLAN I CONTINUED

73
Plan Pays Plan Pays
PPO Network Out-of-Network
Organ Transplants $250,000 per transplant maximum. $250,000 per transplant maximum.Hospital: 100% of the first $10,000 Hospital: 85% after deductible then 90% after deductible Surgeon’s fee: 85% of R&C Surgeon’s fee: 100% of PPO fee charges after deductibleschedule otherwise subject to Anesthesia: 85% of charges R&C charges. after deductibleAnesthesia: 100% of PPO fee schedule
Physical Exams Covered for Member and spouse only(includes all lab, x-ray Paid at 100% up to calendar year maximum of $150and immunizations)
Physical Therapy 100% after $10 copay per visit, up 85% after deductible, up to (requires physician letter to a combined lifetime maximum a combined lifetime maximum of medical necessity) of $40,000 for physical, speech of $40,000 for physical, speech
and occupational therapy and occupational therapy
Podiatrist Services 100% after $10 copay to a calendar 85% after deductible to a calendar year maximum of $500 per person year maximum of $500 per person
Prescription Drugs $20 copay for generics, $40 for Brand Preferred and $60 for (Mail Order, 90-day supply) Brand Non-Preferred
Prescription Drugs $10 copay for generics, $20 for Brand Preferred and $30 for Brand (Retail, 34-day supply) Non-Preferred
Skilled Nursing Facility 100% of the first $10,000 then 85% after deductible payable at 90% after deductible
Speech Therapy 90% after deductible up to a 85% after deductible up to a(requires physician letter combined lifetime maximum of combined lifetime maximum of of medical necessity) $40,000 for physical, speech and $40,000 for physical, speech
occupational therapy and occupational therapy
Substance Abuse 90% after deductible to a 85% after deductible to a Treatment (Inpatient) maximum of 30 days per person maximum of 30 inpatient days
per calendar year. per calendar year per person. Maximum of two lifetime Maximum of two lifetimeoccurrences per person occurrences per person
Substance Abuse 100%, after a $10 copay, to a 85% after deductible to a Treatment (Outpatient) maximum of $500 per person maximum of $500 per person
per calendar year per calendar year
Surgeon’s Expenses 100% of PPO fee schedule 85% of R&C charges after otherwise subject to R&C deductible schedule
Temporomandibular 100% after a $10 copay to a 85% after deductible to a Joint Disorders (TMJ) lifetime maximum of $1,500, lifetime maximum of $1,500,
within limitations covered under within limitations covered under Plan exclusions (page 52) Plan exclusions (page 52)
Well-Child Care 100% after a $10 copayment for children from birth through age 5;(includes all lab, x-ray For children 6 and older, 100% to a calendar year maximum of $70 and immunizations) until they turn 19 (or through 23 if a full-time student)
SCHEDULE OF BENEFITS FOR PLAN I CONTINUED
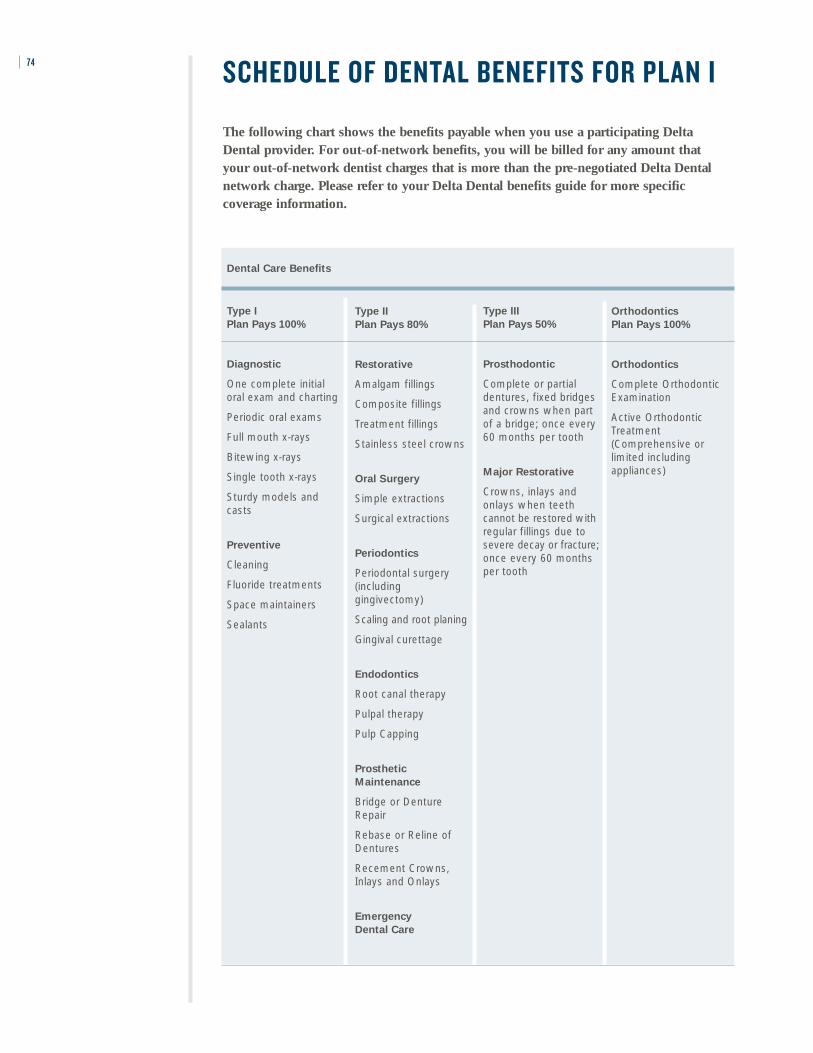
SCHEDULE OF DENTAL BENEFITS FOR PLAN I
The following chart shows the benefits payable when you use a participating DeltaDental provider. For out-of-network benefits, you will be billed for any amount that your out-of-network dentist charges that is more than the pre-negotiated Delta Dentalnetwork charge. Please refer to your Delta Dental benefits guide for more specificcoverage information.
