47
Case history 2
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | smrithi3 |
| View: | 245 times |
| Download: | 0 times |
Case history 2
45 years old, female
Pandikadu
Agriculture worker,
History from husband

Presenting complaints
1. Deviation of angle of mouth to left
2. Weakness of right upper and lower limbs 12 days
History of present illness
Abrupt onset deviation of angle of mouth to left side and weakness of both right upper and lower limb for last 12 days
• Attended a funeral function and was stressed after that, complained of sudden onset giddiness
• 2-3 hours later relatives found her lying floppy on the bed, was unconscious, not respondingto call, not moving any limb with deviation of angle of mouth towards left.
On the way, there was abnormal jerky movement of all limbs, lasted for few minutes.
It was associated with frothy discharge from mouth, involuntary passage of urine. No h/o tongue biting.
Was admitted in ICU, bladder catheterised, nasogastric tube inserted.
Shifted to ward 3 days back, was drowsy, not oriented to place or person, unable to move right upper and lower limb, butopens her left eye when called, speech output was nil except for some grunting
sound she produce.
Not able to open her right eye
History of faecal incontinence
No h/o fever, headache, projectile vomiting, neck stiffness
No h/o (nasal regurgitation)
History of past illness
Had history of fever and joint pain 22 years back.
• 6 months later she had gradual onset dyspnoea( NYHA II)
• Fever, respiratory infections aggravated the symptoms. Within 2 years symptoms worsened (NYHA III)
• Associated with palpitation, irregular, rest
• Detected to have valvular heart disease, advised surgery,13 yrs back
• On regular medication (Kaypen, Betaloc, Amifru) daily, also advised to reduce emotional stress and severe exertion.
• (She was unable to continue medication for 20 days before admission)
• h/o orthopnea and paroxysmal nocturnal dyspnoea for past 4-5 months
• h/o recurrent fever, sore throat
• h/o hypertension for past 20 years, on medication
• No h/o diabetes, treatment for pulmonary tuberculosis, epilepsy
• No h/o similar weakness
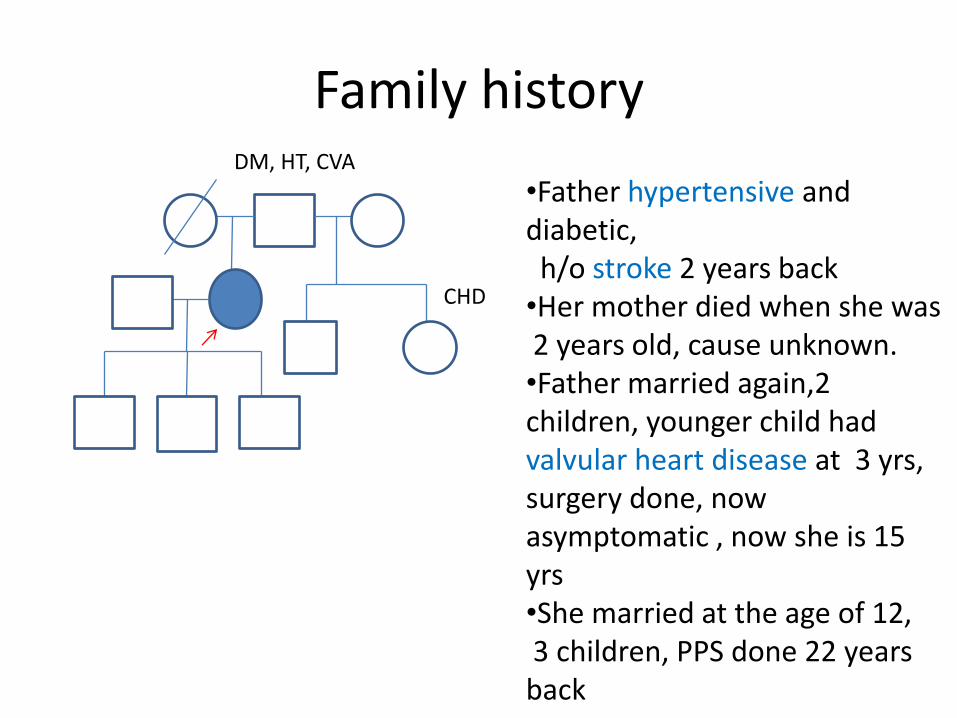
Family historyDM, HT, CVA
CHD
•Father hypertensive and diabetic, h/o stroke 2 years back
•Her mother died when she was 2 years old, cause unknown.•Father married again,2 children, younger child had valvular heart disease at 3 yrs, surgery done, now asymptomatic , now she is 15 yrs•She married at the age of 12,3 children, PPS done 22 years back
Personal history
• Takes mixed diet
• Sleep and appetite normal prior to onset of symptoms
• Bladder incontinence present and catheterised
• Bowel incontinence present one episode
• No addictions
Socioeconomic history
• Living with her family in 3 bed room concrete house, husband is an agricultural worker, proper water and sanitation facilities. Belongs to a middle class family.
General examination
• Lying supine on bed
• Drowsy, responds to painful stimuli & localises it
• Moderately build and nourished
• Pallor and clubbing (grade I) present
• No icterus, cyanosis, lymphadenopathy, pedal oedema
• Nasogastric tube in situ
• Bladder catheterised, clear urine
• IV cannula present on both hands.
