Case descriptions do not accompany MMPI-2 reports, but are provided here as background information. The following report was generated from Q-global™, Pearson’s web-based scoring and reporting application, using Mr. C.’s responses to the MMPI-2. Additional MMPI-2 sample reports, product offerings, training opportunities, and resources can be found at PearsonClinical.com/mmpi2.
Case Description: Del C. — Personal Injury Neurological Interpretive Report
Del C., a 50-year-old married construction worker, is being evaluated as part of a personal injury lawsuit. Del claims severe head injuries as a result of an automobile accident. Although he was not hospitalized at the time of the accident, he sought medical attention the following week for impaired vision, headaches, and dizziness. He has not returned to his job since the accident and is seeking compensation for his lost ability to function as a result of his reported symptoms, which include visual impairment, ringing in his ears, dizziness, and headaches.
Minnesota Multiphasic Personality Inventory and MMPI are registered trademarks and The Minnesota Report is a trademark of theUniversity of Minnesota. Pearson, the PSI logo, and PsychCorp are trademarks in the U.S. and/or other countries of Pearson Education,Inc., or its affiliate(s).
TRADE SECRET INFORMATIONNot for release under HIPAA or other data disclosure laws that exempt trade secrets from disclosure.
[ 3.9 / 1 / QG ]
SAMPLE
30
40
50
60
70
90
100
110
30
40
50
60
70
80
90
100
110
FBVRIN TRIN F
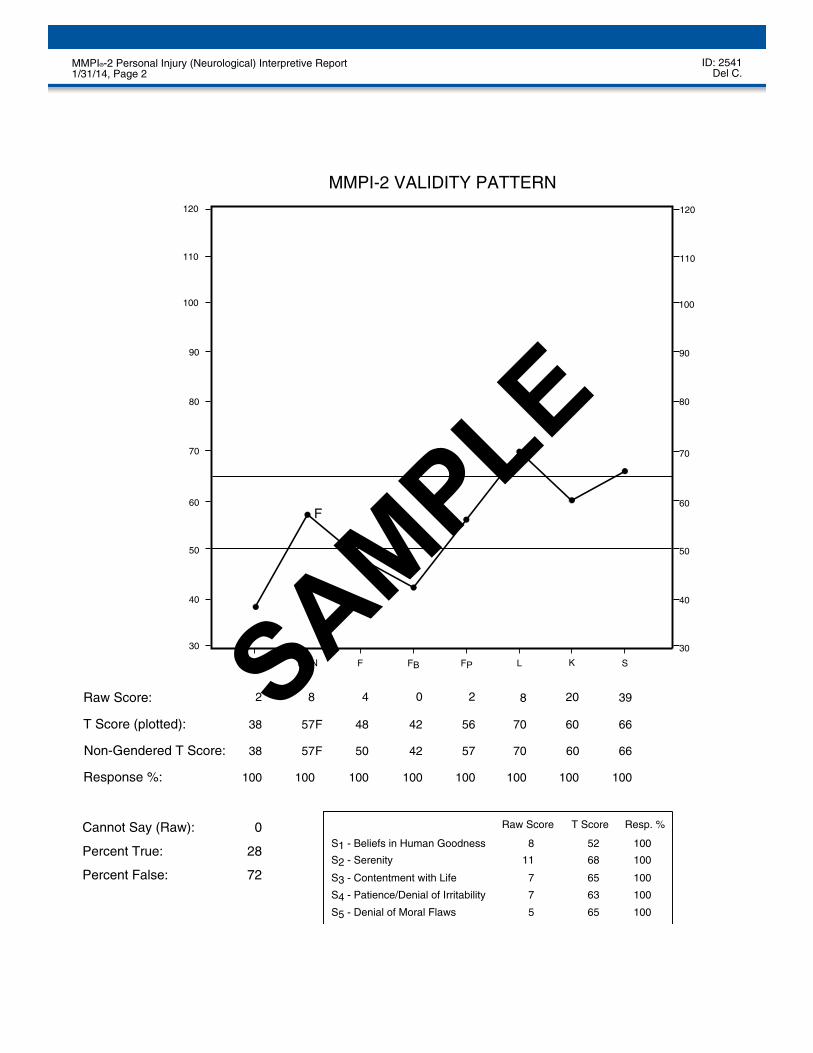
MMPI-2 VALIDITY PATTERN
KL
80
72
28
57 7048 6042 66
100 100 100100 100100 100
38
2 8 4 2080 39
0
120 120
Raw Score:
Cannot Say (Raw):
FP S
56
100
2
S5 - Denial of Moral Flaws
S4 - Patience/Denial of Irritability
S3 - Contentment with Life
S2 - Serenity
S1 - Beliefs in Human Goodness
Raw Score T Score Resp. %
Percent True:
Percent False:
100
100
100
100
11
8 52
10068
5
7
7
65
63
65
FT Score (plotted):
Non-Gendered T Score:
Response %:
6638 57 50 42 57 70 60F
F
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 2 Del C.
