159
Section B Presents
| Date post: | 18-Nov-2014 |
| Category: |
Documents |
| Upload: | quolette-constante |
| View: | 103 times |
| Download: | 2 times |

Section B Presents
Case Study of a Client Diagnosed with Hypertensive Atherosclerotic Cardiovascular
Disease (HASCVD)GRAND CASE PRESENTATIONBS NURSING III SECTION BSECOND SEMESTER AY 2009-2010 MARCH 11, 2010: THURSDAY Submitted to:Ms. MARILOU GENODIA, R.N.Ms. GLENDA NAGALLO, R.N.ADVISERS
INTRODUCTION
Hypertensive Atherosclerotic Cardiovascular Disease (HASCVD) is an arterial disease characterized by narrowing of the arteries by atherosclerosis (plaque formation) that obstruct (stenosis) or narrow (sclerosis) necessary blood flow to a specific part of the heart accompanied with increased blood pressure.
HASCVD is a medical way of saying "blocked arteries secondary to cholesterol plaques and in the setting of hypertension." It describes a common clinical syndrome, where the walls of coronary (heart) arteries are lined with cholesterol plaques.

It’s the progressive hardening of the arteries due to long standing hypertension. In this case cardiovascular arteries are hardened, compromising blood flow to the heart muscle and tissue. Complications include Angina Pectoris, MI (Heart Attack) and Heart failure.

CASE ABSTRACT

Patient C.G., female, aged 55, consulted the Medical Center Muntinlupa (MCM) Emergency Room (ER) last November 25, 2009 with chief complaint of numbness on her left arm coincided with chest pain which she described as radiating from her sternum area towards her xyphoid process.

She roughly estimated it lasting about 10-15 minutes. A week prior to admission, she reported experiencing generalized body weakness and occasional radiating chest pain related to stress and fatigue. She was accompanied by her husband.

She stated that approximately 10 years ago (year 2000) she was first diagnosed of hypertension. When asked about medications she is currently taking, she stated that she takes ‘Neobloc’, an anti hypertensive drug belonging to the classification of Calcium channel blockers.

With this, she also claimed no familial history of hypertension or any related cardiovascular disease but she stated a link in the genealogy that manifested diabetes on her paternal side.

When asked about her lifestyle, she openly shared that when she was at her peak age (she approximated it between teens to her late twenties) she lived carefree and was engaging in vices like smoking, drinking and eating foods high in fat and sodium.

By the time morning came, she was so exhausted that she’d doze off through the day and listen to music. Realization of her ‘sedentary lifestyle’ only dawned upon her when she started her family.
Upon initial assessment, patient was 57 inches tall and weighed 106.7 lbs. She is not in distress and is conscious and coherent. Initial vital signs T=36˚C, PR= 120bpm, RR=20 and BP=150/90 clearly shows presence of hypertension. In relation to this, she was confined to rest and given a dose of Nitroglycerin.

She was also ordered to undergo several diagnostic tests such as: 1. Blood Studies, 2. BUN, Creatinine, 3. Troponin T, 4. Urinalysis, 5. CT Scan, 6. FBS and Cholesterol level.
Upon analysis of the data stated, patient was diagnosed with Hypertensive Atherosclerostic Cardiovascular Disease (HASCVD).

OBJECTIVES

A. General ObjectivesThis study aims to convey
familiarity and provide effective nursing care to a patient diagnosed with Hypertensive Atherosclerotic Cardiovascular Disease (HASCVD) through understanding the patient history, disease process and management.

B. Specific ObjectivesAt the end of the session, the students
will be able to:
1. Present a thorough assessment regarding HASCVD, through Nursing Health History, Gordon’s Functional Health Pattern, Physical Assessment, and the interpretation of the laboratory examinations done on the patient.

2. Discuss the anatomy and physiology of the heart, pathophysiology of the patient’s condition, usual clinical manifestations and possible complications of the condition.
3. Enumerate the necessary medications needed and be familiar to its mode of action.

4. Formulate a workable nursing care plan on the subjective and objective cues gathered through nurse-patient interaction to be able to help the patient towards wellness.

PATIENT'S
PROFILE

A. Biographical DataDate: November 28, 2009: Saturday Clinical Area: 3rd Floor Left Wing; MCM Private RoomName Mrs. C. G.
Address
Date of Birth July 24, 1954
Age 55 years old
Sex Female
Civil Status Married
Nationality Filipino
Religious Preferences Roman Catholic
Place of Birth
Educational Attainment College Graduate
Occupation Housewife
Language Spoken Tagalog and English
Health Care Financing Medocare (Meralco)
Date of Admission November 25, 2009

Diagnosis Hypertensive
Atherosclerotic
Cardiovascular Disease
(HASCVD)
Admitting Physician Dr. Yason
B. Chief Complaint
Client experienced numbness on her left arm coincided with chest pain which she described as radiating from her sternum area towards her xyphoid process lasting approximately for about 10-15 minutes which prompted consult.
She also stated that a week prior to admission, she experienced generalized body weakness and occasional radiating chest pain related to stress and fatigue.
Vital Signs upon admission are as follows:
T = 36.2˚C PR = 120 bpm
BP = 170/100 mmHg RR = 20 cpm

NURSING
HEALTH
HISTORY

A. History of Present Illness
A week prior to admission, client experienced generalized body weakness and occasional radiating chest pain related to stress and fatigue. A day prior to admission she claimed of same symptoms.
B. Past History • Client was diagnosed about 10 years
ago (year 2000) of Hypertension. • Client has a childhood illness of
allergic rhinitis related to dust that is still presently manifested.
• Client hadn’t encountered any form of accident nor serious injuries at the moment.

• Client was previously hospitalized and undergone Bilateral Tubal Ligation approximately 21 years ago. She was about 34 years old.
• Client takes multivitamins and calcium channel blockers as maintenance drugs.
C. Family History
Client claimed with familial history of hypertension (maternal side) and she stated a link in the genealogy that manifested diabetes on her paternal side.
CURRENT
HEALTH STATUS
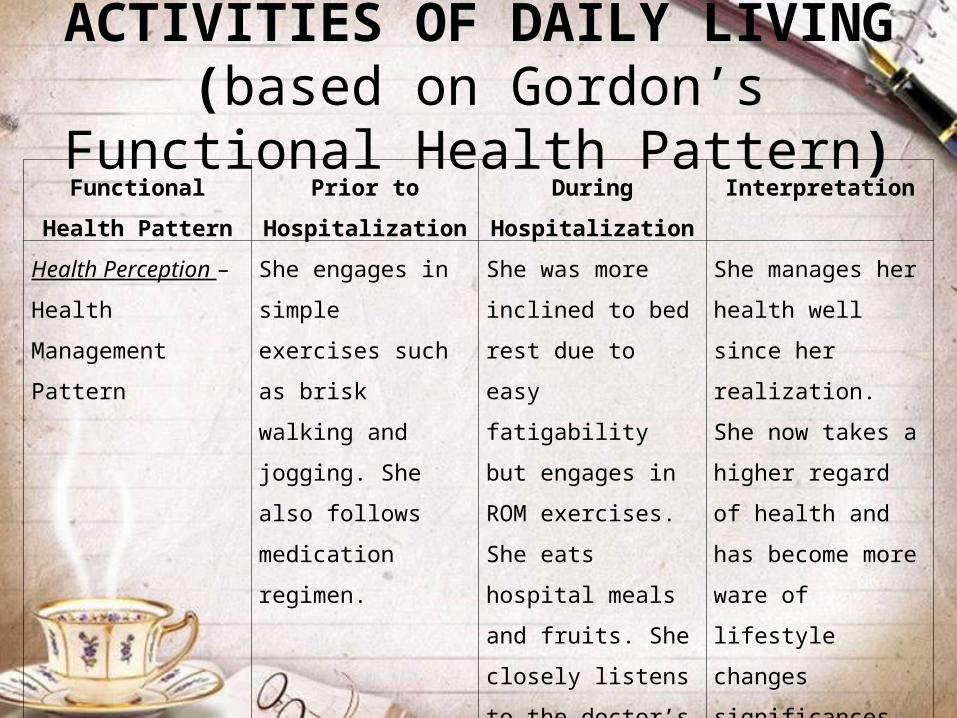
ACTIVITIES OF DAILY LIVING (based on Gordon’s Functional Health Pattern)
Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Health Perception –
Health Management
Pattern
She engages in
simple exercises
such as brisk
walking and jogging.
She also follows
medication regimen.
She was more
inclined to bed rest
due to easy
fatigability but
engages in ROM
exercises. She eats
hospital meals and
fruits. She closely
listens to the doctor’s
and nurse’s health
advices.
She manages her
health well since her
realization. She now
takes a higher
regard of health and
has become more
ware of lifestyle
changes
significances.

Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Nutritional –
Metabolic Pattern
a. number of meals
per day
b. appetite
c. glass of water per
day
d. body built
e. height and weight
4 small frequent
meals a day (usually
s lot of fatty
foods)with good
appetite
6 - 8 glasses of
water a day
Pear shaped
(BMI=23.15)
Height: 57 in’
Weight: 106.7 lbs.
4 small frequent meals a day (meal regulated – low sodium and low fat) with good appetite6 - 8 glasses of water a dayPear shaped (BMI=23.15)
Height: 57 in’
Weight: 106.7 lbs.
There were no
significant changes
in except for a
restriction of low
sodium and low fat
diet.
Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
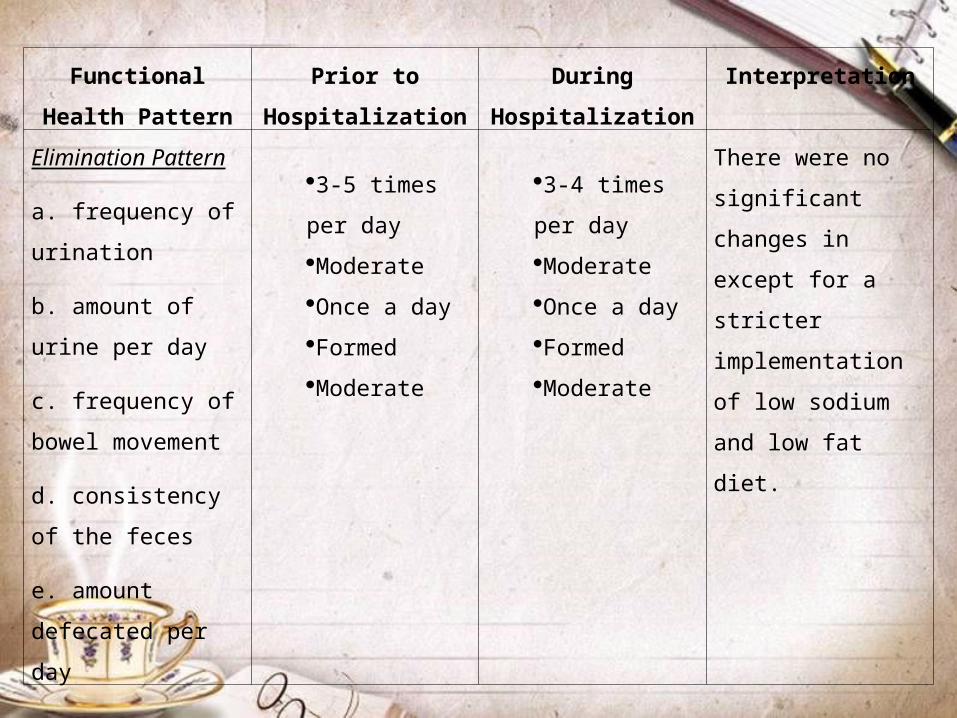
Elimination Pattern
a. frequency of
urination
b. amount of urine
per day
c. frequency of
bowel movement
d. consistency of the
feces
e. amount defecated
per day
3-5 times per
day
Moderate
Once a day
Formed
Moderate
3-4 times per
day
Moderate
Once a day
Formed
Moderate
There were no
significant changes
in except for a
stricter
implementation of
low sodium and low
fat diet.
Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
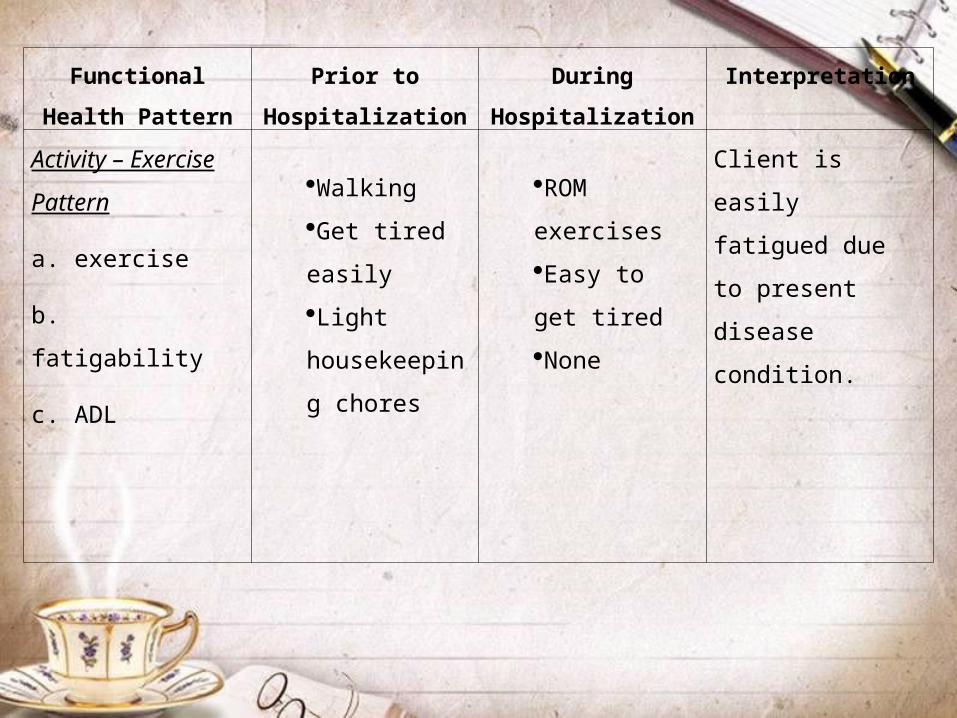
Activity – Exercise
Pattern
a. exercise
b. fatigability
c. ADL
Walking
Get tired
easily
Light
housekeeping
chores
ROM
exercises
Easy to get
tired
None
Client is easily
fatigued due to
present disease
condition.
Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
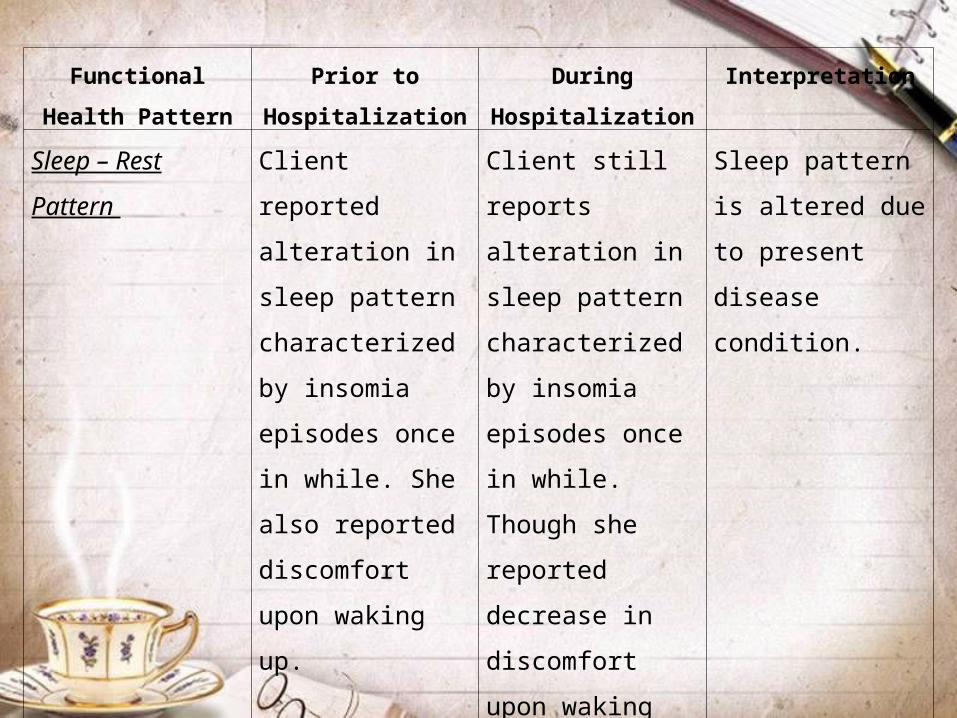
Sleep – Rest
Pattern
Client reported
alteration in sleep
pattern
characterized by
insomia episodes
once in while. She
also reported
discomfort upon
waking up.
Client still reports
alteration in sleep
pattern
characterized by
insomia episodes
once in while.
Though she
reported decrease
in discomfort upon
waking up.
Sleep pattern is
altered due to
present disease
condition.
Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
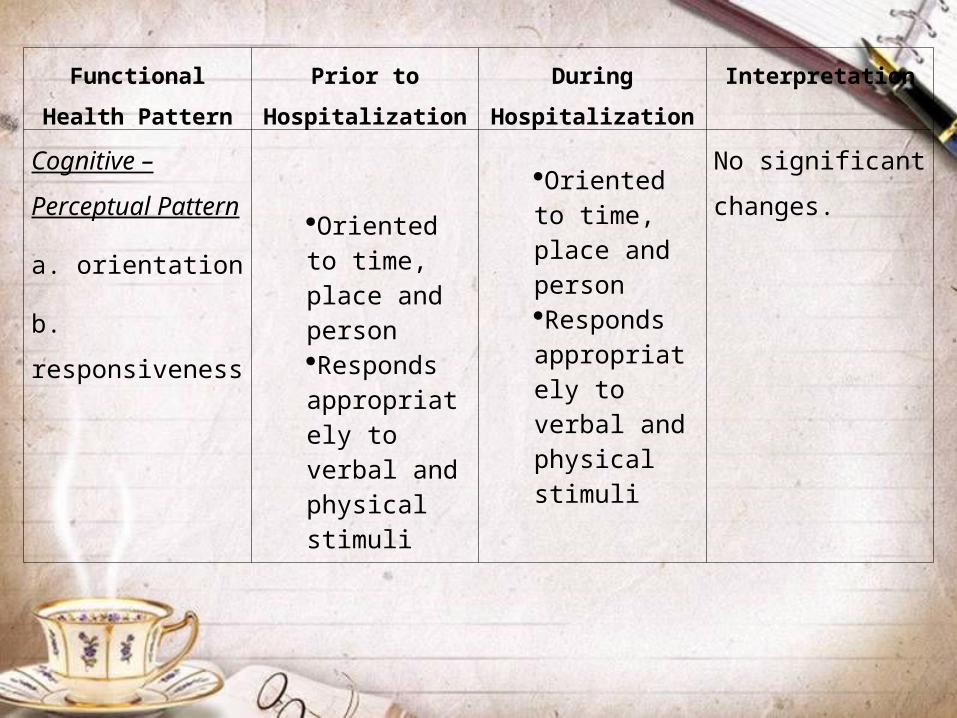
Cognitive –
Perceptual Pattern
a. orientation
b. responsiveness
Oriented to time, place and personResponds appropriately to verbal and physical stimuli
Oriented to time, place and personResponds appropriately to verbal and physical stimuli
No significant
changes.

Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Self-Perception –
Self-Concept
Pattern
Client has high
regard of self worth.
Client still has high
regard of self worth
despite of disease
process.
No significant
changes.

Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Role – Relationship
Pattern
a. as a sister
b. as a wife
c. a mother and
grandmother
With good relationship with her siblings and provided support whenever neededWith good relationship with husband; performs duties as housewifeWith good relationship with sons and daughters as well as with in-laws and grandchildren
Still with good relationship with her siblings and provided support whenever neededStill with good relationship with husband; performs duties as housewifeWith good relationship with sons and daughters as well as with in-laws and grandchildren
No significant
changes

Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Sexuality –
Reproductive
Client was gifted with four children and
was ligated approximately 21 years ago
when she was 34 years old. Due to age,
she confessed that sexual contact is
rarely done.
Changes were
brought about by
three main factors:
Ligation
Age
Menopause

Functional Health
Pattern
Prior to
Hospitalization
During
Hospitalization
Interpretation
Coping – Stress
Tolerance Pattern
In spite of challenges, she is enthusiastic
of overcoming them. She is a strong
willed person and her support system
(family and friends) has strong
foundation.
This helps in a
better prognosis of
her disease
condition.
Value – Belief
Pattern
She is a devout Catholic and believes
that having faith in God will help us get
through challenges. She also believes
that “One should not abuse his/her body
for it will be ourselves who would reap its
effects later on.”. She bases it on her
experience.
Moral belief have
developed and are
applied which helps
in better prognosis
of her disease
condition.

PHYSICAL
ASSESSMENT
Date: November 28, 2009: 9:00am Clinical Area: Medical Center Muntinlupa
Initial vital signs: T = 36˚C
CR = 120bpm RR = 20cpmBP = 150/90mmHg

General Appearance
The patient is conscious, coherent and is not in distress. She looks according to age and is calm and engaging. One can see that she is well nourished and practices good hygiene.

Anthropometric Measurements:
Height: 57 inchesWeight: 106.7 lbsChest Circumference: 38 inchesAbdominal Circumference: 32 inches

Body Part
Assessed
Technique
Used
Actual Finding Interpretation
Skin Inspection
Palpation
Skin color is fair and even
Skin is smooth with fair skin
turgor
Normal
Normal


Body Part
Assessed
Technique
Used
Actual Finding Interpretation
HEENT Nose
Inspection
Palpation
PERRLA
Normoset
No discharge
Non tender
No presence of mass or nodules
Symmetrical nasal folds
Nasal septum at midline
Mucosa is moist, pinkish, intact and no discharge
Airways patent on both nares
Non tender sinuses
Normal
Normal
Normal
Normal
Normal






DISEASE and
TREATMENT

Hypertensive Arteriosclerotic Cardiovascular disease
Atherosclerosis (also known as Arteriosclerotic Vascular Disease or ASVD) is the condition in which an artery wall thickens as the result of a build-up of fatty materials such as cholesterol.
It is a syndrome affecting arterial blood vessels, a chronic inflammatory response in the walls of arteries, in large part due to the accumulation of macrophage white blood cells and promoted by Low density lipoproteins (plasma proteins that carry cholesterol and triglycerides) without adequate removal of fats and cholesterol from the macrophages by functional high density lipoproteins (HDL), (see apoA-1 Milano).
It is commonly referred to as a hardening or furring of the arteries. It is caused by the formation of multiple plaques within the arteries.
CAUSES
Atherosclerosis develops from low-density lipoprotein molecules (LDL) becoming oxidized (ldl-ox) by free radicals, particularly oxygen free (ROS). When oxidized LDL comes in contact with an artery wall, a series of reactions occur to repair the damage to the artery wall caused by oxidized LDL.
The LDL molecule is globular shaped with a hollow care to carry cholesterol throughout the body to generate brain tissues, vitamin D, and soon cholesterol can move in the bloodstream only by being transported by lipoprotein. The body's immune system responds to the damage to the artery wall caused by oxidized LDL by sending specialized white blood cells (macrophages and T-lymphocytes) to absorb the oxidized-LDL forming specialized foam cells.