Vital signs
• Pulse rate: 103/min
• Irregularly irregular, with apex pulse deficit 13/min
• Variable volume
• Character and condition of vessel wall normal
• No radio radial or radio femoral delay
• All peripheral pulses palpable bilaterally equal

• Blood pressure: 110/70 mm Hg, right arm supine position
• Respiratory rate: 42/min, regular, thoracoabdominal
• She is afebrile
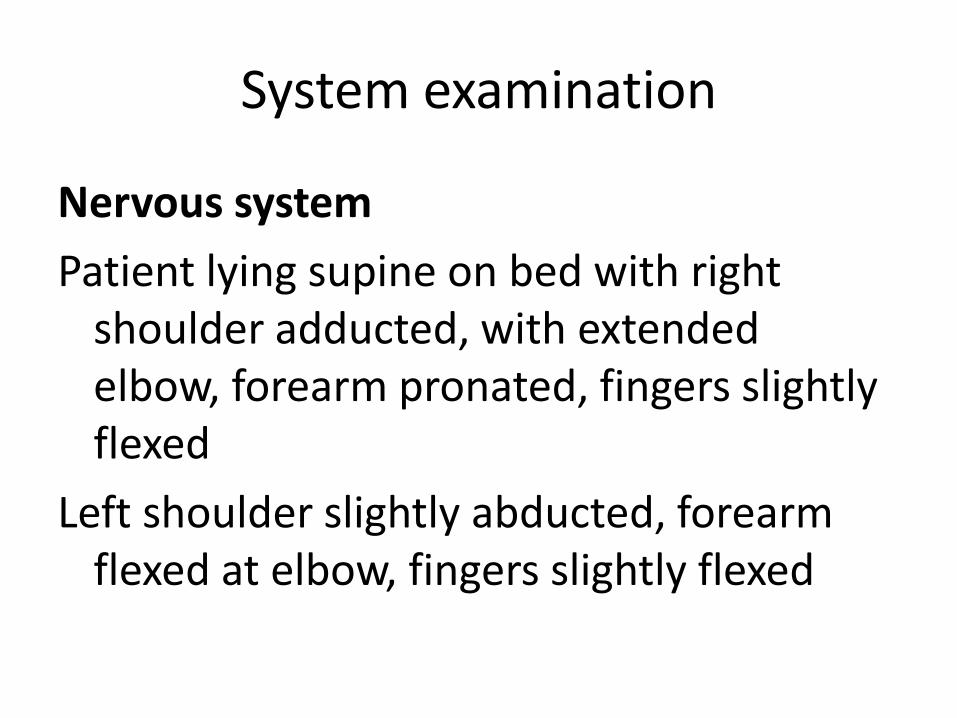
System examination
Nervous system
Patient lying supine on bed with right shoulder adducted, with extended elbow, forearm pronated, fingers slightly flexed
Left shoulder slightly abducted, forearm flexed at elbow, fingers slightly flexed
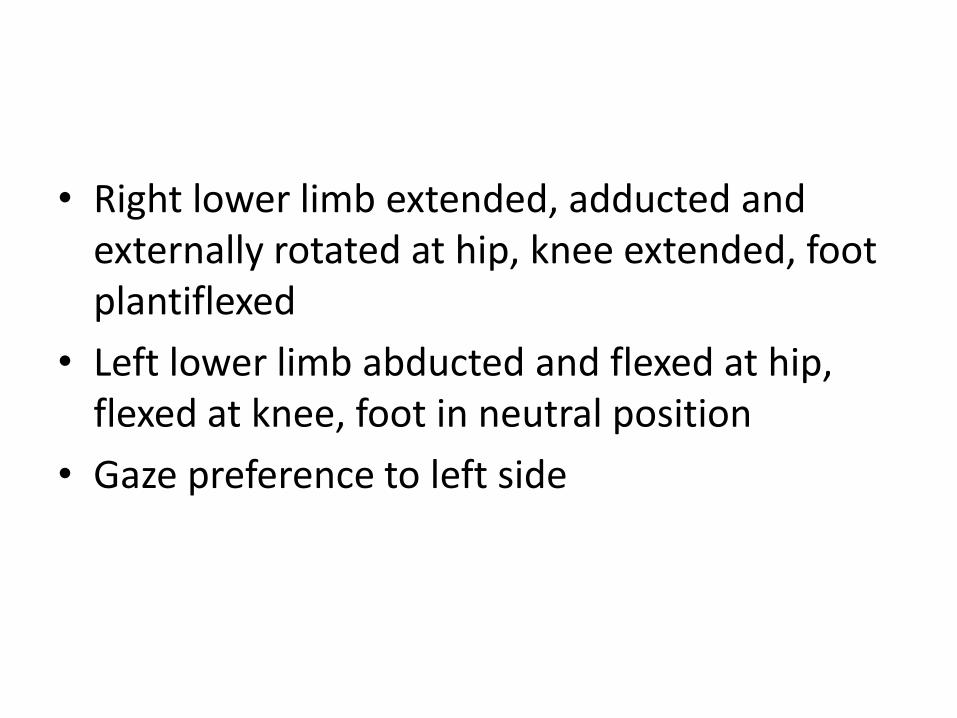
• Right lower limb extended, adducted and externally rotated at hip, knee extended, foot plantiflexed
• Left lower limb abducted and flexed at hip, flexed at knee, foot in neutral position
• Gaze preference to left side
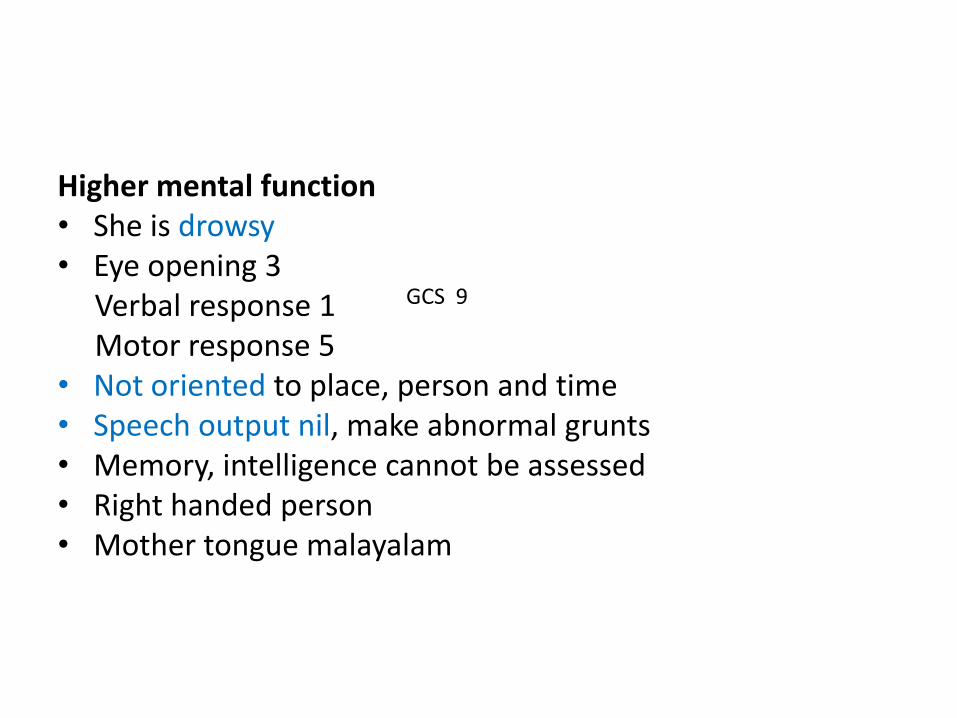
Higher mental function• She is drowsy• Eye opening 3
Verbal response 1Motor response 5
• Not oriented to place, person and time• Speech output nil, make abnormal grunts• Memory, intelligence cannot be assessed• Right handed person• Mother tongue malayalam
GCS 9
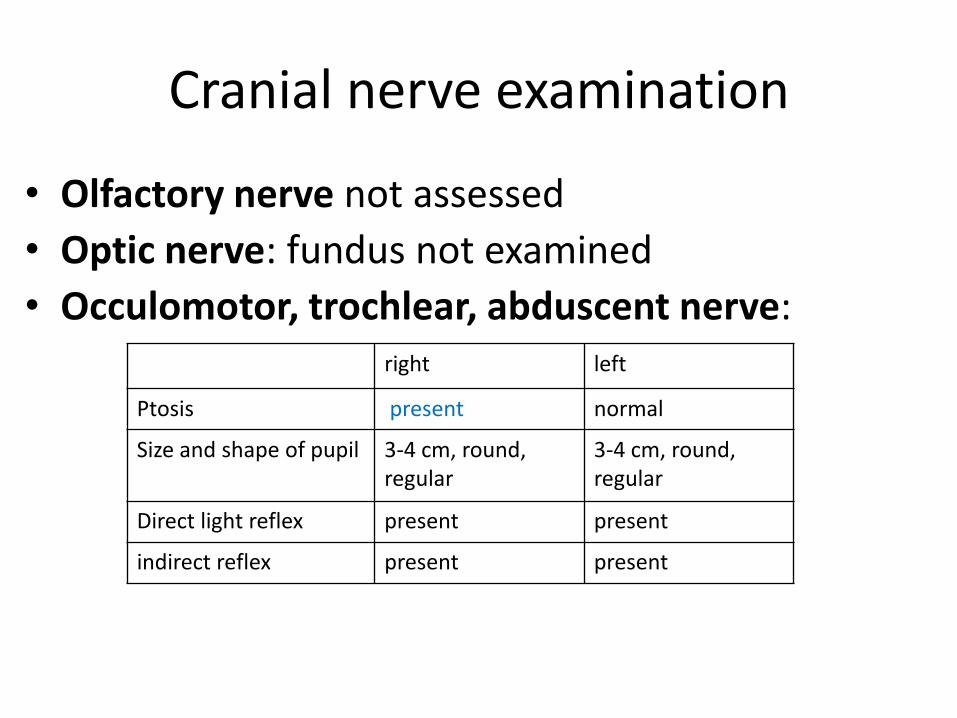
Cranial nerve examination
• Olfactory nerve not assessed
• Optic nerve: fundus not examined
• Occulomotor, trochlear, abduscent nerve: right left
