Centennial Care Reporting Instructions Utilization Management – Report #41 Utilization Management Report - #41 Rev. v6 2014-12 Page 1 of 58 Report Objective To monitor unduplicated member utilization of behavioral health (BH) services, physical health (PH) services and long-term care (LTC) services and the corresponding managed care organization (MCO) paid amounts for the services. The report captures member utilization by date of service for paid claims. General Instructions The managed care organization (MCO) is required to submit the Utilization Management (UM) report on a quarterly basis. This report is due on April 30, July 30, October 30, and January 30 of each year. An annual supplement is also required for this report. The annual supplement is a restatement of all four quarterly report submissions related to the reporting periods within the particular calendar year. The restated reports are to reflect data as of March 30 of the following year, thus benefiting from the additional paid claims run out. Please adhere to the following reporting periods and due dates. Quarter Reporting Period Report Due Date 1 January 1 – March 31 April 30 2 April 1 – June 30 July 30 3 July 1 – September 30 October 30 4 October 1 – December 31 January 30 Annual Supplement January 1 – December 31 April 30 (following year) An Excel workbook is provided as a separate attachment for submission. Quantitative data and any qualitative data must be entered in the Excel workbook. The MCO must ensure that data is entered in all fields. The report will be considered incomplete if any field is left blank. Use “ND” if there is no data available to report. Use “N/A” if the data field is not applicable. All formulas provided in the workbook are locked and shall not be altered by the MCO. An electronic version of the report in Excel must be submitted to the New Mexico Human Services Department (HSD) by the report due date listed above. The report shall be submitted via the State’s secure DMZ FTP site. The date of receipt of the electronic version will serve as the date of receipt for the report. To assist MCOs with the use of the template, all cells within the template are viewable. This allows the user to move the cursor into any cell of the template and enables the user to see the formulas in the cells that calculate automatically. Although certain cells are locked and protected, the user’s ability to view the formulas should assist in the MCO’s understanding of the template and calculations performed. It is important to note that when populating the templates with data, users are not to use the “cut and paste” function in Excel, as this may cause errors to the cell formulas. Additionally, certain cells have been shaded and locked to prevent data entry where data is not required or not applicable to the particular item or category. Please note that the majority of this report captures information based on paid claims with dates of service within each quarterly reporting period. For sections of this report that capture data for multiple reporting periods (both current and prior quarters), the MCO is required to restate previously submitted data. Reporting data in this manner will take advantage of the most recent look at the claims paid data, thus benefiting from the additional months of claims paid run out. Amounts entered into this report are to be based on actual data and exclude any estimates or accruals.
Transcript
Centennial Care Reporting InstructionsUtilization Management – Report #41
Report ObjectiveTo monitor unduplicated member utilization of behavioral health (BH) services, physical health (PH)services and long-term care (LTC) services and the corresponding managed care organization (MCO)paid amounts for the services. The report captures member utilization by date of service for paidclaims.
General InstructionsThe managed care organization (MCO) is required to submit the Utilization Management (UM) report on aquarterly basis. This report is due on April 30, July 30, October 30, and January 30 of each year. Anannual supplement is also required for this report. The annual supplement is a restatement of all fourquarterly report submissions related to the reporting periods within the particular calendar year. Therestated reports are to reflect data as of March 30 of the following year, thus benefiting from the additionalpaid claims run out. Please adhere to the following reporting periods and due dates.
Quarter Reporting Period Report Due Date1 January 1 – March 31 April 302 April 1 – June 30 July 303 July 1 – September 30 October 304 October 1 – December 31 January 30
AnnualSupplement
January 1 – December 31 April 30 (following year)
An Excel workbook is provided as a separate attachment for submission. Quantitative data and anyqualitative data must be entered in the Excel workbook. The MCO must ensure that data is entered in allfields. The report will be considered incomplete if any field is left blank. Use “ND” if there is no dataavailable to report. Use “N/A” if the data field is not applicable. All formulas provided in the workbook arelocked and shall not be altered by the MCO. An electronic version of the report in Excel must besubmitted to the New Mexico Human Services Department (HSD) by the report due date listed above.The report shall be submitted via the State’s secure DMZ FTP site. The date of receipt of the electronicversion will serve as the date of receipt for the report.
To assist MCOs with the use of the template, all cells within the template are viewable. This allows theuser to move the cursor into any cell of the template and enables the user to see the formulas in the cellsthat calculate automatically. Although certain cells are locked and protected, the user’s ability to view theformulas should assist in the MCO’s understanding of the template and calculations performed. It isimportant to note that when populating the templates with data, users are not to use the “cut and paste”function in Excel, as this may cause errors to the cell formulas. Additionally, certain cells have beenshaded and locked to prevent data entry where data is not required or not applicable to the particular itemor category.
Please note that the majority of this report captures information based on paid claims with dates ofservice within each quarterly reporting period. For sections of this report that capture data for multiplereporting periods (both current and prior quarters), the MCO is required to restate previously submitteddata. Reporting data in this manner will take advantage of the most recent look at the claims paid data,thus benefiting from the additional months of claims paid run out. Amounts entered into this report are tobe based on actual data and exclude any estimates or accruals.
Centennial Care Reporting InstructionsUtilization Management – Report #41
The MCO shall submit the electronic version of the report using the following file name labeling format:MCO Name.HSD41.Q1CY14.v1. With each report submission, please change the reporting periodreference (e.g., Q1), the calendar year (e.g., CY14), and the version number (e.g., v1), as appropriate.
The MCO’s name, the reporting period, and the report run date must be entered on the top portion of thefirst worksheet in the report. The report run date refers to the date that the data was retrieved from theMCO’s system. The dates and MCO name entered on the first worksheet will automatically appear on thetop of all other worksheets of the report. The start and end of the reporting period must be entered in theformat illustrated below:
Attestation and PenaltiesThe MCO shall ensure that all data is accurate and appropriately formatted in the workbook prior tosubmitting the report. Per Section 7.3 of the Centennial Care contract, failure to submit accurate reportsand/or failure to submit properly formatted reports in accordance with the contract may result in liquidateddamages of $5,000 per report, per occurrence.
The MCO shall include a signed attestation with each report. Failure to submit a signed attestation formby the report due date will result in the entire report being late. Per Section 7.3 of the Centennial Carecontract, failure to submit timely reports in accordance with the contract may result in liquidated damagesof $1,000 per report, per calendar day. The $1,000 per calendar day damage amounts will double everyten calendar days.
Related Contract Requirements1. Section 4.21 – Reporting Requirements 2. Section 7.3 – Failure to Meet Agreement
Requirements
DefinitionsEVALUATION HIERARCHY CRITERIA
When completing this report, the MCO must apply the program area-specific service categorizationcriteria by each program area beginning with the Behavioral Health program area, followed by the LTCprogram area, and ending with the PH program area. See Addendum A (Behavioral Health Codes andCategories), Addendum B (Physical Health Codes and Categories), and Addendum C (Long-Term CareCodes and Categories) for tables detailing the program area-specific service categorization criteria.
When assigning data to one of the three distinct program areas, the MCO is to follow the guidelines belowstarting with BH:
1. Behavioral Health Program Member Utilizationa. Assign data to the BH program area by applying the criteria detailed in the table below for
identifying behavioral health services.b. Assign BH program area data to the designated BH service categories using the provider types,
Reporting Period 1/1/2014MCO NameReport Run Date
through 3/31/2014MCO A4/1/2014
Centennial Care Reporting InstructionsUtilization Management – Report #41
service codes (with modifiers when applicable), and any other distinguishing criteria detailedwithin Addendum A.
c. BH add-on CPT codes are to be used in conjunction with the other CPT codes identified withineach applicable BH category. BH add-on CPT codes are not to be reported as stand-aloneservices.
2. Long-Term Care Program Member Utilizationa. Assign data to the LTC program area according to the provider types, service codes (and
modifiers as applicable), and any other distinguishing criteria detailed within Addendum C.b. Assign LTC program area data to the designated LTC service categories using the provider
types, service codes (with modifiers when applicable), and any other distinguishing criteriadetailed within Addendum C.
3. Physical Health Program Member Utilizationa. Assign data to the PH program area according to the provider types, service codes, and any
other distinguishing criteria detailed within Addendum B.b. Assign PH program area data to the designated PH service categories using the provider types,
service codes, and any other distinguishing criteria detailed within Addendum B.
Note that all program area/service category/service-specific utilization data is to be reported mutuallyexclusive of any other utilization reported within this report. Once data has been assigned to a particularservice within a program area-specific service category grouping, it is not to be reported within any otherprogram area categories within this report.
Value added services must be excluded from the data included within this report.
IDENTIFYING BEHAVIORAL HEALTH SERVICES
Be certain to report a behavioral service only once even if the service meets more than one of thefollowing definitions for identifying behavioral health services:
1. Exclude any billing provider type 363 and 344 (community based services and waiver services)
2. Include any service for which a billing or rendering provider is one of the following:
a. Type 301, 302, 303 (physicians) with specialty 026, 047, 050 (psychiatry, child psychiatry, oraddictionologist).
b. Type 316 CNP with specialty 097 (psychiatric).c. One of the following provider types:
204 Inpatient – Psych. Unit in General Hospital205 Inpatient – Freestanding Psych. Hospital216 Accredited Residential Facility (ARTC)217 Non-accredited Residential Facility (RTC)218 Treatment Foster Care I & II (TFC I & TFC II)219 Residential Non-JACHO Group Home (GH)343 Methadone Clinic
Centennial Care Reporting InstructionsUtilization Management – Report #41
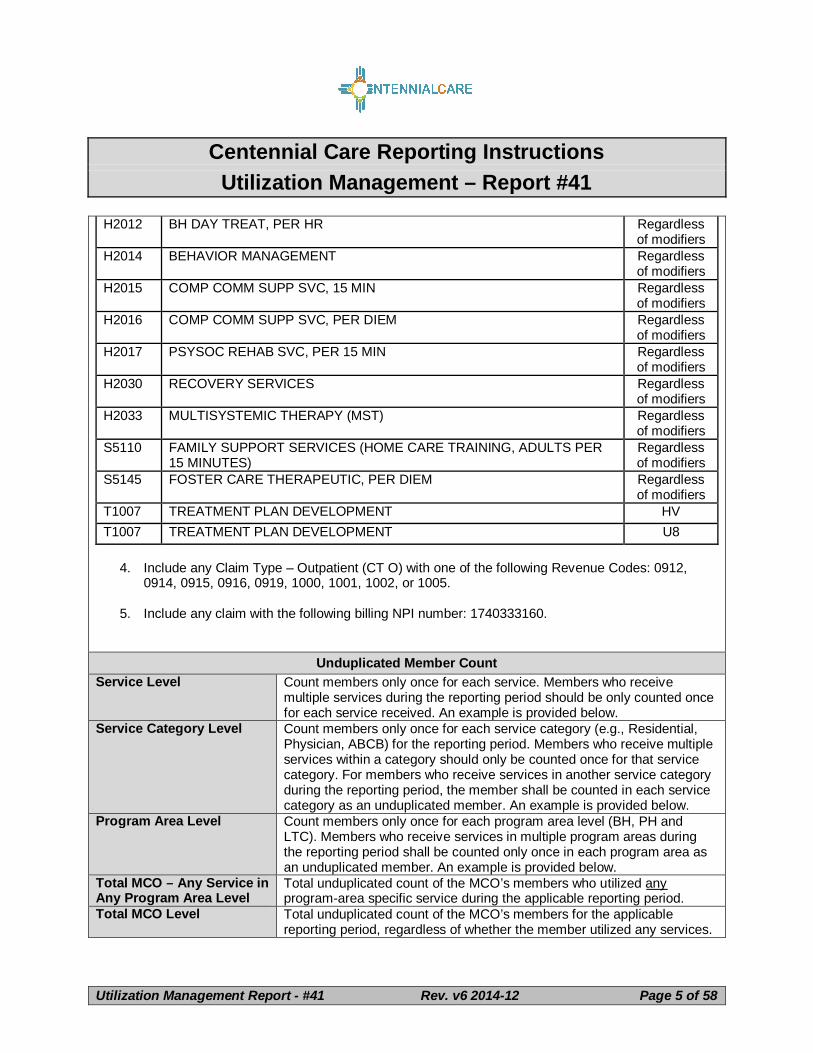
H0019 BEHAVIORAL HEALTH; LONG-TERM RESIDENTIAL (NON-MEDICAL,NON-ACUTE CARE IN A RESIDENTIAL TREATMENT PROGRAMWHERE STAY IS TYPICALLY LONGER THAN 30 DAYS), WITHOUTROOM AND BOARD, PER DIEM
S5110 FAMILY SUPPORT SERVICES (HOME CARE TRAINING, ADULTS PER15 MINUTES)
Regardlessof modifiers
S5145 FOSTER CARE THERAPEUTIC, PER DIEM Regardlessof modifiers
T1007 TREATMENT PLAN DEVELOPMENT HVT1007 TREATMENT PLAN DEVELOPMENT U8
4. Include any Claim Type – Outpatient (CT O) with one of the following Revenue Codes: 0912,0914, 0915, 0916, 0919, 1000, 1001, 1002, or 1005.
