PARIMAL BHATTACHARY Death - M/V ¨IBRA LNG¨ _____ Accidents Investigator Panama Maritime Authority Directorate General of Merchant Marine Investigation of Wrecks and Maritime Accidents Department Panama, Republic of Panama Page 1 of 63 CASUALTY INVESTIGATION REPORT S.S. “IBRA LNG”
Transcript
PARIMAL BHATTACHARY Death - M/V ¨IBRA LNG¨ _____ Accidents Investigator
Panama Maritime Authority Directorate General of Merchant Marine
Investigation of Wrecks and Maritime Accidents Department Panama, Republic of Panama
Page 1 of 63
CASUALTY INVESTIGATION
REPORT
S.S. “IBRA LNG”
PARIMAL BHATTACHARY Death - M/V ¨IBRA LNG¨ _____ Accidents Investigator
Panama Maritime Authority Directorate General of Merchant Marine
Investigation of Wrecks and Maritime Accidents Department Panama, Republic of Panama
Page 2 of 63
INDEX
SL. NO. CONTENTS
PAGE NO.
1. SUMMARY 5
2. FORWARD 6
3. DESCRIPTION OF VESSEL 6
3.1 GENERAL DATA 7-8
3.2 MANNING 9
4. INCIDENT VOYAGE 9
4.1 SEQUENCE OF EVENTS 10-13
4.2 DEATH CERTIFICATE 14
4.3 OFFICIAL LOG BOOK ENTRY 15-17
5. ACTION TAKEN BY CREW 18
6. ACTION TAKEN BY COAST GUARD 19
6.1 POST MORTEM REPORT 19
6.1.1 INJURIES 20-21
6.1.2 OPINION AS TO CAUSE OF DEATH 22
6.2 DETAILS OF CASUALTY 22
7. INVESTIGATION 23
7.1 INVESTIGATION INITIATION 24
7.2 ELEVATOR DETAILS 24-25
7.3 LAY OUT OF ELEVATOR 26-28
7.4 PERIODIC MAINTENANCE 29-31
PARIMAL BHATTACHARY Death - M/V ¨IBRA LNG¨ _____ Accidents Investigator
Panama Maritime Authority Directorate General of Merchant Marine
Investigation of Wrecks and Maritime Accidents Department Panama, Republic of Panama
Page 3 of 63
8. FLEET NOTICE 32
8.1 SAFETY SYSTEM OF CAGE AND DOOR 32-33
8.2 SAFETY IN ELEVATOR HOIST WAY 33
8.3 SAFETY IN MACHINE ROOM 34-35
8.4 SAFETY DURING MAINTENANCE 35
8.5 PREPARATION FOR MAINTENANCE/INSPECTION PROCEDU 35-36
8.6 POINTS TO CONSIDER DURING MAINTENANCE 37-38
8.7 CONFIRMATION OF WORK COMPLETION 39
9. COMPANY’S PROCEDURE 39
9.1 FAMILARISATION 39
9.2 IBRA LNG ELEVATOR 40
9.3 MAINTENANCE AS PLANNED 40
10. INCIDENT INVESTIGATION 40-43
10.1 DATA GATHERING 43
10.1.1 PEOPLE 43-53
10.1.2 ENVIRONMENT 54
10.1.3 THE EQUIPMENT 54-55
10.1.4 PROCEDURE 55
10.1.5 THE ORGANISATIONAL FACTOR 56
11. APPARENT CAUSE ANALYSIS 57-60
12. CONCLUSION 60-61
13. RECAPITULATION 61-62
PARIMAL BHATTACHARY Death - M/V ¨IBRA LNG¨ _____ Accidents Investigator
Panama Maritime Authority Directorate General of Merchant Marine
Investigation of Wrecks and Maritime Accidents Department Panama, Republic of Panama
1858 Hrs : Casualty disembarked by crane into Fishing Boat “Olympia”
1940 Hrs : Coast Guard informed vessel to await at anchor till further
notice whilst also confirming the casualty as deceased.
4.2 DEATH CERTIFICATE
Death Certificate signed by the Master gives following details :
(a) Date of death : 03RD FEBRUARY 2007.
(b) Place of death : 080° 21’ N 076° 57’ E
(c) Name : IOAN CUMPAT
(d) Sex : MALE
(e) Date of Birth : 17 MAY 1958
(f) Occupation : ELECTRICIAN
(g) Domicile at : ROMANIA
(h) Time of death : 1755 Hrs L.T. / S.M.T.
(i) Passport No. : I 1669423
Page 15 of 63
4.3 OFFICIAL LOG BOOK ENTRY
Official Log Book Entry of the incident is reproduced below :
Page 16 of 63
Page 17 of 63
Page 18 of 63
5. ACTION TAKEN BY CREW
When the crew learnt about Mr. Ioan Cumpat getting trapped in the elevator, they
made an attempt to open the elevator door from ’B’ deck, which took nearly 4 to 5
minutes to open. After opening the door, the crew learnt the position of Mr. Ioan
Cumpat, who was trapped in an inverted position. Considering the risk involved in
making an attempt to remove the casualty with the help of the elevator. Mr. Ioan
Cumpat, was tied to a safety harness and heaved-up, and finally was brought to
the ship’s hospital. He was continuously given cardiac massage and artificial
respiration. As the condition of Mr. Ioan Cumpat, with open wounds and
multiple injuries, was considered critical, the Master informed the Owners and also
the Indian Coast Guard requesting immediate medical attention. The vessel was
diverted to off the South Indian Coast, as advised by the Owners and the Coast
Guard. The position from where the vessel was diverted is shown in the chart
below.
Page 19 of 63
As the vessel was moving towards the position instructed by the Coast Guard, the
casualty finally died. The time of his death was 1755 hrs L.T., the vessel’s position
at that time was 080 21’ N, 0760 57’ E. The death certificate issued by the Master
recorded the time as 1755 hrs. L.T. / S.M.T.. At 1858 hrs L.T., the mortal remains
of Mr. Ioan Cumpat was finally handed over to the Indian Coast Guard.
6. ACTION TAKEN BY COAST GUARD
After taking the dead body in the custody of the Coast Guard, the Deputy
Commandant, Mr. Deepak Singh, filed a First Information Report ( F.I.R. )
with Vizhinjam Police Station for the necessary action. Subsequently, the body of
Mr. Ioan Cumpat was sent for post-mortem and the findings of the post-mortem
report had been handed over to the vessel.
6.1 POST MORTEM REPORT
P.M. No. 284/07 Date
: 04.02.07
I, Dr. C. S. Sreedevi, Asst. Professor of Forensic Medicine, certify as hereunder:-
Dead body of a male by name IONA CUMPAT, aged about 49 years, was sent
by Sub Inspector of Police, Vizhinjam Police Station, with a requisition dated 04th
February 2007 through the H.C. No.7633, for conducting postmortem
examination and report.
The body was in-charge-of the H.C. No.7633, who identified it as that of the
deceased in Crime No. 52/07 of Vizhinjim Police Station. The post-mortem
Page 20 of 63
commenced at 2.30 p.m. L.T. on 04th February 2007 and was concluded at 3.30
p.m. L.T. / I.S.T. The following findings were observed.
Body was that of a well built and nourished fair skinned adult male of height 170
cm and weight 94 kg. Eyes were closed. Conjunctivae congested. Pupils dilated.
Blood stained fluid present at nostrils. Other external body orifices were normal.
Finger nails were blue. Old scar 25 x 2 cms, vertical, on the abdomen in the
middle. 5 cm below the lower end of breast bone.
Corneae clear. Rigor mortis fully established and retained all over the body. Post-
mortem staining at the back and sides of body, not fixed. No sign of
decomposition ( Body was kept in the cold chamber ).
