22
Dizziness Presenter : (68) Zainab Aleid Group: (7) Tutor: Dr.Shereen Refaie
| Date post: | 07-May-2015 |
| Category: |
Education |
| Upload: | zainab-aleid |
| View: | 670 times |
| Download: | 0 times |

Dizziness
Presenter : (68) Zainab Aleid
Group: (7)
Tutor: Dr.Shereen Refaie

Objectives:
Dizziness and its types. Causes for each type of dizzinessDifferential diagnosis.DiagnosisExamination Investigations. Treatment.

The Case:
65 years old female presents with primary complaint of being dizzy. The patient present with chief complient of dizziness, she discribed it as sudden and severe spinning sensation precepitated by rollaing over in bed into her R side. The symptoms typically last less than 30 seconds. They have occured mightly in last months and occisionally during the day when she tilt her head up. She described no asossiaited worning sign, tinnitus or other nurological symptoms.
Definition of dizziness
Dizziness is a term used to describe everything from feeling faint or lightheaded to feeling weak or unsteady.
There are four types of dizziness: Vertigo, dysequilibrium, presyncope, and syncope. The most prevalent type is vertigo which accounts for 54% of reports of dizziness in primary care.

Vertigo: sensation of movement either of the patient or of the surroundings. Disequilibrium: sensation of imbalance.
Presyncope: Sense of impending fainting due to episodic diffuse temporary cerebral ischemia and associated with sweating, pallor, telescoping of peripheral vision.
Syncope: sudden transient loss of consciousness with concurrent loss of postural tone and most common causes are vasovagal episodes or orthostatic hypotension.
Causes of vertigo According to the duration of vertigo attack:
1.Less than one minute: BPPV ( benign paroxysmal positional vertigo) or vertebro-basilar insufficiency. 2.Less than one day and more than one minute: Meniere’s disease or migraine vertigo.3.Longer than one day without HL: vestibular neuritis or hysteric. 4.Longer than one day with HL: labyrinthitis.

Peripheral causes:• Canalithiasis (BPPV) - 30%• Vestibular neuritis (labyrinthitis) - 20%• Meniere’s disease - 10%• Drugs (aminoglycosides)
Central causes:• Vascular (vertebrobasilar insufficiency) - 50% of central causes.•Demyelinating (multiple sclerosis).•Drugs (anticonvulsants, alcohol, hypnotics).

Disequilibrium Multisensory disorder due to any combination of: • peripheral neuropathy • visual impairment • musculoskeletal disorder interfering with gait • vestibular disorder • cervical spondylosis
Presyncopepsychiatric disorders • major depression 25% • generalized anxiety or panic disorder 25% • somatization disorder • alcohol dependence • personality disorder • hyperventilation
Syncope • “nearly blacking out”, “nearly fainting” • lasts seconds to minutes • orthostatic hypotension • cardiac arrhythmias • vasovagal attacks

Analysis of the case:
Dizziness :No loss of consciousness = SyncopeNo sensation of fainting , No associated symptoms ( pallor , sweating ) , No psychiatric disorders = Presyncope.No neurological symptoms = Disequilibrium So
Vertigo

Differential diagnosis:
Vestibular neuritis ( more than one day )Migraine ( more than one minute + warning signs + headache )Meniere's disease ( more than one minute + hearing loss + tinnitus )Labyrinthitis. ( more than one day + hearing loss )Multiple sclerosis ( no neurological symptoms )Drugs ( no history )Symptoms occur only with positional changes, about 30 Sec
SO Benign paroxysmal positional vertigo(BPPV)

•General examination
•What are her vitals?• Anything out of ordinary to correlate with her other complaints? •Does the condition occur when she stand from sitting position?
Physical exam:
• Vestibular exam• Neurologic exam• Hearing tests

Vestibular exam
Head shaking test:
Fistula test
Finger test:
Romberg test:
Past-pointing test
Unterberger stepping test:

Ophthalmology examination to detect :
•Nystagmus
Neurologic exam
• Test her cranial nerves.