5. Include any claim with the following billing NPI number: 1740333160.
Unduplicated Member CountService Level Count members only once for each service. Members who receive
multiple services during the reporting period should be only counted oncefor each service received. An example is provided below.
Service Category Level Count members only once for each service category (e.g., Residential,Physician, ABCB) for the reporting period. Members who receive multipleservices within a category should only be counted once for that servicecategory. For members who receive services in another service categoryduring the reporting period, the member shall be counted in each servicecategory as an unduplicated member. An example is provided below.
Program Area Level Count members only once for each program area level (BH, PH andLTC). Members who receive services in multiple program areas duringthe reporting period shall be counted only once in each program area asan unduplicated member. An example is provided below.
Total MCO – Any Service inAny Program Area Level
Total unduplicated count of the MCO’s members who utilized anyprogram-area specific service during the applicable reporting period.
Total MCO Level Total unduplicated count of the MCO’s members for the applicablereporting period, regardless of whether the member utilized any services.
Centennial Care Reporting InstructionsUtilization Management – Report #41
Example The following is an example for determining unduplicated member countsfor a member receiving physical health services.
An MCO member was seen at the Primary Care Physician’s (PCP’s)office and was transported via emergency ground ambulance to an acutecare Diagnosis Related Group (DRG) hospital with acute abdominal pain.The member was seen in the emergency room by an emergency room(ER) physician. The physician ordered an abdominal ultrasound and acomplete blood count (CBC). When the results returned, the patient wasdiagnosed with acute appendicitis. A surgical consult was done, and themember was scheduled for surgery as an out-patient. A chest x-ray, EKGand blood type and cross were ordered prior to surgery.
The member would be counted as an unduplicated member at thefollowing levels:
Section I: SummaryThis section of the report provides summary information of cumulative and aggregate data captured inSections III through V of the report. The summary section consists of multiple tabs that contain tables andcharts of aggregated data. This section of the report is useful for high level analysis and monitoringcumulative utilization of each program area of the report. The MCO’s name, the reporting period, and thereport run date must be entered on the top portion of the first worksheet. Data entry is not required in anyother field in this section of the report.
Summary - YTD Charts
Two separate unduplicated member counts are required to be input by the MCO within thissection of the report.
Centennial Care Reporting InstructionsUtilization Management – Report #41
Ensure that the “Summary – YTD Charts” tab is selected. Enter the following unduplicated membercounts within the two yellow-shaded cells within the “Program Area – YTD Unduplicated Member Count”table.
1. Within the row labeled “ANY”, enter the total unduplicated count of the MCO’s members whoutilized any program-area specific service during the applicable reporting period.
2. Within the row labeled “TOTAL MCO”, enter the total unduplicated count of the MCO’s membersfor the applicable reporting period, regardless of whether the member utilized any services.
Please note that these two cells requiring data entry will only display the yellow shading if there are nocounts entered within the respective cells. Once a count is entered in the cell, the yellow shading will nolonger be visible.
Section II: AnalysisBefore entering data in the workbook, ensure that the “Analysis” tab is selected. This section of the reportcollects qualitative analysis regarding the utilization of services. Please respond to the following questionsin the analysis worksheet, taking into consideration the data reported for the reporting period. For eachquestion, identify any changes compared to previous reporting periods and trends over time and providean explanation of the identified changes. Additionally, describe any action plans or performanceimprovement activities addressing any negative changes found during the current reporting period orprevious reporting periods.
1. Identify and explain any trends observed within the reported data. As part of the explanation,describe any action steps/performance improvement measures to be taken to address thechanges. How does this compare to previous reporting periods? Please be specific to eachprogram area (Behavioral Health, Physical Health, and Long-Term Care).
2. For each program area (Behavioral Health, Physical Health, and Long-Term Care), discuss anyabnormalities, irregularities or exceptions that were observed in the quarter. An explanation is tobe provided that describes any action steps to be taken to address the issues. How does thiscompare to previous reporting periods?
3. Identify and explain any system changes that might have affected the reported data. Theexplanation should address the impact of the change on reported data in the current reportingperiod and the expected impacts to data to be reported in the next report submission. How doesthis compare to previous reporting periods? Please be specific to each program area (BehavioralHealth, Physical Health, and Long-Term Care).
4. Provide any additional information pertinent to the quarter. Please be specific to each programarea (Behavioral Health, Physical Health, and Long-Term Care).
5. Please list all services that were not utilized (0 in the total number of services row) for thereporting period. Please specify the applicable program area (Behavioral Health, Physical Health,and Long-Term Care), service category, and service. How does this compare to previousreporting periods?
6. Identify any strategies the MCO is using to address the lack of utilization associated with theservices identified in Question 5 above. Please be specific to each program area (BehavioralHealth, Physical Health, and Long-Term Care).
Section III: Behavioral Health UtilizationBefore entering data in the workbook, ensure that the “BH” tab is selected. This section of the reportcaptures utilization information on behavioral health services by each type of service/category based on
Centennial Care Reporting InstructionsUtilization Management – Report #41
the date of service for paid claims. The services captured in this report include only services billed by aCPT, revenue or Healthcare Common Procedure Code (HCPC).
This section captures quarterly and year-to-date (YTD) data for each service and service categoryoutlined below. The MCO is required to restate previously submitted data. Reporting data in this mannerwill take advantage of the most recent look at the claims paid data, thus benefiting from the additionalmonths of claims paid run out.
PROGRAM AREA LEVEL – TOTAL BH – ALL CATEGORIES – ALL AGES
Row Header Row DescriptionTotal Number of UnduplicatedMembers Receiving Services atProgram Level (BH)
8 The total number of unduplicated members who receivedBH services during the reporting period based on the dateof service for paid claims. The MCO must manually enterdata for each reporting period and calculate the YTD count.The MCO must restate data for previous report periods.
Total Dollar Amount All ServiceCategories at Program Level(BH)
9 The total dollar amount expended on BH services duringthe reporting period based on date of service for paidclaims. Data entry is not required in this field.
PROGRAM AREA LEVEL – TOTAL BH – ALL CATEGORIES – AGE BREAKDOWN
Row Header Row DescriptionTotal Number of UnduplicatedMembers Receiving Services atProgram Level (BH)
14 The total number of unduplicated members (per each agegroup) who received BH services during the reportingperiod based on date of service for paid claims. The MCOmust manually enter data for each reporting period andcalculate the YTD count. The MCO must restate data forprevious report periods.
Total Dollar Amount All ServiceCategories at Program Level(BH)
15 The total dollar amount expended (per each age group) onBH services during the reporting period based on date ofservice for paid claims. Data entry is not required in thisfield.
For the Behavioral Health Utilization section only, the MCO must stratify data by age groups and servicecategories.
Age Groups
Member age classifications are based on the age of the member at the end of the reporting period.
Column Header Column DescriptionUnder 18 B,G,L,Q Members under the age of 18 as of the last day of the
reporting period.18-20 C,H,M,R Members between the age of 18 and 20 as of the last day
of the reporting period.
Centennial Care Reporting InstructionsUtilization Management – Report #41
Column Header Column Description21-64 D,I,N,S Members between the age of 21 and 64 as of the last day
of the reporting period.65+ E,J,O,T Members 65 years or older as of the last day of the
reporting period.Total (Quarter) F,K,P,U These columns capture a quarterly total for each reporting
period. The MCO must restate the quarterly columns for anunduplicated count of members. All other quarterlycalculations do not require data entry from the MCO.
YTD V, W, X,Y, Z
These columns capture the year-to-date (YTD) totals foreach service and each age category. The MCO mustrestate the YTD columns for an unduplicated count ofmembers. All other YTD calculations do not require dataentry from the MCO.
Services and Service Categories
The table below outlines the service categories for this section of the report. Each service categorycontains a list of services relevant to the service category. At the end of each service category is asection that automatically calculates the total dollar amount paid for services per service category foreach age group and reporting period. The MCO is required to manually populate the total unduplicatedmember count for each service and service category level for each reporting period and YTD. Refer to thedefinitions section on calculating the unduplicated member count at the service category level.
Note: YTD unduplicated member count is not a summation of multiple quarters. The YTD must bedetermined independently from quarterly totals. See definition section for additional guidance.
154-198 BH services classified as intensive outpatientservices.
Recovery Services Category 202-262 BH services classified as recovery services.Outpatient Services Category 266-622 BH services classified as outpatient services.
Each service listed in Column A requires the MCO to report the following information for each reportingperiod, based on the age of the member at the end of the reporting period and the date of service of paidclaims.
Note: The MCO must refer to Addendum A “Behavioral Health Codes and Categories” todetermine the appropriate unit calculation and codes for each service.
Row Header DescriptionTotal Number of Unduplicated MembersReceiving Service
The total number of unduplicated members receiving theservice for each age group and reporting period. The MCO
Centennial Care Reporting InstructionsUtilization Management – Report #41
Row Header Descriptionmust report an unduplicated count of members for eachservice based on date of service for paid claims. Member ageclassifications are based on the age of the member at the endof the reporting period.
Total Number of Services The total number of services rendered based on a normalizedsum of service units for each age group and reporting period.Service units are converted into common unit types using themultiplier factor in Addendum A.
It is critical the MCO use correct unit calculations foraccurate reporting.
Service units based on minutes or 15 minute increments mustbe converted to hours when indicated in the unit value column.For example; one 15-minute unit, when instructed to bereported in the unit of an hour, would be reported as .25 units.
Service units based on days or per diem are reported as “perdiem” as indicated in the unit value column which is thenumber of days, not including a discharge day for an inpatientor residential stay.
Other unit types (session, visit and product) are reported asindicated in the unit value column.
[Unit Type] Per Client Receiving Service The total number of services divided by the total number ofunduplicated members receiving services for each age groupand reporting period. Data entry is not required in this field.
Note: The unit of measurement may differ from one service toanother. It is imperative the MCO reviews Addendum A todetermine the correct unit calculation for each service.
Total Dollar Amount for Service(s) The total MCO paid dollar amount for the service for each agegroup and reporting period.
Section IV: Physical Health UtilizationBefore entering data in the workbook, ensure that the “PH” tab is selected. This section of the reportcaptures utilization information on physical health services by each type of service/category based on thedate of service for paid claims. The services captured in this report include only services billed by aCPT, Current Dental Terminology (CDT), revenue or HCPC code.
This section captures quarterly and YTD data for each service and service category outlined below. TheMCO is required to restate previously submitted data. Reporting data in this manner will take advantageof the most recent look at the claims paid data, thus benefiting from the additional months of claims paidrun out.
Centennial Care Reporting InstructionsUtilization Management – Report #41
Row Header Row DescriptionTotal Number of UnduplicatedMembers Receiving Services atProgram Level (PH)
8 The total number of unduplicated members who receivedPH services during the reporting period based on the dateof service for paid claims. The MCO must manually enterdata for each reporting period and calculate the YTD count.The MCO must restate data for previous report periods.
Total Dollar Amount All ServiceCategories at Program Level(PH)
9 The total dollar amount expended on PH services duringthe reporting period based on date of service for paidclaims. Data entry is not required in this field.
Services and Service Categories
The table below outlines the service categories for this section of the report. Each service categorycontains a list of services relevant to the service category. At the end of each service category is asection that automatically calculates the total dollar amount paid for services per service category for thereporting period. The MCO is required to manually populate the total unduplicated member count for eachservice and service category level for each reporting period and YTD. Refer to the definitions section oncalculating the unduplicated member count at the service category level.
Note: YTD unduplicated member count is not a summation of multiple quarters. The YTD must bedetermined independently from quarterly totals. See definition section for additional guidance.
Row Header RowNumber Description
Hospital Services Category 12-96 PH services classified as hospital services.Other Facilities and ServicesCategory
100-144 PH services classified as other facilities and services.
Physician Services Category 148-192 PH services that are classified as physician services.Other Healthcare ServicesCategory
196-376 PH services classified as other healthcare physicianservices.
