Acta Scientiae Veterinariae, 2012. 40(2): 1045. CASE REPORT Pub. 1045 ISSN 1679-9216 (Online) 1 Received: December 2011 www.ufrgs.br/actavet Accepted: February 2012 Graduanda, Faculdade de Veterinária (FaVet), Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil. 2Departamento Medicina Animal, FaVet-UFRGS. 3Setor de Patologia Veterinária (SPV), Departamento de Patologia Clínica Veterinária, FaVet-UFRGS. CORRESPONDENCE: L. ZANG [[email protected] - Tel.: + 55 (51) 3308-6971]. Faculdade de Veterinária - UFRGS, Av. Bento Gonçalves n. 9090, Bairro Agrono- mia. CEP 91540-000 Porto Alegre, RS, Brazil. Narcolepsia sintomática em um cão com macroadenoma hipofisário Symptomatic Narcolepsy in a Dog with Hypophisary Macroadenoma Luciana Zang 1 , Ana Cristina Pacheco de Araújo 2 , Daniele Mariath Bassuino 1 , Ana Paula Merlo dos Santos 1 , Angélica Terezinha Barth Wouters 3 & David Driemeier 3 ABSTRACT Background: Narcolepsy is a neurologic sleep disorder, in humans characterized by excessive and recurrent daytime sleepiness, rapid eye movement in the beginning of the sleep, in association with hypnagogic hallucinations and sleep paralysis, with or without cataplexy. In dogs, the characteristic symptom is cataplexy and narcolepsy exists in two forms, one genetic and one acquired. This article describes one case of narcolepsy as a symptom due to an adenohypophysis tumor. Case: Dog presenting progressive signs of appetite loss, incoordination and constant falling. At clinical evaluation, the dog presented cachexia, hipocolored mucosae and compulsively walking in circles to the right, the four limbs collapsed from physical exhaustion, remaining in a narcoleptic state. Complementary exams, like x-ray, ultrasonography, hemogram and biochemical examination did not show significant alterations. The patient was hospitalized for recovery of general status and corticoid treatment was initiated, but after two days it died. Necropsy reported that the cause of death was 180º gastric torsion and adrenals presented diffuse and marked enlargement of the cortical layer, 1.5 cm diameter neoplasia at the base of the brain and 0.5 cm diameter cavitation in the cerebral parenchyma. In the microscopic examination, adrenals were hyperplastic at the cortical region and there was round cell proliferation, with some basophilic cytoplasm and others more eosinophilic at the hypophysis with parenchyma nervous tissue invasion, reaching the diagnosis of macroadenoma of adenohypophysis chromophil cells. Discussion: secondary or symptomatic narcolepsy is not commonly described in animals, with just one case report being found in the literature, in which the patient presented narcolepsy-cataplexy secondary to post-vaccination encephalitis. In humans, it has been reported in cases of hypothalamic pathologies, like Niemann-Pick type C disease, neoplasia, trauma, vascular issues, post-encephalitis, agenesis of the corpus callosum, sarcoidosis, neurocysticercosis and limbic encephalitis. In the described case, probably, there was an infiltration from the hypophysis macroadenoma to the adjacent tissues, causing destruction and compression of hypothalamic neurons. The hypophisary macroadenomas, with nervous symptoms, occur due to tumor dorsal extention, dorso-caudal direction, comprising and invading the hypothalamus and the third ventricle. The most common signs are apathy, ataxy, behavioral changes, sight reduction and facial paralysis, being some of these symptoms observed in the present case. According to several reports in humans, the hypocretin levels (neurotransmitter which presents the function of sleep regulation, alertness and food intake) is used to diagnose narcolepsy, however, in case of secondary narcolepsy, the neurotransmitter can or not be decreased. Cases in which it had normal amount, the authors based on clinical signs concluded that the hypocretinergic system (hypocretin-1 and 2, and its respective receptors) would be compromised. The patient died before the hypocretin dosage was performed to confirm secondary narcolepsy. For that, it would be necessary to collect cephalorachidian fluid, under sedation, but the dog was not in adequate physical condition to go under such procedure. Because of that, it was concluded that, by symptomatology, its hypocretinergic system was affected, because the location of the tumor lesion is similar to other cases reported in humans. Keywords: narcolepsy, cataplexy, hypocretin, hypophisary tumor. Descritores: narcolepsia, cataplexia, hipocretina, tumor hipofisário.