74
Dental Care Benefits
Type I
Plan Pays 100%
Diagnostic
One complete initialoral exam and charting
Periodic oral exams
Full mouth x-rays
Bitewing x-rays
Single tooth x-rays
Sturdy models andcasts
Preventive
Cleaning
Fluoride treatments
Space maintainers
Sealants
Type II
Plan Pays 80%
Restorative
Amalgam fillings
Composite fillings
Treatment fillings
Stainless steel crowns
Oral Surgery
Simple extractions
Surgical extractions
Periodontics
Periodontal surgery(includinggingivectomy)
Scaling and root planing
Gingival curettage
Endodontics
Root canal therapy
Pulpal therapy
Pulp Capping
Prosthetic
Maintenance
Bridge or DentureRepair
Rebase or Reline ofDentures
Recement Crowns,Inlays and Onlays
Emergency
Dental Care
Type III
Plan Pays 50%
Prosthodontic
Complete or partialdentures, fixed bridgesand crowns when partof a bridge; once every60 months per tooth
Major Restorative
Crowns, inlays andonlays when teethcannot be restored withregular fillings due tosevere decay or fracture;once every 60 monthsper tooth
Orthodontics
Plan Pays 100%
Orthodontics
Complete OrthodonticExamination
Active OrthodonticTreatment(Comprehensive orlimited includingappliances)
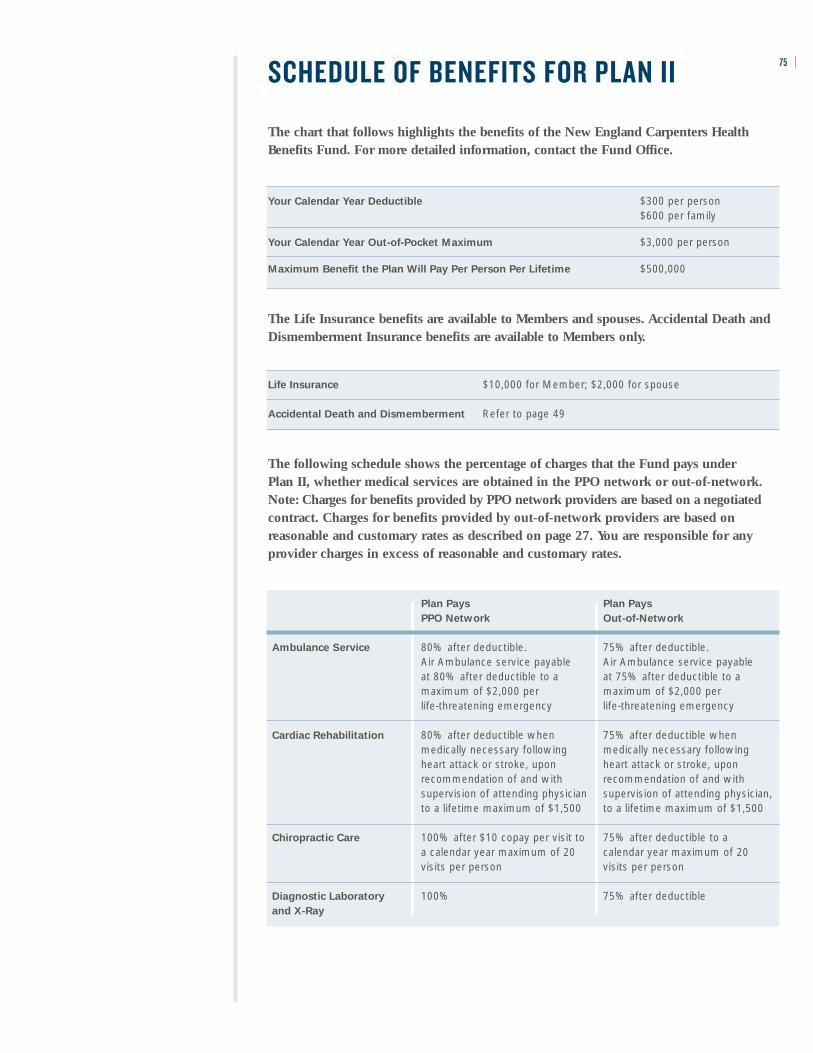
SCHEDULE OF BENEFITS FOR PLAN II
The chart that follows highlights the benefits of the New England Carpenters HealthBenefits Fund. For more detailed information, contact the Fund Office.
Your Calendar Year Deductible $300 per person$600 per family
Your Calendar Year Out-of-Pocket Maximum $3,000 per person
Maximum Benefit the Plan Will Pay Per Person Per Lifetime $500,000
The Life Insurance benefits are available to Members and spouses. Accidental Death andDismemberment Insurance benefits are available to Members only.
Life Insurance $10,000 for Member; $2,000 for spouse
Accidental Death and Dismemberment Refer to page 49
The following schedule shows the percentage of charges that the Fund pays under Plan II, whether medical services are obtained in the PPO network or out-of-network. Note: Charges for benefits provided by PPO network providers are based on a negotiatedcontract. Charges for benefits provided by out-of-network providers are based onreasonable and customary rates as described on page 27. You are responsible for anyprovider charges in excess of reasonable and customary rates.