404-592 All services classified as transportation services.
Each service listed in Column A requires the MCO to report the following information for each reportingperiod, based on the date of service of paid claims.
Note: The MCO must refer to Addendum B “Physical Health Codes and Categories” to determinethe appropriate unit calculation and codes for each service.
Row Header DescriptionTotal Number of Unduplicated MembersReceiving Service
The total number of unduplicated members receiving theservice for each reporting period. The MCO must report anunduplicated count of members for each service based on
Centennial Care Reporting InstructionsUtilization Management – Report #41
Row Header Descriptiondate of service for paid claims.
Total Number of Services The total number of services rendered based on a normalizedsum of service units for each reporting period. Service unitsare converted into common unit types using the multiplierfactor in Addendum B.
It is critical the MCO use correct unit calculations foraccurate reporting.
Service units based on minutes or 15 minute increments mustbe converted to hours when indicated in the unit value column.For example; one 15-minute unit, when instructed to bereported in the unit of an hour, would be reported as .25 units.
Service units based on days or per diem are reported as “perdiem” as indicated in the unit value column which is thenumber of days, not including a discharge day for an inpatientor residential stay.
Other unit types (session, visit, product, encounter, admission,diagnostic test, 1-way transport, mile, meal and payment) arereported as indicated in the unit value column.
[Unit Type] Per Client Receiving Service The total number of services divided by the total number ofunduplicated members receiving services for each reportingperiod. Data entry is not required in this field.
Note: The unit of measurement may differ from one service toanother service. It is imperative the MCO reviews AddendumB to determine the correct unit calculation for each service.
Total Dollar Amount for Service(s) The total MCO paid dollar amount for the service for eachreporting period.
Section V: Long-Term Care Benefit UtilizationBefore entering data in the workbook, ensure that the “LTC” tab is selected. This section of the reportcaptures utilization information on LTC services by each type of service/category based on the date ofservice for paid claims. The services captured in this report include only services billed by a CPT,revenue or HCPC code.
This section captures quarterly and YTD data for each service and service category outlined below. TheMCO is required to restate previously submitted data. Reporting data in this manner will take advantageof the most recent look at the claims paid data, thus benefiting from the additional months of claims paidrun out.
PROGRAM AREA LEVEL – TOTAL LTC – ALL CATEGORIES
Row Header Row Description
Centennial Care Reporting InstructionsUtilization Management – Report #41
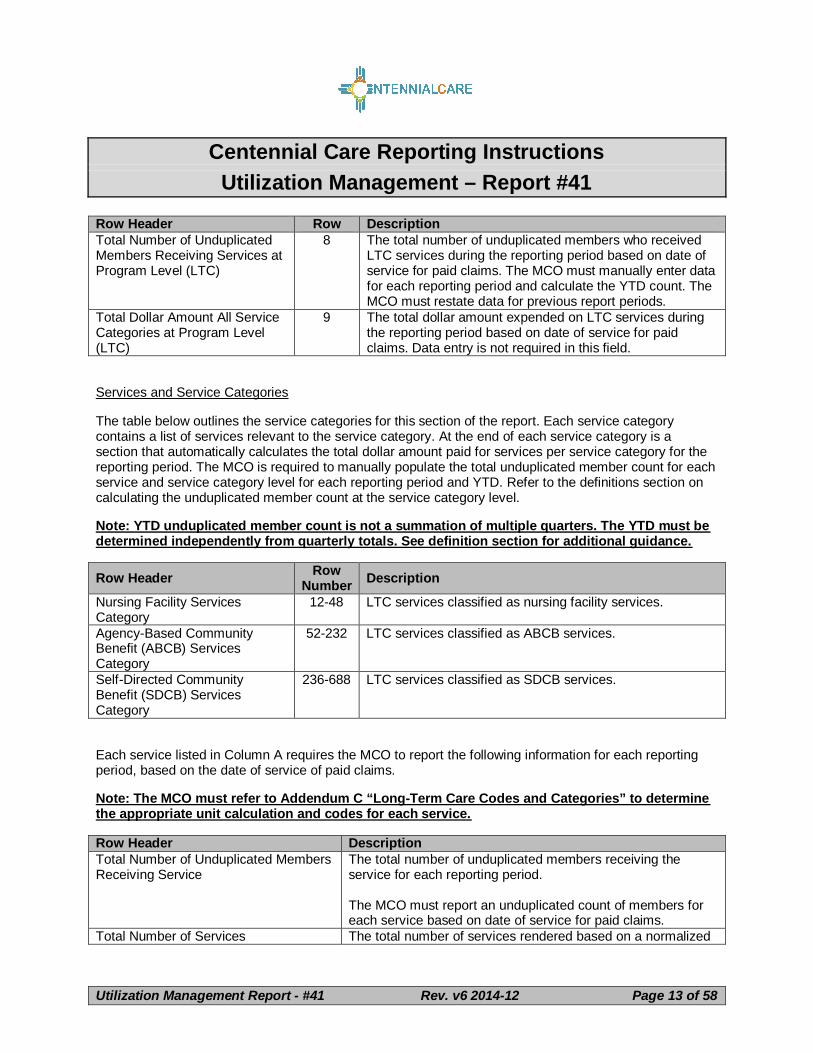
Row Header Row DescriptionTotal Number of UnduplicatedMembers Receiving Services atProgram Level (LTC)
8 The total number of unduplicated members who receivedLTC services during the reporting period based on date ofservice for paid claims. The MCO must manually enter datafor each reporting period and calculate the YTD count. TheMCO must restate data for previous report periods.
Total Dollar Amount All ServiceCategories at Program Level(LTC)
9 The total dollar amount expended on LTC services duringthe reporting period based on date of service for paidclaims. Data entry is not required in this field.
Services and Service Categories
The table below outlines the service categories for this section of the report. Each service categorycontains a list of services relevant to the service category. At the end of each service category is asection that automatically calculates the total dollar amount paid for services per service category for thereporting period. The MCO is required to manually populate the total unduplicated member count for eachservice and service category level for each reporting period and YTD. Refer to the definitions section oncalculating the unduplicated member count at the service category level.
Note: YTD unduplicated member count is not a summation of multiple quarters. The YTD must bedetermined independently from quarterly totals. See definition section for additional guidance.
Row Header RowNumber Description
Nursing Facility ServicesCategory
12-48 LTC services classified as nursing facility services.
Each service listed in Column A requires the MCO to report the following information for each reportingperiod, based on the date of service of paid claims.
Note: The MCO must refer to Addendum C “Long-Term Care Codes and Categories” to determinethe appropriate unit calculation and codes for each service.
Row Header DescriptionTotal Number of Unduplicated MembersReceiving Service
The total number of unduplicated members receiving theservice for each reporting period.
The MCO must report an unduplicated count of members foreach service based on date of service for paid claims.
Total Number of Services The total number of services rendered based on a normalized
Centennial Care Reporting InstructionsUtilization Management – Report #41
Row Header Descriptionsum of service units for each reporting period. Service unitsare converted into common unit types using the multiplierfactor in Addendum C.
