5/10/2017 1 Central Venous Catheter (CVC) Care is More Than Just Guidelines: Examine Why We Do What We Do… Class Objectives • At the end of the course, you will be able to: • Understand the statistics of CVC related bloodstream infections. • Identify types of CVCs & list the site placement that increase bloodstream infections. • Identify EBPs related to the prevention of CLABSI and for central line maintenance & care. • Describe methods to enhance compliance with these practices. • List tools/strategies used to improve teamwork and build a safety culture. What About Placement? • Placement of a central lines can be complicated by: • Pneumothorax • Hemothorax • Arrhythmias • Arterial punctures • Inadvertent arterial placement • Maintaining a central line places patient at risk for: • Deep vein thrombosis and pulmonary embolis • Central line - associated bloodstream infection (CLABSI) • Central Line Removal - risk’s air embolism Why are You Hearing About This? • What is the Problem? • Central Line Associated Blood Stream Infection (CLABSI) – what does that mean to you? To your patient? • Intervention (You are the intervention) • A course to achieve standardization of infection control practices during central line insertion, maintenance and care • Outcome (Lets see if it will make a difference) • Education in one medical center achieved a relative reduction (rates have decreased below the national average) in central line infections & saved 1.3 million dollars 4 The Problem • Consumer Reports: among worst teaching hospitals in US for CLABSI • For many years • Other UCs are among the best in the country “Our patients/specialties are special” is not an excuse” SYSTEM FAILURE: Nurse not in room for insertion “It would take forever if I waited in there.” Attending did not supervise Fellow at clinic Supervising resident “signed off,” but never trained on dressing AND THE RESULT… Catheter hub not scrubbed in between IVP meds Biopatch not 360 o Line sutured Tegaderm overlaps ETT holder Blood under Tegaderm Visible blood in lumen The Problem • Patient signed out to another nurse, who dated dressing but did not recognize any of these issues
Transcript
5/10/2017
1
Central Venous Catheter (CVC) Care is More Than Just Guidelines:
Examine Why We Do What We Do…
Class Objectives
• At the end of the course, you will be able to:• Understand the statistics of CVC related bloodstream
infections.• Identify types of CVCs & list the site placement that
increase bloodstream infections. • Identify EBPs related to the prevention of CLABSI and for
central line maintenance & care. • Describe methods to enhance compliance with these
practices. • List tools/strategies used to improve teamwork and build
a safety culture.
What About Placement?
• Placement of a central lines can be complicated by:• Pneumothorax• Hemothorax• Arrhythmias• Arterial punctures
• Inadvertent arterial placement
• Maintaining a central line places patient at risk for:• Deep vein thrombosis and pulmonary embolis• Central line - associated bloodstream infection (CLABSI)• Central Line Removal - risk’s air embolism
Why are You Hearing About This?• What is the Problem?
• Central Line Associated Blood Stream Infection (CLABSI) –what does that mean to you? To your patient?
• Intervention (You are the intervention)• A course to achieve standardization of infection control
practices during central line insertion, maintenance and care
• Outcome (Lets see if it will make a difference)• Education in one medical center achieved a relative
reduction (rates have decreased below the national average) in central line infections & saved 1.3 million dollars
4
The Problem
• Consumer Reports: among worst teaching hospitals in US for CLABSI• For many years
• Other UCs are among the best in the country
“Our patients/specialties are special” is not an excuse”
SYSTEM FAILURE:
Nurse not in room for insertion
“It would take forever if I waited
in there.”
Attending did not supervise
Fellow at clinic
Supervising resident “signed off,” but
never trained on dressing
AND THE RESULT…
Catheter hub not scrubbed in between
IVP meds
Biopatch not 360o
Line sutured
Tegaderm overlaps ETT holder
Blood under Tegaderm
Visible blood in lumen
The Problem
• Patient signed out to another nurse, who dated dressing but did not recognize any of these issues
5/10/2017
2
CDC 2011 GuidelinesEducate healthcare personnel regarding the indications for intravascular catheter use, proper procedures for the insertion and maintenance of intravascular catheters, and appropriate infection control measures to prevent intravascular catheter-related infections.
• Periodically assess knowledge of and adherence to guidelines for all persons who are involved in the insertion and maintenance of intravascular catheters.
• Designate only trained personnel who demonstrate competence for the insertion and maintenance of peripheral and central intravascular catheters
5/10/2017
3
Central Venous Catheters 101
What is the difference?
What is a Central Line?• The distal catheter tip is
ideally positioned in the lower one third of the SVC at the cavo-atrial junction, the right atrium or the inferior vena cava
• Common areas for insertion are: • Brachiocephalic veins • Internal jugular veins • Subclavian veins • External iliac veins• Femoral veins.
15
Why do we need central lines?
• Delivery of IV medication • Vasopressors, antibiotics, chemotherapy• Reduced the risk of phlebitis from a PIV
• Delivery of fluids, intermittent infusions and blood or blood products
• Provide parenteral nutrition• Monitoring central venous pressure• Plasmapheresis, aphersis, hemodialysis, continuous
renal replacement therapy• Frequent blood draws• IV therapy when peripheral access is not feasible
Venous Access Devices• What do you call this catheter?
• Is identified by the type of vessel it occupies• Peripheral vein, central vein, artery
• Its intended lifespan• Short term or long term
• Its site of insertion• Subclavian, femoral, internal jugular, peripheral insertion
• Its physical shape (long vs. short)
• Special Characteristics• Presence of a valve, cuff, impregnated (heparin, abx, antiseptics),
number of lumens, brand, purpose (power, dialysis)
To accurately define a specific catheter all aspects should be described
• Surgically placed by tunneling the catheter under the skin from the vein entry point to an exit point on the chest wall
• Provides long term venous access
5/10/2017
4
Tunneled vs. Non-Tunneled
• Non-Tunneled Catheters (single or multi lumen) Swan Ganz, hemodialysis, triple lumen, plasmapheresis…
• External catheter that does not have a cuff and is inserted percutaneously over a wire or through an introducer sheath
• Introducer sheath (Cordis) is indicated for the introduction of an intravascular device that may damage the vascular wall. It may be used as an intravascular catheter but is NOT centrally located (i.e. not a central line)
• Provide short and/or long term access
Peripherally Inserted Central Line Catheter (PICC)
• Catheter inserted 2 inches above/below the antecubital space, in the basilic, cubital, or cephalic vein
• Provide short and/or long term venous access
Midline Catheter
• Inserted 2 inches above/ below the antecubital space and inserted in the basilic, cubital, or cephalic vein
• tip lies in a vein between the antecubital and midclavicular area.
