32
Case Discussion: Redefining Best Practices in HCV Management in the Transplant Setting This activity is supported by an independent educational grant from Gilead Sciences
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | herbert-todd |
| View: | 216 times |
| Download: | 1 times |
Case Discussion: Redefining Best Practices in HCV Management in the Transplant Setting
This activity is supported by an independent educational grant from Gilead Sciences

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Faculty
Program Director
Norah Terrault, MD, MPH Professor of Medicine and SurgeryDepartment of MedicineDivision of GastroenterologyUniversity of California, San FranciscoSan Francisco, California
Additional Faculty
Jean C. Emond, MDThomas S. Zimmer Professor of Surgery Executive Director, Transplant InitiativeNewYork-Presbyterian HospitalColumbia University Medical CenterNew York, New York
Paul Y. Kwo, MDProfessor of MedicineMedical Director of TransplantationDivision of Medicine/Gastroenterology/ HepatologyIndiana University School of MedicineIndianapolis, Indiana

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 1: 62-Yr-Old Female With Cirrhosis and HCC GT1a HCV, IL28B CT
Previous treatment
– Standard IFN for 1 yr followed by 5 yrs of maintenance IFN
– Most recently triple therapy with pegIFN/RBV + boceprevir in 2012: nonresponder
History of varices (on nadolol) but no prior bleeding
No ascites, hepatic encephalopathy, or infectious complications
3-mm HCC treated with TACE and RFA without residual HCC on latest CT
History of depression, on citalopram
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
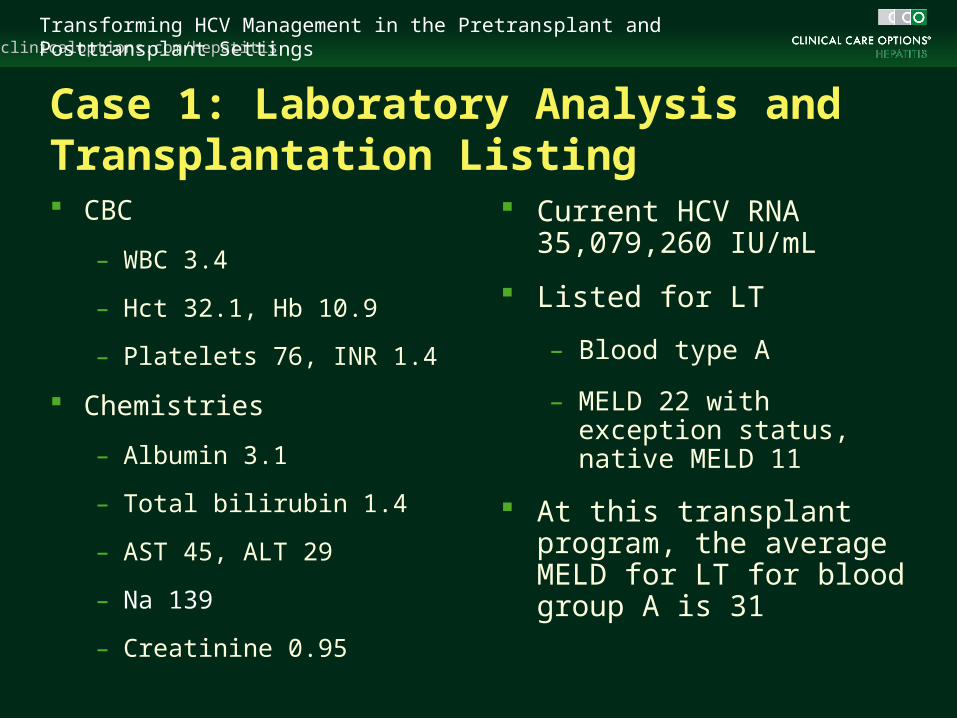
Case 1: Laboratory Analysis and Transplantation Listing CBC
– WBC 3.4
– Hct 32.1, Hb 10.9
– Platelets 76, INR 1.4
Chemistries
– Albumin 3.1
– Total bilirubin 1.4
– AST 45, ALT 29
– Na 139
– Creatinine 0.95
Current HCV RNA 35,079,260 IU/mL
Listed for LT
– Blood type A
– MELD 22 with exception status, native MELD 11
At this transplant program, the average MELD for LT for blood group A is 31
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: Should Further Tests Be Ordered? Some experts would order additional testing if simeprevir
is being considered
– Resistance testing, given the failure on boceprevir and the potential for cross resistance
– Q80K, since SVR rates are reduced with simeprevir for patients having this polymorphism