6.1.1 INJURIES (ANTEMORTEM) :
1. Contusion of scalp 9 x 5 x 0.5 cms on the left side of head just above the
ear.
2. Abrasion 1.8 x 0.2 cms on right side of chin 6 cm outer to midline. Brain
showed subdural and subarachnoid haemorrhage. Sulci were narrowed and
gyri flattened.
3. Lacerated wound 5.5 x 4 cms enterining into the abdominal cavity of the
perineum just behind the scrotum. Fracture separation of pubic symphasis.
The soft tissues around were seen infiltrated with blood.
4. Multiple small abrasions over an area 22 x 2 to 7 cms on the front aspect of
right arm 7 cms below the shoulder tip with fracture of humerus underneath.
5. Abrasion 9 x 1.5 to 3 cms on the back of right forearm 13 cms above wrist.
Page 21 of 63
6. Abrasion 1 x 0.3 cms on the back of the right wrist.
7. Abrasion 1 x 0.3 cms on the outer aspect of right forearm 4 cms above
wrist.
8. Abraded contusion 7 x 4.5 x 1 cms on the inner aspect of the right arm 7
cms above elbow with an abrasion ( 6 x 4 cms ).
9. Multiple small abrasions over an area of 4 x 3.5 cms on the back of right
elbow.
10. Abraded contusion 18 x 7 x 2 cms involving the inguinal area and adjacent
part of front of thigh.
11. Abrasion 6 x 4 cms on the inner aspect of right thigh 20 cms above knee.
12. Abrasion 8 x 4 cms on the back and inner aspect of right knee and adjacent
part of thigh.
13. Lacerated wound 5 x 1 x 0.4 cms on the front of right knee with multiple
small abrasions over an area 30 x 7 cms around and adjacent parts of front
of thigh and leg.
14. Multiple abrasions over an area 30 x 13 cms on the inner aspect of left thigh
and knee.
15. Abrasion 7 x 0.5 cms on the front aspect of left thigh 32 cms above knee.
16. Abrasion 4 x 2 cms on the left groin.
17. Multiple abrasions over an area 30 x 3 to 8 cms on the left side of front of
chest its upper outer and just below the front fola of armpit.
18. Abrasion 29 x 6 to 12 cms on the right armpit and adjacent part of left side
of chest.
Page 22 of 63
Air passage contained blood stained fluid. Lungs were congested and
oedematous. Liver was fatty. Stomach was full with starchy food materials and
other unidentifiable food materials having no unusual smell, mucosa normal.
Urinary bladder was empty.
All other internal organs were pale, otherwise appeared normal.
Sample of blood was preserved and sent for chemical analysis
6.1.2 OPINION AS TO CAUSE OF DEATH:
Death was due to injuries sustained to head and pelvis.
6.2 DETAILS OF CASUALTY
Name : Mr. Ioan Cumpat.
Rank : Electrician.
Date of Birth : 17th May 1958.
Manning Agency : AZA LEA MARITIME B.V.
Years in Rank : More than 20 years.
Date of Joining vessel : 23rd January 2007.
Page 23 of 63
Hours worked on previous day : 8 hours.
Hours worked on the day of
accident
: 5.5 hours.
Nature of work : In charge of maintenance & operation
of all electrical installations on board
including personnel elevator.
Passport No. : I 1669423
7. INVESTIGATION
The investigation was carried out on board the vessel on 5th & 6th March 2007 at
whilst she lay safely anchored at Fujairah Anchorage, Fujairah Port, U.A.E.. It was
carried out as per American Bureau of Shipping incident investigation methodology
MARCAT guidelines and also as MINICAM guide. The objective of the
investigation is to conduct RCA of the loss of human life on board and to determine
whether the loss was related to safety environment or human element. However, in
this particular event, which resulted in the death of an officer on board, RCA was
not possible as nobody was witness to the incident. Therefore, the analysis is
based on ACA technique as the various available data related to the incident were
viewed after more than a month of the actual date of occurrence.
Page 24 of 63
7.1 INVESTIGATION INITIATION
The vessel SS “IBRA LNG” is fitted with one set of electric motor driven counter
weight type personal elevator capable of moving in an enclosed steel trunk from
engine room floor below Navigation deck.
As the incident of death occurred during the discharge of routine maintenance
work of the Elevator, it is essential to take a closer look at the design specification
of the Elevator and its maintenance requirement.
7.2 ELEVATOR DETAILS
TYPE OF ELEVATOR CREW ELEVATOR
CAPACITY 500 KG (6 PERSONS)
SPEED 45M/MIN
DRIVE VVVF
TYPE OF CONTROL 2 BC (SELECTIVE COLLECTIVE CONTROL
SYSTEM)
TRAVELLING HEIGHT 33900
CAR INTERNAL SIZE 950 (W) X 1300 (D) X 2100 (H)
NO. OF SERVICE 9 STOPS (MAIN, 4TH, 3RD, 2ND, UPP, A, B. C. D
DK)
CLEARANCE OF DOOR 800(W) X 1200(H)
DOOR OPERATION 1 SPEED CENTER OPENING DOOR (ISCO)
Page 25 of 63
LANDING DOOR (E/R) GAS TIGHT SWING DOOR WITH A-60
INSULATION
LANDING DOOR (ACCOM) 1 SPEED CENTER OPENING DOOR WITH A-0
INSULATION
TRACTION MACHINE TM 400
DIA OF MAIN SHEAVE O 570
MAIN ROPE O 12 X 4 (1:1 ROPING)
CAR RAIL 13K RAIL
CWT RAIL 8K RAIL
MOTOR CAPACITY 5.5 KW
POWER SUPPLY MAIN 3 PH 440 V 60 HZ
LIGHT 1 PH 220 V 60 HZ
PAINTING COLOUR CAR INSIDE & DOOR STAINLESS HAIRLINE
FINISH CAR CEILING STAINLESS HAIRLINE
FINISH LANDING DOOR MAIN - 2ND DK
MUNSELL NO. 2.5 Y 9/2 UPP-D DK
STAINLESS AIRLINE ELECTRIC EQUIPMENT
MUNSELL NO. 7.5 BG 7/2.