• Provide short term venous access
• This is not considered a central venous catheter
• This is cared for the same way as a Central Line (PICC).
Dialysis/Pheresis• Two large bore lumens that allow for exchange of arterial and venous
blood at a high rate (200 to 500 ml/min) via machine. • Red is usually arterial• Blue is usually venous
• Dialysis catheters - cared for by a Dialysis RN.
• Pheresis catheters in the BMT population - cared for by the BMT RN.• Once pheresis is complete, an order from the Nephrologist is required to use a
pheresis catheter for infusion of fluids or medications. • Mahukar Catheter has a 3rd lumen. You may access this dedicated lumen for
medication, IV fluid delivery or blood draws as you would a CVC, including flushing.
• Dialysis AND Phereis catheters are “Locked” with 3 mL of high dose of sodium citrate to prevent clotting
• IMPORTANT: Prior to use aspirate 3 mL to rid the catheter of the sodium citrate.
• Due to large bore, these catheters carry a risk of air embolism if not properly accessed and / or locked.
Subcutaneous Implanted Venous Ports• Reservoir port with an attached catheter
implanted into the blood vessel
• Surgically implanted and totally under the skin
• Accessed with a non-coring needle (Huber) to minimize trauma to the self-sealing septum
• Provide long term venous access
• May be open or closed-ended with a single or double lumen barrel.
• The needle and dressing are changed every 7 days & PRN
What if your patient comes in with a port, but no one on the floor can
access it?
Open-ended vs. Valved
Open-ended Catheters (i.e. Hickman, Cook and Broviac)
• Require a continuous infusion, “heparin lock” or frequent flushing with saline to keep patent
• Always has a CLAMP
• Provide short or long term venous access
• If catheter type is unknown, treat catheter as open-ended
5/10/2017
5
Open-Ended vs. Valved
Closed (Valved) Catheters (Groshong/Xcela)
• Uses a slit valve at the proximal or distal end which closes automatically when not in use
• No Clamps
• Only flush with normal saline to keep patent
• Provide long term venous access
Central Catheter Assessment
• Central catheter assessment includes aspirating for blood return prior to the administration of medications and other solutions
jlz/July2011
Catheter Care and Maintenance
• All arterial catheters will be care for like a central catheter
• Dressings and tubing are changed every 7 days and PRN that includes changing the neutral displacement device (cap) Coordinate with infusion replacements if able
• Label new dressing with current date, time and initials
• Label tubing using a Day of the Week sticker indicating the date and time the tubing is to be changed next
• When a secondary administration set is used, back priming is preferred to limit disconnecting from the primary administration set
• TPN/Lipid infusion, tubing and neutral displacement connector are changed every 24 hrs
jlz/July2011
Pressure Bags for Transduced Lines
• Normal Saline will be used in all pressurized, transduced lines unless ordered by physician.
• Heparin flush concentration may be ordered for pressurized, transduced lines for patients when indicated.
jlz/July2011
Which one do I use?What determines appropriate choice of
venous access:
• Type of solution(s)
• Number of lumens
• Duration of therapy
• Flow requirements
• Frequency of access
• Patient and physician preference
Who needs the CVC line? The patient or the nurse? Help decrease utilization rates!
Central Line –Associated Bloodstream Infections: First, Do No
Harm
5/10/2017
6
Why Aren’t We Doing The Right Thing? We’ve heard…
• “It takes too much time”
• “It’s not me…it’s somebody else”
• “I’m very busy. I’ve got important things to
do.”
• “I can’t tell a Dr. to wash their hands!”
• “You just don’t understand what it’s like to
work here every day.”
• “I don’t believe there’s a problem. I’m a good
nurse.”
How do
patients get infections?
Patient – Related Risk Factors•Location: Placement of catheters in emergency situations; subclavian vein poses less risk than internal jugular or femoral vein
•Multiple lumen catheters • Increased tissue trauma• More manipulation and contamination of multiple ports/hubs
•The presence of catheters for extended periods of time
•Certain patient populations:• Men, neutropenic patients, or those receiving total parenteral nutrition (TPN)
and/or lipid• Infection elsewhere (e.g. UTI or wound) as a secondary source• Age & immune system status
33
Why?
The number of lumens does not affect complication rate? What does???
Impact of CLABSIs
• Central line usage• Disrupt the integrity of the skin• Infection spreads to bloodstream, sepsis leading to
hemodynamic changes, organ dysfunction• Approx. 90% of CLABSIs occur with acute care non –
tunneled lines
• 48% of ICU patients have central lines
• 15 million CVC days/year in ICUs
• While 80,000 CLABSIs occur in ICUs each year, a total of 250,000 cases of BSIs have been estimated to occur annually, if entire hospitals are assessed
Joint Commission 2009 34
Impact of CLABSIs
•Mortality rate is 12-25% for each infection
•250,000 CLABSI infections annually
•Up to 62,000 deaths result from CLABSI each year
•Average cost: $45,000 each
•$300 million - $2.3 billion/year avoidable costs
•Most are preventable
Joint Commission 2009 35
General Definition of a BSI
•Criterion 1: Recognized pathogen cultured from one or more blood cultures not from another recognized site (SSI)
•Criterion 2: Clinical S/S to include• Fever >38.0 C, chills and hypotension and• S/S and + lab results are not related to an infection at
another site• A common skin contaminant is cultured from two or
more blood cultures drawn on separate occasions
Who is the NHSN??? And Why do we compare our rates to them?
5/10/2017
7
Who says it is a CLABSI?
