33
Case Study: Prader-Willi Syndrome Mujan Noroozian UTMB Dietetic Intern http://hmg.oxfordjournals.org/content/19/7.
| Date post: | 14-Aug-2015 |
| Category: |
Documents |
| Upload: | mujan-noroozian |
| View: | 142 times |
| Download: | 0 times |

Case Study: Prader-Willi SyndromeMujan Noroozian
UTMB Dietetic Intern
http://hmg.oxfordjournals.org/content/19/7.cover-expansion

Overview
At the end of this presentation, you will be able to
• Define Prader-Willi Syndrome and identify causes and the different behaviors that are associated with patients of PWS.
• Recognize the complex management of PWS and the nutritional care that is needed to help support patients.

Patient Background
• K.P. is a 20 month old African-American male
• Born at 37 5/7 weeks
• Birth Wt: 2.56 kg (5 lbs. 10 oz.)
• Birth Ht: 51 cm
• Pregnancy complicated by IUGR (34 weeks gestation size at delivery)
• APGAR• 1 minute—7• 5 minute—8
• Diagnosed with Prader-Willi Syndrome: hypotonia and feeding difficulties noted since birth
• Tube feeding—DOL #2

Diagnosis & Genetics
http://www.aafp.org/afp/2005/0901/p827.html
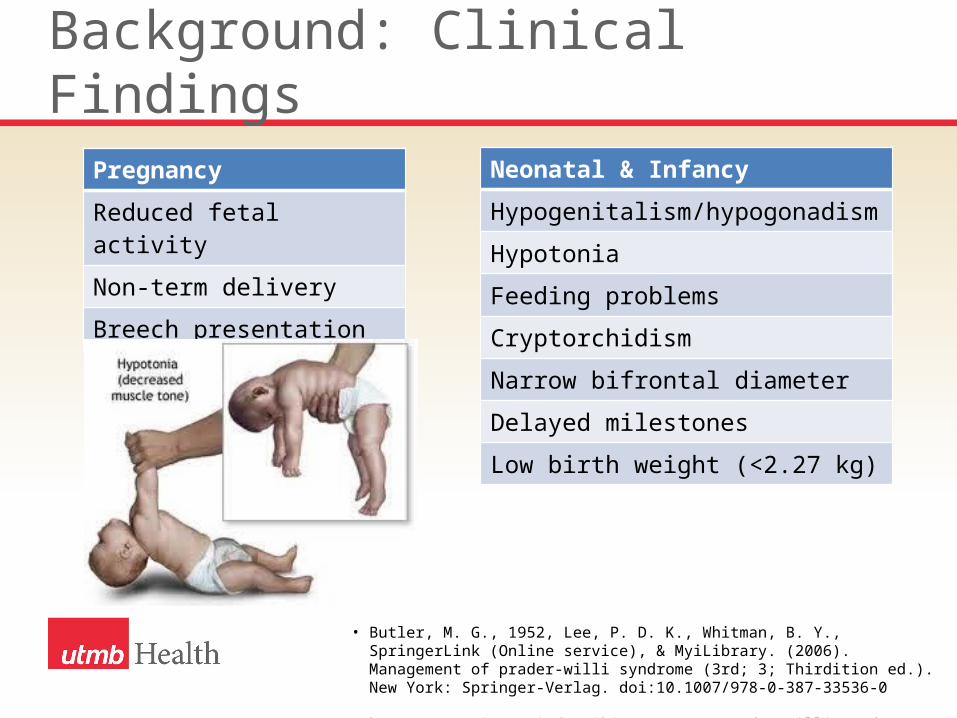
Background: Clinical Findings
Pregnancy
Reduced fetal activity
Non-term delivery
Breech presentation
Neonatal & Infancy
Hypogenitalism/hypogonadism
Hypotonia
Feeding problems
Cryptorchidism
Narrow bifrontal diameter
Delayed milestones
Low birth weight (<2.27 kg)
• Butler, M. G., 1952, Lee, P. D. K., Whitman, B. Y., SpringerLink (Online service), & MyiLibrary. (2006). Management of prader-willi syndrome (3rd; 3; Thirdition ed.). New York: Springer-Verlag. doi:10.1007/978-0-387-33536-0
• http://geneticsperiod4.wikispaces.com/Prader-Willi+Syndrome

