Category 4: Class II Division 2 malocclusionwith deep overbiteBaharak Fooladi,a Tarryn MacCarthy,b Tracy Maloney,c and Lokesh Surid
Boston, Mass
This case report was part of the resident display of cases sponsored by the College of Diplomates of theAmerican Board of Orthodontics at the annual session of the American Association of Orthodontists, May
20-24, 2005, in San Francisco, Calif. (Am J Orthod Dentofacial Orthop 2007;132:252-9)
SUMMARY OF TREATMENT
Case report category: 4Patient’s date of birth: 12/19/1986Age: 15 years 9 months
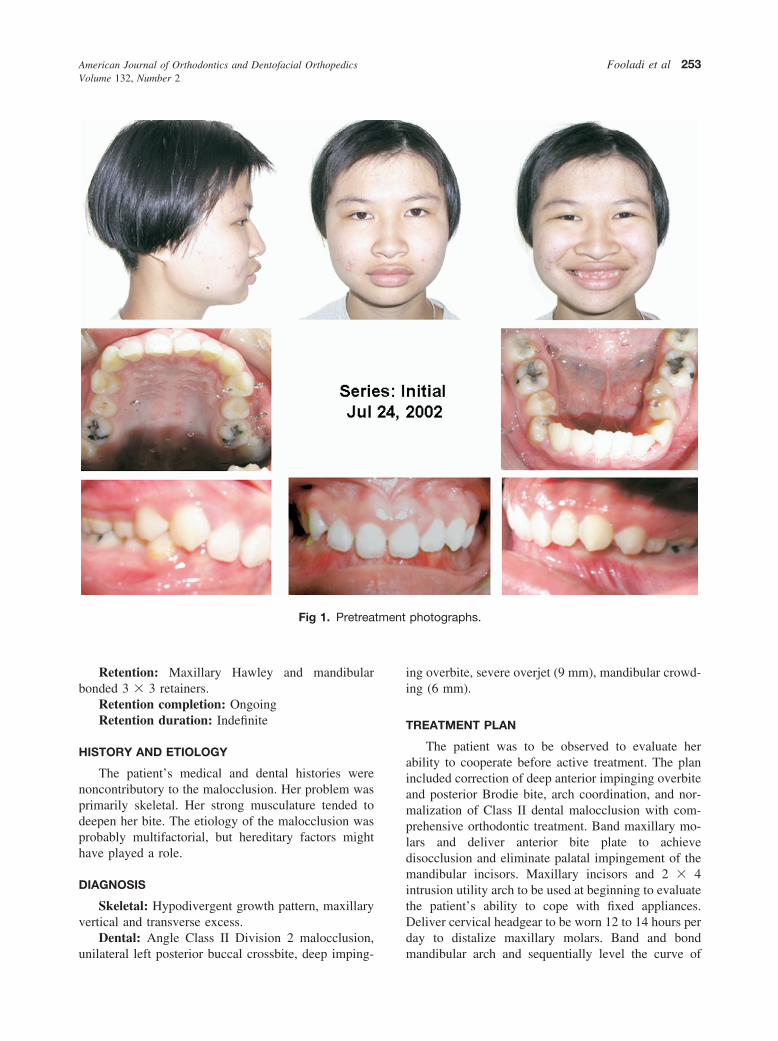
Dental: Angle Class II Division 2 malocclusion,unilateral buccal crossbite (Brodie bite) of maxillaryleft premolars and second molar, asymmetric maxillaryand mandibular arches, 100% deep and impingingoverbite, mandibular crowding (6 mm), excessive over-jet (6 mm), upper midline 1 mm to the left of facialmidline.
Facial: Brachycephalic facial pattern, symmetrical,orthognathic profile, full lips with an acute nasolabialangle (79°), deficient lower third anterior face height,5-mm gingival display on smiling with minimal incisordisplay.
Correct deep anterior impinging overbite and pos-terior Brodie bite, coordinate arches, and normalizeClass II dental malocclusion with comprehensive orth-odontic treatment. Band maxillary molars and deliveranterior bite plate to achieve disocclusion and eliminatepalatal impingement of mandibular incisors. Intrusionarch to be used at the beginning of treatment. Delivercervical headgear to be worn by the patient 12 to 14hours per day to distalize maxillary molars. Band andbond mandibular arch and sequentially level curve ofSpee. Create space for mandibular left second premo-lar. Bond maxillary incisors and use 2 � 4 intrusionutility arch. Coordinate arch forms and use crosselastics to correct Brodie bite. Class II elastics to beused as needed. Detailing, remove appliances, andretain.