Ptosis present normal
Size and shape of pupil 3-4 cm, round, regular
3-4 cm, round, regular
Direct light reflex present present
indirect reflex present present
• Trigeminal nerve: corneal and conjunctivalreflex not assessed
• Facial nerve: Angle of mouth deviated to left
Nasolabial fold absent on right
Grimace absent on right
• Vestibulocochlear nerve: normal dolls eye reflex
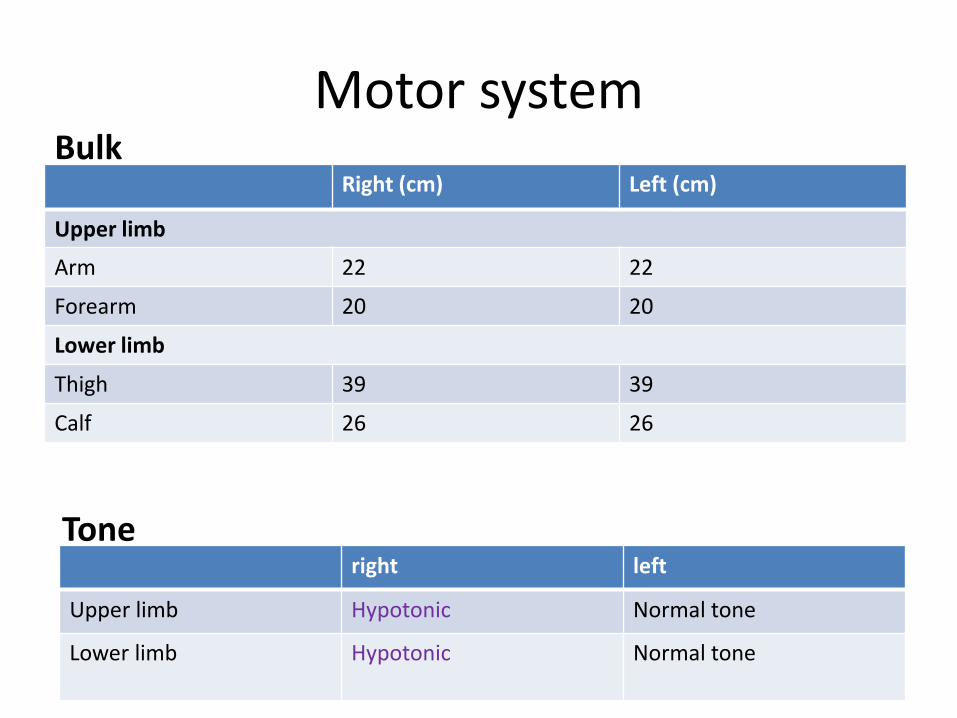
Motor system
Right (cm) Left (cm)
Upper limb
Arm 22 22
Forearm 20 20
Lower limb
Thigh 39 39
Calf 26 26
Bulk
Tone right left
Upper limb Hypotonic Normal tone
Lower limb Hypotonic Normal tone
• Power
• Right: Upper limb not moving (grade 0)
Lower limb not moving (grade 0)
• Left: Upper limb moving spontaneous against
gravity
Lower limb moving spontaneous against
gravity
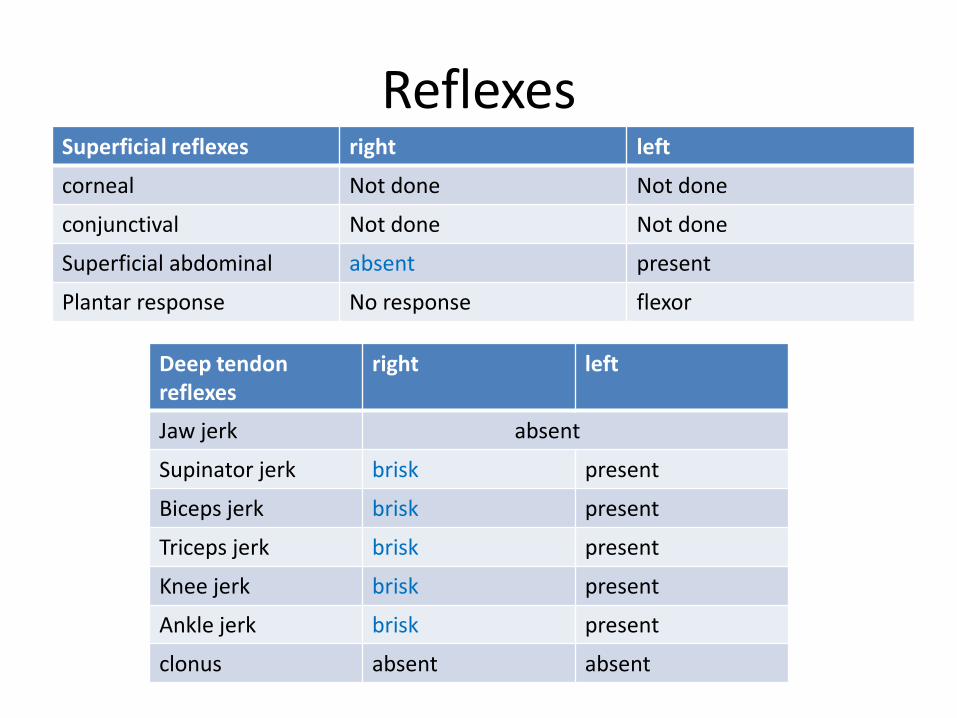
Reflexes Superficial reflexes right left
corneal Not done Not done
conjunctival Not done Not done
Superficial abdominal absent present
Plantar response No response flexor
Deep tendon reflexes
right left
Jaw jerk absent
Supinator jerk brisk present
Biceps jerk brisk present
Triceps jerk brisk present
Knee jerk brisk present
Ankle jerk brisk present
clonus absent absent
• Primitive reflexes absent
• Sensory system and coordination cannot be assessed
• No peripheral nerve thickening
• Skull and spine normal
• No carotid bruit

Cardiovascular system