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: What HCV Treatment Approach Would You Recommend? 2 potential approaches
– Viral suppression
– Try for SVR
Sofosbuvir + RBV for long-term suppression or sofosbuvir + simeprevir ± RBV for SVR were approaches favored by the panel
Child’s-Pugh classification should be considered when making choice to ensure medications are safe for the individual patient

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 1: Follow-up
Treatment deferred until exception MELD = 29, then started on sofosbuvir 400 mg/day and RBV 800 mg/day
HCV RNA results
– Baseline: 35 million IU/mL
– Wk 1: 14,334 IU/mL
– Wk 2: 2274 IU/mL
– Wks 4, 6, and 8: < 43, DETECTED
Tolerating well except for mild anemia
– RBV reduced to 600 mg/day for Hct decline to 29 at Wk 4
– MELD upgraded to 31 (average MELD at LT in this region)

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
On-Treatment VR With SOF + RBV in Patients With CTP-A and CTP-B Cirrhosis
Afdhal N, et al. EASL 2014. Abstract O68.
HC
V R
NA
< L
LO
Q (
%)
100
80
60
40
20
0Wk 2 Wk 4 Wk 8 Wk 12
56
100 94
Wk 24
CTP ACTP B
44
75
100 100 10094 93
N = 25

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: What Would You Do Next? Some experts would consider adding an additional agent
to try to achieve SVR prior to transplantation
– Simeprevir or daclatasvir (compassionate use)