Transcript
Acta Scientiae Veterinariae, 2012. 40(2): 1045.
CASE REPORTPub. 1045
ISSN 1679-9216 (Online)
1
Received: December 2011 www.ufrgs.br/actavet Accepted: February 2012
Graduanda, Faculdade de Veterinária (FaVet), Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil. 2Departamento Medicina Animal, FaVet-UFRGS. 3Setor de Patologia Veterinária (SPV), Departamento de Patologia Clínica Veterinária, FaVet-UFRGS. CORRESPONDENCE: L. ZANG [[email protected] - Tel.: + 55 (51) 3308-6971]. Faculdade de Veterinária - UFRGS, Av. Bento Gonçalves n. 9090, Bairro Agrono-mia. CEP 91540-000 Porto Alegre, RS, Brazil.
Narcolepsia sintomática em um cão com macroadenoma hipofi sário
Symptomatic Narcolepsy in a Dog with Hypophisary Macroadenoma
Luciana Zang1, Ana Cristina Pacheco de Araújo2, Daniele Mariath Bassuino1, Ana Paula Merlo dos Santos1,
Angélica Terezinha Barth Wouters3 & David Driemeier3
ABSTRACT
Background: Narcolepsy is a neurologic sleep disorder, in humans characterized by excessive and recurrent daytime sleepiness, rapid eye movement in the beginning of the sleep, in association with hypnagogic hallucinations and sleep paralysis, with or without cataplexy. In dogs, the characteristic symptom is cataplexy and narcolepsy exists in two forms, one genetic and one acquired. This article describes one case of narcolepsy as a symptom due to an adenohypophysis tumor.Case: Dog presenting progressive signs of appetite loss, incoordination and constant falling. At clinical evaluation, the dog presented cachexia, hipocolored mucosae and compulsively walking in circles to the right, the four limbs collapsed from physical exhaustion, remaining in a narcoleptic state. Complementary exams, like x-ray, ultrasonography, hemogram and biochemical examination did not show signifi cant alterations. The patient was hospitalized for recovery of general status and corticoid treatment was initiated, but after two days it died. Necropsy reported that the cause of death was 180º gastric torsion and adrenals presented diffuse and marked enlargement of the cortical layer, 1.5 cm diameter neoplasia at the base of the brain and 0.5 cm diameter cavitation in the cerebral parenchyma. In the microscopic examination, adrenals were hyperplastic at the cortical region and there was round cell proliferation, with some basophilic cytoplasm and others more eosinophilic at the hypophysis with parenchyma nervous tissue invasion, reaching the diagnosis of macroadenoma of adenohypophysis chromophil cells.Discussion: secondary or symptomatic narcolepsy is not commonly described in animals, with just one case report being found in the literature, in which the patient presented narcolepsy-cataplexy secondary to post-vaccination encephalitis. In humans, it has been reported in cases of hypothalamic pathologies, like Niemann-Pick type C disease, neoplasia, trauma, vascular issues, post-encephalitis, agenesis of the corpus callosum, sarcoidosis, neurocysticercosis and limbic encephalitis. In the described case, probably, there was an infi ltration from the hypophysis macroadenoma to the adjacent tissues, causing destruction and compression of hypothalamic neurons. The hypophisary macroadenomas, with nervous symptoms, occur due to tumor dorsal extention, dorso-caudal direction, comprising and invading the hypothalamus and the third ventricle. The most common signs are apathy, ataxy, behavioral changes, sight reduction and facial paralysis, being some of these symptoms observed in the present case. According to several reports in humans, the hypocretin levels (neurotransmitter which presents the function of sleep regulation, alertness and food intake) is used to diagnose narcolepsy, however, in case of secondary narcolepsy, the neurotransmitter can or not be decreased. Cases in which it had normal amount, the authors based on clinical signs concluded that the hypocretinergic system (hypocretin-1 and 2, and its respective receptors) would be compromised. The patient died before the hypocretin dosage was performed to confi rm secondary narcolepsy. For that, it would be necessary to collect cephalorachidian fl uid, under sedation, but the dog was not in adequate physical condition to go under such procedure. Because of that, it was concluded that, by symptomatology, its hypocretinergic system was affected, because the location of the tumor lesion is similar to other cases reported in humans.