SAMPLE
PROFILE VALIDITY
Unrealistic claims of virtue, as shown in this profile, reflect conscious attempts to influence theoutcome of litigation by giving the appearance of having extremely high moral virtue and honesty. Thistest-taking attitude weakens the validity of the test and shows an unwillingness or inability on the part ofthe client to disclose personal information. The resulting MMPI-2 profile is unlikely to provide muchuseful information about the client because he was too guarded to cooperate in the self-appraisal. Manyreasons may be found for this pattern of uncooperativeness: conscious distortion to present himself in afavorable light, lack of psychological sophistication, or rigid neurotic adjustment.
The client's conscious efforts to influence the outcome of the evaluation and to project an overlypositive self-image produced an MMPI-2 profile that substantially underestimates his psychologicalmaladjustment. The test interpretation should proceed with the caution that the clinical picture reflectedin the profile is probably an overly positive one and may not provide sufficient information forevaluation.
Scales Hs and Hy were used as the prototype to develop this report. His MMPI-2 clinical profilepresents a rather mixed pattern of symptoms in which somatic reactivity under stress is a primarydifficulty. The client presents a picture of physical problems and a reduced level of psychologicalfunctioning. He is likely to have a hysteroid adjustment to life and may experience periods ofexacerbated symptom development under stress. Some individuals with this profile develop patterns of"invalidism" in which they become incapacitated and dependent on others. His physical complaints maybe vague, may have appeared suddenly after a period of stress, and may not be traceable to actualorganic changes. He may be manifesting fatigue, vague pain, weakness, or unexplained periods ofdizziness. He may view himself as highly virtuous and he may exhibit a "Pollyannish" attitude towardlife. Such clients may not appear greatly anxious or depressed about their symptoms and may exhibit "labelle indifference." Apparently sociable and rather exhibitionistic, this individual seems to manageconflict by excessive denial and repression.
In addition, the following description is suggested by the content of the client's item responses. He findsit difficult to manage routine affairs, and the items he endorsed suggest a poor memory, concentrationproblems, and an inability to make decisions. He appears to be immobilized and withdrawn and has noenergy for life. He views his physical health as failing and reports numerous somatic concerns. He feelsthat life is no longer worthwhile and that he is losing control of his thought processes. He appears tohave good social skills and reports that he has no problems interacting with other people. He complainsabout feeling quite uncomfortable and in poor health. The symptoms he reports include vague weakness,fatigue, and difficulty concentrating. In addition, he feels that others are unsympathetic toward hisperceived health problems.
SYMPTOMATIC PATTERNS
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 3 Del C.
SAMPLE
PROFILE FREQUENCY
It is usually valuable in MMPI-2 clinical profile interpretation to consider the relative frequency of agiven profile pattern in various settings. The client's MMPI-2 high-point clinical scale score (Hy) isfound in 12.1% of the MMPI-2 normative sample of men. However, only 3.8% of the normative menhave Hy as the peak score at or above a T score of 65, and only 2.3% have well-defined Hy spikes. Hiselevated MMPI-2 two-point profile configuration (1-3/3-1) is rare in samples of normals, occurring in1.8% of the MMPI-2 normative sample of men.
The relative frequency of his profile in various medical settings is informative. In the PearsonAssessments medical sample, this is the most frequent MMPI-2 high-point clinical scale score (Hy),occurring in 20.7% of the men. In addition, 16.3% of the men have the Hy scale spike at or above a Tscore of 65, and 9.3% have a well-defined Hy high point in that range. His elevated MMPI-2 two-pointprofile configuration (1-3/3-1), in this elevation range, is very common in samples of medical patients. Itoccurs in 16.4% of the men in the Pearson Assessments medical sample.