It is critical the MCO use correct unit calculations foraccurate reporting.
Service units based on minutes or 15 minute increments mustbe converted to hours when indicated in the unit value column.For example; one 15-minute unit, when instructed to bereported in the unit of an hour, would be reported as .25 units.
Service units based on days or per diem are reported as “perdiem” as indicated in the unit value column which is thenumber of days, not including a discharge day for an inpatientor residential stay.
Other unit types (visit, session, per service, per project, day,month, mile, and invoice) are reported as indicated in the unitvalue column.
[Unit Type] Per Client Receiving Service The total number of services divided by the total number ofunduplicated members receiving services for each reportingperiod. Data entry is not required in this field.
Note: The unit of measurement may differ from one service toanother. It is imperative the MCO reviews Addendum C todetermine the correct unit calculation for each service.
Total Dollar Amount for Service(s) The total MCO paid dollar amount for the service for eachreporting period.
Centennial Care Reporting InstructionsUtilization Management – Report #41
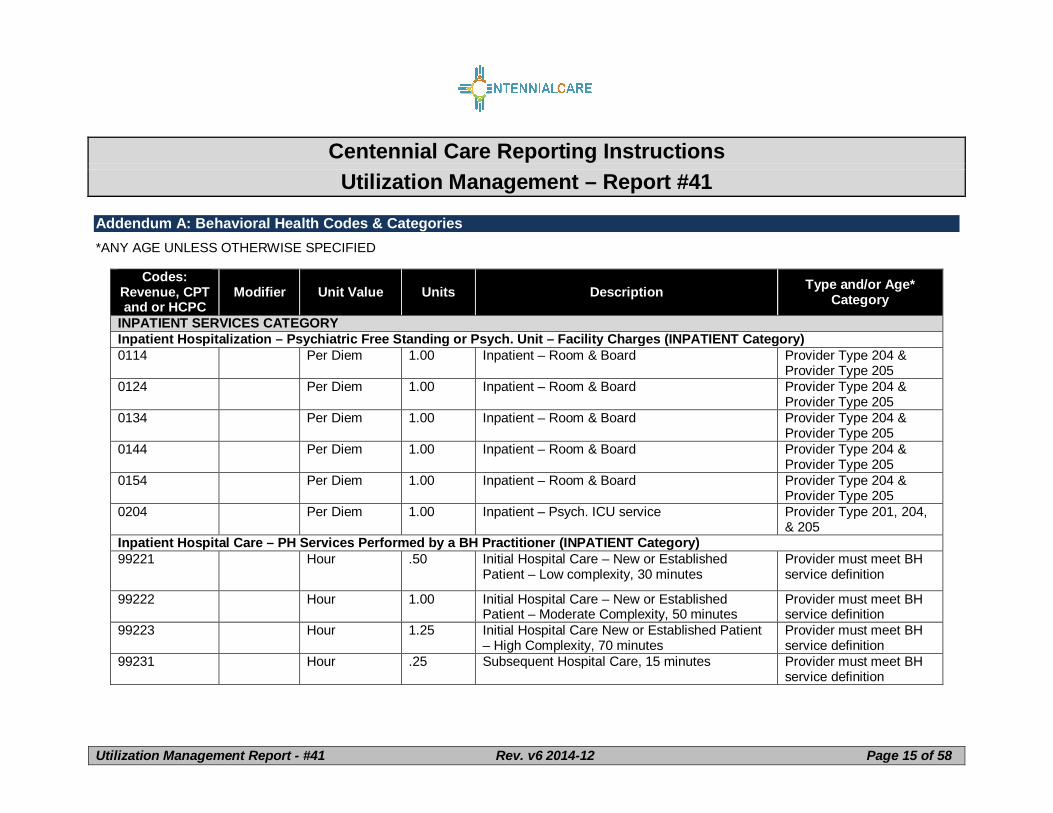
Addendum A: Behavioral Health Codes & Categories*ANY AGE UNLESS OTHERWISE SPECIFIED
Codes:Revenue, CPTand or HCPC
Modifier Unit Value Units Description Type and/or Age*Category
INPATIENT SERVICES CATEGORYInpatient Hospitalization – Psychiatric Free Standing or Psych. Unit – Facility Charges (INPATIENT Category)0114 Per Diem 1.00 Inpatient – Room & Board Provider Type 204 &
Provider Type 2050124 Per Diem 1.00 Inpatient – Room & Board Provider Type 204 &
Provider Type 2050134 Per Diem 1.00 Inpatient – Room & Board Provider Type 204 &
Provider Type 2050144 Per Diem 1.00 Inpatient – Room & Board Provider Type 204 &
Provider Type 2050154 Per Diem 1.00 Inpatient – Room & Board Provider Type 204 &
Provider Type 2050204 Per Diem 1.00 Inpatient – Psych. ICU service Provider Type 201, 204,
& 205Inpatient Hospital Care – PH Services Performed by a BH Practitioner (INPATIENT Category)99221 Hour .50 Initial Hospital Care – New or Established
Patient – Low complexity, 30 minutesProvider must meet BHservice definition
99222 Hour 1.00 Initial Hospital Care – New or EstablishedPatient – Moderate Complexity, 50 minutes
Provider must meet BHservice definition
99223 Hour 1.25 Initial Hospital Care New or Established Patient– High Complexity, 70 minutes
Provider must meet BHservice definition
99231 Hour .25 Subsequent Hospital Care, 15 minutes Provider must meet BHservice definition
Centennial Care Reporting InstructionsUtilization Management – Report #41
Initial Observation Care, Per Day – PH Services Performed by a BH Practitioner (INPATIENT Category) Inpatient Hospitalizationrules apply to this section99217 Per Diem 1.00 Observation and discharge day management Provider must meet BH
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
service definition99218 Per Diem 1.00 Initial Observation Care per day – Low Severity Provider must meet BH
service definition99219 Per Diem 1.00 Initial Observation Care per day – Moderate
SeverityProvider Must meet BHservice definition
99220 Per Diem 1.00 Initial Observation Care per day – High Severity Provider must meet BHservice definition
Inpatient Professional Services – Nursing Facility PH Services Performed by a BH Practitioner (INPATIENT Category)99304 Hour .50 Initial evaluation and management – Low
Severity, 25 minutesProvider must meet BHservice definition
Modifier Unit Value Units Description Type and/or Age*Category
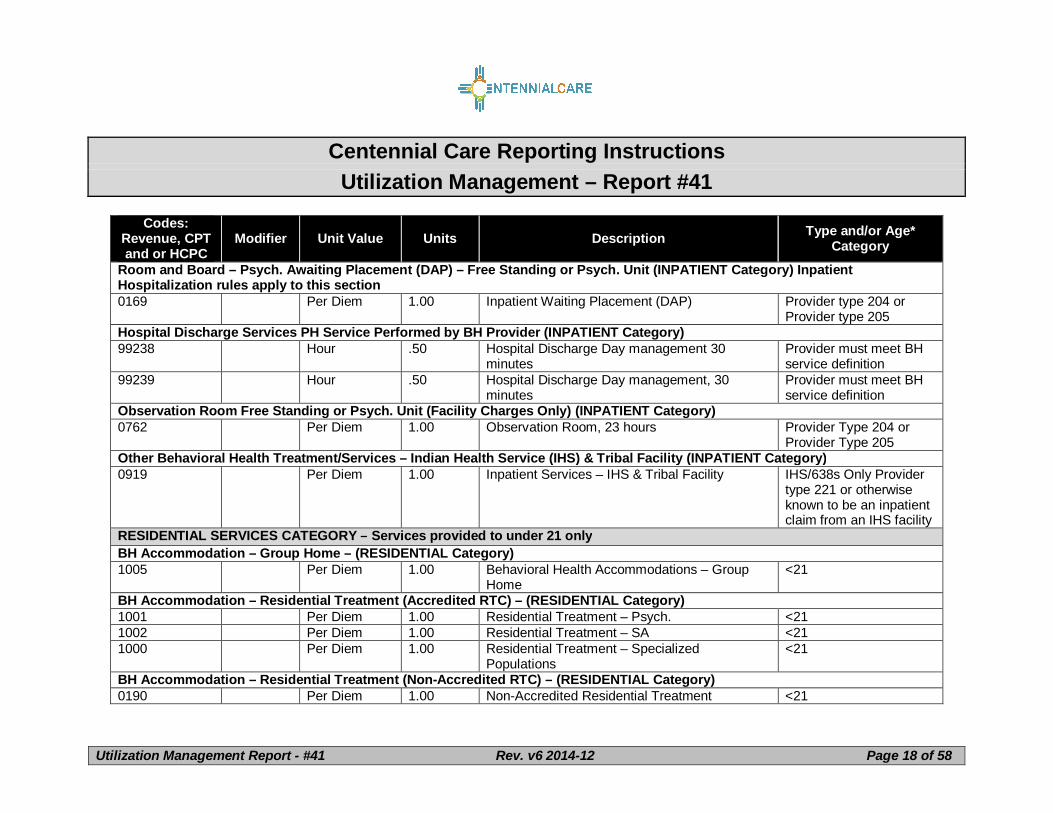
Room and Board – Psych. Awaiting Placement (DAP) – Free Standing or Psych. Unit (INPATIENT Category) InpatientHospitalization rules apply to this section0169 Per Diem 1.00 Inpatient Waiting Placement (DAP) Provider type 204 or
Provider type 205Hospital Discharge Services PH Service Performed by BH Provider (INPATIENT Category)99238 Hour .50 Hospital Discharge Day management 30
minutesProvider must meet BHservice definition
99239 Hour .50 Hospital Discharge Day management, 30minutes
Provider must meet BHservice definition
Observation Room Free Standing or Psych. Unit (Facility Charges Only) (INPATIENT Category)0762 Per Diem 1.00 Observation Room, 23 hours Provider Type 204 or
Provider Type 205Other Behavioral Health Treatment/Services – Indian Health Service (IHS) & Tribal Facility (INPATIENT Category)0919 Per Diem 1.00 Inpatient Services – IHS & Tribal Facility IHS/638s Only Provider
type 221 or otherwiseknown to be an inpatientclaim from an IHS facility
RESIDENTIAL SERVICES CATEGORY – Services provided to under 21 onlyBH Accommodation – Group Home – (RESIDENTIAL Category)1005 Per Diem 1.00 Behavioral Health Accommodations – Group
Home<21
BH Accommodation – Residential Treatment (Accredited RTC) – (RESIDENTIAL Category)1001 Per Diem 1.00 Residential Treatment – Psych. <211002 Per Diem 1.00 Residential Treatment – SA <211000 Per Diem 1.00 Residential Treatment – Specialized
Populations<21
BH Accommodation – Residential Treatment (Non-Accredited RTC) – (RESIDENTIAL Category)0190 Per Diem 1.00 Non-Accredited Residential Treatment <21
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
Include only Providertype 217 Non AccreditedRTC
0191 Per Diem 1.00 Residential Treatment Facility – DESERT HILLSGIRLS TREATMENT UNIT ONLY