FLOORING LUCKSTRONG ( TYPE : RS-90028 )
RULES & REGULATIONS AMERICAN BUREAU OF SHIPPING (ABS)
Page 26 of 63
7.3 LAYOUT OF ELEVATOR
Page 27 of 63
Page 28 of 63
Page 29 of 63
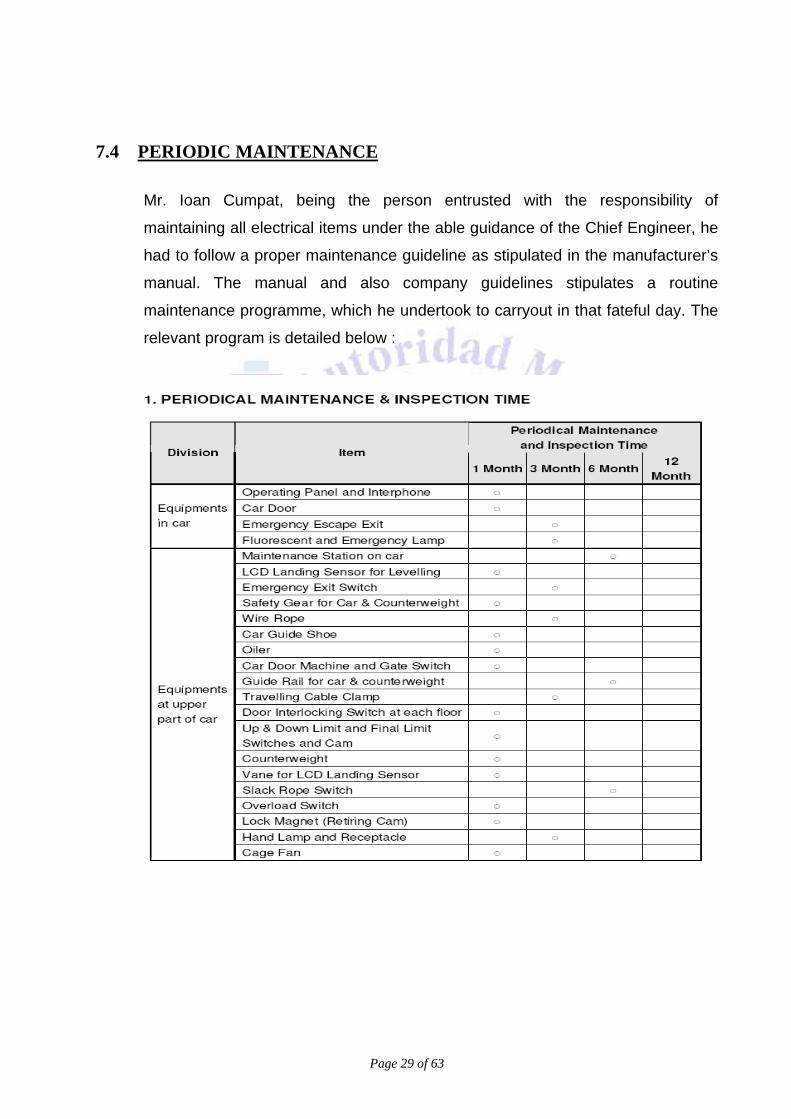
7.4 PERIODIC MAINTENANCE
Mr. Ioan Cumpat, being the person entrusted with the responsibility of
maintaining all electrical items under the able guidance of the Chief Engineer, he
had to follow a proper maintenance guideline as stipulated in the manufacturer’s
manual. The manual and also company guidelines stipulates a routine
maintenance programme, which he undertook to carryout in that fateful day. The
relevant program is detailed below :
Page 30 of 63
Page 31 of 63
Page 32 of 63
8. FLEET NOTICE
The Owners M/s Oman Ship Management Co. Ltd., Oman, by their Fleet Notice
OSMC–06–01 dated : 27th March 2006, which was subsequently updated on 17th
February 2007, specifies that basic safety measures should be taken during
maintenance & inspection of Elevators as per “Marine Elevator” handling
guidelines. The guidelines are given below :
Marine elevators tend to be regarded as ‘simple and convenient machines’ by
those who use them, but they are actually a combination of several dozen different
pieces of equipment and devices. Mishandling and wrongful maintenance /
inspection of any one of these components can lead to not only damage to the
equipment itself, but also accidents causing injury or death.
All crew members are expected to understand some of the basic structures and
operations, and to be able to take appropriate responses during an emergency.
In general, rope-type elevators are used for marine elevators.
Elevator performs as a type of “well bucket”, with a “cage” to contain the
passengers / load on one side of the pulley, and a counterweight on the other side
to raise or lower the cage with the minimum of power.
8.1 SAFETY SYSTEM OF THE CAGE AND DOOR
The part of the elevator which holds people or cargo is called a “cage”. The
size of the cage decides its capacity, or the maximum number of persons it
can hold, with one person calculated as 65 kg.
Generally, an elevator is equipped with the following safety systems ( though
they may vary by manufacturer or type ) :
Page 33 of 63
a. Gate switch : a type of safety switch that becomes operable once the door of
the cage is completely shut.
b. Door switch : a type of safety switches that becomes operable once the
hoistway door on each floor is completely shut.
c. Emergency switch : the switch used to stop the elevator when there is an
emergency in the cage.
d. Safety edge of door : a device to open the door automatically when
passenger(s) or cargo get caught in the door of the cage.
e. Emergency bell and telephone : used to communicate with the outside in the
case of an emergency.
f. Emergency light : a lighting apparatus which receives electricity from a battery
and illuminates in the event of a blackout.
g. Safety switch : blackout / operating switch used for maintenance, provided on
cage top.
h. Door locking device : once the hoistway door closes, this device prevents the
door being manually opened.
8.2 SAFETY IN ELEVATOR HOISTWAY
Safety to be implemented in Elevator Hoistway involving :
1. Termination switch
2. Overrun limit switch
3. Buffer
Page 34 of 63
8.3 SAFETY IN MACHINE ROOM Safety system to be implemented in Machine Room involving the following :
a. Electromagnetic brake : also known as an “eddy-current braking”, this type of
brake utilizes the braking torque between the electric current and magnetic
field generated when the magnet and metal plates on both ends of the poles
are in motion; that is, the brake moves with the friction from the
electromagnetic power. When the overrun limit switch or emergency switch is
activated, the cage is brought to a sudden stop, and the brake keeps the cage
in that position. In general, the brake works as follows:
1 The buttons in the cage operating panel or on the floor are pressed to operate
the elevator.
2. Electricity is supplied to the motor.
3. Auxiliary contact on the main relay of the control panel turns ON.
4. Electricity is supplied to the coil attached to the top of the brake device, and
the core is activated.
5. The link mechanism sets the brake shoe apart from the brake drum, and the
brake opens.
In this way, the elevator starts to move. When the cage arrives at its
destination, electricity is supplied to the motor, the coil is cut-off, and the
spring located at the bottom of the brake device thrusts the brake shoe
toward the brake drum. The friction at the brake lining stops the elevator
cage.
Page 35 of 63
b. Speed regulator : also known as the governor, this device utilizes centrifugal
force to adjust the spinning body so that a constant rotary speed can be
maintained regardless of the shift in the load applied to the revolving
machine. The speed regulator is activated not only when the overrun limit
switch or other safety system is turned on, but also when the speed of the
elevator exceeds the rated speed. At the first motion, the speed regulator cuts
off the electric circuit to the motor when the speed reduction is below 130%,
and activates the electromagnetic brake to stop the cage. If the cage does not
stop and speed reduction approaches 140%, then the speed regulator grabs
the speed regulator rope to bring the cage to an emergency halt.
8.4 SAFETY DURING MAINTENANCE
In order to maintain the safe operational status of the elevator, planned
maintenance and regular inspections are important, as is true of all engines
and equipment. When conducting routine maintenance and inspection work,
“Under inspection/ Do not use” announcements must be clearly
communicated to all other personnel, not just the maintenance workers. Close
communication between the maintenance workers must be kept, and relevant
equipment and devices be appropriately used at all times.
8.5 PREPARATION FOR MAINTENANCE / INSPECTION PROCEDURES
a. Before commencing these procedures, obtain all necessary permissions
from the Captain and the Chief Engineer.
b. Always hold a meeting, and confirm the following before starting work:
Page 36 of 63
1. Who will take part in the work and what is the role of each worker ( Note
: work should always be conducted by two or more workers ).
2. What should be worn, and what equipment is needed to carry out the
work ( work clothes, safety shoes, helmet, torch, transceiver, etc. )
3. Means of communication during the work ( in-cage telephone,
transceiver, etc. )
4. Special / general tools required for the work.
c. Clearly and comprehensively announce that the elevator is “Under
inspection - Do not use”
d. Put up a sign “Under inspection / Do not use” in front of the hoistway door
on each floor, and cover the “cage call button” with vinyl, duct, or other
suitable tape. To prevent the button from being accidentally pressed, a
plastic / wooden cover hung over the button on each floor can be effective.
e. Make sure that the emergency alarm and telephone are operational.
f. Personnel other than maintenance / inspection workers must not perform
any of the maintenance / inspection procedures.
g. Ensure that there is sufficient light in the work area.
Page 37 of 63
8.6 POINTS TO CONSIDER DURING MAINTENANCE
a. Perform the inspection procedures according to the checklist, and make notes
on any necessary information required.
b. Activate the emergency stop switch in the cage top operating panel so that
the cage cannot move, and make sure that all openings are closed.
c. Elevator machine room :
1. When conducting inspection/ adjustment of moving parts such as the hoist
or the deflector sheave, make sure that the power supply is turned off.