Background: Clinical FindingsAdolescence & Adulthood
Menstruation
Seizures
Diabetes/reduced glucose tolerance
Childhood
Obesity
Small hands/feet
Skin picking
Mental deficiency & personality problems
Short stature
Scoliosis & delayed bone age
Early cavities & enamel hypoplasia
Strabismus
Almond shaped eyes
• Butler, M. G., 1952, Lee, P. D. K., Whitman, B. Y., SpringerLink (Online service), & MyiLibrary. (2006). Management of prader-willi syndrome (3rd; 3; Thirdition ed.). New York: Springer-Verlag. doi:10.1007/978-0-387-33536-0
• http://geneticsperiod4.wikispaces.com/Prader-Willi+Syndrome

Management
Current treatment is based on treating symptoms
• Genetic counseling
• Routine pediatric examinations by primary physician and Prader-Willi specialist
• Dietary evaluations/counseling by Dietitian
• Physical therapy evaluation (developmental, neuromuscular)
• Psychological evaluations and counseling
• Educational evaluations and recommendations
• Growth hormone therapy by Endocrinologist
Eiholzer, U., & Whitman, B. Y. (2004). A comprehensive team approach to the management of patients with prader-willi syndrome. Journal of Pediatric Endocrinology & Metabolism : JPEM, 17(9), 1153.

Background: How Nutritional Status is Assessed
Phase 0 Decreased fetal movements and lower birth weight• Full-term birth weight and BMI are about 15–20% less than the siblings• Typically normal gestational age• 85% have decreased fetal movements
Phase 1a Hypotonia with difficulty feeding (0–9 months)• Weak, uncoordinated suck. Usually cannot breastfeed• Needs assistance with feeding either through feeding tubes (nasal/oral gastric tube or
gastrostomy tube) or orally with special, widened nipples. Many would die without assisted feeding
• Oral feeds are very slow• Severely decreased appetite. Shows little or no evidence of being hungry• Does not cry for food or get excited at feeding time• If feeding just occurred when baby “acted hungry” then would have severe “failure-
to-thrive”• Weak cry
Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951

Background: How Nutritional Status is Assessed
Phase 1b No difficulty feeding and growing appropriately on growth curve (9–25 months)
• No longer needs assisted feeding• Growing steadily along growth curve with normal feeding• Normal appetite
Phase 2a Weight increasing without an increase in appetite or excessive calories (2.1–4.5 years)
• Infant starts crossing growth curve centile lines• No increase in appetite• Appetite appropriate for age• Will become obese if given the recommended daily allowance (RDA) for calories or if
eating a “typical” toddler diet of 70% carbohydrates• Typically needs to be restricted to 60–80% of RDA to prevent obesity
Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951
Background: How Nutritional Status is Assessed
Phase 2b Weight increasing with an increase in appetite (4.5–8 years)• Increased interest in food. Frequently asking “food related” questions• Preoccupied with food. Very concerned about the next meal/snack (e.g., “Did you
remember to pack my lunch?”)• Increased appetite• Will eat more food than a typical child if allowed• Will eat food within their line of sight if unattended• Will become obese if allowed to eat what they want• Can be fairly easily redirected about food• Can feel full• Will stop eating voluntarily
Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951

Background: How Nutritional Status is Assessed
Phase 3 Hyperphagic, rarely feels full (8 years adulthood)• Constantly thinking about food• While eating one meal they are already thinking about the next meal• Will awaken from sleep early thinking about food• Will continue eating if portion size is not limited• Rarely (truly) feels full• Will steal food or money to pay for food• Can eat food from garbage and other unsavory/inedible sources (e.g., dog food,
frozen food, crayons, etc.)• Typically are not truthful about what they have eaten (i.e. amount and types of food)
• Will gain considerable amount of weight over a short period of time if not supervised (e.g., some individuals are known to have gained up to 20 pounds in one weekend)
• Food typically needs to be locked up. Frequently the child will ask the parent to lock the food if the parent has forgotten
• Will break into neighbors’ houses for food• Temper tantrums and “meltdowns” frequently related to food• Needs to be placed on a diet that is approximately 50–70% of the RDA to maintain a
healthy weight
Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951