<21Include only Providertype 216 Accredited RTC
BH Accommodation – Residential Treatment (Sub Acute) – (RESIDENTIAL Category)0194 Per Diem 1.00 Sub-acute Hospital-based residential services
(For a residential service in an accreditedresidential treatment center that meets criteriaestablished by the MCO for sub-acute care –provided only under managed care – notincluded in FFS.)
<21
Foster Care Therapeutic (TFC I) – (RESIDENTIAL Category)S5145 Per Diem 1.00 Foster Care, Therapeutic, Per Diem Level I <21
Foster Care Therapeutic (TFC II) – (RESIDENTIAL Category)S5145 U1 Per Diem 1.00 Foster Care, Therapeutic, Per Diem Level II <21
INTENSIVE OUTPATIENT SERVICES CATEGORYIntensive Outpatient Program Services – (INTENSIVE OUTPATIENT Category)H0015 Hour 1.00 Alcohol and/or Drug Services; Intensive
Outpatient Program (IOP) – Substance Abuseor Integrated MH/SA
The provider must be aCSA (type 446), a CMHC(type 443) or aBehavioral HealthAgency (type 432)
T1007 U6 Product 1.00 Alcohol and/or Substance Abuse Services, The provider must be a
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
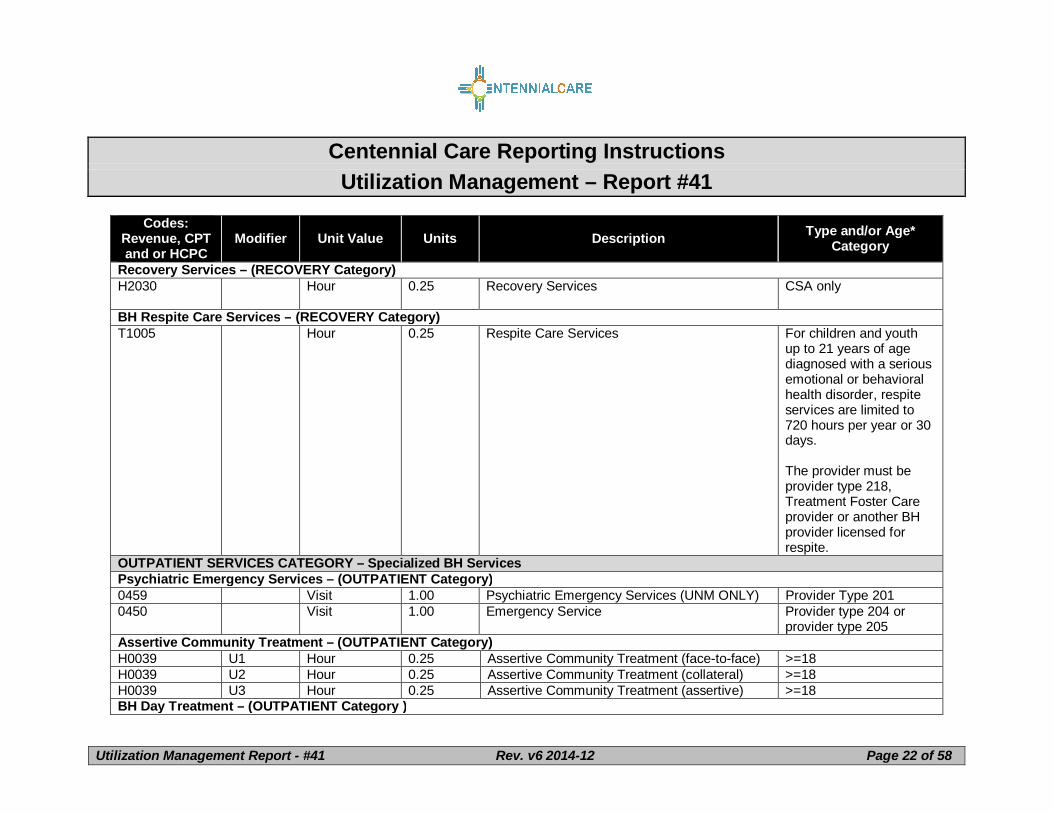
205RECOVERY SERVICES CATEGORYComprehensive Community Support Services – (RECOVERY Category)H2015 HM Hour 0.25 Comprehensive Community Support Services,
per 15 minutes; HM modifier is paraprofessionalor less than a bachelor’s)
Provider must meet BHservice definition
H2015 HN Hour 0.25 Comprehensive Community Support Services,per 15 minutes; HN modifier is bachelor’s level
Provider must meet BHservice definition
H2015 HO Hour 0.25 Comprehensive Community Support Services,per 15 minutes; HO is master’s level or above
Provider must meet BHservice definition
Behavior Management Skills Development (BMS) – (RECOVERY Category)H2014 Hour 0.25 Skills Training and Development, per 15
minutes – Behavior Management <21
Adaptive Skills Building – (RECOVERY Category)H2014 U1 Hour 0.25 Adaptive Skills Building Training and
Development, per 15 minutesPsychosocial Rehab SVCS-PSR – (RECOVERY Category)H2017 Hour 0.25 Psychosocial Rehab Services, per 15 minutes >=18H2017 HQ or
blank
HQ justemphasizes that it isa groupservice
Hour 0.25 Psychosocial Rehab Services, per 15 minutes –Group or classroom
>=18
Family Support Services – (RECOVERY Category)S5110 Hour 0.25 Family Support Services CSA only
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
H2012 Per Diem 1.00 Behavior Health Day Treatment, per hour <21MH Assessment & Initial Treatment Plan Non Physician – (OUTPATIENT Category)H0031 U8 Product 1.00 Mental Health Assessment by non-physician –
Multi-disciplinary assessment and initialtreatment plan
CSAs – any age
Not part of PSRBH Treatment Plan Update – (OUTPATIENT Category)T1007 U8 Product 1.00 Alcohol and/or Substance Abuse Services,
Treatment Plan Modification or Update MedicaidCSAs - any age
Not part of PSRBrief Office Visit for Purpose of Monitoring or Changing Drug – (OUTPATIENT Category)M0064 Hour 0.25 Brief Office Visit for Drug Monitoring/Changing
RxCrisis Intervention – (OUTPATIENT Category)H2011 U6 Hour 0.25 Crisis Intervention Services Not part of PSR.H2011 U6 & U2 Hour 0.25 Crisis Intervention Services (face-to-face) Not part of PSR.H2011 U6 & U3 Hour 0.25 Crisis Intervention Services (mobile) Not part of PSR.Suboxone Induction – (OUTPATIENT Category)H0033 Product 1.00 Induction Phase of Suboxone Treatment >=16
Other Behavioral Health Treatment/Services – Indian Health Service (IHS) & Tribal Facility – (OUTPATIENT Category )0919 Per Diem 1.00 Other Behavioral Health Treatment/Services –
IHS or 638 Tribal FacilityOther Behavioral Health Treatment/Service – Federally Qualified Health Centers (FQHC) or Rural Health Clinics (OUTPATIENTCategory)0919 Per Diem 1.00 Behavioral Health Treatment Services – FQHC
or RHCCrisis Intervention – PSR – (OUTPATIENT Category)H2011 U1 Hour 0.25 Crisis Intervention Services, per 15 minutes 18 and above
Centennial Care Reporting InstructionsUtilization Management – Report #41
90833 U8 Hour 0.50 Add on code 30 minutes with an E&M service 18 and above
90836 U8 Hour 0.75 Add on code 30 minutes with an E&M service 18 and above
90838 U8 Hour 1.00 Add on code 60 minutes with an E&M service 18 and above
MH Assessment & Initial Treatment Plan Non Physician – PSR – (OUTPATIENT Category)H0031 U8 Product 1.00 Mental Health Assessment by a non-physician
non-independently licensed in an agency –Medicaid PSRMaster Treatment Plan – annually assessed
18 and above
PSR
Specialized Consultation – PSR – (OUTPATIENT Category)90791 U8 Product 1.00 An initial evaluation provided by a non-physician 18 and above PSR90792 U8 Product 1.00 An initial evaluation provided by a physician 18 and above+ PSR90899 U8 Hour 0.25 Specialized consultation 18 and above+ PSRBH Treatment Plan Update – PSR – (OUTPATIENT Category)T1007 U8 Product 1.00 Alcohol and/or Substance Abuse Services,
Treatment Plan Modification or Update –Medicaid PSR
18 and above
Pharmacological Management – PSR – (OUTPATIENT Category)90863 U8 Hour 0.25 Add on Code – Pharmacological Management
when provided with psychotherapy18 and abovePSR
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
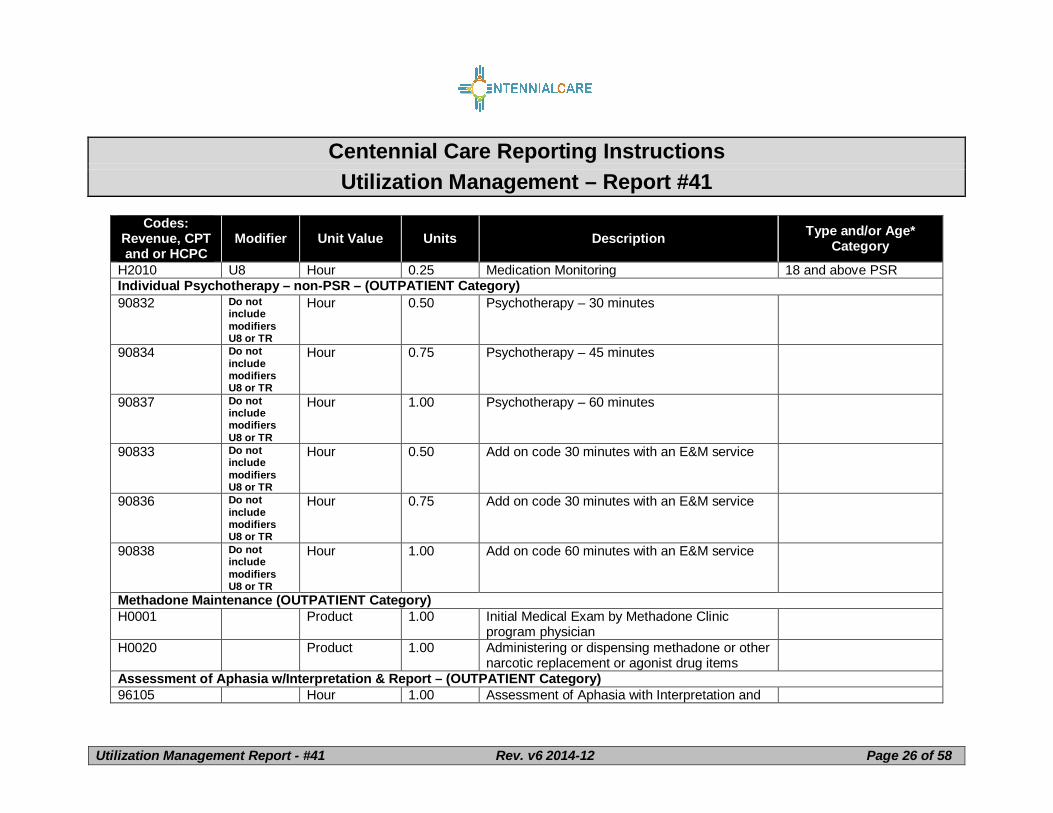
H2010 U8 Hour 0.25 Medication Monitoring 18 and above PSRIndividual Psychotherapy – non-PSR – (OUTPATIENT Category)90832 Do not
includemodifiersU8 or TR
Hour 0.50 Psychotherapy – 30 minutes
90834 Do notincludemodifiersU8 or TR
Hour 0.75 Psychotherapy – 45 minutes