• Inspection
• Prominent venous pulsations
• Trachea central
• Chest wall symmetrical
• No precordial bulge
• Apical impulse not visible
• No visible pulsations, scar, dilated vein
• Palpation
• JVP not measured
• Trachea central
• Apex beat palpable at left sixth intercostal space on midclavicular line, tapping in character
• Left parasternal impulse felt, no heave
• No thrill
• Palpable epigastric pulsation present
• Percussion
• Right cardiac border behind sternum
• Left cardiac border corresponds to apex
• 2nd left intercostal space resonant
• Liver dullness present in right fifth intercostalspace in mid clavicular line
Auscultation
• Mitral area: Loud 1st heart sound,
• 2nd heart sound heard with normal split
• No 3rd and 4th heart sound
• A low pitched diastolic rumbling murmur of grade III is audible at apex, without any radiation, with bell of stethoscope with patient lying in left lateral position, at the height of expiration, opening snap present.
• Tricuspid area
• Aortic area
1st heart sound normal2nd heart sound heard with normal splitNo 3rd and 4th heart soundsNo murmur
• Pulmonary area: 1st heart sound normal2nd heart sound loudNo 3rd and 4th heart soundsNo murmur

Respiratory system
• Trachea central, respiratory movements equal on both sides
• Normal vesicular breath sound normal intensity in all chest areas, bilateral basal crepitations present
Gastrointestinal system