Timing of expected transplantation an important consideration
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
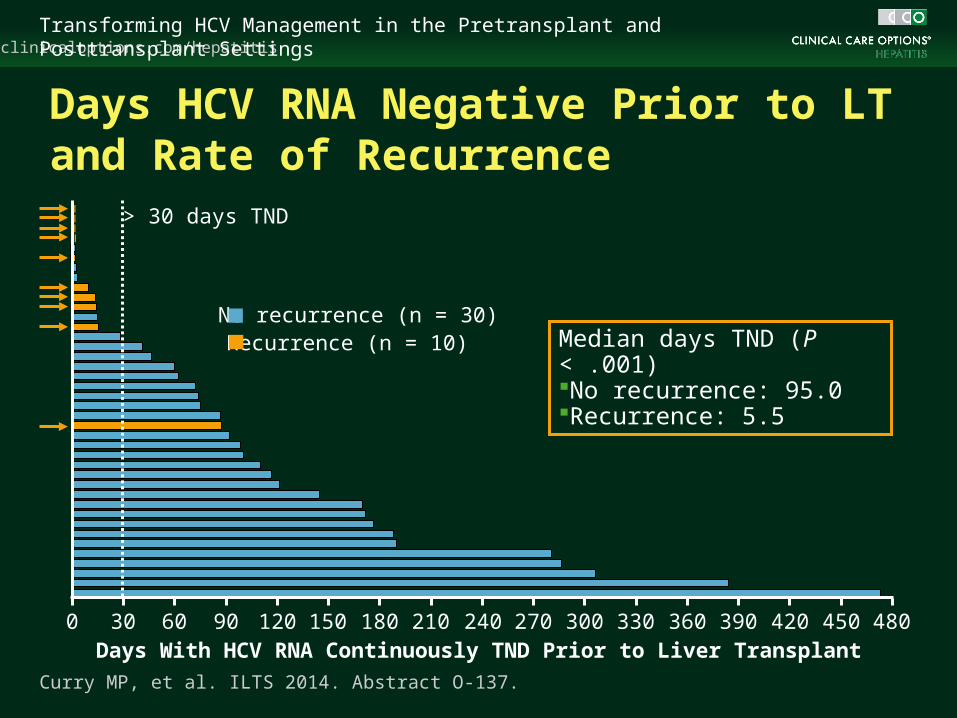
Days HCV RNA Negative Prior to LT and Rate of Recurrence
Median days TND (P < .001)No recurrence: 95.0Recurrence: 5.5
No recurrence (n = 30)
> 30 days TND
Recurrence (n = 10)
Curry MP, et al. ILTS 2014. Abstract O-137.
0 30 60 90 120 150 180 210 240 270 300 330 360 390 420 450 480Days With HCV RNA Continuously TND Prior to Liver Transplant
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
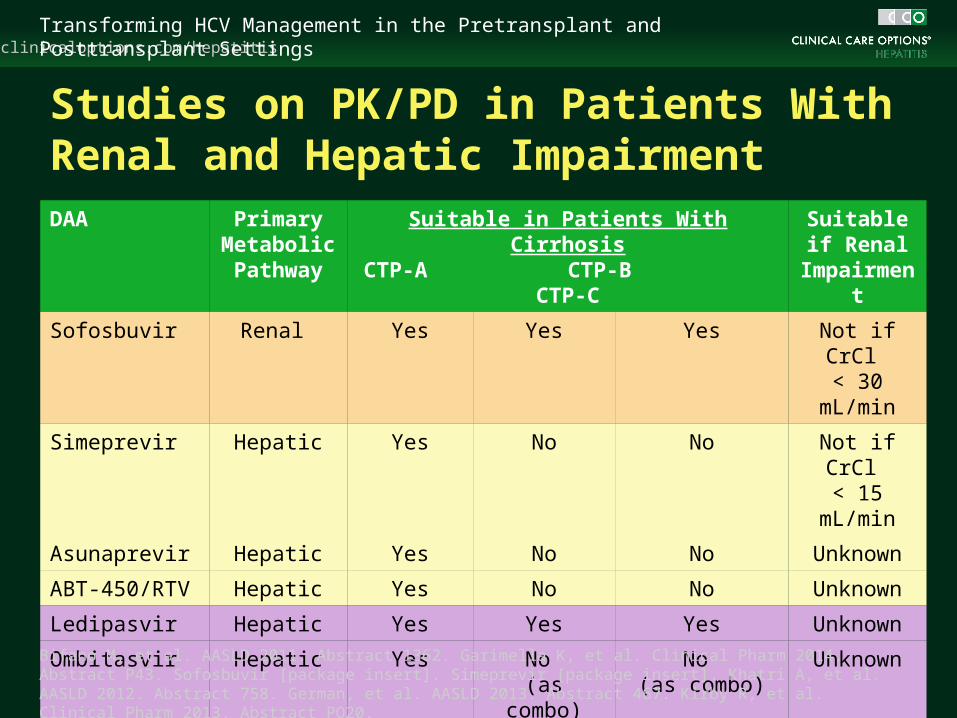
DAA Primary Metabolic Pathway
Suitable in Patients With CirrhosisCTP-A CTP-B CTP-C
Suitable if Renal
Impairment
Sofosbuvir Renal Yes Yes Yes Not if CrCl < 30 mL/min
Simeprevir Hepatic Yes No No Not if CrCl < 15 mL/min
Asunaprevir Hepatic Yes No No Unknown
ABT-450/RTV Hepatic Yes No No Unknown
Ledipasvir Hepatic Yes Yes Yes Unknown
Ombitasvir Hepatic Yes No (as combo)
No (as combo)
Unknown
Daclatasvir Hepatic Yes Yes Yes Yes
Dasabuvir Hepatic Yes No No UnknownBifano M, et al. AASLD 2011. Abstract 1362. Garimella K, et al. Clinical Pharm 2014. Abstract P43. Sofosbuvir [package insert]. Simeprevir [package insert]. Khatri A, et al. AASLD 2012. Abstract 758. German, et al. AASLD 2013. Abstract 467. Kirby R, et al. Clinical Pharm 2013. Abstract PO20.
Studies on PK/PD in Patients With Renal and Hepatic Impairment