2. When checking the controller (insulation, resistance measurements, etc.),
make sure it is turned off.
3. Use the telephone in the elevator machine room to communicate with the
worker in the cage ( if vessel has a telephone equipped ). When
communicating with other parts of the vessel use the transceiver, and
keep in close contact with each other throughout the maintenance/
inspection procedures.
4. Take extra care not to spill oil / grease on the pulley of the hoist, defector
sheave, or wire rope. The presence of oil / grease can cause slippage of
the wire rope, which is extremely dangerous.
d. Top of the cage and hoistway :
1. Turn on the inspection light on the cage top, and ensure that there is
adequate lighting.
Page 38 of 63
2. Always keep the area tidy, and make sure that there is enough space to
put up a scaffold.
3. Once on the cage, turn the AUTO-MANUAL switch in the cage top
operating station to MANUAL.
4. While these procedures are being carried out, keep the emergency switch
in the cage top operating station active.
5. When moving the cage, or opening / closing the door manually, contact
the other workers to ensure that the surrounding area is secure ( beware
of the counterweight or projections in the hoistway ). When operating,
release the emergency stop and make sure that the worker knows what
buttons to press.
6. After finishing these procedures, contact the other workers to ensure that
the surrounding area is secure, and turn the AUTO-MANUAL switch in the
cage top operating station back to AUTO.
e. Bottom of the hoist way :
1. Turn off the control panel main switch in the elevator machine room.
2. When conducting counterweight - clearance measurements, bring the
cage to the top floor, press the emergency stop button in the cage, and
put up an “Under inspection / Do not use” sign.
3. Use the release key to open the lowermost door manually, and go down to
the bottom of the hoistway keeping the door open with a wedge or rope.
4. If the pit of the hoistway is stained with oil, wipe it clean to avoid slippage.
Page 39 of 63
8.7 CONFIRMATION OF WORK COMPLETION
a. Check the number of tools ( to ensure none have been left behind ).
b. Test elevator operation, and make sure that there are no abnormities.
c. Report to the captain and chief engineer that the procedures have been
completed, and let the personnel on the bridge know that the inspection is
finished. Make an in-vessel announcement, and then remove all plates
around the elevator doors on each floor and tapes covering the buttons.
9. COMPANY’S PROCEDURE
M/s Oman Shipping Co. maintains a familiarization programme for every officer
joining the vessel, as a standard procedure.
9.1 FAMILIARIZATION
As per the company’s familiarization programme and the ISM requirement, the
Electrician was required to familiarize himself as to the working of the Elevator and
its maintenance aspect. It was reported that having worked on a sister ship of the
company, Mr. Ioan Cumpat had adequate knowledge about the elevator
maintenance and its working principle.
However, he still had to carry out the familiarization of all electrical hardwares as
per the company procedure towards requirement of the ISM. It appears that Mr.
Ioan Cumpat had complied with the familiarization programme immediately after
joining the vessel.
Page 40 of 63
9.2 “IBRA LNG” ELEVATOR
The Elevator, as fitted in the vessel, is a modern Elevator built by Hyundai It has
all the safety systems incorporated in it such as gate switch, door switch,
emergency switch, safety edge of door ( a device do open the door automatically
when passengers or cargo get caught in the door of the case ), emergency bell
and telephone, emergency light etc. The elevator is also provided with safety
switch which is the operating switch used for maintenance. The switch is
provided on cage top. There is door locking device which prevents the door from
being manually opened once the hoistway door closes.
9.3 MAINTENANCE AS PLANNED
It was decided to carry out a normal routine maintenance of the passenger lift.
Accordingly a safety meeting was held on 3rd February 2007, in the morning.
During the safety meeting the Electrician was advised to take the ‘wiper’ along
with him during his maintenance work.
The work was started soon after the afternoon safety meeting. The normal
maintenance routine was then reportedly carried out as per the manufacturer’s
instructions after taking all necessary safety precautions. However, during the
course of his normal maintenance work, the Electrician, Mr. Ioan Cumpat,
expired at 1755 hrs L.T. on 03rd February 2007 at the Elevator trunk ( the
sequence of events have been very elaborately narrated elsewhere in this Report
). During the course of investigation, the place where the accident took place was
identified by the principal investigator.
10 INCIDENT INVESTIGATION
Once identified the place where Mr. Ioan Cumpat got trapped in the elevator, the
incident site was examined for a quick overview. Whatever data were available at
the time of our visit were duly examined and various witnesses were interrogated
Page 41 of 63
in order to ascertain the veracity of the written statements of the witnesses which
were made earlier .The findings were noted as below :
• Position of the Casualty was identified as being trapped in the inverted position
inside the elevator trunk.
• Ship’s position: 08 58.9 N Latitude, 076 43.2 E Longitude.
• Routine maintenance was being carried out on Elevator cage.
• Tools used to carry out the maintenance were normal electrician tools.
• Safety devices in use were the normal safety gears that include safety boots and
boiler suit. There was no sign of helmet whereas the safety harness was found
outside the elevator trunk.
• The top of the elevator cage was provided with a safety guard above the
emergency escape. Escape ladder was also provided all the way from Floor
Deck to Navigational Bridge Deck. Electrician had a walkie talkie with him at the
time of the incident.
• As far as safety was concerned, the elevator cage was equipped with an
emergency switch ( and was reportedly found not activated ) inside the cage. The
control box on top of cage had the following :
1. Auto / Inspection Selector switch which was left on Auto.
2. Door Open / Close Switch which was left in the Open Position.
3. Door Switch ( No indication ).
4. Emergency Stop that was not activated.
Page 42 of 63
• A Remote Control that has 2 buttons ( Up / Down ) and an Emergency
stop, which was not activated.
• The elevator is also equipped with an emergency stop at the Elevator
Switchboard in the Elevator Machinery Room. This stop was not activated
in order to be able to move the cage using the Remote Control on the top
of the Elevator Cage.
• Warning signs were posted at all levels ( Elevator Under Maintenance ).
• There was no apparent damage to the equipment. However, the door at
‘A’ deck did not open using the Emergency Opening Key at the time of the
rescue operation and had to be opened from inside the trunk. It was
noticed that the bulkhead openings doors at all decks were provided with
3 sides frame instead of 4 sides frame, although means of fixing the fourth
side were provided.
• The area was kept at very good housekeeping. No signs of oil leaks.
• The weather at the time of the incident was fair with slight sea and low
swell. Air temp +30C. Vessel moving easily at 14.75 knots.
• Lighting level was adequate as the trunk is equipped with fluorescent
lights all throughout.
• No unusual noise was detected.
During the investigation, as many relevant facts as possible were collected. Many
photographs for both the general area and specific items were taken. Some
photographs were taken by the ship’s staff earlier which were carefully studied and
analyzed in order to help revealing any conditions or observations that might be missed
Page 43 of 63
out. Sketches of the specific location and the position of the casualty as seen by the
ship’s crew were also made.
The photographs and sketches had a major role in understanding the incident and the
event leading upto it.
10.1 DATA GATHERING
The collection of data contributing factors were divided into the following main
areas :
1. People
2. Environment
3. Equipment
4. Procedure
5. Organization
10.1.1 PEOPLE
People who might have information about the incident were identified and the
following statements were obtained from them :
MASTER’S STATEMENT
“03rd February 2007, shortly after 1425 hrs L.T., I was alerted to the fact that
someone was trapped in the lift, initially by 2nd Officer, then the Chief Officer. On
leaving my cabin and proceeding to bridge, I heard much commotion and shouting
from lower in the accommodation.