Atherosclerosis typically begins in early adolescence, and is usually found in most major arteries, yet is asymptomatic and not detected by most diagnostic methods during early stages of life.
PHYSIOLOGIC FACTORS THAT INCREASE RISK
Various anatomic, physiological & behavioral risk factors for atherosclerosis are known. These can be divided into various categories: congenital vs acquired, modifiable or not, classical or non-classical. The points labeled '+' in the following list form the core components of "metabolic syndrome".

Treatment
Some symptoms such as angina pectoris can be treated. Non-pharmaceutical means are usually the first method of treatment, such as cessation of smoking and practicing regular exercise.

If these methods do not work, medicines are usually the next step in treating cardiovascular diseases, and, with improvements, have increasingly become the most effective method over the long term. However, medicines are criticized for their expense, patented control and occasional undesired effects.

LABORATORY
FINDINGS
HEMATOLOGY (NOVEMBER 25, 2009)


CHEMISTRY (NOVEMBER 25, 2009)

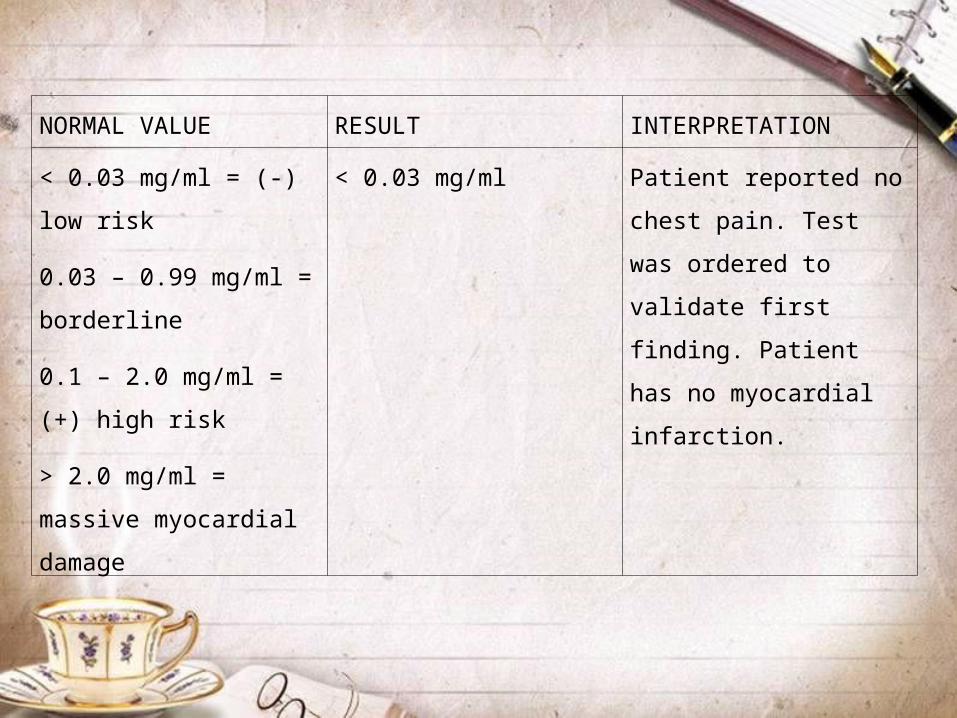
TROPONIN T (NOVEMBER 25, 2009)

NORMAL VALUE RESULT INTERPRETATION
< 0.03 mg/ml = (-) low risk
0.03 – 0.99 mg/ml =
borderline
0.1 – 2.0 mg/ml = (+) high
risk
> 2.0 mg/ml = massive
myocardial damage
< 0.03
mg/ml
Though having an episode of chest
pain, patient has no myocardial
infarction.

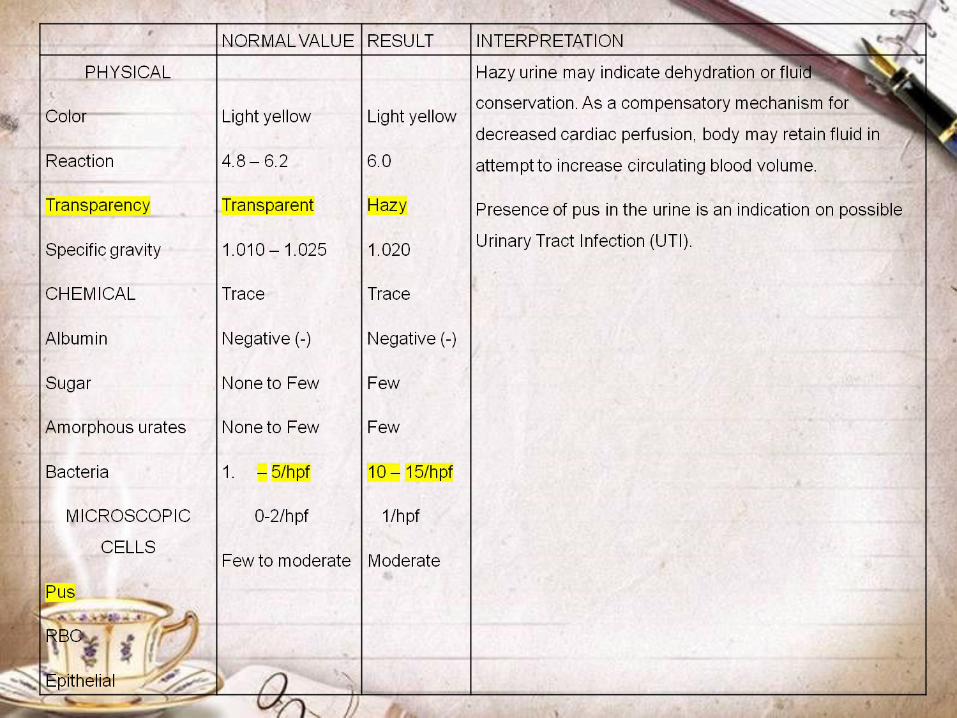
URINALYSIS (NOVEMBER 25, 2009)
PLAIN CRANIAL COMPUTED TOMOG RAPHY (CT) SCAN (NOVEMBER 25, 2009)


TROPONIN T (NOVEMBER 26, 2009)
NORMAL VALUE RESULT INTERPRETATION
< 0.03 mg/ml = (-) low risk
0.03 – 0.99 mg/ml =
borderline
0.1 – 2.0 mg/ml = (+) high
risk
> 2.0 mg/ml = massive
myocardial damage
< 0.03 mg/ml Patient reported no chest
pain. Test was ordered to
validate first finding.
Patient has no myocardial
infarction.

CHEMISTRY (NOVEMBER 26, 2009)


CARDIAC DIAGNOSTIC TEST - ELECTROCARDIOGRAM (ECG) RESULT (NOVEMBER 25, 2009)

DIMENSION NORMAL
VALUE
RESULT FUNCTION NORMAL
VALUE
RESULT
(ed)
(es)
RV (ed)
LA (es)
RA (es)
Aorta
PA
IVS (ed)
IIS (es)
LVPW (ed)
LVPW (es)
MV ANNU
4.5 – 5.0
2.2 – 3.5
3.0 – 3.5
3.5
3.5
3
(0.8 – 1.1)
(0.8 – 1.1)
4.2
3.0
3.1
3.1
3.1
2.9
2.5
1.1
1.3
1.1
1.3
LVEPV
LVESV
Stroke Volume
(SV)
Cardiac Output
(CO)
EF%
FS%
VSF
EPSS
Wall Stress
Wall Stress
LVWMSI
LVTD
(55 – 77%)
(28 – 92% 0
(0.8 – 1.1)
(< 195)
(< OOD)
44 ml
2 L/min
55%
28%
1
1.7
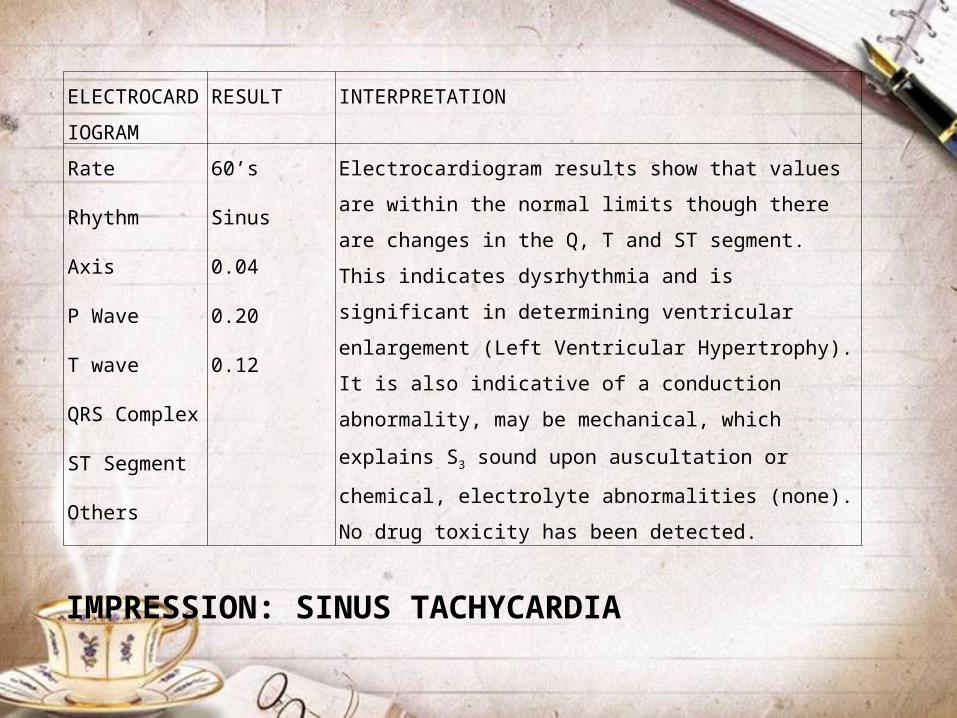
ELECTROCAR
DIOGRAM
RESULT INTERPRETATION
Rate
Rhythm
Axis
P Wave
T wave
QRS Complex
ST Segment
Others
60’s
Sinus
0.04
0.20
0.12
Electrocardiogram results show that values are within the
normal limits though there are changes in the Q, T and ST
segment. This indicates dysrhythmia and is significant in
determining ventricular enlargement (Left Ventricular
Hypertrophy). It is also indicative of a conduction
abnormality, may be mechanical, which explains S3 sound
upon auscultation or chemical, electrolyte abnormalities
(none). No drug toxicity has been detected.
IMPRESSION: SINUS TACHYCARDIA
DRUG STUDY