Background: How Nutritional Status is Assessed
Phase 4 Appetite is no longer insatiable (adulthood)• Appetite may still be increased or may be normal or less than normal• Previously in phase 3, but now a noticeable improvement in their appetite
control• Can feel full• Appetite can fluctuate in this phase, but the key component is noticeable
improvement in control of appetite compared to when they were younger
• Not as preoccupied with food• Absence of major temper tantrums and “meltdowns” related to food• Onset in adulthood. Could be as early as 20s or as late as 40–50s• Most adults have not gone into this phase and maybe some (most?) never
will
Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951

Anthropometric Assessment
• Wt: 16.3 kg (99.92%ile)• Ht: 85.3 cm (60.63%ile)• Wt/Ht: 100%ile• IBW: 11.6 kg (140% IBW)

Growth Chart: Weight/Age

Growth Chart: Height/Age

Growth Chart: Weight/Height

Physical Assessment
Physical Appearance• Hypo-pigmented compared to parents• Almond shaped eyes• Small hands/feet• No significant rashes• No appearance of scoliosis• No strabismus or anicteric sclera• Abdomen-soft, non-tender without masses or hepatosplenomegaly

Developmental Milestones
2 months age appropriate:
• Social smile=Yes
4 months age appropriate:
• Lifts head off ground when lying prone=Yes
• Lifts head to 45° off ground when lying prone=Yes
• Lifts head to 90° off ground when lying prone=No
• Laughs out loud without being tickled/touched=Yes
• Plays with hands by touching them together=Yes
6 months age appropriate:
• Can keep head from lagging when pulled from supine to sitting=Yes
12 months age appropriate:
• Makes ‘mama’/’dada’ sounds=Yes
• Can go from sitting to standing without help=No
• Uses ‘pincer grasp’ between thumb and fingers to pick up small objects=Yes

Developmental Milestones
15 months age appropriate:
• Can play ‘pat-a-cake’ or wave ‘bye-bye’ without help=Yes
18 months age appropriate:
• Can drink from a regular cup (not one with a spout without spilling)=Yes
3 years age appropriate:
• Adequately follows instructions: ‘put the paper on the floor; put the paper on the chair; give the paper to me=Yes

Biochemistry Assessment
10/8/2013 10/9/2013 5/14/2014
BUN 12 13 7 (L)
10/9/2013
Ammonia 13 (L)
10/10/2013
Cystine 60 (H)
10/10/2013
Tyrosine 109 (H)

Previous Nutritional Needs
Energy Needs 10/9/2013 12/5/2013 1/6/2014
Total Energy Estimated Needs
Enteral: 100-130 kcal/kg/day
120-130 kcal/kg/day 175 kcal/kg/day
Method Baylor College of Medicine Guideline
Catch-up growth Current intakes + 20%
Total Protein Estimated Needs
Enteral: 1.5-3 g/kg/day
1.8 g/kg/day 1.9 g/kg/day
Method Baylor College of Medicine Guideline
DRI + catch-up DRI + catch-up
Total Fluid Estimated Needs
100 mL/kg/day 100 mL/kg/day
Method Holliday-Segar Holliday-Segar
Texas Children’s Hospital, Pediatric Nutrition Reference Guide, 10th ed. Houston, TX: McGraw-Hill Professional; 2013.

Nutrition Assessment
Previous diet
• At birth: EBM• At 2 months: Similiac Advanced (20 kcal/oz) 2 oz. Q3H via NG
• At 3-6 months: Similac Advance (25 kcal/oz) 3 oz. 8x/day
• At 9 months: Similac Advance 5-8 oz. Q3-4H + Solid Food (cereal, fruits/vegetables)

Nutrition Assessment
Current Nutrition needs• Energy: 988 kcals/day (Based on DRI/age-82 kcals/kg/day)• Protein: 13 g/day (Based on DRI/age-1.08 g/kg/day)
Current Diet: Table foods appropriate for toddlers
Current Intake• 2-3 cups of silk almond milk daily• 3-5 cups of juice daily• Oatmeal & fruit for breakfast• Table food throughout the day
Texas Children’s Hospital, Pediatric Nutrition Reference Guide, 10th ed. Houston, TX: McGraw-Hill Professional; 2013.