75
Plan Pays Plan Pays
PPO Network Out-of-Network
Ambulance Service 80% after deductible. 75% after deductible. Air Ambulance service payable Air Ambulance service payable at 80% after deductible to a at 75% after deductible to a maximum of $2,000 per maximum of $2,000 per life-threatening emergency life-threatening emergency
Cardiac Rehabilitation 80% after deductible when 75% after deductible when medically necessary following medically necessary following heart attack or stroke, upon heart attack or stroke, upon recommendation of and with recommendation of and with supervision of attending physician supervision of attending physician, to a lifetime maximum of $1,500 to a lifetime maximum of $1,500
Chiropractic Care 100% after $10 copay per visit to 75% after deductible to a a calendar year maximum of 20 calendar year maximum of 20 visits per person visits per person
Diagnostic Laboratory 100% 75% after deductible and X-Ray
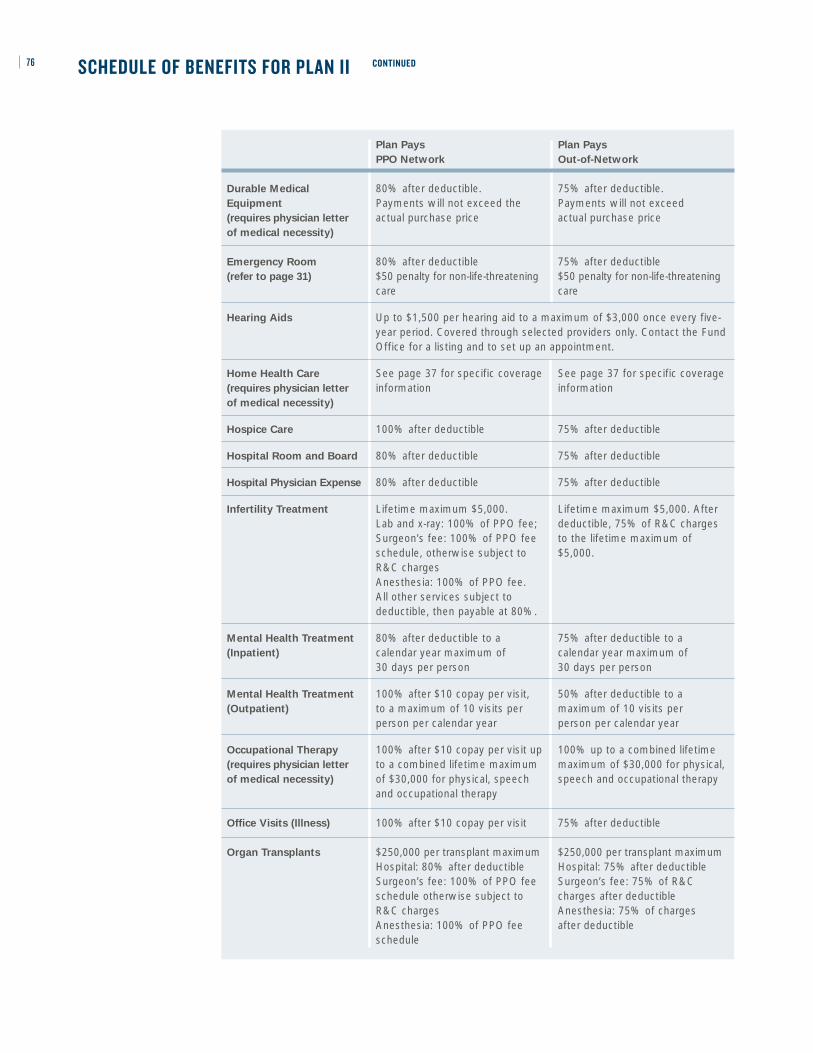
76
Plan Pays Plan Pays
PPO Network Out-of-Network
Durable Medical 80% after deductible. 75% after deductible. Equipment Payments will not exceed the Payments will not exceed (requires physician letter actual purchase price actual purchase price of medical necessity)
Emergency Room 80% after deductible 75% after deductible(refer to page 31) $50 penalty for non-life-threatening $50 penalty for non-life-threatening
care care
Hearing Aids Up to $1,500 per hearing aid to a maximum of $3,000 once every five-year period. Covered through selected providers only. Contact the FundOffice for a listing and to set up an appointment.
Home Health Care See page 37 for specific coverage See page 37 for specific coverage(requires physician letter information information of medical necessity)
Hospice Care 100% after deductible 75% after deductible
Hospital Room and Board 80% after deductible 75% after deductible
Hospital Physician Expense 80% after deductible 75% after deductible
Infertility Treatment Lifetime maximum $5,000. Lifetime maximum $5,000. After Lab and x-ray: 100% of PPO fee; deductible, 75% of R&C charges Surgeon’s fee: 100% of PPO fee to the lifetime maximum of schedule, otherwise subject to $5,000. R&C chargesAnesthesia: 100% of PPO fee. All other services subject to deductible, then payable at 80%.
Mental Health Treatment 80% after deductible to a 75% after deductible to a (Inpatient) calendar year maximum of calendar year maximum of
30 days per person 30 days per person
Mental Health Treatment 100% after $10 copay per visit, 50% after deductible to a (Outpatient) to a maximum of 10 visits per maximum of 10 visits per
person per calendar year person per calendar year
Occupational Therapy 100% after $10 copay per visit up 100% up to a combined lifetime (requires physician letter to a combined lifetime maximum maximum of $30,000 for physical, of medical necessity) of $30,000 for physical, speech speech and occupational therapy
and occupational therapy
Office Visits (Illness) 100% after $10 copay per visit 75% after deductible
Organ Transplants $250,000 per transplant maximum $250,000 per transplant maximumHospital: 80% after deductible Hospital: 75% after deductible Surgeon’s fee: 100% of PPO fee Surgeon’s fee: 75% of R&C schedule otherwise subject to charges after deductible R&C charges Anesthesia: 75% of charges Anesthesia: 100% of PPO fee after deductibleschedule
SCHEDULE OF BENEFITS FOR PLAN II CONTINUED

77
Plan Pays Plan Pays
PPO Network Out-of-Network
Physical Exams Covered for Member and spouse only(includes all lab, x-ray Paid at 100% to a calendar year maximum of $75and immunizations)
Physical Therapy 100% after $10 copay per visit, up 75% after deductible, up (requires physician letter to a combined lifetime maximum to a combined lifetime maximum of medical necessity) of $30,000 for physical, speech of $30,000 for physical, speech
and occupational therapy and occupational therapy
Podiatrist Services 100% after $10 copay to a calendar 75% after deductible to a calendar year maximum of $500 per person year maximum of $500 per person
Prescription Drugs $20 copay for generics, $40 for Brand Preferred and $60 for Brand (Mail Order, 90-day supply) Non-Preferred
Prescription Drugs $10 copay for generics, $20 for Brand Preferred and $30 for Brand (Retail, 34-day supply) Non-Preferred
Skilled Nursing Facility 80% after deductible 75% after deductible
Speech Therapy 80% after deductible up to a 75% after deductible up to a(requires physician letter combined lifetime maximum of combined lifetime maximum of of medical necessity) $30,000 for physical, speech and $30,000 for physical, speech and
occupational therapy occupational therapy
Substance Abuse 80% after deductible to a 75% after deductible to a Treatment (Inpatient) maximum of 30 days per person maximum of 30 days per person
per calendar year. per calendar year. Maximum of two lifetime Maximum of two lifetimeocurrences per person ocurrences per person
Substance Abuse 100% after $10 copay to a 75% after deductible to a Treatment (Outpatient) maximum of $500 per person per maximum of $500 per person
calendar year per calendar year
Surgeon’s Expenses 100% of PPO fee schedule 75% of R&C charges after otherwise subject to R&C charges deductible
Temporomandibular 100% after $10 copay to a lifetime 75% after deductible to a lifetime Joint Disorders (TMJ) maximum of $1,000 within maximum of $1,000 within
limitations covered under limitations covered underPlan Exclusions (page 52) Plan Exclusions (page 52)
Well-Child Care 100% after $10 copayment Not covered (includes all lab, x-ray for children from birth and immunizations) through age 5; not covered for
children age 6 and older
SCHEDULE OF BENEFITS FOR PLAN II CONTINUED

SCHEDULE OF BENEFITS FOR THE RETIREE PLAN
The chart that follows highlights the benefits of the New England Carpenters Health BenefitsFund. For more detailed information, contact the Fund Office.
