A patient with an acute coronary syndrome one year ago. Options for antiplatelet treatment Ronen Durst, MD Cardiology Department Hadassah, Hebrew University Medical Center. Chairman, Israeli society for treatment and prevention of atherosclerosis.
Transcript
A patient with an acute coronary syndrome one year ago. Options for antiplatelet treatment
Ronen Durst, MD Cardiology Department Hadassah, Hebrew University Medical Center.
Chairman, Israeli society for treatment and prevention of atherosclerosis.
Case presentation
• 67 year old man.
• PMH: – PUD at 40 treated with PPI and antibiotics
– DM HbA1c 7.5,
– HTN
– Smoking
• 12 months ago had MI. Primary PCI on the LAD with DES. NOA of the RCA and M2
• Treatment: – Atorvastain 80mg
– Aspirin 100mg
– Prasugrel 10mg
– Ramipril 10mg
– Januet (sitagliptin and metformin 50/1000)*2
Wants to stop some of the medication
Should we stop Prasugrel?
Sangkuhl Katrin, Shuldiner Alan R, Klein Teri E, Altman Russ B. "Platelet aggregation pathway" Pharmacogenetics and genomics (2010).
Platelet activation pathways
Coronary stents: historical development
Time Person(s) Landmark events
1964 Dotter and Judkins Conceptual description of coronary angioplasty using an implantable prosthetic device
May 1977 Gruntzig and Myler First coronary angioplasty during coronary artery bypass graft surgery
September 1977
Andreas Gruntzig First coronary angioplasty in an awake patient; a revolution in interventional cardiology
1979 Geoffrey Hartzler First balloon angioplasty to treat AMI
1986 Sigwart and Puel The first implantation of a stent in human coronary arteries; second revolution in interventional cardiology
1991 Cannon and Roubin First coronary stenting to treat AMI
1994 Serruys et al. and Fischman et al.
Publication of first two landmark (Benestent and STRESS) trials
1994 FDA FDA-approved use of stents to treat acute and threatened vessel closure after failed balloon angioplasty
1999 Eduardo Sousa The first drug (sirolimus) eluting stent implanted in human coronary artery; third revolution in interventional cardiology
2002–04 EME and FDA Approvals of Cypher and Taxus stents in Europe and USA
2011 EME Approval of Absorb BVS (bioresorbable vascular scaffold) in Europe; fourth revolution in interventional cardiology
British Medical Bulletin Volume 106, Pp. 193-211
Stent complications
• These initial stents had high metallic density: sub-acute stent thrombosis Intimal proliferation and restenosis
• Exposed metal struts acts as a nidus for platelet aggregation and thrombosis
• This potentially devastating complication is associated with a 50% incidence of AMI and a 20% mortality rate
Stent antiplatelets
• Initially, stent thrombosis was tackled by the use of complex anticoagulation regimens using aspirin, heparin and warfarin
• Combination led to high rates of major bleeding, vascular complications and prolonged hospital stays.
• The development of new anti-platelet agents led to a breakthrough with the adoption of a dual anti-platelet treatment (DAPT) combining aspirin with a thienopyridine – Aspirin and ticlopidine
– Aspirin and clopidogrel
Figure 3. Kaplan-Meler cumulative hazard rates for cardiovascular death or myocardial infarction from randomisation to end of
follow-upA=median time from randomisation to percutaneous coronary intervention. B=30 days after median time of PCI.