• Shape of abdomen normal
• Liver not palpable
• Normal bowel sounds heard
Summary
• 45years old, lady, with past h/o rheumatic fever 22 years back,
• gradually progressive dyspnea, palpitation 6 months later,
• detected to have cardiac disease 18 years back on regular medication,
• hypertensive for past 18 years,
• orthopnea and paroxysmal nocturnal dyspneafor past 4 months,
• With drug default 20 days back presented with giddiness followed by loss of consciousness,
• Abrupt onset deviation of angle of mouth to left and weakness of right upper and lower limb for past 12 days,
• No speech output,
• Bladder and bowel incontinence present

• On examination pallor present,
clubbing grade I present,
• pulse rate 103/min, irregularly irregular, apex pulse deficit 13/min, variable volume, tachypnea present

• On nervous system examination,
• She is drowsy GCS 9,
• Nasolabial fold absent on right,
• Angle of mouth deviated to left,
• Right sided ptosis present,
• Hypotonic, brisk deep tendon reflexes and plantar response mute on right side
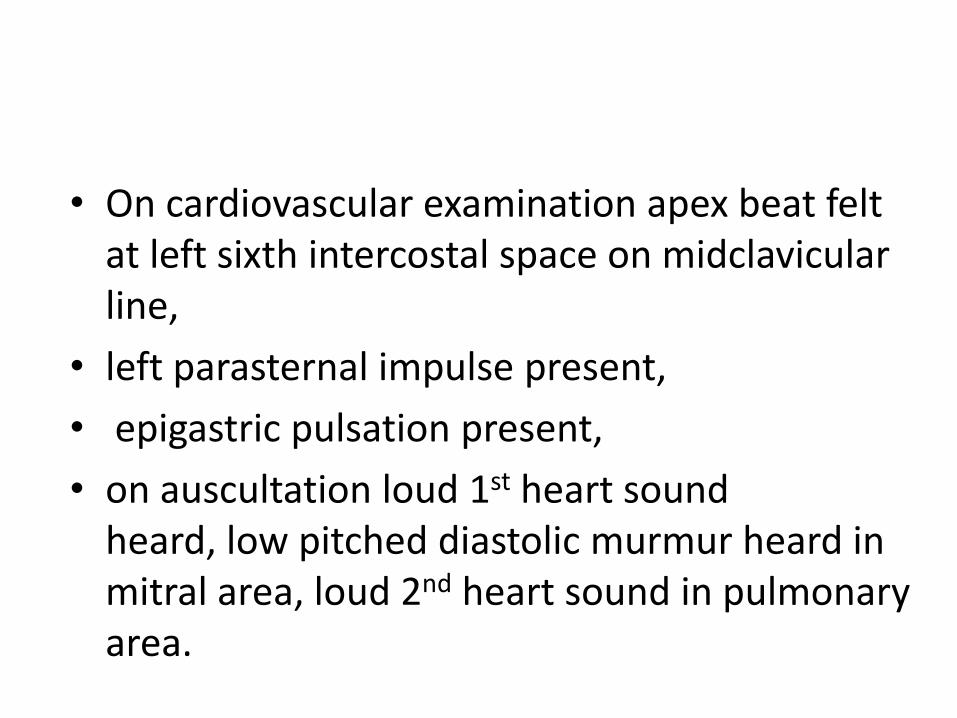
• On cardiovascular examination apex beat felt at left sixth intercostal space on midclavicularline,
• left parasternal impulse present,
• epigastric pulsation present,
• on auscultation loud 1st heart sound heard, low pitched diastolic murmur heard in mitral area, loud 2nd heart sound in pulmonary area.