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: New Considerations With All-Oral Therapy in the Pretansplant Setting All-oral therapy offers safe, effective option for wait-list
patients
Best outcomes with sofosbuvir + RBV pre-LT achieved if HCV RNA is undetectable for > 4 wks prior to LT
– Approved for treatment up to 48 wks
Lack of data on safety in patients with advanced renal and liver disease may limit treatment options
– Sofosbuvir not recommended if CrCl < 30 mL/min
– Simeprevir not recommended if CTP B or C disease
– Daclatasvir (compassionate access) may be option if advanced liver or renal disease
Case 2

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 2: 59-Yr-Old Male With GT3 HCV Who Received Liver Transplantation 59-yr-old male with cirrhosis due to HCV
Underwent transplantation with deceased donor (age 50 yrs, CDC high risk)
GT3A HCV, IL28B CT, treatment naive
Past history
– CAD, s/p LAD stent placement 2013
– Hypertension and dyslipidemia
Early posttransplantation course complicated by early mild rejection, managed with increase in tacrolimus dose
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
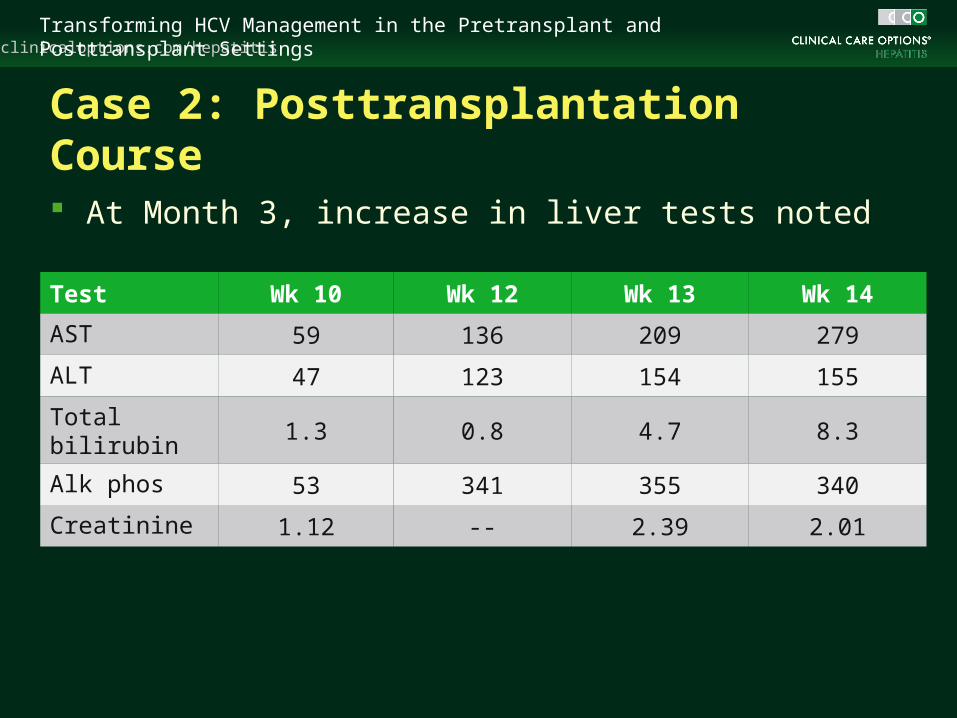
Case 2: Posttransplantation Course
At Month 3, increase in liver tests noted
Test Wk 10 Wk 12 Wk 13 Wk 14
AST 59 136 209 279
ALT 47 123 154 155
Total bilirubin 1.3 0.8 4.7 8.3
Alk phos 53 341 355 340
Creatinine 1.12 -- 2.39 2.01
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
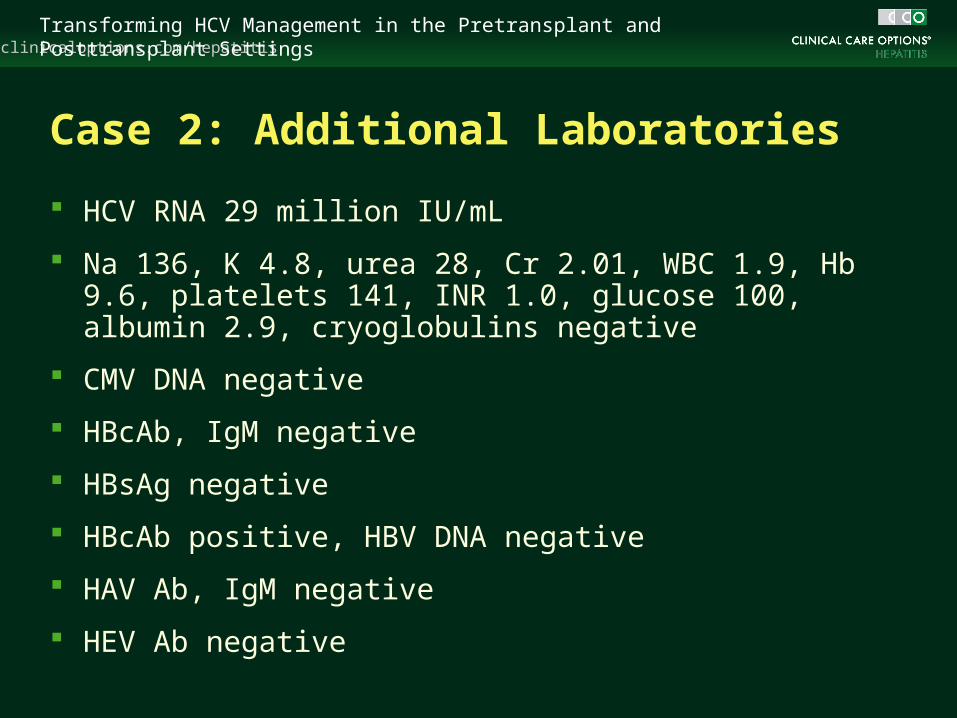
Case 2: Additional Laboratories
HCV RNA 29 million IU/mL
Na 136, K 4.8, urea 28, Cr 2.01, WBC 1.9, Hb 9.6, platelets 141, INR 1.0, glucose 100, albumin 2.9, cryoglobulins negative
CMV DNA negative
HBcAb, IgM negative
HBsAg negative
HBcAb positive, HBV DNA negative
HAV Ab, IgM negative
HEV Ab negative