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Glimipiride(Amaryl)
Anti diabetesGlucagon
2mgOD
PO Lowers blood glucose level. Stimulates release of insulin from functioning pancreatic beta cells and lead to increased sensitivity of peripheral tissues to insulin.
Adjunct to diet and exercise to lower glucose level (DM type 2) whose hyperglycemia can’t be managed by diet and exercise alone.
1. Advise patient to take it with first main meal of the day.
2. Teach patient to carry candy or simple sugars to treat mild episodes of low sugar level.
NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
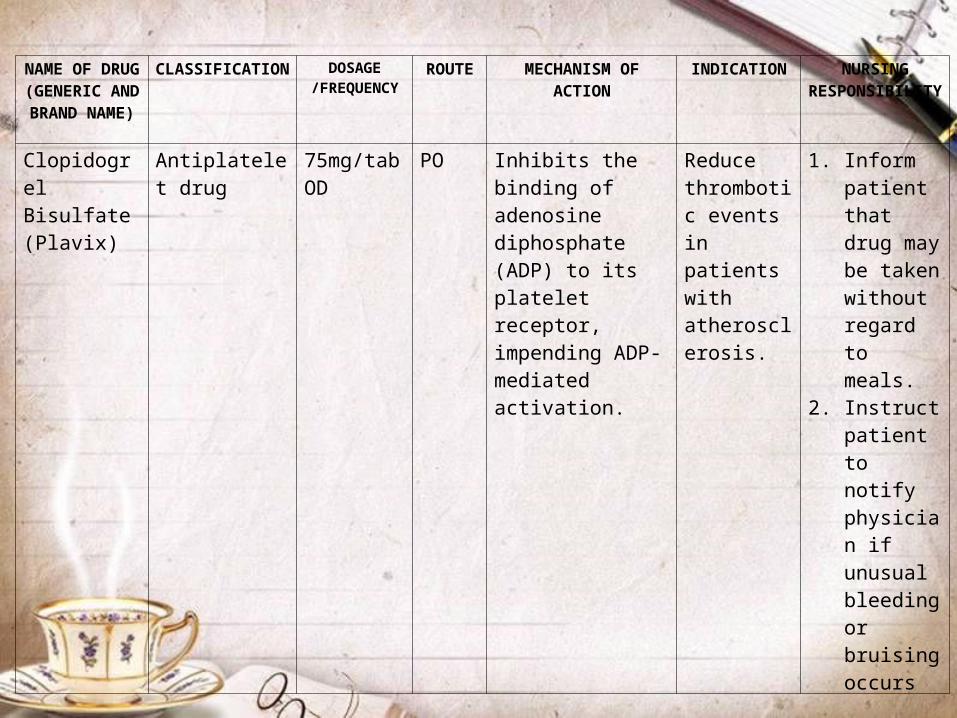
Clopidogrel Bisulfate(Plavix)
Antiplatelet drug
75mg/tabOD
PO Inhibits the binding of adenosine diphosphate (ADP) to its platelet receptor, impending ADP-mediated activation.
Reduce thrombotic events in patients with atherosclerosis.
1. Inform patient that drug may be taken without regard to meals.
2. Instruct patient to notify physician if unusual bleeding or bruising occurs

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Lactulose (Duphalac)
Laxative 30ccOD Hs
PO Produces an osmotic effect in colon;Promote peristalsis, decrease ammonia as a result of bacterial degradation which lowers the pH of the colon contents.
Constipation; prevent stimulation of the vagal nerve
1. Inform patient about adverse effect and to notify physician once it occurs

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Simvastatin(Synvinolin)
Anti lipemics 40g/tabOD
PO Inhibits HMG-COA reductase, an early and rate limiting step in cholesterol biosynthesis.
Reduce risk of death from cardiovascular disease and cardiovascular events in patients at high risk for coronary events;Reduce total LDL cholesterol
1. Instruct patient to take drug with evening meals because taking this enhances absorption and increase cholesterol biosynthesis.
2. Instruct patient to inform physician if adverse reactions occur particularly muscle pains
NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
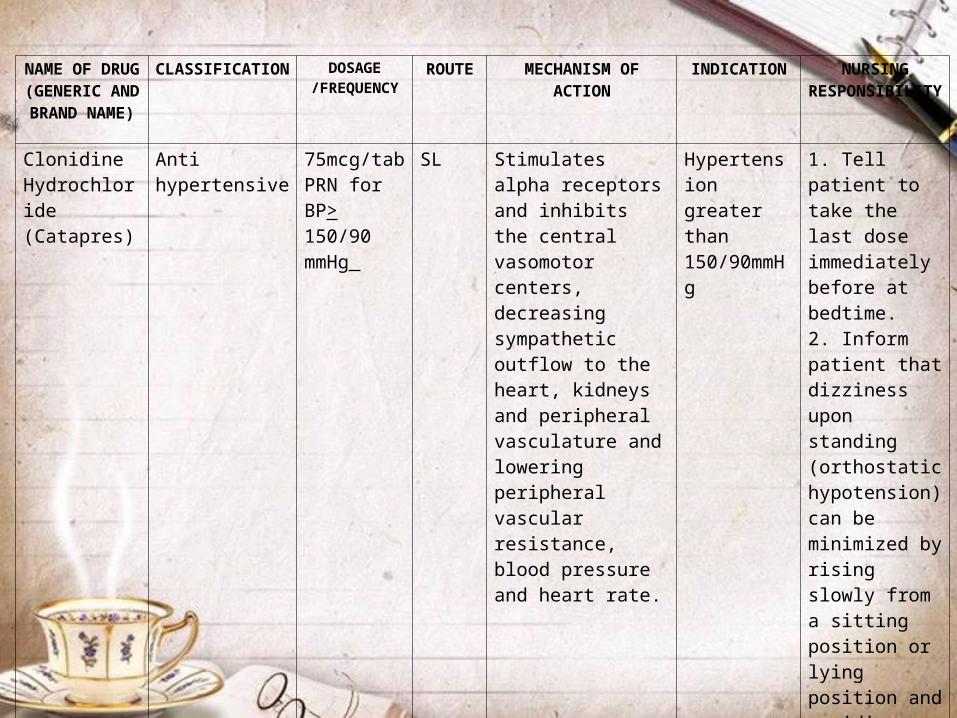
Clonidine Hydrochloride(Catapres)
Anti hypertensive
75mcg/tabPRN for BP> 150/90 mmHg
SL Stimulates alpha receptors and inhibits the central vasomotor centers, decreasing sympathetic outflow to the heart, kidneys and peripheral vasculature and lowering peripheral vascular resistance, blood pressure and heart rate.
Hypertension greater than 150/90mmHg
1. Tell patient to take the last dose immediately before at bedtime.2. Inform patient that dizziness upon standing (orthostatic hypotension) can be minimized by rising slowly from a sitting position or lying position and avoiding sudden position changes.

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Nitroglycerin Vasodilator, Antianginal
5mg. OACW q 8 NFI
Patch Decreases oxygen demand by decreasing preload and afterload
To prevent or minimize anginal attacks before stressful events
1. Closely monitor V/S esp. BP
2. Applied to any nonhairy parts of the skin except distal parts of the arms and legs
NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
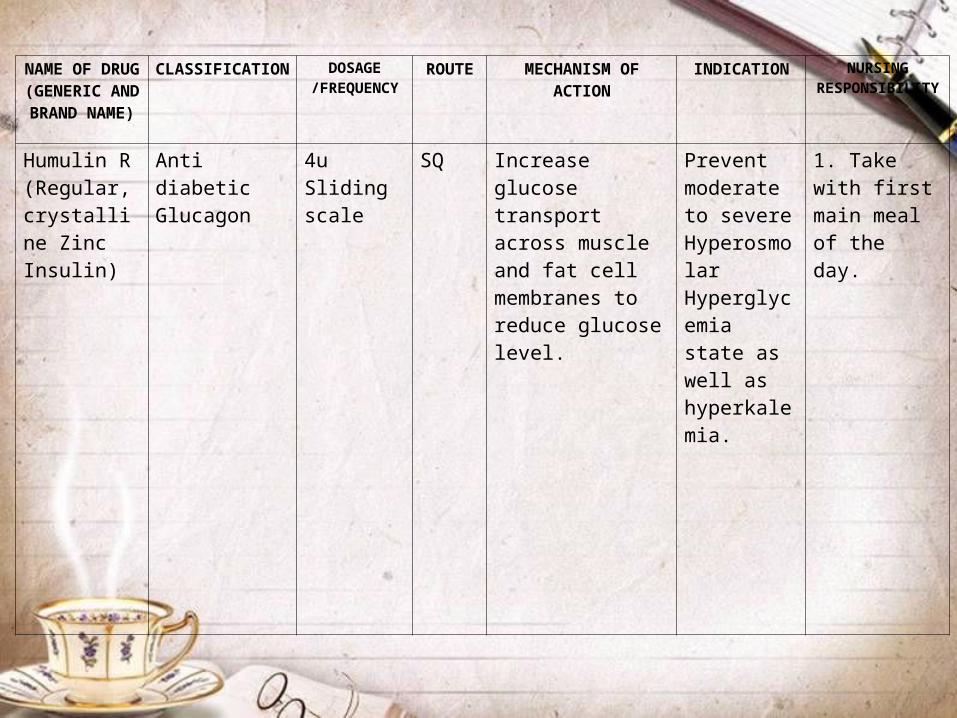
Humulin R(Regular, crystalline Zinc Insulin)
Anti diabeticGlucagon
4uSliding scale
SQ Increase glucose transport across muscle and fat cell membranes to reduce glucose level.
Prevent moderate to severe Hyperosmolar Hyperglycemia state as well as hyperkalemia.
1. Take with first main meal of the day.

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Levofloxacin(Levaquin)
Anti infective 1 tablet TID
PO Inhibits bacterial DNA gyrase and prevents DNA replication, transcriptions, repair and recombination in
Acute bacterial infections caused by susceptible strains of streptococcus
1. Tell patient to take medication 1 hr before or 2 hrs after eating for increased absorption.

NAME OF DRUG
(GENERIC AND BRAND NAME)
CLASSIFICATION DOSAGE/FREQUENCY
ROUTE MECHANISM OF ACTION
INDICATION NURSING RESPONSIBILITY
Isosobide Mononitrate(Indur)
Anti angina 60g/1/2 tab
OD
SL Reduces cardiac oxygen demand by decreasing preload and afterload; Increases blood flow through the collateral coronary vessels.
Prevent acute anginal attacks; Acute anginal attacks
1. Tell patient to take sublingual tablet at first sign of attack. 2. Wet tablet with saliva and place under tongue until absorbed.3. Take in sitting down and at rest.