•CLABSI can only be accurately diagnosed through clinical evaluation and microbiologic confirmation.• Must be associated with a Central Line• 48 hours
Time to draw cultures
• 2 sets of blood samples should be drawn from 2 sites• Peripheral vein• Central line (if unable to get peripheral cultures,
use other lumen of central line)• Catheter tip?
But sometimes it is not that clear clinically
•Diagnosis can sometimes be challenging
•Clinical features are typically indistinguishable from bloodstream infections that arise from other sources
This is where the Infection Control
Department comes in. They spend the time analyzing the cases.
EPIC Central Line insertion checklist
CLIP Bundle Adherence Components
California Confidential Evidence Code 1157
5/10/2017
8
CHG Bathing for ALL Patients
• Bathing with CHG reduces the bio burden
2 x A Day wipe down of the environment, allow to sit for full
minute, then rinse with dampened cloth
Where do Infections Come?
• The most recognizable route of line contamination is the migration from the skin followed by hub contamination.
• Gram positive cocci is a common organism found in the skin.
So…
•What do you think of this information?
•Have you seen it before?
•Where can you access this information?
•What does it make you think about?
•What can you do to make a difference?
Best Practices & Implementation Strategies of Central Line Bundle
Video Central Venous CatheterizationNew England Journal of Medicine Alan S. Graham, M.D., Caroline Ozment, M.D., Ken Tegtmeyer, M.D., Susanna Lai, M.P.H., and Dana A.V. Braner, M.D.
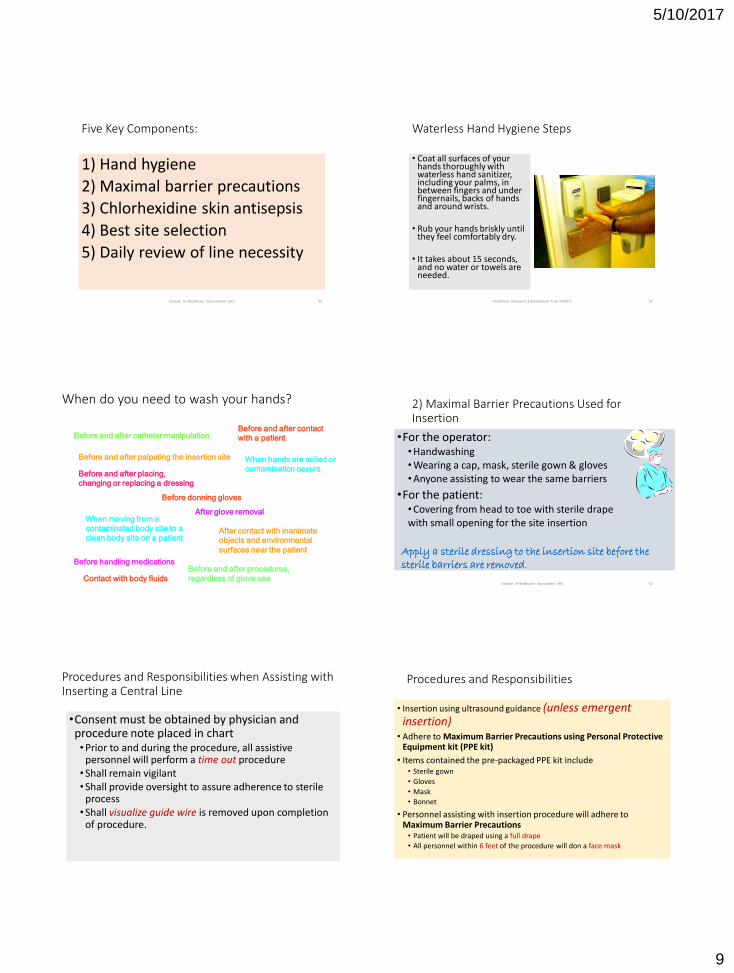
• Coat all surfaces of your hands thoroughly with waterless hand sanitizer, including your palms, in between fingers and under fingernails, backs of hands and around wrists.
• Rub your hands briskly until they feel comfortably dry.
• It takes about 15 seconds, and no water or towels are needed.
Healthcare Research & Educational Trust (HRET) 50
When do you need to wash your hands?
Before and after catheter manipulation
Before and after palpating the insertion site
Before and after placing,
changing or replacing a dressing
When moving from a
contaminated body site to a
clean body site on a patient
Before donning gloves
After contact with inanimate
objects and environmental
surfaces near the patient
After glove removal
When hands are soiled or
contamination occurs
Before and after procedures,
regardless of glove use
Before handling medications
Before and after contact
with a patient
Contact with body fluids
2) Maximal Barrier Precautions Used for Insertion
•For the operator:• Handwashing• Wearing a cap, mask, sterile gown & gloves• Anyone assisting to wear the same barriers
•For the patient:• Covering from head to toe with sterile drape with small opening for the site insertion
Institute of Healthcare Improvment (IHI) 52
Apply a sterile dressing to the insertion site before the sterile barriers are removed.
Procedures and Responsibilities when Assisting with Inserting a Central Line
•Consent must be obtained by physician and procedure note placed in chart• Prior to and during the procedure, all assistive
personnel will perform a time out procedure• Shall remain vigilant• Shall provide oversight to assure adherence to sterile
process• Shall visualize guide wire is removed upon completion
of procedure.
Procedures and Responsibilities
• Insertion using ultrasound guidance (unless emergent insertion)
• Adhere to Maximum Barrier Precautions using Personal Protective Equipment kit (PPE kit)
• Items contained the pre-packaged PPE kit include• Sterile gown
• Gloves
• Mask
• Bonnet
• Personnel assisting with insertion procedure will adhere to Maximum Barrier Precautions
• Patient will be draped using a full drape
• All personnel within 6 feet of the procedure will don a face mask
5/10/2017
10
Nurses Role and Responsibility as Assistant
• Remain at bedside and available to assist when needed
• Provide oversight of sterile procedure and may interrupt and/or stop procedure if a break in sterility has been noted
• Visualize guide wire has been removed and disposed of in regular trash according to UCSD MC MCP 813.3, “Hazardous Materials and Hazardous Waste Management”
Procedures and Responsibilities
• Once the central catheter is placed, a chlorhexidine impregnated disc (BioPatch) and sterile dressing will be applied with current date, time and initialed
• A gauze and transparent semipermeable membrane dressing may be applied if oozing at the insertion site is anticipated.• Oozing gauze dressing will then be
changed within 24 hours• Dry gauze dressing will be changed in 48
hours
jlz/July2011
jlz/July2011
To view the Procedure Note in Epic, click on Notes, then the Proc tab. Search for the date and time the procedure was
completed
Placement and Documentation
• Central line placement is verified with x-ray or fluoroscopy to identify the location of the tip of the catheter.