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 2: Follow-up Liver Biopsy
Ultrasound results
– Heterogeneity of liver parenchyma, no biliary dilatation, hepatic and portal veins patent, spleen normal size, no fluid collections
Liver transplantation biopsy
– Chronic hepatitis consistent with recurrent hepatitis C with septal fibrosis and features suggestive of an aggressive/fibrocholestatic variant; no evidence of rejection
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: Management Approach for Severe Recurrence For a patient with genotype 3, options are limited
– Sofosbuvir plus ribavirin or sofosbuvir plus daclatasvir (compassionate use)
Additional options could be considered for genotype 1
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
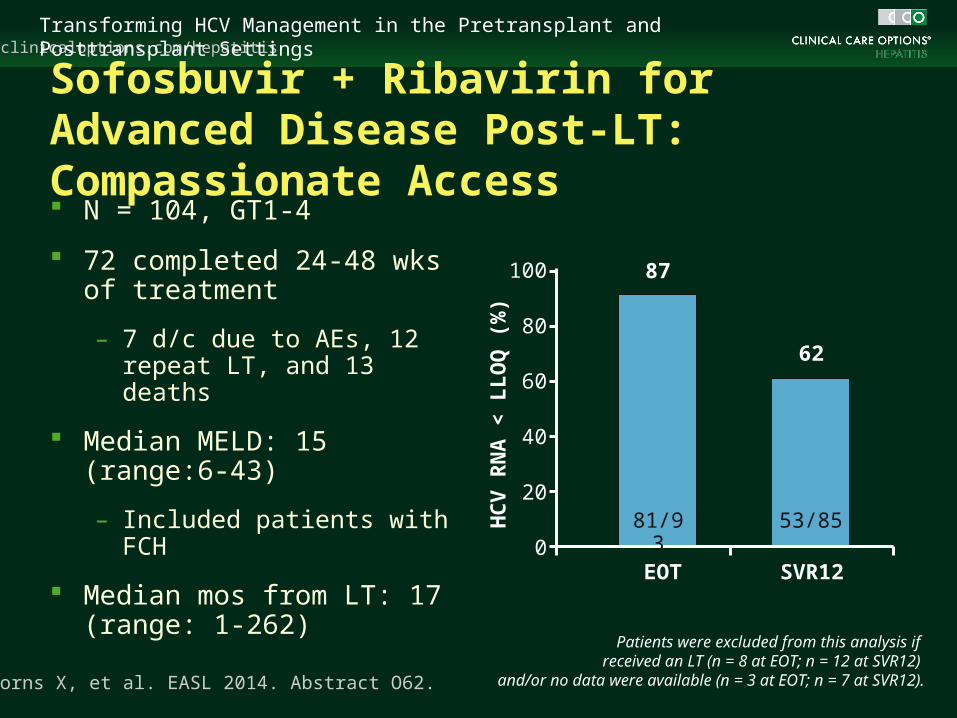
Sofosbuvir + Ribavirin for Advanced Disease Post-LT: Compassionate Access N = 104, GT1-4
72 completed 24-48 wks of treatment
– 7 d/c due to AEs, 12 repeat LT, and 13 deaths
Median MELD: 15 (range:6-43)
– Included patients with FCH
Median mos from LT: 17 (range: 1-262)
Forns X, et al. EASL 2014. Abstract O62.
EOT SVR12
HC
V R
NA
< L
LO
Q (
%)
100
80
60
40
20
0
87
62
81/93 53/85
Patients were excluded from this analysis if received an LT (n = 8 at EOT; n = 12 at SVR12)
and/or no data were available (n = 3 at EOT; n = 7 at SVR12).

