1 Current Issues in Otolaryngology Steven D. Pletcher MD Assistant Professor Department of Otolaryngology – Head and Neck Surgery University of California, San Francisco Otorhinolaryngology – Head and Neck Surgery Formerly known as ENT Early Nights and Tennis Easy, Not Tough Ear, Nose, and Throat Ear Hearing Loss Case #1 72 y/o woman with hearing loss and tinnitus Otologic History No vertigo, otalgia, or otorrhea No history of prior surgery or frequent infections + history of hearing loss in family (father and grandfather) Went to “Rock concerts” in the sixties
Transcript
1
Current Issues in Otolaryngology
Steven D. Pletcher MDAssistant Professor
Department of Otolaryngology –Head and Neck Surgery
University of California, San Francisco
Otorhinolaryngology – Head and Neck Surgery
Formerly known as ENTEarly Nights and TennisEasy, Not Tough
Ear, Nose, and Throat
Ear
Hearing Loss
Case #172 y/o woman with hearing loss and tinnitusOtologic History
No vertigo, otalgia, or otorrheaNo history of prior surgery or frequent infections
+ history of hearing loss in family (father and grandfather)Went to “Rock concerts” in the sixties
2
Case #1
PMH: noneMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane
Case #1
Tuning fork tests (512 Hz)Weber: MidlineRinne: Air conduction > Bone Conduction Bilaterally
Weber & Rinne Tests Audiogram
3
Diagnosis
PresbycusisTreatment
Consideration of Hearing AidsListening strategies and assistive devicesAvoidance of noise exposure
New Frontiers?Implantable hearing aidsCochlear Implants “partial insertion”
Case #2
Hearing Loss
Case #236 y/o woman with hearing loss and tinnitus
Symptoms worse on right sideOtologic History
No vertigo, otalgia, or otorrheaNo prior ear surgery No history of ear infections+ family history of hearing loss (mother in late 20’s)No history of noise exposure
Case #2
PMH: recently delivered first childMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane
4
Case #2Tuning fork tests (512 Hz)
Weber: To the RightRinne
Bone conduction > Air conduction bilaterally
Audiogram
Most Likely Diagnosis?
Meniere’s diseaseOtosclerosisOtitis Media with EffusionCholesteatomaAcoustic Neuroma
DiagnosisOtosclerosis
Disease of abnormal bone remodeling within the middle/inner earMost patients present with unilateral conductive hearing loss and normal TM examination
More severe cases may be bilateral with associated sensorineural hearing loss
Conductive loss due to fixation of the Stapes footplate within the Oval Window
5
Ear Picture Otosclerosis
Patients often have a family history of hearing lossIn women, symptoms may worsen during pregnancy
Popularized by Dr. John Shea in the 1956Revolutionized treatment of otosclerosis
Stapes bone partially removedProsthesis inserted and linked to incus
6
Stapes Surgery
Results90% with complete or near complete correction of conductive component of hearing loss9% with no change in hearing1% with complete sensorineural loss
Post-op Audiogram
7
Post-op Audiogram
Case #3
Hearing Loss
Case #360 y/o woman with right-sided hearing loss and tinnitusOtologic History
No vertigo, otalgia, or otorrheaNo history of prior surgery or frequent infectionsNo history of hearing loss in family Went to “Rock concerts” in the sixties
Case #3
PMH: noneMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane
8
Case #3
Tuning fork tests (512 Hz)Weber MidlineRinne Air conduction > Bone Conduction Bilaterally
Audiogram