• Documentation is completed in Epic under Results Review / Imaging that identifies the location of the catheter tip.
3) Chlorhexidine Skin Antisepsis• Using Chlorhexidine than any other antiseptic agents
• Technique is as follows:• Chlorhexidine 2%/ Isopropyl alcohol 70%• Pinch wings on the applicator to break down the ampule.
Hold the applicator down.• Apply solution with back & forth FRICTION for at least 30 (2
min femoral) seconds. Do not wipe or blot.• AIR Dry completely
Institute of Healthcare Improvement (IHI) 62
CHLORHEXIDINE GLUCONATE
PROS:• Disrupts microbial cell membrane
and precipitates cell contents• Broad spectrum against bacteria,
fungi and viruses• Persistent: binds to skin proteins
and is active for 48 hours after application
• Antibacterial properties work on contact, but must dry thoroughly before proceeding with any procedure
CONS:• Skin allergy (very unlikely)• Not recommended for use in NICU
or children under 2 months of age
• For insertion skin prep• CHG vs Iodine reduced the
risk of catheter related infection by 49%
• Leading to a cost savings of $113 per catheter
Alcohol Hand Gel 60 seconds
Maximum Sterile
Barriers 50 seconds
Chloraprep Apply 30 seconds
Dry ~ 40 seconds _______
3 minutes
3 Minutes to Save a Life. . .PRICELESS
4) Best Site Selection
• Use subclavian site unless medically contraindicated (e.g. patient has an anatomic deformity, coagulopathy, or has renal disease that may require dialysis)• Subclavian vein site with lower risk of infection than the
internal jugular vein• Femoral site with greater risk of infection in adults
Institute of Healthcare Improvement (IHI) 65
Avoidance of the Femoral Vein!!!
(Except in emergencies)
Internal Jugular or Subclavian Placement
Why might a physician prefer to insert in the Jugular vein?
•Pneumothroax
•Subclavian artery puncture
•Subclavina vein laceration
•Subvlavian vein stenosis
•Hemothorax
•Thrombosis
•Air embolism
•Catheter misplacement
5/10/2017
12
5) Daily Review of Line Necessity
• Removal of unnecessary lines
• Include daily review of line necessity as part of your multidisciplinary rounds • State the line day (e.g. “Today is
line day 6”).
• Record time/date of line placement
Institute of Healthcare Improvement (IHI) 67
Probability of CLABSI as Catheter Days Progress
Catheter Days Probability
By day 15 6 in 100
By day 25 14 in 100
By day 30 21 in 100
By day 320 53 in 100
McLaws M.L., Berry G.: Nonuniform risk of bloodstream infection with increasing central
venous catheter days. Infect Control Hosp Epidemiol 26:715–719, Aug. 2005.
What does this mean for you and your practice?
Question…
•Can I implement most of the central line bundle but exclude some items?
•How do I address line necessity with the team?
CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections
Major areas of emphasis include:
1.Using maximal sterile barrier precautions during central venous catheter insertion;
2.Using a > 0.5% chlorhexidine (CHG) preparation with alcohol for skin antisepsis;
3.Avoiding routine replacement of central venous catheters as a strategy to prevent infection; and
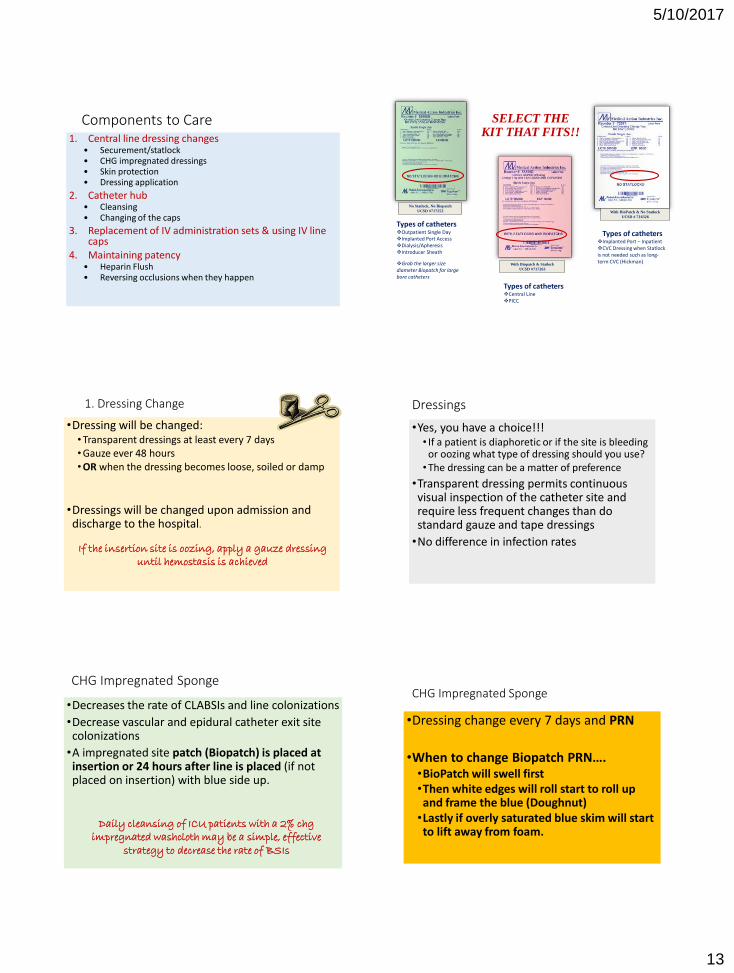
2. Catheter hub • Cleansing • Changing of the caps
3. Replacement of IV administration sets & using IV line caps
4. Maintaining patency• Heparin Flush• Reversing occlusions when they happen
No Statlock, No Biopatch
UCSD #717253
With Biopatch & Statlock
UCSD #717263
With BioPatch & No Statlock
UCSD # 716326
Types of cathetersOutpatient Single DayImplanted Port AccessDialysis/ApheresisIntroducer Sheath
Grab the larger size diameter Biopatch for large bore catheters
SELECT THE KIT THAT FITS!!