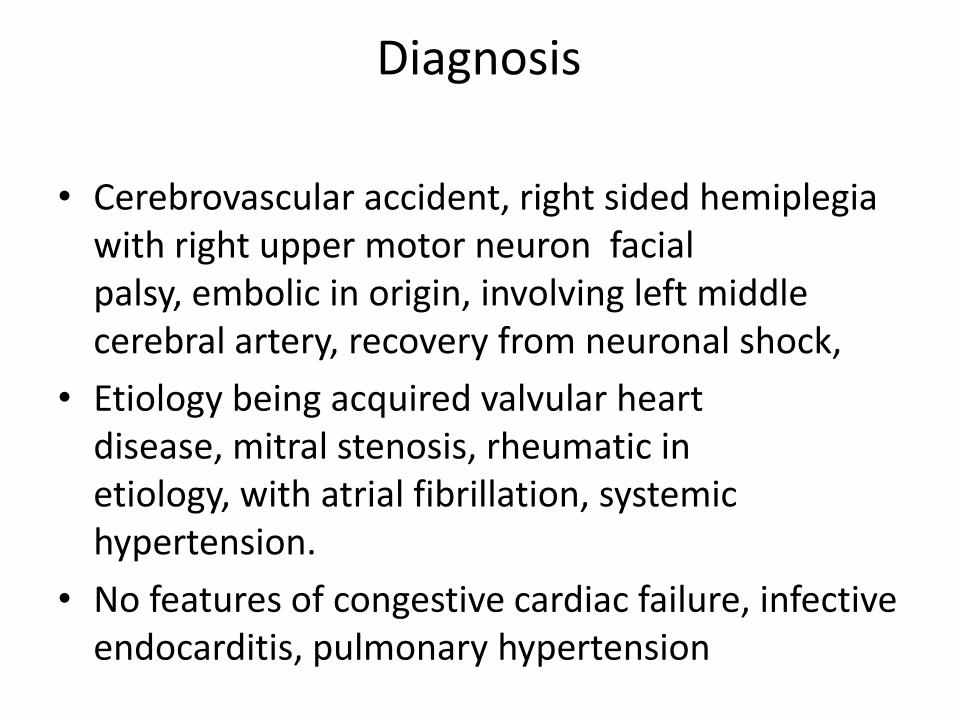
Diagnosis
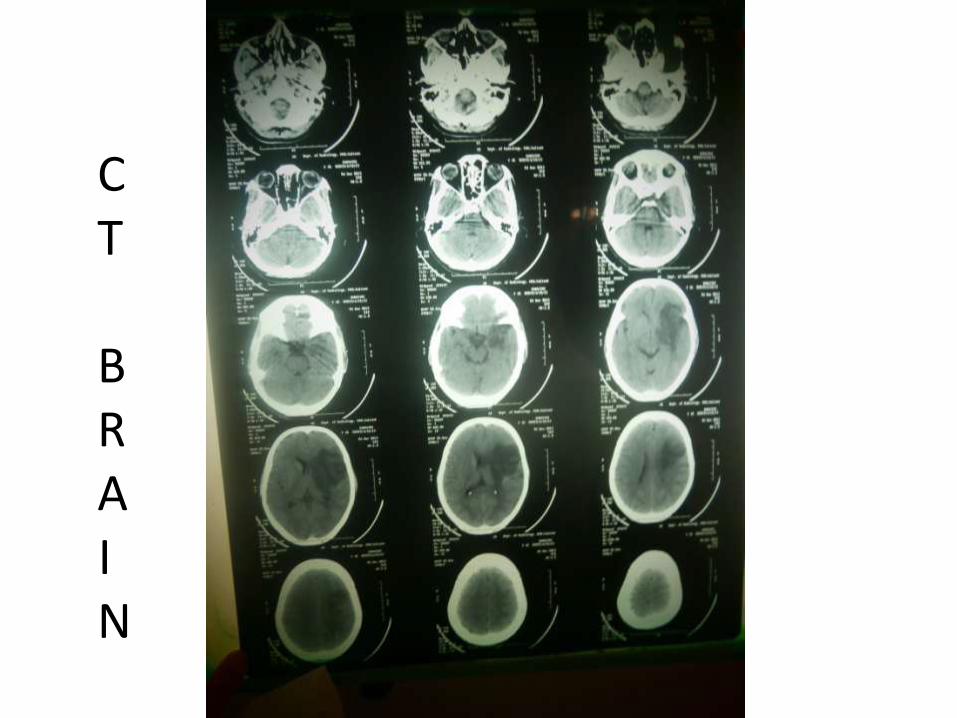
• Cerebrovascular accident, right sided hemiplegia with right upper motor neuron facial palsy, embolic in origin, involving left middle cerebral artery, recovery from neuronal shock,
• Etiology being acquired valvular heart disease, mitral stenosis, rheumatic in etiology, with atrial fibrillation, systemic hypertension.