Shamir R Mehta, Salim Yusuf, Ron JG Peters, Michel E Bertrand, Basil S Lewis, Madhu K Natarajan, Klas Malmberg, Hans-
Jürgen Rupprecht, Feng Zhao, Susan Chrolavicius, Ingrid Copland, Keith AA Fox
Effects of pretreatment with clopidogrel and aspirin followed by long-term
therapy in patients undergoing percutaneous coronary intervention: the PCI-
CURE study
null, Volume 358, Issue 9281, 2001, 527–533
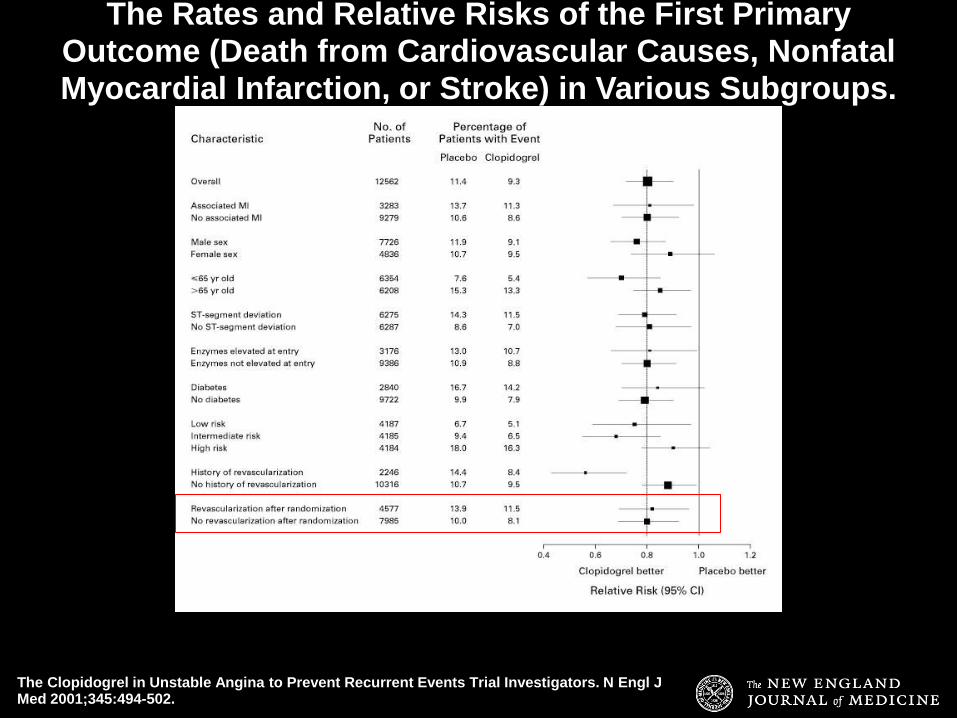
The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. N Engl J Med 2001;345:494-502.
Cumulative Hazard Rates for the First Primary Outcome (Death from Cardiovascular Causes, Nonfatal Myocardial Infarction, or Stroke) during the 12 Months of the Study.
The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. N Engl J Med 2001;345:494-502.
The Rates and Relative Risks of the First Primary Outcome (Death from Cardiovascular Causes, Nonfatal Myocardial Infarction, or Stroke) in Various Subgroups.