When I was informed of the situation and went to the scene, I was able to see Mr.
loan Cumpat in inverted position. At this time he was quite conscious and coherent
although his position was very awkward and he had obviously suffered severe
trauma, with open wounds and a fractured leg.
Page 44 of 63
I alerted OSMC ( Owners ) of the situation requesting their assistance in arranging
medical rescue assistance etc. and initially altered course towards Trivandrum Port.
Meanwhile attempts to release Mr. Ioan Cumpat were made by the crew, his
situation was extremely dangerous being supported by his trapped leg and foot in an
inverted position trapped between the Lift Cage, Trunk Ladder and angle Iron
brackets, there being a 12 - 15 meter drop beneath him.
Around 1450 hrs L.T., before he could be freed, he slipped into unconscious state,
ship’s crew secured line around casualty. Pan Pan message was transmitted with
little response. This was repeated several times.
1526 hrs L.T., vessel was instructed by Company to make full speed to Cochin, for
assistance, vessel’s course was adjusted accordingly.
1530 hrs L.T., he was finally freed and taken to ship’s hospital where cardiac
compression and artificial respiration with oxygen were administered by ship’s crew,
his pulse very rapid and very weak, his breathing stopped.
At 1538 hrs L.T., Radio Medical advice was sought via 32# Netherlands Coastguard,
who on being told our situation advised that what we had done was the most
appropriate action, and to continue until help could be received. But, however, that
we were probably not going to revive the casualty.
1615 hrs L.T., on gaining contact with local Coast Guard vessel was advised to
make for Kovalam point where Coast Guard would meet vessel with medical
assistance. Course was adjusted accordingly.
1650 hrs L.T., we were requested to anchor 5 miles off Vilinjam light. At this time
Mr. Ioan Cumpat was showing no vital signs, he was neither breathing nor was there
any pulse, his eyes were dilated and no response to light, attempts to resuscitate Mr.
Ioan Cumpat continued throughout.
Page 45 of 63
Throughout there was frequent communications between Vessel, OSMC Casualty
Room and Coast Guard, both by telephone and VHF.
Vessel as requested anchored safely off Vilinjam at 1755 hrs local time, in
position 080 21’ N 0760 57’ E. At this time it was apparent that Mr. Ioan Cumpat
was in fact dead, however, crew continued attempts to revive Mr. Ioan Cumpat
until finally the Indian Coast Guard arrived.
1830 hrs L.T., Coast Guard were unable to board vessel due to sea state hence
it was decided to land Mr. Ioan Cumpat’s to the Coast Guard boat using the
crane, this was also not easy due to superstructure of the Coast Guard boat, so
on coast Guard instruction, we landed body to fishing boat “Olympia”, which was
standing-off nearby.
At 1940 hrs L.T. Coast Guard confirmed that Mr. Ioan Cumpat was dead upon
his being received to their custody. Vessel was instructed to remain anchored
until further notice/ formalities completed.
It appears that whilst completing routine maintenance on vessel’s Elevator Mr.
Ioan Cumpat accidentally fell resulting in his becoming trapped until further
precarious position, leading to his tragic death.
I believe that my crew did everything possible in the circumstance, and commend
them for their efforts”.
Page 46 of 63
CHIEF OFFICER’S STATEMENT
“Around 1425 hrs L.T. I heard the shouting from the elevator. I advised the
Bridge and all the crew over the VHF public system.. I rushed to the ‘A’ deck and
with Chief and First Engineer was decided to open the ‘B’ deck elevator door.
All crew were mustered and Medical team was instructed to prepare first aid
equipment.
After few minutes we access the top of the elevator and we found Mr. Ioan
Cumpat ( ship’s electrician ) trapped at side of elevator in inverted
position.
His leg was twisted and trapped between elevator and casing preventing him
from failing.
Bridge (Captain) was updated with situation.
After we insured him from failing, elevator was manually operated from the E/R
and Electrician leg was freed obstruction.
After several attempts from the outside, we manage to open the Upper Deck
elevator doors from inside of elevator trunk, Electrician was .lowered to upper
Deck and taken out from the elevator trunk space.
Electrician was found unconscious with stopped breathing and pulse very rapid
and very weak.
We rushed to the hospital and artificial respiration was given together with
cardiac massage. Above attempts continued until Indian Coast Guard arrived
without signs of life from injured person.
Page 47 of 63
At 1755 hrs L.T. the casualty was declared dead by the Captain.
I solemnly pledge that the above statement is true and in the best of my knowledge. Ch / Off SS IBRA LNG Dated: 3rd
February 2007
Nenad Martinovic”
STATEMENT OF 1ST OFFICER
“I received a call from the Chief Officer at 1430 hrs saying that there is somebody
stuck up in the elevator and needed to be given First Aid. I rushed to the ‘B’ deck
to find the Electrician hanging in an inverted position hanging by his foot/leg
outside the elevator cage (in the maintenance area). Rescue work was in full
swing to remove the casualty from the elevator area and bring him to the hospital
on the stretcher. Meanwhile, I got the First Aid equipment ready. Casualty Mr.
Ioan Cumpat (Electrician) was tied a safety harness to heave him up. The door of
the elevator on the upper deck was opened by emergency key and he was finally
taken out and brought to the hospital on the stretcher. He was found to have
external as well as internal bleeding. He was immediately given artificial
respiration followed by oxygen resuscitation via the resuscitator. His pulse was
very weak and he was showing no vital signs. Artificial respiration continued till
the Coastal Guard vessel arrived but the casualty still did not show any sign of
improvement.
1755 hrs the casualty was declared dead by the Captain.
I solemnly pledge that the above statement is true and to the best of my
knowledge.
Page 48 of 63
-sd/-
(Gaurav
Choudhary)
1st Officer
SS IBRA LNG
03 February 2007”
STATEMENT OF CHIEF ENGINEER
“Work carried out on ship’s elevator was part of routine maintenance prepared and
discussed at morning meeting and in Engine Room just before work.
Before work starts warning signals posted “ELEVATOR UNDER MAINTENANCE” at all deck elevator doors. All preparation works carried out.
Elevator was functioning normally during all this time.
Electrician and wiper was assigned for maintenance work.
Just before accident happened, wiper took mat out of elevator cabin to clean it in
upper deck on electrician instructions. Then Electrician went into the elevator
cabin and went down. It seemed that the Electrician decided to further routine
maintenance on top of the elevator cabin. At the time accident happened,
elevator was switched off.
The electrician was experienced in his rank. His last contract spent on sister ship
equipped with same elevator.
At the time of accident I was in the Engine Room workshop and I was called
immediately after the accident happened. I went to ‘B’ deck to do as much as
possible help to release injured electrician Mr. Cunpat. After ‘B’ deck was opened
Page 49 of 63
to access and electrician released, I went down to the Engine Room to handle
main engine to full speed (course altered towards Trivandrum).
- sd/-
CH. ENG. HIGIN BASIC
At and on 04 Feb 2007”
STATEMENT OF 1 A/E ( Assistant Engineer ).
“I heard a scream around the elevator trunk around 1425 hrs. I went to elevator
entrance door on ‘A’ deck where I heard voice from electrician calling for help.
After a few minutes we managed to access inside elevator trunk via door ‘B’
deck. I noticed E/E was trapped in an inverted position at the side of elevator, by
the ladder, his leg was twisted and trapped thereby preventing him from falling. I
realize it to be risky to try to get him out at that position by moving the elevator.
So we decided that one team will tie a safety harness of rope around him and
other in engine room will manually operate the elevator. After a while he was
finally taken out and brought to the hospital. He was found with external bleeding
and inside hospital I realized also with internal bleeding. He was immediately
given artificial respiration. Oxygen was also given continuously. Artificial
respiration continued till the Coast Guard vessel arrived but the casualty never
gave signs of life.