L. Zang, A.C.P. Araújo, D.M. Bassuino, et al. 2012. Narcolepsia sintomática em um cão com macroadenoma
hipofi sário. Acta Scientiae Veterinariae. 40(2): 1045.
INTRODUÇÃO
A narcolepsia é um distúrbio cerebral que em humanos é caracterizada por excessiva e recorrente sonolência diurna, movimento rápido dos olhos no inicio do sono, associado a alucinações hipnagógi-cas e paralisia do sono, acompanhada ou não por cataplexia (atonia muscular fl ácida desencadeada por excitação emocional) [6,10]. A narcolepsia canina se assemelha comportalmente, eletrofi siologicamente e farmacologicamente, entretanto a cataplexia é o sinal dominante enquanto que a paralisia do sono e as alu-cinações são difíceis de serem avaliadas devido a sua natureza subjetiva [1,16]. A narcolepsia em cães já foi relatada em 17 raças [24] e se caracteriza por dois tipos de apresentação, uma forma hereditária (dobermans, labrador retrievers e daschunds), se desenvolvendo até 6 meses de idade. Este distúrbio ocorre devido a um gene autossômico recessivo, responsável por mutações na hipocretina-receptor-2 [11,13]. A outra forma se caracteriza por afetar animais com idade avançada e está associada à perda da ligação da hipocretina. Essa é a forma mais comum e mais semelhante à humana [14,20].
Os tumores intracranianos são causa comum para disfunções neurológicas em cães de meia idade e idosos, apresentando incidência variável, alguns estudos citam até 3% [22]. As neoplasias podem ser primárias ou secundárias [8] e os sinais neurológicos podem ser variados dependendo do tamanho e estru-turas envolvidas [18]. As neoplasias de hipófi se são relativamente comuns, 80 a 85% dos animais com hiperadrenocorticismo padecem dessa mal, porém nem todos apresentam sintomas neurológicos. A manifesta-ção neurológica é dependente do tamanho e infi ltração tumoral [8,9].
RELATO DO CASO
Foi atendido no Hospital de Clínicas Veteriná-rias (HCV) da Universidade Federal do Rio Grande do Sul (UFRGS) um canino, boxer, de 8 anos de idade, com histórico de diminuição progressiva do apetite, incoordenação e quedas constantes. O proprietário relatou convulsões esporádicas e que o animal parecia “dormir em pé”, fato este, que já estaria acontecen-do a cerca de um ano e de maneira progressiva. Ao exame clínico as alterações constatadas foram: caque-xia, desidratação moderada, mucosas hipocoradas, linfonodos submandibulares aumentados, alopecia