• Ear clinical examination
Otoscope Weber’s testRinne'test:

•Dix Hall pike test: positive in BPPV

Investigation:
•Audiological evaluation: Meniere disease.•Conventional radiograph aid in the diagnosis of cervical vertigo (i.e., vertigo triggered by somatosensory input from head and neck movements) .•MRI : useful in diagnosing vascular causes of vertigo such as: vertebrobasilar insufficiency, thrombosis of the labyrinthine artery, and neoplasms.•Laboratory tests such as electrolytes, glucose, blood counts,and thyroid function tests identify the etiology of vertigo.
Treatment:
• Exercise therapy rather than drug use is the main line of ttt in vestibular dizziness.
•Treat the underlying disease: migraine vertebrobasilar ischemia multiple sclerosis cerebellar tumors
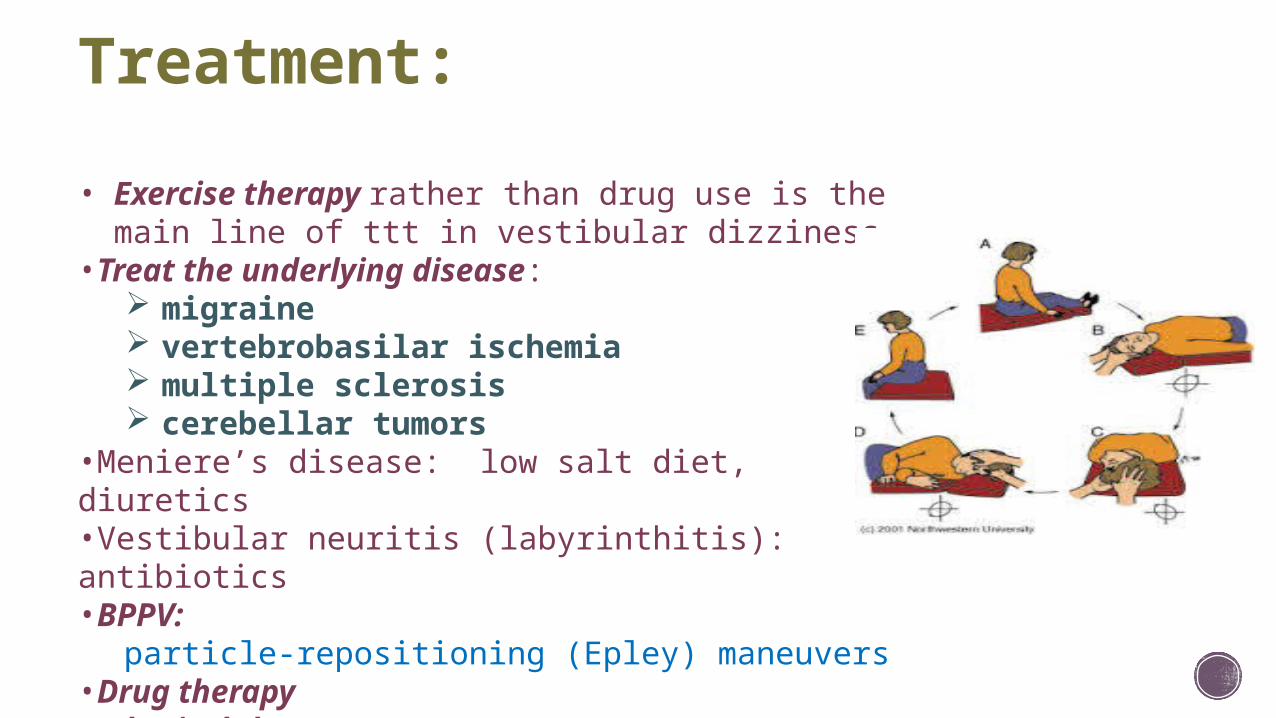
•Meniere’s disease: low salt diet, diuretics•Vestibular neuritis (labyrinthitis): antibiotics •BPPV:
particle-repositioning (Epley) maneuvers•Drug therapy• physical therapy

Summary

References:http://www.mayoclinic.com/health/dizziness/DS00435
http://dizzy.com/dizzines_and_equilibrium.htm
ENT, 3rd Edition, Behrbohm

Thank you

