Nursing Care
Plan
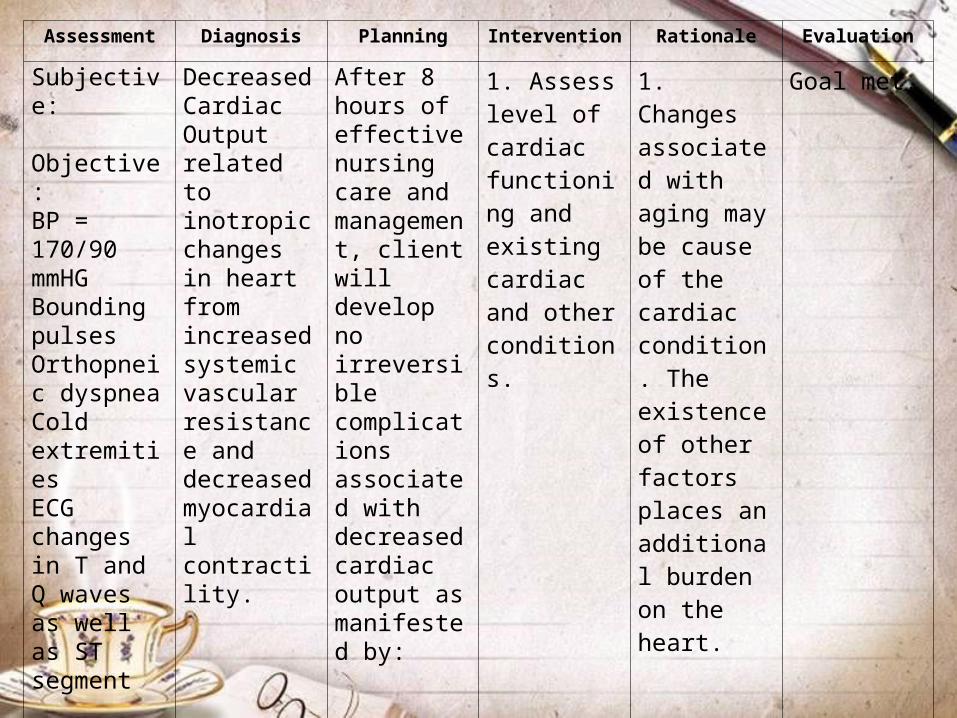
Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective: Objective:BP = 170/90 mmHGBounding pulsesOrthopneic dyspneaCold extremitiesECG changes in T and Q waves as well as ST segment
Decreased Cardiac Output related to inotropic changes in heart from increased systemic vascular resistance and decreased myocardial contractility.
After 8 hours of effective nursing care and management, client will develop no irreversible complications associated with decreased cardiac output as manifested by:
1. Assess level of cardiac functioning and existing cardiac and other conditions.
1. Changes associated with aging may be cause of the cardiac condition. The existence of other factors places an additional burden on the heart.
Goal met.

Assessment Diagnosis Planning Intervention Rationale Evaluation
No jugular vein distentionNo episodes of angina /chest painNo respiratory distress
2. Assess BP (150/90 mmHG), pulse rate and rhythm (69 bpm; bounding), apical pulse (69 bpm; with tachycardia intensity), respiratory rate, depth and ease (20 cpm; not in distress).
2. Indicates reduced cardiac output, vasodilation and lower blood volume. Respiratory changes or difficulties that decrease oxygen intake can cause hypoxia.
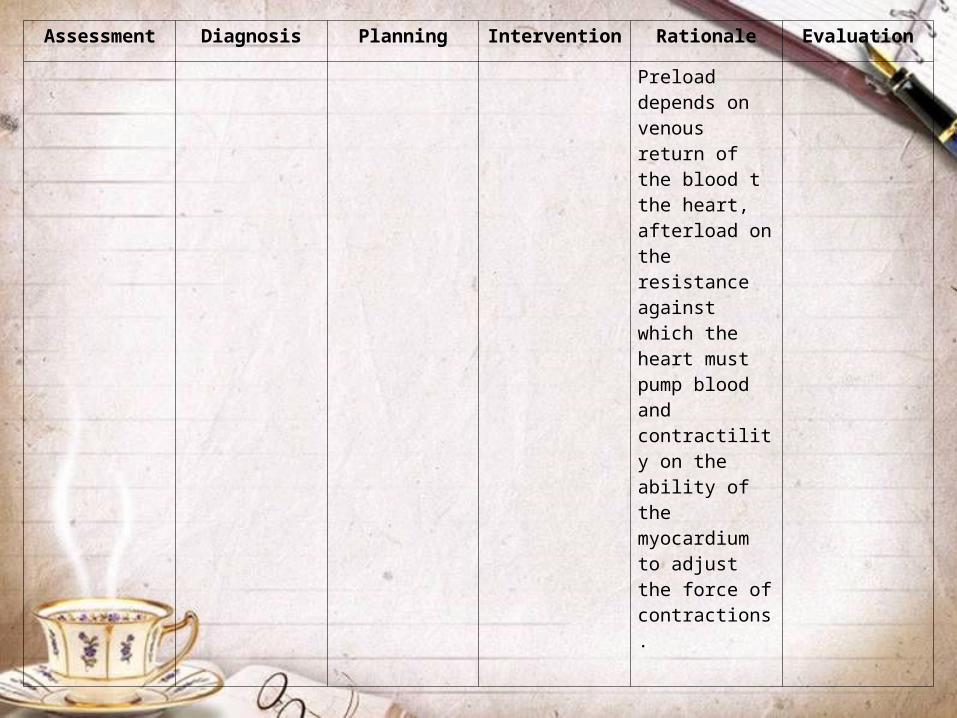
Assessment Diagnosis Planning Intervention Rationale Evaluation
Preload depends on venous return of the blood t the heart, afterload on the resistance against which the heart must pump blood and contractility on the ability of the myocardium to adjust the force of contractions.

Assessment Diagnosis Planning Intervention Rationale Evaluation
3. Auscultate heart sounds for abnormal sounds; breath sounds for crackles or wheezes (not present).
3. Reveals mechanical or electrical alterations in cardiac function, presence of fluid congestion in heart and/or lungs and cardiac dysfunction. Crackles or wheezes may indicate the presence of, or impending, congestive failure and fluid overload.

Assessment Diagnosis Planning Intervention Rationale Evaluation
4. Monitor for existence of dysrhythmias, cardiac conduction and rhythm (ECG changes).
4. The heart conduction system controls the rhythmic contractions and relaxations of the heart and maintains its pumping efficiency, rate and rhythm which ultimately affect cardiac output. Dysrhythmias and conduction aberrations decrease cardiac output by increasing the workload of the heart and decreasing myocardial perfusion.

Assessment Diagnosis Planning Intervention Rationale Evaluation
5. Assess lower extremities and sacral area for edema, distended neck veins, cold hands and feet (present) or oliguria (not present).
Dysrhythmias and conduction aberrations decrease cardiac output by increasing the workload of the heart and decreasing myocardial perfusion
5. Indicates reduced venous return to the heart and low cardiac output.
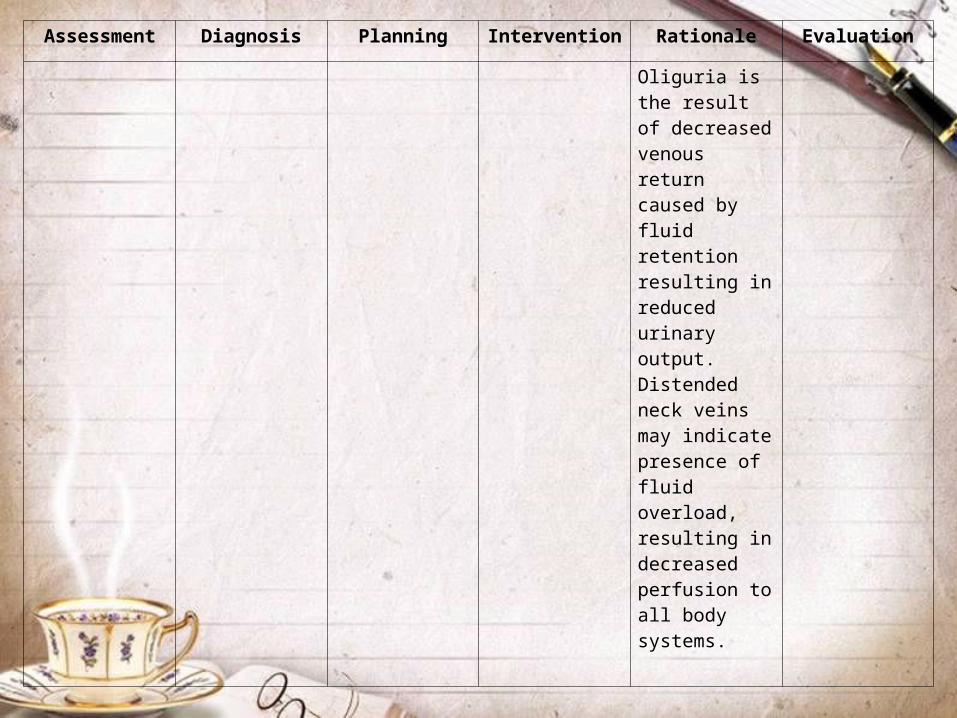
Assessment Diagnosis Planning Intervention Rationale Evaluation
Oliguria is the result of decreased venous return caused by fluid retention resulting in reduced urinary output. Distended neck veins may indicate presence of fluid overload, resulting in decreased perfusion to all body systems.
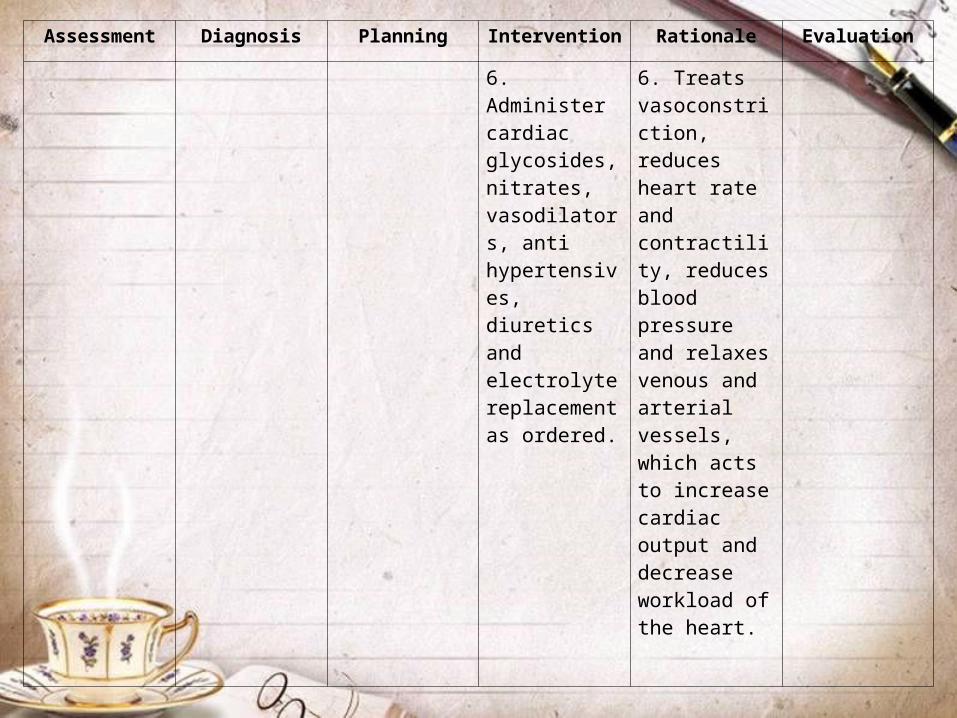
Assessment Diagnosis Planning Intervention Rationale Evaluation
6. Administer cardiac glycosides, nitrates, vasodilators, anti hypertensives, diuretics and electrolyte replacement as ordered.
6. Treats vasoconstriction, reduces heart rate and contractility, reduces blood pressure and relaxes venous and arterial vessels, which acts to increase cardiac output and decrease workload of the heart.
Assessment Diagnosis Planning Intervention Rationale Evaluation
7. Position in semi or high Fowler’s position.
8. Weigh on same scale at the same time.
7. Prevents pooling of blood in pulmonary vessels and facilitates breathing via increased lung expansion.
8. Weight gain of >1lb/day may indicate fluid retention. Utilization of the same scale facilitates consistent data to ensure correct correlation with fluid status.
Assessment Diagnosis Planning Intervention Rationale Evaluation
9. Pace activities, avoiding going past point of tolerance and progress in exercise regimen as able.
10. Avoid Valsalva maneuvers with straining and coughing.
9. Prevents undue demands on heart and protects cardiac function by preventing sudden reduction in cardiac output.
10. Results in sudden reduction in cardiac output by increasing intra abdominal pressure and intra thoracic pressures.