Your Calendar Year Deductible $250 per individual
Your Calendar Year Out-of-Pocket Maximum $3,000 per individual
Maximum Benefit the Plan Will Pay Per Person Per Lifetime $1,000,000
!! YOU MUST USE THE PPO NETWORK TO RECEIVE BENEFITS FROM THE RETIREE PLAN
UNLESS YOU LIVE OUTSIDE A 20-MILE RADIUS FROM A PREFERRED PROVIDER.
78
Plan Pays Out-of-Area
PPO Network Benefits
Ambulance Service 80% after deductible. Air Ambulance service payable at 80% afterdeductible to a maximum of $2,000 per life-threatening emergency
Cardiac Rehabilitation 80% after deductible, when 80% after deductible when medically necessary following medically necessary following heart attack or stroke, upon heart attack or stroke, upon recommendation of and with recommendation of and with supervision of attending physician supervision of attending physician,to a lifetime maximum of $1,500 to a lifetime maximum of $1,500
Chiropractic Care 100% after $10 copay per visit 80% after deductible to a calendar to a calendar year maximum year maximum of 20 visits per of 20 visits per person person
Diagnostic Laboratory 100% 80% after deductible and X-Ray
Durable Medical Equipment 80% after deductible. (requires physician letter Payments will not exceed the actual purchase price of medical necessity)
Emergency Room 80% after deductible.50% after deductible for non-life-threatening care
Hearing Aids Up to $1,500 per hearing aid to a maximum of $3,000 once every five-year period. Covered through selected providers only. Call the FundOffice for a listing and to set up an appointment.
Home Health Care See page 37 for specific See page 37 for specific (requires physician letter information information of medical necessity)
Hospice Care/Extended Not covered Care Facility
Hospital Physician Expenses 80% after deductible
Hospital Room and Board 80% after deductible
Infertility Treatment Not covered
The following schedule shows the percentage of charges that the Fund pays under the Retiree Planwhether medical services are obtained in the PPO Network or Out-of-Area. Note: Charges forbenefits provided by PPO network providers are based on a negotiated contract. Charges for benefitsprovided by out-of-area providers are based on reasonable and customary rates described on page27. You are responsible for any provider charges in excess of the reasonable and customary rates.

79
Plan Pays Out-of-Area
PPO Network Benefits
Mental Health Treatment 80% after deductible to a maximum of 15 days per calendar year (Inpatient) per person
Mental Health Treatment 100% after $10 copay to a calendar 50% after deductible to a calendar (Outpatient) year maximum of 25 visits per person year maximum of 25 visits per person
Occupational Therapy 100% after $10 copay up to a 100% up to a combined lifetime (requires physician letter combined lifetime maximum of maximum of $30,000 for physical,of medical necessity) $30,000 for physical, speech and speech and occupational therapy
occupational therapy
Office Visits (Illness) 100% after $10 copay 80% after deductible
Organ Transplants $250,000 per transplant maximum $250,000 per transplant maximumHospital: 80% after deductible Hospital: 70% after deductible Surgeon’s fee: 100% of PPO fee Surgeon’s fee: 70% of R&C schedule otherwise subject to charges after deductible R&C charges Anesthesia: 70% of chargesAnesthesia: 100% of PPO fee after deductibleschedule
Physical Exams Covered for Members and spouses only(includes all lab, x-ray Paid at 100% to a calendar year maximum of $100and immunizations)
Physical Therapy 100% after $10 copay up to 80% after deductible up to (requires physician letter combined lifetime maximum of combined lifetime maximum of of medical necessity) $30,000 for physical, speech and $30,000 for physical, speech and
occupational therapy occupational therapy
Podiatrist Services 100% after $10 copay up to a 80% after deductible up to a calendar year maximum of $500 calendar year maximum of $500 per person per person
Prescription Drugs $20 copay for generics, $40 for Brand Preferred and $60 for Brand (Mail Order, 90-day supply) Non-Preferred. Calendar year maximum of $15,000 per person
Prescription Drugs $10 copay for generics, $20 for Brand Preferred and $30 for Brand (Retail, 34-day supply) Non-Preferred. Calendar year maximum of $15,000 per person
Speech Therapy 80% after deductible up to a 80% after deductible up to a(requires physician letter combined lifetime maximum of combined lifetime maximum of of medical necessity) $30,000 for physical, speech and $30,000 for physical, speech and
occupational therapy occupational therapy
Substance Abuse 80% after deductible to a 80% after deductible to a Treatment (Inpatient) maximum of 15 days per person maximum of 15 days per person
per calendar year per calendar year
Substance Abuse 100% after $10 copay to a 80% after deductible to a Treatment (Outpatient) maximum of $500 per person maximum of $500 per person
per calendar year. per calendar year. Maximum of two lifetime Maximum of two lifetimeoccurrences per person occurrences per person
Surgeon’s Expenses 100% of PPO fee schedule 80% of R&C charges after deductible otherwise subject to R&C charges
Temporomandibular Not covered Joint Disorders (TMJ)
SCHEDULE OF BENEFITS FOR THE RETIREE PLAN CONTINUED
80 GLOSSARY OF TERMS
This section defines some of the terms used in this document. Please take the time to read these termscarefully. They will help you to better understand your benefits. Also, in order for benefits to be payable,the expenses must meet the requirements of these terms.
Ambulatory Surgical Facility means an establishmentlicensed as such by the state with an organized med-ical staff of physicians with permanent facilities thatare equipped and operated primarily for the purposeof performing surgical procedures and continuousphysician services and registered professional nursingservices whenever a patient is in the facility.
Coinsurance – Once you satisfy the calendar yeardeductible, depending on the type of service youreceive, the Fund may pay a portion of the benefit.The remainder is your share, or coinsurance amount.Refer to the Schedule of Benefits, beginning on page71, for specific coinsurance information.
Copayment – A copayment is a fixed dollar amountthat you pay for certain services that are coveredunder the Plan. For example, doctor’s office visits inthe PPO network for Plan I require a $10 copayment.
Covered Medical Expenses means expenses formedical (including prescription drug, vision, hearingand mental health/substance abuse) and/or dentalservices or supplies, but only to the extent that:
• they are Medically Necessary, as defined in thisDefinitions chapter of the document; and
• the charges for them are the negotiated fees for in-network services or the Reasonable and CustomaryCharges for out-of-network services; and
• coverage for the services or supplies is notexcluded, as provided in the General ExclusionsSection; and
• the charges do not exceed the calendar yearmaximum, lifetime maximum or the Plan’sindividual lifetime maximum benefit.