90837 Do notincludemodifiersU8 or TR
Hour 1.00 Psychotherapy – 60 minutes
90833 Do notincludemodifiersU8 or TR
Hour 0.50 Add on code 30 minutes with an E&M service
90836 Do notincludemodifiersU8 or TR
Hour 0.75 Add on code 30 minutes with an E&M service
90838 Do notincludemodifiersU8 or TR
Hour 1.00 Add on code 60 minutes with an E&M service
Methadone Maintenance (OUTPATIENT Category)H0001 Product 1.00 Initial Medical Exam by Methadone Clinic
program physicianH0020 Product 1.00 Administering or dispensing methadone or other
narcotic replacement or agonist drug itemsAssessment of Aphasia w/Interpretation & Report – (OUTPATIENT Category)96105 Hour 1.00 Assessment of Aphasia with Interpretation and
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
Report, per hourDevelopmental Testing w/Interpretation & Report by BH Provider – (OUTPATIENT Category)96110 Hour 0.25 Developmental Testing with Interpretation and
Family Psychotherapy – (OUTPATIENT Category)90846 Do not
includemodifiersU8 or TR
Hour 0.25 Family Psychotherapy (without patient)
90847 Do notincludemodifiersU8 or TR
Hour 0.25 Family Medical Psychotherapy (with patient)
Functional Family Therapy – (OUTPATIENT Category)90846 HK Hour 0.25 Patient-Child/Adolescent
90847 HK Hour 0.25 Patient-Child/AdolescentGroup Psychotherapy – (OUTPATIENT Category)90853 Do not
includemodifiersU8 or TR
Hour 0.25 Group Psychotherapy (other than multi-family) Use 90853 in conjunctionwith 90785 for specifiedpatient when grouppsychotherapy includesinteractive complexity.
90785 Do notincludemodifiersU8 or TR
Hour 0.25 Interactive Group Psychotherapy
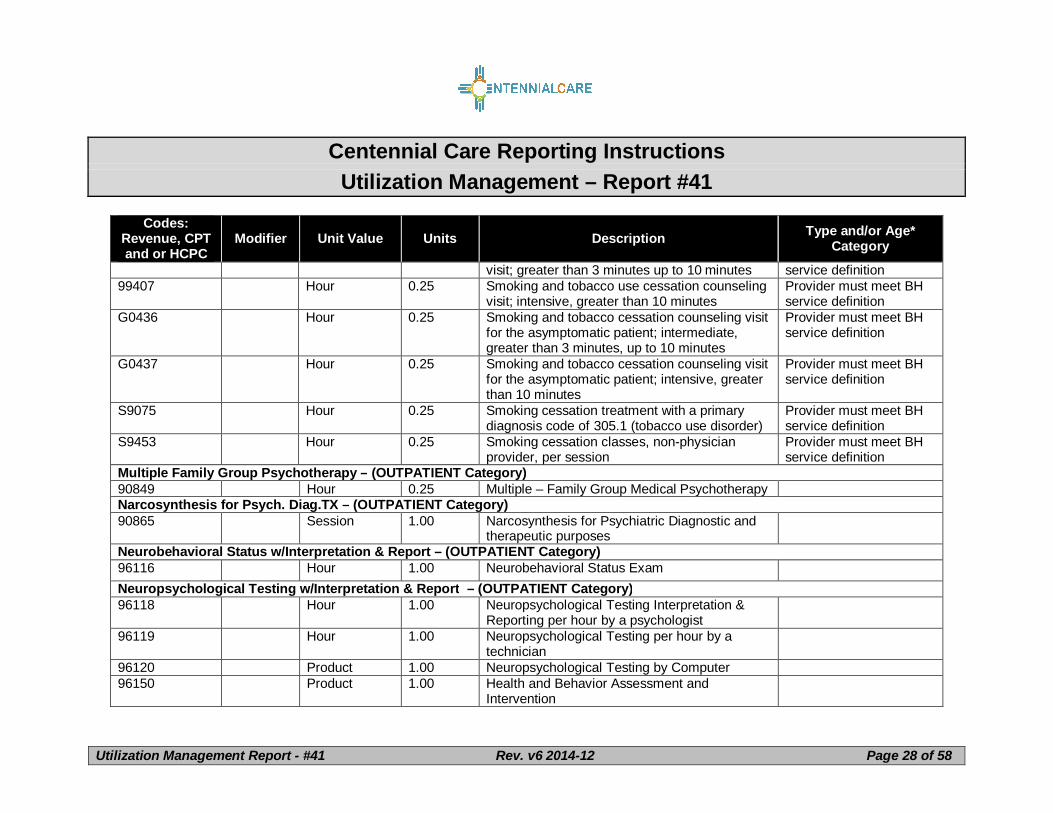
Smoking and Tobacco – Counseling Visits – (OUTPATIENT Category)99406 Hour 0.25 Smoking and tobacco use cessation counseling Provider must meet BH
Centennial Care Reporting InstructionsUtilization Management – Report #41
Modifier Unit Value Units Description Type and/or Age*Category
visit; greater than 3 minutes up to 10 minutes service definition99407 Hour 0.25 Smoking and tobacco use cessation counseling
visit; intensive, greater than 10 minutesProvider must meet BHservice definition
G0436 Hour 0.25 Smoking and tobacco cessation counseling visitfor the asymptomatic patient; intermediate,greater than 3 minutes, up to 10 minutes
Provider must meet BHservice definition
G0437 Hour 0.25 Smoking and tobacco cessation counseling visitfor the asymptomatic patient; intensive, greaterthan 10 minutes
Provider must meet BHservice definition
S9075 Hour 0.25 Smoking cessation treatment with a primarydiagnosis code of 305.1 (tobacco use disorder)
Provider must meet BHservice definition
S9453 Hour 0.25 Smoking cessation classes, non-physicianprovider, per session
Provider must meet BHservice definition
Multiple Family Group Psychotherapy – (OUTPATIENT Category)90849 Hour 0.25 Multiple – Family Group Medical PsychotherapyNarcosynthesis for Psych. Diag.TX – (OUTPATIENT Category)90865 Session 1.00 Narcosynthesis for Psychiatric Diagnostic and
Modifier Unit Value Units Description Type and/or Age*Category
Psychological Testing with w/Interpretation & Report (Hourly) – (OUTPATIENT Category)96101 Hour 1.00 Psychological Testing96102 Hour 1.00 Psychological Testing – by Technician96103 Hour 1.00 Psychological Testing – by ComputerPsychiatric Diagnostic Interview (Product) – (OUTPATIENT Category)90791 Do not
includemodifiersU8 or TR
Product 1.00 An initial evaluation provided by a non-physician
90792 Do notincludemodifiersU8 or TR
Product 1.00 An initial evaluation provided by a physician
Family Psychotherapy – (OUTPATIENT Category – School Based Health Center (SBHC) Sub-Category)90846 TR Hour 0.25 Family Psychotherapy without patient present <2190847 TR Hour 0.25 Family Psychotherapy with patient School
Based<21
Group Psychotherapy – (OUTPATIENT Category – SBHC Sub-Category)90853 TR Hour 0.25 Group Psychotherapy School Based <21Individual Psychotherapy – (OUTPATIENT Category – SBHC Sub-Category)90832 TR Hour 0.50 Psychotherapy – 30 minutes <2190834 TR Hour 0.75 Psychotherapy – 45 minutes <2190837 TR Hour 1.00 Psychotherapy – 60 minutes <2190833 TR Hour 0.50 Add on code 30 minutes with an E&M service <2190836 TR Hour 0.75 Add on code 30 minutes with an E&M service <21
90838 TR Hour 1.00 Add on code 60 minutes with an E&M service <21Pharmacological Management – (OUTPATIENT Category – SBHC Sub-Category)90863 TR Hour 0.25 Add on Code – Pharmacological Management
when provided with psychotherapy<21
Centennial Care Reporting InstructionsUtilization Management – Report #41
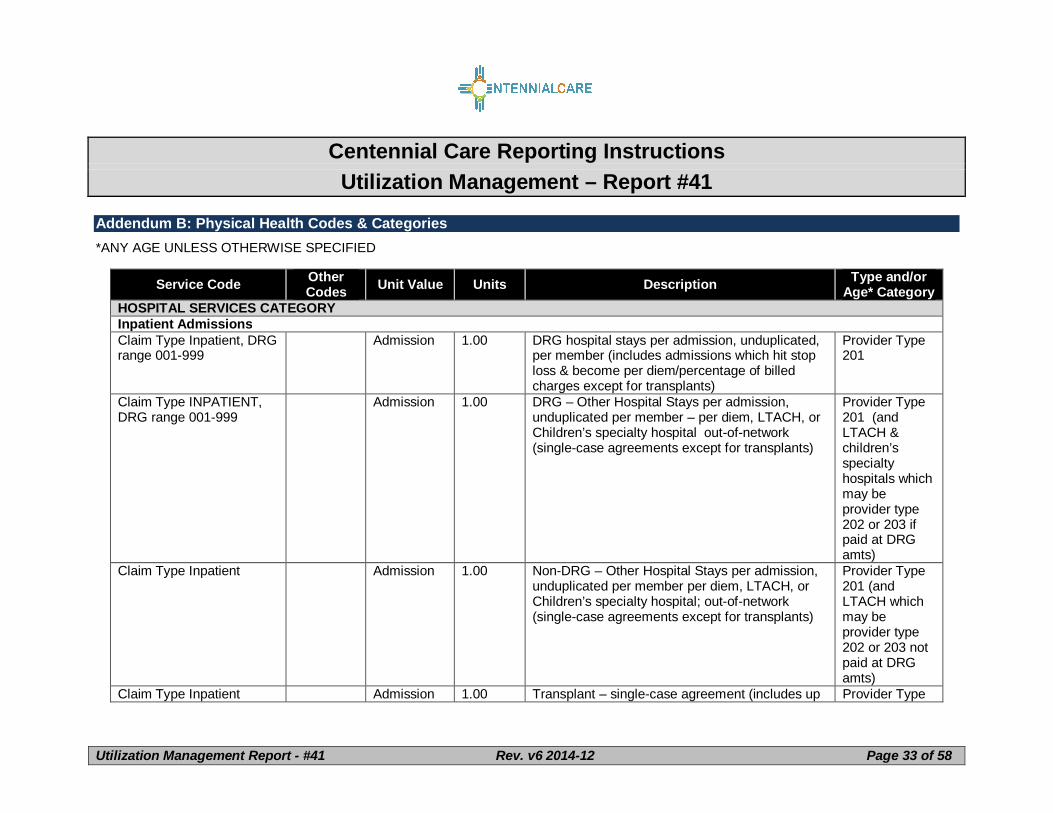
Addendum B: Physical Health Codes & Categories*ANY AGE UNLESS OTHERWISE SPECIFIED
Service Code OtherCodes Unit Value Units Description Type and/or
Age* CategoryHOSPITAL SERVICES CATEGORYInpatient AdmissionsClaim Type Inpatient, DRGrange 001-999
Admission 1.00 DRG hospital stays per admission, unduplicated,per member (includes admissions which hit stoploss & become per diem/percentage of billedcharges except for transplants)
Provider Type201
Claim Type INPATIENT,DRG range 001-999
Admission 1.00 DRG – Other Hospital Stays per admission,unduplicated per member – per diem, LTACH, orChildren’s specialty hospital out-of-network(single-case agreements except for transplants)
Provider Type201 (andLTACH &children’sspecialtyhospitals whichmay beprovider type202 or 203 ifpaid at DRGamts)