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Clinical Case: Fibrosing Cholestatic Hepatitis
0 4 8/0 4 8 12 16 20 24/0 4 8
HC
V R
NA
(IU
/mL
)
Biliru
bin
Leve
l (mg
/dL
)
108
106
104
102
LOD
Wk
25
20
15
10
5
1
HCV RNA: 541,000,000 IU/mL
Fibrosing Cholestatic Hepatitis Diagnosed 2 Mos After LT
TE: 9.6 kPaLT TE: 17 kPa Ascites No Ascites
*Bilirubin normalized at Wk 9.
After LT SOF + RBV TreatmentPost-
treatmentFollow-up
HCV RNA Bilirubin level
*
Forns X, et al. AASLD 2013. Abstract 1084.

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel: New Considerations With All-Oral Therapy for Severe Recurrence PegIFN is best avoided in the early post-LT period
SOF + RBV offers pangenotypic option for FCH and safety supported by compassionate access experience
Other oral combinations likely in future, but applicability will be depend on safety and PK/PD in moderate to severe hepatic impairment (typical of FCH)
GT3 recurrence has limited options for treatment
– SOF + RBV ± pegIFN
– Combination of SOF + NS5A inhibitors (LDV or DCV) can be considered in future
– Protease inhibitors not effective
Case 3
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 3: 63-Yr-Old Male Transplanted 13 Yrs Ago With Cirrhosis on Recent Biopsy 63-yr-old male with transplanted HCV in 2001
Recent liver biopsy shows recurrent disease with stage 4 fibrosis (cirrhosis) and grade 2 necroinflammation
Previous post-LT treatment
– PegIFN/RBV (null response, stopped after 3 mos)
– PegIFN/RBV + telaprevir x 48 wks (response with relapse)
– No treatment in past yr
Returns to discuss treatment options in light of newly approved therapies
GT1b HCV, IL28B TT
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 3: History and Laboratories
Past history
– Hypertension, controlled
– Diabetes, HbA1c 7.6
– Mild renal insufficiency, creatinine 1.6
– Depression, stable on citalopram
– No history of rejection
Immunosuppression: tacrolimus 1 mg BID with trough level 4.6
Laboratories
– WBC 4.3, Hb 11, platelets 74, INR 1.2
– AST 70, ALT 65, alk phos 104, total bilirubin 1.0, albumin 3.4
– Cr 1.6, Na 139, K 3.8
– HCV RNA 1.2 million IU/mL
– NS3A/4 GenoSure: negative for resistance mutations