Assessment Diagnosis Planning Intervention Rationale Evaluation
11. Instruct client in administration of prescribed medications, actins and side effects. Advise client to avid over the counter (OTC) drugs without physician advice.
11. Promotes desired action and results. Prevents adverse interactions with other drugs.

Assessment Diagnosis Planning Intervention Rationale Evaluation
12. Instruct patient in program of activities; combination of interchanging active and passive range of motion (ROM) activity.
13. Instruct client in establishing pattern of bowel elimination of soft stool; proper administration of stool softer or laxative if ordered.
12. Promotes circulation by preserving muscle tone and strength. Heat generated by exercises promotes cellular metabolism.
13. Promotes easy elimination without straining.

Assessment Diagnosis Planning Intervention Rationale Evaluation
14. Instruct client in elevation of legs when sitting, to avoid standing in one place or for long periods of time.
15. Instruct client in reporting edema, chest pain, changes in vital signs and input and output imbalance.
16. Instruct client and significant other in techniques for taking pulse and blood pressure.
14. Promotes venous blood return.
15. May indicate complications of reduced cardiac output.
16. Allows for self-monitoring.

Assessment Diagnosis Planning Intervention Rationale Evaluation
17. Instruct client regarding dietary restrictions and methods to reduce fat, cholesterol and sodium intake.
17. May assist with reduction in cholesterol levels to control atherosclerosis and its effect on blood flow. Sodium restriction may also improve hypertension and prevent edema.

#2Nursing care Plan

Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective: Objective:Chest pain Numbness of left arm ECG changes in T and Q waves as well as ST segmentCold extremitiesIncreased BUN 8.4 mg/dL
Ineffective Tissue Perfusion related to decreased cardiac output
After 8 hours of effective nursing care and management, client will show signs of adequate perfusion to all body systems as evidenced by:Warm extremitiesNo paresthesia (numbness)Absence of chest pain/angina
1. Monitor vital signs q2˚ and prn.
2. Monitor ECG for cardiac rhythm, conduction defects and dysrhythmias.
1. Tachypnea, tachycardia and hypertension will most likely occur with hypoperfusion and decreased cardiac output.
2. Fluid shifting can create electrolyte imbalances and cardiac hypoperfusion that may result in cardiac rhythm irregularities.

Assessment Diagnosis Planning Intervention Rationale Evaluation
3. Auscultate lung fields and heart tones.
4. Auscultate abdomen for presence and character of bowel sounds. Observe for abdominal distention.
3. Wheezes and crackles may indicate possible pulmonary edema. May indicate impending cardiac failure and cardiac hypoperfusion.
4. Decreasing or absent bowel sounds may indicate presence of ileus, obstruction or hypoperfused state.

Assessment Diagnosis Planning Intervention Rationale Evaluation
5. Palpate peripheral pulses and observe extremities for color, temperature, capillary refill and sensation.
6. Avoid Trendelenburg’s position.
5. Hypoperfusion causes the body to shunt blood from the periphery to vital organs, leading to cold extremities and change in peripheral pulse intensity.
6. Position, impedes gas exchange, increases pulmonary blood flow and may decrease cerebral perfusion.

Assessment Diagnosis Planning Intervention Rationale Evaluation
7. Assist with ambulation and combination of passive and active range of motion (ROM) exercises.
8. Monitor patient for orientation status. Reorient as needed.
7. Assists to improve peripheral and arterial circulation and prevents venous stasis.
8. Hypoperfusion may result in decreased level of consciousness (LOC). Re orientation helps to maintain sense of well-being and orientation to surroundings to decrease risk of injury.

Assessment Diagnosis Planning Intervention Rationale Evaluation
9. Instruct client regarding dietary restrictions and methods to reduce fat, cholesterol and sodium intake.
9. May assist with reduction in cholesterol levels to control atherosclerosis and its effect on blood flow. Sodium restriction may also improve hypertension and prevent edema.

#3Nursing care Plan

Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective:“Naninikip and dibdib ko”, as verbalized by the patient
Impaired Gas Exchange related to ineffective ventricular function
After 8 hours of effective nursing care and management: client will:Achieve and maintain adequate ventilation, without adventitious breath sounds on auscultationBe able to perform activities without experiencing dyspnea.
1. Assess patient and establish baseline values for vital signs. Assess for coexisting disease processes.
1. Baseline data is crucial to help recognize age-related changes. Elderly patients usually have a shorter respiration, which decreases their maximum breathing capacity, vital capacity, functional capacity and residual volumes.
After the shift, with effective nursing care and management: client:Achieved and maintained adequate ventilation, without adventitious breath sounds on auscultationWas able to perform activities without experiencing dyspnea.
Assessment Diagnosis Planning Intervention Rationale Evaluation
2. Auscultate lung fields.
3. Place client in semi or high Fowler’s position as tolerated.
2. Wheezes and chackles may indicate presence of pulmonary emboli. 3. Facilitates maximum lung expansion. In elderly patients, the muscles of the larynx and pharynx may deteriorate and these positions may be required to achieve adequate thoracic expansion.
Assessment Diagnosis Planning Intervention Rationale Evaluation
4. Instruct patient in relaxation techniques and guided imagery. Discuss patient’s method of relaxation and adapt them as appropriate.
4. The ability of patient to relax may enhance and facilitate reduction of oxygen demand to the tissues. Using patient’s previous experiences with relaxation may enhance ability to decrease oxygen consumption and improve oxygenation.

Assessment Diagnosis Planning Intervention Rationale Evaluation
5. Instruct patient in positions to use to assist when dyspnea occurs, such as high Fowler’s or orthopneic position.
5. Because of anatomic changes n the elderly, compensation with different positions may be required to achieve maximum chest excursion and facilitate oxygenation.

Assessment Diagnosis Planning Intervention Rationale Evaluation
6. Instruct client to schedule rest periods between activities.
6. Older patients may have decreased exertional capacity and need rest periods to conserve respiratory effort. Their alveoli are usually more fibrous and less elastic and contain fewer functional capillaries in which to achieve oxygenation.
Assessment Diagnosis Planning Intervention Rationale Evaluation
7. Instruct client and significant others regarding lifestyle changes.
7. Patient may need to have bedroom or living area moved to first floor, be moved close to the bathroom, have smaller meals more frequently and have frequent rest periods during activities in order to reduce exertion and oxygen demand and consumption.
#3Nursing care Plan

Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective:“Ang sakit ng dibdib ko”, as stated by the patient.Objective:Chest pain radiating to armExertional dyspneaPain occurring after activityPain scale of 6-7
Acute Pain related to decreased myocardial perfusion.
After 4 hours of effective nursing care and intervention, client will:Be free of painBe able to identify pain, communicate needs and utilize methods to reduce pain
1. Assess characteristic of pain, precipitating factors, verbal and non-verbal responses, pain onset, location, severity, duration and radiation.
2. Monitor VS during pain episode.
1. Pain from angina occurs when myocardial need for oxygen exceeds the ability of coronary vessels to supply needed blood flow as the lumen is narrowed by atherosclerosis.
Goal met

Assessment Diagnosis Planning Intervention Rationale Evaluation
3. Administer vasodilators as ordered.
2. Increases in pulse and BP are caused by anxiety and stress may precipitate angina episode. In elderly patients, dyspnea with exertion may be seen more commonly that chest pain because of increasing left ventricular end diastolic pressures as a result of reduced ventricular compliance.
Assessment Diagnosis Planning Intervention Rationale Evaluation
4. Administer analgesics as ordered, prn.
5. Administer oxygen at 2-4 L/min via nasal cannula as ordered.
3. Vasodilators improve blood flow and reduce ischemia and pain.
4. Increases patient’s pain threshold. Morphine may be administered to decrease after load and preload and improving contractility.
5. Relieves heart muscle hypoxia.

Assessment Diagnosis Planning Intervention Rationale Evaluation
7. Limit activity and maintain bed rest.
8. Maintain quiet, calm environment, provide relaxing backrub, guided imagery.
7. Decreases myocardial oxygen consumption and strain on the heart. 8. Reduces stimuli that increase oxygen demand.
8. Hypoperfusion may result in decreased level of consciousness (LOC). Re orientation helps to maintain sense of well-being and orientation to surroundings to decrease risk of injury.

Assessment Diagnosis Planning Intervention Rationale Evaluation
9. Instruct client regarding dietary restrictions and methods to reduce fat, cholesterol and sodium intake.
9. May assist with reduction in cholesterol levels to control atherosclerosis and its effect on blood flow. Sodium restriction may also improve hypertension and prevent edema.

#4Nursing care Plan

Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective:“Ang sakit ng dibdib ko”, as stated by the patient.Objective:Chest pain radiating to armExertional dyspneaPain occurring after activityPain scale of 6-7
Acute Pain related to decreased myocardial perfusion.
After 4 hours of effective nursing care and intervention, client will:Be free of painBe able to identify pain, communicate needs and utilize methods t
1. Assess characteristic of pain, precipitating factors, verbal and non-verbal responses, pain onset, location, severity, duration and radiation.
2. Monitor VS during pain episode.
1. Pain from angina occurs when myocardial need for oxygen exceeds the ability of coronary vessels to supply needed blood flow as the lumen is narrowed by atherosclerosis.
Goal met

Assessment Diagnosis Planning Intervention Rationale Evaluation
2. Increases in pulse and BP are caused by anxiety and stress may precipitate angina episode. In elderly patients, dyspnea with exertion may be seen more commonly that chest pain because of increasing left ventricular end diastolic pressures as a result of reduced ventricular
Assessment Diagnosis Planning Intervention Rationale Evaluation
3. Administer vasodilators as ordered
4. Administer analgesics as ordered, prn.
5. Administer oxygen at 2-4 L/min via nasal cannula as ordered.
3. Vasodilators improve blood flow and reduce ischemia and pain.
4. Increases patient’s pain threshold. Morphine may be administered to decrease after load and preload and improving contractility.
5. Relieves heart muscle hypoxia.

Assessment Diagnosis Planning Intervention Rationale Evaluation
7. Limit activity and maintain bed rest.
8. Maintain quiet, calm environment, provide relaxing backrub, guided imagery.
9. Instruct pain to report pain lasting longer that 5 – 15 minutes; review effect of medication administration.
7. Decreases myocardial oxygen consumption and strain on the heart.
8. Reduces stimuli that increase oxygen demand.
9. Indicates that medication adjustment needs to be made or cardiac complication is present.