1755 hrs L.T. the casualty was declared dead by the Captain.
I solemnly pledge that the above statement is true & in best of my knowledge.
sd/-
Page 50 of 63
1 A/E MARIO
MATISAS
04th February 2007
STATEMENT OF 2 A/E ( Assistant Engineer )
“I Patel Afzal Hajimubarak, 2nd Assistant Engineer on SS IBRA LNG testify the following. On 3rd Feb’ 2007, at 1300 hrs, as usual we had a job meeting with the engine
staff in the Engine Control Room. At 1310 hrs, I along with one of the oiler went
to the forward heavy fuel oil transfer pump room to purge the suction filters of the
transfer pumps and to start the forward fuel oil tank heating.
At 1415 hrs I returned back to the Engine Room. At 1425 hrs I was informed by Third Assistant Engineer on the radio that
electrician was stuck inside the elevator trunk so I along with Third engineer took
the elevator door opening key from Engine Control room and went to the upper
deck. As instructed by the Chief Officer there, we tried to open the elevator door
of the upper deck but it was stuck. Then, as per First Engineer’s instructions, I
went to the elevator machinery room to prepare for emergency manual operation
of the elevator if in case required. We were standby there for any instructions
from the rescue party to manually move the elevator cage. At 1500 hrs, I was instructed by the First Engineer to go to the Engine Control
Room and take care of the operation as we were increasing the ship’s speed to
full rpm. Since then I was in the Engine Control Room with the Chief Engineer till
the arrival anchorage point.
Page 51 of 63
After arrival anchorage, as per First Engineer’s instructions, I along with Third
Engineer & wiper opened the main floor (M/F) deck elevator door to clean the
elevator trunk bottom. We found blood drops and some tools and one shoe in the
elevator pit. We removed the tools & shoe and cleaned the blood. There were
some blood drops on the tools which we washed and then secured the tools in
workshop.
Date – 06th February
2007
-sd/- Patel Afzal Hajimubarak
( Second Assistant Engineer )
STATEMENT OF 3 A/E ( Assistant Engineer ).
“I, Kanwar Udyan Rathore, 3 A/E on SS IBRA LNG testify the following.
On 3rd Feb’ 2007 at 1300 hrs, as usual we had job meeting in the Engine Control Room.
At 1310 hrs., I went for testing E/R fire dampers and funnel flaps. After finishing
this I started overhauling package Air Conditioner, F.W. booster P/P in workshop
where I heard on radio that electrician stuck in the elevator, then I call on the
radio to the 2 AE & we took the elevator key from ECR. We opened the B deck
door with rescue team. Then we tried to open the upper deck door which was
stuck and we could not open it. Then as per C/O instructions we went to elevator
machinery room for manual emergency operation of elevator. Then as per
instructions we lowered the elevator few centimeters manually. Then I went up to
Upper deck. Then rescue team opened the upper deck door from inside & we
tried to lower the electrician with the help of ropes. Electrician was recovered
from upper deck and we sent him to the hospital. After that I came back to
Engine Control Room for maneuvering/anchorage.
Page 52 of 63
After arrival anchorage as per 1st Engineer instruction, I along with 2nd Engineer
& wiper opened the main floor deck elevator door to clean the elevator trunk
bottom. We found blood drops and some tools and one shoe and cleaned the
blood. There were some blood drops on the tools, which we washed and then
returned the tools in workshop.
Date : 06th February 2007
-sd/-
Kunwar Udyan Rathore
( Third Assistant Engineer )
STATEMENT OF WIPER
“During morning safety meeting in ECR, I received a job order from 1st Engineer
to work together with electrician in his monthly maintenance routine of elevator.
1300 hrs, after receiving an order from 1st Engineer, I & electrician posted a
warning sign “ ELEVATOR MAINTENANCE” from ‘D’ deck down to main floor.
After that, we proceeded to 4th deck where electrician turned off the power of
elevator. He then opened the door of main deck for inspection. After a while he
told me to clean the bottom of elevator trunk. 1345 hrs I called up electrician to
look & see if I would still need to mop the bottom trunk or not. After seeing,
electrician told me to secure my cleaning gear & so I did. Assuming that
everything is finished, I went to ECR to get a cleaning foam and proceeded to
upper deck when I saw that the elevator cage landed there. 1400 hrs I met
electrician at upper deck & he asked me to clean the elevator mat. After that he
went inside the elevator cage. I just saw that the elevator landed on 4th deck of
the main floor (I don’t remember the exact deck No. it had landed). With the new
Page 53 of 63
job order from electrician, I went to “B” deck to take the vaccum & clean the mat
on the upper deck. After cleaning I was not satisfied so I decided to go to A deck
at the cleaning gear locker to take a mop and cleaned the mat once again. After
a few minutes of cleaning, I decided to return the cleaning gear to their
respective decks when I heard some body screaming inside the elevator. I knew
it was electrician because he is the one working inside the elevator. I met oiler #
1 & informed him that electrician was screaming for help. Then instructed me to
inform 1st Engineer or anyone from the engine room what I did.
- sd/-
Fritz Andrew B. Rosel
Wiper, IBRA LNG
Broad questions such as Who, What, When, Where, Why and How were asked to all
parties. All concerned were interrogated in order to elicit information related to the
incident.
All individuals were assured that the investigation / interviews were being conducted
to promote safety and not to apportion blame at any of them.
Everyone explained in his own words what happened and the action taken on
occurrence of the incident. They were asked if they knew of any near-miss history of
the Elevator.
During the interview / interrogation of all individuals been interviewed were observed
to be in physically & mentally sound condition. From the interviewers / interrogation
of the concerned person, it was found that the casualty was an experienced person
who had just signed off a sister ship with exactly the same elevator system. Looking
into the fact that he had been an electrician in the past twenty years, it could be said
that Mr. Ioan Cumpat was well experienced in the task and was fit for the job.
It was reported that the casualty was neither under stress nor under the influence of alcohol.
Page 54 of 63
10.1.2 ENVIRONMENT
The Environmental Factor was not found to be applicable to the causes of the
incident as the weather was fair and the air temperature was good. No signs of
toxic or hazardous gases, dust or fumes presented in the site.
10.1.3 THE EQUIPMENT
The electrician was carrying out routine maintenance on the equipment. The
elevator was reported to be in good condition and nothing untowards noticed
about its normal operation since the vessel was built. The only thing noticed
was the distorted bottom guide underneath the right hand side of the bulkhead
opening slide door ( looking from inside ). This may be due to a missing frame
side, as mentioned earlier above. This could not have contributed to the
accident as it would keep the sliding door in the open position, in which case
the electrician could easily escape from the scene. The possibility of the
accident was more likely with a closed door.
Other important issues with the equipment were checked. There was no apparent
equipment failure at the time of the incident.
The purpose of the Electrician being on the top of the cage was purely for routine
maintenance that involved the following :
1. Cage emergency stop switches test, 2. Cage telephone communication test, 3. Cage bell - call to the bridge test, 4. Wire rope visual inspection, 5. Elevator motor gear case oil check, 6. Greasing of electric motor bearings,
Page 55 of 63
7. Landing door interlock switches inspection, 8. Safety devices and alarm test, 9. Electric motor insulation resistance test, 10. Oil level in the lubricator of the cage, 11. Oil level in the lubricator of the counter weight, 12. Tightness of mounting bolts of the rail, 13. Trunk lighting inspection, 14. Clearance between brake lining and brake drum, 15. Clearance between counter weights and buffer springs.
The work was carried out as per the checklist which points out the possible hazards
and the safety countermeasures that should be adopted. The vessel has the
COSWP and Company SMS Fleet Notice No: OSMC 06-01 which gives guidelines
for handling marine elevator. Both documents were reported to be understood by the
Electrician. However, no risk assessment was made as it was a routine work.