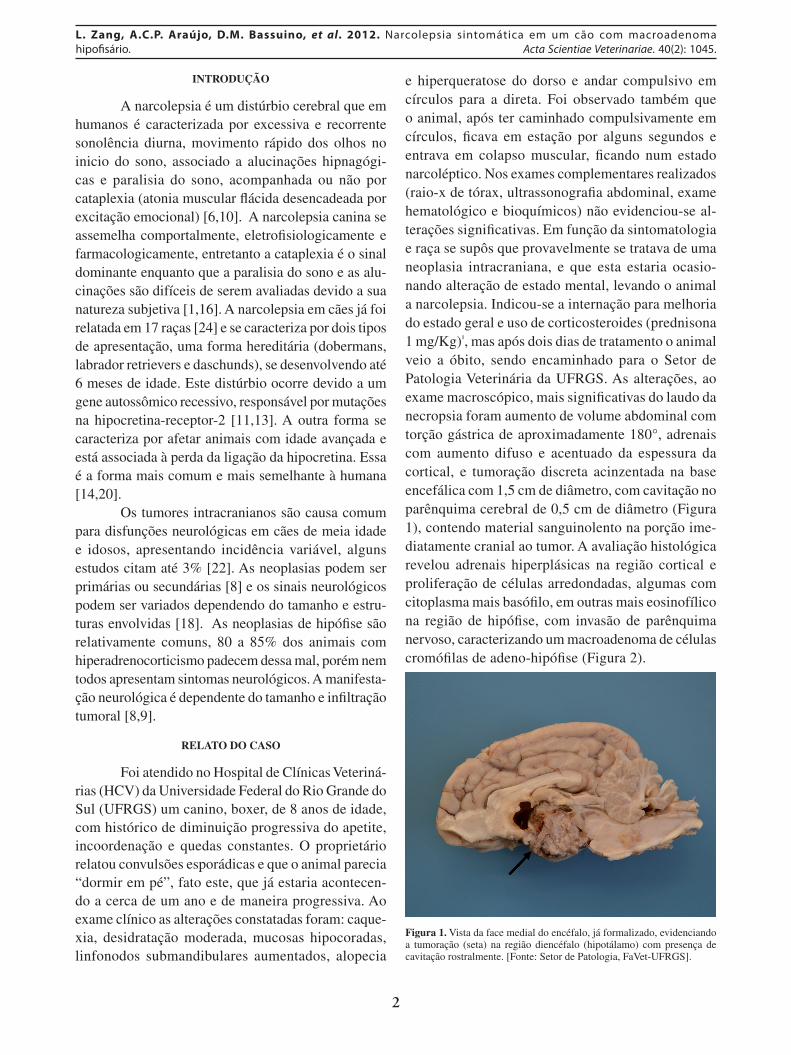
e hiperqueratose do dorso e andar compulsivo em círculos para a direta. Foi observado também que o animal, após ter caminhado compulsivamente em círculos, fi cava em estação por alguns segundos e entrava em colapso muscular, fi cando num estado narcoléptico. Nos exames complementares realizados (raio-x de tórax, ultrassonografi a abdominal, exame hematológico e bioquímicos) não evidenciou-se al-terações signifi cativas. Em função da sintomatologia e raça se supôs que provavelmente se tratava de uma neoplasia intracraniana, e que esta estaria ocasio-nando alteração de estado mental, levando o animal a narcolepsia. Indicou-se a internação para melhoria do estado geral e uso de corticosteroides (prednisona 1 mg/Kg)¹, mas após dois dias de tratamento o animal veio a óbito, sendo encaminhado para o Setor de Patologia Veterinária da UFRGS. As alterações, ao exame macroscópico, mais signifi cativas do laudo da necropsia foram aumento de volume abdominal com torção gástrica de aproximadamente 180°, adrenais com aumento difuso e acentuado da espessura da cortical, e tumoração discreta acinzentada na base encefálica com 1,5 cm de diâmetro, com cavitação no parênquima cerebral de 0,5 cm de diâmetro (Figura 1), contendo material sanguinolento na porção ime-diatamente cranial ao tumor. A avaliação histológica revelou adrenais hiperplásicas na região cortical e proliferação de células arredondadas, algumas com citoplasma mais basófi lo, em outras mais eosinofílico na região de hipófi se, com invasão de parênquima nervoso, caracterizando um macroadenoma de células cromófi las de adeno-hipófi se (Figura 2).
Figura 1. Vista da face medial do encéfalo, já formalizado, evidenciando a tumoração (seta) na região diencéfalo (hipotálamo) com presença de cavitação rostralmente. [Fonte: Setor de Patologia, FaVet-UFRGS].
3
L. Zang, A.C.P. Araújo, D.M. Bassuino, et al. 2012. Narcolepsia sintomática em um cão com macroadenoma
hipofi sário. Acta Scientiae Veterinariae. 40(2): 1045.
Figura 2. Macroadenoma corticotrófi co de adeno-hipófi se, evidenciando a proliferação de células arredondadas com citoplasma fracamente corado ( ) com invasão do parênquima nervoso () (Coloração H & E x 10). [Fonte: Setor de Patologia, FaVet-UFRGS].