Medications
• Montelukast (Singulair) chew tab 4 mg: Asthma treatment
• Cetirizine PO syrup 5mg/5mL: Antihistamine
• Albuterol 90 mcg/puff: Asthma treatment/breathing problems
• Somatropin (Genotropin) subcutaneous injection: Growth hormone
• Multivitamin with iron (Poly-vi-sol drop)

Nutrition Diagnosis
Excessive (nutrient) energy intake related to altered metabolism as evidenced by diagnosis of PWS and BMI >95%.

Nutrition Intervention
• Avoid sugary beverages-provide sugar free beverages such as water, soy milk (milk allergy)…
• Provide age appropriate portion sizes for 2 year old.
• Provide regularly scheduled meals daily.
• Obtain measurements (height and weight) every 3 months at visit to assess growth.

Goals of Nutrition Intervention
• Age appropriate weight gain and linear growth
• Weight: 4-9 g/day (typical in most children)• Comprehension of nutrition education: family members.
• Adherence to nutrition recommendations: family members.

Monitoring & Evaluation Plan
• Growth velocity/weight trends
• Compliance with nutrition recommendations
• Monitor labs

Journal Article Review
Sample
• 106 families who had someone in the family with genetically confirmed PWS, participated in study
• 47 pts <10 years of age—Had obstetric & ultrasound reports available.
• 59 pts 10-36 years of age-Mother’s interviewed orally with pre-determined questionnaire.
Methods & Analysis
• Clinical & ultrasound characteristics examined.
• SGA, asymmetrical intrauterine growth, polyhydramnios, breech presentation, decreased fetal movement.
Gross, N., Rabinowitz, R., Gross Tsur, V., Hirsch, H. J., & Eldar Geva, T. (2015). Prader–‐ ‐Willi syndrome can be diagnosed prenatally. American Journal of Medical Genetics Part A, 167(1), 80-85. doi:10.1002/ajmg.a.36812

Journal Article Review
Results
• Combination of asymmetric intrauterine growth in either fetuses with normal growth or SGA, along with polyhydramnios—found in 1/3 of PWS pregnancies.
• The combination of abnormal criteria, alerts obstetricians to the possibility of PWS and indicates need for additional testing by methylation test.
Gross, N., Rabinowitz, R., Gross Tsur, V., Hirsch, H. J., & Eldar Geva, T. (2015). Prader–‐ ‐Willi syndrome can be diagnosed prenatally. American Journal of Medical Genetics Part A, 167(1), 80-85. doi:10.1002/ajmg.a.36812

Summary & Conclusion
Complex physical & behavioral manifestations
• Best to manage in a multidisciplinary setting with a team.
References
• Butler, M. G., 1952, Lee, P. D. K., Whitman, B. Y., SpringerLink (Online service), & MyiLibrary. (2006). Management of prader-willi syndrome (3rd; 3; Thirdition ed.). New York: Springer-Verlag. doi:10.1007/978-0-387-33536-0
• Eiholzer, U., & Whitman, B. Y. (2004). A comprehensive team approach to the management of patients with prader-willi syndrome. Journal of Pediatric Endocrinology & Metabolism : JPEM, 17(9), 1153.
• Gross, N., Rabinowitz, R., Gross‐Tsur, V., Hirsch, H. J., & Eldar‐Geva, T. (2015). Prader–Willi syndrome can be diagnosed prenatally. American Journal of Medical Genetics Part A, 167(1), 80-85. doi:10.1002/ajmg.a.36812
• Miller, J. L., Lynn, C. H., Driscoll, D. C., Goldstone, A. P., Gold, J.-A., Kimonis, V., … Driscoll, D. J. (2011). Nutritional Phases in Prader–Willi Syndrome. American Journal of Medical Genetics. Part a, 155A(5), 1040–1049. doi:10.1002/ajmg.a.33951
• Texas Children’s Hospital, Pediatric Nutrition Reference Guide, 10th ed. Houston, TX: McGraw-Hill Professional; 2013.

QUESTIONS?

