Next Step In Evaluation/Treatment?
Hearing Aid evaluation/referralCT scan of the brain/temporal boneCochlear implantationMRI of the brain/temporal bone
Diagnosis
Assymetric Sensorineural Hearing LossPlan: MRI
9
MRI Acoustic Neuroma
Vestibular SchwannomaBenign nerve sheath tumor from the vestibular component of the VIIIth nerve
Most commonly presents as assymetricsensorineural hearing lossMay have associated imbalance and Vthnerve palsy
TreatmentAntibiotics & Steroids (Oral vs. Topical)Surgery for patients refractory to medical management
Debridement Video
Case #6
Nasal Drainage
15
Case #644y/o woman with clear nasal drainage for 6 monthsHPI
Always right-sided“Gush of water” when I get up in the morningProfessional “9-ball” player, drips on pool table when she leans over to shootNo nasal congestion or facial pain/pressureRare headache
Case #6
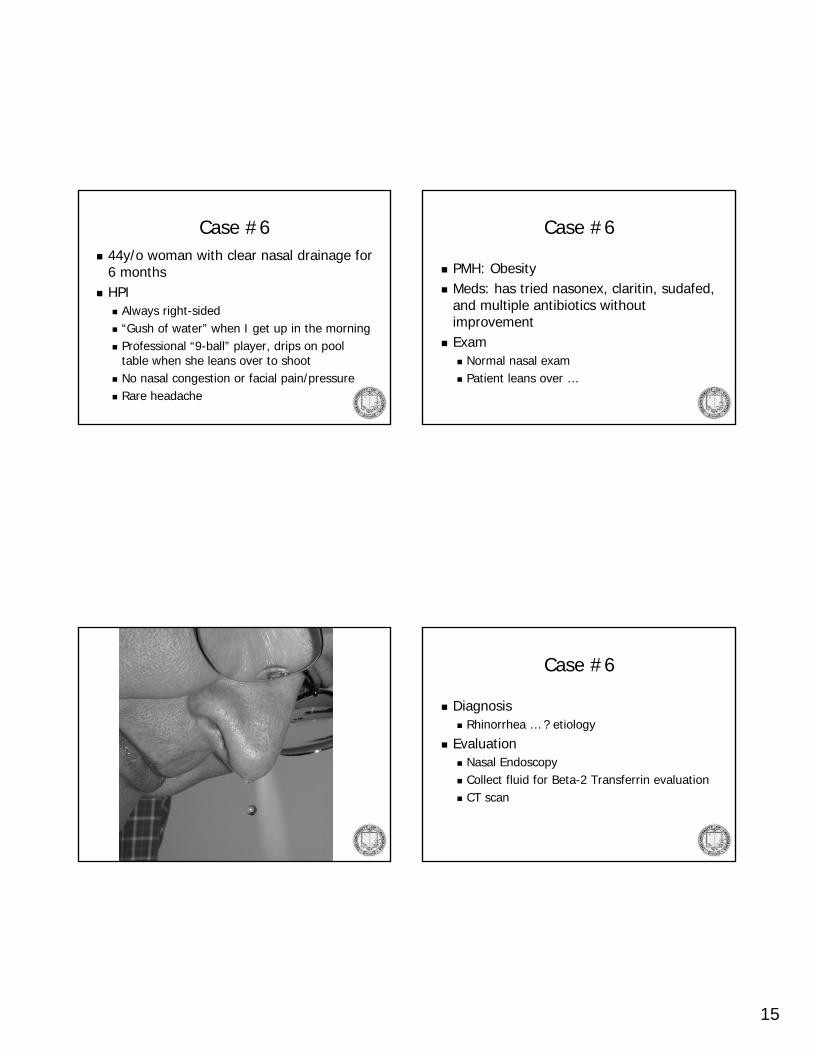
PMH: ObesityMeds: has tried nasonex, claritin, sudafed, and multiple antibiotics without improvementExam
Normal nasal examPatient leans over …
Case #6
DiagnosisRhinorrhea … ? etiology
EvaluationNasal EndoscopyCollect fluid for Beta-2 Transferrin evaluation CT scan
16
CSF Leak
Post-surgicalEndoscopic Sinus SurgeryNeurosurgery (Pituitary and other skull base tumors)
Post-traumaticSpontaneous
CSF Leak
SpontaneousCommonly in obese, middle aged womenOften delay in diagnosisRisk of meningitis approximately 5%/year
May present with meningitis
Spontaneous CSF Leak
Endoscopic RepairIntrathecal flouresceinSkull base defect identified and cleaned Two-layer repair
17
SKULL BASE
MUCOSAL OVERLAY GRAFT
INTRACRANIALCAVITY
NASAL CAVITY
Two Layer RepairCARTILAGE UNDERLAY GRAFT
18
Throat
Hoarseness
Case #744y/o man with worsening hoarseness over the past 6 monthsHPI
Mild intermittent throat painDescribes voice as “gravely”Symptoms worse in morning and eveningGlobus sensation when swallowing, but no dysphagiaNon-smoker, drinks 2-3 glasses of wine/night
Laryngeal manifestations of GERDMay occur without symptoms of heartburn
Typical presentations include hoarseness, globus sensation, chronic sore throatVariable findings on laryngoscopy
20
Laryngopharyngeal Reflux
Gold-standard for diagnosis is 24 hour double pH probeOften treated empirically with PPIArea of controversy
Case #8
Hoarseness
Case #867y/o man with hoarseness for the past monthHPI
No painIncreased effort of speaking“Breathy” voiceVoice worsens throughout dayOccasional coughing with thin liquidsNon-smoker, drinks 2-3 glasses of wine/week
Tobacco and EtOH are primary risk factors4:1 male to female ratioClinical Presentation often depends on site of origin
Anatomy SlideLaryngeal Cancer
GlottisEarlier presentation (voice change)Decreased risk of cervical metastasis
SupraglottisLater presentationIncreased risk of cervical metastasis
26
Laryngeal Cancer
TreatmentSurgery, Radiation, and Chemotherapy are three treatment modalitiesStage of cancer and local expertise determines treatment approachOverall trend towards increased use of radiation/chemotherapy and “laryngeal conservation” surgery

























![CONTRASTING PURULENT AND NON-PURULENT MIDDLE EAR …€¦ · the presence of middle ear effusion (otorrhea), ear pain (otalgia), and erythema of the TM [15-17]. Most AOM occurs between](https://static.documents.pub/doc/80x56/5f6191e00b408f3a062f96dc/contrasting-purulent-and-non-purulent-middle-ear-the-presence-of-middle-ear-effusion.jpg)