Treatment
Patient cooperation and oral hygiene were to beevaluated before starting treatment. Use bite plate todisocclude the dentition and eliminate mandibular in-cisor impingement on the palate (Fig 5). Deliver cervi-cal headgear and instruct patient to wear it at least 12 to14 hours per day. Use intrusion arch to intrude maxil-lary anterior teeth and reduce gingival display. Levelmandibular arch with sequential archwires and openspace for mandibular left second premolar. Coordinatearchwires and use cross elastics to eliminate buccalcrossbite on left side. Correct sagittal discrepancy ofClass II end-on molar relationship. Class II elastics andfinal detailing of occlusion as needed. Remove appli-ances and deliver retainers.
The patient’s medical and dental histories werenoncontributory to the malocclusion. Her problem wasprimarily skeletal. Her strong musculature tended todeepen her bite. The etiology of the malocclusion wasprobably multifactorial, but hereditary factors mighthave played a role.
DIAGNOSIS
Skeletal: Hypodivergent growth pattern, maxillaryvertical and transverse excess.
Dental: Angle Class II Division 2 malocclusion,
Fig 1. Pretrea
unilateral left posterior buccal crossbite, deep imping-
ing overbite, severe overjet (9 mm), mandibular crowd-ing (6 mm).
TREATMENT PLAN
The patient was to be observed to evaluate herability to cooperate before active treatment. The planincluded correction of deep anterior impinging overbiteand posterior Brodie bite, arch coordination, and nor-malization of Class II dental malocclusion with com-prehensive orthodontic treatment. Band maxillary mo-lars and deliver anterior bite plate to achievedisocclusion and eliminate palatal impingement of themandibular incisors. Maxillary incisors and 2 � 4intrusion utility arch to be used at beginning to evaluatethe patient’s ability to cope with fixed appliances.Deliver cervical headgear to be worn 12 to 14 hours perday to distalize maxillary molars. Band and bond
photographs.
tment
mandibular arch and sequentially level the curve of
American Journal of Orthodontics and Dentofacial OrthopedicsAugust 2007
254 Fooladi et al
Spee. Create space for mandibular left second premo-lar. Coordinate arch forms and use cross elastics tocorrect the Brodie bite. Class II elastics to be used as
Fig 2. Pretrea
Fig 3. Pretreatment cephalometric tracing.
needed. Detailing, remove appliances, and retain.
SPECIFIC OBJECTIVES OF TREATMENTMaxilla
A-P: Hold.
Mandible
A-P: Allow for maximum A-P expression ofgrowth, remove interferences to distally trapped man-dible.
Vertical: Increase via extrusion and uprighting of
dental casts.
Fig 4. Pretreatment panoramic radiograph.
tment
posterior teeth.
; B, fin
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 132, Number 2
Vertical: Increase with extrusion of posterior teeth;anterior teeth to be intruded.
Intermolar width: Decrease transverse widthacross canines, premolars, and second molars andincrease across first molars.
Mandibular dentition
A-P: Procline incisors.Vertical: Increase via extrusion of posterior teeth
and intrusion of anterior teeth.Intermolar/intercanine width: Constrict interca-
nine width.Facial esthetics: Increase lower anterior face
height, decrease gingival display.
APPLIANCES
Full edgewise appliance (American IBD prescrip-tion) with anterior .018 �. 025-in and posterior .022 �.028-in bracket slot; cervical pull headgear worn 12 to14 hours per day; anterior bite plane, and Class II
Table. Cephalometric summary
Area Measurement
Maxilla to cranial base SNA angle (°)Mandible to cranial base SNB angle (°)
Y-axis (°)SN-Go-Gn (°)FMA (°)
Maxillomandibular ANB angle (°)Maxillary dentition 1 to NA (mm)
1 to SN (°)6-6 (mm) (casts) between central fos
Mandibular dentition 1 to NB (mm)1 to Go-Gn (°)6-6 (mm) (casts)3-3 (mm) (casts)
A1, Pretreatment records; A2, interim or progress records if indicated
Fig 5. Progress photo
5/16-oz elastics.
TREATMENT PROGRESS
Because of poor oral hygiene and history of delayedmaturation with learning disability, the patient and theparent were advised that treatment would begin afterevaluation of the patient’s cooperation and improve-ment in home care. After 6 weeks of evaluation, themaxillary molars were banded and a bite plate deliv-ered. The patient’s home care and cooperation im-proved significantly over the next few weeks. Subse-quently, the mandibular arch was banded with IBDbidimensional edgewise appliances: anterior .018 �.025-in and posterior .022 � .028-in bracket slots.Sequentially larger wires were used to level the man-dibular arch, and a push coil was used to open space forthe mandibular left second premolar. Sectional .014-instainless steel archwire was used to level the maxillaryanterior teeth followed by a .016 � .022-in intrusion 2� 4 arch. The patient wore cervical headgear to distalizethe maxillary molars. The remaining maxillary teeth werebonded, and cross elastics were used to upright the man-dibular posterior teeth while the maxillary bite plate wastrimmed on the palatal to allow for arch coordination.