This MMPI-2 profile peak score on the Hy scale occurs with very high frequency among individualsinvolved in personal injury litigation. This is the most frequent profile peak (30.6%). Moreover, 17.2%of the cases have well-defined scores at or above a T score of 65 (Butcher, 1997b). In addition, amonglitigants who produce a somewhat defensive profile, this MMPI-2 profile peak score on the Hy scale isfound with very high frequency (33.3%). Additionally, 22.2% are well-defined with a high-point scoreat or above a T of 65 (Butcher, 1997b).
His MMPI-2 profile peak score on the Hy scale occurs with relatively high frequency in head injurypatients. Putnam et al. (1995) reported this high-point score for 5.8% of individuals with mild headinjury and 5.1% with moderate to severe head injury.
PROFILE STABILITY
The relative elevation of the highest scales in his clinical profile reflects high definition. If he is retestedat a later date, the peak scores are likely to retain their relative salience. His high-point score on Hy islikely to remain stable over time. Short-term test-retest studies have shown a correlation of 0.72 for thishigh-point score. Spiro, Butcher, Levenson, Aldwin, and Bosse (1993) reported a 0.65 stability index fora large study of normals in a five-year test-retest period.
INTERPERSONAL RELATIONS
Individuals with similar profiles tend to be somewhat passive-dependent and demanding ininterpersonal relationships. The client may attempt to control others by complaining of physicalsymptoms. He is likely to have a low sex drive and may have problems in his marriage because of this.He seems to require an excessive amount of emotional support from his spouse. He is likely to use hisphysical complaints to gain attention for his perceived illness.
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 4 Del C.
SAMPLE
He has an average interest in being with others and is not socially isolated or withdrawn. He appears tomeet and talk with other people with relative ease and is not overly anxious at social gatherings.
MENTAL HEALTH CONSIDERATIONS
Individuals with this profile typically exhibit a neurotic pattern of adjustment and would probablyreceive a clinical diagnosis of conversion disorder or somatization disorder. They might also receive anAxis II diagnosis of dependent personality.
The client would probably be resistant to mental health treatment because he has little psychologicalinsight and seeks medical explanations for his disorder. He is probably defensive and reluctant to engagein self-exploration. In addition, he seems to experience little anxiety about his situation and may havelittle motivation to change his behavior. Some individuals with this profile respond to placebos or mildsuggestion or to stress inoculation training if it is not too threatening. They will probably requirelong-term commitment to therapy before their personality will change substantially. However,individuals with this profile often terminate treatment early.
PERSONAL INJURY (NEUROLOGICAL) CONSIDERATIONS
The validity profile suggests that there are questionable aspects of his performance that must beaddressed before credibility can be assured. Some problems are evident in his MMPI-2 profile. Hisprofile pattern indicates an interest in portraying himself as being physically disabled. He reportedextensive vague physical problems that are unlikely to be the result of a specific physical disorder. Thisis most likely the result of a long-term, chronic pattern of somatization that stems from basic ingrainedpersonality problems. He reports being unable to function effectively because of his physical symptoms,which appear to intensify when he faces life conflicts. Individuals with this clinical pattern tend to beuninsightful when it comes to understanding the causes of their symptoms, in part because they prefer torely on medical explanations for their symptoms. Individuals with this pattern often obtain substantialsecondary gain from their symptoms.
In addition to the problems indicated by his MMPI-2 clinical scale scores, he endorsed some items onthe content scales that could reflect difficulties for him. His proneness to experience problems with hishealth might make it difficult for him to think clearly or function effectively.
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 5 Del C.
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 9 Del C.