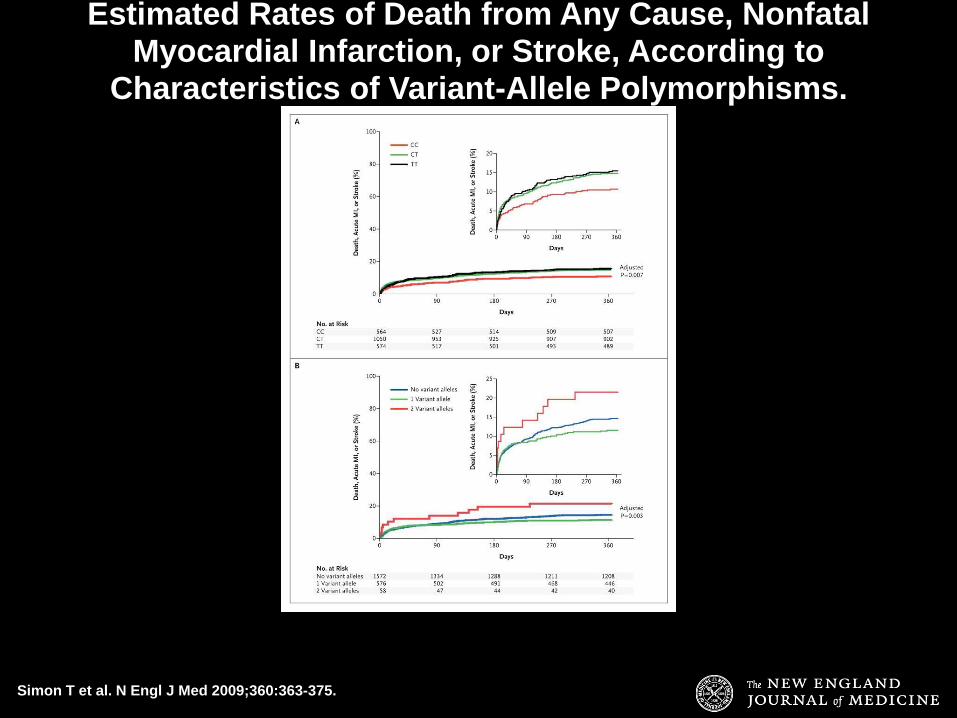
Clopidogrel Pathway
Sangkuhl Katrin, Klein Teri E, Altman Russ B. "Clopidogrel pathway" Pharmacogenetics and genomics (2010).
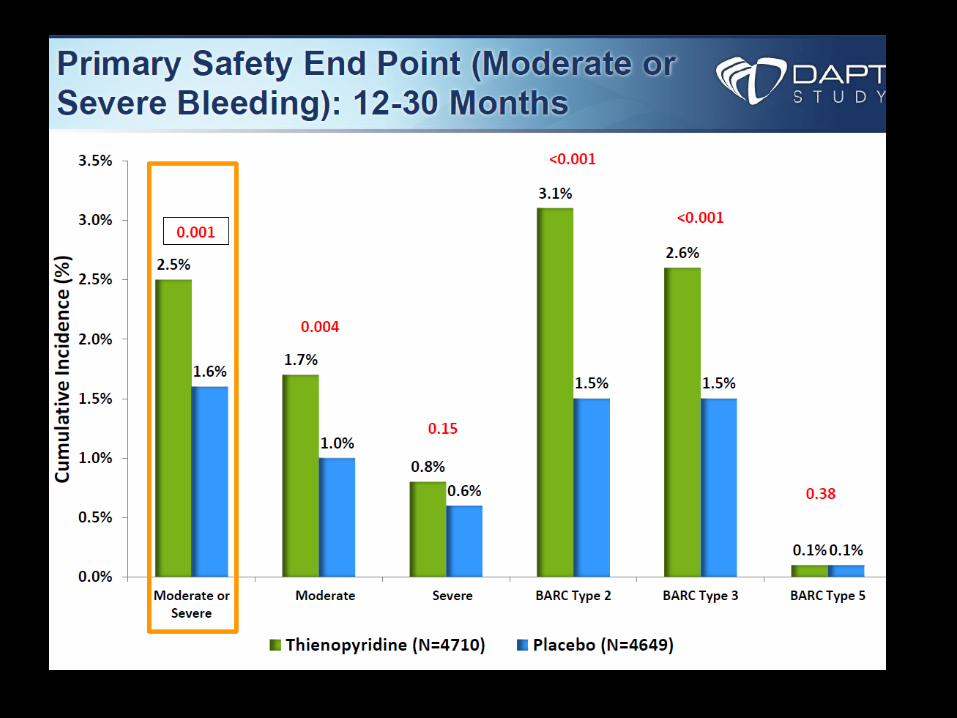
• A new risk score (the “DAPT score”), derived from the Dual Antiplatelet Therapy study
• Analysis of study data suggest that in patients treated for 1 year with DAPT without significant bleeding or ischemic events, the benefit/risk ratio with prolonged DAPT may be favorable for those with a high DAPT score (≥2)