Types of cathetersCentral LinePICC
Types of cathetersImplanted Port – InpatientCVC Dressing when Statlockis not needed such as long-term CVC (Hickman)
1. Dressing Change
•Dressing will be changed:• Transparent dressings at least every 7 days• Gauze ever 48 hours• OR when the dressing becomes loose, soiled or damp
•Dressings will be changed upon admission and discharge to the hospital.
If the insertion site is oozing, apply a gauze dressing until hemostasis is achieved
Dressings
•Yes, you have a choice!!!• If a patient is diaphoretic or if the site is bleeding
or oozing what type of dressing should you use?• The dressing can be a matter of preference
•Transparent dressing permits continuous visual inspection of the catheter site and require less frequent changes than do standard gauze and tape dressings
•No difference in infection rates
CHG Impregnated Sponge
•Decreases the rate of CLABSIs and line colonizations
•Decrease vascular and epidural catheter exit site colonizations
•A impregnated site patch (Biopatch) is placed at insertion or 24 hours after line is placed (if not placed on insertion) with blue side up.
Daily cleansing of ICU patients with a 2% chg impregnated washcloth may be a simple, effective
strategy to decrease the rate of BSIs
CHG Impregnated Sponge
•Dressing change every 7 days and PRN
•When to change Biopatch PRN….•BioPatch will swell first•Then white edges will roll start to roll up and frame the blue (Doughnut)
•Lastly if overly saturated blue skim will start to lift away from foam.
5/10/2017
14
1. Place BIOPATCH Dressing around catheter with blue side up and white
foam side next to patient's skin. Blue product placement indicator facilitates
correct application.
2. To ensure easy removal, place BIOPATCH Dressing so that catheter rests on
or near the radial slit. Edges of slit must touch to assure efficacy.
3. Secure catheter and BIOPATCH Dressing with transparent film dressing.
Assure complete contact between skin and BIOPATCH Dressing.
4. To remove: Lift corner of transparent film dressing and stretch away from
catheter, holding catheter in place.
5. BIOPATCH Dressing will remain attached to transparent film dressing,
making removal simultaneous.
Transparent Semipermeable Membrane (TSM)
•Gently smooth dressing from center toward edge; do not apply excessive tension as skin shearing may result.
•Change transparent semipermiablemembrane every 7 days or PRN.
• Lift corner of dressing and stretch away from catheter holding catheter in place. Alcohol wipes help!
• Change dressing immediately if integrity is compromised, and/or there is excessive drainage or moisture.
Lets Practice – Remove your tegaderm
Question…
•For a hemodialysis catheter, if the dressing becomes loose, soiled or damp, can you as the primary nurse change it? • No! Call the dialysis nurse and they will come to
change it.
•If you have a transparent membrane dressing and gauze is over the site, how often do you need to change it? • Every 48 hours
Application of StatLock
• Securing device will be changed upon admission, every 7 days with the dressing change or when the dressing becomes loose, soiled or wet.
• Use painting motion for skin prep & ALLOW TO DRY
• Use Alcohol to remove!
Use a sutureless securement device to reduce the risk of infection for intravascular catheters. Category II
1) “Scrub the Hub”
Every hub every time… using alcohol and friction in a twisting motion as if you were juicing an orange for at least 15 seconds.
83
Kaler, Wendy; Chinn, Raymond (2007) Successful Disinfection of Needleless Access Ports: A Matter
of Time and Friction. Journal of the Association for Vascular Access, Volume 12, Number 3, pp.
140-142
Why are Caps Important
• Entry into vascular system
• There are a lot of caps out there,• Why we use this one here….
• Internal fluid path
• Small dead space
• The cap is changed every 96 hours unless signs of blood, precipitate, leaks or cracks are noted or the septum is no longer intact.• Change the cap with the tubing…clean to clean
5/10/2017
15
To be used on all patients with CVCs
You asked the question…
• Inconsistent compliance with scrubbing hub prior to accessing line
•“Scrub the Hub” Remind one another. NURSING ACCOUNTABILITY!
•What do you do during a blood draw? Or if you disconnect?
Time to “change” the caps on your line!
•Turn to your partner and explain how you would change the cap• Prime your tubing• Scrub the connection • What happens every time you open the line?• Did you clamp your catheter?
Where do you document?
Change the needleless components at least as frequently as the administration set. There is no benefit to changing these more frequently
than every 96 hours. Category II
PROTECTION
COMPONENTHIGHLIGHTS OF THE RATIONALE AND DIRECTIONS
HAND
HYGIENE
Rationale: Removes or destroys disease-producing microorganisms that can cause illness / infection
Directions: Water and soap, lather for 15 seconds. Hand Sanitizer, coat all surfaces of hands and rub until dry.
CHG SKIN
PREP
Rationale: Skin asepsis
Directions: Use back and forth strokes for 30 seconds (2 minutes for wet sites). ALLOW TO THOROUGHLY AIR DRY
NO STING SKIN
BARRIER
Rationale: Forms a breathable, transparent coating on the skin designed to protect intact or damaged skin from tape trauma
Directions: Apply a uniform coating of film as a frame for where the dressing will go, allow to air dry
Directions: Prep, Press (tabs), Peel and Place. To remove, disengage and dissolve, alcohol wipes help! Change with dressing
change.
CHG
impregnated
disc(BIOPATCH)
Rationale: Decreases line colonizations for vascular, arterial and epidural catheter exit sites
Directions: Change with dressing and PRN. Ensure skin prep is dry, place BioPatch around catheter printed side up. Align
Cather with radial slit at slight diagonal and ensure edges of slit touch.