Assessment Diagnosis Planning Intervention Rationale Evaluation
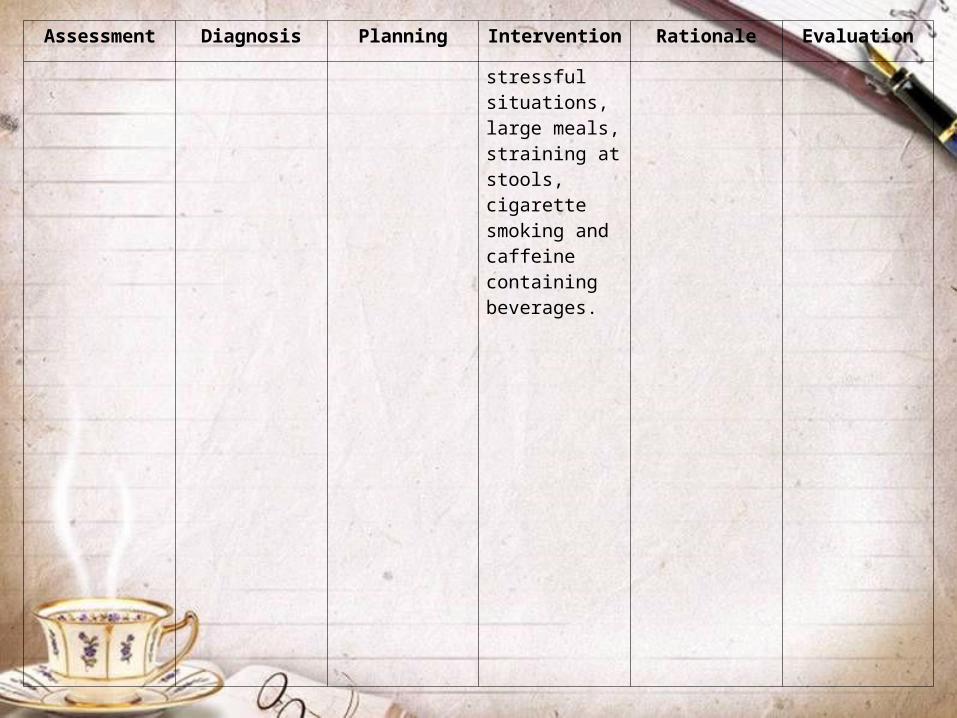
10. Instruct patient to maintain log of time, duration and location of angina episodes, amount of medication taken and so forth.
11. Instruct patient to avoid activities that precipitate angina episodes such as, sudden exposure to cold, drinking cold fluids,
10. Offers comparisons for physician to review.
11. Reduces frequency of attacks.
Assessment Diagnosis Planning Intervention Rationale Evaluation
stressful situations, large meals, straining at stools, cigarette smoking and caffeine containing beverages.

#5Nursing care Plan
Assessment Diagnosis Planning Intervention Rationale Evaluation
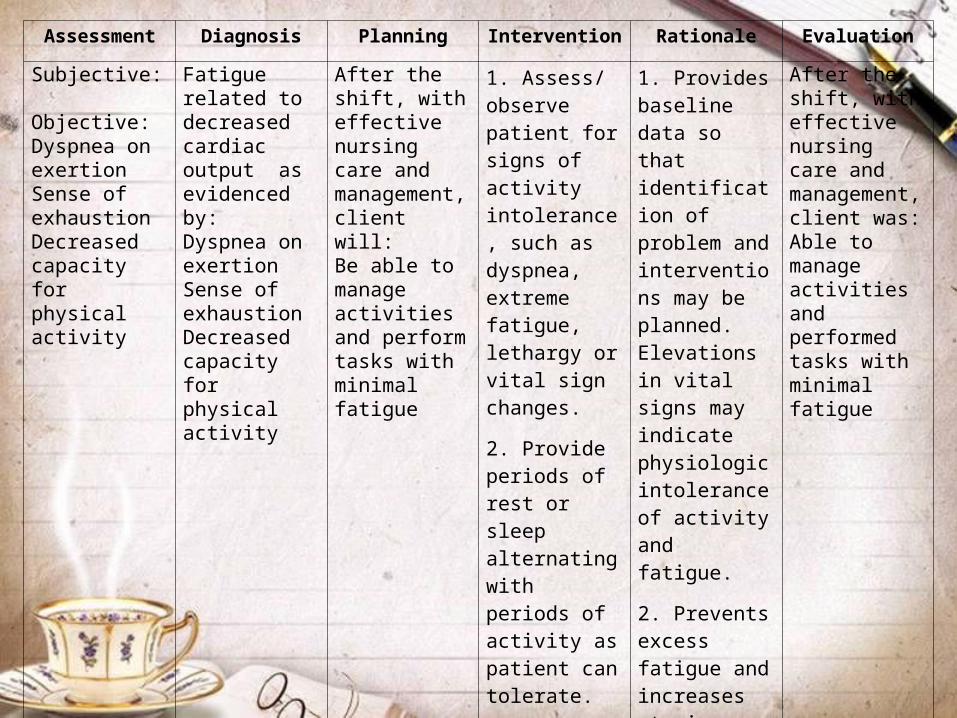
Subjective: Objective:Dyspnea on exertionSense of exhaustionDecreased capacity for physical activity
Fatigue related to decreased cardiac output as evidenced by:Dyspnea on exertionSense of exhaustionDecreased capacity for physical activity
After the shift, with effective nursing care and management, client will:Be able to manage activities and perform tasks with minimal fatigue
1. Assess/ observe patient for signs of activity intolerance, such as dyspnea, extreme fatigue, lethargy or vital sign changes.
2. Provide periods of rest or sleep alternating with periods of activity as patient can tolerate.
1. Provides baseline data so that identification of problem and interventions may be planned. Elevations in vital signs may indicate physiologic intolerance of activity and fatigue.
2. Prevents excess fatigue and increases stamina.
After the shift, with effective nursing care and management, client was:Able to manage activities and performed tasks with minimal fatigue
Assessment Diagnosis Planning Intervention Rationale Evaluation
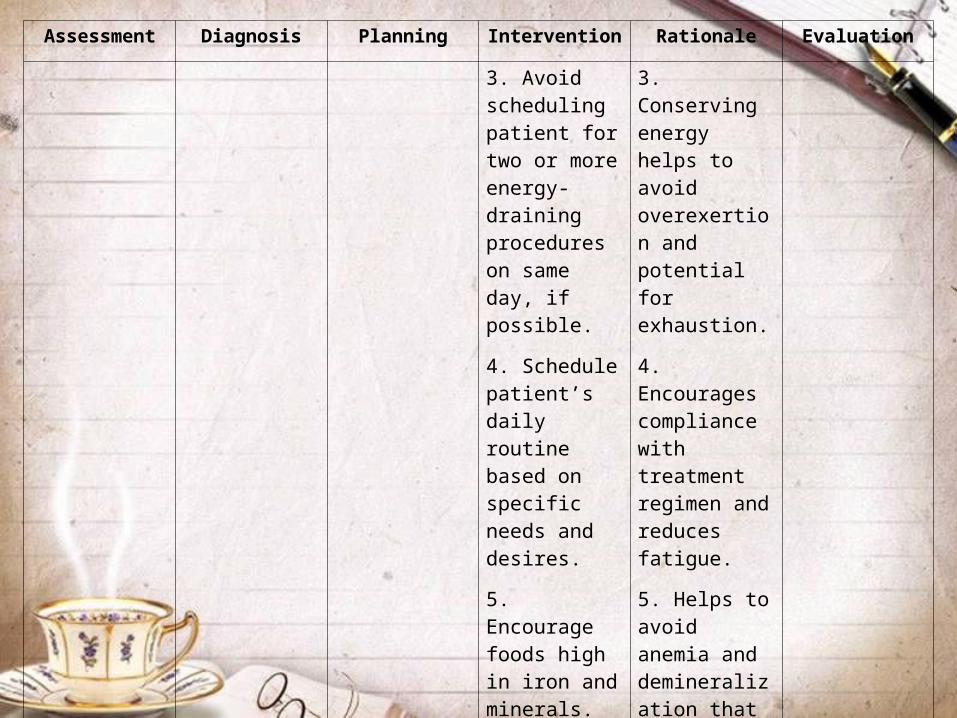
3. Avoid scheduling patient for two or more energy-draining procedures on same day, if possible.
4. Schedule patient’s daily routine based on specific needs and desires.
5. Encourage foods high in iron and minerals.
3. Conserving energy helps to avoid overexertion and potential for exhaustion.
4. Encourages compliance with treatment regimen and reduces fatigue.
5. Helps to avoid anemia and demineralization that can affect fatigue. Low RBCs affect a patient’s oxygenation as oxygen molecules are carried throughout the body via hemoglobin molecules.

Assessment Diagnosis Planning Intervention Rationale Evaluation
6. Provide small, easily digestible meals.
7. Instruct patient regarding effects of fatigue on daily activity and personal lifestyle.
Low RBCs affect a patient’s oxygenation as oxygen molecules are carried throughout the body via hemoglobin molecules.
6. Frequent small meals conserve energy and encourage increased intake of nutritive sustenance.

Assessment Diagnosis Planning Intervention Rationale Evaluation
8. Instruct patient to schedule rest periods between activities.
9. Instruct patient and help him to establish a regular sleeping pattern.
7. Helps to increase patient compliance and allows for planning schedule of activity and rest.
8. Helps to decrease fatigue and increase stamina.
9. Adequate amounts of sleep each night will help decrease fatigue.

#6Nursing care Plan

Assessment Diagnosis Planning Intervention Rationale Evaluation
Subjective: Objective:Dyspnea on exertionFatigueChest pain during activity
Activity Intolerance related to imbalance between oxygen supply and demand caused by disease process and aging as evidenced by:Dyspnea on exertionFatigueChest pain during activity
After the shift, with effective nursing care and management client will:Achieve optimal activity level with increased energy and endurance within imposed restrictions
1. Assess baseline tolerance for activity, ability to adapt to limitations and/or restrictions to lifestyle.
2. Asses pulse, BP, respiration, before, during and after activity.
3. If activity causes pain, administer vasodilators as ordered.
1. Promotes and protects circulatory function and reduces cardiac workload.
2. Pulse increase more than 20bpm and increases in BP and respirations indicate need for reduction of activity.
3. Controls pain during activity by decreasing oxygen demand and improving perfusion.
After the shift, with effective nursing care and management client will:
Achieve optimal activity level with increased energy and endurance within imposed restrictions

Assessment Diagnosis Planning Intervention Rationale Evaluation
4. Schedule activities around rest periods.
5. Instruct patient to avoid extending activities beyond tolerance.
6. Instruct patient to avoid activity after eating, bathing or during rest periods.
7. Instruct patient to keep medication nearby when performing activity.
4. Maintains activity below angina threshold.
5. Conserves energy and prevents angina.
6. Requires additional oxygen for activities.
7. Availability to administer when needed.

Assessment Diagnosis Planning Intervention Rationale Evaluation
8. Inform to cease activity when pain occurs and when taking medication, to sit on chair and wait for pain to pass.
9. Suggest cardiac rehabilitation program to establish a daily acceptable exercise plan within determined limits.
8. Prevents falls if feeling dizzy or faint and decreases oxygen requirement.
9. Provides necessary activity without causing increased workload to the heart and improves circulation.