Custodial Services means any services that are notintended primarily to treat a specific injury or sickness(including mental illness, alcohol or drug abuse).Custodial Services include, but are not limited to:
• Services related to watching or protecting a person;
• Services related to performing or assisting aperson in performing any activities of daily living,such as walking, grooming, bathing, dressing,getting in or out of bed, toileting, eating,preparing foods or taking medications that can beself-administered; and
• Services not required to be performed by trainedor skilled medical or paramedical personnel.
Deductible – The deductible is the amount you(and/or your family) must pay in medical expensesbefore the Fund will begin to pay benefits. Theamount of your calendar year deductible depends onthe Plan of Benefits you’re covered under.
Eligible Dependent – The term “dependent” means (1)your lawful spouse; (2) your unmarried children(including a legally adopted child) who are under 19years of age; (3) your unmarried children who are 19through 23 years of age and who are enrolled as full-time students in an accredited school, college oruniversity, not employed on a full-time basis anddependent upon you for financial support.
IMPORTANT: You are required to furnish thefollowing documentation for dependent coverage ifyou have not already done so:
1. Marriage certificate;
2. Birth certificate document showing both parents’names, court document or written statement onletterhead from appropriate governmental agencyshowing legal guardianship and date of birth ofeach child;
3. Divorce decree if applicable;
4. Proof of a dependent child’s attendance at anaccredited school or college as a full-time studentupon attainment of age 19 must be submitted tothe Fund Office twice each year as directed by theFund Office on an original form which containsthe accredited institution’s seal.

The term “child” also includes a stepchild or fosterchild provided the child depends upon you forsupport and maintenance and has been reported tothe Fund Office. See page 8 for details.
If an unmarried dependent child is incapable of self-sustaining employment because of physical handicapor mental retardation and he is dependent upon youfor support and maintenance, his coverage will becontinued provided his incapability commenced priorto attaining age 19 or age 24 if a full-time student.You must submit proof of your dependent child’sincapability to the Fund Office on the later of 31 daysafter the date he attains 19 years of age or age 24 if afull-time student or 31 days after you are notified ofhis eligibility. Contact the Fund Office for anapplication.
Proof of the continued existence of such incapabilityshall be furnished to the Fund Office from time totime at its request.
Emergency Treatment means treatment for an injuryor sudden serious illness that poses an urgent orpressing need and is treated within hours of thecommencement of the illness or injury.
Experimental Treatment/Procedure means a treatmentor procedure performed to demonstrate a knowntruth, examine the validity of a hypothesis, todetermine the efficacy of something previouslyuntried or which has not been proven.
Extended Care Facility means an institution or adistinct part of an institution which
• is operated pursuant to law and is primarilyengaged in providing, for compensation from itspatients, skilled nursing care for patients whorequire medical care because of injury or sickness;
• provides 24-hour-a-day nursing service under thesupervision of a full-time employee who is eithera doctor or a registered nurse;
• maintains clinical records on all patients;
• provides for having a doctor available to furnishnecessary medical care in case of emergency; and
• provides appropriate methods and procedures forthe dispensing and administering of drugs andbiologicals.
In no event shall “Extended Care Facility” includeany institution or part of an institution which is ahospital or which is primarily for the care of mentalillness, drug addiction, alcoholism or tuberculosis orwhich is primarily engaged in providing domiciliary,custodial or educational care or care for the aged.
Home Health Aide means a person who provides careof a medical or therapeutic nature and reports to andis under the direct supervision of a Home Health CareAgency.
Home Health Care Agency means an agency ororganization (or a distinct part of) which:
• is primarily engaged in providing skilled nursingand other therapeutic services for and in theprivate residence of participants recovering froman injury or sickness;
• is properly licensed or approved according to anyapplicable state or local standards and is federallycertified as a Home Health Care Agency;
• is operated according to policies established by aprofessional staff including at least one physicianand at least one registered nurse;
• provides for supervision of its services by aphysician or a registered nurse;
• maintains medical records for all patients.
Hospital – The term “hospital” means an institutionoperated pursuant to law which is primarily engagedin providing for compensation from its patientsmedical, surgical and diagnostic facilities for the careand treatment of sick and injured persons on an in-patient basis and which provides such facilities underthe supervision of a staff of physicians and with 24-hour-a-day nursing services by registered graduatenurses. Unless it meets this definition, the term“hospital” shall not include any institution or partthereof which is used principally as a rest facility,nursing facility, convalescent facility or facility for theaged. A licensed institution used principally for thecare and treatment of alcoholics will be includedunder the definition of “hospital” with the applicablecoverage in accordance with the schedule of benefitsfor which you or a family member are eligible forconfinement in such institution. A licensedinstitution used principally for the care and treatmentof mental illness will be included under the definitionof “hospital” with the applicable coverage for
81

confinement in such institution in accordance withthe schedule of benefits for which you or a familymember are eligible.
Hospital Charges, Surgical Charges and Medical
Charges – The term “hospital charges” means thecharges for covered medical expenses, which are:
• made by a legally constituted hospital for boardand room and for other hospital services andsupplies (but not including charges for specialnursing services or for services for physicians orsurgeons) furnished by the hospital duringconfinement;
• The term “surgical charges” means the charges forcovered medical expenses for surgery and fornecessary post-operative treatment in connectionwith the surgery.
• The term “medical charges” means those chargesfor covered medical expenses that are other thanhospital charges or surgical charges as definedabove.
Hospital Confinement – The term “period of hospitalconfinement” includes successive periods of hospitalconfinement for the same or a related disease orbodily injury unless separated by complete recoveryfrom the disease or bodily injury which caused theprevious period of hospital confinement or, in thecase of the Member, a return to active work for atleast one day.
Hospice Care Facility means an institution thatprovides care and service for terminally ill personsand which:
a. provides 24-hour-a-day nursing care for theterminally ill person with the necessary physical,psychological and spiritual needs, with acuteinpatient and outpatient care, home care,bereavement counseling directly or indirectly;
b. has a medical director who is a physician;
c. has an interdisciplinary team that coordinates thecare and services it provides and which includesat least one physician, one registered professionalnurse and one social worker;
d. maintains central clinical records on all patients; and
e. is licensed or accredited as a Hospice if required.