DISCUSSÃO
A narcolepsia sintomática ou secundaria é rara e vem sendo mais relatada em humanos que animais. É observada em casos de patologias hipotalâmicas, como doença de Niemann-Pick tipo C, neoplasia, trauma, problemas vasculares, pós-encefalite, age-nesia de corpo caloso, sarcoidose, neurocisticercose e encefalites límbicas [7,15], enquanto que em cães foi apenas encontrado, pelo autor deste artigo, um caso descrito de narcolepsia-cataplexia secundaria a encefalite pós-vacinal [5].
A região do hipotálamo apresenta os neurônios produtores de hipocretina (Hcrt) e estes se projetam para todo o cérebro [2,12]. A Hcrt é um neurotransmis-sor excitatório com papel fundamental na regulação do sono, vigília e apetite [21,23], e pode ser usada como marcador para o diagnóstico da narcolepsia idiopática (dosado a partir do líquido cefalorraquidiano, colhido com o animal sedado) [3,4]. Entretanto em alguns re-
latos de narcolepsia sintomática, a Hcrt pode não estar diminuída [17], porém os sinais clínicos demonstraram destruição do sistema hipocretinérgico (Hcrt-1 e 2 e seus respectivos receptores) [15]. No caso descrito o animal veio a óbito antes da possibilidade de dosagem da Hcrt, visto que o animal não estava em condições para ser sedado para proceder à coleta, no entanto, baseado na sintomatologia apresentada, deduziu-se que havia comprometimento do sistema hipocretinérgico.
Os macroadenomas hipofi sários, que apresen-tam sintomatologia nervosa, ocorrem pela extensão dorsal do tumor, sentido dorso-caudal, comprimindo e invadindo o hipotálamo e terceiro ventrículo, obtendo como sinais mais comuns apatia, ataxia, alteração de comportamento, redução de visão e paralisia facial [19], sendo alguns destes observados no presente relato.
O caso citado apresenta os sinais clínicos compatíveis com alterações do sistema hipocretinér-gico, visto que a narcolepsia e a cataplexia ocorreram tardiamente, descartando a hipótese de ser hereditária. Além disso, a área de destruição do tumor é compatí-vel com os casos humanos de narcolepsia-cataplexia secundária, sugerindo que a neoplasia adenohipofi sária foi responsável pela narcolepsia sintomática. A torção gástrica secundária a compressão da região responsá-vel pelo apetite e quantidade de ingestão de alimentos pelo paciente, é sugestivo da causa mortis imediata do animal.
Declaration of interest. The authors report no confl icts of interest. The authors alone are Responsible for the content and writing of the paper.
REFERÊNCIAS
1 Baker T.L. & Dement W.C. 1985. Canine narcolepsy-cataplexy syndrome: evidence for an inherited monoaminergic-chohnergic imbalance. In: McGintv D.J., Drucker-Colin R., Morrison A. & Parmeggiani P.L. (Eds). Brain mechanisms of sleet. New York: Raven, pp.199-233.
2 Beuckmann C.T. & Yanagisawa M. 2002. Orexins: from neuropeptides to energy homeostasis and sleep/wake regula-tion. Journal of Molecular Medicine. 80(6): 329-342.
3 Billiard M. 2007. Diagnosis of narcolepsy and idiopathic hypersomnia. An update based on the International Classifi ca-tion of Sleep Disorders. Sleep Medicine Reviews. 11(5): 377-388.
4 Bougin P., Zeitzer J.M. & Mignot E. 2008. CSF hypocretin-1 assessment in sleep and neurological disorders. Lancet Neurology. 7(7): 649-662.
4
L. Zang, A.C.P. Araújo, D.M. Bassuino, et al. 2012. Narcolepsia sintomática em um cão com macroadenoma
hipofi sário. Acta Scientiae Veterinariae. 40(2): 1045.
www.ufrgs.br/actavetPub. 1045
5 Cantile C., Baroni M. & Arispici M. 1999. A Case of Narcolepsy-Cataplexy associated with Distemper Encephalitis. The Journal of Veterinary Medicine. 46(5): 301-308.