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
New HCV Regimens Under Study in Posttransplantation Patients
1. Samuel D., et al. EASL 2014. Abstract P1232. 2. Forns X, et al. EASL 2014. Abstract O62. 3. Kwo PY, et al. EASL 2014. Abstract O114. 4. Pellicelli A, et al. Dig Liver Dis. 2014;46:923-927.
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
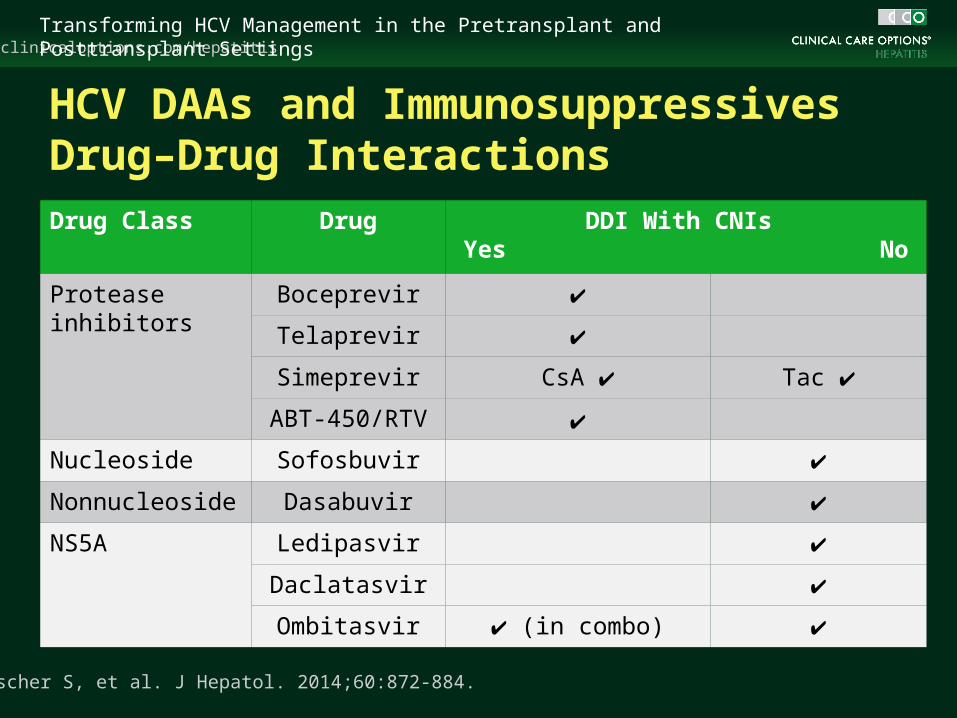
HCV DAAs and ImmunosuppressivesDrug–Drug Interactions Drug Class Drug DDI With CNIs
Yes No
Protease inhibitors
Boceprevir ✔
Telaprevir ✔
Simeprevir CsA ✔ Tac ✔
ABT-450/RTV ✔
Nucleoside Sofosbuvir ✔
Nonnucleoside Dasabuvir ✔
NS5A Ledipasvir ✔
Daclatasvir ✔
Ombitasvir ✔ (in combo) ✔
Tischer S, et al. J Hepatol. 2014;60:872-884.

clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Case 3: Initial Treatment and Results
Started on sofosbuvir 400 mg/day + simeprevir 150 mg/ day with planned treatment duration of 12 wks
HCV RNA on treatment
– Baseline: 1,357,200
– Wk 2: 3100
– Wk 4: < 25, DETECTED
– Wk 6: < 25, DETECTED
– Wk 8: < 25, DETECTED
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
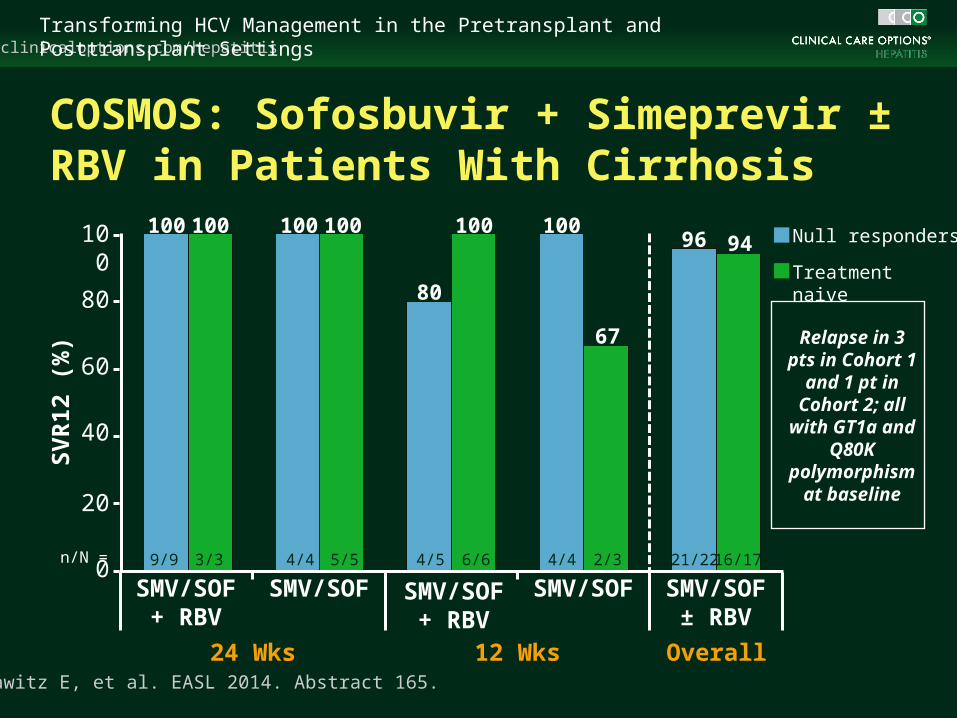
COSMOS: Sofosbuvir + Simeprevir ± RBV in Patients With Cirrhosis
Lawitz E, et al. EASL 2014. Abstract 165.
Null responders
Treatment naive
Relapse in 3 pts in Cohort 1
and 1 pt in Cohort 2; all
with GT1a and Q80K
polymorphism at baseline
24 Wks 12 Wks Overall
SV
R12
(%
)
n/N =
100
80
60
40
20
0SMV/SOF
+ RBVSMV/SOF SMV/SOF
+ RBVSMV/SOF SMV/SOF
± RBV
9/9 3/3 4/4 5/5 4/5 6/6 4/4 2/3 21/22 16/17
100 100 100 100
80
100 100
67
96 94
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Panel Discussion: New Considerations With All-Oral Therapy for Posttransplant IFN-free therapies offer advantages over previous
pegIFN/RBV/ PI therapy
– High efficacy and significantly improved tolerability
Anticipate more IFN-free and RBV-free options in near future (within 2014 in the US)
As choices increase, the factors that are likely to influence treatment choices are:
– DDIs
– Previous treatment experience (resistance)
– Availability/cost
clinicaloptions.com/hepatitisTransforming HCV Management in the Pretransplant and Posttransplant Settings
Summary
Renal and hepatic clearance of DAAs
– Impact on management/treatment choice pretransplantation and posttransplantation
NS5A inhibitors and polymerase inhibitors do not have clinically significant DDIs with immunosuppression
– Simeprevir has DDI with cyclosporine, but not tacrolimus
IFN-free therapy add a much greater degree of safety and tolerability than previous therapies

Go Online for More From This Program!
Downloadable slides for use in your own presentations
clinicaloptions.com/transforming




![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://static.documents.pub/doc/80x56/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)