Medically Necessary means any service, supply,treatment or hospital confinement (or part of ahospital confinement) which is essential to thetreatment of the injury or illness for which it isprescribed or performed, meets generally acceptedstandards of medical practice and is ordered by aphysician. The fact that a Physician or otherprovider may prescribe, order, recommend, orapprove a service or supply does not, of itself, makeit Medically Necessary or make the expense aCovered Charge.
Physician means a licensed medical practitioner whois practicing within the scope of his license and whois licensed to diagnose, prescribe and administerdrugs or to perform surgery. It will also include anyother licensed medical practitioner whose services arerequired to be covered by law in the locality wherethe policy is issued if he is:
• operating within the scope of his license, and
• performing a service for which benefits areprovided under this plan when performed by a physician.
Reasonable and Customary Charges – The term“reasonable and customary” means the amountnormally charged for similar services and supplieswhich does not exceed the amount ordinarily chargedfor comparable services and supplies in the localitywhere the services or supplies are received.
82
S E C T I O N 1 : P U R P O S E O F T H I S N O T I C E A N DE F F E C T I V E DAT E
THIS NOTICE DESCRIBES HOW MEDICALINFORMATION ABOUT YOU MAY BE USED ANDDISCLOSED AND HOW YOU CAN GET ACCESSTO THIS INFORMATION. PLEASE REVIEW ITCAREFULLY.
This Privacy Notice applies to the Fund Office of theNew England Carpenters Health Benefits Fund (“theFund”) and the services that the Fund provides throughHines & Associates, CCN, Delta Dental, UllicareRx/Medco., Davis Vision and other business associates ofthe Fund. The Fund’s insurers will send you a notice oftheir privacy practices separately.
Effective date.
The effective date of this Notice is April 14, 2003.
This Notice is required by law.
The Fund is required by law to take reasonable stepsto ensure the privacy of your personally identifiablehealth information and to inform you about:
1. The Fund’s uses and disclosures of ProtectedHealth Information (PHI),
2. Your rights to privacy with respect to your PHI,
3. The Fund’s duties with respect to your PHI,
4. Your right to file a complaint with the Fund andwith the Secretary of the United StatesDepartment of Health and Human Services(HHS), and
5. The person or office you should contact forfurther information about the Fund’s privacypractices.
S E C T I O N 2 : YO U R P R O T E C T E D H E A LT HI N F O R M AT I O N
Protected Health Information (PHI) Defined
The term “Protected Health Information” (PHI)includes all individually identifiable healthinformation related to your past, present or futurephysical or mental health condition or to payment forhealth care. PHI includes information maintained bythe Fund in oral, written, or electronic form.
When the Fund May Disclose Your PHI
Under the law, the Fund may disclose your PHIwithout your consent or authorization, or theopportunity to agree or object, in the following cases:
• For treatment, payment or health careoperations. The Fund and its business associateswill use PHI in order to carry out:1. Treatment,2. Payment, or 3. Health care operations.
Treatment is the provision, coordination ormanagement of health care and related services. Italso includes but is not limited to consultationsand referrals between one or more of yourproviders.
For example, the Fund may disclose to a treatingorthodontist the name of your treating dentist sothat the orthodontist may ask for your dental x-rays from the treating dentist.
Payment includes but is not limited to actions tomake coverage determinations and payment(including billing, claims management,subrogation, Fund reimbursement, reviews formedical necessity and appropriateness of care andutilization review and preauthorizations).
For example, the Fund may tell a doctor whetheryou are eligible for coverage or what percentageof the bill will be paid by the Fund. If we contractwith third parties to help us with paymentoperations, such as a physician that reviewsmedical claims, we will also disclose information
83NEW ENGLAND CARPENTERS HEALTH BENEFITS FUND PRIVACY NOTICE

to them. These third parties are known as“business associates.”
Health care operations includes but is not limitedto quality assessment and improvement,reviewing competence or qualifications of healthcare professionals, underwriting, premium ratingand other insurance activities relating to creatingor renewing insurance contracts. It also includesdisease management, case management,conducting or arranging for medical review, legalservices, and auditing functions including fraudand abuse compliance programs, businessplanning and development, business managementand general administrative activities.
For example, the Fund may use informationabout your claims to refer into a diseasemanagement program, a well-pregnancy program,project future benefit costs or audit the accuracyof its claims processing functions.
• Disclosure to the Fund’s Trustees The Fund will also disclose PHI to the FundSponsor, which is the Board of Trustees of theNew England Carpenters Health Benefits Fund,for purposes related to treatment, payment, andhealth care operations, and has amended the PlanDocument to permit this use and disclosure asrequired by federal law. For example, we maydisclose information to the Board of Trustees toallow them to decide an appeal or review asubrogation claim.
• In addition, the Fund may disclose “summaryhealth information” to the Board of Trustees forobtaining premium bids or modifying, amendingor terminating the Fund’s group health plan.Summary information summarizes the claimshistory, claims expenses or type of claimsexperience by individuals for whom a PlanSponsor such as the Board of Trustees hasprovided health benefits under a group healthplan. Identifying information will be deletedfrom summary health information, in accordancewith federal privacy rules.
• At your request. If you request it, the Fund isrequired to give you access to certain PHI in orderto allow you to inspect and/or copy it.
• When required by applicable law.
• As required by HHS. The Secretary of the UnitedStates Department of Health and Human Servicesmay require the disclosure of your PHI toinvestigate or determine the Fund’s compliancewith the privacy regulations.
• Public health purposes. To an authorized publichealth authority if required by law or for publichealth and safety purposes. PHI may also be usedor disclosed if you have been exposed to acommunicable disease or are at risk of spreading adisease or condition, if authorized by law.
• Domestic violence or abuse situations. Whenauthorized by law to report information aboutabuse, neglect or domestic violence to publicauthorities if a reasonable belief exists that youmay be a victim of abuse, neglect or domesticviolence. In such case, the Fund will promptlyinform you that such a disclosure has been or willbe made unless that notice would cause a risk ofserious harm.
• Health oversight activities. To a health oversightagency for oversight activities authorized by law.These activities include civil, administrative orcriminal investigations, inspections, licensure ordisciplinary actions (for example, to investigatecomplaints against health care providers) andother activities necessary for appropriate oversightof government benefit programs (for example, tothe Department of Labor).
• Legal proceedings. When required for judicial oradministrative proceedings. For example, yourPHI may be disclosed in response to a subpoenaor discovery request that is accompanied by acourt order.
• Law enforcement health purposes. Whenrequired for law enforcement purposes (forexample, to report certain types of wounds).