The Electrician was in charge of both maintenance and operation of the elevator.
Total running hours of the machine was reported to be 652 hours since the date of
delivery of the vessel.
10.1.4 PROCEDURE
The work procedures, as well as the scheduling of the work, were examined in
order to ascertain whether they contributed to the incident or not. It was found
that the work was planned in advance and the Wiper was assigned to assist.
However, the Electrician dismissed the Wiper who was assigned to help and to
be part of the team in case something went wrong. The Wiper was dismissed
before the job was completed. This had changed the condition making the
normal procedure unsafe. Although safety harness was provided, it was not
Page 56 of 63
being worn at the time of the incident. No safety helmet was found in or around
the accident location. All emergency stops were not activated and interlock
switches were put to Auto position.
10.1.5 THE ORGANISATIONAL FACTOR
From the above it appears that the organizational factor as reflected in this
incident clearly shows that the ship used all possible sources to enhance the
safety during this task but was violated by the Electrician. From the
interrogation of concerned higher management, it appears that the safety rules
were communicated in a way that they were understandable by all crew
members. The written procedures were provided such as the COSWP, on
board OPM, SMS Fleet Notices and Safety campaigns. Safety procedures
being enforced but unfortunately dismissing the Wiper resulted in a broken
safety chain. Going into the elevator trunk with all the safety interlock /
emergency stops not activated had resulted is a devastating incident.
Although the Electrician was experienced and well trained, a risk assessment
had to be carried out. This was not done due to unknown reason. There was, of
course, no direct violation of the safety rules. The reason for not conducting risk
assessment was because the task involved was of routine nature which does
not appear to be convincing.
However, the Chief Engineer being the Head of Engineering Department under
whose guidance the Electrician works on any vessel, cannot escape his
responsibility for not enforcing Risk Assessment of the task prior to undertaking
the maintenance work in a potentially risk prone area. It appears that just
because the Electrician was an experienced person, and just because the
maintenance work was of routine nature, entire task was left on to the
Electrician and his assistant. During the course of Lift Maintenance no feed
back of work progress was obtained and no cross check was carried out by the
Chief Engineer (as reflected in his statement).
Page 57 of 63
The Chief Engineer was expected to carry out a proactive analysis of the
situation during safety meeting and decide on the maintenance strategy to be
adopted by the Electrician and his assistant.
It was reported that the Elevator did not have any previous history of any
operational problem. Therefore, elevator maintenance work need not have
been done at ‘A’ deck / UD level. The ideal position for maintenance should
have been the lift’s Lowermost position, and the lift operation should have been
done manually and not electrically. The Chief Engineer should have instructed
the Electrician accordingly.
11. APPARENT CAUSE ANALYSIS
The following analysis had helped to classify the facts in the ICAM model for
inclusion in the investigation report and for briefing the PMA on the investigation
findings :
1. A series of mistakes were made by the casualty. This was initiated by
dismissing the direct assistance from the job, followed by not putting the full
PPE, entering the elevator trunk on self initiative and changing the safety
switches settings, missing the facts that this might be very dangerous as
proved later. These errors had an adverse effect associated with the person
having a direct contact with the equipment. It is believed that these acts have
led directly to the incident.
2. The location of the incident reportedly made the rescue operation very difficult
as the casualty was in the inverted position with his knee trapped between two
iron brackets, there being a drop of about 25 meters beneath him.
3. At first the sliding door reportedly did not open using the emergency key from
‘A’ deck. A crew member had to enter from the above deck and open the door
Page 58 of 63
by releasing the locking mechanism from the inside. The total time used to
secure the casualty into the ship’s hospital was 1 hour 5 minutes. The casualty
was reported to be bleeding and blood drops could be traced all the way down
from ‘A’ deck to the bottom floor. It was believed that the casualty had suffered
from broken leg, twisted ankle, broken arm, internal and external bleeding. The
casualty confirmed to be deceased by the Indian Coast Guard doctor at 1940
hrs L.T. The time when the incident first happened was about 1425 hrs L.T..
4. Organizational factor presented as inadequate procedures were used i.e. No
Risk Assessment made for this specific operation.
5. Failures into Organizational Factor using the Organizational Factor Type (OFT)
were not applicable as far as the hardware is concerned. However, when it
came to training, it could be seen that making assumption about the Electrician
knowledge and skills seemed to be over-confident as he dismissed the
assistant provided for him. The Electrician failed to assess the sequences of
that decision as well as being inside the elevator trunk with no safety measures
to stop the elevator from moving.
6. As far as organization is involved, it could be seen that the Electrician had
missed the definition of the objectives of the Wiper being with him due to
unclear accountability and the understanding of the wiper being not directly
trained on that particular job. This led into wrong decision making.
7. With regards to communication, a poor feed back could be noticed as neither
Bridge nor ECR were informed of the dismissal of the Wiper prior to completion
of work.
8. Incompatible Goals were demonstrated by the presence of conflicts between
safe work and production priorities. The Electrician went into the Elevator Trunk
as a conscious person who was trying to produce a good result out of his job
Page 59 of 63
being the person looking after the Elevator. Seemingly, he did not consider the
safety aspects and the hazards involved.
9. Error Enforcing Condition did not apply in this incident as there was no
apparent human limitation, external disturbance, social factors and personality
factor which are not known. The Electrician had recently joined the ship (12
days prior to the date of the incident).
10. Procedures should have been easily identified as they are clearly written,
documented and controlled. The missing risk assessment could have resulted
in a poor feedback on practicality.
11. Maintenance management was enforced as the job was pre-planned from early
morning to take place in the afternoon. There had been enough time for
everything to be set and for the safety measures to be considered.
12. Although the maintenance manual does not provide any safety instruction
before undertaking any maintenance work, it does provide “Escape method in
an emergency”. However, considering the place of work being Elevator shaft,
the general risk perception is obvious and hence additional guidelines as to
‘safety preparation’ is considered not necessary and code of safe works
practice is considered adequate.
13. Apart from the missing frame side, which believed not to have contributed to
the incident, there is no apparent design failure on the Elevator cage. During
the rescue operation and while carrying out the investigation, it was noticed that
the bulkhead opening sliding door could not be opened using the emergency
key. This had happened at ‘A’ deck and ‘B’ deck and UD.
14. Once the elevator started to move upwards ( will be explained later in this
Report ), the Electrician was able to understand the hazardous conditions
which could occur but he failed to control the recovery defense and could not
Page 60 of 63
get out of trouble without injury due to the fast moving cage and the restricted
area inside the elevator trunk.
15. The casualty tried to prevent escalation of the injury by applying a containment
defense procedure using his left leg to prevent him from falling all the way down
to the elevator floor ( 25 meters drop ).
16. Due to the restricted area failure to open the bulkhead slide door as quickly as
possible, the emergency team could not manage to evacuate the potential
casualty from the danger zone at a relatively good time. Medical first aid
although given but could not improve the condition of the casualty. The site was
isolated since then.
12. CONCLUSION
1. Usual practice of wearing PPE was not adhered to. Necessary PPE were left
outside the elevator trunk.
2. The Electrician appeared to be over-confident so much so that he entered the
elevator trunk without assistance resulting in vital human error.
3. Deliberately caused break in safety procedure by dismissing safety team,
although he was specifically instructed to the contrary during safety briefly in
the afternoon of 3rd February 2007.
4. Emergency stops were not achieved and “Inspection” selector switch was
changed into Auto position.
5. Vital time was lost as the lift door could not be opened in time.
6. Rescue operation became difficult due to space restriction.
Page 61 of 63
7. Considering the awkward position of the casualty who was trapped in an
“Inverted” position, appropriate decision making process was delayed for quick
rescue operation.
8. The casualty had been unconscious for about 40 minutes before he was finally
freed and shifted to ship’s hospital before first aid could be started.
