Case Report #0431 Submitted by: Jin T. Kim, M.D. Faculty reviewer: Clark W. Sitton, M.D. Date accepted: 25 November 2007 Radiological Category: Principal Modality (1): Principal Modality (2): Neuroradiology Nuclear Scintigraphy CT
Transcript
Case Report #0431
Submitted by: Jin T. Kim, M.D.
Faculty reviewer: Clark W. Sitton, M.D.
Date accepted: 25 November 2007
Radiological Category: Principal Modality (1):
Principal Modality (2):
Neuroradiology
Nuclear Scintigraphy
CT
Case History
6 year-old girl with dysphagia.
Radiological Presentations
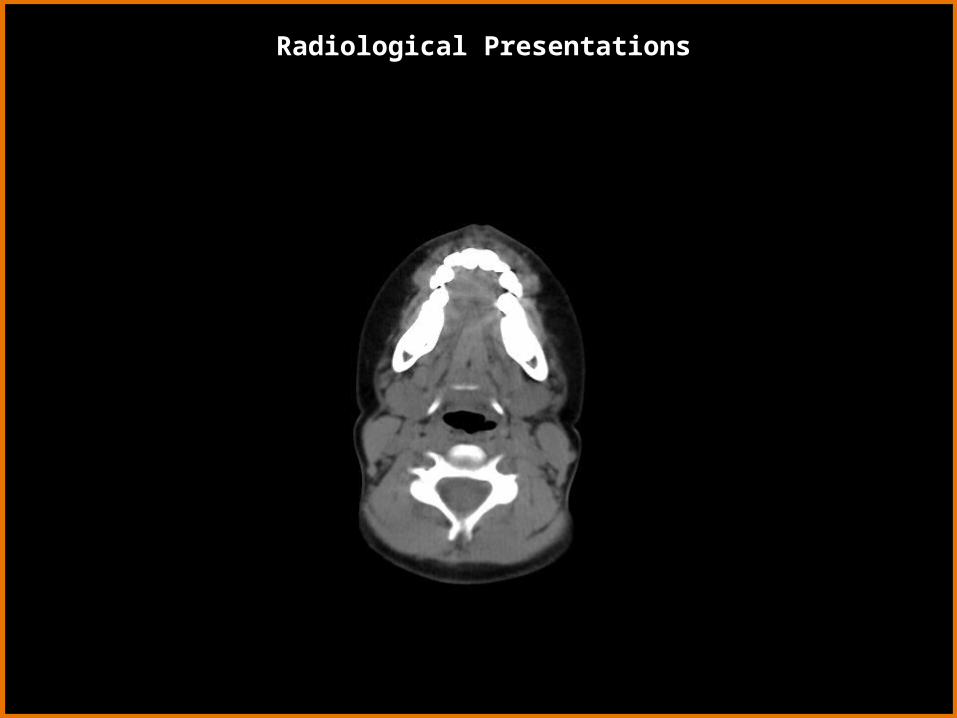
Non-contrast CT – Axial View
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Non-contrast CT – Coronal View
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Non-contrast CT – Sagittal View
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Radiological Presentations
Anterior View Lateral View
Radiological Presentations
• Hemangioma
• Enlarged Lingual Tonsils
• Lymphoma
• Thyroglossal Duct Cyst
• (Ectopic) Lingual Thyroid
• Squamous Cell Carcinoma
• Dermoid Cyst
Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page.
Test Your Diagnosis
Noncontrast enhanced CT demonstrates a hyperdense mass at the base of the tongue centered in the midline 1.5 cm TV x 1.4 cm AP x 1.5 cm CC. The mass impinges on the oral airway at the back of the tongue.
Tc-99m pertechnate scan demonstrates focal area of intense radiotracer activity in the midline of the oropharyngeal region. A small curvilinear activity consistent with saliva activity was noted anterosuperiorly on the lateral and obliques images. Otherwise, no focal radiotracer activity in the neck or upper thorax.