Claim Type Inpatient Admission 1.00 Non-DRG – Other Hospital Stays per admission,unduplicated per member per diem, LTACH, orChildren’s specialty hospital; out-of-network(single-case agreements except for transplants)
Provider Type201 (andLTACH whichmay beprovider type202 or 203 notpaid at DRGamts)
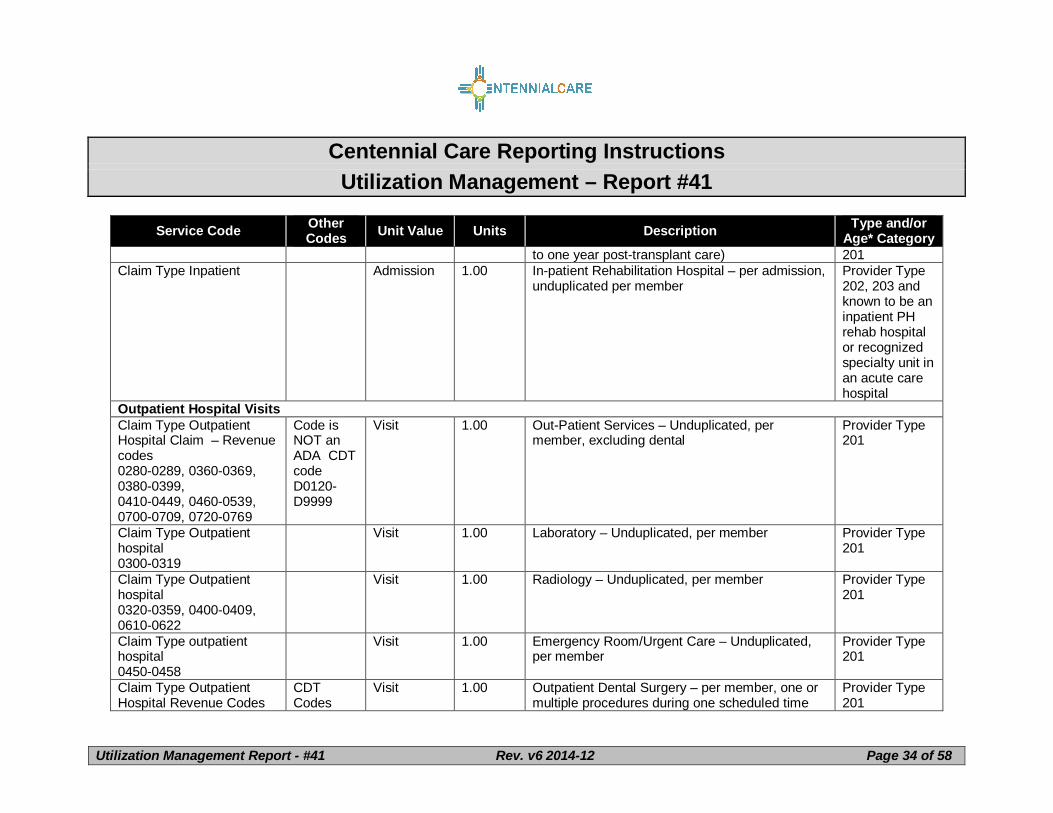
Claim Type Inpatient Admission 1.00 Transplant – single-case agreement (includes up Provider Type
Centennial Care Reporting InstructionsUtilization Management – Report #41
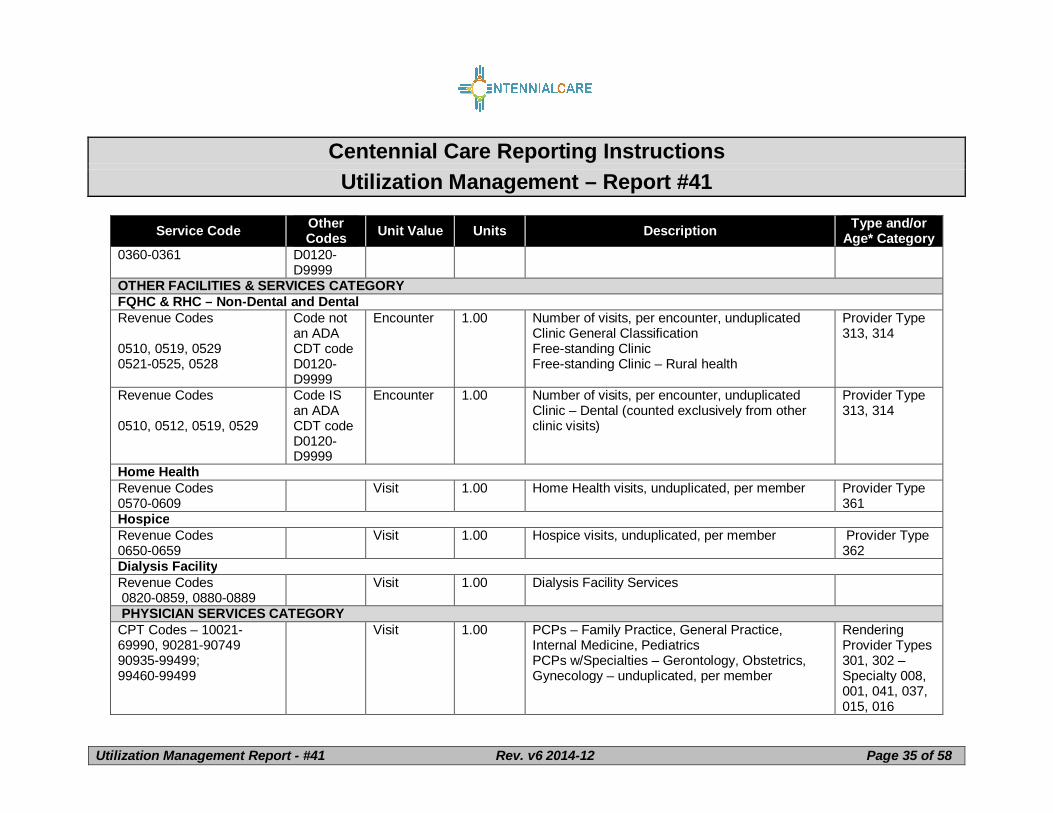
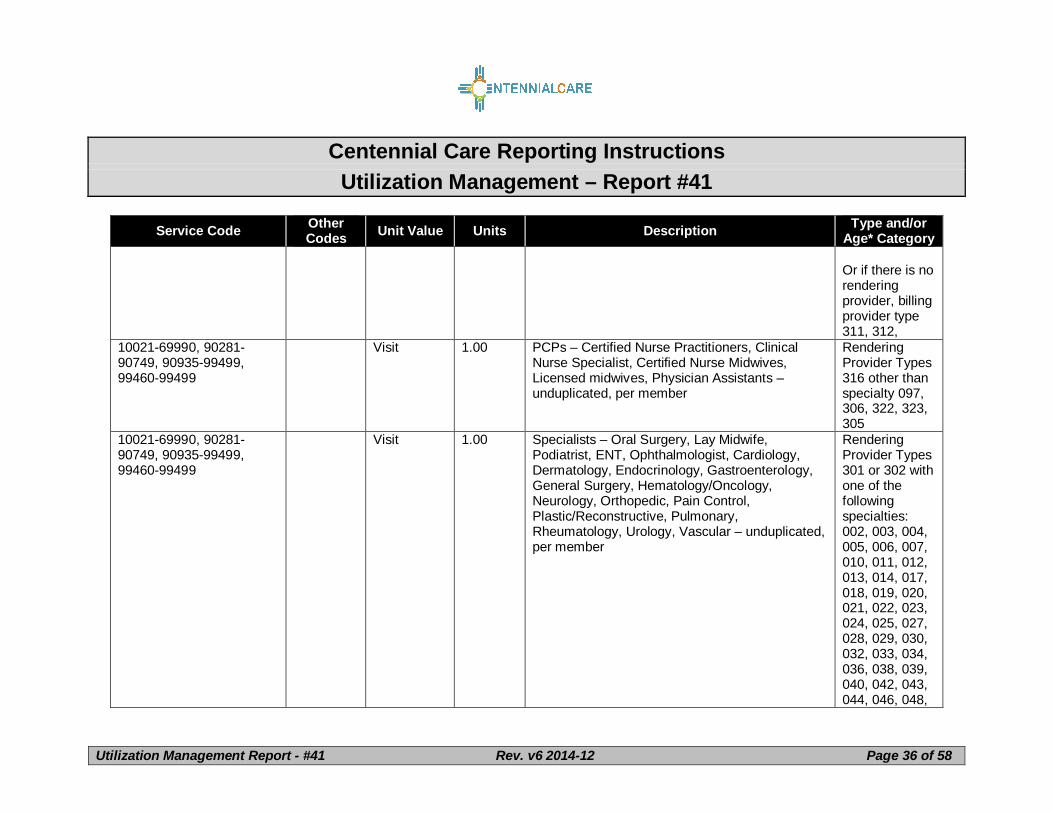
Visit 1.00 PCPs – Family Practice, General Practice,Internal Medicine, PediatricsPCPs w/Specialties – Gerontology, Obstetrics,Gynecology – unduplicated, per member
Service Code OtherCodes Unit Value Units Description Type and/or
Age* CategoryCommunity (S5135) Provider Type
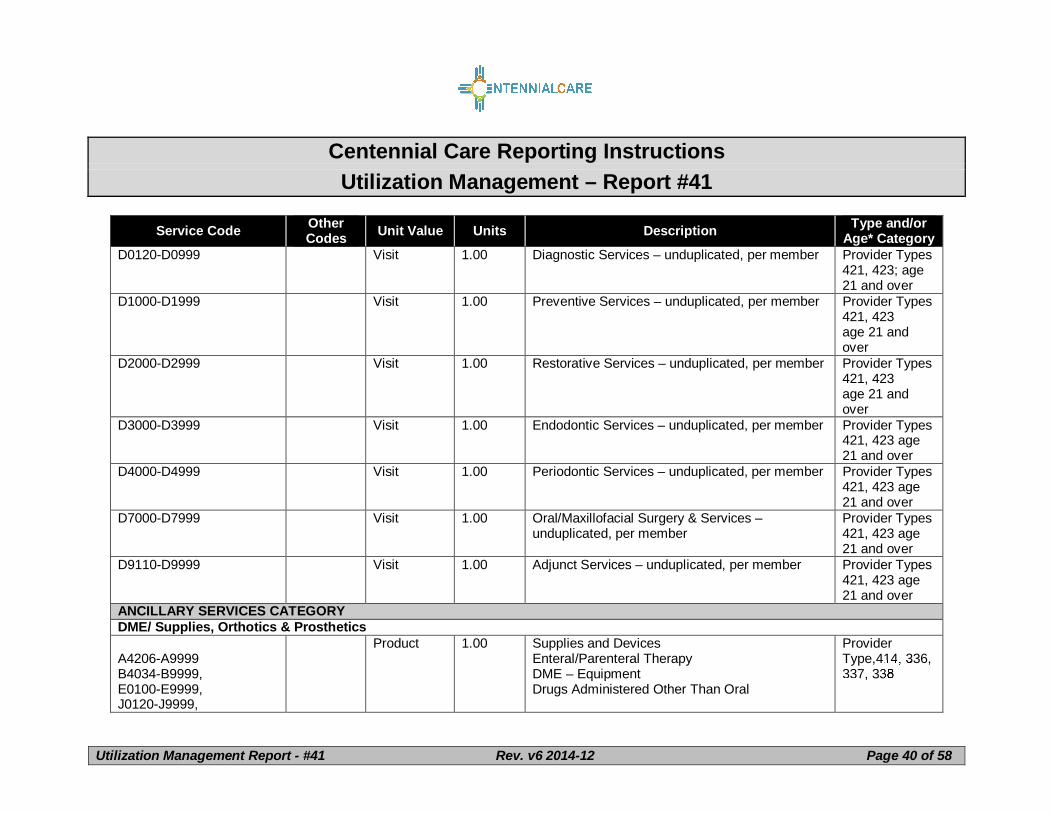
904Dental Services – Ages 20 and Under – Note that outpatient hospital claims may have these codes as the procedure code on theUB format – so do not include claims billed on the UB format under this sectionD0120-D0999 Visit 1.00 Diagnostic Services – unduplicated, per member Provider Types
421, 423Under age 21
D1000-D1999 Visit 1.00 Preventive Services – unduplicated, per member Provider Types421 423Under age 21
D2000-D2999 Visit 1.00 Restorative Services – unduplicated, per member Provider Types421, 423 Underage 21
D3000-D3999 Visit 1.00 Endodontic Services – unduplicated, per member Provider Types421, 423 Underage 21
D4000-D4999 Visit 1.00 Periodontic Services – unduplicated, per member Provider Types421, 423 Underage 21
D7000-D7999 Visit 1.00 Oral/Maxillofacial Surgery & Services –unduplicated, per member
Provider Types421, 423 Underage 21
D8000-D8999 Visit 1.00 Orthodontics – unduplicated, per member Provider Types421, 423 Underage 21
D9110-D9999 Visit 1.00 Adjunct Services – unduplicated, per member Provider Types421, 423 Underage 21
Dental Services – Ages 21 and Over – Note that outpatient hospital claims may have these codes as the procedure code on theUB format – do not include claims billed on the UB format under this section
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* Category
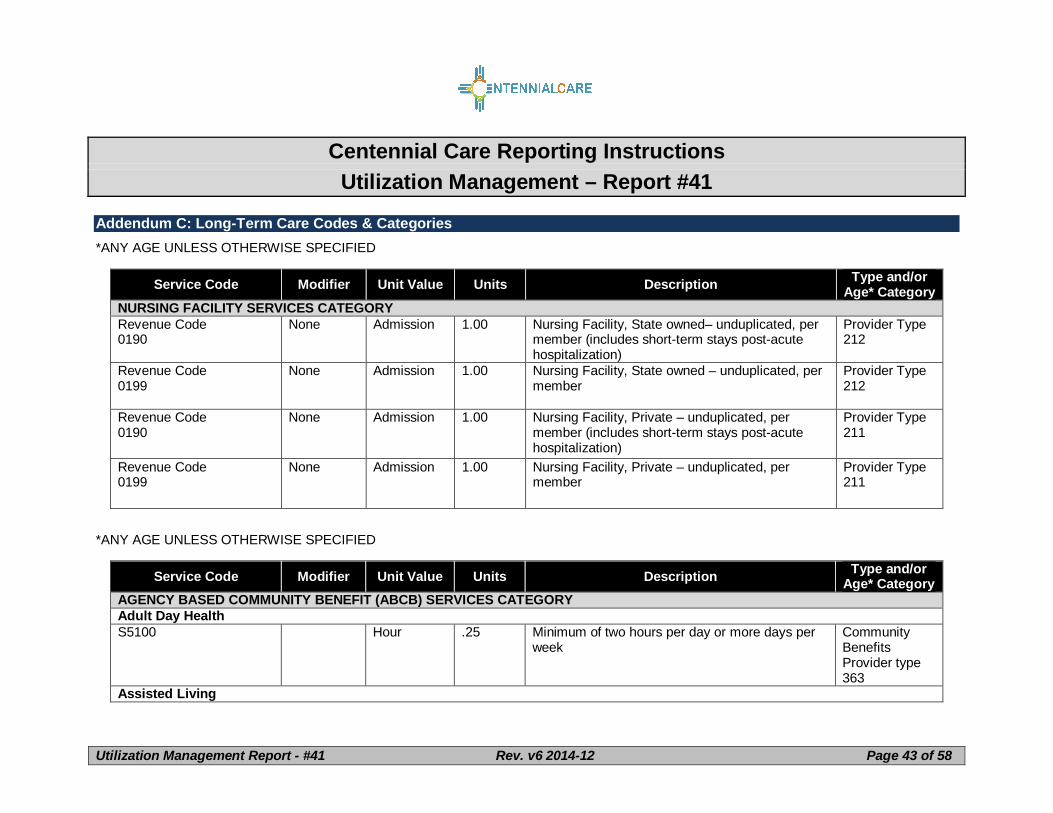
T2031 Month 1.00 The following services will not be provided torecipients in Assisted Living facilities: PersonalCare, Respite, Environmental Modifications,Emergency Response or Adult Day Health. TheAssisted Living Program is responsible for all ofthese services at the Assisted Living Facility.
CommunityBenefitsProvider type363
Community Transition ServicesT2038 Service 1.00 Community Transition Services do not include
monthly rental or mortgage expense, food, regularutility charges, and/or household appliances oritems that are intended for purelydiversional/recreational purposes. CommunityTransition Services are limited to $3,500 perperson every five years. In order to be eligible forthis service, the person must have a nursingfacility stay of at least 90 days prior totransition to the community.
CommunityBenefitsProvider type363
Emergency ResponseS5161 Month 1.00 Eligible recipient must have a landline phone. Community
BenefitsProvider type363
Emergency Response High NeedS5161 U1 Month 1.00 Same service as above except this has a different
transmitter/receiver box that is voice activated.CommunityBenefitsProvider type363
Environmental Modification
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* Category
S5165 Project 1.00 Environmental Modification services are limited tofive thousand dollars ($5,000) every five (5) years.Additional services may be requested if an eligiblerecipient’s health and safety needs exceed thespecified limit.
CommunityBenefitsProvider type363
Behavior Support ConsultationH2019 Hour .25 Based on the eligible recipient’s care plan,
services are delivered in an integrated/naturalsetting or in a clinical setting.
CommunityBenefitsProvider type363
Behavior Support Consultation, Clinic BasedH2019TT Hour .25 Clinic Based – same service as above except
services are delivered in a clinic settingCommunityBenefitsProvider type363
Employment SupportsH2024 Day 1.00 Payment shall not be made for incentive
payments, subsidies, or unrelated vocationaltraining expenses such as the following: 1)Incentive payments made to an employer toencourage or subsidize the employer'sparticipation in a supported employment program;2) Payments that are passed through to users ofsupported employment programs; or 3) Paymentsfor training that is not directly related to anindividual's supported employment program.Federal financial participation cannot be claimedto defray expenses associated with starting up oroperating a business.
CommunityBenefitsProvider type363
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* Category
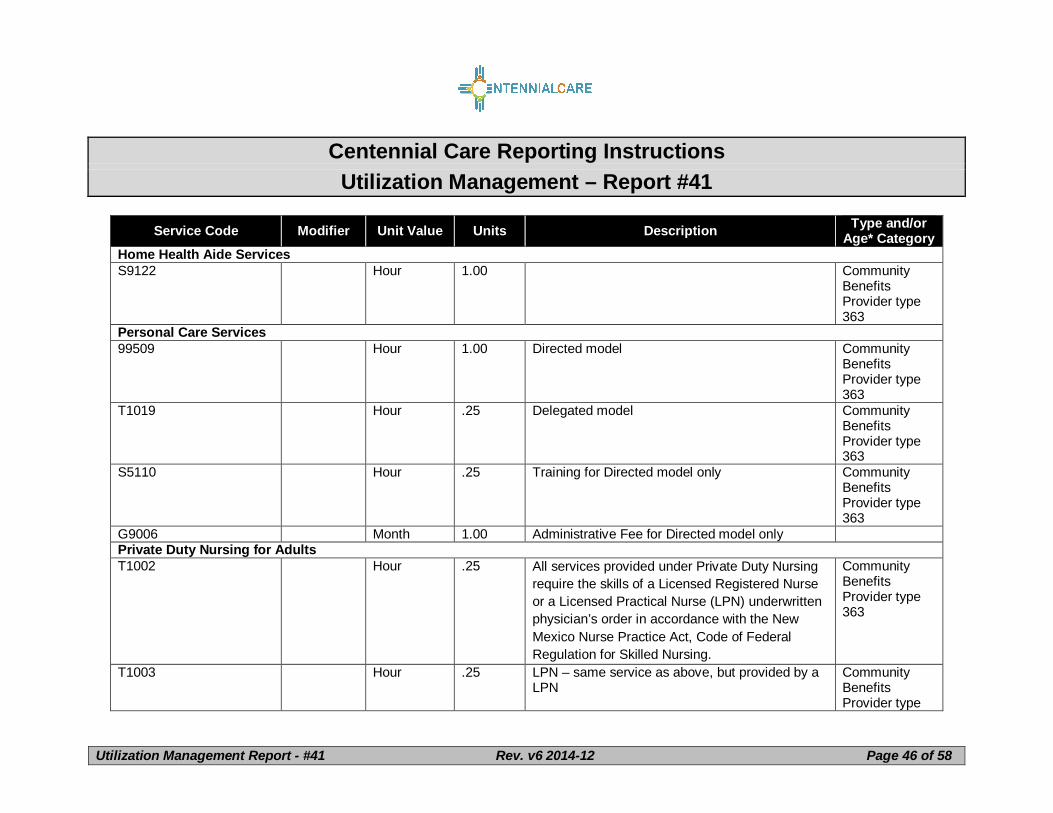
Home Health Aide ServicesS9122 Hour 1.00 Community
BenefitsProvider type363
Personal Care Services99509 Hour 1.00 Directed model Community
BenefitsProvider type363
T1019 Hour .25 Delegated model CommunityBenefitsProvider type363
S5110 Hour .25 Training for Directed model only CommunityBenefitsProvider type363
G9006 Month 1.00 Administrative Fee for Directed model onlyPrivate Duty Nursing for AdultsT1002 Hour .25 All services provided under Private Duty Nursing
require the skills of a Licensed Registered Nurseor a Licensed Practical Nurse (LPN) underwrittenphysician’s order in accordance with the NewMexico Nurse Practice Act, Code of FederalRegulation for Skilled Nursing.