Rationale: Provides a barrier to external contaminants through effective moisture management, firm hold, and gentle
release
Directions: Gently smooth dressing from center toward edge; do not apply excessive tension as skin shearing may result.
Change PRN and every 7 days. To remove lift corner of dressing and stretch away from insertion site holding catheter in
place, alcohol wipes help too!
Rationale: Protect entry into the vascular system. Needles access system
Directions: The cap is changed every 96 hours unless signs of blood, precipitate, leaks or cracks are noted or the septum is
no longer intact. Change the cap with the tubing…clean to clean
CUROS PORT
PROTECTOR
Rationale: Disinfects ports, port care needs to be optimized, including consistent and proper disinfection of
the hubs.
Directions: Place Curos on port following port access. Needs 3 minutes to disinfect before use again. Scrub
HUB in between multiple IVP injections.
ALCOHOL
PREP PAD
Rationale: Friction and time disinfects the port and hub prior to entry or changing of the port
Directions: Anytime a Curos in not in place, hub scrub for 15 seconds and allow to dry
DRESSING
CHANGE KITS
Rationale: All needed supplies are available in one package making dressing changes easier and consistent
every time.
Directions: Change PRN and every 7 days. Date dressing with the date it was changed!
Rationale: Reduced risk of bacterial colonization in IV tubing.
Directions: Change tubing every 96 hours, 24 hours for TPN. All IV tubing will be labeled with Day of Week
sticker, time when tubing is to be changed. Initial label!
FLUSHING
Rationale: A clot and/or fibrin sheath serves as a nidus for bacteria. Keep the line patent with flushing and / or
declotting as needed
Directions: Use a 10mL NS syringe every shift, before and after each infusion (if line is locked) and PRN. Use 20
mL NS flush after administration of blood, blood products or blood sampling.
DECLOTTING
Rationale: Use of Cathflo for a partially / fully occluded or sluggish / clotted line opens the line, prevents
infection and a delay in intravenous therapies
Directions: RN must complete competency during orientation
CHG BATHING
ALL Pt’s with
CVAD
Rationale: Decreases Bio-burden
Directions: Daily bathing by using 1 of the 3 products available. Avoid using chg bathing products in the groin
and above the neck.
ENVIROMENT
AL WIPE
DOWNS
Rationale: To decrease the bio-burden on frequent touch points in patient rooms and transmission out of the
room and into the unit.
Directions: Twice a day clean the unit (computers, counters, door knobs, railing, etc.)
Replacement of IV Administration Sets•Lipids and blood products (enhance microbial growth)• Change every 24 hours
•All other IV administration sets• No more frequently than every 96
hours• Safe and cost effective
Remember to use the caps to keep the IV lines clean once they are disconnected from the hub. NO circling back in!
What about all those piggybacks hanging there?
And extra sets?
Replace caps at the same time of the set change
5/10/2017
16
Do you need to replace your IV tubing when you have a new
PICC Line or Central Line placed?
Intravenous Therapy Policy
All IV tubing will be labeled with date and time tubing is to be changed.
There is a big difference in tubing changed on 5/4 at 0100 or 2300
Don’t
forget to
write the
date and
time!
Ara
n T
ava
ko
li, RN
, AO
CN
S,
5/5
/08
Keep your line patent!
•This will reduce CLABSI. A clot and/or fibrin sheath serves as a nidus for bacteria.• Adherence – a CVC is a foreign body! Biofilm potentiates
pathogenicity of microbes• Host proteins (fibrinogen, fibronectin) are commonly present of catheters
and bound by clumping factos (ClfA, ClfB)
• S. aureus can adhere to host proteins
• Microbial organisms can enhance adherence by producing extracellular polymeric substance (EPS)
What interventions do we use to maintain patency?
Maintaining Patency
• Blockage disposes the device to • Damage, infection, inconvenience and disruption of drug
therapy
• Most common cause is a blood clot• Precipitate formation (inadequate flushing)• Fat emulsions• Fibrin Sheath
• Maintain patency by continuous IV or intermittent flushing
Flush To Prevent Occlusion Avoid this Open the flow
Flushing• Syringe Size - use 10 mL will be used for flushing and checking
patency
• Lines are flushed when:• Accessed
• Locked
• After CVC blood draws (20 mL)
• Lines with continuous IV fluids running, will be flushed with saline after lab draws.
• Never forcefully flush a CVC!
• Always use the PUSH-PAUSE technique when flushing to create turbulence in the line.
Flow Characteristics
Turbulent FlowLaminar Flow
5/10/2017
17
CVC Flushing
Short term CVC 300 Units
PICC Line
Normal Saline
Or Heparin 300 units (if non-valved)
SubQ Port 500 Units
Dialysis/Pheresis4% sodium citrate by dwell volume
Evaluation ofCatheter Occlusion
• Ability to infuse
• Inability to aspirate
Activity
• Blood Draw
• Transfusion
• Reflux of blood
• Failure to flush
• Incompatible medication
• Poor solubility
• Inability to infuse
• Inability to aspirate
Cause
• Blood Clot
• Blood Clot
• Blood Clot
• Blood Clot
• Precipitate
• Precipitate
Declotting CVCs
• Attempt corrective action.• Rule out tubing kinks and precipitate.• Have patient take deep breaths and cough.• Have patient raise arm on side of catheter above the head.• Instruct the patient to lie flat or if lying down sit up (if
change of position is indicated).• Attempt to flush the catheter with 10 mL of normal saline
and attempt to withdraw blood.
• If unsuccessful, move to the following steps.• Obtain order for tPA for declotting, may repeat 2 times• Syringe with thrombolytic (Alteplase),• Two (2) 10 mL syringes: empty, normal saline flush• Only administered by trained RNs• Takes 30 to 120 minutes
It flushes great, but I don’t get a blood return?
• Great question, here is the answer whether it is a port or a PICC or a CVC. • When there is no blood return the nurse needs to problem
solve!
• If you do not have a blood return follow the policy.