9. The casualty was reported to be bleeding for nearly an hour before actual first
aid could be commenced.
13. RECAPITULATION
1. Electrician at Deck ‘A’ opened the elevator trunk door using emergency keys,
slides onto the top of the elevator car (cage) which is at Upper Deck ( UD ),
Door closed automatically ( as designed ),
2. Electrician carried out routine maintenance that involved checking of all fittings
and lubrication etc.,
3. He decided to go out through ‘A’ deck so took the elevator (using the remote
box) to a position where he could reach and unlock the door locking
mechanism, approximately 50 cms above floor of ‘A’ deck,
4. Changed over from Inspection to Auto (Maintenance control box), taking into
account that there is a delay period for the system to re-set, so he can reach
the door,
5. Re-set time complete ( around 40 seconds ) before he succeeded in opening
the door and elevator moves towards the nearest deck. ‘A’ deck being the
nearest ( 1700 mm to travel up towards ‘A’ deck, where as it needed
2050 mm to travel downwards to UD level ),
6. Initial movement caused the electrician to panic and therefore he turns towards
the ladder for easy escape,
Page 62 of 63
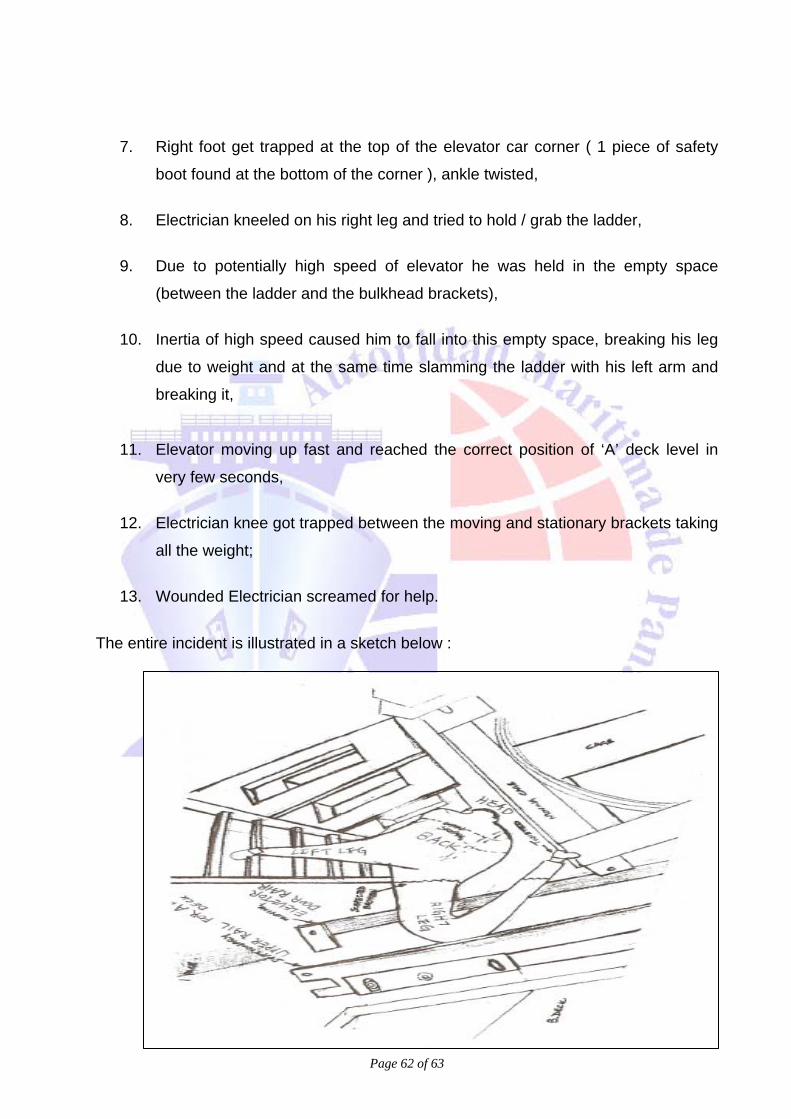
7. Right foot get trapped at the top of the elevator car corner ( 1 piece of safety
boot found at the bottom of the corner ), ankle twisted,
8. Electrician kneeled on his right leg and tried to hold / grab the ladder,
9. Due to potentially high speed of elevator he was held in the empty space
(between the ladder and the bulkhead brackets),
10. Inertia of high speed caused him to fall into this empty space, breaking his leg
due to weight and at the same time slamming the ladder with his left arm and
breaking it,
11. Elevator moving up fast and reached the correct position of ‘A’ deck level in
very few seconds,
12. Electrician knee got trapped between the moving and stationary brackets taking
all the weight;
13. Wounded Electrician screamed for help.
The entire incident is illustrated in a sketch below :
Page 63 of 63
14. RECOMMENDATION
The following corrective actions were identified in order to prevent recurrences of
such incident. At first a proactive analysis is to be carried out to identify
significant risks and safeguards to prevent and mitigate the associated
consequences as to what could go wrong, what are the consequences and what
could cause these consequences. Based on this analysis, a Management
System has to be set-up in order to control risk so that maintenance, strategies,
methods and procedures could be developed. Although not all causes can be
completely eliminated, effort must be made to enhance the safety awareness of
the crew and the fleet as a whole. The corrective actions recommended are
specific, measurable, accountable, timely, effective and can be reviewed
whenever required. The Principal Investigator is of the opinion that the following
formulated recommendations, if implemented, will reduce the risk of recurrence
of the incident and the consequences thereof.
• The job is to be planned well in advance to allow for all safety measures to
be carried out,
• A risk assessment should form a part of the planned maintenance and must
be obtained prior to carrying out maintenance,
• At least two persons should be involved when elevator maintenance is
carried out,
• A good communication must be established between all parties involved at
all time. A time interval can be agreed between the involved parties,
• All safety procedure must be strictly observed. Every person involved in the
work must have clear understanding of their duties and associated risks.
Page 64 of 63
• Elevator trunk must be treated as a confined space, therefore, an entry
permit must be obtained,
• Elevator door at specific deck to be locked open during maintenance,
• Instruction for emergency opening of elevator doors should be posted by
each door,
• Clear warning of both the presence and the nature of a potentially
hazardous situation must be explained to all members involved,
• Must ensure that the team members understand the nature and severity of
the hazardous conditions presents at the worksite,
• Under no circumstances an individual is to be allowed to enter the Elevator
trunk with the emergency stops not activated,
• An announcement must be made through the ship’s PA prior to carrying out
any maintenance on elevator,
• The controls in cage maintenance call box must be configured in such a
manner that it would not be possible to activate them accidentally.
• No “complete maintenance” announcement is to be carried out until a full
head count is conducted,
• Owners must obtain makers recommendation towards safety enhancement
for prevention of accidental fall (when opening the doors using emergency
keys).
Page 65 of 63
• Person involved in elevator maintenance must demonstrate the capability of
doing such task to the Chief Engineer before conducting the first routine
maintenance.
• Warning notices must be posted so that accidental use of all call buttons is
prevented.
• Design of the Elevator should include a safety barrier around the cage.
• Company OPMs must include instructions on elevator maintenance.
• All maintenance on the elevator must be carried out at lowermost position
unless the situation demands otherwise.
15. OUTCOMES OF THE INCIDENT
1. Loss of life of one of the ship’s officer,
2. This incident will not be forgotten by any of the crew members due to the
psychological effect on the individuals,
3. Equipment is left isolated since the day of the incident,
4. Lessons learnt and more precautions will be adhered to when attending
any maintenance in future.
P. K. Bhattacharyya PRINCIPAL INVESTIGATOR, HENDERSON INT’L (INDIA) PVT. LTD., KOLKATA, INDIA.