84

• Law enforcement emergency purposes. Forcertain law enforcement purposes, including:1. identifying or locating a suspect, fugitive,
material witness or missing person, and2. disclosing information about an individual
who is or is suspected to be a victim of acrime.
• Determining cause of death and organ donation.When required to be given to a coroner ormedical examiner to identify a deceased person,determine a cause of death or other authorizedduties. We may also disclose PHI for cadavericorgan, eye or tissue donation purposes.
• Funeral purposes. When required to be given tofuneral directors to carry out their duties withrespect to the decedent.
• Research. For research, subject to certainconditions.
• Health or safety threats. When, consistent withapplicable law and standards of ethical conduct,the Fund in good faith believes the use ordisclosure is necessary to prevent or lessen aserious and imminent threat to the health orsafety of a person or the public and the disclosureis to a person reasonably able to prevent or lessenthe threat, including the target of the threat.
• Workers’ compensation programs. Whenauthorized by and to the extent necessary tocomply with workers’ compensation or othersimilar programs established by law.
• Specialized Government Functions. Whenrequired, to military authorities under certaincircumstances, or to authorized federal officialsfor lawful intelligence, counter intelligence andother national security activities.
Except as otherwise indicated in this notice, uses anddisclosures will be made only with your writtenauthorization subject to your right to revoke yourauthorization.
When the Disclosure of Your PHI Requires Your
Written Authorization
Although the Fund does not routinely obtainpsychotherapy notes, it must generally obtain yourwritten authorization before the Fund will use ordisclose psychotherapy notes about you. However,the Fund may use and disclose such notes whenneeded by the Fund to defend itself against litigationfiled by you.
Psychotherapy notes are separately filed notes aboutyour conversations with your mental healthprofessional during a counseling session. They do notinclude summary information about your mentalhealth treatment.
The Fund may provide health information for thepurpose of evaluating and processing a claim fordisability benefits or to process a hardship loan fromthe Annuity Fund; however, the Fund will obtainyour written authorization before it will use ordisclose any health information for this purpose.
When You Can Object and Prevent the Fund from
Using or Disclosing PHI
Disclosure of your PHI to family members, otherrelatives, your close personal friends and any otherperson you choose is allowed under federal law if:
• The information is directly relevant to the familyor friend’s involvement with your care or paymentfor that care, and
• You have either agreed to the disclosure or havebeen given an opportunity to object and have notobjected.
Other Uses or Disclosures
The Fund may contact you to provide you withinformation about treatment alternatives or otherhealth-related benefits and services that may be ofinterest to you.
85

S E C T I O N 3 : YO U R I N D I V I D U A L P R I VACY R I G H TS
You May Request Restrictions on PHI Uses and
Disclosures
You may request the Fund to:
1. Restrict the uses and disclosures of your PHI tocarry out treatment, payment or health careoperations, or
2. Restrict uses and disclosures to family members,relatives, friends or other persons identified byyou who are involved in your care.
The Fund, however, is not required to agree to yourrequest.
You or your personal representative will be requiredto complete a form to request restrictions on uses anddisclosures of your PHI. Make such requests to thePrivacy Official at:
The New England Carpenters Health BenefitsFund350 Fordham RoadWilmington, MA 01887Phone: (800) 344-1515
You May Request Confidential Communications
The Fund will accommodate an individual’sreasonable request to receive communications of PHIby alternative means or at alternative locationswhere the request includes a statement thatdisclosure could endanger the individual.
You or your personal representative will be requiredto complete a form to request restrictions on uses anddisclosures of your PHI. Make such requests to thePrivacy Official (at the address listed above).
You May Inspect and Copy PHI
You have a right to inspect and obtain a copy of yourPHI contained in a “designated record set,” for aslong as the Fund maintains the PHI.
The Fund must provide the requested informationwithin 30 days if the information is maintained onsite or within 60 days if the information ismaintained offsite. A single 30-day extension is
allowed if the Fund is unable to comply with thedeadline.
You or your personal representative will be requiredto complete a form to request access to the PHI. Areasonable fee may be charged. Requests for access toPHI should be made to the Privacy Official (at theaddress listed at left).
If access is denied, you or your personalrepresentative will be provided with a written denialsetting forth the basis for the denial, a description ofhow you may exercise your review rights and adescription of how you may complain to the Fundand HHS.
Designated Record Set: includes your medicalrecords and billing records that are maintained by orfor a covered health care provider. Records includeenrollment, payment, billing, claims adjudication andcase or medical management record systemsmaintained by or for a health plan or otherinformation used in whole or in part by or for thecovered entity to make decisions about you.Information used for quality control or peer reviewanalyses and not used to make decisions about you isnot included.
You Have the Right to Amend Your PHI
You have the right to request that the Fund amendyour PHI or a record about you in a designatedrecord set for as long as the PHI is maintained in thedesignated record set subject to certain expectations.See the Fund’s Right to Amend Policy (available onrequest from the Fund’s Privacy Official) for a list ofexceptions.
The Fund has 60 days after receiving your request toact on it. The Fund is allowed a single 30-dayextension if the Fund is unable to comply with the60-day deadline. If the Fund denied your request inwhole or part, the Fund must provide you with awritten denial that explains the basis for the decision.You or your personal representative may then submita written statement disagreeing with the denial andhave that statement included with any futuredisclosures of that PHI.
86

You should make your request to amend PHI to thePrivacy Official (at the address listed above). You oryour personal representative will be required tocomplete a form to request amendment of the PHI.
You Have the Right to Receive an Accounting of the
Fund’s PHI Disclosures
At your request, the Fund will also provide you withan accounting of certain disclosures by the Fund ofyour PHI. We do not have to provide you with anaccounting of disclosures related to treatment,payment, or health care operations, or disclosuresmade to you or authorized by you in writing. See theFund’s Accounting for Disclosure Policy (available onrequest from the Fund’s Privacy Official) for thecomplete list of disclosures for which an accountingis not required.
The Fund has 60 days to provide the accounting. TheFund is allowed an additional 30 days if the Fundgives you a written statement of the reasons for thedelay and the date by which the accounting will beprovided.
If you request more than one accounting within a 12-month period, the Fund may charge a reasonable,cost-based fee for each subsequent accounting.
You Have the Right to Receive a Paper Copy of This
Notice Upon Request
To obtain a paper copy of this Notice, contact thePrivacy Official (at the address listed above).
Your Personal Representative
You may exercise your rights through a personalrepresentative who will be required to produceevidence of authority to act on your behalf before thepersonal representative will be given access to yourPHI or be allowed to take any action for you. Proof ofsuch authority will be a completed, signed andapproved Appointment of Personal Representativeform. You may obtain this form by calling the FundOffice.