Assessment Diagnosis Planning Intervention Rationale Evaluation
10. Instruct patient to rest by sitting in chair than lying in bed and to conserve energy during activities.
10. Sitting is the preferred position for resting because it prevents pooling of blood in the pulmonary vessels. Sitting upright also helps to prevent complications associated with immobility and facilitates better chest excursion.
#7Nursing care Plan
Assessment Diagnosis Planning Intervention Rationale Evaluation
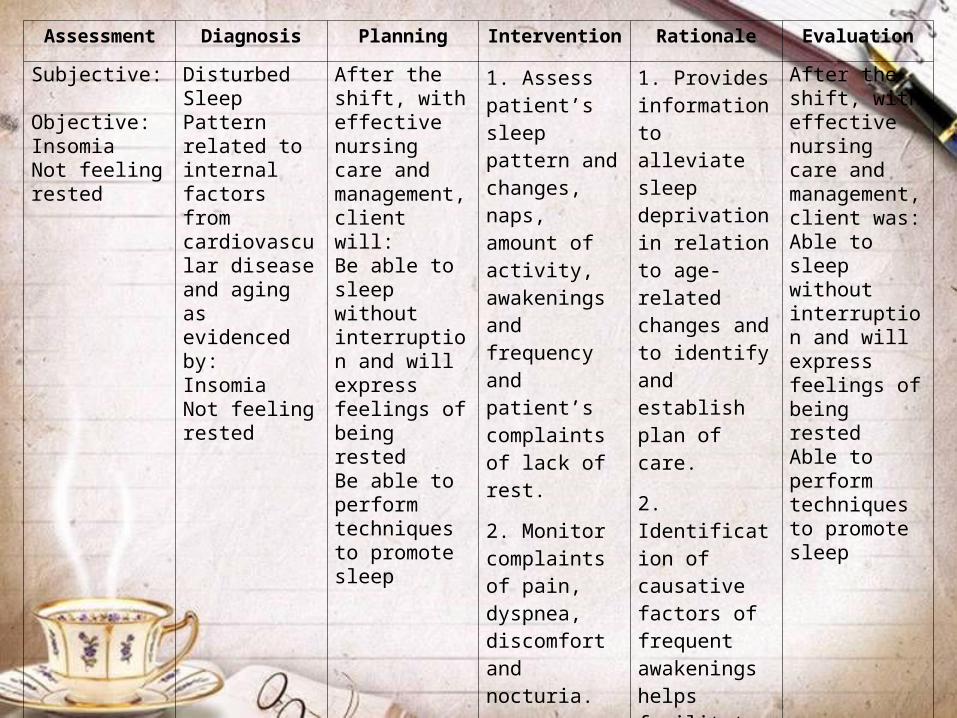
Subjective: Objective:Insomia Not feeling rested
Disturbed Sleep Pattern related to internal factors from cardiovascular disease and aging as evidenced by:Insomia Not feeling rested
After the shift, with effective nursing care and management, client will:Be able to sleep without interruption and will express feelings of being restedBe able to perform techniques to promote sleep
1. Assess patient’s sleep pattern and changes, naps, amount of activity, awakenings and frequency and patient’s complaints of lack of rest.
2. Monitor complaints of pain, dyspnea, discomfort and nocturia.
1. Provides information to alleviate sleep deprivation in relation to age-related changes and to identify and establish plan of care.
2. Identification of causative factors of frequent awakenings helps facilitate changes in sleep pattern.
After the shift, with effective nursing care and management, client was:Able to sleep without interruption and will express feelings of being restedAble to perform techniques to promote sleep

Assessment Diagnosis Planning Intervention Rationale Evaluation
3. Provide calm, quiet environment, closing curtains, adjusting lighting and so forth.
4. Provide warm drinks, extra cover, and warm bath prior to bedtime and so forth.
3. Helps to promote conducive atmosphere for restful sleep. External stimulus may interfere with going to sleep and increase awakenings in the elderly patient because sleep is usually of less intensity.
Assessment Diagnosis Planning Intervention Rationale Evaluation
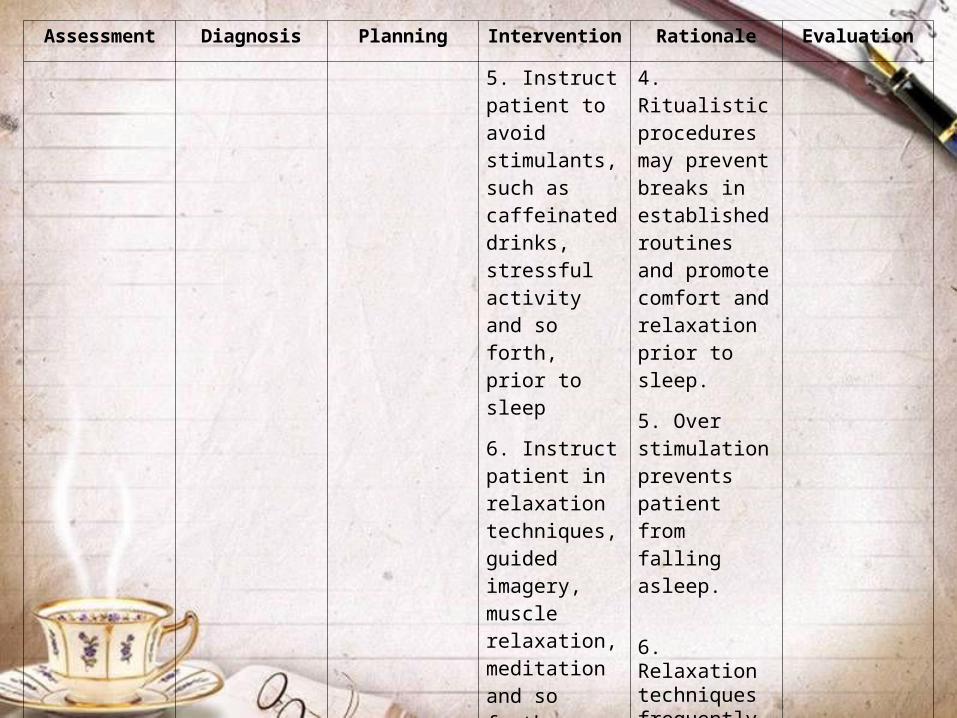
5. Instruct patient to avoid stimulants, such as caffeinated drinks, stressful activity and so forth, prior to sleep
6. Instruct patient in relaxation techniques, guided imagery, muscle relaxation, meditation and so forth.
4. Ritualistic procedures may prevent breaks in established routines and promote comfort and relaxation prior to sleep.
5. Over stimulation prevents patient from falling asleep.
6. Relaxation techniques frequently help promote sleep
Assessment Diagnosis Planning Intervention Rationale Evaluation
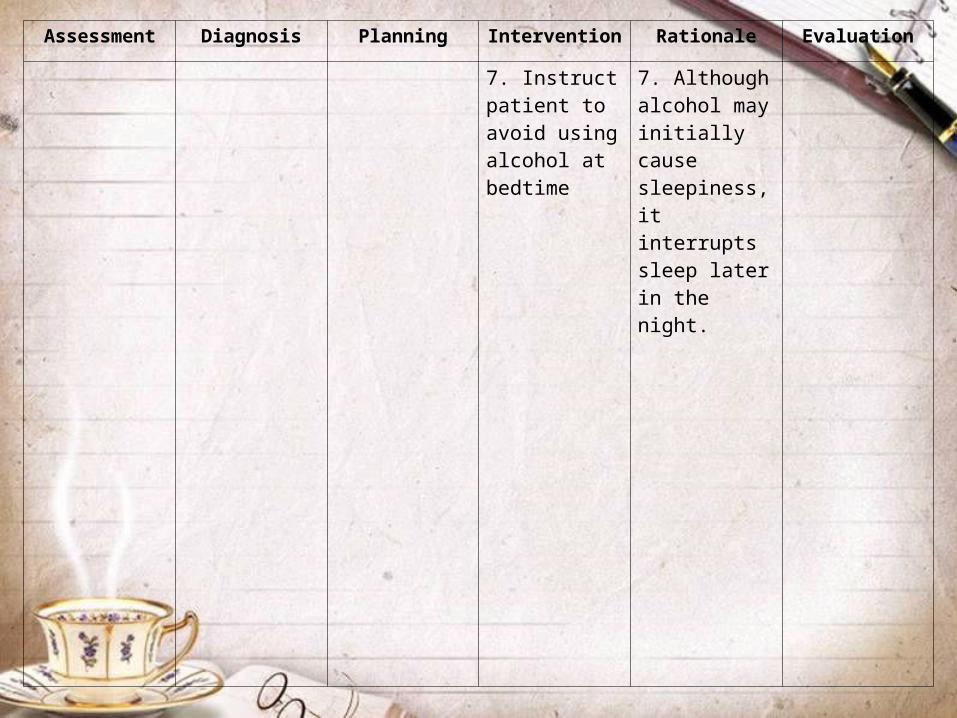
7. Instruct patient to avoid using alcohol at bedtime
7. Although alcohol may initially cause sleepiness, it interrupts sleep later in the night.
DISCHARGE PLAN
(METHOD)
Medications:
• Advise patient to take the prescribed medications continuously at home
• Always check the expiration date of the medicine before taking

Environment:
• Avoid crowded areas, especially during cold and flu season.
• Avoid close contact with anyone who is ill.• Provide safety measure to promote safe
environment and individual safety.• Sanitary handling of food and water.

Treatment:
• Eating a healthy diet (eating more fruits, vegetables, and low fat dairy products, less saturated and total fat).
• Reducing the amount of sodium in your diet to 2,300 milligrams (about 1 teaspoon of salt) a day or less.

• Getting regular aerobic exercise (such as brisk walking at least 30 minutes a day, several days a week).
• In addition to lowering blood pressure, these measures enhance the effectiveness of high blood pressure drugs.
Health Teachings• Teach the patient to use a self-monitoring
blood pressure cuff and to record the reading at least twice a week.
• Tell the patient to take his blood pressure at the same hour each time, with out more than usually activity preceding the measurement.
• Tell the patient and family to keep a record of drugs used in the past.

• To encourage compliance with antihypertensive therapy, suggest establishing a daily routine for taking medication. Warn the patient that uncontrolled hypertension may cause stroke and heart attack. Tell him to report any adverse reactions to prescribed drugs. Advise him to avoid high-sodium antacids and over-the-counter cold and sinus medications containing harmful vasoconstrictors.
• Help the patient examine and modify his lifestyle behavior.
• Suggest stress-reduction groups, dietary changes, and an exercise program.
• Encourage a change in dietary habits. Help the obese patient plan a reducing diet.
• Tell to the patients to avoid high-sodium foods, table salt, and foods high in cholesterol and saturated fat.
• Encourage a change in dietary habits. Help the obese patient plan a reducing diet.
• Tell to the patients to avoid high-sodium foods, table salt, and foods high in cholesterol and saturated fat.
Diet
• Reduction of sodium intake • Moderation of alcohol• Weight loss in the obese• Possibly increasing potassium and calcium
intake• Ingestion of a vegetarian diet or fish oil
supplements.

BIBLIOGRAPHY• Book• Smeltzer, Suzanne C., et. al. Brunner &
Suddarth’s Textbook of Medical-Surgical Nursing. 11th Edition. Volume 1 and 2. Lippincott Williams and Wilkins. © 2008.
• Nurse’s Pocket Guide. 11th Edition• Davis’ Drug Guide. 10th Edition

