• Fibrin tail on the tip of the catheter • would explain the great flushing, but poor return. • The fibrin tale acts as a lid, opening with flushing but closing over
the tip with withdrawing. • This can also serve as a nidus for infection, so dissolve and see if
that fixes the line!• If that still does not work, then it is time for a flow/dye study.
• Port specific, sometime the needle is at an angle, so you can remove it and access again with a new needle and see if that helps.
Central Line RemovalGeneral Considerations
• CVCs are removed when therapy is completed, a mechanical malfunction has occurred, the catheter has become occluded or mal-positioned, or the patient has developed a central line associated blood stream infection (CLABSI).
• The nurse must validate that the catheter has been removed intact in documentation.
• Air embolism can occur during the removal of the catheter. The pathologic effects depend on the volume and rate of air aspirated.
• Coagulation status and vital signs should be assessed prior to catheter removal.
• MD order required for catheter removal. MD to culture catheter tip if required.
Removal of Central Lines
•Obtain an MD order to remove central line.
•CVADs, PICCs & Midlines can be removed by RN’s who have obtained bedside competency evaluation by competent staff member.
5/10/2017
18
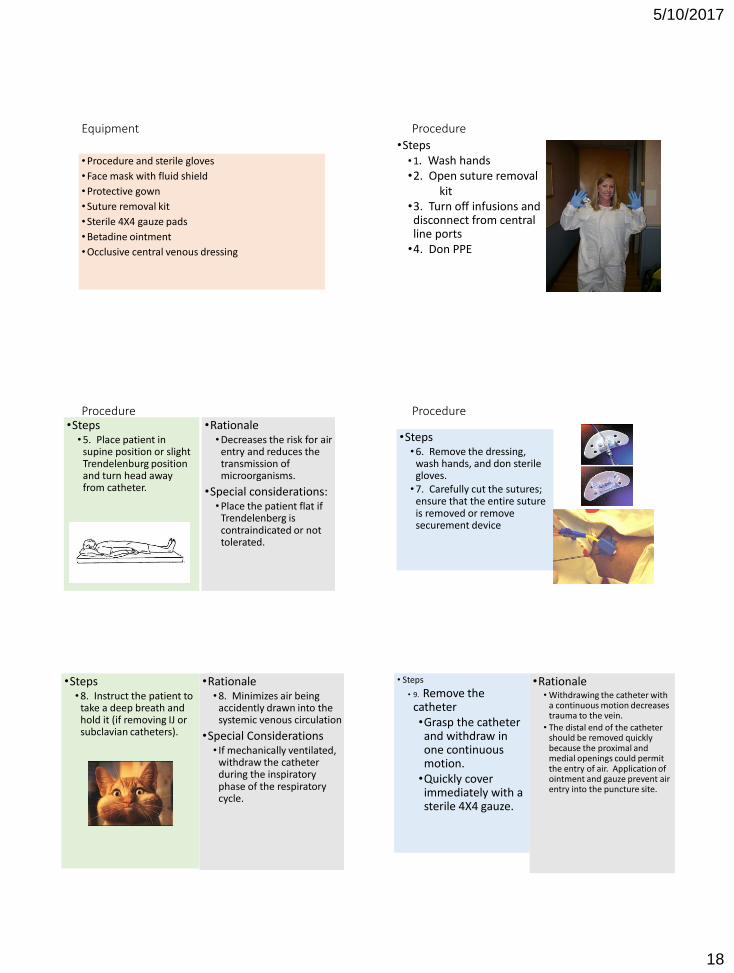
Equipment
• Procedure and sterile gloves
• Face mask with fluid shield
• Protective gown
• Suture removal kit
• Sterile 4X4 gauze pads
• Betadine ointment
• Occlusive central venous dressing
Procedure
•Steps• 1. Wash hands•2. Open suture removal
kit•3. Turn off infusions and disconnect from central line ports
•4. Don PPE
Procedure•Steps
• 5. Place patient in supine position or slight Trendelenburg position and turn head away from catheter.
•Rationale• Decreases the risk for air
entry and reduces the transmission of microorganisms.
•Special considerations:• Place the patient flat if
Trendelenberg is contraindicated or not tolerated.
Procedure
•Steps• 6. Remove the dressing,
wash hands, and don sterile gloves.
• 7. Carefully cut the sutures; ensure that the entire suture is removed or remove securement device
•Steps• 8. Instruct the patient to
take a deep breath and hold it (if removing IJ or subclavian catheters).
•Rationale• 8. Minimizes air being
accidently drawn into the systemic venous circulation
•Special Considerations• If mechanically ventilated,
withdraw the catheter during the inspiratory phase of the respiratory cycle.
• Steps
• 9. Remove the catheter•Grasp the catheter and withdraw in one continuous motion.
•Quickly cover immediately with a sterile 4X4 gauze.
•Rationale• Withdrawing the catheter with
a continuous motion decreases trauma to the vein.
• The distal end of the catheter should be removed quickly because the proximal and medial openings could permit the entry of air. Application of ointment and gauze prevent air entry into the puncture site.
5/10/2017
19
Procedure
•Steps:•10. Maintain pressure for a minimum of 5 minutes or until hemostasis is achieved.
•Recheck site after 15 minutes, 30 minutes, 60 minutes, and 120 minutes.
• Rationale:
• Prevents bleeding and hematoma formation.
• Special considerations:
• Longer periods of direct pressure may be needed to achieve hemostasis in patients receiving systemic heparin or thrombolytics or those who have a coagulopathy.
Procedure
•Steps• 11. Apply an occlusive,
sterile dressing over the site.
• 12. Inspect the catheter after it is removed.
• 13. Reposition the patient.• 14. Discard supplies in
appropriate waste containers, wash hands.
•Rationale• Minimizes the risk for
air entry and infection at the site and ensures that the entire catheter has been removed.
Documentation
• Patient and/or family education
• Date and time of catheter removal
• Site assessment
• Inspection of catheter
• Application of occlusive dressing
• Patient tolerance of procedure
• Unexpected outcomes and interventions Between June 2009 and June 2011, the National Patient Safety Agency (NPSA)
received nine incident reports describing how patients suddenly deteriorated
following the removal of a central line. In all reports, it was stated that nurses had
not followed the correct procedures, but had removed the catheter while the
patient was sitting up.