SAMPLE
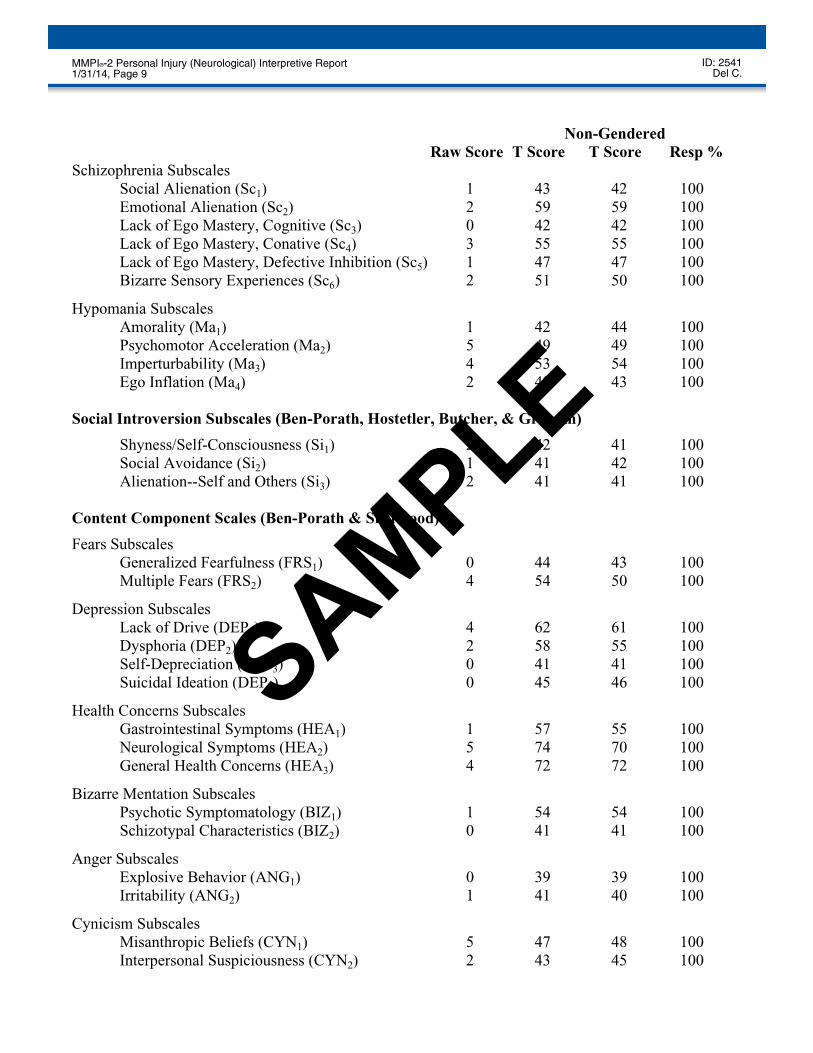
Non-GenderedRaw Score T Score T Score Resp %
Uniform T scores are used for Hs, D, Hy, Pd, Pa, Pt, Sc, Ma, the content scales, the content componentscales, and the PSY-5 scales. The remaining scales and subscales use linear T scores.
Gass Head Injury Items
The Gass Correction for Head Injury has been found to be useful in accounting for some scaleelevations in neuropsychological cases. The client endorsed 1 of the 14 Gass Correction items in thescored direction. The practitioner might consider the effect of reducing the designated scale raw scoresin this case if there is a history of head injury that might account for the scale elevations. The items andtheir scale membership are listed below. (See Appendix A of the User's Guide or Gass, 1991.)
179. Item Content Omitted. (False) Scales 1, 3, and 8
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 10 Del C.
Special Note: The content of the test items is included in the actual reports. To protect the integrity of the test, the item content does not appear in this sample report.
ITEMSNOT
SHOWN
SAMPLE
NOTE: This MMPI-2 interpretation can serve as a useful source of hypotheses about clients. This reportis based on objectively derived scale indices and scale interpretations that have been developed withdiverse groups of people. The personality descriptions, inferences, and recommendations containedherein need to be verified by other sources of clinical information because individual clients may notfully match the prototype. The information in this report should only be used by a trained and qualifiedtest interpreter. The report was not designed or intended to be provided directly to clients. Theinformation contained in the report is technical and was developed to aid professional interpretation.
This and previous pages of this report contain trade secrets and are not to be released in response torequests under HIPAA (or any other data disclosure law that exempts trade secret information fromrelease). Further, release in response to litigation discovery demands should be made only in accordancewith your profession's ethical guidelines and under an appropriate protective order.
ID: 2541MMPI®-2 Personal Injury (Neurological) Interpretive Report 1/31/14, Page 11 Del C.