• Hemangioma
• Enlarged lingual tonsils
• Thyroglossal duct cyst
• Lingual thyroid
Findings:
Differentials:
Findings and Differentials
The thyroglossal duct cyst is the most common of the congenital cysts in the neck. The thyroglossal duct is the epithelial tract along which the thyroid gland descends to its final position from the foramen cecum at the base of the tongue (at the 3rd week of gestational age), to the lower neck. The duct usually involutes by the 8-10th week of fetal life. In 5% of cases, thyroid cells may remain in the thyroglossal duct and give rise to thyroglossal duct cysts. It presents as an enlarging painless neck mass. 50% are less than 10 years of age at presentation, with a second peak at 20-30 years.
The lesion is located in the midline or paramedian (usually on the left) between the thyroid gland and the hyoid bone. While thyroglossal duct cysts are more common than lingual thyroid glands, thyroglossal duct cysts are usually infrahyoidal. Thyroglossal duct cysts may also occur in the tongue base or floor of mouth.
A thyroglossal duct cyst will characteristically move with swallowing. The thyroglossal duct cyst usually does not appear as a simple cyst and sonographically appears as a cystic lesion with low-level intraluminal reflectors, presumably due to bleeding or infection.
Discussion – Thyroglossal Duct Cyst
The thyroid gland originates at the tip of the foramen cecum of the developing tongue and migrates inferiorly, beginning in the first month of gestation. The thyroid reaches the final location in the 7th week.
Only the lingual thyroid tissue shows marked hyperdensity on the noncontrast enhanced CT scan due to its natural iodine content. The nuclear medicine study will demonstrate whether or not there is the presence of additional thyroid tissue. The nuclear medicine scan should clinch the diagnosis with the absence of thyroid tissue in the usual expected location.
The lesion usually manifests during young adulthood and adolescence because of thyroid enlargement, leading to dysphagia or airway obstruction. In 80% of cases the lingual thyroid tissue is the only functioning thyroid tissue in the body. Because thyroid hormone is vital for healthy growth as a child, the surgeon will often leave the lingual thyroid tissue in through adolescence, unless there is secondary airway obstruction. The presence of the ectopic thyroid does place the patient at risk (5% chance) of papillary cell carcinoma of the thyroid gland at the base of the tongue.
Discussion – Lingual Thyroid
Radiological Presentations – Embryology of Thyroid Gland
From Larsen WJ. Human Embryology. 2nd Ed. New York: Churchill Livingstone, 1997.
The hemangioma will enhance intensely and appear similar in appearance to that of an ectopic thyroid on a noncontrast CT. An ectopic thyroid gland may be mistaken for a hemangioma if an enhanced CT is performed prior to a noncontrast CT. Phleboliths may be present.
Discussion – Hemangioma
The lingual tonsillar tissue may be also seen at the base of the tongue at the midline position. The lingual tonsillar tissue, however, will not be hyperattenuating on the noncontrast CT and the thyroid gland will be in the expected location on the nuclear medicine study. Hypertrophied tonsillar tissue may simulate an exophytic lymphoma and will appear slightly hyperintense on T1-weighted MRI and very hyperintense on T2-weighted MRI.
Discussion – Enlarged Lingual Tonsils
Lingual thyroid
Diagnosis
Chung EM. Diseases Affecting the Pediatric Airway. In Levy AD, Chung EM, eds. Radiologic Pathology. Washington, D.C.: American Registry of Pathology, 2006:1369-1370.
Grossman RI and Yousem DM. Neuroradiology: the Requisites. 2nd Ed. Philadelphia: Mosby, 2003:651-653, 661, 738-739.
Larsen WJ. Human Embryology. 2nd Ed. New York: Churchill Livingstone, 1997: 372.
Yousem DM and Da Motta ACBS, Head and Neck Imaging: Case Review Series.2nd Ed. Philadelphia: Mosby, 2006: 215-216.


























































![Case Report # [] Submitted by:Ladi Oki, MSIV Faculty reviewer:Dr. Sandra Oldham, MD Date accepted:28 September 2011 Radiological Category:Principal Modality.](https://static.documents.pub/doc/80x56/56649cf95503460f949cb136/case-report-submitted-byladi-oki-msiv-faculty-reviewerdr-sandra-oldham.jpg)