• No features of congestive cardiac failure, infective endocarditis, pulmonary hypertension
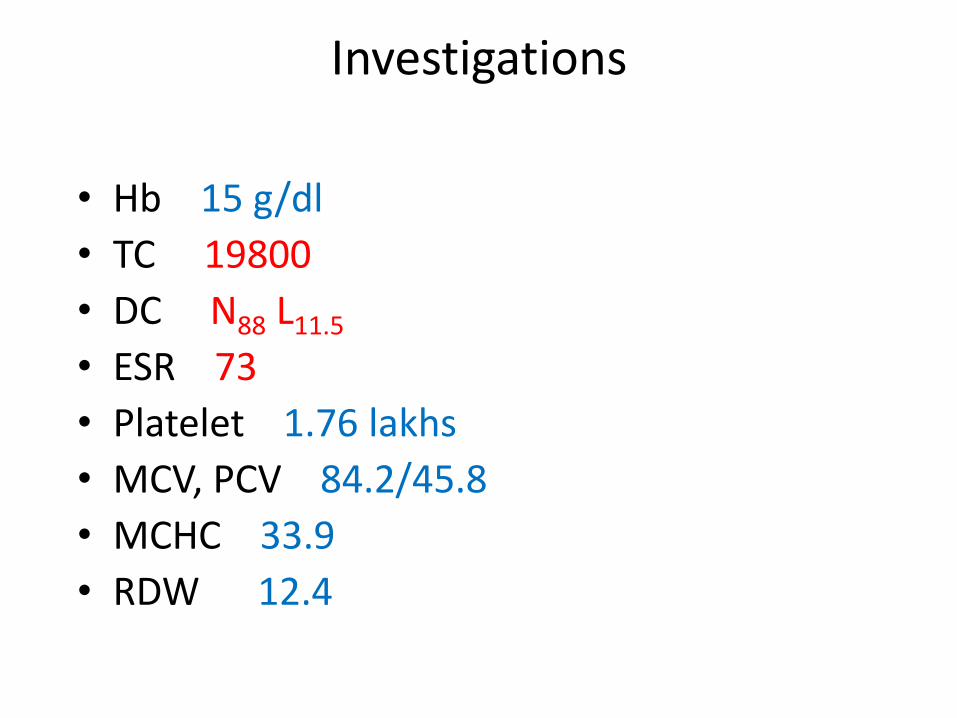
Investigations
• Hb 15 g/dl
• TC 19800
• DC N88 L11.5
• ESR 73
• Platelet 1.76 lakhs
• MCV, PCV 84.2/45.8
• MCHC 33.9
• RDW 12.4
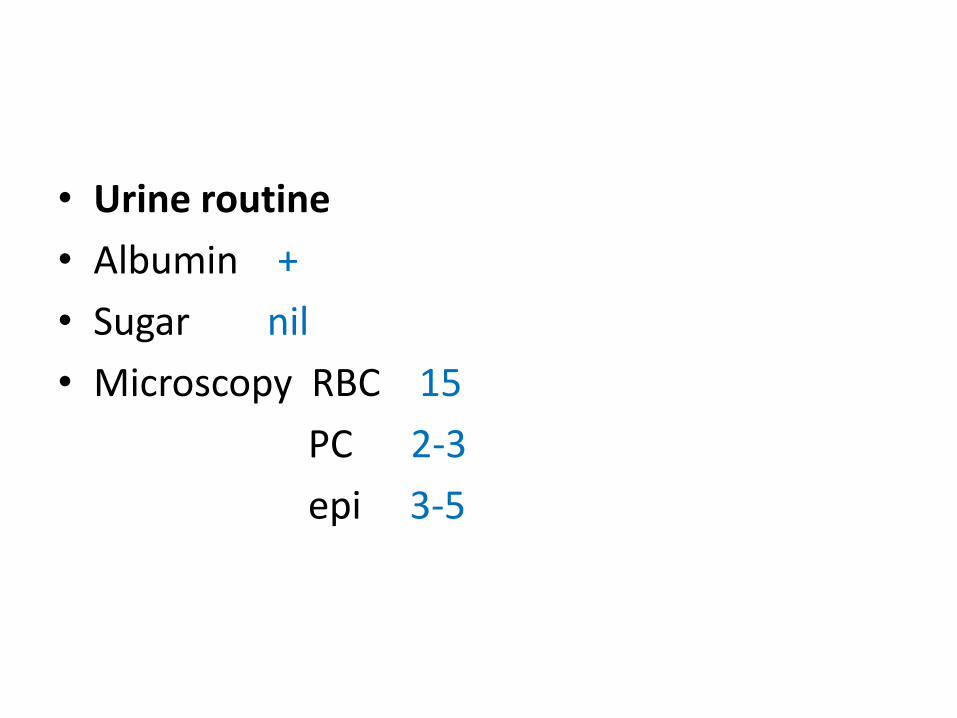
• Urine routine
• Albumin +
• Sugar nil
• Microscopy RBC 15
PC 2-3
epi 3-5
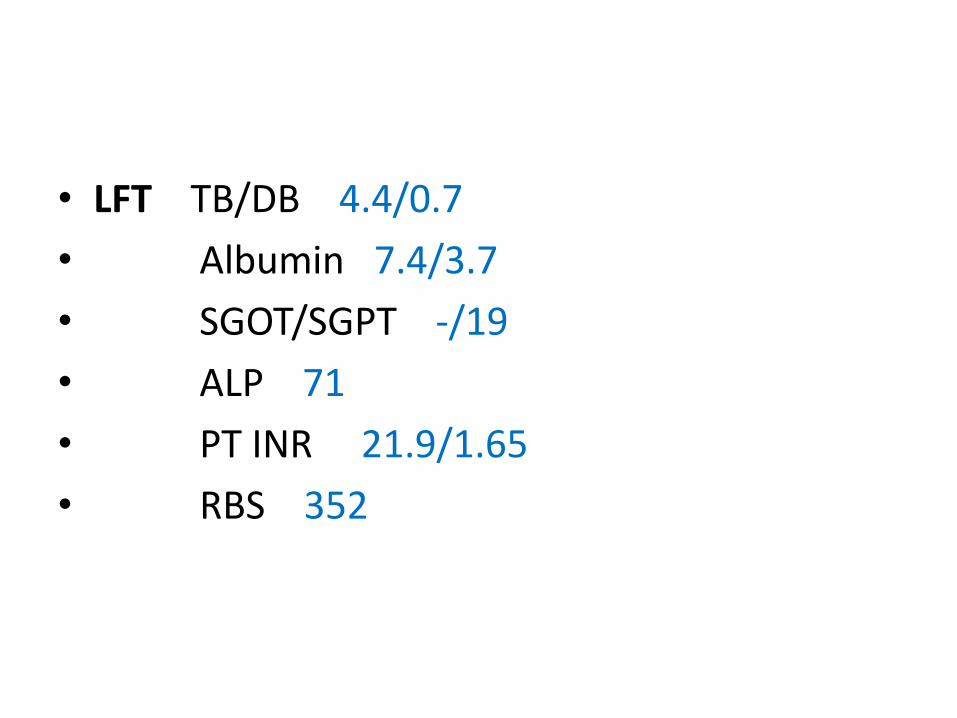