The Fund retains discretion to deny access to yourPHI to a personal representative to provide protectionto those vulnerable people who depend on others to
exercise their rights under these rules and who maybe subject to abuse or neglect.
The Fund will recognize certain individuals aspersonal representatives without you having tocomplete an Appointment of Personal Representativeform. For example, the Fund will automaticallyconsider a spouse, parent of a Member, or an adultchild (age 18 or over) of a Member to be the personalrepresentative of an individual covered by the Fund.In addition, the Fund will consider a parent orguardian as the personal representative of anunemancipated minor except in a few types ofsituations. A spouse, a parent, or child may act on anindividual’s behalf, including requesting access totheir PHI. Spouses and unemancipated minors may,however, request that the Fund restrict informationthat goes to family members as described above at thebeginning of Section 3 of this Notice.
You should also review the Fund’s Policy andProcedure for the Recognition of PersonalRepresentatives (available upon request from theFund’s Privacy Official) for a more completedescription of the circumstances where the Fund willautomatically consider an individual to be a personalrepresentative for purposes of exercising your rightsunder this Privacy Notice.
87

S E C T I O N 4 : T H E F U N D ’ S D U T I E S
Maintaining Your Privacy
The Fund is required by law to maintain the privacyof your PHI and to provide you with notice of itslegal duties and privacy practices.
This notice is effective beginning on April 14, 2003and the Fund is required to comply with the terms ofthis notice. However, the Fund reserves the right tochange its privacy practices and to apply the changesto any PHI received or maintained by the Fund priorto that date. If a privacy practice is changed, a revisedversion of this notice will be provided to you and toall past and present participants and beneficiaries forwhom the Fund still maintains PHI.
The Privacy Notice will be provided by first class mailto all named participants. Any other person,including dependents of named participants, mayreceive a copy upon request.
Any revised version of this notice will be distributedwithin 60 days of the effective date of any materialchange to:
1. The uses or disclosures of PHI,
2. Your individual rights,
3. The duties of the Fund, or
4. Other privacy practices stated in this notice.
Disclosing Only the Minimum Necessary Protected
Health Information
When using or disclosing PHI or when requestingPHI from another covered entity, the Fund will makereasonable efforts not to use, disclose or request morethan the minimum amount of PHI necessary toaccomplish the intended purpose of the use,disclosure or request, taking into considerationpractical and technological limitations.
However, the minimum necessary standard will notapply in the following situations:
1. Disclosures to or requests made by a health careprovider for treatment,
2. Uses or disclosures made to you,
3. Uses or disclosures made pursuant to yourwritten authorization,
4. Disclosures made to the Secretary of the UnitedStates Department of Health and Human Servicespursuant to its enforcement activities underHIPAA,
5. Uses or disclosures required by law, and
6. Uses or disclosures required for the Fund’scompliance with the HIPAA privacy regulations.
This notice does not apply to information that hasbeen de-identified. De-identified information isinformation that:
1. Does not identify you, and
2. With respect to which there is not reasonablebasis to believe that the information can be usedto identify you.
S E C T I O N 5 : YO U R R I G H T TO F I L E A C O M P L A I N TW I T H T H E F U N D O R T H E H H S S E C R E TA R Y
If you believe that your privacy rights have beenviolated, you may file a complaint with the Fund incare of the Privacy Official (at the address listedabove).
You may also file a complaint with the Secretary ofthe U.S. Department of Health and Human Services(“HHS”). Please contact the nearest office of theDepartment of Health and Human Services, listed inyour telephone directory, visit the HHS website atwww.hhs.gov, or call the Privacy Official for moreinformation about how to file a complaint.
The Fund will not retaliate against you for filing acomplaint.
S E C T I O N 6 : I F YO U N E E D M O R E I N F O R M AT I O N
If you have any questions regarding this notice or thesubjects addressed in it, you may contact the PrivacyOfficial at the Fund Office.
88

S E C T I O N 7 : C O N C LU S I O N
PHI use and disclosure by the Fund is regulated bythe federal Health Insurance Portability andAccountability Act, known as HIPAA. You may findthese rules at 45 Code of Federal Regulations Parts160 and 164. This notice attempts to summarize theregulations. The regulations will supersede this noticeif there is any discrepancy between the information inthis notice and the regulations.
89
Employer Trustees
William J. Sullivan, Secretary/TreasurerDaniel O’Connell’s Sons, Inc.480 Hampden StreetP.O. Box 267Holyoke, MA 01041
Stephan A. AdamicCo-Secretary/Treasurer P.O. Box 302Grantham, NH 03753
George M. BidgoodBidgood Associates, Inc.99 Essex StreetMelrose, MA 02176
Theodore H. BrodieA.F. Underhill, Inc.P.O. Box 376Canton, MA 02021-0376
Donald L. Colavecchio105 Reflection DriveSandwich, MA 02563
Thomas J. GunningThe Building Trades Employers Assoc.1400 Hancock Street, 7th FloorQuincy, MA 02169
Michael ShaughnessyShaughnessy Crane Service, Inc.P.O. Box 366South Boston, MA 02127-0992
William SheaJ.F. White Contracting Company10 Burr StreetFramingham, MA 017001-4617
Thomas SteevesT.J. McCartney, Inc.3 Capitol Street, Suite 1Nashua, NH 03063
Union Trustees
Thomas J. Harrington, ChairmanNew England Regional Council ofCarpenters803 Summer Street, 4th FloorSouth Boston, MA 02127
Mark L. ErlichCarpenters Local Union 4010 Holworthy StreetCambridge, MA 02138
Thomas J. FlynnCarpenters Local Union 67760 Adams Street, 2nd FloorDorchester, MA 02122
Simon R. JamesLocal Union No. 10829 Oakland StreetSpringfield, MA 01108
Bruce KingLocal Union 199660 Industrial DriveAugust, ME 04330-9302
John MurphyNew England Regional Council of Carpenters803 Summer StreetBoston, MA 02127
Michael NelsonLocal Union 42421 Mazzeo Drive, Suite 201Randolph, MA 02368
David R. WallaceCLMP803 Summer StreetBoston, MA 02127
Jack WinfieldLocal Union 112190 Braintree StreetAllston, MA 02134
David A. WoodmanLocal Union 56Marine Industrial Park/EDIC22 Drydock Avenue, 3rd FloorBoston, MA 02210-2386
90 BOARD OF TRUSTEES
NOTES 91
92 NOTES


