The objectives of increasing lower anterior facialheight and decreasing gingival display were obtained.Facial esthetics were dramatically improved on smil-ing. The patient has 90% maxillary incisal display withno gingival display upon smiling. Her profile did notchange significantly.
RETENTION
A maxillary Hawley retainer was delivered, and the
photographs.
tment
patient was instructed to wear it full time for the first 6
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 132, Number 2
Fooladi et al 257
months and nights thereafter. The mandibular fixed 3 �3 retainer was bonded on the canines only. The patientwas instructed on home care and maintenance of theretainers. Her third molars are developing, and she was
Fig 7. Posttrea
Fig 8. Posttreatment cephalometric tracing.
referred to an oral surgeon for evaluation for removal.
FINAL EVALUATION OF TREATMENT
A significant improvement in the occlusion wasachieved; the objectives of increasing the verticaldimension and relieving the deep impinging overbitewere attained (Fig 6). The Brodie bite on the leftposterior segment was resolved via arch coordina-tion. Gingival display upon smiling was also re-duced. Our goal was to level the maxillary andmandibular incisors forward. This result was ex-pected with the crowding and curve of Spee that were
t dental casts.
Fig 9. Posttreatment panoramic radiograph.
tmen
present. To prevent proclination of the maxillary and
American Journal of Orthodontics and Dentofacial OrthopedicsAugust 2007
258 Fooladi et al
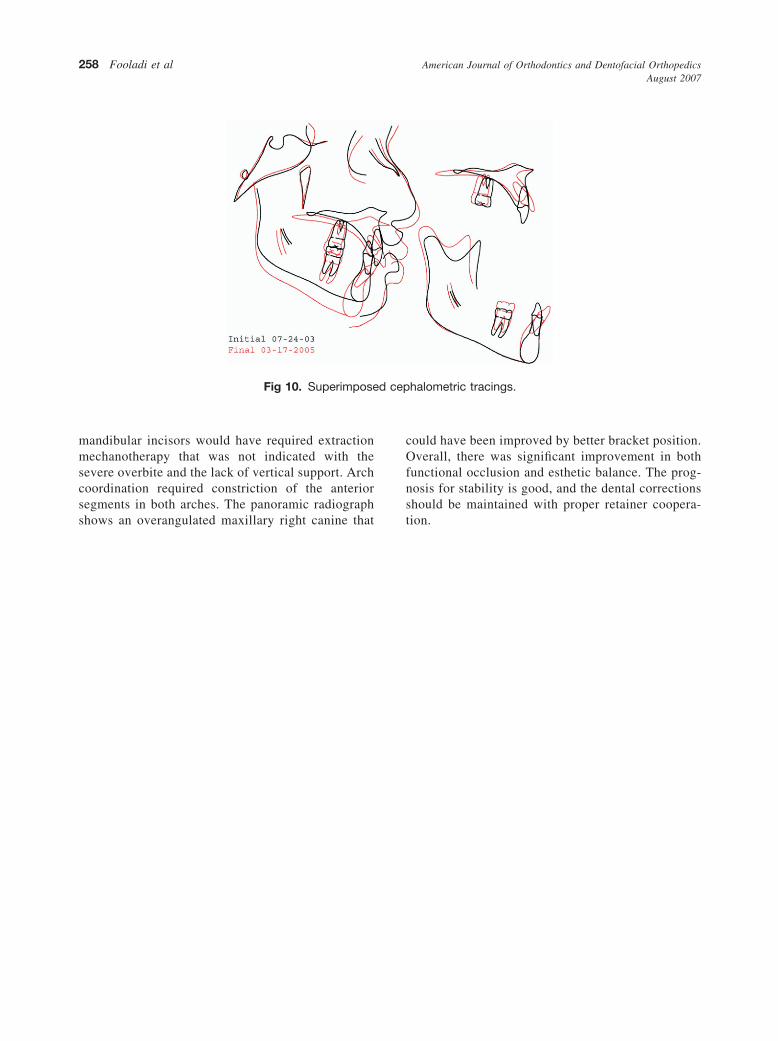
mandibular incisors would have required extractionmechanotherapy that was not indicated with thesevere overbite and the lack of vertical support. Archcoordination required constriction of the anteriorsegments in both arches. The panoramic radiograph
Fig 10. Superimpose
shows an overangulated maxillary right canine that
could have been improved by better bracket position.Overall, there was significant improvement in bothfunctional occlusion and esthetic balance. The prog-nosis for stability is good, and the dental correctionsshould be maintained with proper retainer coopera-
halometric tracings.
d cep
tion.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 132, Number 2