Management of Suspected Air Embolus
• Signs and symptoms• Confusion• Lightheadedness• Anxiety• Unresponsiveness
• Interventions• Call MD• Turn patient on left side
in Trendelenburg position• Administer oxygen
PICC Catheter Removal
•Requires physician order
•Only qualified personnel may remove
•Technique:• Patient supine• Arm below the level of heart• Remove in short 1-2 inch increments• Never pull with force
•Apply occlusive dressing
•Document catheter intact, site
5/10/2017
20
Difficult Removal of PICC
•Venospasm typical but rare cause• Apply warm moist heat for 20-30 minutes
• Allow patient to relax
• If resistance still met, redress and notify MD
Discharging with a Line
•Provide Education & Document • Follow-up• Signs and symptoms to report• Flushing • What about Curos?
•Work with CM for home health / supplies for catheter care
References• Allegranzi B., Pittet D.: Healthcare-associated infection in developing countries: simple solutions to
meet complex challenges. Infect Control Hosp Epidemiol 28:1323–1327, Dec. 2007.
• Cimiotti J.P., et al.: Impact of staffing on bloodstream infections in the neonatal intensive care unit. Arch Pediatr Adolesc Med 160:832–836, Aug. 2006.
• Damani N.: Simple measures save lives: an approach to infection control in countries with limited resources. J Hosp Infect 65 Suppl 2:151–154, Jun. 2007.
• Graves N., et al.: The effect of healthcareacquired infection on length of hospital stay and cost. Infect Control and Hosp Epidemiol 28:280–292, 2007.
• Horan T.C., Andrus M., Dudeck M.A.: CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36:309– 332, Jun. 2008.
• Institute for Healthcare Improvement. 5 Million Lives Campaign. Getting Started Kit: Prevent Central Line Infections How-to-Guide. Cambridge, MA: Institute for Healthcare improvement. 2008.
• Institute for Healthcare Improvement. Implement the Central Line Bundle. Cambridge, MA: Institute for Healthcare Improvement. http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementtheCentralLineBundle.htm (accessed Oct. 19, 2009).
• Institute for Safe Medication Practice (ISMP): Failure to cap IV tubing and disinfect IV ports place patients at risk for infections. Jul. 26, 2007. http://www.ismp.org/Newsletters/acutecare/articles/20070726.asp (accessed Oct. 19, 2009).
• The Joint Commission: Measuring Hand Hygiene Adherence: Overcoming the Challenges. Oakbrook Terrace, IL: The Joint Commission, 2009.
References• Kaler, W & Chinn, R. (2007). Successful Disinfection of Needleless Access Ports: A Matter of Time
and Friction. JAVA, 12(3), 140-142
• Koll B.S., et al.: The CLABs collaborative: a regionwide effort to improve the quality of care in hospitals. Jt Comm J Qual Patient Saf 34:713, Sep. 2009.
• Maki D.G., Mermel L.A.: Infections Due to Infusion Therapy. In Jarvis W.R. (ed.): Bennett and Brachman's Hospital Infections, 5th ed. Philadelphia, PA: Wolters Kluwer/Lippincott, Williams & Wilkins, 2007, pp. 611–647.
• Maki D.G., Mermel L.A.: Infections Due to Infusion Therapy. In Jarvis W.R. (ed.): Bennett and Brachman's Hospital Infections, 5th ed. Philadelphia, PA: Wolters Kluwer/Lippincott, Williams & Wilkins, 2007, pp. 611–647.
• Marschall J., et al.: Strategies to prevent central line–associated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 29 Suppl 1:S22–30, Oct. 2008.
• Marschall J., et al.: Strategies to prevent central line–associated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 29 Suppl 1:S22–30, Oct. 2008
• Marschall J.: Catheter-associated bloodstream infections: looking outside of the ICU. Am J Infect Control 36:S172 e175–178, Dec. 2008.
• McGoldrick M.: Preventing central line– associated bloodstream infections and the Joint Commission's Home Care NationalPatient Safety Goals. Home Healthc Nurse 27:220–228; quiz 229–230, Apr. 2009.
• McGoldrick M.: Preventing central line–associated bloodstream infections and the Joint Commission's Home Care National Patient Safety Goals. Home Healthc Nurse 27:220-228; quiz 229–230, Apr. 2009.
References• Menyhay, S. & Maki, D. (2006). Disinfection of Needleless Catheter and Access Ports with Alcohol
May not Prevent Microbial Entry: The Promise of a Novel Antiseptic Barrier Cap. Infection Control Hospital Epidemiology. 27, 23-27.
• Scott R.D.: The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Division of Healthcare Quality Promotion, National Center for Preparedness,Detection, and Control of Infectious Diseases. Coordinating Center for Infectious Diseases. Centers for Disease Control and Prevention. Mar. 2009.
• Taylor B.B., et al.: Do medical inpatients who report poor service quality experience more adverse events and medical errors? Medical Care 46(2):224–228, 2008.
• Taylor R.W., Palagiri A.V.: Central venous catheterization: concise definitive review. Crit Care Med 35:1390–1396, May 2007.
• Tsuchida T., et al.: The effectiveness of a nurse-initiated intervention to reduce catheter-associated bloodstream infections in an urban acute hospital: an intervention study with before and after comparison. Int J Nurs Stud 44:1324–1333, Nov. 2007.
• University of Pennsylvania School of Medicine: Road map for elimination of central line-associated bloodstream infections. ScienceDaily, Mar. 27, 2009. http://www.sciencedaily.com/releases/2009/03/090321103805.htm (accessed Oct. 19, 2009).
• Woeltje K.F., et al.: Automated surveillance for central line-associated bloodstream infection in intensive care units. Infect Control Hosp Epidemiol 29:842–846, Sep.2008.
• World Health Organization: WHO Guidelines on Hand Hygiene in Health Care. First Global Patient Safety Challenge: Clean Care is Safer Care. 2009. http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf (accessed Oct. 19, 2009).