CommunityBenefitsProvider type363
T1003 Hour .25 LPN – same service as above, but provided by aLPN
CommunityBenefitsProvider type
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* Category363
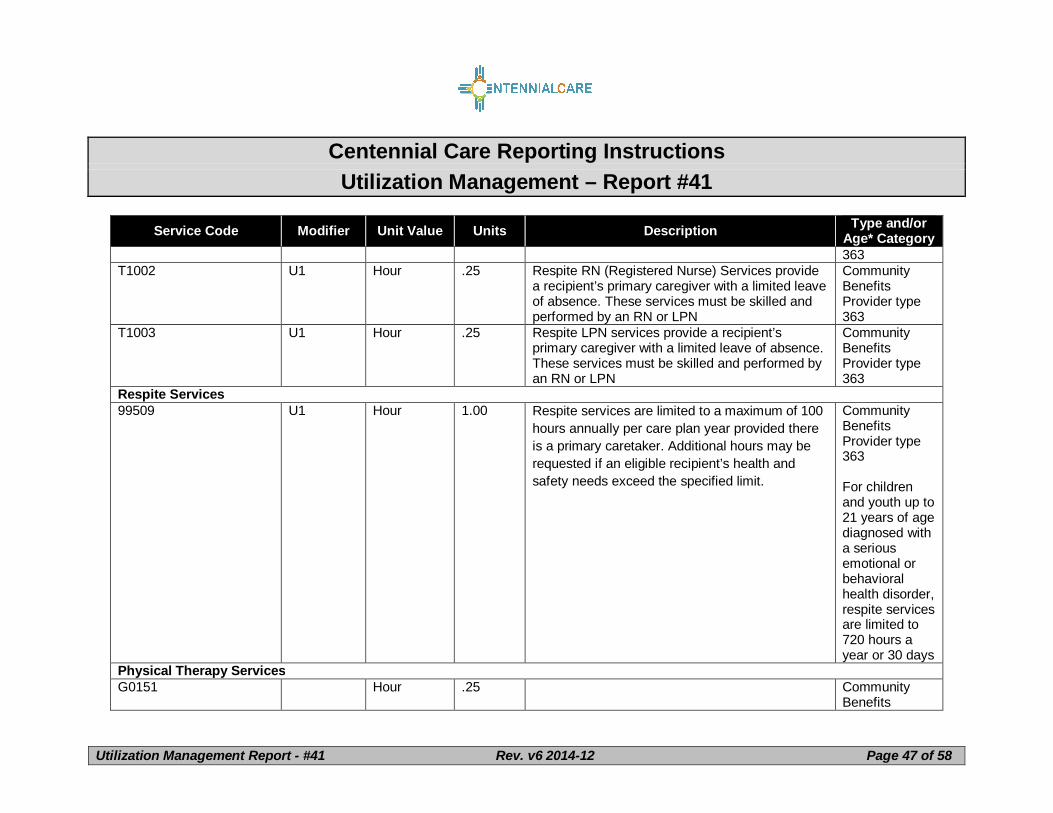
T1002 U1 Hour .25 Respite RN (Registered Nurse) Services providea recipient’s primary caregiver with a limited leaveof absence. These services must be skilled andperformed by an RN or LPN
CommunityBenefitsProvider type363
T1003 U1 Hour .25 Respite LPN services provide a recipient’sprimary caregiver with a limited leave of absence.These services must be skilled and performed byan RN or LPN
CommunityBenefitsProvider type363
Respite Services99509 U1 Hour 1.00 Respite services are limited to a maximum of 100
hours annually per care plan year provided thereis a primary caretaker. Additional hours may berequested if an eligible recipient’s health andsafety needs exceed the specified limit.
CommunityBenefitsProvider type363
For childrenand youth up to21 years of agediagnosed witha seriousemotional orbehavioralhealth disorder,respite servicesare limited to720 hours ayear or 30 days
Physical Therapy ServicesG0151 Hour .25 Community
Benefits
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* CategoryBenefitsProvider type363
Environmental ModificationS5165 Project 1.00 Environmental Modification services are limited to
five thousand dollars ($5,000) every five (5) years.Additional services may be requested if an eligiblerecipient’s health and safety needs exceed thespecified limit.
CommunityBenefitsProvider type363
Behavior Support ConsultationH2019 Hour .25 Based on the eligible recipient’s care plan,
services are delivered in an integrated/naturalsetting or in a clinical setting.
CommunityBenefitsProvider type363
Employment SupportsT2019 Hour .25 Job Coach
Payment shall not be made for incentivepayments, subsidies, or unrelated vocationaltraining expenses such as the following: 1)Incentive payments made to an employer toencourage or subsidize the employer'sparticipation in a supported employment program;2) Payments that are passed through to users ofsupported employment programs; or 3) Paymentsfor training that is not directly related to anindividual's supported employment program.Federal financial participation cannot be claimedto defray expenses associated with starting up oroperating a business.
CommunityBenefitsProvider type363
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* Category
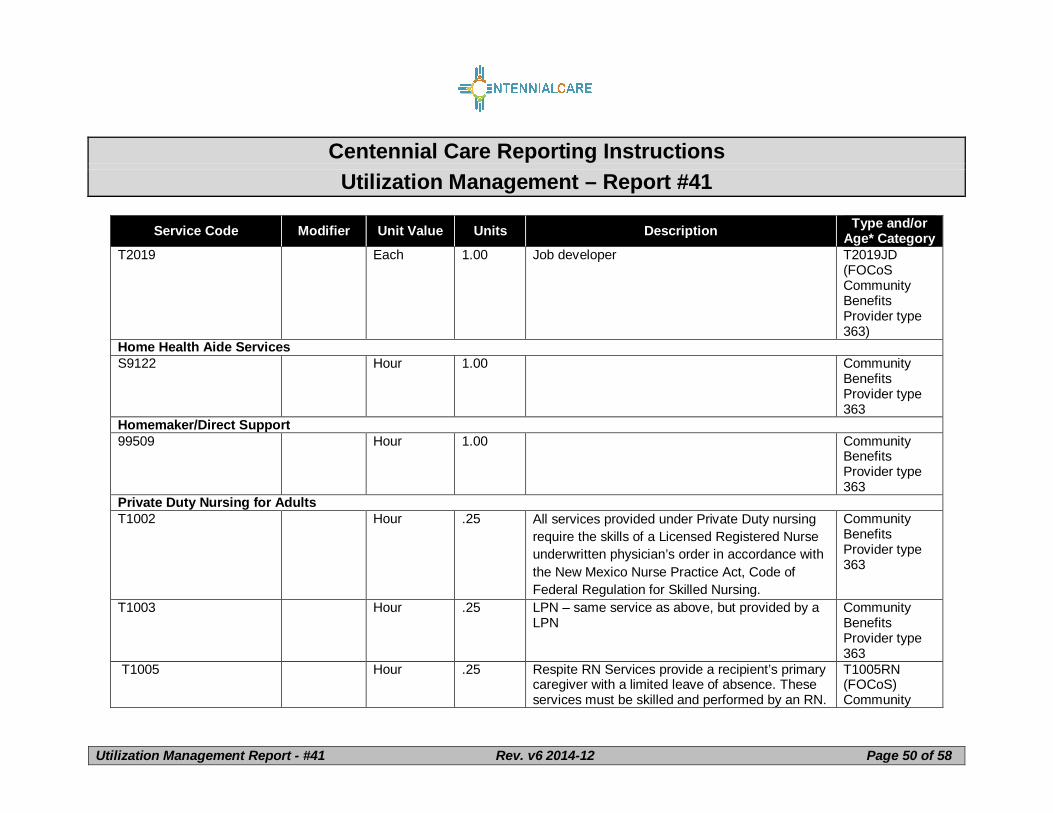
T2019 Each 1.00 Job developer T2019JD(FOCoSCommunityBenefitsProvider type363)
Home Health Aide ServicesS9122 Hour 1.00 Community
BenefitsProvider type363
Homemaker/Direct Support99509 Hour 1.00 Community
BenefitsProvider type363
Private Duty Nursing for AdultsT1002 Hour .25 All services provided under Private Duty nursing
require the skills of a Licensed Registered Nurseunderwritten physician’s order in accordance withthe New Mexico Nurse Practice Act, Code ofFederal Regulation for Skilled Nursing.
CommunityBenefitsProvider type363
T1003 Hour .25 LPN – same service as above, but provided by aLPN
CommunityBenefitsProvider type363
T1005 Hour .25 Respite RN Services provide a recipient’s primarycaregiver with a limited leave of absence. Theseservices must be skilled and performed by an RN.
T1005RN(FOCoS)Community
Centennial Care Reporting InstructionsUtilization Management – Report #41
Service Code Modifier Unit Value Units Description Type and/orAge* CategoryBenefitsProvider type363
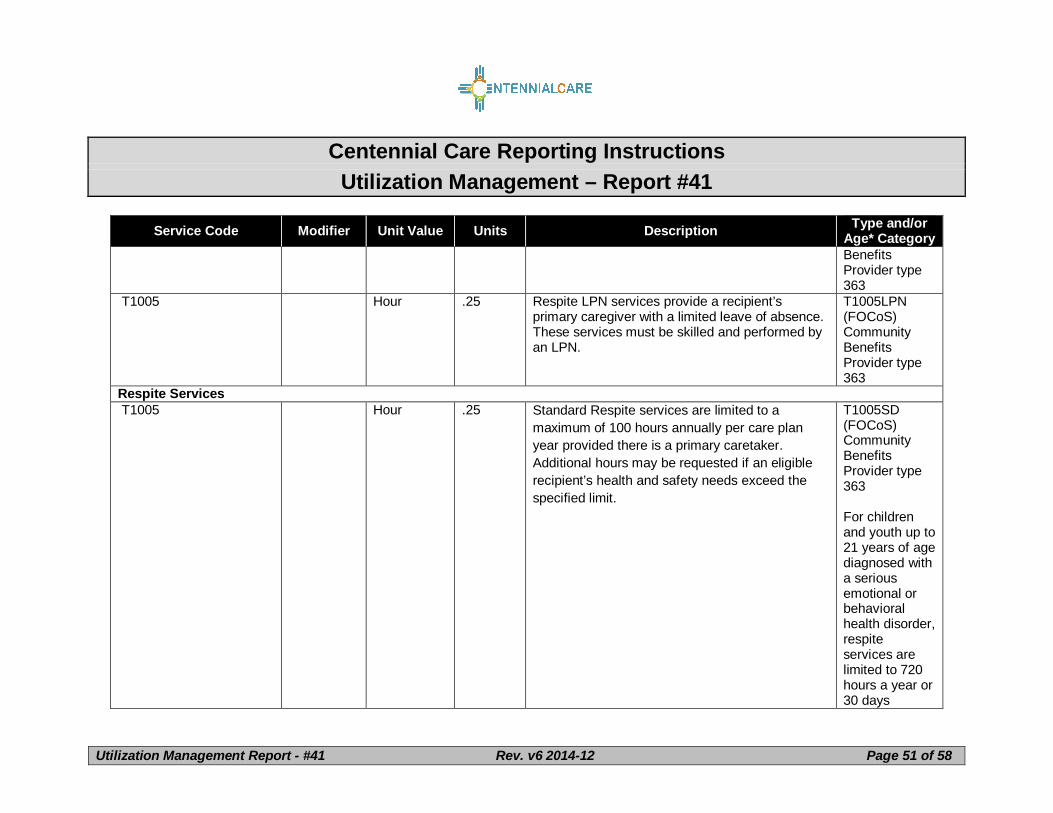
T1005 Hour .25 Respite LPN services provide a recipient’sprimary caregiver with a limited leave of absence.These services must be skilled and performed byan LPN.
T1005LPN(FOCoS)CommunityBenefitsProvider type363
Respite Services T1005 Hour .25 Standard Respite services are limited to a
maximum of 100 hours annually per care planyear provided there is a primary caretaker.Additional hours may be requested if an eligiblerecipient’s health and safety needs exceed thespecified limit.
T1005SD(FOCoS)CommunityBenefitsProvider type363
For childrenand youth up to21 years of agediagnosed witha seriousemotional orbehavioralhealth disorder,respiteservices arelimited to 720hours a year or30 days
Centennial Care Reporting InstructionsUtilization Management – Report #41