• LFT TB/DB 4.4/0.7
• Albumin 7.4/3.7
• SGOT/SGPT -/19
• ALP 71
• PT INR 21.9/1.65
• RBS 352

Chest X rayChest X-RAY
CT
BRAIN
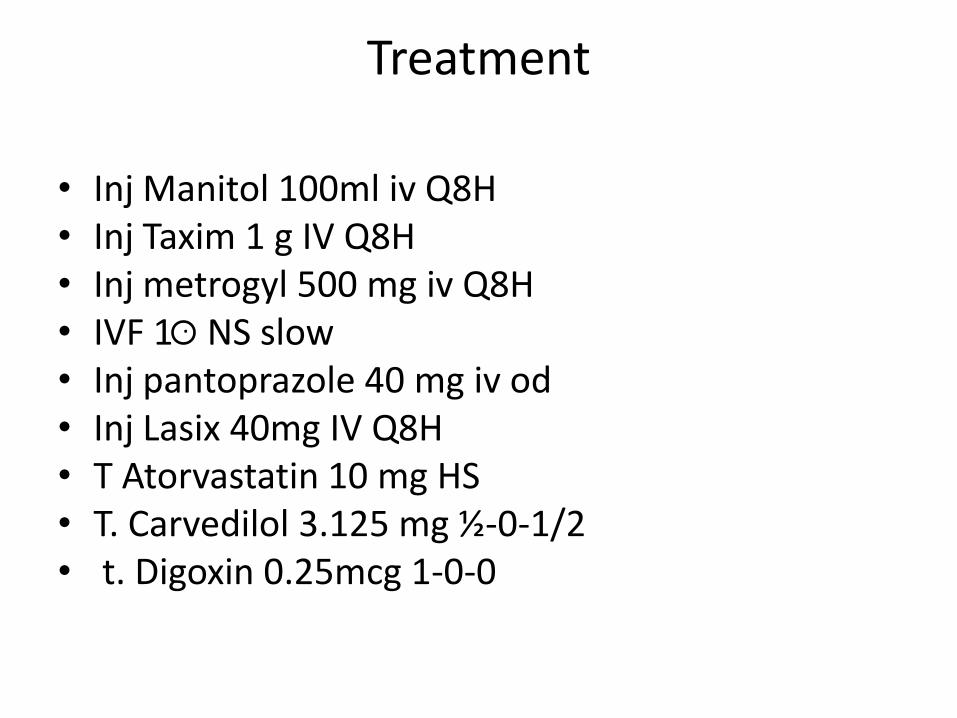
Treatment
• Inj Manitol 100ml iv Q8H• Inj Taxim 1 g IV Q8H• Inj metrogyl 500 mg iv Q8H• IVF 1 . NS slow• Inj pantoprazole 40 mg iv od• Inj Lasix 40mg IV Q8H• T Atorvastatin 10 mg HS• T. Carvedilol 3.125 mg ½-0-1/2• t. Digoxin 0.25mcg 1-0-0

