6 Daniels L.E. 1934. Narcolepsy. Medicine. 13(1): 1-22.7 D’Cruz O., Vaughn B. & Gold S. 1994. Symptomatic cataplexy in pontomedullary lesions. Neurology. 44(11): 2189-2191.8 Ettinger S.J. & Feldman E.C. 2007. Enfermidades cerebrales. In: Tratado de Medicina Interna Veterinaria - Enfermi-
dades del perro y el gato. 6.ed. Madrid: Elsevier, pp.803-835. 9 Fitzmaurice S.N. 2011. Colapso. In: Neurologia em Pequenos Animais. Rio de Janeiro: Elsevier, pp.232-237.10 Guilleminault C., Wilson R.A. & Dement W.C. 1974. A study on cataplexy. Archives of Neurology. 3(1): 255-261.11 Hungs M., Fan J., Lin L., Lin X., Maki R.A. & Mignot E. 2001. Identifi cation and functional analysis of mutations
in the hypocretin (orexin) genes of narcoleptic canines. Genome Research. 11: 531-539.12 Hungs M. & Mignot E. 2001. Hypocretin/orexin, sleep and narcolepsy. Bioessay. 23(5): 397-408.13 Lin L., Faraco J., Li R., Kadotani H., Rogers W., Lin X., Qiu X., de Jong P.J., Nichino S. & Mignot E. 1999. The
sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell. 98: 365-376.14 Mignot E., Lin L., Rogers W., Honda Y., Qiu X., Lin X., Okun M., Hohjoh H., Miki T., Hsu S.H., Leffell M.S.,
Grumet F.C., Fernandez-Vina M., Honda M. & Risch N. 2001. Complex HLA-DR and -DQ interactions confer risk of narcolepsy-cataplexy in three ethnic groups. The American Journal of Human Genetics. 68: 686-699.
15 Nishino S. & Kanbayashi T. 2005. Symptomatic narcolepsy, cataplexy and hypersomnia, and their implications in the hypothalamic hypocretin/orexin system. Sleep Medicine Reviews. 9(4): 269-310.
16 Nishino S., Reid M.S., Dement W.C. & Mignot E. 1994. Neuropharmacology and neurochemistry of canine narcolepsy. Sleep Medicine Reviews. 17(8): 84-93.
17 Nishino S., Ripley B., Overeem S., Lammers G.J. & Mignot E. 2000. Hypocretin (orexin) defi ciency in human narcolepsy. Lancet Neurology. 355(9197): 39-40.
18 Pellegrino F., Suraniti A. & Garibaldi L. 2003. El libro de neurología para la práctica clínica. Buenos Aires: Intermédica, p.708.
19 Plummer C.E., Specht A. & Gelatt K.N. 2007. Ocular manifestations of Endocrine Disease Compendium. Continuing Education for Veterinarians. 29(12): 733-743.
20 Ripley B., Fujiki N., Okura M., Mignot E. & Nishino S. 2001. Hypocretin levels in sporadic and familial cases of canine narcolepsy. Neurobiology of Disease. 8(3): 525-534.
21 Sakurai T., Amemiya A., Ishii M., Matsuzaki I., Chemelli R.M., Tanaka H., Williams S.C., Richardson J.A., Ko-zlowski G.P., Wilson S., Arch J.R., Buckingham R.E., Haynes A.C., Carr S.A., Annan R.S., McNulty D.E., Liu W.S., Terrett J.A., Elshourbagy N.A., Bergsma D.J. & Yanagisawa M. 1998. Orexins and orexin receptors: a family of hypothalamic neuropeptides and G protein-coupled receptors that regulate feeding behavior. Cell. 92(5): 573-585.
22 Snyder J.M., Shofer F.S., Van Winkle T.J. & Massicotte C. 2006. Canine intracranial primary neoplasia: 173 cases (1986-2003). Journal of Veterinary Internal Medicine. 20(3): 669-675.
23 Sutcliffe J.G. & De Lecea L. 2000. The hypocretins: excitatory neuromodulatory peptides for multiple homeostatic systems, including sleep and feeding. Journal of Neuroscience Research. 62(2): 161-168.
24 Tonokura M., Fujita K., Morozumi M., Yoshida Y.,Kambayashi T. & Nishino S. 2003. Narcolepsy in a hypocretin/orexin-defi cient chihuahua. Veterinary Record. 152(25): 776-779.